Back to Journals » Vascular Health and Risk Management » Volume 19
Structured Rehabilitation for Patients with Atrial Fibrillation Based on an Integrated Care Approach: Protocol for a Prospective, Observational Cohort Study
Authors Zhang H, Jin Z, Wang H, Guo Y ![]() , Lip GYH
, Lip GYH
Received 10 February 2023
Accepted for publication 27 July 2023
Published 31 July 2023 Volume 2023:19 Pages 485—494
DOI https://doi.org/10.2147/VHRM.S407974
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Hui Zhang,1 Zhigeng Jin,1 Hao Wang,2 Yutao Guo,1,3 Gregory YH Lip3,4
1Medical School of Chinese PLA, Department of Pulmonary Vessel and Thrombotic Disease, Sixth Medical Center, Chinese PLA General Hospital, Beijing, People’s Republic of China; 2Department of Cardiology, Second Medical Centre, National Clinical Research Centre for Geriatric Diseases, Chinese PLA General Hospital, Beijing, People’s Republic of China; 3Liverpool Centre for Cardiovascular Sciences, University of Liverpool and Liverpool Heart & Chest Hospital, Liverpool, UK; 4Aalborg Thrombosis Research Unit, Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
Correspondence: Yutao Guo, Department of Pulmonary Vessel and Thrombotic Disease, Six Medical Center, Chinese PLA General Hospital, 5 Fucheng Road, Beijing, 100048, People’s Republic of China, Email [email protected]
Background: Guideline-recommended integrated care based on the ABC (Atrial fibrillation Better Care) pathway for “general” patients with atrial fibrillation (AF) improves clinical outcomes, as demonstrated in our prior mobile Atrial Fibrillation Application (mAFA)-II cluster randomized trial. The present study aims to investigate whether mAFA III-supported structured follow-up rehabilitation packages adapted to patient risk profiles and different treatment patterns (eg, for patients receiving drug treatment only, AF ablation, or left atrial appendage occlusion [LAAO]) will improve guideline adherence and reduce the risk of adverse cardiovascular events.
Methods and Analysis: In this prospective, observational mAFA III pilot cohort study, patients with AF aged ≥ 18 years will be enrolled using the mAFA III App for self-management. Assuming an annual rate of composite outcome of “ischaemic stroke or systemic embolism, all-cause death and cardiovascular hospitalization” of 29.3% for non-ABC pathway compliance compared with 20.8% for ABC pathway compliance, at least 1475 patients would be needed to detect the outcome of the A, B and C components of the ABC pathway, assuming a withdrawal rate of 20% in the first year. The primary endpoint is adherence to guidelines regarding the A, B and C components of the ABC pathway. Ancillary analyses will be performed to determine the impact of the ABC pathway using smart technologies on the outcomes among the “high-risk” population (eg, ≥ 75 years old, with multimorbidities, with polypharmacy) and the application of artificial intelligence machine-learning AF risk prediction management in assessing AF recurrence. The individualised anticoagulants with AF burden will be monitored by smart devices.
Trial Registration Number: ISRCTN13724416.
Keywords: atrial fibrillation, rehabilitation, mobile health
Introduction
Atrial fibrillation (AF) is an increasing global epidemic and public health challenge.1 Guideline-recommended integrated care based on the ABC (atrial fibrillation better care) pathway for “general” patients with AF improves clinical outcomes, as demonstrated in our prior mobile Atrial Fibrillation Application (mAFA)-II cluster randomized trial. The ABC pathway refers to the following: Avoid stroke, Better symptom control, and Cardiovascular risk and comorbidity management, and it has been recommended in updated guidelines for the management of AF.2
The inappropriate prescription of oral anticoagulants (OACs) is common. Many AF patients are not anticoagulated according to their CHA2DS2-VASc (Congestive heart failure; Hypertension; Age ≥75 years; Diabetes Mellitus; Stroke; Vascular disease; Age 65–74 years; Sex category) risk score.3 In a large US administrative database, 13.3% of AF patients with no renal indication for dose reduction were underdosed.4 Approximately 3 in 10 Asian AF patients were treated with off-label dosing of nonvitamin K antagonist oral anticoagulants (NOACs) in daily practice.5 Of concern, only 40.2% of AF patients on OACs were both adherent and persistent at 1 year in UK primary care,6 while in a Danish national patient registry, half of the AF patients discontinued NOAC therapy after one year.7 Noncompliance with anticoagulant guidelines for AF is associated with an increased risk of adverse outcomes, including ischaemic stroke, bleeding, and death.8
In China, there is an increasing trend for more OAC use, especially in the era of NOACs; however, there remains much heterogeneity in OAC use. The 2019 Clinical Performance and Quality Measures for Atrial Fibrillation in China demonstrated that the prescription rate of OACs upon discharge was 66% in Class III hospitals but only 25.8% in Class II hospitals in 2018.9 A screening program with handheld single-lead electrocardiography (ECG) in Chinese community health centres involving 4531 participants showed that only 20% of identified AF patients were receiving OACs (mainly warfarin), but 85% should have been administered guideline-recommended anticoagulants.10
In our mobile health (mHealth) technology in improving screening and integrated care for atrial fibrillation (mAFA II) study, mHealth supported integrated care based on the ABC pathway and improved the adherence to OAC (mainly NOAC) use from 63.4% at baseline to 73.2% in one year11 and reduced the short- and long-term composite outcome of ischaemic stroke, bleeding, and rehospitalization.12,13
Indeed, mHealth and other innovative technologies are proposed for arrhythmia management.14,15 Nonetheless, mHealth-supported guideline-recommended treatment adoption in routine clinical care needs to be further clarified and adapted to the patient’s risk profile and specific patient groups (eg, for patients receiving drug treatment only, AF ablation, or left atrial appendage occlusion [LAAO]).
