")
Back to Journals » Infection and Drug Resistance » Volume 13
Stenotrophomonas maltophilia Infections: Clinical Characteristics and Factors Associated with Mortality of Hospitalized Patients
Authors Insuwanno W, Kiratisin P, Jitmuang A
Received 14 March 2020
Accepted for publication 16 May 2020
Published 28 May 2020 Volume 2020:13 Pages 1559—1566
DOI https://doi.org/10.2147/IDR.S253949
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Worachart Insuwanno,1 Pattarachai Kiratisin,2 Anupop Jitmuang3
1Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2Department of Microbiology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 3Division of Infectious Diseases and Tropical Medicine, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Anupop Jitmuang Email [email protected]
Purpose: To study the clinical characteristics and factors associated with mortality of patients who had Stenotrophomonas maltophilia infections.
Patients and Methods: We conducted a retrospective study to determine the clinical characteristics and factors associated with mortality for S. maltophilia infections among hospitalized adult patients at Siriraj Hospital. The clinical and microbiological data were collected from medical records December 2013–December 2016.
Results: Of 1221 subjects whose clinical samples grew S. maltophilia, 213 were randomly selected for chart review. One hundred patients with a true infection were analyzed. Their median age was 66 years; 47 were males; 46 were critically ill with a median APACHE II score of 18 (2– 32); and 91 received antibiotic treatment, mainly with carbapenems (56%), before being diagnosed with a S. maltophilia infection. Pulmonary (53%) and bloodstream infections (25%) were the most common infections. The median length of hospitalization was 19 days before infection onset. The in-hospital mortality rate was 54%. The following factors were associated with mortality: a pre-existing respiratory infection (OR 6.28, 1.33– 29.78; p.021); critical illness (OR 3.33, 1.45– 7.62; p.005); multi-organ dysfunction (OR 2.44, 1.05– 5.70; p.039); being on mechanical ventilation (OR 4.44, 1.90– 10.39; p.001); concurrent immunosuppressive therapy (OR 2.67, 1.10– 6.47; p.029); intravascular (OR 4.43, 1.79– 10.92; p.001) and urinary catheterization (OR 4.83, 1.87– 12.47; p.001); and serum albumin < 3 g/dL (OR 4.13, 1.05– 16.33; p.043). A multivariate analysis identified two independent factors associated with mortality: being on mechanical ventilation (OR 4.43, 1.86– 10.59; p 0.001) and receiving concurrent immunosuppressive therapy (OR 2.26, 1.04– 6.82; p 0.042).
Conclusion: S. maltophilia can cause nosocomial infections with high mortality, particularly in patients with a prolonged hospitalization. Concurrent immunosuppressive therapy and being on mechanical ventilation are the independent factors associated with a fatal outcome.
Keywords: Stenotrophomonas maltophilia infection, hospitalized patients, mortality
Introduction
Stenotrophomonas maltophilia is a motile, aerobic, glucose non-fermenting, gram-negative bacterium.1 S. maltophilia has been recognized as a cause of severe nosocomial infections, mainly in debilitated patients, such as bloodstream infections and pneumonia.2
S. maltophilia infections have been associated with high mortality,3–5 with one study reporting that the crude mortality rates in uncontrolled clinical trials ranged from 21% to 69%.6 In 2007–2008, S. maltophilia was the third most frequent, non-fermentative, gram-negative bacterium causing hospital-associated bacteremia at Siriraj Hospital.7 The risk factors for S. maltophilia colonization and infections include previous exposure to broad-spectrum antibiotics, prolonged hospitalization, an intensive care unit stay, mechanical ventilation, use of intravascular devices, and an immunocompromised host.8,9
S. maltophilia is usually resistant to several antibiotics because it confers various mechanisms of drug resistance, such as decreased permeability, the production of beta-lactamase and carbapenemase enzymes, the production of aminoglycoside-modifying enzymes, and the presence of multidrug efflux pumps. The treatment of S. maltophilia is challenging due to its multidrug resistance. The administration of appropriate antibiotics to combat this organism is occasionally delayed because physicians do not recognize the risk factors and clinical characteristics of S. maltophilia infections, which later leads to high mortality.10,11 The clinical characteristics and treatment outcomes of S. maltophilia infections in Thailand have rarely been described. This study set out to establish the clinical characteristics of patients who had S. maltophilia infections and to identify the risk factors associated with mortality. Knowing such information about S. maltophilia infections may increase physicians’ abilities to make early diagnoses, thereby improving the clinical outcomes.
Patients and Methods
Study Population
We conducted a retrospective study to determine the clinical characteristics and factors associated with mortality of S. maltophilia infections among hospitalized adult patients at Siriraj Hospital. The clinical characteristics, microbiological data, and treatment outcomes were collected from medical records December 2013–December 2016. Subjects aged over 18 years who had at least one positive culture of S. maltophilia isolated from clinical samples were included. We only enrolled subjects who had clinical signs and/or findings of an S. maltophilia infection.
