Back to Journals » Clinical Epidemiology » Volume 14
Statin Use and Severe Acute Liver Injury Among Patients with Elevated Alanine Aminotransferase
Authors Verma SK ![]() , Huang J, Hutchinson HG, Estevez I
, Huang J, Hutchinson HG, Estevez I ![]() , Kuang K, Reynolds SL
, Kuang K, Reynolds SL ![]() , Schneeweiss S
, Schneeweiss S
Received 10 September 2022
Accepted for publication 30 November 2022
Published 14 December 2022 Volume 2022:14 Pages 1535—1545
DOI https://doi.org/10.2147/CLEP.S385712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Santosh K Verma,1,2 Joanna Huang,3 Howard G Hutchinson,4 Irisdaly Estevez,1 Kammy Kuang,1 Shannon L Reynolds,1 Sebastian Schneeweiss1,5
1Science, Aetion, Inc, New York, NY, USA; 2Department of Family Medicine and Community Health, University of Massachusetts Medical School, Worcester, MA, USA; 3Payer Evidence, AstraZeneca, Wilmington, DE, USA; 4Global Medicines Development, AstraZeneca, Wilmington, DE, USA; 5Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA
Correspondence: Santosh K Verma, Director, Science, Aetion, Inc, 50 Congress Street, Suite 1025, Boston, MA, 02109, USA, Tel +1 401-765-8817, Email [email protected]
Introduction: While serious liver injury among statin users is extremely rare, baseline liver enzyme testing is still recommended prior to initiating therapy. The benefit of such screening should be reevaluated based on empirical evidence. This study compared the risk of severe acute liver injury (SALI) between statin initiators with an elevated ALT (> 35U/L) matched to statin initiators with a normal ALT level (≤ 35U/L). Statin initiators with an elevated ALT were additionally compared against matched non-users.
Methods: The study created cohorts from Optum and MarketScan claims data. Exposed and comparison cohorts were propensity score (PS) matched in each dataset and findings were pooled using meta-analysis. Proportional hazards regression was used to estimate hazard ratios (HRs), and a prespecified non-inferiority margin for SALI was set at a HR of 1.8.
Results: 232,889 patients with elevated ALT were PS-matched to 232,889 with normal ALT level. The overall incidence rate of SALI was about 19/100,000 person-years among statin initiators. Statin initiators with elevated ALT had no meaningfully increased risk of SALI compared to those with normal ALT (HR=1.15; 95% CI 0.75 to 1.75). Comparing statin initiators with non-initiators with elevated ALT values equally yielded no increased risk (HR=0.76; 95% CI 0.52 to 1.11).
Conclusion: In this large population-based study, SALI in statin users was rare. Importantly, the results showed no evidence that baseline ALT status is a reliable indicator for an increased risk of severe liver injury among statin initiators.
Keywords: statins, liver injury, liver failure, alanine aminotransferase
Plain Language Summary
Research has shown that liver injury from statins is very rare. However, liver testing is still recommended before starting a treatment with statins. This requirement may increase the cost associated with the statin treatment and may reduce the use of statins, which are effective in preventing heart diseases. Our study has shown that baseline liver testing does not predict who may be at risk for severe liver injury among people who start statins.
Introduction
Statins are one of the most widely prescribed medications and have demonstrated substantial benefit in the primary and secondary prevention of cardiovascular (CV) events and mortality.1 Despite the clear benefits of statin therapy in preventing adverse CV events, approximately 55% of US adults who would qualify for treatment based on guidelines are not treated.2 While several factors contribute to undertreatment with statins, physician concerns about potential hepatotoxicity may be a contributing factor.3,4 The concerns for hepatotoxicity arose when the National Institute of Health Guidelines at the Fogarty conference in 1978 deemed liver alanine aminotransferase (ALT) values larger than three times the upper level of normal should be used as an indicator for induced liver injury, introducing this measure as standard monitoring practice in the statin clinical trials that followed in 1980s.5 In a survey conducted among primary care physicians, thirty-seven percent of respondents had falsely elevated perceptions of statin hepatotoxicity risk based on baseline liver Alanine Aminotransferase (ALT) values, and these perceptions correlated inversely with statin prescribing.4
Initial labeling for all statins recommended baseline liver enzyme testing and periodic liver enzyme monitoring because hepatic adverse effects were a concern.5 Based on a literature review assessing the overall incidence of liver failure among statin users, the incidence rate for acute liver failure (ALF) is estimated to be between 1 and 2 per 100,000 person-years.6,7 Overall, data published since 2006 continue to demonstrate the rarity of statin-associated liver failure.7,8
In February 2012, after extensive review of statin data, the US Food and Drug Administration (FDA) revised labels to remove the need for routine periodic monitoring of liver enzymes in patients taking statins. The FDA concluded that serious liver injury with statins is rare and unpredictable in individual patients; routine periodic monitoring of liver enzymes does not appear to be effective in detecting or preventing serious liver injury.9 However, baseline liver enzyme tests are still a requirement.9 The benefits of baseline liver enzyme testing are unproven, and the recommendation is based on expert opinion - the lowest quality of evidence.6 The requirement for baseline liver enzyme testing, however, may present a potential undue barrier to statin initiation.4
Despite the low risk of liver injury from statin use, a scientific question remains whether patients with elevated liver enzymes at baseline when initiating a statin are at higher risk of developing liver injury compared to those patients with normal liver enzymes at baseline. If the risk of developing liver injury is similar in the two groups, then routine baseline liver enzyme testing prior to initiation may not provide additional benefit, and a potential barrier to statin initiation could be eliminated.
