")
Back to Journals » Cancer Management and Research » Volume 15
Spotlight on Cemiplimab-rwlc in the Treatment of Non-Small Cell Lung Cancer (NSCLC): Focus on Patient Selection and Considerations
Authors Ahn J, Nagasaka M
Received 9 April 2023
Accepted for publication 15 June 2023
Published 11 July 2023 Volume 2023:15 Pages 627—634
DOI https://doi.org/10.2147/CMAR.S325856
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Jeffrey Ahn,1 Misako Nagasaka1,2
1Department of Medicine, University of California Irvine School of Medicine, Chao Family Comprehensive Cancer Center, Orange, CA, USA; 2St. Marianna University School of Medicine, Kawasaki, Japan
Correspondence: Misako Nagasaka, Department of Medicine, University of California Irvine School of Medicine, Chao Family Comprehensive Cancer Center, 101 The City Drive South, Orange, CA, 92868, USA, Email [email protected]
Abstract: In metastatic non-small cell lung cancer (NSCLC), tumors that do not harbor driver mutations in EGFR or gene fusions in ALK and ROS, PD-1 and PD-L1 inhibitors have become a cornerstone in first line treatment, either as monotherapy or in combination with chemotherapy. This paper reviews cemiplimab-rwlc, the third PD-1/L1 inhibitor to be approved in the setting for first line treatment in NSCLC, as monotherapy or in combination therapy with chemotherapy, to provide a perspective on the subtle differences in patient population for the cemiplimab studies and consideration of its primary and subgroup results in the context of first line therapies for NSCLC.
Keywords: immunotherapy, monotherapy, combination chemotherapy, PD-L1
Since the first FDA approval of nivolumab for treating metastatic NSCLC in patients whose disease has progressed on platinum-containing chemotherapy in 2015, immune checkpoint blockade, particularly in the forms of anti-programmed cell death-1 (PD-1), programmed cell death ligand-1 (PD-L1) and anti-cytotoxic T-lymphocyte-associated protein-4 (CTLA4) antibodies, became an indispensable treatment options in the management of non-small cell lung cancer (NSCLC).1 Across various stages of NSCLC, immunotherapy has demonstrated its efficacy and become a major part of standard care. For instance, in February 2018, durvalumab, a human immunoglobulin G1 (IgG1) kappa monoclonal antibody against PD-L1, was approved by the FDA for patients with unresectable stage III NSCLC whose disease has not progressed following concurrent platinum-based chemotherapy and radiation, based on the PACIFIC trial, a randomized double-blind trial.2 In October 2022, atezolizumab, a humanized IgG1 monoclonal anti-PD-L1 antibody, was approved for adjuvant treatment following resection and platinum-based chemotherapy in patients with stage II to IIIA tumors with PD-L1 expression ≥1% on tumor cells, based on IMpower010, a randomized, open-label phase 3 trial.3 In March 2022, nivolumab, a fully human monoclonal IgG4 antibody against the PD-1 receptor, was approved by the FDA, in conjunction with platinum-doublet chemotherapy, for adults with resectable NSCLC in the neoadjuvant setting, based on the CHECKMATE-816 trial, which included histologically confirmed stage IB, II or IIIA tumors, regardless of the tumor PD-L1 status.4
In metastatic NSCLC tumors that do not harbor driver mutations in EGFR or gene fusions in ALK and ROS, immunotherapy has become a cornerstone in first line treatment, either as monotherapy or in combination with chemotherapy. Cemiplimab-rwlc, which is a highly potent, hinged, stabilized, human IgG4 monoclonal antibody directed against PD-1, is a newly FDA-approved immunotherapy option in treating metastatic NSCLC, either as monotherapy or in combination with chemotherapy, based on the EMPOWER-Lung 1 and EMPOWER-Lung 3 trials, respectively.
