")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Sputum Biomarkers in Wood and Tobacco Smoke Etiotypes of Chronic Obstructive Pulmonary Disease
Authors Giraldo-Montoya ÁM, Torres-Duque CA , Giraldo-Cadavid LF, Laucho-Contreras ME, González-Flórez A, Santos AM, Tuta-Quintero EA, Celli BR, González-García M
Received 7 September 2023
Accepted for publication 19 December 2023
Published 30 December 2023 Volume 2024:19 Pages 1—10
DOI https://doi.org/10.2147/COPD.S439064
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Min Zhang
Ángela María Giraldo-Montoya,1,2,* Carlos A Torres-Duque,1,3,* Luis F Giraldo-Cadavid,4,5 Maria E Laucho-Contreras,1 Angélica González-Flórez,1 Ana María Santos,3 Eduardo A Tuta-Quintero,1,5 Bartolomé R Celli,6 Mauricio González-García1,7
1CINEUMO, Research Center, Fundación Neumológica Colombiana, Bogotá, Colombia; 2School of Medicine, Universidad Tecnológica de Pereira, Pereira, Colombia; 3Biosciences Doctoral, Universidad de La Sabana, Chía, Colombia; 4Medical Department, Fundación Neumológica Colombiana, Bogotá, Colombia; 5Epidemiology and Biostatistics Department, Universidad de La Sabana, Chía, Colombia; 6Harvard Medical School, Boston, MA, USA; 7School of Medicine, Universidad de La Sabana, Chía, Colombia
*These authors contributed equally to this work
Correspondence: Carlos A Torres-Duque, Research Department, Fundación Neumológica Colombiana, Bogotá, Colombia, Biosciences Doctoral, Universidad de La Sabana, Chía, Colombia, Email [email protected]
Introduction: There is a need to better understand the etiotypes of chronic obstructive pulmonary disease (COPD) beyond the tobacco-smoke (TS-COPD). Wood smoke COPD (WS-COPD) is characterized by greater airway compromise, milder emphysema, and slower rate of lung function decline than TS-COPD. However, it is unclear if these two etiotypes of COPD have differences in sputum biomarker concentrations. Objective was to compare sputum levels of selected sputum biomarkers between WS-COPD and TS-COPD, and healthy controls.
Methods: Eighty-eight women (69± 12 years) were recruited and classified into: WS-COPD (n=31), TS-COPD (n=29) and controls (n=28). Using ELISA, we determined induced sputum levels of metalloproteinase 9 (MMP-9), chemokine ligand 5 (CCL5), interleukin-8 (IL-8), chemokine ligand 16 (CCL16/HCC-4) and vascular endothelial growth factor (VEGF-1). Differences were analyzed by Kruskal–Wallis and Mann–Whitney-U tests and correlation between airflow limitation and biomarkers by Spearman’s test.
Results: At similar degree of airflow obstruction, anthropometrics and medications use, the level of sputum CCL5 was higher in TS-COPD than WS-COPD (p=0.03) without differences in MMP-9, IL-8, CCL16/HCC-4, and VEGF-1. Women with WS-COPD and TS-COPD showed significantly higher sputum levels of MMP-9, IL-8 and CCL5 compared with controls (p< 0.001). FEV1% predicted correlated negatively with levels of MMP-9 (rho:-0.26; P=0.016), CCL5 (rho:-0.37; P=0.001), IL-8 (rho:-0.42; P< 0.001) and VEGF (rho:-0.22; P=0.04).
Conclusion: While sputum concentrations of MMP-9, IL-8, and CCL5 were higher in COPD women compared with controls, women with TS-COPD had higher levels of CCL5 compared with those with WS-COPD. Whether this finding relates to differences in pathobiological pathways remains to be determined.
Keywords: COPD, wood smoke, biomass fuels, tobacco smoke, biomarkers, sputum, cytokines
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous and complex disease with multiple clinical presentations or phenotypes and remains a highly prevalent condition, causing significant morbidity and mortality worldwide.1,2 The 2023 Report of the Global Strategy for Prevention, Diagnosis and Management of Chronic Obstructive Pulmonary Disease (GOLD) and other recent publications have highlighted the relevance of risk factors different from tobacco smoke (TS) and the need for a better characterization and understanding of these causative types (etiotypes) of COPD.2–4 These publications underline several different causes of COPD including chronic exposure to smoke from biomass fuels (indoor use of materials of plant or animal origin), alterations in lung development, epigenetics, and occupational exposure to organic and inorganic substances (etiotypes).2–4
Of special relevance is that indoor air pollution derived from burning biomass fuels, very often wood, has been clearly related to airflow obstruction and COPD in women in developing countries such as Colombia.5–7 The PREPOCOL Study (Prevalence of COPD in Colombia) showed that 61% of the population had used wood as fuel for cooking and that the exposure to wood smoke for more than ten years was an independent risk factor for developing COPD.8 An increasing number of studies have described the clinical characteristics of COPD related to wood smoke (WS-COPD) and have shown some significant differences of this condition compared with TS-COPD.9–11 Notably, compared with TS-COPD, WS-COPD occurs more frequently in women, affecting primarily the airways with relatively mild or no emphysema.9,10,12–17 One of the plausible explanations for the differences between WS-COPD and TS-COPD may be that individuals have different patterns of exposure and/or different pathophysiological mechanisms and inflammatory responses to exposure to wood (biomass) and tobacco smoke.7
There is a growing information about the pathogenic mechanisms in COPD due to biomass smoke exposure.17,18 Some studies have focused on differences in the type of inflammation and the proteolytic activity and have suggested that biomass COPD is associated with a predominant Th2 cell profile and eosinophilic responses,19,20 while TS-COPD shows a predominantly Th17 cells responses.19 However, there is paucity of studies evaluating the biomarker profile of patients with either COPD etiotype that can help clarify the potential mechanisms responsible for the clinical differences.