In this study, we aim to address this gap in evidence by conducting an observational cohort study using two nationwide databases in the US to compare the risk of severe acute liver injury (SALI) between statin initiators with an elevated ALT value (>35 U/L) matched to statin initiators with a normal ALT level. We also compared the risk of SALI among statin initiators matched to non-initiators with an elevated ALT value (>35 U/L).
Methods
Data Source and Study Design
This cohort study was conducted using longitudinal insurance claims data from IBM MarketScan (about 63 million patients) and Optum Clinformatics Data Mart (about 196 million patients). For the primary objective, the risk of hospitalization or emergency department (ED) visit for SALI was compared among statin initiators with elevated ALT values (>35 U/L) with statin initiators with normal ALT values (≤35 U/L) during the 6 months before initiating the statins which was the cohort entry date. Among those with elevated ALT levels we compared statin initiators to non-initiators requiring at least one statin indication and a low-density lipoprotein (LDL) test during the six months before cohort entry. Given the potential for non-equivalency between the user and non-user arms, a negative outcome analysis, with humerus bone fracture as the negative outcome, was performed before conducting the final analysis to confirm the equipoise and detect any residual confounding.10 A sensitivity analysis with an active comparison group of patients initiating non-liver-toxic glaucoma medication was also conducted.11 However, due to the rare occurrence of SALI, the study did not have the sufficient size to achieve adequate power. We also conducted a positive outcome analysis, with LDL reduction, to test the sensitivity of the study to detect a change when LDL reduction is expected with statin use.
Appendix A depicts the longitudinal study design.
Study Population
The study included adult patients in the US enrolled in either of the Optum CDM database and the MarketScan Claims-Lab linked database who initiated statin medications or were eligible for the secondary comparison between statin new-users and non-initiators. The index date was the date of statin initiation with a 6-month washout period. For the secondary comparison of statin initiators to non-initiators, the index date for non-statin initiators was the initiation day of the matched treatment-exposed patient (statin initiator). Based on data availability, study eligibility ranged from January 1, 2007 to December 31, 2017 in Optum and from January 1, 2008 to December 31, 2017 in MarketScan. Both Optum and MarketScan data included non-identifiable information, and the study was exempt from IRB review.
Other eligibility criteria included continuous enrollment with pharmacy and medical benefits for a minimum of six months before the index date /cohort entry date. Participants were required to have at least one ALT liver enzyme test result and no statin use in the prior six months. In addition, for the secondary comparison between statin new-users and non-initiators, participants had an LDL-Cholesterol (LDL-C) test within 180 days before the ALT test and had an indication for statin initiation. Statin indication was defined as LDL-C greater than 160 mg/dl and age greater than 20 years; or a diabetes diagnosis and age greater than 40 years; or LDL-C between 70 and 160 mg/dl and older than 40 years and at least one of the risk factors or risk enhancing factors for cardiovascular disease.12
Patients with SALI, acute liver failure, or chronic liver disease at any time before cohort entry were excluded. In addition, patients with a diagnosis of cancer, jaundice, or hyperbilirubinemia (serum total bilirubin of greater than 2 times the upper limit of normal) were excluded.
The follow-up period began on the day after cohort entry (date of first statin dispensing) and continued until the end of the study, end of enrollment in a continuous health plan, occurrence of a study outcome, discontinuation of the statins or initiation of the statin medication in the non-user comparator cohort or diagnosis of chronic liver disease.
Treatment
Statin use was the primary drug exposure of interest (Appendix B). Patients were classified as treated from the day of the first statin dispensing until discontinuation. The last day of treatment was defined as the last day of a drug dispensing’s days supply, if no subsequent prescription was filled within the 90 days grace period. If the drug was refilled during the 90 days grace period, drug use was continued and the same algorithm was applied to this dispensing. Discontinuation was defined as 30 days after the last day of treatment. Sensitivity analyses were conducted around the allowable gap definitions of 30 and 60 days to assess statin discontinuation.
Study Outcome
Severe acute liver injury (SALI) with a hospitalization or an emergency department (ED) visit was defined using ICD-9 CM and ICD-10 CM diagnosis codes. Diagnosis codes included in at least two out of three validation studies were used to identify SALI (Appendix C).13–15
ALF, as identified by two hepatologists using claims data, was also explored as a narrow clinical outcome. However, due to the infrequency of ALF, the study did not have sufficient size to achieve adequate power.6,7,16
Patient Characteristics
A range of pre-exposure patient characteristics were considered in the propensity score (PS) matching (Table 1). They included demographic characteristics (age, gender, region), medications (medications associated with drug induced liver injury, anti-diabetics, pharmacy dispensed acetaminophen), comorbidities (obesity, alcohol consumption, Charlson comorbidity score, etc.) and the calendar year of the index date. All covariates were selected a priori and assessed during the 180 days before the index date.
 |
Table 1 Baseline Characteristics of Statin Initiators with Normal Baseline ALT Value and Statin Initiators with Abnormal Baseline ALT Value After Propensity Score Matching |
WCG IRB reviewed the study protocol, and the study was exempted from IRB review as information is recorded in such a manner that the identity of the human subjects cannot readily be ascertained directly or through identifiers linked to the subjects. The study authors did not contact the subjects.