A positive culture without evidence of a clinical infection was considered to be colonization, and it was thus excluded from the analysis. The terms “infections” and “colonization” were defined according to the US CDC definitions for nosocomial infection surveillance.12 In the case of patients who had multiple episodes of S. maltophilia, only the first infection episode was analyzed by the current study.
Data Collection
The medical records of the enrolled patients were reviewed to obtain relevant information. Details of the following were compiled: demographic data; hospitalization unit (namely, the medical, surgical, or intensive care unit); comorbidities; previous antimicrobial therapy; the use of systemic corticosteroids, chemotherapy, or radiation therapy; recent operations or medical procedures; placement of catheterization; duration of hospitalization; type of infection attributed to S. maltophilia, co-infection with other organisms; treatment; outcomes of the S. maltophilia infection; and all-cause in-hospital mortality.
In our institute, a conventional gram-negative biochemical-testing panel is usually performed to identify gram-negative bacterial isolates, including S. maltophilia. If the isolate identification remains unclear, the automated identification system, such as VITEK system, will be tested for the species identification. Regarding the Clinical and Laboratory Standards Institute (CLSI), a disk diffusion method of three antimicrobial agents, namely minocycline, levofloxacin, and trimethoprim-sulfamethoxazole is routinely performed for the antimicrobial susceptibility testing (AST) of S. maltophilia isolates.
In addition, the microbiological data collected comprised the source and type of clinical sample positive for S. maltophilia isolates; co-pathogens isolated from the same sample in which S. maltophilia was first identified; and the antimicrobial susceptibilities of the S. maltophilia isolates.
Definitions
A “hospital-acquired infection” was defined as an episode of infection that occurred more than 48 hours after hospitalization. A “community-acquired infection” was defined as an infection onset occurring at the home of a patient who had no recent contact with a healthcare facility or an infection onset occurring within the first 48 hours of hospitalization. “Immunosuppression” was defined as the administration of immunosuppressive therapy for an autoimmune disease, of chemotherapy for neoplasia, or of systemic corticosteroids; or the presence of leukemia, lymphoma, an HIV-infection, or a splenectomy. The source of each S. maltophilia infection was determined clinically and was based on the location of the active site of infection, with the S. maltophilia isolates identified and assessed by the investigators.
As to the antimicrobial treatments, “empirical antimicrobial therapy” was defined as the antimicrobial agent(s) administered from the infection onset until the initial isolation of S. maltophilia. “Definite antimicrobial therapy” was defined as the antimicrobial agent(s) administered soon after the culture and the antimicrobial susceptibility results were available.
The primary outcome was the all-cause in-hospital mortality, which was defined as death from any cause during hospitalization.
Sample Size Calculation
Our study used the sequential organ failure assessment (SOFA) score being one of the factors significantly associated with the in-hospital mortality for sample size calculation. According to Saugel et al, the median SOFA score in the survival group was 8 (range 1–16), whereas the median SOFA score in the non-survival group was 12.5 (range 4–21).13 The sample size was determined by the Mann–Whitney U-test with 5%Type I error and 20% power of test, in which a total of 32 subjects were required for each factor. We estimated that at least three variables would be identified for being factors significantly associated with in-hospital mortality. Thus, 100 subjects were included in the study.
Statistical Analyses
Data were analyzed using IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA). A univariate analysis was performed to assess the factors associated with all-cause in-hospital mortality. Student’s t-test was used for continuous variables, and the chi-squared test or Fisher’s exact test was used for categorical variables, as appropriate. Any variable determined to have a significant association with mortality in the analysis was subsequently entered in a multivariate, forward, stepwise (likelihood ratio), logistic regression model. A p-value of ≤0.05 was considered statistically significant.
Results
Patient Characteristics
Of the 1221 subjects whose clinical samples grew S. maltophilia during the study period, 213 were randomly selected for chart review. A total of 100 patients with a true S. maltophilia infection were identified. The median age of those subjects was 66 years; 47 were males; 46 were critically ill, having a median Acute Physiological Assessment and Chronic Health Evaluation (APACHE) II score of 18 (2–32); and 100 episodes (100%) of hospital-acquired infections were confirmed. Only 2 infection episodes were acquired infections following the hospital discharge. One of those 2 patients developed S. maltophilia septicemia following a 1-day-long endoscopic retrograde cholangiopancreatography procedure, while the other patient was diagnosed with a complicated urinary tract infection due to a percutaneous nephrostomy infection. The most frequent infections were respiratory tract infections (53%) and bloodstream infections (25%), with the latter comprised of catheter-related bloodstream infections (14%) and primary bacteremia (11%). Forty-three patients (43%) developed bacteremia following the onset of the S. maltophilia infection. The median length of hospitalization was 19 days before infection onset. Only 16 (16%) patients received appropriate empirical antimicrobial treatment, whereas 72 (72%) patients received appropriate definite antimicrobial treatment after the culture results were known. Additional baseline characteristics and clinical data of the subjects are detailed in Table 1.