Some cytokines have been related to the development or protection of emphysema and others mainly to airway inflammation.21–24 The matrix metalloproteinase 9 (MMP-9),25 the chemokine ligand 5 (CCL5),26 the vascular endothelial growth factor (VEGF-1),27 the interleukin 8 (IL-8)28 and the chemokine ligand 16/hemofiltrate CC chemokine 4 (CCL16/HCC-4)22,23 are among the studied cytokines in TS-COPD. These studies suggest that patients with TS-COPD, in whom emphysema predominates, would have higher concentrations of MMP-925 and CCL5,26 and lower concentrations of VEGF-1,27 while patients with WS-COPD, in which airway inflammation predominates, could have higher levels of IL-8 and other cytokines.14,17,29,30
A better characterization of the potential pathobiological mechanisms involved in the genesis of WS-COPD is necessary, not only because 40% of the world population (2.8 billion persons), continue using solid fuels (wood, charcoal, dung or other biomass materials) as their habitual household energy source,31,32 but also because the treatment of biomass-related and WS-COPD could be different and its prevention could imply alternative approaches from that of TS-COPD.
We hypothesized that induced sputum cytokines (as a measure of specific local inflammatory response) could provide information regarding the nature of the differences in the clinical expression of both etiotypes of COPD. To test this hypothesis, we determined the induced sputum levels of MMP-9, VEGF-1, CCL5, IL-8 and CCL16/HCC-4 in women with WS-COPD, TS-COPD, and healthy controls, and then related these levels to the degree of airflow limitation to test their biological plausibility.
Methods
Design and Participants
This is an analytical cross-sectional study comparing the local inflammatory response as expressed by biomarkers measured in the induced sputum in women with WS-COPD, TS-COPD and in healthy subjects. The study was performed in a tertiary health care institution dedicated to respiratory health in Bogotá, Colombia, complies with the Declaration of Helsinki, and was approved by the Institutional Review Board. All participants completed written informed consent.
The COPD participants were prospectively and consecutively recruited according to the following inclusion criteria: women older than 40 years, diagnosis of COPD confirmed by a post bronchodilator spirometry FEV1/FVC <0.70 and exposure to only wood smoke (WS-COPD) or only tobacco smoke (TS-COPD). Patients were considered as having WS-COPD if they had a history of exposure to wood smoke ≥10 years8 without tobacco smoke exposure (no current smoker and pack-year index [PYI] <1) or as having TS COPD if they had a history of exposure to tobacco smoke with a PYI ≥ 10 without wood smoke exposure. We excluded participants with a medical history of pulmonary diseases other than COPD as documented in their medical records (such as asthma, interstitial disease, pulmonary hypertension, bronchiectasis, etc.), pharmacological immunosuppression, simultaneous exposure to wood and tobacco smoke, contraindications, or inability to produce induced sputum or spirometry. They could not have a respiratory infection or exacerbation during the eight weeks prior to the sample collection. The control group consisted of healthy women older than 40 years who did not have any respiratory symptoms or disease, had no exposure to wood or tobacco smoke and had normal spirometry.
Procedures
Clinical Evaluation, Questionnaire, and Spirometry
All patients received a standardized clinical evaluation by a pulmonologist, including the ATS-DLD-78 standard respiratory questionnaire,33 adapted for wood smoke exposure,8 a complete physical examination, pre and post bronchodilator spirometry and chest-x-ray. Spirometry was performed and interpreted according to the American Thoracic Society (ATS)/European Respiratory Society (ERS) standards.34
Sputum Induction and Processing
The sputum was induced in all participants following existing protocols.35 All subjects received four inhalations of albuterol 100 μg, subsequently they were nebulized with 5% hypertonic saline solution. The biological material was undergone to filtration and centrifugation to remove any contaminating particles. A fluidizing solution was added, passed through a 48 micron filter, to avoid the presence of sediment, and the filtrate was collected in an Eppendorf tube, allowed to stand for 5 minutes, then cytocentrifuged at 750 g (3000 rpm for 4 minutes) and stored in cryovials at a temperature of −80 ° C.36
Biomarkers Measurement
The cytokines and chemokines were selected based on previous studies and their potential role in COPD pathogenesis. MMP-9, IL-8, VEGF-1, CCL16/HCC-4 and CCL5 were chosen because they have been widely studied in COPD, and some related to poor prognosis and development of emphysema (MMP-9 and CCL5). The enzyme-linked immunosorbent assay (ELISA) technique was performed for each biomarker in a total of 440 tests for the 88 patients and 40 tests for the technique standardization. The samples were processed using Abcam human ELISA Kits in vitro (Cambridge, MA, USA). This assay employs an antibody specific for different molecules, in this case MMP-9 (ab 100610), IL-8 (ab 214030), VEGF-1 (ab 222510), CCL5 (ab 174446) and CCL16/HCC-4 (ab100532), which were measured simultaneously according to manufacturer’s recommendations. Concentrations were determined by spectrophotometry iMark Microplate absorbance reader-1681135 (Biorad, Hercules, California, USA), for reading at 450 nm.37
Statistical Analysis
The quantitative variables were described as average ± standard deviation (SD) or as median and interquartile range (IQR), depending on their normal or abnormal distribution, respectively. We used the Shapiro–Wilk test to determine if the variables had normal distribution. The qualitative variables were described by means of absolute frequencies and proportions. We performed a comparison of clinical qualitative variables among the subject groups using the Fisher´s exact test (recommended for small sample sizes, as it calculates the exact probability of the observed data under the null hypothesis).
The comparison of the cytokine levels among the different groups was performed by the Kruskal Wallis test, with a maximum of two post hoc analyzes using the Mann Whitney U-test, because the distribution of the variables was asymmetric. We assessed the correlation between clinical quantitative variables and cytokine levels using the Spearman rho correlation coefficient. We selected this test due to the asymmetric distribution of the data.
Using information gleaned from prior publications on TS-COPD and WS-COPD,38–40 we estimated the sample size by assessing potential mean differences ranging between 1.0 and 1.6 for MMP-9, IL-8, VEGF, and CCL5 when comparing TS-COPD with healthy controls. Assuming that the differences between TS-COPD and WS-COPD would be smaller, we calculated a standardized effect size of 0.75 with a confidence level of 95% and a power of 80%. This computation yielded a minimum sample size requirement of 90 subjects, comprising 30 individuals for each COPD group, and 30 controls.