Statistical Analysis
To control for baseline confounding, PS-matching with match ratios of 1:1 was used for the primary objective and 1:4 for the secondary objective. Logistic regression was used to estimate propensity scores. For the primary objective, PS-matching was performed using 1:1 nearest neighbor matching with a maximum matching caliper of 1%. For the secondary objective, PS-matching was performed using 1:4 nearest neighbor matching. In PS-matched analyses, confounding control was addressed through the matching process. After matching, the treatment effect measures were directly derived from the balanced populations without any further adjustment.
The treatment was specified as the dependent variable. All the predefined baseline covariates were used to calculate PS; no variable selection was conducted. Cases with missing values for any of the following covariates were excluded from the analyses: age, gender, region, acute liver injury, and ALT categories. Missing indicators were created for all other variables reported in Table 1. Missing categorical variables were coded as “Missing”, furthermore analyzed and reported with this missing indicator. For numeric variables, an additional binary covariate was created to indicate missing data and the missing numeric variable was assigned as value of 0. A caliper of 0.01 was used for matching and a standardized difference <0.1 was used to indicate balance between the comparison groups.17,18 Standardized differences for the primary and secondary objectives were reported in Appendices D and E, respectively.
Among statin new users, patients with an elevated ALT were compared to those matched with normal ALT using Cox proportional hazards regression assuming an on-treatment analysis.19 Incidence rate per 100,000 person-years, and hazard ratios (HR) with 95% confidence intervals (CI) are presented.
In addition, we performed a negative outcome analysis for the secondary objective comparing statin initiators versus non-initiators and the association with humerus bone fracture as the negative outcome. Randomized controlled trials have shown no relationship between statin use and risk of fractures.20,21 Similarly, in our analysis we found no association between statin initiation and humerus fracture providing confidence that our data analytic approach would unlikely be subject to major biases.
To test the sensitivity of the study in finding an expected association, we performed a positive outcome analysis for the secondary objective comparing statin initiators versus non-initiators and the association with LDL-C reduction as the positive outcome. In MarketScan, statin initiators experienced 17.95 mg/dl greater LDL-C reduction compared to non-initiators (95% CI 17.46, 18.44) in the first 6 months. Among those with LDL-C > 130 mg/dl at baseline, this difference was 25.79 mg/dl (95% CI 25.11, 26.47) and even among those with LDL-C was <= 130 mg/dl during baseline, the reduction was statistically significant (11.42 mg/dl; 95% CI 10.85, 11.99). Similar LDL-C reductions were observed in Optum data for the overall population (21.36 mg/dl; 95% CI 20.90, 21.82), those with LDL-C >130 mg/dl during baseline (31.37 mg/dl; 95% CI 30.74, 32.00) and those with LDL-C <=130 mg/dl during baseline (14.49 mg/dl; 95% CI 13.96, 15.01).
Once the potential for unmeasured confounding was assessed, the outcome of SALI was compared between the groups using Cox proportional hazards regression conducting an on-treatment analysis.
To obtain summary estimates of effect across both databases, a fixed effect meta-analysis was performed. Given the infrequency of the outcome, a non-inferiority margin of HR=1.8 was prespecified.22 For the primary objective, the necessary study size was calculated for event probability ranging from 17 to 21 per 100,000 participants, using one-sided alpha of 0.025, a non-inferiority margin of 1.8, and a 1:1 matching ratio between the exposed to reference groups. The event probability observed in the study was about 19 per 100,000 participants. Combining data from Optum and MarketScan provides 80% power to detect associations within the non-inferiority margin of HR=1.8.
Results
Primary Objective
In the Optum dataset, we identified 877,304 patients who initiated a statin prescription; among those, 740,396 patients had normal baseline ALT values and 136,908 patients had elevated baseline ALT values. In the MarketScan dataset, a total of 626,641 patients met the eligibility criteria; among those, 528,578 patients had normal baseline ALT values and 98,063 patients had elevated baseline ALT values. After 1:1 PS-matching, 135,264 and 97,625 statin initiators with elevated ALT were matched to statin initiators with normal ALT levels in the Optum and Marketscan databases, respectively (Table 1). All covariates reported in Table 1 were balanced after the PS-matching with the standardized difference of <0.1. Appendix D shows the standardized differences for each covariate and PS overlap curves.
In the Optum database, the statin initiators with normal ALT had an incidence rate of 13 events per 100,000 person-years; statin initiators with elevated ALT had an incidence rate of 15 events per 100,000 person-years (Table 2). These rates were 21 and 24 per 100,000 person-years in MarketScan, respectively. The PS-matched hazard ratio was 1.18 (95% CI: 0.64, 2.19) and 1.11 (95% CI: 0.62, 1.99) in Optum CDM and MarketScan, respectively, corresponding to a pooled hazard ratio of 1.15 (95% CI: 0.75, 1.75). Similar hazard ratios were observed in the sensitivity analyses with allowable gap of 30 and 60 days. The crude incidence rates of SALI among statin initiators who were not PS-matched were also not significantly different in both Optum and MarketScan databases (data not shown).