Moreover, the elderly patient population may have more limited technical skills related to smart technology use, while they are likely to have the most possible benefit from adherence to the guidelines. Multimorbidity and polypharmacy are common among patients with AF, and up to 40% of AF patients suffer more than four comorbidities.16,17 The current mHealth opportunities, combined with clinical pathways, need to be explored in this “high-risk” population.
The present study aims to investigate whether mAFA-supported structured follow-up rehabilitation packages adapted to patient risk profiles and different treatment patterns (eg, for patients receiving drug treatment only, AF ablation, or LAAO) will improve guideline adherence and reduce the risk of adverse cardiovascular events.
Primary and Secondary Hypotheses
The primary hypothesis is to analyse adherence to guidelines based on the ABC pathway (Avoid stroke, Better symptom control, and Cardiovascular risk or comorbidity management) with mHealth-supported structured follow-up rehabilitation packages adapted to the patient’s risk profile and different management patterns (eg, for patients receiving drug treatment only, AF ablation, or LAAO).
The secondary hypotheses are to explore the application of artificial intelligence machine-learning AF risk prediction management in AF recurrence, the impact of the ABC pathway upon smart technologies on outcomes among a “high-risk” population (eg, ≥75 years old, multimorbidities, polypharmacy), and the influence of mAFA III system support in reducing the heterogeneity of treatment among primary care/Class-I, Class-II, and III hospitals.
Methods
The present study is a prospective, multicentre, observational registry (Figure 1). The study was approved by the Central Medical Ethics Committee of Chinese PLA General Hospital (Approval number: HZKY-PJ-2021-13) and was also approved by local institutional review boards. All patients will provide written informed consent. The study was performed in accordance with the Declaration of Helsinki document on human research ethics. The study is registered on https://www.isrctn.com/ISRCTN13724416 (Registration number: ISRCTN13724416).
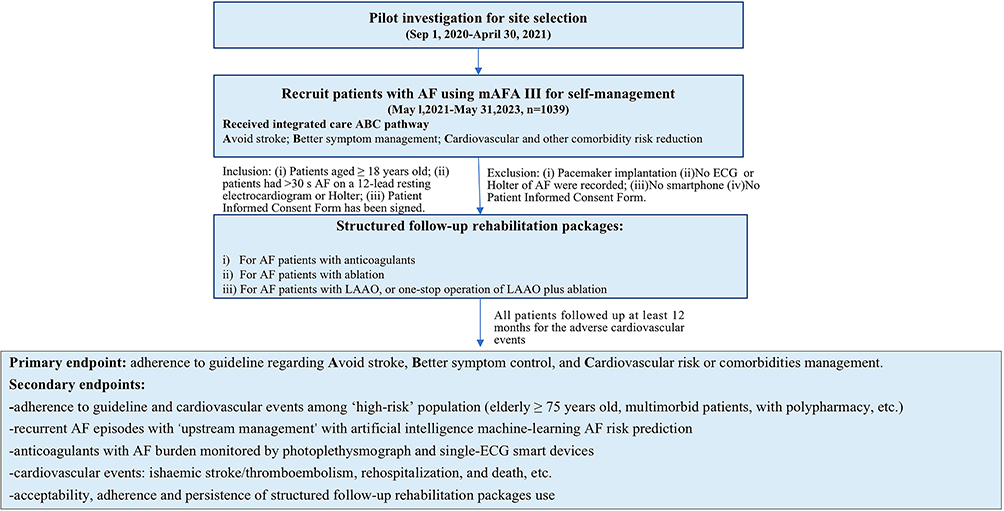 |
Figure 1 Flow chart. Abbreviations: mAFA, mobile Atrial fibrillation Application; LAAO, left atrial appendage occlusion. |
Study Population
The inclusion criteria include the following: (i) patients aged ≥ 18 years old; (ii) patients had >30-s AF on a 12-lead resting electrocardiogram or Holter; and (iii) the patient informed consent form is signed. The exclusion criteria are as follows: (i) no ECG of AF is recorded.
Patients will be consecutively recruited at each site to ensure representative inclusion of the overall population in each practice setting in China. Enrolment will occur between May 1, 2021, and May 31, 2023.
We previously developed a user-friendly mobile Atrial Fibrillation Application (mAFA) for doctors and patients for the management of AF based on the Android Operating System.18 The mAFA provides clinical decision support tools (CHA2DS2‐VASc, HAS‐BLED, SAMe‐TT2R2 scores), guideline‐based treatment recommendations, educational materials and patient involvement strategies with self‐care protocols to support implementation of the ABC pathway for integrated or holistic AF management.19
In the present study, the structured follow‐up packages guiding the rehabilitation at home have been updated for mAFA (mAFA III) and are suitable for patients receiving drug treatment only, AF ablation, or LAAO. The specified structured follow‐up package, matching the patient’s treatment pattern, was initiated when patients were discharged or after consultation in the clinic. All structured follow-up packages are compliant with the 2020 ESC Guideline on AF management2 but focus on different features of patients who received different treatment patterns.