We employed Robust Regression analysis to evaluate differences in biomarker levels between individuals with WS-COPD and TS-COPD, while adjusting for potential confounding factors. The selection of potential confounders for inclusion in the saturated model was based on biological plausibility and guided by directed acyclic graphs (DAGs). Variables identified in the DAGs as potentially linked to both the exposure and the outcome, without serving as mediators or collider variables, were incorporated into the saturated model. Subsequently, a final parsimonious model was derived by iteratively excluding variables from the saturated model that exhibited no statistically significant association with the outcome, and whose exclusion did not significantly impact the R2 or coefficients of the model.
Statistical significance was set at a P <0.05 at to two tails, except in the post-hoc analyzes, in which the Bonferroni correction was applied and a P value of less than 0.025 was required (a maximum of two post hoc analyses were made by family of tests). The Bootstrap method was used to increase the precision in the estimation of confidence intervals. The data were analyzed in the statistical package Stata version 16 (Stata Corp LLC, College Station, TX, US).
Results
Population Characteristics
A total of 88 women were included, 31 in the WS-COPD group, 29 in the TS-COPD group and 28 in the control group (Figure E1). Table 1 shows that patients with WS-COPD were slightly older, shorter and had a lower airflow limitation than those with TS-COPD without other significant differences, including the macroscopic features and weight of sputum (Table 1). Per definition, the control group had not airflow obstruction.
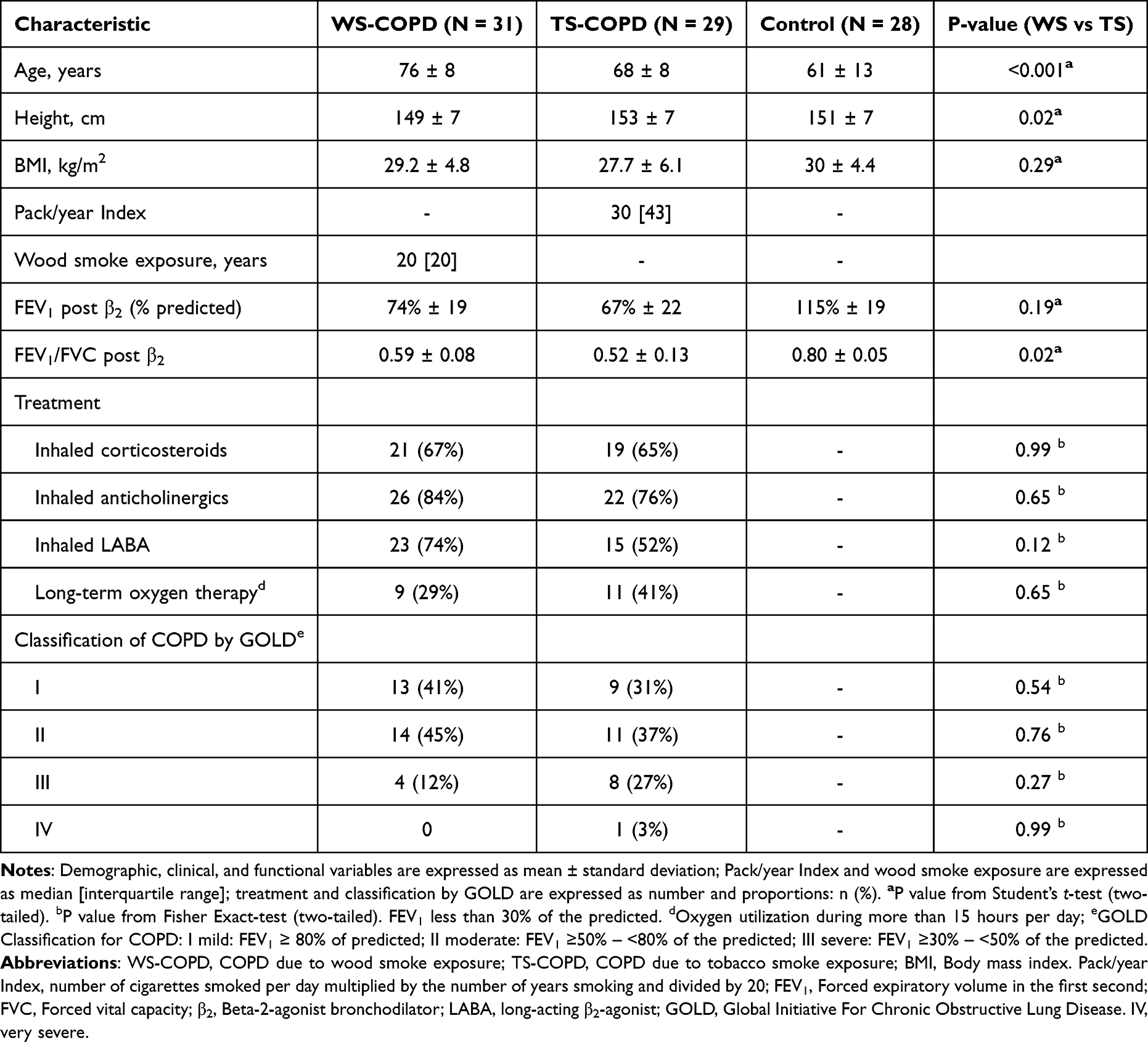 |
Table 1 Demographic and Clinical Characteristics of the Women Participating in the Study |
Inflammatory Profile in COPD Patients and Differences Between Groups
The cytokine and chemokine levels in Table 2 show that compared to controls, the WS-COPD and TS-COPD had higher levels of MMP-9 (P=0.004), CCL5 (P=0.002) and IL-8 (P<0.001), while no significant differences were found for VEGF-1 and CCL16/HCC-4 (P = 0.22 and 0.27, respectively) (Figure 1) (Table E1). After the Robust Regression analysis, among COPD groups, CCL5 was higher in TS-COPD compared with WS-COPD (P=0.03) (Table 2, Figure 1). Table E2 shows the comparison of biomarker levels between patients with TS-COPD and WS-COPD.