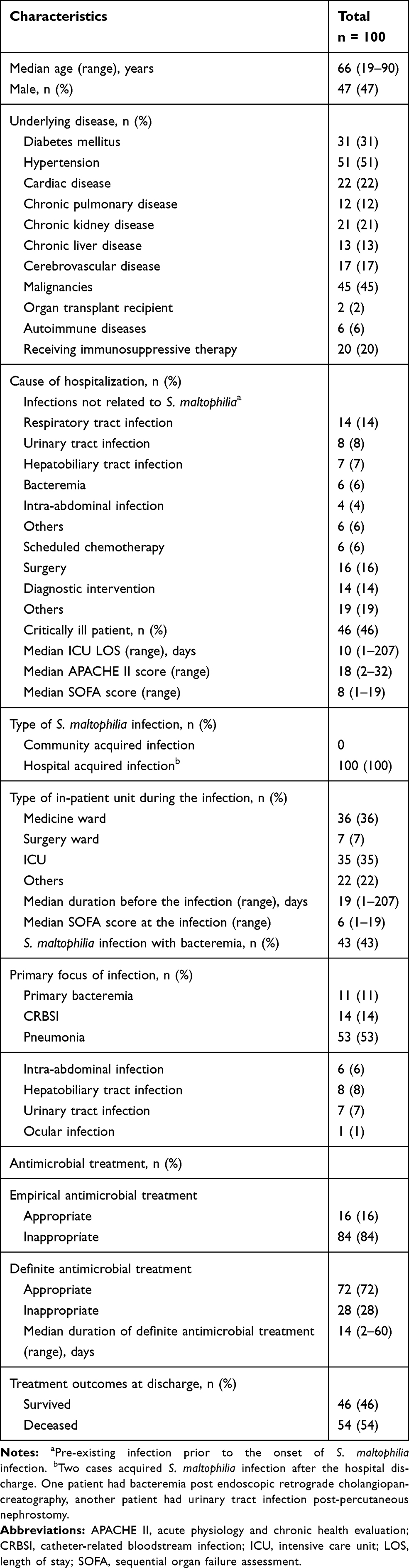 |
Table 1 Baseline Characteristics, Clinical Data, and Treatment Outcomes of Hospitalized Patients Who Had S. maltophilia Infections |
Regarding the clinical characteristics of the patients with an S. maltophilia infection, most (91%) had received prior antibiotic treatments, mainly with carbapenems (56%); and 58 (58%) were on mechanical ventilation (58%). Moreover, 77 (77%) had retained intravascular catheterization: 37 (37%) of these had a central venous catheter, while 40 (40%) had an indwelling catheter (usually a double lumen catheter, Hickman catheter, or arterial line). Additional clinical characteristics are listed in Table 2.
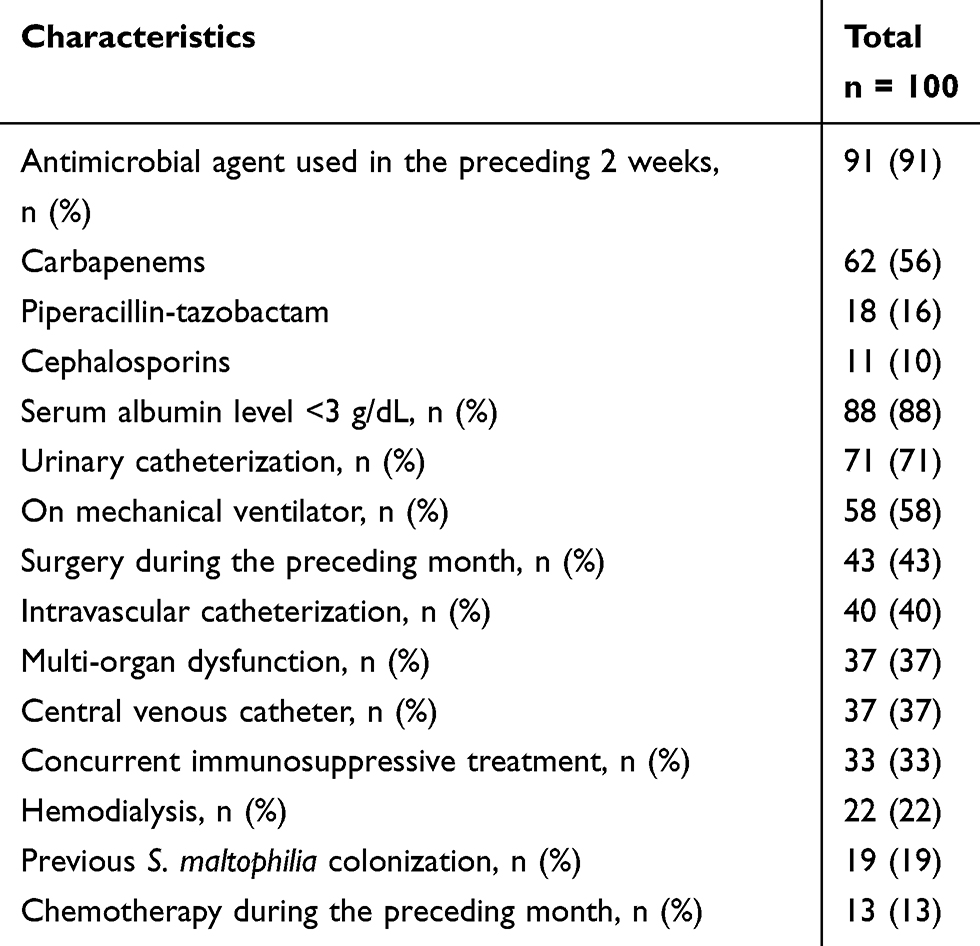 |
Table 2 Clinical Characteristics at the Onset of the S. maltophilia Infections |
Microbiological Data
Sixty-five patients (65%) had isolations of polymicrobial organisms with two or more organisms. The samples with multiple organisms were obtained from