Structured Follow-Up Rehabilitation Packages
i) For AF patients with anticoagulants or other drug treatment only who do not receive AF ablation or LAAO, the structured follow-up rehabilitation package will include ABC pathway components, timely communication, and the patient educational programme (Table 1 and Figure 2A).
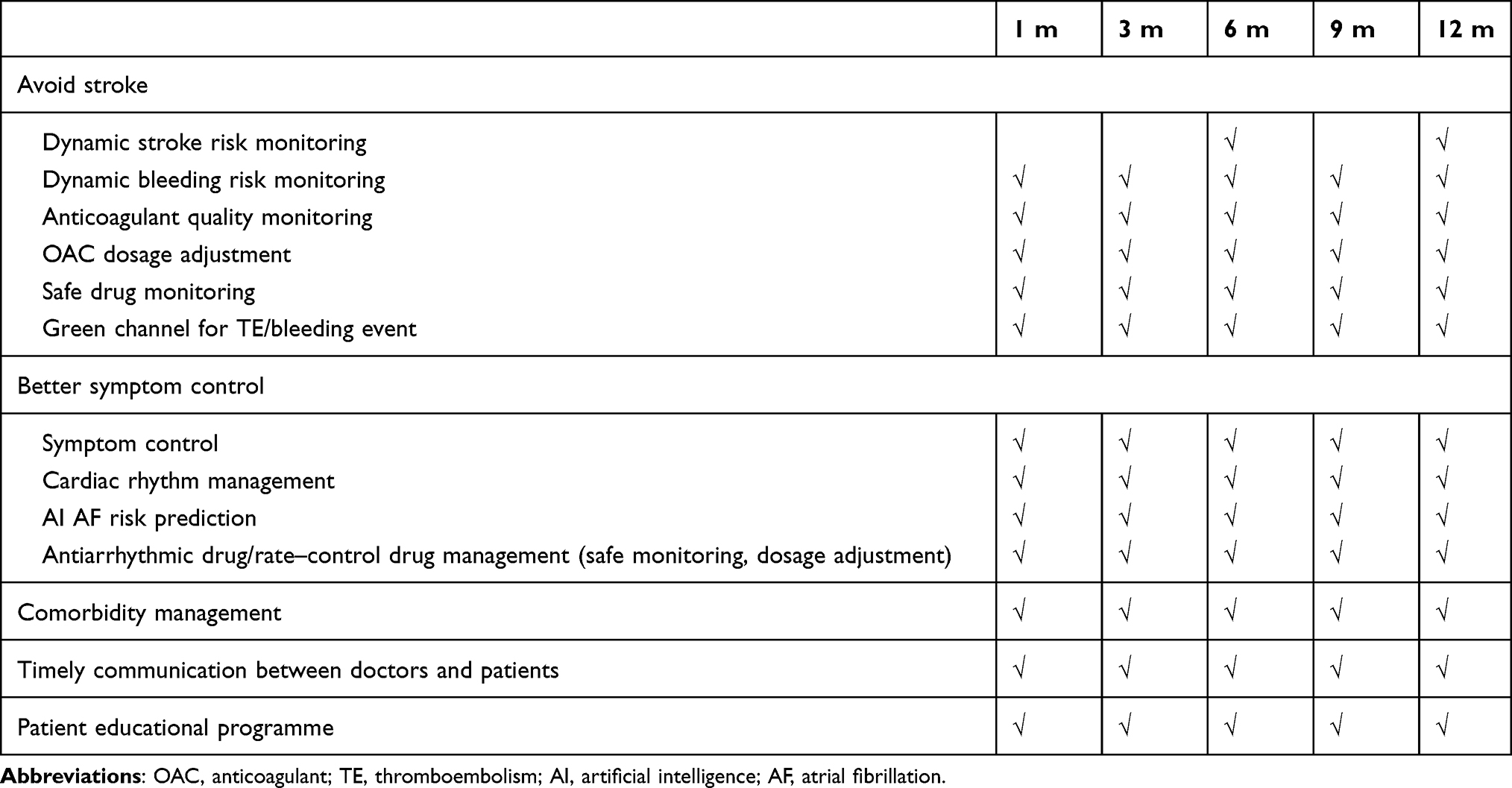 |
Table 1 Structured Follow-Up Rehabilitation Package for AF Patients Not Undergoing Invasive Procedures |
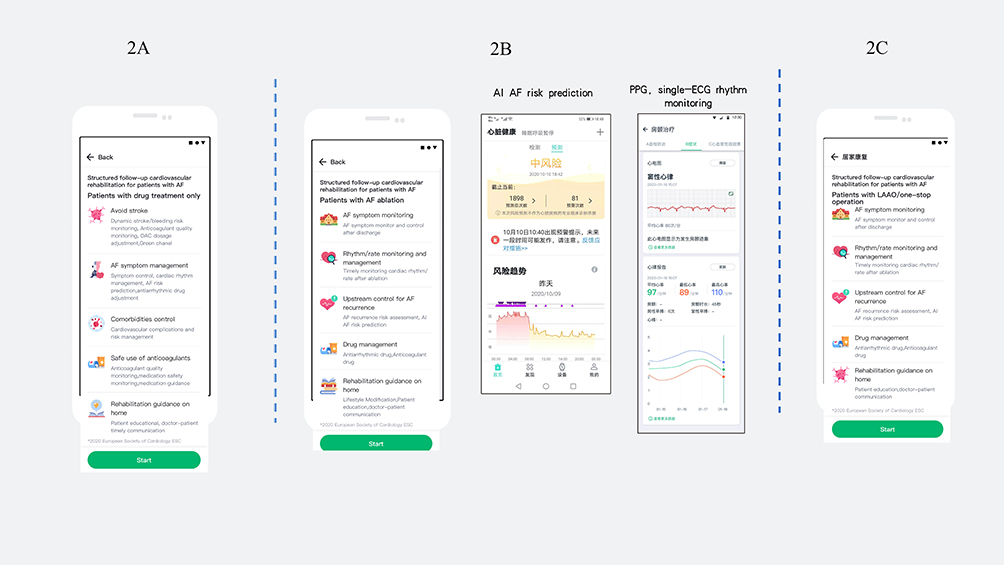 |
Figure 2 Structured follow-up rehabilitation packages. (A) Structured follow-up rehabilitation package for AF patients with drug treatment only. (B) Structured follow-up rehabilitation package for patients undergoing AF ablation. (C) Structured follow-up rehabilitation package for patients undergoing LAAO or LAAO plus ablation. Abbreviations: mAFA, mobile Atrial fibrillation Application; LAAO, left atrial appendage occlusion; AI, artificial intelligence; AF, atrial fibrillation. |
The follow-up report and recommendation based on the updated patient’s profile will be automatically generated and proposed for the patients at 1, 3, 6, 9, and 12 months by mAFA III to aid patients in self-management.