EMPOWER-Lung 1
In EMPOWER-Lung 1, a multicenter, open-label, global, phase 3 study, the efficacy of cemiplimab monotherapy compared to the investigator’s choice of platinum-doublet chemotherapy was evaluated in the first line treatment setting in adults with histologically or cytologically confirmed advanced NSCLC whose tumors express PD-L1 in at least 50% of tumor cells. Eligible patients were at least 18 years old, with an ECOG status of 0 or 1, had histologically or cytologically confirmed stage IIIB/IIIC cancer and were not candidates for definitive chemoradiotherapy, or stage IV squamous or non-squamous NSCLC with PD-L1 expression of ≥50% of tumor cells without EGFR mutations, ALK translocations or ROS1 fusions. Notable exclusion criteria included being a non-smoker (defined as ≤100 cigarettes in a lifetime), and having active or untreated brain metastases, uncontrolled hepatitis B/C or HIV infection or suspected autoimmune disease that required systemic treatment in the 2 years preceding enrollment. Those with controlled hepatitis B/C or HIV infection were eligible for the study. Eligible patients were randomly assigned to either cemiplimab monotherapy 350 mg every 3 weeks for up to 108 weeks or four to six cycles of the investigator’s choice of platinum-doublet chemotherapy, with the option of continuing maintenance pemetrexed afterwards. The primary endpoints included overall survival (OS) and progression-free survival (PFS), and secondary endpoints included the objective response rate (ORR), duration of response (DOR) and health-related quality of life (HRQoL). A total of 563 patients were randomly assigned and the overall median duration of follow-up was 10.8 months for cemiplimab and 10.9 months for the chemotherapy arm at the time of the initial publication. The median OS was not reached with cemiplimab (95% CI 17.9 to not evaluable [NE]) versus 14.2 months (95% CI 11.2–17.5) with chemotherapy (hazard ratio [HR] 0.57; 95% CI 0.42–0.77; p=0.002) and median PFS was 8.2 (95% CI 6.1–8.8) with cemiplimab versus 5.7 (95% CI 4.5–6.2) with chemotherapy (HR 0.54; 95% CI 0.43–0.68; p<0.0001). The OS and PFS benefits with cemiplimab were evident in all subgroups examined, including in all age groups (<60 years old and ≥60 years old), with squamous and non-squamous histology, both locally advanced and metastatic disease, and in the presence of brain metastases, except for OS in female patients. However, given the small number of events involving female patients (25 out 84 female patients), the investigators pointed out that it may be difficult to draw any firm conclusions on the benefit of cemiplimab in this subpopulation group.5
In terms of the objective response, the cemiplimab group demonstrated 39% (95% CI 34–45) versus 20% for the chemotherapy group (95% CI 16–26), with an odds ratio (OR) of 2.53 95% CI 1.74–3.69; p<0.0001). The exploratory analysis of different PD-L1 expression proportion scores showed that the PD-L1 expression scores correlated with incremental improvements in OS, PFS and ORR. For instance, PD-L1 ≥90% had a median OS of not reached (95% CI 17.3–NE) versus 15.1 months (95% CI 11.1–NE) (HR 0.46; 95% CI 0.25–0.85), median PFS of 15.3 months (95% CI 10.4–18.7) versus 5.9 months (95% CI 4.3–6.2) (HR 0.28; 95% CI 0.17–0.46) and ORR of 46% versus 18%, whereas PD-L1 ≥50 to ≤60% had a median OS of 21.9 versus 14.0 (HR 0.77; 95% CI 0.49–1.23), median PFS of 4.3 versus 6.2 (HR 0.79; 95% CI 0.56–1.12) and ORR of 32% versus 23%.5
Regarding the rest of the secondary endpoints, the median duration of response was 16.7 months (95% CI 12.5–22.8) for cemiplimab versus 6 months (95% CI 4.3–6.5) for chemotherapy. In addition, early and sustained clinically meaningful improvements in HRQoL were observed with cemiplimab but not with chemotherapy. Treatment-related adverse events occurred in 57% of the cemiplimab group and 89% of the chemotherapy group. Treatment-emergent adverse events, regardless of attribution, that led to death occurred in 10% of patients treated with cemiplimab versus 9% in patients treated with chemotherapy. When specifically looking at immune-related adverse events (irAEs), 17% of patients had adverse events in the cemiplimab group, with one patient succumbing to immune-related nephritis, compared with 2% in the chemotherapy group, with no reported immune-related deaths.5
Based on the EMPOWER-Lung 1 study data, in February 2021, the FDA approved cemiplimab as first line monotherapy for patients with advanced NSCLC with PD-L1 expression ≥50% otherwise negative for EGFR, ALK or ROS1 aberrations.6
The 3 year follow up of the EMPOWER-Lung 1 study has been presented at the European Society for Medical Oncolology (ESMO) 2022, and reported an updated median OS of 26.1 months in the cemiplimab arm versus 13.3 months in the chemotherapy arm (HR 0.57; 95% CI 0.46-0.71; p<0.0001). The median PFS was 8.1 months versus 5.3 months (HR 0.51; 95% CI 0.42-0.62; p<0.0001), and the ORR was 46.5% versus 21.0% (OR 3.26; p<0.0001) with cemiplimab arm versus chemotherapy arm, respectively.7
At the European Lung Cancer Congress (ELCC) 2023, updated subgroup analyses from the EMPOWER-Lung 1 study were presented. In locally advanced NSCLC, which was largely excluded in prior immunotherapy clinical trials, the cemiplimab group had a median OS of 26.1 months versus 13.9 months in the chemotherapy group (HR 0.67; CI 95% 0.38–1.17). PFS was 8.1 months in the cemiplimab group versus 6.2 months in the chemotherapy group (HR 0.56; 95% CI 0.35–0.95). Tumor response was 48.9% in the cemiplimab group versus 31% in the chemotherapy group (OR 2.08; 95% CI 0.88–4.95).8 Patients with treated, clinically stable brain metastases at baseline were evaluated as well. Median OS was NE in the cemiplimab group versus 20.7 months in the chemotherapy group (HR 0.42; 95% CI 0.20–0.87). PFS was 12.5 months in the cemiplimab group versus 5.3 months in the chemotherapy group (HR 0.34; 95% CI 0.18–0.63).9 Tumor response was 55.9% in the cemiplimab group versus 11.4% in the chemotherapy group (OR 9.27; 95% CI 2.62–32.74; p=0.0002). In these subgroups, which are often excluded in trials on NSCLC involving immunotherapy, cemiplimab continued to demonstrate its clinically relevant efficacy and tolerability.
