Back to Journals » Advances in Medical Education and Practice » Volume 12
Stress and Coping Strategies Among Malawian Undergraduate Nursing Students
Authors Baluwa MA ![]() , Lazaro M, Mhango L, Msiska G
, Lazaro M, Mhango L, Msiska G ![]()
Received 5 January 2021
Accepted for publication 5 May 2021
Published 28 May 2021 Volume 2021:12 Pages 547—556
DOI https://doi.org/10.2147/AMEP.S300457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Masumbuko Albert Baluwa,1 Matthews Lazaro,2 Lucky Mhango,1 Gladys Msiska2
1Department of Nursing and Midwifery, Mzuzu University, Mzuzu, Malawi; 2University of Malawi, Kamuzu College of Nursing, Lilongwe, Malawi
Correspondence: Masumbuko Albert Baluwa
Department of Nursing and Midwifery, Mzuzu University, Private Bag 201 Luwinga, Mzuzu 2, Malawi
Tel +265999229714
Email [email protected]
Purpose: Stress among nursing students has been widely investigated across the globe, and evidence suggests that nursing programs are stressful. Students from resource constrained contexts, such as Malawi, often find it difficult and over stressing to be socialized into the nursing profession. However, this area has not been adequately investigated in Malawi. The aim of the study was to investigate stress and its coping strategies among nursing students in Malawi.
Methods: This was a quantitative study which used a descriptive cross-sectional design that included 102 students in years 2, 3 and 4. Data were collected using the adapted standard tools (Perceived Stress Scale and Adaptive Version of the Nurse Stress Scale) to comprehensively measure levels of stress categorised as clinical, academic and external. The brief Cope was used to measure common coping strategies. Independent samples t test and ANOVA were run at 5% level of significance to analyze the data.
Results: Moderate levels of stress were perceived by this sample. Academic category contributed to more stress than clinical and external sources. Lecturers, clinical teachers and nursing staff were the major contributors of stress among students. Similarly, high levels of stress were found among year 2 and self-sponsored students. In terms of coping strategies, active coping and planning were the common coping strategies. However, substance use was also recorded as a coping strategy.
Conclusion: The study revealed that although nursing students face various challenges in under-resourced environments, teachers and clinical staff highly contribute towards stress. It was then established that stress among nursing students’ can be contained by initiating stress reduction interventions. There is also need to further investigate the extent of substance use as it suggests that some students have not been able to cope with current stress levels hence resorting to use of substances.
Keywords: stress, clinical practice, nursing education, academic staff
Introduction
Stress among nursing students is a known phenomenon in literature with clear evidence that nursing programs are inherently stressful. The concept ‘stress’ is, in this sense, described as a physical or psychological stimulus that disturbs adaptive state of an individual and provokes coping response.1 Folkman and Maskowitz2 conversely, defines the notion of coping as thoughts and behaviours used to manage the internal and external demands of situations that are appraised as stressful. Studies3,4 reveal that high levels of stress upsets and negatively affects academic performance and general health of the students. Accordingly, it is recommended that nurse educators should assess causes and levels of stress associated with each program to formulate scientifically proven interventions that seek to reduce stress and help students effectively cope with their training programs.5
Furthermore, stress and coping strategies among nursing students have been extensively investigated in developed countries,3,6,7 and there is as such a growing body of knowledge among nursing students from eastern countries.4,8,9 However, it is an area that has not been adequately investigated in most sub-Saharan African countries including Malawi. Existing literature; for example, agrees that nursing students experience different degrees of stress during their training programs mainly due to clinical, academic and external factors.3,5,8 Specifically, nursing students are stressed while undertaking academic component of the program due to longer hours of study, a rigorous curriculum, huge workload, assignments and examination.8,10,11 Furthermore, nursing students undergo clinical practices in intrinsically stressful environments. During clinical practice for example, factors such as seeing patients suffering and dying, coupled with inadequate clinical knowledge and skills have often ignited stress.5,12 Similarly, poor relationships with clinical staff and faculty members from the university have immensely contributed towards stress.5 Initial period of clinical placement has also been reported to be highly stressful as students are exposed to clinical environment for the first time.13 However, some students have reported similar levels of stress across the years of study.14 Conversely, others reveal that there are high degrees of stress associated with increased level of the training program.6,7 Besides this, nursing students are also stressed by external factors such as accommodation and financial problems,15 as well as relationships with their peers and relatives.16 In terms of coping, problem solving and staying optimistic have been revealed to be common strategies in alleviating stress and helping students cope with demands of the nursing program.8,16
While the cases above reflects accounts from other countries, there was need for evidence on what could be the common causes and levels of stress among nursing students in developing countries like Malawi. To this end, the current study sought to answer the following questions: What could be the common cause of stress among nursing students in Malawi? What are the differences in terms of reports of stress based on the level of study and type of scholarship? and, what are the common coping mechanisms?