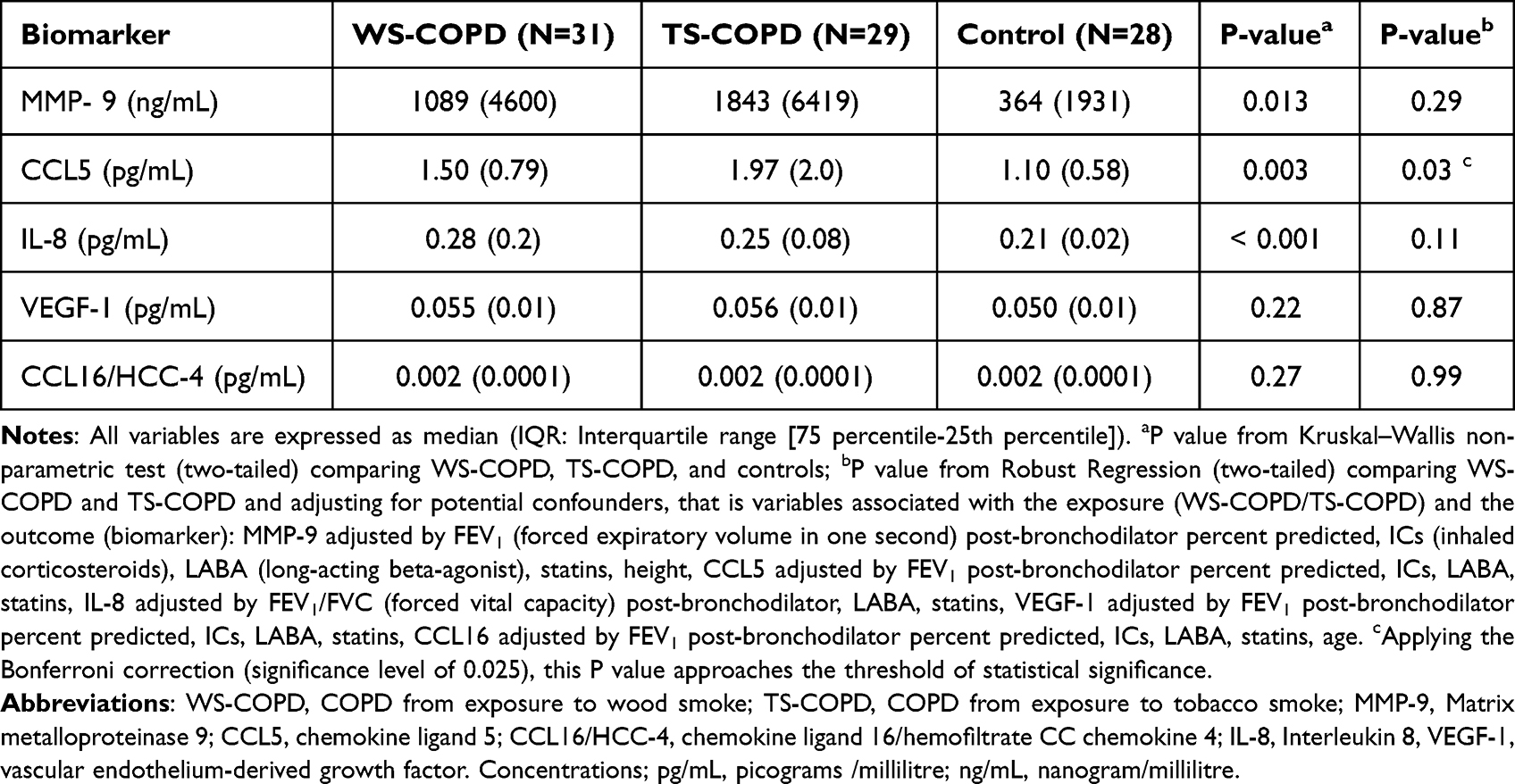 |
Table 2 Concentration of Biomarkers in Women with COPD from Wood Smoke (WS), Tobacco Smoke (TS) and Healthy Controls |
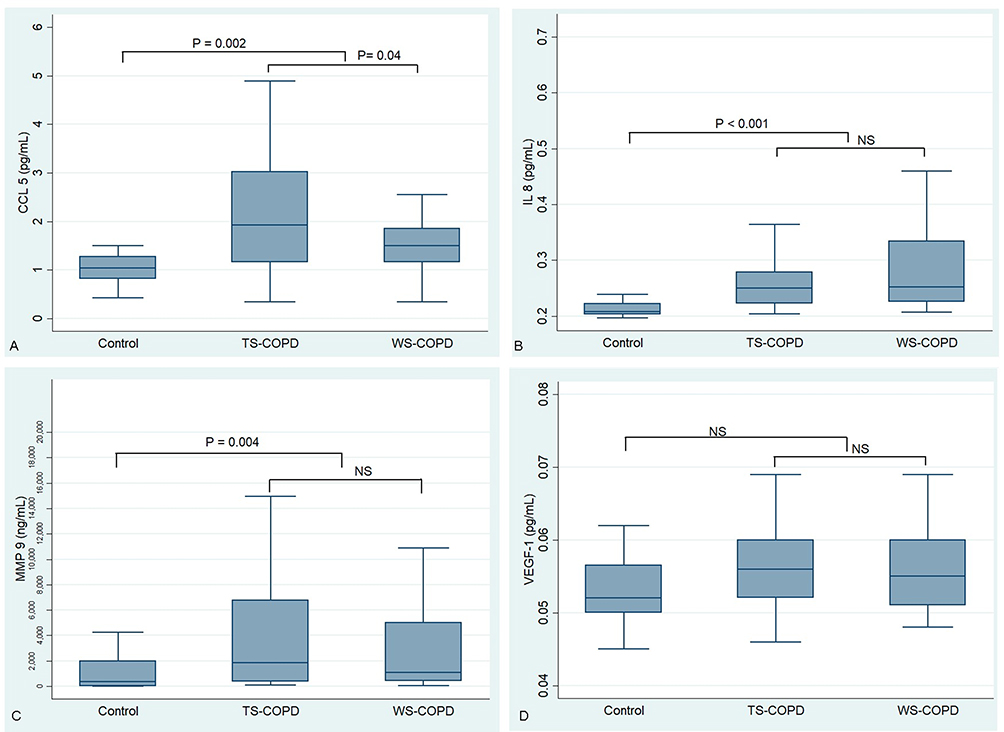 |
Figure 1 Cytokine levels by Group. (A) CCL5; (B) IL-8; (C) MMP-9; (D) VEGF-1. Abbreviations: TS-COPD, COPD from exposure to tobacco smoke; WS-COPD, COPD from exposure to wood smoke; MMP-9, matrix metalloproteinase 9; CCL5, chemokine ligand 5; IL-8, Interleukin 8, VEGF-1, vascular endothelium-derived growth factor-1; pg/mL, picograms/millilitre, ng/mL: nanogram/millilitre. Notes: P values using two-tailed Mann–Whitney U-Test, exact method. For comparison of WS-COPD and TS-COPD, we used de Bonferroni correction. |
Correlations Between Airflow Obstruction and Biomarkers
There was monotonic inverse correlation between the degree of obstruction in COPD and the levels of MMP-9, CCL5, IL-8 and VEGF-1, but not for CCL16/HCC-4 (Table 3). We observed a positive correlation between age and MMP-9 levels (Spearman rho: 0.24; P = 0.025). However, there was no correlation between cytokine levels and other clinical quantitative variables (Table E3).