ii) For AF patients who undergo ablation, a structured follow-up rehabilitation package will include ablation complication monitoring, symptom and cardiac rhythm control after ablation, drug management, AF recurrence management, and cardiovascular risk and comorbidity management (Table 2 and Figure 2B).
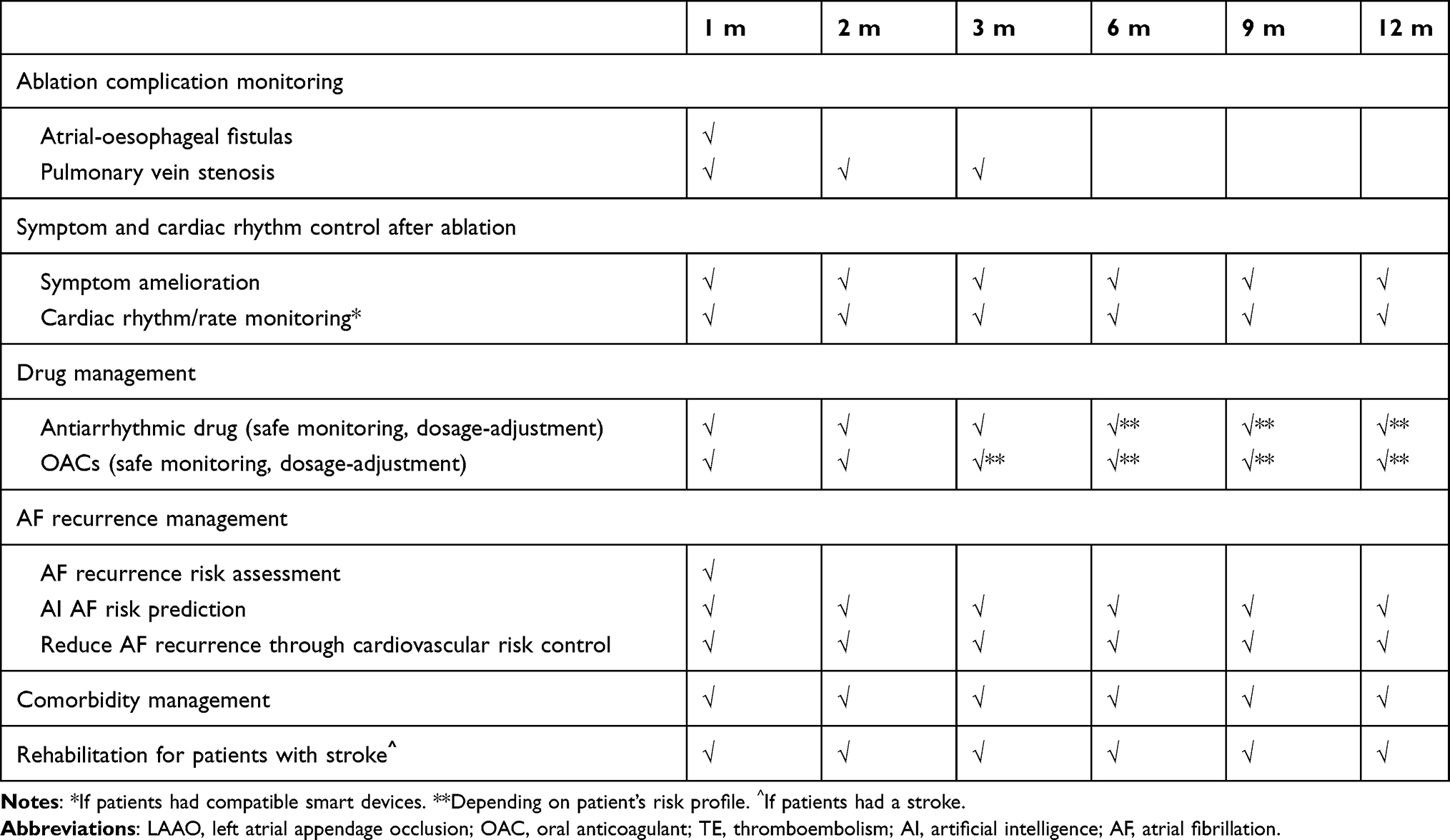 |
Table 2 Structured Follow-Up Rehabilitation Package for AF Patients with Ablation or LAAO |
The follow-up report and recommendation based on the updated patient’s profile will be generated and proposed for the patients at 1, 2, 3, 6, 9, and 12 months by mAFA III to facilitate safe drug use, to predict AF recurrence, and, thus, propose lifestyle modification to decrease the risk for recurrence after ablation.