EMPOWER-Lung 3
In August 2022, Gogishvili et al published EMPOWER-Lung 3, a double-blind, placebo-controlled, phase 3 study evaluating cemiplimab plus platinum doublet chemotherapy in the first line treatment setting for NSCLC, irrespective of PD-L1 expression or histology. Eligible patients included adults ≥18 years old, with ECOG ≤1 and histologically or cytologically confirmed squamous or non-squamous NSCLC, including unresectable locally advanced disease not suitable for definitive chemoradiation or metastatic disease. Notable exclusion criteria included active or untreated brain metastases, tumors with EGFR mutations, ALK translocations or ROS1 fusions, active or suspected autoimmune disease that required systemic treatment, and uncontrolled hepatitis B or C. Again, those with controlled hepatitis B or C were eligible. One major difference in the inclusion criteria compared to EMPOWER-Lung 1 was that never-smokers, defined as individuals who had smoked fewer than 100 cigarettes in their lifetime, were included in the study.10
A total of 466 patients were enrolled and randomly assigned 2:1 to cemiplimab plus chemotherapy (n=312) or placebo plus chemotherapy (n=154), with a median duration of follow-up of 16.3 months in the cemiplimab plus chemotherapy arm and 16.7 months in the chemotherapy arm. In the study, cemiplimab was given 350 mg every 3 weeks for up to 108 weeks in combination with four cycles of platinum-doublet chemotherapy, followed by pemetrexed maintenance as indicated. The primary endpoint was median OS: the cemiplimab plus chemotherapy group had a median OS of 21.9 months (95% CI 15.5–NE) versus 13.0 months (95% CI 11.9–16.1) in the chemotherapy plus placebo group (HR 0.71; 95% CI 0.53–0.93; p=0.014). Exploratory analysis of predefined subgroups demonstrated overall numeric improvement favoring the cemiplimab plus chemotherapy group, except in women, never-smokers and patients with PD-L1 <1%. However, it must be noted that these subgroups were small and not powered to examine these discrepancies. Furthermore, these discrepancies were not observed in other secondary endpoint subgroup analyses including PFS and ORR, which may reflect an earlier treatment effect. As for the secondary endpoints, the cemiplimab plus chemotherapy group showed a median PFS of 8.2 months (95% CI 6.4–9.3) versus 5.0 months (95% CI 4.3–6.2) for the placebo plus chemotherapy group (HR 0.56; 95% CI 0.44–0.70; p<0.0001). Regarding ORR, cemiplimab plus chemotherapy demonstrated 43.3% (95% CI 37.7–49.0) versus 22.7% for the placebo plus chemotherapy group (95% CI 16.4–30.2) (OR 2.68; 95% CI 1.72–4.19; p<0.0001). The median DOR with cemiplimab plus chemotherapy was 15.6 months (95% CI 12.4–NE) versus 7.3 months (95% CI 4.3–12.6) for the placebo plus chemotherapy group. Regarding safety, treatment-related adverse events were observed in 88.1% of patients treated with cemiplimab plus chemotherapy versus 84.3% of patients in the placebo plus chemotherapy group. When specifically looking at irAEs, these occurred in 18.9% of patients treated with cemiplimab plus chemotherapy, with grade ≥3 irAEs occurring in 2.9% of patients. Treatment was discontinued in three patients (1.0%) owing to irAEs, and ultimately one patient (0.3%) died as a result of immune-mediated pneumonitis.10
Based on the EMPOWER-Lung 3 data, in November 2022, the FDA approved cemiplimab in combination with platinum-based chemotherapy for the first line treatment of adult patients with advanced NSCLC with no EGFR, ALK or ROS aberrations, regardless of PD-L1 expression.11
In March 2023, the 2-year follow-up of EMPOWER-Lung 3 was presented. Cemiplimab plus chemotherapy showed an improvement in survival versus placebo plus chemotherapy, with a median OS of 21.1 months for cemiplimab plus chemotherapy versus 12.9 months for placebo plus chemotherapy (HR 0.65; 95% CI 0.51–0.82; p=0.0003), a median PFS of 8.2 vs 5.5 months (HR 0.55; 95% CI 0.44–0.68; p<0.0001) and ORR of 43.6% vs 22.1%. The safety data remained generally consistent with previously reported data.12
Discussion
As demonstrated in both EMPOWER-Lung 1 and EMPOWER-Lung 3, the PD-1/PD-L1 signaling pathway once again proved to be an important target in managing advanced/metastatic NSCLC tumors without EGFR, ALK and ROS aberrations, as monotherapy or in combination with chemotherapy. In the setting of high PD-L1, with the addition of cemiplimab-rwlc, we now have a total of three anti-PD-1/PD-L1 agents that can be used as monotherapy, the others being pembrolizumab and atezolizumab.