It should be admitted that there are some studies that have been done in Malawi, which identified several general challenges students face in clinical learning environment17,18 that may lead to stress. However, specific aspects that cause stress, and its levels in the nursing programs have not been fully investigated. In addition, there was need to establish the most stressing components of the training program between clinical, academic and external factors which are reported as common causes of stress in nursing students.3 Furthermore, factors such as level of study and financial challenges are known to affect levels of stress,6,15 hence, there was need to establish the extent to which these elements contribute towards stress levels. As argued by some scholars, knowledge of stress levels experienced by students is very important in determining the negative elements that should be changed in their behaviors to improve coping skills among nursing students.6
It is, of course, argued that in Malawi and other African countries, nursing students experience high degrees of stress with poor coping strategies when compared with those from the developed countries. One of the reasons for this is that 50.7% of the Malawi population live below poverty line; while 25% live in extreme poverty,19 and these realities cause additional stress on the students. In addition to this, most African countries including Malawi are characterised by poorly resourced clinical settings with high disease burden.20 Some studies have reported that shortage of human and material resources adversely affect nursing students’ clinical learning experiences in Malawi.17,18 This implies that socialisation of nursing students occurs in clinical environments with multiple challenges17,18 and not conducive for learning. Besides these, fears of contracting infections such as HIV and tuberculosis have been reported to cause significant stress among nursing students during clinical practice.21 Considering that nursing is naturally stressful, the foregoing factors help speculate about the existence of high levels of stress among Malawian nursing students. However, this is an area that has not been fully investigated, and this study emerges from this fact. The aim of this study, therefore, was to investigate stress and coping mechanisms among Malawian nursing students. To do this, undergraduate nursing students’ stress was measured based on demographic characteristics (level of study and type of scholarship) to assess levels of stress they experience, and how they eventually cope with it.
Materials and Methods
Design, Setting and Sample
This was a quantitative study which employed a descriptive cross-sectional research design. This approach was chosen to describe stress that nursing students at a Malawian training institution experience, and identify coping strategies and frequency of use.22
The study was conducted at Mzuzu University, a public institution in northern Malawi. This institution trains undergraduate registered nursing students. The study targeted total population of 119 students from years 2, 3 and 4. A census sampling frame was used, and 102 nursing students volunteered to take part in the study. The study measured stressors from clinical practice, academic and external factors. In this case, only students who had previously undertaken academic and clinical elements of the training were engaged. Therefore, students in academic years 2, 3 and 4 were included in the study because they had undergone both theoretical and clinical components of the training program. Conversely, students in year 1 were excluded because they had not yet done clinical practice during the period of this study.
Data were collected in December 2017. During this period, students in years 2 and 4 were on campus covering theoretical components of the training. On the other hand, students in year 3 were in clinical practice at Mzuzu Central hospital, a college teaching hospital and Zomba Mental hospital, a facility located about 350 km away from the university. Students who were around university campus were approached to participate in the study during weekends within the campus. The students who were doing clinical practice were invited to participate during their off days. Questionnaires were mailed for students who were practicing at Zomba Mental hospital. Participants took 40 minutes to complete the research questionnaire.
Data Collection Tools
Data were collected using a self-administered questionnaire which was in three parts. The first part collected data on demographic information which included sex, age, year of study, type of sponsorship and marital status. The second part had items on stressors adapted from the Perceived Stress Scale (PSS) developed by Sheu, Lin and Hwang23 and the Adaptive Version of the Nurse Stress Scale (AVNSS) by Rhead.24
The PSS primarily focuses on clinical stressors and it has 29 clinical stressors which are divided into six subscales namely; stress from taking care of patients (6 items), stress from teachers and nursing staff (6 items), stress from assignments and workload” (5 items), stress from peers and daily life (4 items), stress from lack of professional knowledge and skills (3 items) and stress from clinical environment (3 items). The instrument was originally used to measure Hong Kong nursing students’ sources of clinical stress. This is the reason all these items were included in the questionnaire. The original AVNSS has 32 items with 16 stressors each on clinical and academic sources. For this study, only 16 academic items that were relevant to Malawi’s context were included. Additionally, poor attitude of staff towards students was added as a potential stressor because there is strong evidence suggesting that this is one of the common problem nursing students encounter during clinical practices.17,18 To comprehensively assess students’ stressful experiences, financial problem was also included as part of external stressors based on the context. The authors fully understood the need to get copyright clearance from the creators of the tools hence wrote several emails seeking permission but did get any response.
Precisely, stress was measured from three categories namely clinical, academic and external as identified by Jimenez Navia-Osorio and Diaz.3 Clinical stressors were further sub-categorized into stress from taking care of patients; clinical teachers and nursing staff; lack of professional knowledge and skills and the hospital environment.23 Academic sources of stress were under the sub-categories of stressors related to the course, workload and assignments, and stress related to teachers. External sources of stress were measured based on six items. The questionnaire was set to a five point Likert scale with levels of each stressor measured from 0 (no stress), 1 (mild stress), 2 (moderate stress) 3 (severe stress) and 4 (extreme stress). The questionnaire had 47 items with a score range from 0 to 188. A higher score denoted higher degrees of stress.
The last part of the questionnaire measured coping strategies using a brief measure of COPE that was developed by Carver.25 The instrument consists of 14 sub-scale with two items under each scale for a total of 28 items. The questionnaire is a four-point Likert scales (0= I usually do not do this to 3= I have been doing this a lot) based on the extent to which the coping strategy alleviate student stress.
Validity and Reliability
To quality assure the stress questionnaire, content validation was conducted. At this stage, content validity inventory (CVI) was first conducted.26 The study tool was critically reviewed by 5 experienced academicians in nursing education and mental health. They were requested to rate the content of the tool on a four-point Likert-scale (1 = not relevant, 2 = somewhat relevant, 3 = quite relevant, 4 = highly relevant) and had the option to provide written feedback on questions that needed modification.26 Item Content Validity Index (ICVI) and the Scale Content Validity Index (SCVI) were calculated. All items scored above 0.92 and content validity index of the instrument was 0.94 indicating good content validity.