the respiratory tract (35 samples), bloodstream (14), urine (7), intra-abdominal region (5), and hepatobiliary system (4 samples). Gram-negative bacteria were the most common organisms recovered concomitantly with S. maltophilia; they included Enterobacteriaceae (25 isolates), A. baumannii (19 isolates), and P. aeruginosa (12 isolates). Details of the organisms co-isolated with S. maltophilia are in Table 3.
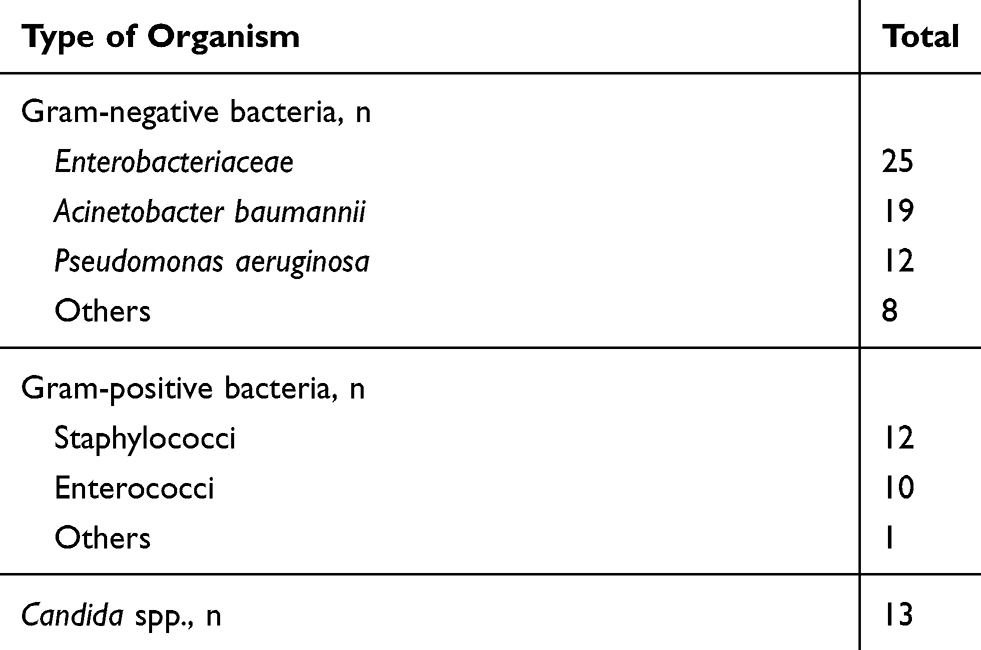 |
Table 3 The Number of Organisms Co-Isolated with S. maltophilia in the Index Culture Specimen for Diagnosis of S. maltophilia Infections from 65 Patients |
Antimicrobial susceptibility testing of the S. maltophilia isolated from the 100 patients revealed a 100% susceptibility to minocycline, 94% susceptibility to levofloxacin, and 91% susceptibility to trimethoprim-sulfamethoxazole. The percentage of antimicrobial susceptibility testing profile of 100 S. maltophilia isolates from the study subjects is shown in Table 4.