iii) For AF patients who undergo LAAO or LAAO plus ablation, the structured follow-up rehabilitation package will include ablation/LAAO complication monitoring, symptom and cardiac rhythm control after ablation, drug management, AF recurrence management, cardiovascular risk and comorbidity management, and rehabilitation for patients with stroke (Table 2 and Figure 2C).
Rehabilitation for Patients with Stroke
For AF patients with stroke, the general condition, mobility, sense, cognitive function, speech, dysphagia at enrolment and the safety of rehabilitation at home will be evaluated by local health providers. Then, the main components of rehabilitation will be proposed as an educational program by mAFA III based on the clinical evaluation as follows: i) mobility rehabilitation: muscle strength training, muscle spasm prevention; ii) mood disorder rehabilitation: anxiety and depression scale, emotional support; iii) speech rehabilitation: communication support, oral and facial muscle training; iv) dysphagia rehabilitation: swallowing reflex training; v) cardiac and pulmonary rehabilitation; and vi) vein thromboembolism prevention: lifestyle modification, ankle pump exercise.
The follow-up report and recommendation based on the updated patient’s profile will be generated and proposed for the rehabilitation of patients at 1, 2, 3, 6, 9, and 12 months.
All patients were followed up for at least 12 months to assess adherence to guidelines and adverse cardiovascular events.
Study Outcomes
The primary endpoint is adherence to guidelines based on the ABC pathway and its individual components.
Secondary outcomes will include the following: i) the composite of stroke/thromboembolism, all‐cause death and rehospitalization. The thromboembolism endpoint includes ischaemic stroke, transient ischaemic attack (TIA), pulmonary embolism, deep vein thromboembolism (DVT), and other thromboembolisms (eg, peripheral embolism, atrial thrombus and left atrial appendage thrombus). All‐cause death will include cardiac death, vascular death and non‐cardiovascular death. Cardiac death includes death caused by ST‐segment elevation myocardial infarction/non‐ST‐segment elevation myocardial infarction (STEMI/NSTEMI), heart failure (HF), arrhythmia, cardiac perforation/tamponade and other deaths of cardiac origin. Vascular death will include death ascribed to ischaemic stroke, haemorrhagic stroke, systemic haemorrhage, peripheral embolism and pulmonary embolism. Rehospitalization for cardiovascular events will include stroke, systemic thromboembolism, angina, STEMI/NSTEMI, HF, and arrhythmia; ii) AF recurrence after 3 months following AF ablation; iii) compliance with guideline-recommended antithrombotic management for patients undergoing LAAO or ablation plus LAAO; iii) event rates: event rate for the composite of ischaemic stroke/TIA and systemic thromboembolism, HF, cardiovascular death or rehospitalization for any cardiac cause; and iv) quality of life.
Study Setting and Site Selection
A pilot investigation was performed to assess possible study sites, hospital size, and focused clinical care (pathways A, B, C), as well as the possible enrolment of AF patients per month, in terms of patients with prior stroke, with ≥ 2 comorbidities, ≥75 years old, and taking more than 5 drugs. In addition, the feasibility of systemic support was investigated among the possible study sites, including a cluster of one central research site and its affiliated small-sized hospitals.
There are 43 hospitals (35 Class III and 8 Class II hospitals). Among them, 94% (40/43) of the investigated hospitals are affiliated with approximately five medical hospitals of different sizes (Supplementary Table 1). Thus, there were an estimated 200 affiliated research centres in a total of 43 central research hospitals (mostly Class III hospitals).
The research sites in the study represent the current hierarchical medical system in China, including Class III hospitals, Class II hospitals, and Class I or community service centres, with Class III hospitals leading medical care. Community service centres are less likely to provide standard AF management (eg, prescribing oral anticoagulants, performing cardioversion), primarily due to the lower level of specialist skills and knowledge among general practices (GPs) who staff Class I or community service centres. Patients diagnosed with AF are usually referred to Class II hospitals or directly to Class III hospitals for treatment.
The medical support staff, referral evaluation, and educational program by mAFA III will be provided to facilitate standard AF management for Class II and Class I hospitals or community services centres through a cluster of one central research site (eg, Class III hospitals) plus five affiliated small-sized hospitals (eg, Class II and Class I hospitals or community service centres).
Health Provider’s Focus and Patient’s Risk Profile
Among the 47.5% of health providers who focused on the Avoid stroke pathway, 27.5% cared about pathway B, and 25.0% cared about Pathway C or the patient’s education (Supplementary Figure 1). The distribution of “high-risk” AF patients among the investigated hospitals is shown in Supplementary Figure 2.
Data Management
Academic Steering Committee (Supplementary Material 1) and Data Management Committee (Supplementary Material 2) will be responsible for the data quality control.