The researchers adapted already validated existing data collection tools. The PSS had a reasonable reliability indexes with Cronbach’s alpha of 0.89 and the one-week test–retest reliability of 0.60 (P < 0.01), while the CVI of 0.94 proved its validity.23 In addition, 50.7% of total variance was accounted for by the six factors which confirmed the construct validity of this instrument. AVNSS was adapted from the original nursing stress scale in a 2-staged pilot study to generate academic activities that are very stressful.24 In this study, the Cronbach’s alpha for the tool was 0.93 indicating excellent internal consistency reliability. The Cronbach’s alpha for the 7 sub-categories ranged from 0.7 to 0.85. Similarly, the Cronbach’s alpha of the 14 items brief cope ranged from 0.50 to 0.90 making it a reliable tool.25
Pilot Study
The data collection instruments were piloted with 10 nursing students from Kamuzu College of Nursing, a nursing institution that also trains undergraduate registered nurses. This was done to ensure that the stressors and the coping strategies in the instrument were clear and applicable to the Malawian context. The data from pilot study were analyzed and changes to the tool were made wherever necessary.
Data Analysis
Data were analysed using Statistical Package for Social Sciences (SPSS) version 20.0. All questionnaires were eligible for data entry and analysis (n=102). The scores on the Likert scale indicated the level and intensity of each stressor. A total for each stressor was calculated by adding together individual scores from each subject. A high score indicated increased intensity, and a common cause of stress. Descriptive statistics were computed, and the results are presented as frequencies, percentages, means and standard deviations. A One Way Analysis of Variance (ANOVA) was used to determine effect of three categories of stressors (academic, clinical and external), and the level of study (2, 3 and 4) on stress. Turkey test was used to separate the means among the three categories. Further, independent samples t-test was also performed to identify the statistical difference in mean stress between students who were on scholarships and those on self-sponsorship. All statistical tests in this study were run at 5% level of significance.
On the brief COPE, scores were calculated for each coping strategy. A higher score for each factor indicated more frequent use and greater effectiveness of that type of coping behavior in alleviating stress. Descriptive statistics were computed, and were presented as frequencies, percentages, and means with standard deviation.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki.
The research proposal was approved by the College of Medicine Research Ethics Committee (COMREC) of the University of Malawi. Permission for the study site was obtained from the Vice Chancellor, Dean of the Faculty of Health Sciences and Head of Nursing department at the University. Informed consent was obtained from each participant. A research assistant collected data to prevent undue influence on the students during data collection from the researchers if familiar educators were to be used.
Results
All the questionnaires that were distributed were responded to by the participants. Among these respondents, 54% (n=55) were male and 46% (n=47) were female. Most students (71.6%) were on government scholarships while the rest were self-sponsored (Table 1).
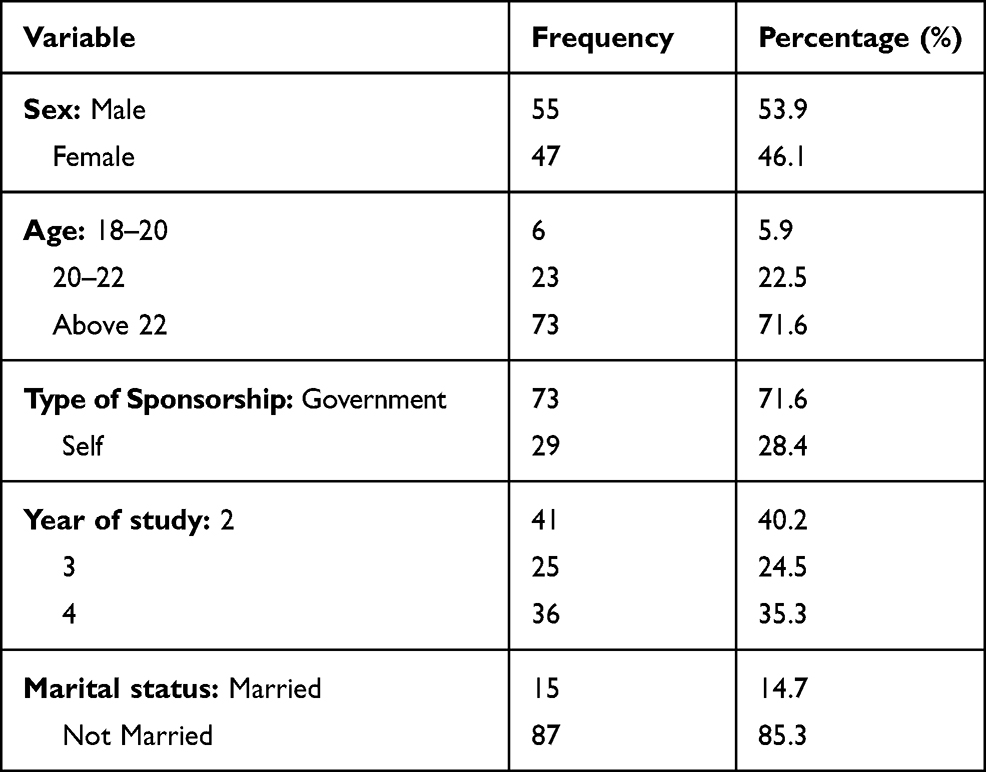 |
Table 1 Socio Demographic Characteristics of Respondents |
All respondents in this study reported experiencing some degrees of stress. Scores for each stressor were calculated, and the total mean level of stress from this sample was moderate (mean 2.24± 0.70). Each stressor on the scale caused some degree of stress. The highest student stress score was from worry about poor grades (mean= 3.26± 1.18). The lowest score was from unfamiliarity with ward facilities in the hospitals (mean=1.30±1.15).
Stress scores from the categories (academic, clinical and external) were calculated. One way ANOVA was run to determine if there was significant difference in the stress scores among the three categories. Based on the results, there was a statistically significant difference among the three categories of stressors as determined by one-way ANOVA (F(2303)=13.18, p<0.0001). A Turkey’s post-hoc test showed that academic category was associated with higher levels of stress (2.59±0.80), p<0.0001 than clinical (2.08±0.77) and external (2.04±0.96), and the difference was statistically significant. Results further revealed that there was no statistical difference between clinical and external categories (P=0.951) (Table 2).