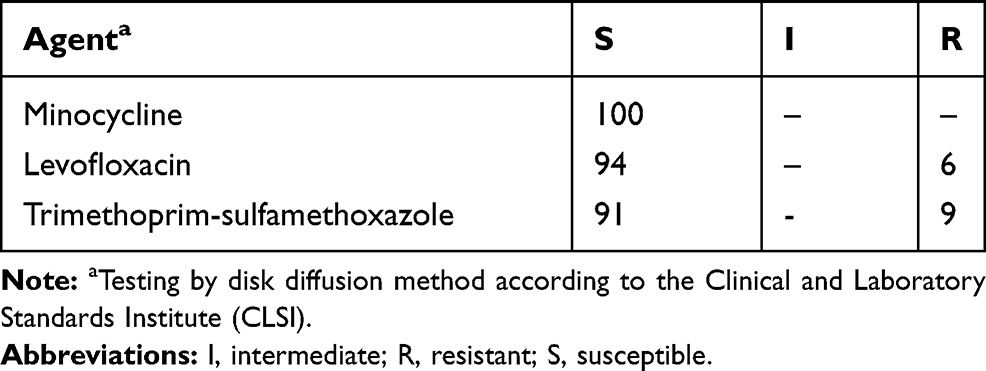 |
Table 4 Percentage of Antimicrobial Susceptibility Testing Profile of 100 S. maltophilia Isolates from the Study Subjects |
Factors Associated with in-Hospital Mortality
The overall, in-hospital mortality rate was 54%. In the univariate analysis, the variables that were significantly associated with increased, all-cause in-hospital mortality were a pre-existing respiratory infection (OR 6.28, 1.33–29.78; p.021); a critical illness (OR 3.33, 1.45–7.62; p.005); multi-organ dysfunction (OR 2.44, 1.05–5.70; p.039); being on mechanical ventilation (OR 4.44, 1.90–10.39; p.001); receiving concurrent immunosuppressive therapy (OR 2.67, 1.10–6.47; p.029); intravascular catheterization (OR 4.43, 1.79–10.92; p.001); urinary catheterization (OR 4.83, 1.87–12.47; p.001); and a serum albumin level of <3 g/dL (OR 4.13, 1.05–16.33; p.043). In 65 patients with the polymicrobial isolations, 29 (44.6%) survived, and 36 (55.4%) had fatal outcomes. In 35 patients who had S. maltophilia infection alone, 17 (48.6%) survived, and 18 (51.4%) had fatal outcomes. The subsequent multivariate logistic regression model was adjusted for the polymicrobial organism variables. That analysis revealed that 2 factors were independently associated with mortality: concurrent immunosuppressive therapy (OR 2.26, 1.04–6.82; p 0.042) and mechanical ventilation (OR 4.43, 1.86–10.59; p 0.001; Table 5). Inappropriate empirical antimicrobial therapy did not have a significant impact on mortality in this study. Of the 54 patients who died, 44 (81.5%) received inadequate empirical antimicrobial treatment for S. maltophilia, whereas of the 46 who survived, 40 (87%) received inadequate empirical antimicrobial treatment (p 0.459). The administration of definite antimicrobial treatment was also not associated with mortality: 36 out of the 46 (78.3%) patients who survived, versus 36 out of the 54 (66.7%) patients who died, received appropriate definite antimicrobial therapy (p 0.201).
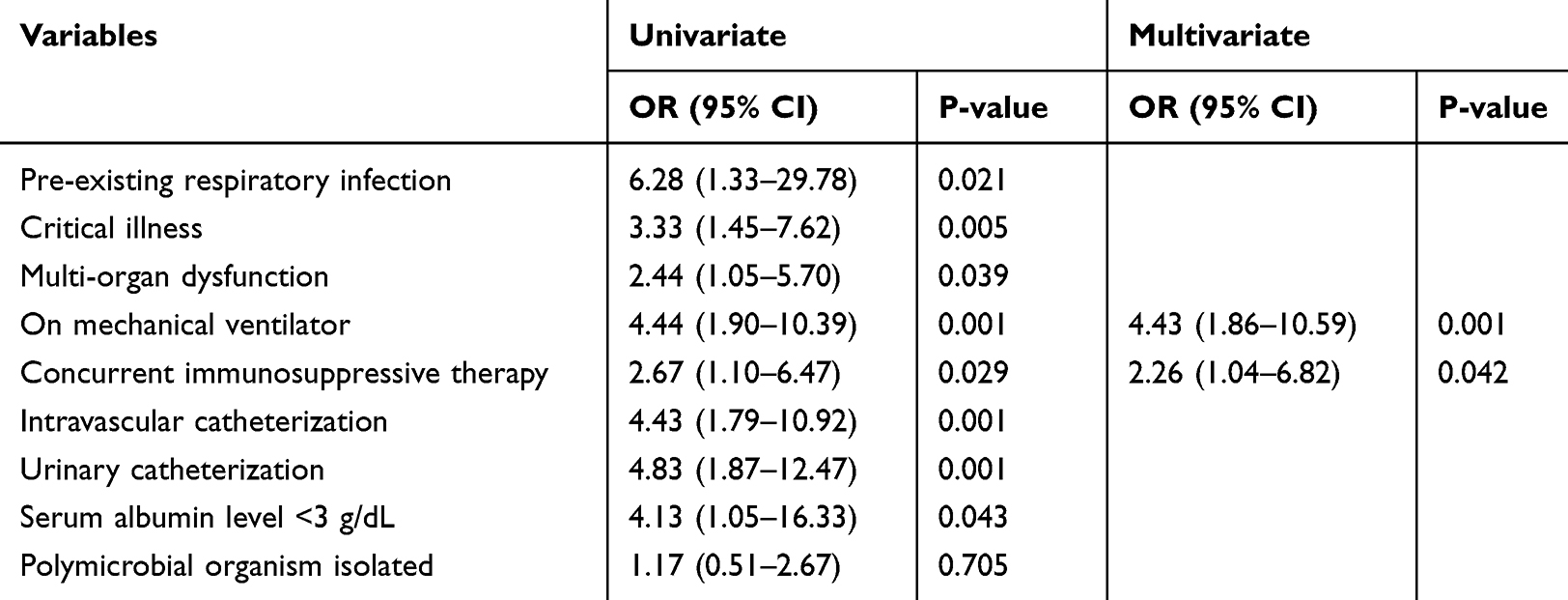 |
Table 5 Factors Associated with All-Cause in-Hospital Mortality of Patients Who Had S. maltophilia Infection |
Discussion
In this study, we reviewed 100 cases with an S. maltophilia infection during a 4-year period at a large tertiary care center, Siriraj Hospital, Bangkok, Thailand. The cases of S. maltophilia infection were drawn from several hospital wards, but mainly from the medicine ward and the intensive care unit. Almost all infections occurred during inpatient care. The median duration of hospitalization before the onset of the infections was 19 days, which was similar to the findings of several other studies.14,15
The main characteristics of the patients who developed S. maltophilia infections were the presence of prior antimicrobial treatment (especially with carbapenems); being cannulated with a vascular catheter; being on mechanical ventilation; having had previous surgery; and a low serum albumin level. A number of patients had immunosuppressed conditions due to underlying disease, receiving corticosteroids, or chemotherapy. Those characteristics were also identified by earlier studies.16–20 Moreover, the most frequent S. maltophilia infections in the current study were similar to those observed in other relevant studies, namely, respiratory tract infections, followed by bloodstream infections and intra-abdominal infections.3,4,15
