Back to Journals » Journal of Pain Research » Volume 16
Spinal Excitability in Patients with Painful Chronic Pancreatitis
Authors Knoph CS ![]() , Nedergaard RB
, Nedergaard RB ![]() , Olesen SS, Kuhlmann L
, Olesen SS, Kuhlmann L ![]() , Drewes AM
, Drewes AM
Received 4 March 2023
Accepted for publication 10 June 2023
Published 5 July 2023 Volume 2023:16 Pages 2287—2298
DOI https://doi.org/10.2147/JPR.S408523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Cecilie Siggaard Knoph,1,2 Rasmus Bach Nedergaard,1 Søren Schou Olesen,1,2 Louise Kuhlmann,1 Asbjørn Mohr Drewes1,2
1Center for Pancreatic Diseases & Mech-Sense, Department of Gastroenterology and Hepatology, Aalborg University Hospital, Aalborg, Denmark; 2Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
Correspondence: Asbjørn Mohr Drewes, Center for Pancreatic Diseases, Department of Gastroenterology and Hepatology, Aalborg University Hospital, Mølleparkvej 4, Aalborg, 9000, Denmark, Tel +45 97663562, Email [email protected]
Purpose: Abdominal pain is common in patients with chronic pancreatitis (CP), but management is challenging – possibly due to altered pain processing within the central nervous system rendering conventional treatments ineffective. We hypothesized that many patients with painful CP have generalized hyperalgesia correlating with central neuronal hyperexcitability.
Patients and Methods: Seventeen CP patients with pain and 20 matched healthy controls underwent experimental pain testing, including repeated pain stimuli (temporal summation), pressure algometry performed in dermatomes with same spinal innervation as the pancreatic gland (pancreatic areas) and remote dermatomes (control areas), a cold pressor test and a conditioned pain modulation paradigm. To probe central neuronal excitability, the nociceptive withdrawal reflex was elicited by electrical stimulation of the plantar skin, and electromyography was obtained from the ipsilateral anterior tibial muscle together with somatosensory evoked brain potentials.
Results: Compared to healthy controls, patients with painful CP had generalized hyperalgesia as evidenced by 45% lower pressure pain detection thresholds (P< 0.05) and decreased cold pressor endurance time (120 vs 180 seconds, P< 0.001). In patients, reflex thresholds were lower (14 vs 23 mA, P=0.02), and electromyographic responses were increased (16.4 vs 9.7, P=0.04) during the withdrawal reflex, reflecting predominantly spinal hyperexcitability. Evoked brain potentials did not differ between groups. A positive correlation was found between reflex thresholds and cold pressor endurance time (ρ=0.71, P=0.004).
Conclusion: We demonstrated somatic hyperalgesia in patients with painful CP associated with spinal hyperexcitability. This highlights that management should be directed at central mechanisms using, eg, gabapentinoids or serotonin-noradrenaline reuptake inhibitors.
Keywords: pain, hyperalgesia, nociceptive withdrawal reflex, electroencephalography, electromyography
Introduction
Chronic pancreatitis (CP) is a progressive fibro-inflammatory disease resulting in fibrosis and atrophy of the gland, which may, in time, lead to anatomical and functional changes. The most common symptom in CP is abdominal pain. Studies have found that 70–85% of the CP patients report abdominal pain,1,2 being the most common cause of hospitalization in these patients.3 Pain in CP may result from mechanical obstruction, neuropathic or inflammatory alterations within the diseased pancreas.4 However, it may also be influenced by hyperalgesia caused by neuroplastic changes within the central nervous system.5–10 The presence of pain is strongly associated with a poor quality of life and health resource utilization.3,11,12 Nevertheless, only 10% of the CP patients with a history of pain are sufficiently treated (pain-free with therapy).1 This warrants an improvement in the management and characterization of pain in CP.
Hyperalgesia in patients with painful CP can be widespread or segmental, depending on the distribution of changes in central pain processing.13 Hence, hyperalgesia may be caused by spinal or supraspinal neuronal changes and typically a combination of both. We and others have previously examined the presence and localization of hyperalgesia in patients with CP using quantitative sensory testing (QST).13,14 In this test battery, spinal convergence of afferents from the pancreas and somatic structures allows for visceral hyperalgesia to be indirectly evaluated using testing of different dermatomes.15,16 Thus, by examining somatic hyperalgesia using QST, information can be provided on changes within the central nervous system, such as neuronal hyperexcitability.