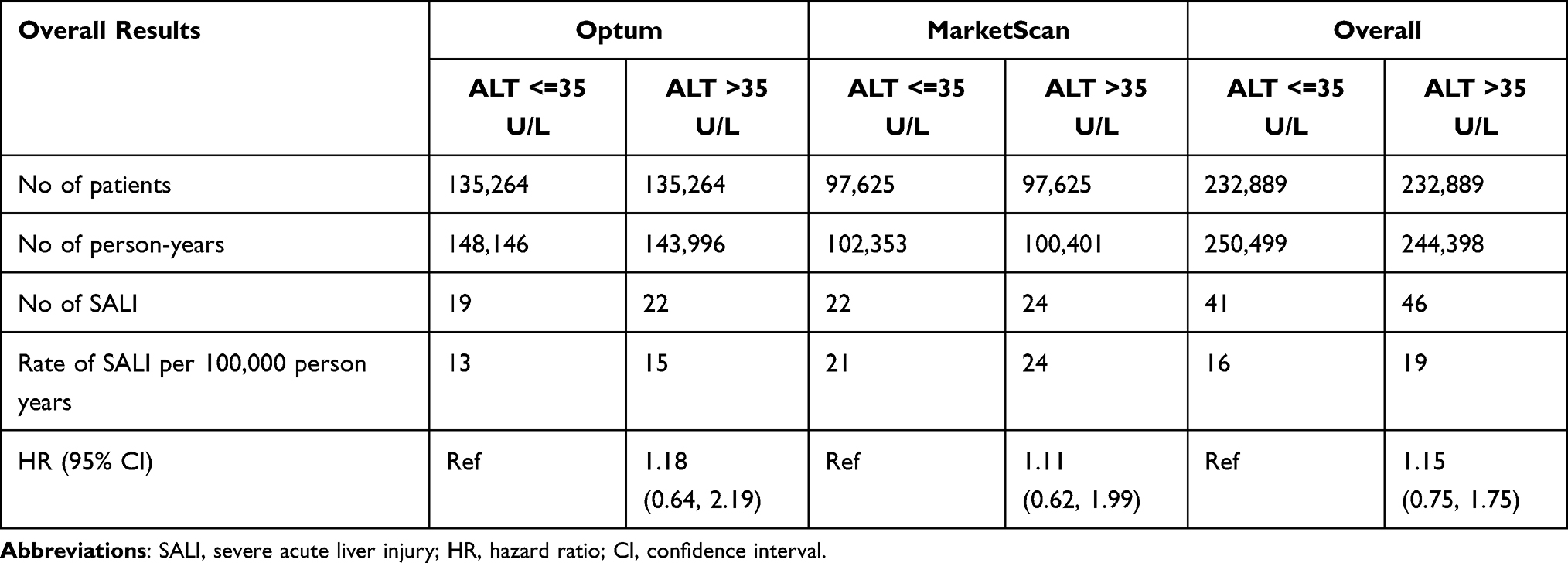 |
Table 2 Primary Objective - Propensity Score Matched Rate of SALI and Hazard Ratios Among Those with Elevated and Normal ALT Values |
Secondary Objective
In the Optum data, a total of 420,186 patients met the eligibility criteria as being indicated for statin initiation. Of these, 84,231 patients initiated statins and 335,955 patients did not (referent group). In the MarketScan data, a total of 345,001 patients were identified. Of these, 69,103 patients initiated statins and 275,898 patients did not (referent group). After the propensity score matching (1:4, statin initiators: non-initiators), 82,451 statin initiators were matched to 287,655 non-initiators in Optum and 66,959 statin initiators were matched to 229,545 non-initiators in MarketScan data (Table 3). All covariates were balanced after the PS-matching with standardized difference of <0.1 (Appendix E).