Statistical Approach
Data will be summarized using the mean (standard deviation (SD), medians (range) for continuous data, and counts (percentages) for categorical data. Continuous variables were tested for distribution by the Kolmogorov–Smirnov test. Those with a normal distribution are presented as the mean and SD and were analysed by the t-test or analysis of variance (ANOVA). Data with a nonnormal distribution are presented as the median with interquartile range (IQR) and were analysed by nonparametric methods. The comparison of discrete variables was performed via the chi-square test. A Cox proportional hazard model on the outcomes will be performed to assess the impact of covariates (eg, patient characteristics, physician characteristics, risk scores, antithrombotic drugs). The analysis will be conducted for various age groups (particularly patients ≥ 75 years old), multimorbid patients (defined as those with > 2 comorbidities), and patients with polypharmacy (with > 5 drugs used) to clarify the adherence to guidelines and outcomes of the “high-risk” population with AF. All statistical analyses will be considered significant at the 5% confidence limit using 2-sided tests or 2-sided confidential intervals (CIs).
The planned analyses include the following:
- Compliance with guidelines regarding stroke avoidance: the rate of risk assessment (CHA2DS2-VASc, HAS-BLED) and dynamic risk assessment, the adherence and persistence of risk-stratified anticoagulant use, and compliance with guidelines will be assessed.
- Adherence to guidelines regarding Better symptom control: rate control in compliance with guidelines (eg, <110 bpm in AF patients without HF, <80 bpm in AF patients with HF) and the rate/rhythm-control drug modification based on patient-reported symptoms (EHRA AF symptom scale) will be investigated.
- Adherence to guidelines regarding cardiovascular risk or comorbidity management: lifestyle modification regarding the cardiovascular risk profile, guide-recommended drug therapy for comorbidities (eg, hypertension, coronary artery disease, HF, high blood pressure, and high lipid values), and compliance with the guidelines will be evaluated.
Other analyses will be explored, such as
- Recurrent AF episodes with “upstream management” with artificial intelligence machine-learning AF risk prediction, through lifestyle modification or comorbidity management (pathway C).
- Anticoagulants with AF burden monitored by PPG or single ECG technologies if patients have compatible smart devices.
- Cardiovascular events: ischaemic stroke/thromboembolism, rehospitalization, death.
- Acceptability, adherence, and persistence of structured follow-up rehabilitation package use.
- Changes in the Quality of Life of AF patients at 12 months.
- Heterogeneity of adherence to guidelines in Class III, II, or I hospitals or community service centres with medical staff supporting teamwork and educational programs by mAFA III.
Other exploratory analyses include i) antithrombotic treatment as a guideline proposed for patients after receiving AF ablation, LAAO, or both AF ablation and LAAO; ii) the reasons why AF patients would not like to use the smartphone application at enrolment and during follow-up, together with their adherence to guidelines and cardiovascular events.
Determination of Sample Size
Based on respective cohort studies on integrated ABC pathway compliance,20,21 an annual rate of composite outcome of “ischaemic stroke or systemic embolism, all-cause death and cardiovascular hospitalization” of 29.3% associated with non-ABC compliance compared with 20.8% associated with ABC compliance (odds ratio 0.53, 95% CI 0.36–0.80), we would need 830 patients to identify a difference in pathway A compliance on the outcome, with a power of 80% and 1-A=0.05. The withdrawal rate is assumed to be 20% for the first year; thus, the sample size for this study will be at least 1039 patients to demonstrate a crude difference in compliance to guidelines recommended by pathway A for one year. The sample size calculation in relation to ABC compliance is shown in Table 3. It is estimated that approximately 1475 patients would be needed to detect the outcome of pathway A, B, and C compliance. However, the present observational study allows the recruitment of patients with AF as soon as possible (n=3000) to achieve 80% power to detect a difference in compliance with all components of the ABC pathway.
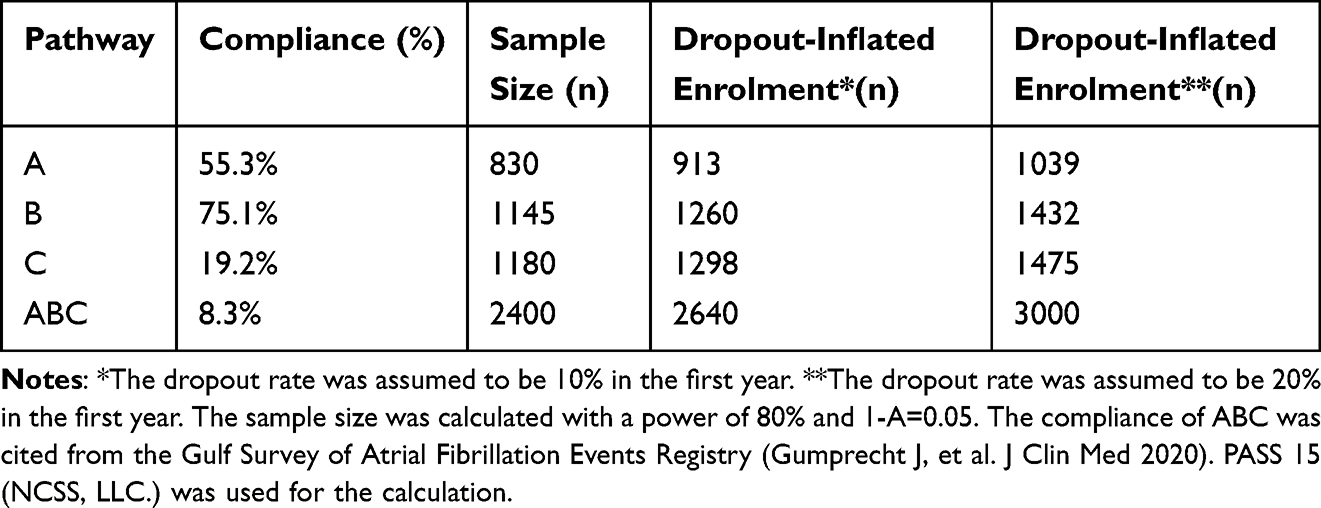 |
Table 3 Sample Size Calculation in Relation to ABC Pathway Compliance |
Discussion
The present study will implement digital health in clinical practice in a real-world setting, aiming to improve adherence to guidelines based on an integrated care ABC pathway, Avoid stroke, Better symptom control, and Cardiovascular risk and comorbidity management for patients with AF.