Although the in-hospital mortality rate of 54% in our study was high, it was consistent with the rates of 20–60% reported by a number of published studies.20–22 While polymicrobial organism isolations constituted a considerable proportion in our study, other more virulent pathogens may be a more important mortality risk factor. The multivariate analysis was adjusted for the polymicrobial organism variables because it was difficult to ascertain the pathogenic role of S. maltophilia, especially in cases of polymicrobial organism isolation. However, the mortality rate of patients with polymicrobial organism isolations was not significantly different from that of patients with only S. maltophilia isolation. Co-infection with multiple isolates might not indicate the true polymicrobial infection, but it may represent microbial colonizations in a prolonged hospitalized patient, which did not alter the patient’s prognosis. The only independent risk factors associated with mortality in patients with S. maltophilia infections were receiving concurrent immunosuppressive therapy and being on mechanical ventilation, which was similar to the results of other research.10,22 Two independent risk factors associated with mortality that were identified by some previous studies—namely, admission to an intensive care unit and an APACHE II score of >1516,17,22 are not consistent with our research. These discrepancies were most probably because of different indications being used by our hospital for intensive care unit admission, and inaccurate APACHE II scores in our medical records. Surprisingly, the inappropriateness of empirical and definitive antimicrobial therapy was not associated with mortality in the current study. In contrast, previous studies have reported that the initial administration of inappropriate antimicrobial treatment was a significant predictor of mortality.19,23,24 Several conditions, such as age, comorbidity, severity of illness, immunosuppression, and malnutrition, may contribute to an increase in the rate of mortality.
For the treatment of S. maltophilia infections, trimethoprim-sulfamethoxazole has long been considered as the first-line therapeutic agent; nevertheless, a 2%–25% resistance rate has been reported.25 The present research demonstrated that levofloxacin and trimethoprim-sulfamethoxazole were still highly active against S. maltophilia isolates, which is different from the findings of previous studies.15,17 Nevertheless, those two agents are frequently prescribed by treating physicians in hospitals as the empirical and targeted therapy for patients who have S. maltophilia infections. When the isolates were susceptible to those agents, levofloxacin did not show significantly more benefit over trimethoprim-sulfamethoxazole in patients with S. maltophilia infections or bacteremia.26,27 However, the rates of susceptibility of fluoroquinolones and trimethoprim-sulfamethoxazole have varied (21%–82%, and 81%–85%, respectively) in different studies.15,17 Some previous studies found fluoroquinolone-resistant strain and inappropriate fluoroquinolone treatment when the organisms resistant to were factors predicting the non-survival outcome.28,29 Although minocycline has demonstrated very promising in vitro activity against the isolates, this agent is unfortunately not presently available in Thailand.