Several key similarities and differences in the IMpower110, KEYNOTE 024 and EMPOWER-Lung 1 studies which led to the approval of atezolizumab, pembrolizumab and cemiplimab, respectively, have been highlighted in Table 1. Similar inclusion and exclusion criteria were utilized in all three studies. They all evaluated patients with NSCLC, and both squamous and non-squamous histology without EGFR mutations or ALK translocations. All patients had an overall ECOG ≤1, and those with uncontrolled autoimmune disease, hepatitis B/C or HIV were excluded. Several differences to highlight, however, are that EMPOWER-Lung 1 included not only patients with metastatic disease but also those with locally advanced (stage IIIB/IIIC, who were not candidates for definitive chemoradiotherapy), and along with EGFR mutations and ALK fusions, the study also excluded ROS1 aberrations and non-smokers.5 Unlike the EMPOWER-Lung 1 study and KEYNOTE 024, which only included PD-L1 ≥50%, IMpower110 included patients with PD-L1 ≥1%, which was later subdivided into the high PD-L1 group, defined as PD-L1 ≥50% or ≥10% of tumor-infiltrating cells.13 Since all three studies had slightly different primary endpoints and variations in their study design, it is difficult to make any definitive comparisons. It is still worth noting that KEYNOTE 024, involving pembrolizumab, has the longest follow-up of these studies and has reported a median PFS of 7.7 months (while IMpower110 had a median of 8.2 months with atezolizumab and EMPOWER-Lung 1 had a median of 8.1 months with cemiplimab), with a similar control group having a median PFS of approximately 6.0 months, although all of the patients enrolled in IMpower110 and KEYNOTE 024 had stage IV disease, while EMPOWER-Lung 1 included patients with unresectable stage III disease as well.14 Comparing the updated OS data from each study, pembrolizumab again has the longest follow-up and has reported its 5-year updates as having a median OS of 26.3 months in the pembrolizumab arm versus 13.4 months in the chemotherapy arm (HR 0.62; 95% CI 0.48–0.81).15 