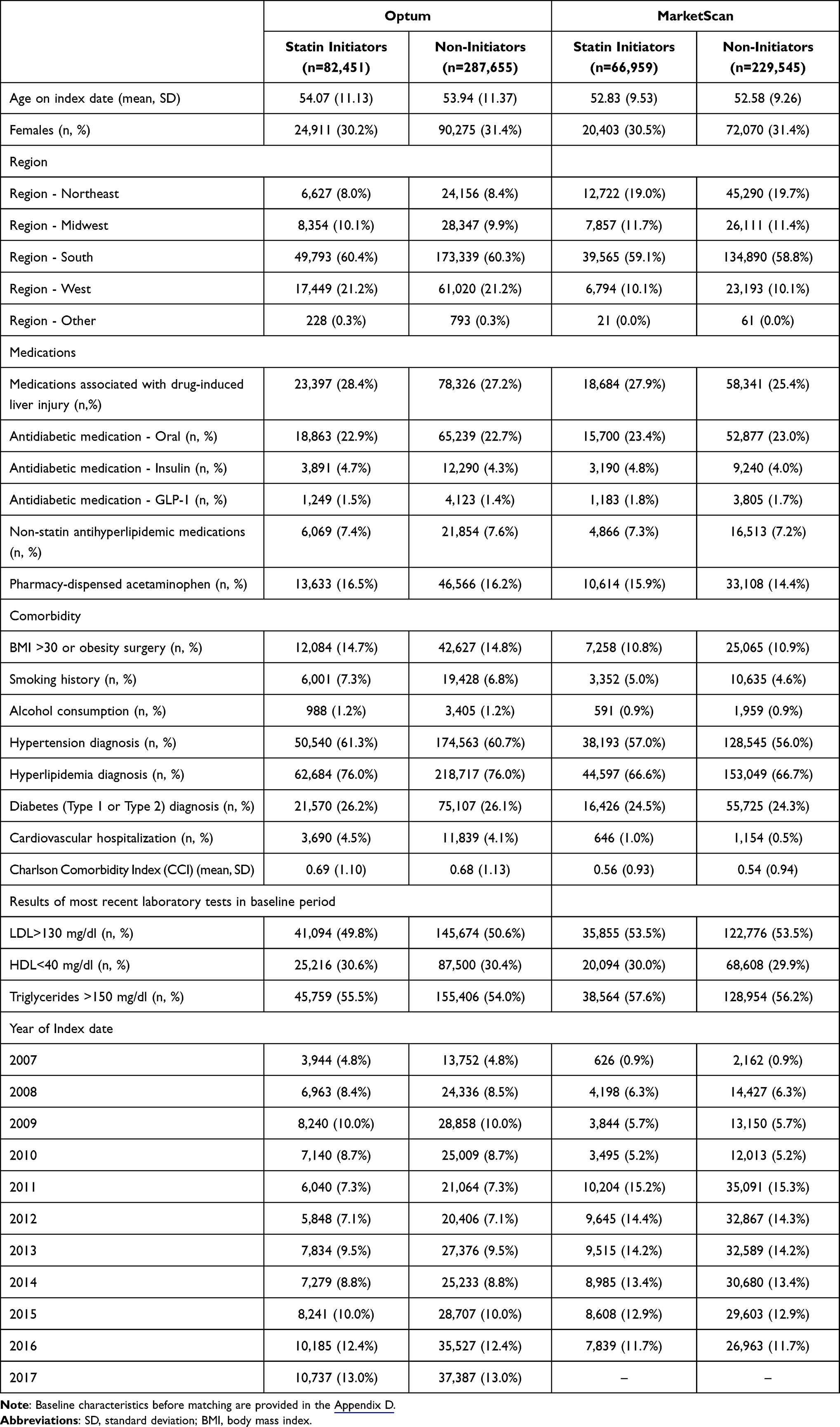 |
Table 3 Baseline Characteristics of Statin Initiators and Non-Initiators with Abnormal Baseline ALT Value After Propensity Score Matching |
In the Optum database, the statin initiators had an incidence rate of 14 events per 100,000 person-years; and the non-initiators had an incidence rate of 22 events per 100,000 person-years; rates were 27 and 29 per 100,000 person-years in MarketScan, respectively (Table 4). The PS-matched hazard ratio was 0.59 (95% CI: 0.33 to 1.06) and 0.91 (95% CI: 0.56 to 1.50) in Optum and MarketScan, respectively, corresponding to a pooled hazard ratio of 0.76 (0.52 to 1.11).
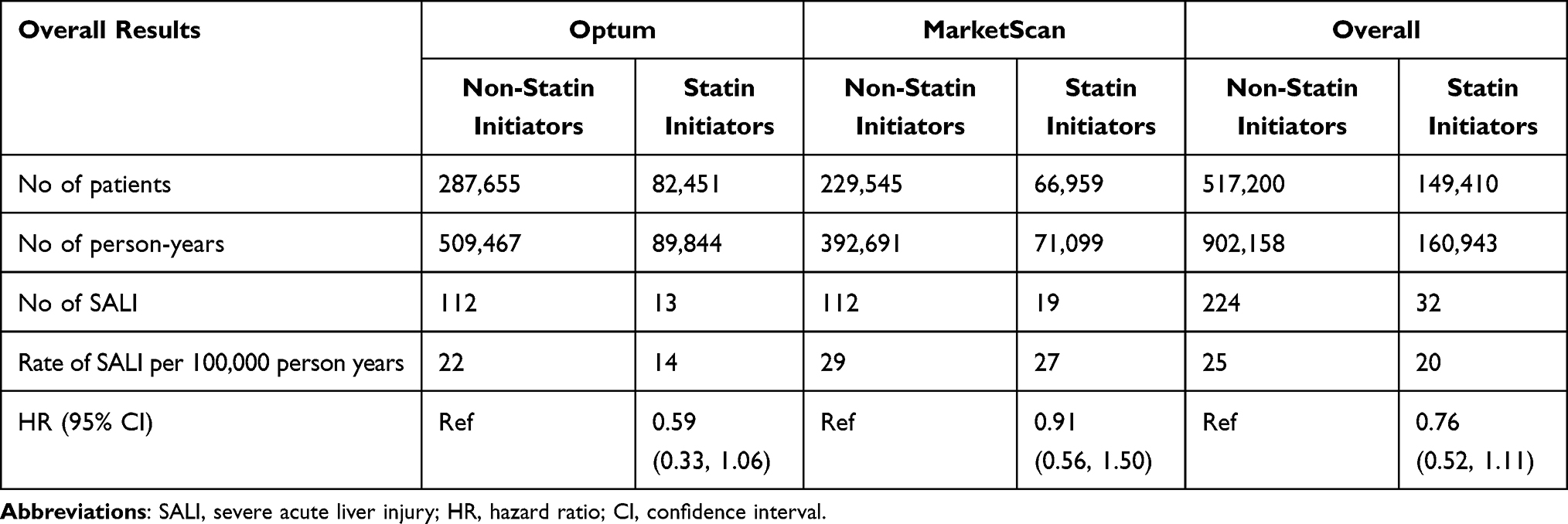 |
Table 4 Secondary Objective - Propensity Score Matched Rate of SALI and Hazard Ratios Among Statin Initiators and Non-Statin Initiators |
Discussion
In this contemporary PS-matched analysis of US insurance claims data, the risk of SALI was not meaningfully different between patients who initiated statins with elevated ALT levels and patients who initiated statins with normal ALT, yielding results below the predefined non-inferiority margin threshold. Similarly, among matched patients with an elevated baseline ALT value (>35 U/L), the risk of SALI was not meaningfully different between statin initiators and non-initiators. These results suggest that statin initiation is not associated with a significantly higher risk of SALI for patients with an elevated baseline ALT test value.