The inappropriate prescription of OACs,22,23 the heterogeneity of OAC use in primary care and academic hospitals,10,11,13 and noncompliance with OAC use7 are common problems in current clinical practice, emphasizing the compelling need to improve risk assessment and management of guideline adherence.
However, addressing nonadherence to the treatment is complex. Only 40.2% of patients with AF had both adherent and persistent OACs at one year, and the risk of noncompliance increased over time at the individual and system levels.6 Being elderly, having a greater number of comorbidities, and having a combined use of multiple drugs are risk factors for nonadherence. In our pilot investigation, 26.3% of AF patients received ≥5 drugs, 17.9% of patients were aged over 75 years, and 23.1% had had a prior stroke (Supplementary Figure 2). Other clinical settings contributing to this complex setting included a high risk for bleeding, renal dysfunction, coronary artery disease, and invasive procedures. Thus, cardiovascular risk and comorbidity management are also important to achieve compliance, other than the prescription of OACs themselves.
Moreover, AF patients are heterogeneous and may have different risk profiles and management patterns (eg, drug therapy only, AF ablation, or LAAO). For patients with persistent/permanent AF who are receiving drug therapy only, Avoid stroke would possibly be the first consideration. However, for patients with paroxysmal AF who receive ablation, Better symptom control would likely be an important aspect. The present study will provide individualized follow-up rehabilitation packages adapted to patients with different management patterns based on the ABC pathway to improve their outcomes.
The supporting health care system is another crucial factor in reducing the heterogeneity of treatments. General practitioners (GPs) appear to have limited confidence in their ability to identify and manage AF, with limited use of appropriate OACs and cardioversion treatment. The mAFA programme could help GPs gain greater knowledge and skills regarding the implementation of the AF Better Care pathway12,18 and will facilitate medical support from senior hospitals through the App team-work function that closely links primary care, Class II hospitals, and Class III hospitals.
In this study, AI technology as a tool for AF prediction and management will also be explored. The introduction of AI technology into clinical practice will allow us to not only predict the risk but also explore the “true” implementation of personalized medicine through AI risk prediction, thus facilitating management.
Limitations
The present study is designed as an observational, real-world cohort study. Selection bias may exist given the enrollment from the different sites. However, we did the pilot investigation to assess possible study sites, hospital size. We did not plan to compare the outcomes of mAFA users and non–mAFA users in this observational study. However, the application of the ABC pathway using mHealth technology has been investigated in our prior cluster randomized clinical trial.12,13
Conclusion
The present study will provide evidence for personalized treatment through the implementation of a digital health technology-supported guideline-recommended clinical care pathway in clinical practice, adapted to the patient’s risk profile and different management patterns, facilitating improved adherence to guidelines.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
The protocol for this study was approved by the Central Medical Ethics Committee of Chinese PLA General Hospital (Approval number: HZKY-PJ-2021-13), which accepted responsibility for supervising all of the aspects of the study and was also approved by local institutional review boards. All patients will provide written informed consent. The study was performed in accordance with the Declaration of Helsinki document on human research ethics. Study outcomes will be disseminated through conference presentations, peer-reviewed publications, the Internet and social media.
Patient and Public Involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Acknowledgments
The authors thank all of the study participants for their great effort.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82170309).
Disclosure
GYHL: Consultant and speaker for BMS/Pfizer, Boehringer Ingelheim and Daiichi-Sankyo. No fees are received personally.
Other authors: None declared.