Our study had some limitations. The chief one was its retrospective design, which prevented us from accurately differentiating between true infections and colonization with S. maltophilia isolates and other polymicrobial organisms, thereby hampering accurate diagnosis. Moreover, as we used the in-hospital all-cause mortality rate as the primary outcome, the effects of underlying diseases or other medical conditions could not be excluded. In addition, given that the subjects were drawn from only a single tertiary center, our results may be limited and not able to be applied to different settings. A prospective, well-designed, case–control study should be conducted to more precisely evaluate the risk factors of S. maltophilia infections, the impact of appropriate antimicrobial therapy, and the mortality outcome.
Conclusion
S. maltophilia can cause nosocomial infections with high mortality, particularly in patients who have prolonged hospitalization, have a critical illness, are on mechanical ventilation, have been cannulated with a vascular catheter or are malnourished. The independent factors associated with a fatal outcome are being on a mechanical ventilator and receiving concurrent immunosuppressive therapy.
Abbreviations
APACHE II, acute physiology and chronic health evaluation; AST, antimicrobial susceptibility testing; CDC, Centers for Disease Control and Prevention; CRBSI, catheter-related bloodstream infection; CLSI, Clinical and Laboratory Standards Institute; HIV, human immunodeficiency virus; I, intermediate; ICU, intensive care unit; LOS, length of stay; R, resistant; S, susceptible; SOFA, sequential organ failure assessment; US, United State.
Data Sharing Statement
Primary datasets from this study will be available from the corresponding author upon request.
Ethics Approval and Informed Consent
The study protocol was approved by the Siriraj Institutional Review Board [Reference number 317/2560(EC2)] with waiving written informed consent for deidentified patient information.
Acknowledgments
We express our sincere thanks to staff at Bacteriology Unit, Department of Microbiology, Siriraj Hospital, for assisting with the microbiological data in this study, and Ms. Khemajira Karaketklang for helping with the data analyses.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brooke JS. Stenotrophomonas maltophilia: an emerging global opportunistic pathogen. Clin Microbiol Rev. 2012;25(1):2–41.
2. Looney WJ, Narita M, Muhlemann K. Stenotrophomonas maltophilia: an emerging opportunist human pathogen. Lancet Infect Dis. 2009;9(5):312–323. doi:10.1016/S1473-3099(09)70083-0
3. Fihman V, Le Monnier A, Corvec S, et al. Stenotrophomonas maltophilia–the most worrisome threat among unusual non-fermentative gram-negative bacilli from hospitalized patients: a prospective multicenter study. J Infect. 2012;64(4):391–398. doi:10.1016/j.jinf.2012.01.001
4. Senol E, DesJardin J, Stark PC, Barefoot L, Snydman DR. Attributable mortality of Stenotrophomonas maltophilia bacteremia. Clin Infect Dis. 2002;34(12):1653–1656. doi:10.1086/340707
5. VanCouwenberghe CJ, Farver TB, Cohen SH. Risk factors associated with isolation of Stenotrophomonas (Xanthomonas) maltophilia in clinical specimens. Infect Control Hosp Epidemiol. 1997;18(5):316–321. doi:10.2307/30141224
6. Paez JI, Costa SF. Risk factors associated with mortality of infections caused by Stenotrophomonas maltophilia: a systematic review. J Hosp Infect. 2008;70(2):101–108. doi:10.1016/j.jhin.2008.05.020
7. Rattanaumpawan P, Ussavasodhi P, Kiratisin P, Aswapokee N. Epidemiology of bacteremia caused by uncommon non-fermentative gram-negative bacteria. BMC Infect Dis. 2013;13167.