Due to the infrequency of ALF and SALI, examining the risk factors associated with severe liver injury has been challenging, requiring very large epidemiological data.6,7,16 Incidence rates of 10–14 acute liver injuries per 100,000 person-years have been previously reported.23,24 We found the incidence rate of SALI resulting in an emergency department visit or hospitalization ranged from 14–28 per 100,000 person-years in two large US-based datasets. Utilizing two large administrative databases and pooling their results allowed us to calculate stable estimates of SALI incidence despite its rarity.
Few epidemiologic studies have systematically examined the association between statin use and liver-related morbidity and mortality. Younoszai et al found that the rate of liver-related mortality was significantly lower among statin users compared to non-statin users in the National Health and Nutrition Examination Survey (NHANES III).25 Similarly, Avins et al found that exposure to lovastatin was not associated with an increased risk of adverse hepatic outcomes.26 Some studies have suggested statin use to be safe or even offer hepatoprotective benefits in patients with stable chronic liver disease, including those with non-alcoholic-fatty liver disease (NAFLD), chronic hepatitis C, and compensated cirrhosis.27,28 Francis and Forman reported that clinically relevant risks to the liver from statins remain remarkably low in patients without cirrhosis and should not outweigh the broad cardiovascular and potential hepatic benefits.29
Due to the lack of evidence between statin use and severe liver injury, the National Lipid Association’s Liver Expert Panel concluded that routine liver function monitoring might inappropriately encourage doctors to discontinue statin therapy upon detection of liver enzyme elevations.30 Likewise, the FDA concurs that routine periodic monitoring of liver enzymes does not appear to be effective in detecting or preventing serious liver injury given the rarity and unpredictability of serious liver injury with statins in individual patients. However, baseline liver enzyme testing prior to the initiation of a statin is still included in the prescribing information for statins.9
Similar to routine monitoring, liver function tests prior to statin initiation may create undue barriers to treatment for hyperlipidemia. In weighing the risk-benefit profile of statins, physicians may unnecessarily overestimate hepatotoxicity with a single, nonspecific liver function test, compromising the treatment of LDL.4 For example, NAFLD is a hepatic manifestation of the metabolic syndrome (MetS) that is highly associated with plasma lipoprotein abnormalities leading to increasing LDL and decreasing HDL as well as being one of the most common causes of elevated ALT.31–33 Patients with NAFLD may not be prescribed statins due to their physician’s false perceptions of a statin’s role in inducing hepatotoxicity based solely on a single ALT test. In fact, emergent data has shown that pre-existing liver dysfunction, such as NAFLD, nonalcoholic steatohepatitis, compensated cirrhosis, and compensated chronic liver disease, does not preclude statin use if treatment is clearly indicated.34 Similarly, our large-scale study using real-world data failed to find an association between SALI and statin initiation among those with elevated ALT levels compared to patients with normal ALT levels at baseline. In addition, no association between statin treatment and SALI among new statin users with an elevated ALT compared to non-initiators with an elevated ALT was observed. These results demonstrate that requisite liver enzyme testing prior to statin initiation is not a useful marker to predict liver injury.