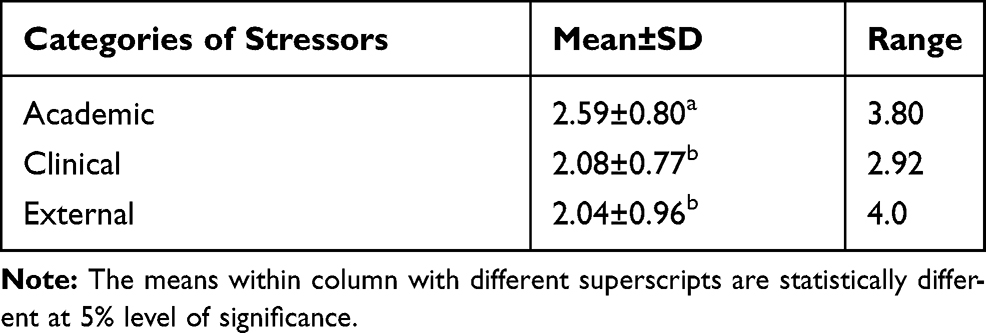 |
Table 2 Mean Scores for the Three Categories of Stressors |
The mean scores from the subcategories of each type of stress were calculated and ranked. Highest mean of stress from academic subcategory was from lecturers (mean=2.88± 0.97) while the clinical subcategory pointed at clinical teachers and nursing staff (mean= 2.55± 0.85). Lack of professional knowledge and skills, and hospital environment had the least score (same mean= 1.74± 1.16 and 0.92) respectively (Table 3).
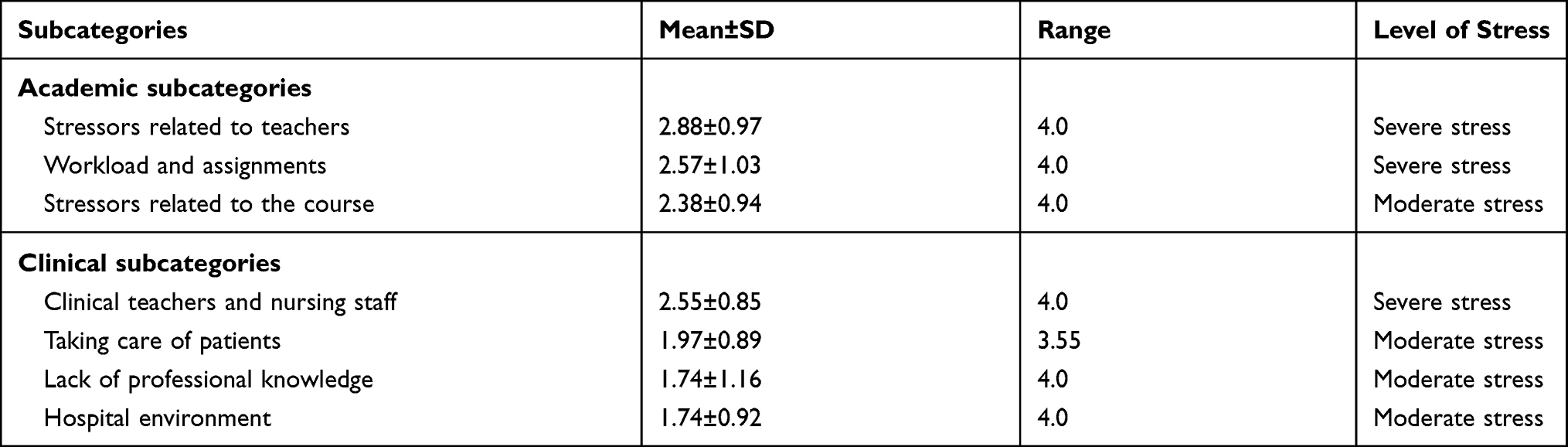 |
Table 3 Means for Subcategories of Stress |
Stressors from lecturers were ranked according to their highest mean to determine events that are most stressing. Pressure from lecturers’ evaluation of students’ performance by comparison (mean=3.10±1.23) was the common cause of stress followed by inadequate support from lecturers (mean=2.94±1.16) (Table 4).
 |
Table 4 Stressors Related to Lecturers |
Scores of stressors related to workload and assignments were calculated to determine the common cause of stress from this source. Worry about poor grades (mean=3.26±1.17) was the highest cause of stress followed by huge amount of academic work involved in the training (mean=2.84±1.38).
In the subcategory of clinical teachers and nursing staff, poor attitude of staff towards students (mean 3.12± 1.17), and lack of care and guidance from teachers (mean= 3.10±1.13) were the highest cause of stress.
In external factors, financial problems (mean=2.79±1.38) and pressure from family members to perform well (mean= 2.11± 1.55) were the highest causes of stress.
Effect of Sponsorship and Level of Study on Stress Levels
An independent sample t-test comparing the mean stress scores between self-sponsored students and those on full scholarships found a significant difference between the mean of the two groups (t(100) = 2.786, p=0.01). The mean for students on scholarship was significantly lower (2.56± 1.43) than that of self-sponsored students (3.38± 1.04). Stress levels from the years of study 2, 3, and 4 were calculated to identify the most stressed group. Results indicated that year 2 students scored high (mean= 2.49 ± 0.60) followed by year 3 (mean=2.07± 0.68) and 4 (mean 2.08± 0.75). A one-way ANOVA of the data reported a significant difference (F(2,99)=4.79, p=0.01) in the mean stress levels from the years of study. Tukey’s HSD indicated that students in year 2 scored significantly high (mean =2.49±0.60) than students in year 3 (mean=2.07±0.68) and 4 (mean=2.08 ± 0.75).