Three year follow up of the EMPOWER-Lung 1 study has reported a median OS of 26.1 months in the cemiplimab arm versus 13.3 months in the chemotherapy arm (HR 0.57; 95% CI 0.46-0.71; p=0.0001) and, lastly, atezolizumab, from the exploratory analysis in high PD-L1 expression, reported a median OS of 20.2 months in the atezolizumab group versus 14.7 months in the chemotherapy group (HR 0.76; 95% CI 0.54–1.09; statistically not significant).7,16 ORR showed similar trends with cemiplimab (46.5%), pembrolizumab (46.1%), and atezolizumab (38.3%). Although it is difficult to determine why the cemiplimab study had good outcomes, it may be at least partially related to inclusion of patients with stage IIIB/IIIC cancer who were not candidates for definitive chemoradiotherapy. However, it is worth noting that the proportion of squamous histology included in each study treatment arm were largely different; EMPOWER-Lung 1 (cemiplimab) had 43.3%, KEYNOTE 024 (pembrolizumab) had 18.8%, and IMpower110 (atezolizumab) had 25.2%. With regard to the safety data looking specifically at immune-mediated adverse events, cemiplimab had the fewest overall immune-mediated adverse events of 22.5%, with 4.8% at grade ≥3, followed by pembrolizumab, with overall immune-mediated adverse events of 34.4% and 13.6% at grade ≥3, and lastly atezolizumab, having overall immune-mediated adverse events of 46.2%, with 10.2% at grade ≥3, although there are differences in follow-up time.15,16
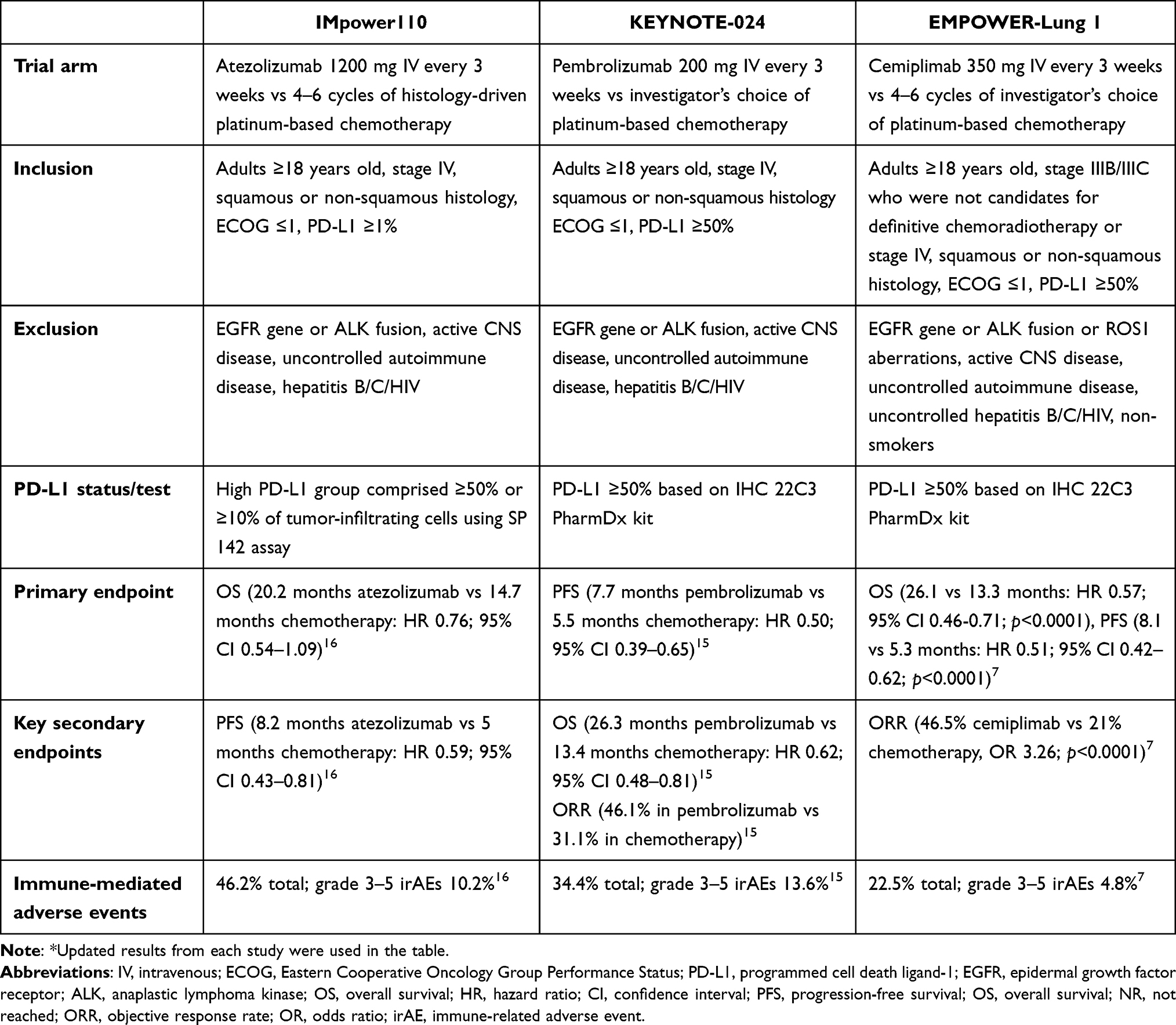 |
Table 1 Key Element Comparison of IMpower110, KEYNOTE-024 and EMPOWER-Lung 1* |
All in all, atezolizumab, pembrolizumab and cemiplimab demonstrated superior efficacy in treating NSCLC patients with PD-L1 ≥50% as a first line monotherapy compared to chemotherapy alone, resulting in FDA approval of each drug. Unfortunately, since there are no head-to-head studies comparing the efficacy of these drugs, it is hard to determine which one is superior, although pembrolizumab has the longest follow-up. Immune-related side effects perhaps least seen with cemiplimab.