Limitations
Given the rarity of SALI, the primary strength of the study was the utilization of two large contemporaneous datasets to appropriately power the study. Meta-analysis to obtain summary estimates of effect across both databases further strengthened the study and provided more precise effect estimates. As a positive control, the study was able to detect LDL-C reduction even among statin initiators who had LDL-C of less than or equal to 130 mg/dl during baseline. In addition, the Optum CDM and IBM MarketScan Commercial and Medicare claims databases included geographically diverse populations, increasing the generalizability of the study findings. However, despite the wide geographic and demographic coverage of both datasets, patients enrolled in some health plans, such as Medicaid, may be under-represented. In addition, some potential confounding factors associated with statin use among those with elevated ALT levels and development of SALI may not be fully captured in the claims data, such as alcohol intake, smoking history, obesity, etc. Despite PS-matching, there may still be some residual confounding. A negative outcome (humerus bone fracture) was used to assess residual confounding, and the risk of humerus bone fracture was not significantly different between the comparison groups in both Optum and MarketScan data, indicating limited residual confounding. The SALI outcome definition was developed based on validation studies using claim-based algorithms. However, outcome misclassification may be present as the positive predictive value (PPV) in each comparison group and within each database is unknown. Exposure misclassification may also be present as claims data denote the date of fills and days supply, but do not have data on actual use of medications. Both outcome and exposure misclassification may bias the results towards the null. Lastly, this study was sponsored by AstraZeneca, the maker of rosuvastatin; however, this study examined statins as a class of drugs and was conducted with high rigor pharmacoepidemiologic methods.
Conclusion
The risk of SALI among statin initiators with elevated ALT levels was not significantly different from matched statin initiators with normal ALT. Furthermore, among patients with elevated ALT levels, statin initiators and matched non-statin initiators had the same risk of SALI. The findings suggest that baseline ALT status is not a reliable indicator for increased risk of SALI for patients initiating statin therapy.
Funding
This work was funded by AstraZeneca.
Disclosure
Santosh K Verma is an employee of and own stock options or equity in Aetion, a software-enabled healthcare analytics company. Joanna Huang is an employee of AstraZeneca, the manufacture of rosuvastatin (a type of studied statins). Howard G. Hutchinson is an employee of AstraZeneca, the manufacture of rosuvastatin (a type of studied statins). Irisdaly Estevez is an employee of Aetion, a software-enabled healthcare analytics company, rapid analytics software used to conduct submitted work. Kammy Kuang worked on the study as an employee of Aetion, a software-enabled healthcare analytics company. Shannon L. Reynolds is an employee of and own stock options or equity in Aetion, a software-enabled healthcare analytics company. Sebastian Schneeweiss is participating in investigator-initiated grants to the Brigham and Women’s Hospital from UCB and Boehringer Ingelheim unrelated to the topic of this study. He is a consultant to Aetion Inc., a software manufacturer of which he owns equity. His interests were declared, reviewed, and approved by the Brigham and Women’s Hospital in accordance with their institutional compliance policies. The authors report no other conflicts of interest in this work.
References
1. Grundy Scott M, Cleeman James I, Noel Bairey MC, et al. Implications of recent clinical trials for the national cholesterol education program adult treatment panel III guidelines. Circulation. 2004;110(2):227–239. doi:10.1161/01.CIR.0000133317.49796.0E
2. Wong ND, Young D, Zhao Y, et al. Prevalence of the American College of Cardiology/American Heart Association statin eligibility groups, statin use, and low-density lipoprotein cholesterol control in US adults using the national health and nutrition examination survey 2011–2012. J Clin Lipidol. 2016;10(5):1109–1118. doi:10.1016/j.jacl.2016.06.011
3. Butalia S, Lee-Krueger RCW, McBrien KA, et al. Barriers and facilitators to using statins: a qualitative study with patients and family physicians. CJC Open. 2020;2(6):530–538. doi:10.1016/j.cjco.2020.07.002
4. Rzouq FS, Volk ML, Hatoum HH, Talluri SK, Mummadi RR, Sood GK. Hepatotoxicity fears contribute to underutilization of statin medications by primary care physicians. Am J Med Sci. 2010;340(2):89–93. doi:10.1097/MAJ.0b013e3181e15da8
5. Davidson C, Leevy C, Chamberlayne E. Guidelines for Detection of Hepatotoxicity Due to Drugs and Chemcials. Bethesda, MD: National Institutes of Health; 1979:79–313.
6. Bays H, Cohen DE, Chalasani N, Harrison SA. An assessment by the statin liver safety task force: 2014 update. J Clin Lipidol. 2014;8(3):S47–S57. doi:10.1016/j.jacl.2014.02.011
7. Karahalil B, Hare E, Koç G, Uslu İ, Şentürk K, Özkan Y. Hepatotoxicity associated with statins. Arh Hig Rada Toksikol. 2017;68(4):254–260. doi:10.1515/aiht-2017-68-2994
8. Reuben A, Koch DG, Lee WM. Drug-induced acute liver failure: results of a U.S. multicenter, prospective study. Hepatol Baltim Md. 2010;52(6):2065–2076. doi:10.1002/hep.23937
9. FDA Drug Safety Communication: important safety label changes to cholesterol-lowering statin drugs. FDA; 2019. https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-important-safety-label-changes-cholesterol-lowering-statin-drugs.