8. Jeon YD, Jeong WY, Kim MH, et al. Risk factors for mortality in patients with Stenotrophomonas maltophilia bacteremia. Medicine (Baltimore). 2016;95(31):e4375. doi:10.1097/MD.0000000000004375
9. Xun M, Zhang Y, Li BL, Wu M, Zong Y, Yin YM. Clinical characteristics and risk factors of infections caused by Stenotrophomonas maltophilia in a hospital in northwest China. J Infect Dev Ctries. 2014;8(8):1000–1005. doi:10.3855/jidc.4236
10. Sanchez MB, Hernandez A, Martinez JL. Stenotrophomonas maltophilia drug resistance. Future Microbiol. 2009;4(6):655–660. doi:10.2217/fmb.09.45
11. Vila J, Marco F. Interpretative reading of the non-fermenting gram-negative bacilli antibiogram. Enferm Infecc Microbiol Clin. 2002;20(6):304–310. doi:10.1016/S0213-005X(02)72803-6
12. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–332. doi:10.1016/j.ajic.2008.03.002
13. Saugel B, Eschermann K, Hoffmann R, et al. Stenotrophomonas maltophilia in the respiratory tract of medical intensive care unit patients. Eur J Clin Microbiol Infect Dis. 2012;31(7):1419–1428. doi:10.1007/s10096-011-1459-8
14. Garazi M, Singer C, Tai J, Ginocchio CC. Bloodstream infections caused by Stenotrophomonas maltophilia: a seven-year review. J Hosp Infect. 2012;81(2):114–118. doi:10.1016/j.jhin.2012.02.008
15. Samonis G, Karageorgopoulos DE, Maraki S, et al. Stenotrophomonas maltophilia infections in a general hospital: patient characteristics, antimicrobial susceptibility, and treatment outcome. PLoS One. 2012;7(5):e37375. doi:10.1371/journal.pone.0037375
16. Aisenberg G, Rolston KV, Dickey BF, Kontoyiannis DP, Raad II, Safdar A. Stenotrophomonas maltophilia pneumonia in cancer patients without traditional risk factors for infection, 1997-2004. Eur J Clin Microbiol Infect Dis. 2007;26(1):13–20. doi:10.1007/s10096-006-0243-7
17. Del Toro MD, Rodriguez-Bano J, Herrero M, et al. Clinical epidemiology of Stenotrophomonas maltophilia colonization and infection: a multicenter study. Medicine (Baltimore). 2002;81(3):228–239. doi:10.1097/00005792-200205000-00006
18. Denton M, Kerr KG. Microbiological and clinical aspects of infection associated with Stenotrophomonas maltophilia. Clin Microbiol Rev. 1998;11(1):57–80.
19. Hanes SD, Demirkan K, Tolley E, et al. Risk factors for late-onset nosocomial pneumonia caused by Stenotrophomonas maltophilia in critically ill trauma patients. Clin Infect Dis. 2002;35(3):228–235. doi:10.1086/341022
20. Muder RR, Harris AP, Muller S, et al. Bacteremia due to Stenotrophomonas (Xanthomonas) maltophilia: a prospective, multicenter study of 91 episodes. Clin Infect Dis. 1996;22(3):508–512. doi:10.1093/clinids/22.3.508
21. Lai CH, Chi CY, Chen HP, et al. Clinical characteristics and prognostic factors of patients with Stenotrophomonas maltophilia bacteremia. J Microbiol Immunol Infect. 2004;37(6):350–358.
22. Wang WS, Liu CP, Lee CM, Huang FY. Stenotrophomonas maltophilia bacteremia in adults: four years’ experience in a medical center in northern Taiwan. J Microbiol Immunol Infect. 2004;37(6):359–365.
23. Friedman ND, Korman TM, Fairley CK, Franklin JC, Spelman DW. Bacteraemia due to Stenotrophomonas maltophilia: an analysis of 45 episodes. J Infect. 2002;45(1):47–53. doi:10.1053/jinf.2002.0978
24. Kwa AL, Low JG, Lim TP, Leow PC, Kurup A, Tam VH. Independent predictors for mortality in patients with positive Stenotrophomonas maltophilia cultures. Ann Acad Med Singapore. 2008;37(10):826–830.
25. Chang LL, Lin HH, Chang CY, Lu PL. Increased incidence of class 1 integrons in trimethoprim/sulfamethoxazole-resistant clinical isolates of Stenotrophomonas maltophilia. J Antimicrob Chemother. 2007;59(5):1038–1039. doi:10.1093/jac/dkm034
26. Ko JH, Kang CI, Cornejo-Juárez P, et al. Fluoroquinolones versus trimethoprim-sulfamethoxazole for the treatment of Stenotrophomonas maltophilia infections: a systematic review and meta-analysis. Clin Microbiol Infect. 2019;25(5):546–554. doi:10.1016/j.cmi.2018.11.008
27. Wang YL, Scipione MR, Dubrovskaya Y, Papadopoulos J. Monotherapy with fluoroquinolone or trimethoprim-sulfamethoxazole for treatment of Stenotrophomonas maltophilia infections. Antimicrob Agents Chemother. 2014;58(1):176–182. doi:10.1128/AAC.01324-13
28. Kim EJ, Kim YC, Ahn JY, et al. Risk factors for mortality in patients with Stenotrophomonas maltophilia bacteremia and clinical impact of quinolone-resistant strains. BMC Infect Dis. 2019;19(1):754. doi:10.1186/s12879-019-4394-4
29. Sumida K, Chong Y, Miyake N, et al. Risk factors associated with Stenotrophomonas maltophilia bacteremia: a matched case-control study. PLoS One. 2015;10(7):e0133731. doi:10.1371/journal.pone.0133731
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.