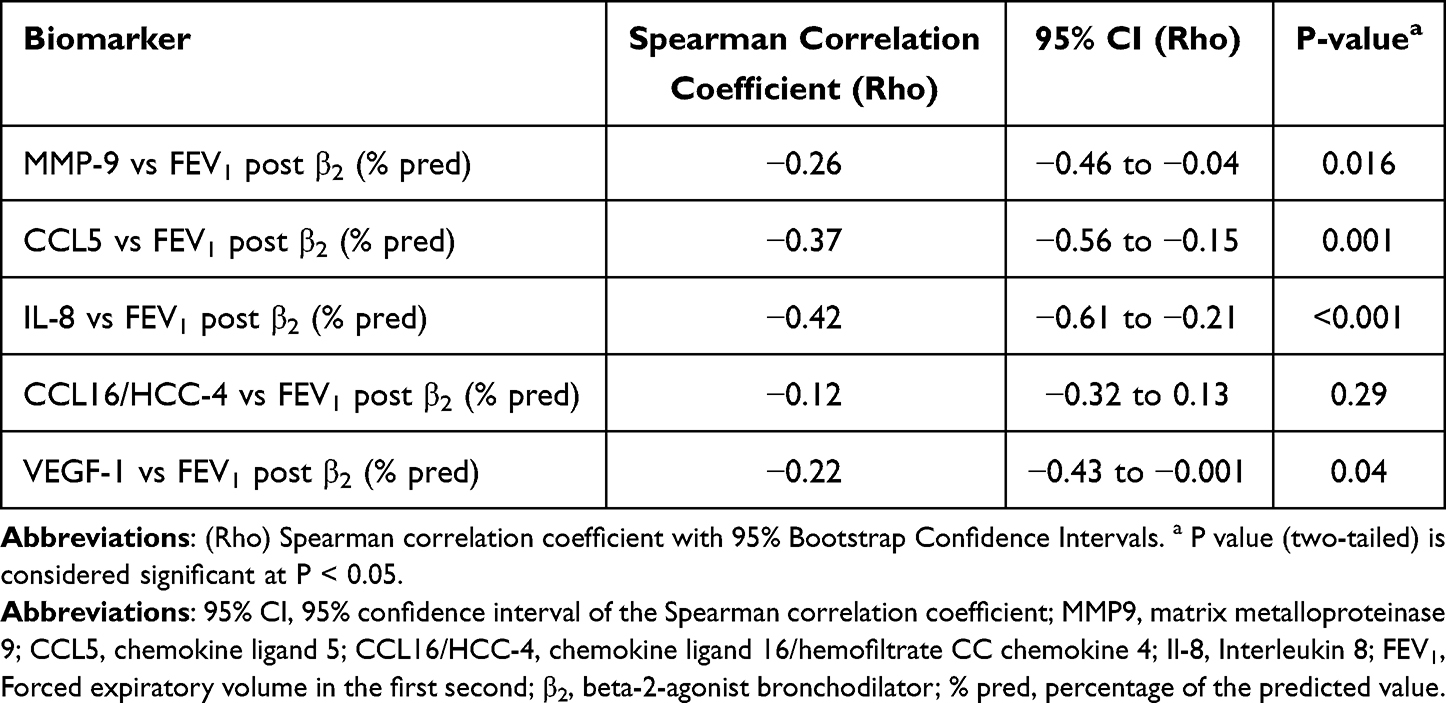 |
Table 3 Correlation Between the Levels of Biomarkers and the Degree of Airflow Obstruction |
Discussion
This study focused on selected sputum biomarkers in women with COPD caused by the exposure to two different risk factors (wood and tobacco smoke), had several novel findings. First, TS-COPD patients have higher sputum levels of CCL5 than women with WS-COPD, a previously unreported observation with potential pathobiological significance. Second, there was a monotonic inverse correlation between the level of sputum biomarkers in COPD patients and the degree of airflow obstruction, suggesting a biological plausibility to our findings. Third, women with COPD, whether caused by tobacco smoke or wood smoke exposure, have higher levels of the inflammatory markers IL-8, MMP-9 and CCL5 than healthy controls, supporting a common generic role of these cytokines in the genesis of these two etiotypes of COPD.