As demonstrated in the EMPOWER-Lung 3 trial, cemiplimab in combination with chemotherapy improved OS, ORR and PFS compared to the chemotherapy plus placebo group, irrespective of PD-L1 status, ultimately leading to the FDA approval. Similar studies have been conducted in the past using pembrolizumab, in KEYNOTE-189 and KEYNOTE-407. Table 2 highlights some key similarities and differences in the KEYNOTE-189, KEYNOTE-407 and EMPOWER-Lung 3 trials. All three studies incorporated immunotherapy into the chemotherapy backbone in the first line treatment for patients with metastatic NSCLC, with ECOG ≤1 and stable CNS and autoimmune disease. Key differences to note are that the EMPOWER-Lung 3 trial included both squamous and non-squamous histology and stage IIIB/IIIC patients who were not candidates for definitive chemoradiation therapy.10,17,18 KEYNOTE-189, however, only specifically looked at patients with metastatic non-squamous NSCLC, whereas KEYNOTE-407 specifically looked at metastatic squamous NSCLC. Primary endpoints were both OS and PFS in all three studies. After a median follow-up of 31 months, KEYNOTE-189 demonstrated a median OS of 22.0 months in the pembrolizumab plus chemotherapy group versus 10.6 months with placebo plus chemotherapy (HR 0.56; 95% CI 0.46–0.69). Median PFS was 9.0 months in the pembrolizumab with chemotherapy group versus 4.9 months in the placebo plus chemotherapy group (HR 0.49; 95% CI 0.41–0.59).19 The EMPOWER-Lung 3 trial had a median OS of 21.1 months in the cemiplimab plus chemotherapy group versus 12.9 months in the placebo plus chemotherapy group (HR 0.65; 95% CI: 0.51-0.82; p=0.0003). The median PFS was 8.2 months in the cemiplimab plus chemotherapy group versus 5.5 months in the placebo plus chemotherapy group (HR 0.55; 95% CI: 0.44-0.68; p<0.0001).10 Lastly, KEYNOTE-407, which only looked at stage IV squamous cell lung cancer histology, showed a median OS of 17.1 months in the pembrolizumab plus chemotherapy group versus 11.6 months in the placebo plus chemotherapy group (HR 0.71; 95% CI, 0.58–0.88).20 The median PFS was 8.0 months in the pembrolizumab plus chemotherapy group versus 5.1 months in the placebo plus chemotherapy group (HR 0.57; 95% CI, 0.47–0.69).20 Of note, in the EMPOWER-Lung 3 study the treatment arm group comprised, overall, 57.4% with non-squamous histology and 42.6% with squamous histology.10
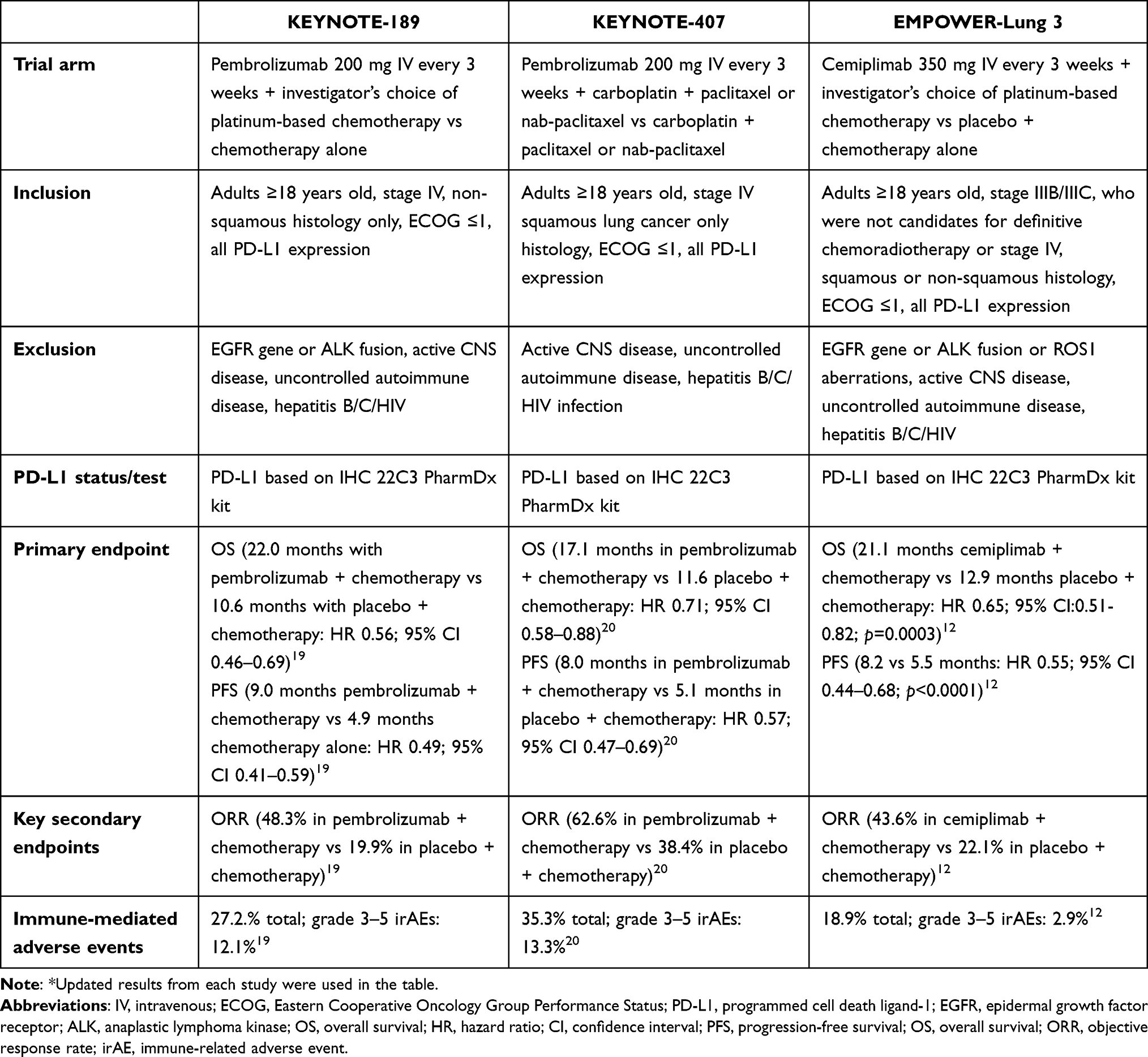 |
Table 2 Key Element Comparison of KEYNOTE-189, KEYNOTE-407 and EMPOWER-Lung 3* |