Further analysis was done to determine how different sources of stress are experienced among the students in years 2, 3 and 4. A one way ANOVA comparing the mean stress scores were calculated to determine if there were significant differences in levels of stress from each source. Tukey’s HSD was used to determine the nature of the differences. Results are presented in Table 5.
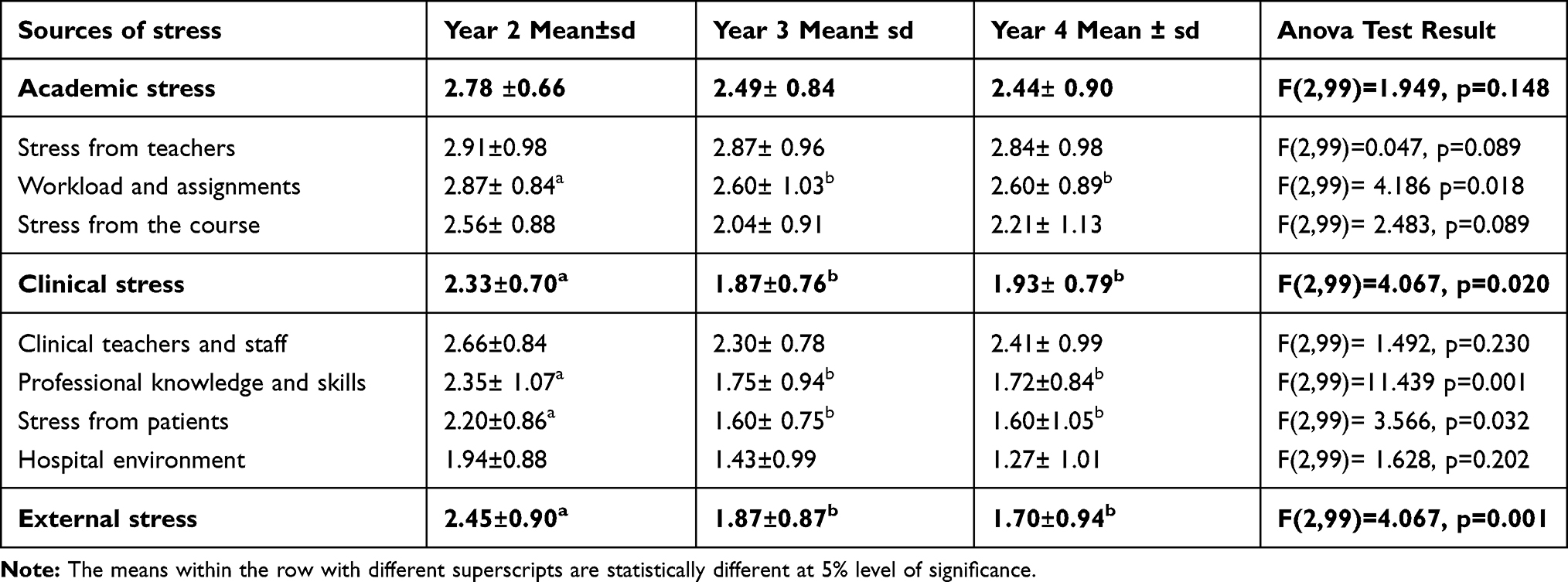 |
Table 5 Stress Levels from Each Source Based on Year of Study |
The results indicate that the three years of study did not differ in the levels of stress from academic factors (Table 5). However, year 2 students scored significantly high levels of stress in clinical and external stress. Furthermore, students in year 2 scored significantly high levels of stress on workload and assignments; lack of professional knowledge and skills, and stress from patients.
Coping Strategies
Active coping (mean =2.12±0.97) and planning (mean=2.10±0.94) were the most frequently used coping strategies. However, substance use was the least strategy frequently used by 12% of the respondents. Results are presented in Table 6.
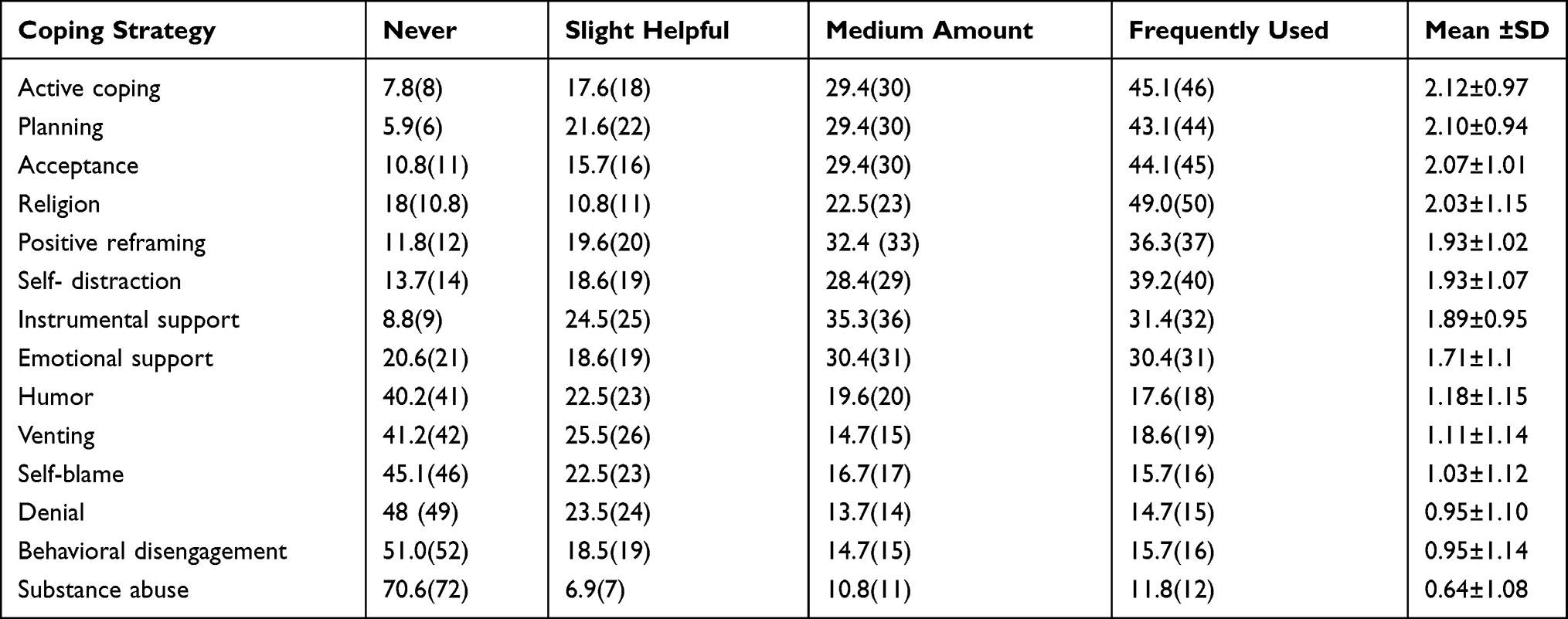 |
Table 6 Coping Strategies (Figures Presented as % (Frequency)) |
Discussion
Demographic findings reveal the current trend in Malawi where more men are joining the nursing profession than women. Traditionally, men in Malawi are regarded as strong and resilient to most challenges that may also include stressors during training program. Molina and Racal27 found high levels of stress in female students than males but attributed it to multiple tasks given to female students from homes/families. However, this study found out that few students (14.7%) who were married and had additional responsibilities at home apart from academic requirements.
This study has uncovered causes of stress and coping strategies among nursing students in under-resourced clinical learning environment. These results amplifies evidence about universality of stress among nursing students regardless of where they are being trained. Moderate degrees of stress recorded in this sample is similar to what has been reported in existing studies.4,8 Malawian nursing students do not experience stress levels more than learners in other countries despite them working in challenged environment due to lack of essential supplies, severe shortage of nurses and negative attitudes among others.17,18 Moderate levels of stress can be attributed to the psychological resilience that students develop having been brought up in environments suffused with acute challenges. Resilience is the ability to overcome adversity and it does grow stronger with experience.28 Additionally, perceived benefits of positive consequences from the stressor is known to increase mental strength and reduce levels of stress.2 Determination could be assisting Malawian students to still learn under difficult conditions and persevere.
The study revealed that academic issues were the highest cause of stress than clinical and external factors. This finding contradicts the studies that reported high stress levels from clinical elements in comparison to academic and external.3,29 High levels of academic stress observed in this study could have been influenced by activities happening during the research period. It is argued that when examining results of stress studies, recent events have to be borne in mind as they may influence ranking of highly stressful aspects.30 Pitt, Oprescu, Tapia and Gray31 also found that stress levels vary depending on educational activities taking place at a certain period of the semester. Within the period of study, majority of respondents (years 2 and 4) were covering theoretical components of the program. They could have been under pressure going through tight classroom schedules and examinations which are inherently stressful.11 Thus, ongoing academic elements during that period of data collection might have influenced learners to rate them very high in comparison to other factors.