To investigate spinal neuronal excitability more directly, the nociceptive withdrawal reflex (NWR) can be used. The NWR is a polysynaptic spinal reflex that facilitates withdrawal from potentially damaging stimuli to the skin.17,18 The NWR has previously been used to evaluate spinal pain processing as there is a relation between reflex thresholds and pain thresholds and a correlation between the size of NWR and experienced pain.17 The NWR is not specific to pancreatic disorders but may reflect alterations to the spinal pain processing in general as shown in several other diseases.19–22 Altered pain processing was expected to occur in patients with painful CP and therefore the NWR is a valid tool in this setting. Supraspinal excitability can be concurrently evaluated by capturing the somatosensory evoked potential triggered by the painful stimulus used to evoke the NWR using electroencephalography (EEG).
We hypothesized that many patients with painful CP would display hyperalgesia during quantitative sensory testing of the pain system and that the QST measures would correlate to spinal and supraspinal hyperexcitability assessed using electromyography (EMG) and EEG when the NWR is evoked. In patients with painful CP as compared to healthy controls, the aims were to assess 1) hyperalgesia using pressure thresholds in various dermatomes, temporal summation, and conditioned pain modulation capacity; 2) spinal excitability by quantifying reflex threshold and size of the NWR; 3) supraspinal excitability by capturing the somatosensory evoked potential triggered by the NWR; and finally, 4) to explore the correlations between QST and central neurophysiologic measures separating CP patients and controls.
Materials and Methods
Study Population
This study was conducted at the Center for Pancreatic Diseases, Department of Gastroenterology and Hepatology, Aalborg University Hospital, Denmark, from February 2014 to December 2018 under a previously published protocol.23 Patients and age- and gender-matched healthy controls were included in a randomized, placebo-controlled study regarding the long-term effects of ketamine on pain treatment in patients with CP. Patients aged 18 or above with a CP diagnosis (according to the Mayo Clinic diagnostic criteria)24 and deemed compliant were eligible for participation in the study. Furthermore, patients had to suffer from chronic abdominal pain (pain ≥3 days per week for at least 3 months), and they should consider their pain insufficiently treated using the prescribed analgesic treatment. Patients were also asked to answer the validated Brief Pain Inventory.25
The study was approved by the North Denmark Region Committee on Health Research Ethics (N-20130040) and the Danish Health and Medicines Authorities (http://www.clinicaltrialsregister.eu, EudraCT no.: 2013-003357-17). All participants gave written informed consent before any study-related procedures, and the study was conducted in agreement with the Helsinki declaration.
Experimental Procedure
Quantitative Sensory Testing
All participants in the study underwent QST measurements as previously described,14 but with few exceptions. Thus, temporal summation was performed using electrical stimulations and not pin-prick. The participants were asked to rate the electrical pain detection threshold. The electrical current intensity used to evoke this was multiplied by 1.5 and applied as a single electrical stimulation. Participants would then rate the sensation using an electronic visual analogue scale (VAS) coupled to a computer with software designed for the purpose. Participants were instructed that VAS ranged from 0–10 (0=no pain, 1=first sensation of pain, 10=maximum imaginable pain). Subsequently, a series of 5 stimulations were applied using the same current intensity, and participants were asked to rate the sensation accordingly.26 The temporal summation score was calculated as the difference in pain score (VAS) after 5 stimulations vs 1 stimulation. This procedure was applied to a control area (right C5 dermatome) and a pancreatic area (ventral Th10 dermatome).