At the European Lung Cancer Congress 2023, Makharadze et al presented the 2-year protocol-specified follow-up results of EMPOWER-Lung 3, which included a subgroup analysis comparing the OS and PFS data in patients with squamous versus non-squamous histology. When specifically looking at the squamous cell histology group, the cemiplimab plus chemotherapy group had a median OS of 22.3 months versus 13.8 months in the placebo plus chemotherapy group (HR 0.61; 95% CI 0.42–0.87). The median PFS was 8.2 months in the cemiplimab plus chemotherapy group versus 4.9 months in the placebo plus chemotherapy group. In contrast, in the non-squamous cell histology group, the median OS in the cemiplimab plus chemotherapy group was 19.4 months versus 12.4 months in the placebo plus chemotherapy group (HR 0.64; 95% CI 0.47–0.88). The median PFS was 7.9 months in the cemiplimab group versus 5.7 months in the placebo plus chemotherapy group (HR 0.53; 95% CI 0.39–0.71).21 Although this subgroup analysis was not statistically powered and the median follow-up time was slightly shorter in the EMPOWER-Lung 3 trial (28.4 months) than in KEYNOTE-407 (31 months), it is still worth noting that the cemiplimab plus chemotherapy group demonstrated better results for both PFS and OS in squamous histology compared to non-squamous histology. In addition, although it is difficult to make a head-to-head comparison between pembrolizumab plus chemotherapy and cemiplimab plus chemotherapy specifically looking at the squamous histology group, cemiplimab plus chemotherapy appears to have better OS (22.3 months vs 17.1 months) compared to the pembrolizumab plus chemotherapy group.
Based on these studies, tumor histology appears to play an important role in determining the efficacy of immunotherapy in combination with chemotherapy, although cross-trial comparisons must be performed with caution.
In conclusion, cemiplimab presents a new option for patients with advanced metastatic NSCLC without EGFR, ALK or ROS1 alterations, which can be used in monotherapy or in combination with chemotherapy. While it may not fulfill an “unmet need”, the addition of another option for immunotherapy in NSCLC, as monotherapy or in combination with chemotherapy, may help us to better manage patients in a more personalized way and could help us to find the best therapeutic strategy for each individual.
Funding
This manuscript did not receive any funding.
Disclosure
There are no direct conflicts of interest to disclose. Dr Ahn has no potential conflicts to disclose. Dr Nagasaka has received consulting fees from Caris Life Sciences, honoraria from AstraZeneca, Daiichi Sankyo, Novartis, Lilly, Pfizer, EMD Serono, Genentech, Mirati, Takeda, Janssen and Blueprint Medicine, and travel support from AnHeart Therapeutics.