10. Ali MS, Prieto-Alhambra D, Lopes LC, et al. propensity score methods in health technology assessment: principles, extended applications, and recent advances. Front Pharmacol. 2019;10. doi:10.3389/fphar.2019.00973
11. Setoguchi S, Glynn RJ, Avorn J, Mogun H, Schneeweiss S. Statins and the risk of lung, breast, and colorectal cancer in the elderly. Circulation. 2007;115(1):27–33. doi:10.1161/CIRCULATIONAHA.106.650176
12. Arnett Donna K, Blumenthal Roger S, Albert Michelle A, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American heart association task force on clinical practice guidelines. Circulation. 2019;140(11):e596–e646. doi:10.1161/CIR.0000000000000678
13. Christine LB, James AK, Jordi C, et al. Validation of acute liver injury cases in a population-based cohort study of oral antimicrobial users. Curr Drug Saf. 2014;9(1):23–28. doi:10.2174/15748863113086660051
14. Lo RV, Carbonari DM, Saine ME, et al. Postauthorization safety study of the DPP-4 inhibitor saxagliptin: a large-scale multinational family of cohort studies of five outcomes. BMJ Open Diabetes Res Care. 2017;5:1. doi:10.1136/bmjdrc-2017-000400
15. Forns J, Cainzos‐Achirica M, Hellfritzsch M, et al. Validity of ICD‐9 and ICD‐10 codes used to identify acute liver injury: a study in three European data sources. Pharmacoepidemiol Drug Saf. 2019;28(7):965–975. doi:10.1002/pds.4803
16. Weiler N, Schlotmann A, Anton Schnitzbauer A, Zeuzem S, Welker M-W. The epidemiology of acute liver failure. Dtsch Ärztebl Int. 2020;117(4):43–50. doi:10.3238/arztebl.2020.0043
17. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–3107. doi:10.1002/sim.3697
18. Franklin JM, Rassen JA, Ackermann D, Bartels DB, Schneeweiss S. Metrics for covariate balance in cohort studies of causal effects. Stat Med. 2014;33(10):1685–1699. doi:10.1002/sim.6058
19. Schneeweiss S, Patorno E. Conducting real-world evidence studies on the clinical outcomes of diabetes treatments. Endocr Rev. 2021;bnab007. doi:10.1210/endrev/bnab007
20. Peña JM, Aspberg S, MacFadyen J, Glynn RJ, Solomon DH, Ridker PM. Statin therapy and risk of fracture: results from the Jupiter randomized clinical trial. JAMA Intern Med. 2015;175(2):171. doi:10.1001/jamainternmed.2014.6388
21. Reid IR, Hague W, Emberson J, et al. Effect of pravastatin on frequency of fracture in the LIPID study: secondary analysis of a randomised controlled trial. LANCET. 2001;357:4. doi:10.1016/S0140-6736(00)04042-3
22. McEvoy B, Frimpong E. Testing A noninferiority hypothesis: what to anticipate when the adverse event is rare. J Biopharm Stat. 2013;23(1):122–128. doi:10.1080/10543406.2013.735779
23. Chan KA, Truman A, Gurwitz JH, et al. A cohort study of the incidence of serious acute liver injury in diabetic patients treated with hypoglycemic agents. Arch Intern Med. 2003;163(6):728. doi:10.1001/archinte.163.6.728
24. Bell LN, Chalasani N. Epidemiology of idiosyncratic drug-induced liver injury. Semin Liver Dis. 2009;29(4):337–347. doi:10.1055/s-0029-1240002
25. Younoszai Z, Zheng L, Stepanova M, Erario M, Cable R, Younossi ZM. Statin use is not associated with liver related mortality. Ann Hepatol. 2014;13(1):84–90. doi:10.1016/S1665-2681(19)30908-1
26. Avins AL, Manos MM, Ackerson L, et al. Hepatic effects of lovastatin exposure in patients with liver disease. Drug Saf. 2008;31(4):325–334. doi:10.2165/00002018-200831040-00006
27. Simon TG, King LY, Zheng H, Chung RT. Statin use is associated with a reduced risk of fibrosis progression in chronic hepatitis C. J Hepatol. 2015;62(1):18–23. doi:10.1016/j.jhep.2014.08.013
28. Meurer L, Cohen SM. Drug-Induced Liver Injury from Statins. Clin Liver Dis. 2020;24(1):107–119. doi:10.1016/j.cld.2019.09.007
29. Francis P, Forman L. Use of statins in patients with and without liver disease. Clin Liver Dis. 2020;15(1):40–45. doi:10.1002/cld.866
30. Cohen DE, Anania FA, Chalasani N. An assessment of statin safety by hepatologists. Am J Cardiol. 2006;97(8):S77–S81. doi:10.1016/j.amjcard.2005.12.014
31. Khoo S, Wong VW-S, Goh G-B-B, et al. Suboptimal treatment of dyslipidemia in patients with nonalcoholic fatty liver disease. J Gastroenterol Hepatol. 2020;35(2):320–325. doi:10.1111/jgh.14794
32. Del Ben M, Baratta F, Polimeni L, et al. Under-prescription of statins in patients with non-alcoholic fatty liver disease. Nutr Metab Cardiovasc Dis. 2017;27(2):161–167. doi:10.1016/j.numecd.2016.09.011
33. van den Berg EH, Wolters AAB, Dullaart RPF, et al. Prescription of statins in suspected non-alcoholic fatty liver disease and high cardiovascular risk, a population-based study. Liver Int off J Int Assoc Study Liver. 2019;39(7):1343–1354. doi:10.1111/liv.14116
34. Jose J. Statins and its hepatic effects: newer data, implications, and changing recommendations. J Pharm Bioallied Sci. 2016;8(1):23–28. doi:10.4103/0975-7406.171699
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.