Different from TS-COPD, WS-COPD is consistently characterized by the presence of mild or total absence of emphysema.9,10,12,15,41 Our finding of a higher sputum level of CCL5 in TS-COPD than in WS-COPD could be related to the different expression of emphysema in these two subtypes of COPD, which is supported by previous studies. The CCL5 is a chemokine that attracts neutrophils and eosinophils and that has been thought to be involved in the pathogenesis of TS-COPD.26,42–44 In comparison with subjects without COPD, Di Stefano et al found that the numbers of CCL5+ cells in the submucosa of patients with stable TS-COPD were 2 to 15 times higher than any other chemokines and also an increased expression of extracellular matrix-binding receptors on neutrophils.26 Similarly, Costa et al showed that CCL5 was increased in sputum from TS-COPD patients compared with nonsmokers45 while Grumelli et al found a high percentage of CD4+ and CD8+ T lymphocytes that expressed CCR5 (the receptor for CCL5), a marker of T helper 1 cells, in patients with TS-COPD that were currently smoking vs ex-smokers.43 Interestingly, polymorphisms of CCL5 gene have been associated with the emphysema expression, with 28G allele genotype inversely associated with computed tomography score of emphysema.42 In addition, Kratzer et al found an increase of CCL5 in a rat model of second-hand smoke-induced emphysema.44 These observations are consistent with the higher sputum level of CCL5 in TS-COPD than in WS-COPD found in our study and could help explain the difference in the high degree of emphysema present in patients with TS-COPD and the low levels of emphysema observed in patients with WS-COPD. Our findings differ from those of Falfan-Valencia et al who compared healthy women exposed to TS or WS and found that the serum CCL5 levels were higher in the individuals exposed to WS exposed vs TS exposed.46 However, this study, which did not include COPD patients, measured the CCL5 in serum and not in sputum and the local and systemic responses could differ in the same individuals.47
We did not find differences between WS-COPD and TS-COPD in the other tested cytokines: IL-8, MMP-9, CCL16/HCC-4 and VEGF. However, both groups had higher levels of the assessed biomarkers than non-COPD control group. The increased levels of cytokines have been consistently observed in patients with stable TS or WS COPD compared to control groups,13,14 but the described inflammatory profiles have exhibited wide heterogeneity, varying according to the population studied and the method used. The increased levels of IL-8 observed in the induced sputum48 of COPD patients could be related to the increased Th1 and Th17 responses described as part of the COPD pathogenesis. MMP-9 is a gelatinase that promotes neutrophil chemotaxis and mediate inflammation, contributing to the development of emphysema; multiple studies had shown an inverse correlation between MMP-9 and FEV1.49 In line with these previous findings, the present study confirms the presence of persistent lung inflammation with higher levels of most of the measured biomarkers in COPD, both in the WS or TS exposure.
One study showed that the sputum levels of VEGF-1 were linked to the chronic bronchitis or emphysema phenotype of TS-COPD (high in chronic bronchitis and low in emphysema)50 and other one that its serum levels were higher in the group with COPD compared with the controls, but without differences between biomass COPD and TS-COPD.46 In our study, there was a trend towards increased sputum levels of VEFG-1 in the COPD group (Table E1) in comparison with the control group without differences between the COPD groups exposed to biomass or tobacco. Although CCL16/HCC-4 levels have been described as being high in COPD,22 we did not find elevated levels of this cytokine in patients with COPD compared to the controls, nor differences between WS-COPD and TS-COPD.
A second important finding of our study is that of a monotonic inverse correlation between the level of sputum biomarkers in COPD patients and the degree of airflow obstruction. Moreover, when we compared the obstruction severity with the levels of CCL5, we observed a moderate, but significant, negative correlation between the FEV1 and the CCL5 levels (Table 3), corroborating that CCL5, at least in part, could mediate a deleterious response on the natural history in COPD patients.26 We also found an inverse correlation between the levels of MMP-9, IL-8, VEGF-1 and FEV1%. This relationship suggests a potential etiological role of the cytokine itself or of the mechanisms responsible for the cytokine generation and its relationship with chronic airflow obstruction. Previous studies have described that the levels of TNF-α, IL-1β and IL-6 are directly proportional to the post-bronchodilator FEV1%.51 A recent study focused on biomarker-based clustering of patients with COPD showed that the degree of airflow limitation was comparable between clusters, indicating a limited value of relating airflow limitation in predicting systemic levels of the biomarkers and vice versa.52
Our third finding was that women with COPD, whether caused by tobacco smoke or wood smoke exposure, had higher levels of IL-8, MMP-9 and CCL5 in sputum than healthy controls, confirming previous observations that have documented similar results and indicating the activation of inflammatory and lung damage mechanisms in COPD.21,22,30,40
Our study has several strengths. First, its prospective inclusion of strictly selected women with stable COPD and healthy controls, thus eliminating the usual gender bias, the clear classification of the two types of causes and the selection of representative inflammatory, lung damage and vascular compromise biomarkers. However, there were also some limitations. First, the study was cross-sectional, reflecting a moment in a patient history, thereby not allowing the establishment of temporal relationships or causal assumptions. Second, we had a relatively small sample size, which does not permit to completely exclude a role in COPD pathogenesis for those cytokines that showed a trend but did not reach the level of statistical significance. Finally, although only a small selected group of biomarkers were tested, they represent some of the best studied biomarkers that have shown some relationship to COPD.
In conclusion, we found higher levels of CCL5 in the sputum of women with TS-COPD than in WS-COPD. This finding could be relevant to explain differences in the pathophysiological pathways in these two etiotypes of COPD, particularly in relation with the higher frequency of emphysema in TS-COPD compared to WS-COPD. We also found an elevation of the sputum levels of CCL5, MPP-9 and IL-8 in women with either tobacco or wood smoke-related COPD compared to a healthy control group. In addition, we describe an inverse correlation between the level of sputum biomarkers in COPD patients and the degree of airflow obstruction. More studies are required to clarify the role of such cytokines to explain the similarities and differences between TS-COPD and WS-COPD.
Data Sharing Statement
The datasets generated and/or analysed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Review Committee of the Universidad de La Sabana School of (Proceedings 337-2015) and Fundación Neumológica Colombiana (Approval number 201505-21008).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was founded by Universidad de La Sabana (Grant: MED-202-2015).
Disclosure
Dr Luis F Giraldo-Cadavid reports grants from Universidad de La Sabana, during the conduct of the study.
Dr Maria E Laucho-Contreras is an Employee & Shareholder of GSK, outside the submitted work. All other authors declare that they have no competing interests in this work.
References
1. Soriano JB, Abajobir AA, Abate KH, et al. GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5:691–706.
2. GOLD. Global Strategy for Prevention, Diagnosis and Management of COPD: 2023 Report; 2023. Available from: https://goldcopd.org/2023-gold-report-2/.