References
1. Kazandjian D, Suzman DL, Blumenthal G, et al. FDA approval summary: nivolumab for the treatment of metastatic non-small cell lung cancer with progression on or after platinum-based chemotherapy. Oncologist. 2016;21(5):634–642. doi:10.1634/theoncologist.2015-0507
2. Antonia SJ, Villegas A, Daniel D, et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N Engl J Med. 2017;377(20):1919–1929. doi:10.1056/NEJMoa1709937
3. Felip E, Altorki N, Zhou C, et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet. 2021;398(10308):1344–1357. doi:10.1016/S0140-6736(21)02098-5
4. Forde PM, Spicer J, Lu S, et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med. 2022;386(21):1973–1985. doi:10.1056/NEJMoa2202170
5. Sezer A, Kilickap S, Gümüş M, et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet. 2021;397(10274):592–604. doi:10.1016/S0140-6736(21)00228-2
6. US Food and Drug Administration. FDA approves cemiplimab-rwlc for non-small cell lung cancer with high PD-L1 expression. 2021.
7. Ozguroglu M, Kilickap S, Sezer A. Three years survival outcome and continued cemiplimab (CEMI) beyond progression with the addition of chemotherapy (chemo) for patients (pts) with advanced non-small cell lung cancer (NSCLC): the EMPOWER-Lung 1 trial. Ann Oncol. 2022;33(suppl_7):S808–S869. doi:10.1016/annonc/annonc1089
8. Kalinka E, Bondarenko I, Gogishvili M, et al. First-line cemiplimab for locally advanced non-small cell lung cancer: updated subgroup analyses from EMPOWER-Lung 1 and EMPOWER-Lung 3. J Thorac Oncol. 2023;18:S106. doi:10.1016/S1556-0864(23)00369-6
9. Kilickap S, Özgüroğlu M, Sezer A, et al. EMPOWER-Lung 1: cemiplimab monotherapy as first-line treatment of patients with brain metastases from advanced non-small cell lung cancer with programmed cell death-ligand 1(PDL1) ≥50%: 3-year update. J Thorac Oncol. 2023;18:S42–S43. doi:10.1016/S1556-0864(23)00264-2
10. Gogishvili M, Melkadze T, Makharadze T, et al. Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: a randomized, controlled, double-blind phase 3 trial. Nat Med. 2022;28(11):2374–2380. doi:10.1038/s41591-022-01977-y
11. US Food and Drug Administration. FDA approves cemiplimab-rwlc in combination with platinum-based chemotherapy for non-small cell lung cancer. 2022.
12. Tamta Makharadze M. Cemiplimab plus chemotherapy versus chemotherapy alone in advanced non-small cell lung cancer: 2-year follow-up from the phase 3 EMPOWER-lung 3 part 2 trial. 2023.
13. Herbst RS, Giaccone G, de Marinis F, et al. Atezolizumab for first-line treatment of PD-L1-selected patients with NSCLC. N Engl J Med. 2020;383(14):1328–1339. doi:10.1056/NEJMoa1917346
14. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
15. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Five-year outcomes with pembrolizumab versus chemotherapy for metastatic non-small-cell lung cancer with PD-L1 tumor proportion score >/= 50. J Clin Oncol. 2021;39(21):2339–2349. doi:10.1200/JCO.21.00174
16. Jassem J, de Marinis F, Giaccone G, et al. Updated overall survival analysis from IMpower110: atezolizumab versus platinum-based chemotherapy in treatment-naive programmed death-ligand 1-selected NSCLC. J Thorac Oncol. 2021;16(11):1872–1882. doi:10.1016/j.jtho.2021.06.019
17. Paz-Ares L, Luft A, Vicente D, et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. 2018;379(21):2040–2051. doi:10.1056/NEJMoa1810865
18. Gandhi L, Rodríguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078–2092. doi:10.1056/NEJMoa1801005
19. Rodriguez-Abreu D, Powell SF, Hochmair MJ, et al. Pemetrexed plus platinum with or without pembrolizumab in patients with previously untreated metastatic nonsquamous NSCLC: protocol-specified final analysis from KEYNOTE-189. Ann Oncol. 2021;32(7):881–895. doi:10.1016/j.annonc.2021.04.008
20. Paz-Ares L, Vicente D, Tafreshi A, et al. A randomized, placebo-controlled trial of pembrolizumab plus chemotherapy in patients with metastatic squamous NSCLC: protocol-specified final analysis of KEYNOTE-407. J Thorac Oncol. 2020;15(10):1657–1669. doi:10.1016/j.jtho.2020.06.015
21. Tamta Makharadze MG, Melkadze T, Baramidze A. Cemiplimab plus chemotherapy versus chemotherapy alone in advanced non-small cell lung cancer: 2-year follow-up results from the Phase 3 EMPOWER-Lung 3 Part 2 trial. 2023.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.