Teachers were a common cause of stress from academic and clinical categories. Similar studies have reported nursing educators as second leading cause of stress in clinical practice.8,28 This finding is not strange in Malawi. There are multiple challenges that students face in relation to clinical teachers and supervisors which have previously been reported by other scholars.17,18 The study revealed that high levels of stress were due to pressure from teachers evaluating students by comparison. This item has equally been ranked very high in comparison to related studies.3,8,29 Arguably, evaluation is not about comparing individual learners’ capabilities with their peers. Every student is a unique learner with own mental ability and learning needs.32 In this case, teachers need to refocus evaluation intentions to cultivate its full benefits to both the learner and the nursing program.
The study established that learners suffer high levels of stress due to poor attitude of clinical staff towards them. Similarly, negative attitudes leading into a hostile environment, poor relationship among staff and students, have previously been reported during clinical practice.17,18 In Malawian context, negative attitudes could be influenced by existing working conditions as hospitals are characterized by high shortages of qualified nurses.20 In this situation, students are viewed as an extra human workforce in patient care activities.18 High expectations placed on these students may contribute to stress as they are still learning skills of care provision but are expected to practice on their own like qualified staff.18 Further, balancing the demands of staff and their own academic needs can contribute to more stress. Conversely, overworked staff may demonstrate negative attitude due to chronic job-related burnout which has previously been reported among Malawian healthcare workers.33 Such workers are physically and psychologically unfit to perform additional duties such as teaching and supervising nursing students.
Worry about bad grades was the highest stressor among nursing students. Similar studies have also rated this fact as the highest event causing stress among nursing students.3,9,10 Arguably, students could be under pressure with academic grades for fear of failure which can then lead to discontinuation of the course. In Malawi, this could be exacerbated by fears of the future due to limited opportunities for tertiary education.34 Conversely, students may have pressure from home as parents expect them to get a high grade in school. Therefore, learners would work tirelessly to satisfy parents’ expectations leading to further stress.
Studies have ranked stress from taking care of patients3,9,10 and lack of professional knowledge and skills3,13 the highest in clinical practice. However, the current findings were congruent with those studies that established these elements as the least causes of stress.4,8 Lower levels of stress on these aspects can be attributed to the favorable atmosphere that patients provide to nursing students. Practical learning activities make clients feel that they are well cared in the context where students also work to cover nurse shortages.17 At the same time, nursing students have a chance to practice their skills. This mutual benefit may nourish good relationships between the students and patients thereby contributing to low levels of stress.