Pressure stimulations were performed using a pressure algometer (Somedic AB, Stockholm, Sweden), which increases pressure at a rate of 30 kPa/sec until the participants reached pain detection threshold (pPDT) and pain tolerance threshold (pPTT), respectively. Values for pPDT and pPTT were an average of three consecutive assessments. For all participants, pressures were applied at 6 locations on the right body side: C5 dermatome, Th4 dermatome, ventral Th10 dermatome, dorsal Th10 dermatome, L1 dermatome, and L4 dermatome. To compare with previous QST findings, we excluded the measurement from the Th4 dermatome.14
During the cold pressor test, participants were asked to keep their right hand immersed in the cold water (temperature of 2 degree Celsius) for 180 seconds or until the pain became unbearable. The period each participant could keep their hand immersed in water was noted as the endurance time. Every 10 seconds, subjects were asked to rate the pain using the VAS. The cold pressor test was used as a conditioning stimulus for activating descending pain modulation from supraspinal structures (conditioning pain modulation).26 This response was evaluated by applying a test pain stimulus before and after the conditioning stimulus (cold pressor test). We used pPTT assessed on the left L4 dermatome as the test pain stimulus. Conditioned pain modulation was subsequently calculated as the percentual rise in pPTT following the conditioning stimulus – thereby giving a measure for descending pain modulation capacity.27
Nociceptive Withdrawal Reflex
The NWR was elicited as outlined in one of our previously published articles.28 At the site of innervation of the medial plantar nerve on the plantar skin, the NWR was elicited by electrical stimulation. The arch of the sole of the right foot was used for placement of the cathode (15 × 15 mm, Neuroline 700; Ambu A/S, Denmark), whereas the anode was placed on the dorsum of the foot (50 × 90 mm, Synapse; Ambu A/S, Denmark). A constant current of five square-wave pulses was delivered as previously described.28 All the electrical stimulations were managed within a custom-made software program (Center for Sensory-Motor Interaction, Aalborg University, Denmark). The stimulus intensity was manually increased with 1 mA at a time. The perception threshold was noted as the stimulation intensity (in mA) where the participant felt first sensation. For identification of the reflex threshold the staircase method was used, as previously described in detail.29 Subsequently, the intensity (in mA) needed for elicitation of the NWR was noted. After identifying and rating the reflex threshold, the participant was given a total of 18 stimuli at three different intensities with intervals of 8–12s between stimuli. Thus, the participant was given six stimuli of each intensity in a randomized order. The intensities were divided into low intensity (1 × Reflex threshold), medium intensity (1.3 X reflex threshold), and high intensity (1.6 × Reflex threshold). This method of stimulations has been used previously.28
Electromyography
EMG data from the belly of the ipsilateral tibialis anterior muscle were obtained during stimulations. For preparation and cleaning of the skin prior to the placement of two surface electrodes, sandpaper and alcohol was used. One electrode (15 × 15 mm, Neuroline 700; Ambu A/S, Ballerup, Denmark) was placed on the muscle, while one grounding electrode (50 × 90 mm, Synapse; Ambu A/S) was placed just below the patella. The signal was then bandpass filtered between 5 and 500 Hz by utilization of a zero-phase digital 12th-order Butterworth filter.
Electroencephalography
During the NWR, EEG data were recorded using the Quick-Cap International (Compumedics® Neuroscan™, El Paso, TX, USA), which is a 62-channel surface electrode EEG cap. For this recording, the 10–20 system was used. Maximum impedance was 5 kΩ. EEG data were recorded continuously with open filters and a sampling rate of 1000 Hz (SynAmp, Neuroscan, El Paso, TX, USA).
Data Analysis
Not all patients were able to complete the whole protocol due to discomfort. A detailed overview of the data available for each examination modality is shown in Figure 1. The EMG and EEG data were analyzed in MATLAB (R 2021a Math-works Inc., Natick, MA, USA).