3. Stolz D, Mkorombindo T, Schumann DM, et al. Towards the elimination of chronic obstructive pulmonary disease: a Lancet Commission. Lancet. 2022;400:921–972. doi:10.1016/S0140-6736(22)01273-9
4. Celli B, Fabbri L, Criner G, et al. Definition and nomenclature of chronic obstructive pulmonary disease: time for its revision. Am J Respir Crit Care Med. 2022;206(11):1317–1325. doi:10.1164/rccm.202204-0671PP
5. Pathak U, Gupta NC, Suri JC. Risk of COPD due to indoor air pollution from biomass cooking fuel: a systematic review and meta-analysis. Int J Environ Health Res. 2020;30(1):75–88. doi:10.1080/09603123.2019.1575951
6. Sana A, Somda SMA, Meda N, Bouland C. Chronic obstructive pulmonary disease associated with biomass fuel use in women: a systematic review and meta-analysis. BMJ Open Respir Res. 2018;5:e000246. doi:10.1136/bmjresp-2017-000246
7. Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-smokers. Lancet. 2009;374(9691):733–743. doi:10.1016/S0140-6736(09)61303-9
8. Caballero A, Torres-Duque CA, Jaramillo C, et al. Prevalence of COPD in five Colombian cities situated at low, medium, and high altitude (PREPOCOL study). Chest. 2008;133:343–349. doi:10.1378/chest.07-1361
9. Perez-Padilla R, Ramirez-Venegas A, Sansores-Martinez R. Clinical Characteristics of Patients With Biomass Smoke-Associated COPD and Chronic Bronchitis, 2004-2014. Chronic Obstructive Pulmonary Dis. 2014;1:23–32. doi:10.15326/jcopdf.1.1.2013.0004
10. Torres-Duque CA, Garcia-Rodriguez MC, Gonzalez-Garcia M. Is Chronic Obstructive Pulmonary Disease Caused by Wood Smoke a Different Phenotype or a Different Entity? Arch Bronconeumol. 2016;52(8):425–431. doi:10.1016/j.arbr.2016.06.026
11. Assad NA, Balmes J, Mehta S, Cheema U, Sood A. Chronic obstructive pulmonary disease secondary to household air pollution. Semin Respir Crit Care Med. 2015;36(03):408–421. doi:10.1055/s-0035-1554846
12. González-García M, Maldonado-Gomez D, Torres-Duque CA, et al. Tomographic and functional findings in severe COPD: comparison between the wood smoke-related and smoking-related disease. J Bras Pneumol. 2013;39(2):147–154. doi:10.1590/S1806-37132013000200005
13. Olloquequi J, Jaime S, Parra V, et al. Comparative analysis of COPD associated with tobacco smoking, biomass smoke exposure or both. Respir Res. 2018;19(1):13. doi:10.1186/s12931-018-0718-y
14. Golpe R, Martín-Robles I, Sanjuán-López P, et al. Differences in systemic inflammation between cigarette and biomass smoke-induced COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2639–2646. doi:10.2147/COPD.S141068
15. Camp PG, Ramirez-Venegas A, Sansores RH, et al. COPD phenotypes in biomass smoke- versus tobacco smoke-exposed Mexican women. Eur Respir J. 2014;43(3):725–734. doi:10.1183/09031936.00206112
16. Gonzalez-Garcia M, Torres-Duque CA, Bustos A, Jaramillo C, Maldonado D. Bronchial hyperresponsiveness in women with chronic obstructive pulmonary disease related to wood smoke. Int J Chron Obstruct Pulmon Dis. 2012;7:367–373. doi:10.2147/COPD.S30410
17. Ortiz-Quintero B, Martínez-Espinosa I, Pérez-Padilla R. Mechanisms of Lung Damage and Development of COPD Due to Household Biomass-Smoke Exposure: inflammation, Oxidative Stress, MicroRNAs, and Gene Polymorphisms. Cells. 2022;12(1):12. doi:10.3390/cells12010012
18. Silva R, Oyarzún M, Olloquequi J. Pathogenic mechanisms in chronic obstructive pulmonary disease due to biomass smoke exposure. Arch Bronconeumol. 2015;51:285–292. doi:10.1016/j.arbr.2015.04.013
19. Solleiro-Villavicencio H, Quintana-Carrillo R, Falfán-Valencia R, Vargas-Rojas MI. Chronic obstructive pulmonary disease induced by exposure to biomass smoke is associated with a Th2 cytokine production profile. Clin Immunol. 2015;161:150–155. doi:10.1016/j.clim.2015.07.009
20. Fernandes L, Rane S, Mandrekar S, Mesquita AM. Eosinophilic Airway Inflammation in Patients with Stable Biomass Smoke- versus Tobacco Smoke-Associated Chronic Obstructive Pulmonary Disease. J Health Pollut. 2019;9(24):191209. doi:10.5696/2156-9614-9.24.191209
21. Stockley RA, Halpin DMG, Celli BR, Singh D. Chronic Obstructive Pulmonary Disease Biomarkers and Their Interpretation. Am J Respir Crit Care Med. 2019;199:1195–1204. doi:10.1164/rccm.201810-1860SO
22. Pinto-Plata V, Toso J, Lee K, et al. Profiling serum biomarkers in patients with COPD: associations with clinical parameters. Thorax. 2007;62:595–601. doi:10.1136/thx.2006.064428
23. Laucho-Contreras ME, Polverino F, Gupta K, et al. Protective role for club cell secretory protein-16 (CC16) in the development of COPD. Eur Respir J. 2015;45(6):1544–1556. doi:10.1183/09031936.00134214
24. Rojas-Quintero J, Laucho-Contreras ME, Wang X, et al. CC16 augmentation reduces exaggerated COPD-like disease in Cc16-deficient mice. JCI Insight. 2023;8.