As expected, financial problem was the highest stressor from external factors. This finding was previously reported in similar studies.15 Financial problems are not strange in a country where the majority of citizens live in abject poverty.19 Consequently, health-care trainings are largely funded by government and its partners through scholarships that cover school fees and upkeep.20 However, the scholarships are not adequate to cover all the needy students and the money given to individuals may not suffice their needs. Hence, self-sponsored students experienced significantly high levels of stress from financial problems unlike those on scholarships. Such students are more vulnerable to negative effects of stress35 and require additional protective interventions.
Students in year 2 experienced high levels of stress than those in years 3 and 4. This finding is in contrast with studies that reported high stress levels in experienced students than novice.6,12 This result can be linked to the structure of the curriculum. The curriculum is arranged in that year 2 students start covering core clinical nursing courses and clinical practice which is known to be highly stressful for beginners.3 Students in early years of study are still learning to work in a stressful clinical setting unlike experienced students who have more confidence and nursing skills.27 They may not have developed adequate coping resources hence experiencing more stress from clinical elements than the other two groups.
Common coping strategies used among this sample of nursing students were active coping and planning. Active coping strategies such as problem-solving skills have also been reported in related studies.8,29 The use of active coping strategies among these students signifies positive attitude and adaptation to stress8 despite learning in resource constrained clinical environments. Literature recommends that teachers should encourage the use of proven interventions to effectively cope with stress.5 The use of active strategies such as development of professional competency, correcting mistakes, confronting stressful situations and reflecting on stressful issues have been found to be helpful.36 Faculty members should reinforce the use of these strategies to overcome stressful situations in this context.
The study further revealed that some students (11.8%) use substances, and this may indicate that they are not effectively coping with current levels of stress. This agrees with Boulton and O’Connell37 who revealed frequent abuse of substances among students experiencing high degrees of stress. There is nevertheless need for further investigation on use of substances among these students to fully understand and explain it.
Conclusion and Recommendations
This study was aimed at assessing stressors and coping strategies among nursing students in under-resourced clinical environments. Findings revealed that nursing students in this context encounter similar stressors, and use coping strategies that are similar to other settings.4,8,29 However, highest scores from teachers and clinical staff recorded in this study is unusual which call for further research to understand why this is the case. Further, the study unsurprisingly recorded high level of financial problems especially for self-sponsored students who require additional support to meet their needs to reduce stress levels. The use of substances as a coping strategy shows that some students are not adapting well to the current degrees of stress.37 As such, there is need to further investigate the type of substances that are used to develop tailored strategies for promoting effective coping.
The study also revealed that it is possible to minimize nurse-student stress in Malawi’s context. Teachers and clinical staff are key in reducing students’ stress by carefully designing and conducting stressful activities of the training such as examination and grades to alleviate fear and anxiety.11 In addition, school leaders should initiate stress reduction interventions to help students overcome several challenges in this environment with few resources for classroom and clinical learning.
Results of this study are from one public university and this could be the limitation of this study since the sample was small. There is therefore need for national studies to include all nursing colleges in Malawi to generalize stressors and coping strategies in this context.
Acknowledgments
We sincerely thank all nursing students who voluntarily took part in this study.
Funding
None. The research was undertaken for academic advancement, and did not receive any grant from funding agencies in public, commercial or private sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gomathi S, Jasmindebora S, Baba V. Impact of stress on nursing students. Int J Innovative Res Adv Studies. 2017;4(4):107–110.
2. Folkman S, Moskowitz JT. Coping: pitfalls and promise. Annu Rev Psychol. 2004;55:745–774. doi:10.1146/annurev.psych.55.090902.141456
3. Jimenez C, Navia-Osorio PM, Diaz CV. Stress and health in novice and experienced nursing students. J Adv Nurs. 2010;66(2):442–455. doi:10.1111/j.1365-2648.2009.05183.x
4. Labrague LJ, McEnroe-Petitte DM, Papathanasiou IV, et al. A cross-country comparative study on stress and quality of life in nursing students. Perspect Psychiatr Care. 2018;54(4):469–476. doi:10.1111/ppc.12248
5. Labrague LJ, McEnroe-Petitte DM, Gloe D, Thomas L, Papathanasiou IV, Tsaras K. A literature review on stress and coping strategies in nursing students. J Ment Health. 2017;26(5):471–480. doi:10.1080/09638237.2016.1244721
6. Onieva-Zafra MD, Fernández-Muñoz JJ, Fernández-Martínez E, García-Sánchez FJ, Abreu-Sánchez A, Parra-Fernández ML. Anxiety, perceived stress and coping strategies in nursing students: a cross-sectional, correlational, descriptive study. BMC Med Educ. 2020;20(1):1–9.
7. Gurková E, Zeleníková R. Nursing students’ perceived stress, coping strategies, health and supervisory approaches in clinical practice: a Slovak and Czech perspective. Nurse Educ Today. 2018;1(65):4–10. doi:10.1016/j.nedt.2018.02.023
8. Hamaideh SH, Al-Omari H, Al-Modallal H. Nursing students’ perceived stress and coping behaviors in clinical training in Saudi Arabia. J Ment Health. 2017;26(3):197–203. doi:10.3109/09638237.2016.1139067
9. Ahmed WA, Mohammed BM. Nursing students’ stress and coping strategies during clinical training in KSA. J Taibah Univ Sci. 2019;14(2):116–122.