References
1. Zhang J, Johnsen SP, Guo Y, et al. Epidemiology of atrial fibrillation: geographic/ecological risk factors, age, sex, genetics. Card Electrophysiol Clin. 2021;13(1):1–23. doi:10.1016/j.ccep.2020.10.010
2. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2021;42(5):373–498. doi:10.1093/eurheartj/ehaa612
3. Vesa ŞC, Vlaicu SI, Sabin O, et al. Evaluating physician adherence to antithrombotic recommendations in patients with atrial fibrillation: a pathway to better medical education. Int J Environ Res Public Health. 2020;17(11):4008. doi:10.3390/ijerph17114008
4. Yao X, Shah ND, Sangaralingham LR, et al. Non-Vitamin K antagonist oral anticoagulant dosing in patients with atrial fibrillation and renal dysfunction. J Am Coll Cardiol. 2017;69(23):2779–2790. doi:10.1016/j.jacc.2017.03.600
5. Chan YH, Chao TF, Chen SW, et al. Off-label dosing of non-vitamin K antagonist oral anticoagulants and clinical outcomes in Asian patients with atrial fibrillation. Heart Rhythm. 2020;17(12):2102–2110. doi:10.1016/j.hrthm.2020.07.022
6. Banerjee A, Benedetto V, Gichuru P, et al. Adherence and persistence to direct oral anticoagulants in atrial fibrillation: a population-based study. Heart. 2020;106(2):119–126. doi:10.1136/heartjnl-2019-315307
7. Nielsen-Kudsk JE, Korsholm K, Damgaard D, et al. Clinical outcomes associated with left atrial appendage occlusion versus direct oral anticoagulation in atrial fibrillation. JACC Cardiovasc Interv. 2021;14(1):69–78. doi:10.1016/j.jcin.2020.09.051
8. Krittayaphong R, Winijkul A, Kunjara-Na-Ayudhya R, et al. Adherence to anticoagulant guideline for atrial fibrillation improves outcomes in asian population: the COOL-AF registry. Stroke. 2020;51(6):1772–1780. doi:10.1161/strokeaha.120
9. Working Group on Atrial Fibrillation NCfCQI. 2019 clinical performance and quality measures for atrial fibrillation in China. Chin Circul J. 2020;35(5):427–437.
10. Chen Y, Huang QF, Sheng CS, et al. Detection rate and treatment gap for atrial fibrillation identified through screening in community health centers in China (AF-CATCH): a prospective multicenter study. PLoS Med. 2020;17(7):e1003146. doi:10.1371/journal.pmed.1003146
11. Guo Y, Lane DA, Chen Y, et al. Regular bleeding risk assessment associated with reduction in bleeding outcomes: the mAFA-II randomized trial. Am J Med. 2020;133(10):1195–202.e2. doi:10.1016/j.amjmed.2020.03.019
12. Guo Y, Lane DA, Wang L, et al. Mobile health technology to improve care for patients with atrial fibrillation. J Am Coll Cardiol. 2020;75(13):1523–1534. doi:10.1016/j.jacc.2020.01.052
13. Guo Y, Guo J, Shi X, et al. Mobile health technology-supported atrial fibrillation screening and integrated care: a report from the mAFA-II trial Long-term Extension Cohort. Eur J Intern Med. 2020;82:105–111. doi:10.1016/j.ejim.2020.09.024
14. Varma N, Cygankiewicz I, Turakhia MP, et al. 2021 ISHNE/HRS/EHRA/APHRS expert collaborative statement on mhealth in arrhythmia management: digital medical tools for heart rhythm professionals: from the international Society for Holter and Noninvasive Electrocardiology/Heart Rhythm Society/European Heart Rhythm Association/Asia-Pacific Heart Rhythm Society. Circ Arrhythm Electrophysiol. 2021:Circep120009204. doi:10.1161/circep.120.009204
15. Varma N, Marrouche NF, Aguinaga L, et al. HRS/EHRA/APHRS/LAHRS/ACC/AHA worldwide practice update for telehealth and arrhythmia monitoring during and after a pandemic. Europace. 2021;23(2):313. doi:10.1093/europace/euaa187
16. Kozieł M, Simovic S, Pavlovic N, et al. Impact of multimorbidity and polypharmacy on the management of patients with atrial fibrillation: insights from the Balkan-AF survey. Ann Med. 2021;53(1):17–25. doi:10.1080/07853890.2020.1799241
17. Lip GYH, Tran G, Genaidy A, et al. Prevalence/incidence of atrial fibrillation based on integrated medical/pharmacy claims, and association with co-morbidity profiles/multi-morbidity in a large US adult cohort. Int J Clin Pract. 2021;75:e14042. doi:10.1111/ijcp.14042
18. Guo Y, Chen Y, Lane DA, et al. Mobile health technology for atrial fibrillation management integrating decision support, education, and Patient Involvement: mAF app trial. Am J Med. 2017;130(12):1388–96.e6. doi:10.1016/j.amjmed.2017.07.003
19. Guo Y, Lane DA, Wang L, et al. Mobile Health (mHealth) technology for improved screening, patient involvement and optimising integrated care in atrial fibrillation: the mAFA (mAF-App) II randomised trial. Int J Clin Pract. 2019;73(7):e13352. doi:10.1111/ijcp.13352
20. Domek M, Gumprecht J, Li YG, et al. Compliance of atrial fibrillation treatment with the ABC pathway in patients with concomitant diabetes mellitus in the middle east based on the gulf SAFE registry. Eur J Clin Invest. 2020;51:e13385. doi:10.1111/eci.13385
21. Gumprecht J, Domek M, Proietti M, et al. Compliance of atrial fibrillation treatment with the atrial fibrillation better care (ABC) pathway improves the clinical outcomes in the middle east population: a report from the gulf survey of atrial fibrillation events (SAFE) registry. J Clin Med. 2020;9(5):1286. doi:10.3390/jcm9051286
22. Ferrat E, Fabre J, Galletout P, et al. Inappropriate direct oral anticoagulant prescriptions in patients with non-valvular atrial fibrillation: cross-sectional analysis of the French CACAO cohort study in primary care. Br J Gen Pract. 2021;71(703):e134–e39. doi:10.3399/bjgp20X714005
23. Feng Y, Pai CW, Seiler K, et al. Adverse outcomes associated with inappropriate direct oral anticoagulant starter pack prescription among patients with atrial fibrillation: a retrospective claims-based study. J Thromb Thrombolysis. 2021;51:1144–1149. doi:10.1007/s11239-020-02358-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.