25. Vernooy JH, Lindeman JH, Jacobs JA, Hanemaaijer R, Wouters EF. Increased activity of matrix metalloproteinase-8 and matrix metalloproteinase-9 in induced sputum from patients with COPD. Chest. 2004;126:1802–1810. doi:10.1378/chest.126.6.1802
26. Di Stefano A, Caramori G, Gnemmi I, et al. Association of increased CCL5 and CXCL7 chemokine expression with neutrophil activation in severe stable COPD. Thorax. 2009;64(11):968–975. doi:10.1136/thx.2009.113647
27. Kanazawa H, Yoshikawa J. Elevated oxidative stress and reciprocal reduction of vascular endothelial growth factor levels with severity of COPD. Chest. 2005;128(5):3191–3197. doi:10.1378/chest.128.5.3191
28. Zhang X, Zheng H, Zhang H, et al. Increased interleukin (IL)-8 and decreased IL-17 production in chronic obstructive pulmonary disease (COPD) provoked by cigarette smoke. Cytokine. 2011;56(3):717–725. doi:10.1016/j.cyto.2011.09.010
29. Barregard L, Sallsten G, Andersson L, et al. Experimental exposure to wood smoke: effects on airway inflammation and oxidative stress. Occup Environ Med. 2008;65:319–324. doi:10.1136/oem.2006.032458
30. Vishweswaraiah S, Thimraj TA, George L, et al. Putative Systemic Biomarkers of Biomass Smoke-Induced Chronic Obstructive Pulmonary Disease among Women in a Rural South Indian Population. Dis Markers. 2018;2018:4949175. doi:10.1155/2018/4949175
31. Bonjour S, Adair-Rohani H, Wolf J, et al. Solid fuel use for household cooking: country and regional estimates for 1980-2010. Environ Health Perspect. 2013;121:784–790. doi:10.1289/ehp.1205987
32. World Health Organization. World Health Statistics 2015. Risk Factors; 2015. Available from: http://www.who.int/gho/publications/world_health_statistics/EN_WHS2015_Part2.pdf?ua=1.
33. Ferris BG. Epidemiology Standardization Project (American Thoracic Society). Am Rev Respir Dis. 1978;118:1–120.
34. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST
35. Efthimiadis A, Spanevello A, Hamid Q, et al. Methods of sputum processing for cell counts, immunocytochemistry and in situ hybridisation. Eur Respir j. 2002;37:19s–23s. doi:10.1183/09031936.02.00001902
36. Voynow JA, Rubin BK. Mucins, mucus, and sputum. Chest. 2009;135(2):505–512. doi:10.1378/chest.08-0412
37. Balsam J, Ossandon M, Bruck HA, Lubensky I, Rasooly A. Low-cost technologies for medical diagnostics in low-resource settings. Expert Opin Med Diagn. 2013;7(3):243–255. doi:10.1517/17530059.2013.767796
38. Frankenberger M, Eder C, Hofer TP, et al. Chemokine expression by small sputum macrophages in COPD. Mol Med. 2011;17:762–770. doi:10.2119/molmed.2010.00202
39. Aviles B, Belda J, Margarit G, Bellido-Casado J, Martinez-Bru C, Casan P. Markers of airway remodeling in induced sputum from healthy smokers. Archi de bronconeumologia. 2006;42:235–240. doi:10.1016/S1579-2129(06)60452-7
40. Aaron SD, Vandemheen KL, Ramsay T, et al. Multi analyte profiling and variability of inflammatory markers in blood and induced sputum in patients with stable COPD. Respir Res. 2010;11(1):41. doi:10.1186/1465-9921-11-41
41. Meneghini AC, Koenigkam-Santos M, Pereira MC, et al. Biomass smoke COPD has less tomographic abnormalities but worse hypoxemia compared with tobacco COPD. Braz J Med Biol Res. 2019;52(5):e8233. doi:10.1590/1414-431x20198233
42. Hizawa N, Makita H, Nasuhara Y, et al. Functional single nucleotide polymorphisms of the CCL5 gene and nonemphysematous phenotype in COPD patients. Eur Respir J. 2008;32(2):372–378. doi:10.1183/09031936.00115307
43. Grumelli S, Corry DB, Song LZ, et al. An immune basis for lung parenchymal destruction in chronic obstructive pulmonary disease and emphysema. PLoS Med. 2004;1:e8. doi:10.1371/journal.pmed.0010008
44. Kratzer A, Salys J, Nold-Petry C, et al. Role of IL-18 in second-hand smoke-induced emphysema. Am J Respir Cell Mol Biol. 2013;48:725–732. doi:10.1165/rcmb.2012-0173OC
45. Costa C, Rufino R, Traves SL, Lapa ESJR, Barnes PJ, Donnelly LE. CXCR3 and CCR5 chemokines in induced sputum from patients with COPD. Chest. 2008;133(1):26–33. doi:10.1378/chest.07-0393
46. Falfán-Valencia R, Ramírez-Venegas A, Pérez Lara-Albisua JL, et al. Smoke exposure from chronic biomass burning induces distinct accumulative systemic inflammatory cytokine alterations compared to tobacco smoking in healthy women. Cytokine. 2020;131:155089. doi:10.1016/j.cyto.2020.155089
47. Ji J, von Schéele I, Bergström J, et al. Compartment differences of inflammatory activity in chronic obstructive pulmonary disease. Respir Res. 2014;15(1):104. doi:10.1186/s12931-014-0104-3
48. Yamamoto C, Yoneda T, Yoshikawa M, et al. Airway inflammation in COPD assessed by sputum levels of interleukin-8. Chest. 1997;112:505–510. doi:10.1378/chest.112.2.505
49. Beeh KM, Beier J, Kornmann O, Buhl R. Sputum matrix metalloproteinase-9, tissue inhibitor of metalloprotinease-1, and their molar ratio in patients with chronic obstructive pulmonary disease, idiopathic pulmonary fibrosis and healthy subjects. Respir Med. 2003;97(6):634–639. doi:10.1053/rmed.2003.1493
50. Kanazawa H, Asai K, Hirata K, Yoshikawa J. Possible effects of vascular endothelial growth factor in the pathogenesis of chronic obstructive pulmonary disease. Am J Med. 2003;114(5):354–358. doi:10.1016/S0002-9343(02)01562-0
51. Singh S, Verma SK, Kumar S, et al. Correlation of severity of chronic obstructive pulmonary disease with potential biomarkers. Immunol Lett. 2018;196:1–10. doi:10.1016/j.imlet.2018.01.004
52. Vanfleteren LEGW, Weidner J, Franssen FME, et al. Biomarker-based clustering of patients with chronic obstructive pulmonary disease. ERJ Open Res. 2023;9:00301–02022. doi:10.1183/23120541.00301-2022
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.