10. Akhu-Zaheya LM, Shaban IA, Khater WA. Nursing students’ perceived stress and influences in clinical performance. I J Adv Nurs Stud. 2015;4(2):44. doi:10.14419/ijans.v4i2.4311
11. Quinn BL, Peters A. Strategies to reduce nursing student test anxiety: a literature review. J Nurs Educ. 2017;56(3):145–151. doi:10.3928/01484834-20170222-05
12. Bhurtun HD, Turunen H, Estola M, Saaranen T. Changes in stress levels and coping strategies among Finnish nursing students. Nurse Educ Pract. 2021;50:102958. doi:10.1016/j.nepr.2020.102958
13. Alshahrani Y, Cusack L, Rasmussen P. Undergraduate nursing students’ strategies for coping with their first clinical placement: descriptive survey study. Nurse Educ Today. 2018;1(69):104–108. doi:10.1016/j.nedt.2018.07.005
14. Shukla A, Kalra G, Pakhare A. Understanding stress and coping mechanisms in Indian student nurses. SL J Psychiatr. 2013;4(2):29–33. doi:10.4038/sljpsyc.v4i2.5387
15. McCarthy B, Trace A, O’Donovan M, et al. Nursing and midwifery students’ stress and coping during their undergraduate education programmes: an integrative review. Nurse Educ Today. 2018;1(61):197–209. doi:10.1016/j.nedt.2017.11.029
16. Labrague LJ, McEnroe-Petitte DM, Papathanasiou IV, et al. Stress and coping strategies among nursing students: an international study. J Ment Health. 2018;27(5):402–408. doi:10.1080/09638237.2017.1417552
17. Kamphinda S, Chilemba EB. Clinical supervision and support: perspectives of undergraduate nursing students on their clinical learning environment in Malawi. Curationis. 2019;42(1):1–10. doi:10.4102/curationis.v42i1.1812
18. Mbakaya BC, Kalembo FW, Zgambo M, et al. Nursing and midwifery students’ experiences and perception of their clinical learning environment in Malawi: a mixed-method study. BMC Nurs. 2020;19(1):1–14. doi:10.1186/s12912-020-00480-4
19. International Monetary Fund. International Monetary Fund. Malawi economic development report. Washington DC: International Monetary Fund; 2017. Report No.: 17/184.
20. Government of Malawi. Government of Malawi. (2017, April). Malawi government healthcare strategic plan 2017-222.
21. Msiska G, Kamanga M, Chilemba E, Msosa A, Munkhondya TE. Sources of stress among undergraduate nursing students during clinical practice: a Malawian perspective. Open J Nurs. 2019;9(01):1. doi:10.4236/ojn.2019.91001
22. Grove SK, Burns N, Gray J. The practice of nursing research: appraisal, synthesis, and generation of evidence. Elsevier Health Sciences; 2012.
23. Sheu S, Lin H-S, Hwang S-L. Perceived stress and physio-psycho-social status of nursing students during their initial period of clinical practice: the effect of coping behaviors. Int J Nurs Stud. 2002;39(2):165–175. doi:10.1016/S0020-7489(01)00016-5
24. Rhead MM. Stress among student nurses: is it practical or academic? J Clin Nurs. 1995;4(6):369–376. doi:10.1111/j.1365-2702.1995.tb00038.x
25. Carver CS. You want to measure coping but your protocol’too long: consider the brief cope. Int J Behav Med. 1997;4(1):92. doi:10.1207/s15327558ijbm0401_6
26. Yusoff MSB. ABC of content validation and content validity index calculation. Med.Educ. 2019;11(2):49–54. doi:10.21315/eimj2019.11.2.6
27. Molina S, Racal SJ. Stress, coping, and mental health status among nursing students at a private university in Nakhon Pathom, Thailand. J Glob Health. 2018;2(3):63–69.
28. Thomas LJ, Asselin M. Promoting resilience among nursing students in clinical education. Nurse Educ Pract. 2018;(28):231–234. doi:10.1016/j.nepr.2017.10.001
29. Al-Gamal E, Alhosain A, Alsunaye K. Stress and coping strategies among Saudi nursing students during clinical education. Perspec Psychiatr Care. 2018;54(2):198–205. doi:10.1111/ppc.12223
30. Burnard P, Edwards D, Bennett K, et al. A comparative, longitudinal study of stress in student nurses in five countries: Albania, Brunei, the Czech Republic, Malta and Wales. Nurse Educ Today. 2008;28(2):134–145. doi:10.1016/j.nedt.2007.04.002
31. Pitt A, Oprescu F, Tapia G, Gray M. An exploratory study of students’ weekly stress levels and sources of stress during the semester. Act Learn High Educ. 2018;19(1):61–75. doi:10.1177/1469787417731194
32. Ormrod JE, Anderman EM, Anderman LH. Educational psychology: developing learners. Pearson; 2016.
33. Kim MH, Mazenga AC, Simon K, et al. Burnout and self-reported suboptimal patient care amongst health care workers providing HIV care in Malawi. PLoS One. 2018;13(2):e0192983. doi:10.1371/journal.pone.0192983
34. Chawinga WD, Zozie PA. Increasing access to higher education through open and distance learning: empirical findings from Mzuzu University, Malawi. INT REV RES OPEN DIS. 2016;17(4):1–20.
35. Cheung T, Wong SY, Wong KY, et al. Depression, anxiety and symptoms of stress among baccalaureate nursing students in Hong Kong: a Cross-Sectional Study. Int J Environ Res Public Health. 2016;13(8):779. doi:10.3390/ijerph13080779
36. Rafati F, Nouhi E, Sabzevari S, Dehghan-Nayeri N. Coping strategies of nursing students for dealing with stress in clinical setting: a qualitative study. Electron Physician. 2017;9(12):6120. doi:10.19082/6120
37. Boulton M, O’Connell KA. Nursing students’ perceived faculty support, stress, and substance misuse. J Nurs Educ. 2017;56(7):404–411. doi:10.3928/01484834-20170619-04
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.