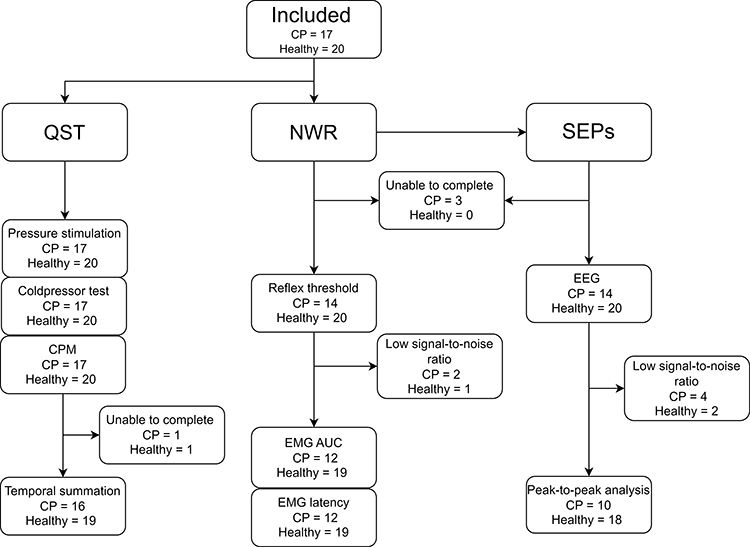 |
Figure 1 Overview of data available for each measure. Abbreviations: CP, chronic pancreatitis; QST, quantitative sensory testing; NWR, nociceptive withdrawal reflex; SEPs, somatosensory evoked potentials; CPM, conditioned pain modulation; EEG, electroencephalography; EMG, electromyography. |
Electromyography
For the analysis of EMG data, the interval peak z-scores were quantified on single sweeps.30 The z-score was defined as previously described.31 Definitions for the pre-stimulus window and the reflex window were set as previously described.28 In all cases, a rectified area under the curve (AUC) was calculated in the reflex window. For each subject, we calculated a mean AUC from all stimulations. A peak interval z-score was set at 6 based on a previously published method.32 If the z-score was above 6 at any time during the reflex window, this was interpreted as an elicited NWR. In case of successful elicitation, we defined the latency as the first timepoint where the z-score was above 6. For each subject, we calculated a mean latency.
Electroencephalography
Data were analyzed using the EEGLAB toolbox for MATLAB (version 14.1.2; Schwartz Center for Computational Neuroscience, Institute for Neural Computation, University of California, San Diego, CA, USA). The EEG data were filtered using a 1 Hz filter to remove direct current drift and a 49–51 Hz notch filter to remove mains noise. The Clean_artifacts Toolbox with default settings and “window criterion” off was used to remove additional noise from the dataset. Channels containing noise were interpolated using spherical interpolation, and all channels were afterward referenced to a standard reference. All data were visually inspected prior to independent component analysis (ICA). The data were down-sampled to 250 Hz for ICA, “runica” was used in combination with ICALabel to visually distinguish independent components containing biological or outside noise.33 After selecting components containing non-biological signals, the analyzed data were added to the entire dataset (1000 Hz), and the components selected for removal were pruned from the dataset. Evoked potentials were averaged across stimulations.
Evoked Potential Feature Extraction
The amplitudes and corresponding latencies of averaged evoked potentials for each subject from the peaks P1, N1, and P2 were extracted from the Cz electrode. These were manually selected by an assessor blinded to the two groups (CP patient or healthy control).
Statistics
Continuous variables were checked for normality using the Shapiro–Wilks test and presented as mean ± SD or median (IQR) as appropriate. Group comparisons were performed using the Student’s t-test or the non-parametric Wilcoxon Rank Sum test. Proportions were presented as %, and group differences were tested using the chi-squared test. A multilevel mixed-effects model compared groups with pressure thresholds as dependent variables and interaction between disease status and examination site as independent variables. Repeated measurements were included with subjects and stimulation sites as random effects. Group comparisons of the reported VAS during the cold pressor test were also performed using a mixed linear model of repeated measures. In this model, we included subjects and time as random effects. Individual stimulation sites during pressure stimulations were compared using post hoc Bonferroni corrections; however, we refrained from Bonferroni corrections when comparing individual timepoints during the cold pressor test due to the high number of repeated measures. EEG measures were illustrated graphically groupwise, and groups were compared using a multilevel mixed-effects model. The same approach was used as for the pressure stimulation thresholds. Correlation between NWR findings, clinical characteristics, and QST measures were examined using Spearman’s ρ. P-values below 0.05 were considered statistically significant. All statistical calculations were conducted in R version 1.4.
Results
Seventeen patients with CP and 20 healthy controls were included. Patients had a higher proportion of smokers and were shorter than the healthy controls, but the groups were otherwise comparable (Table 1).
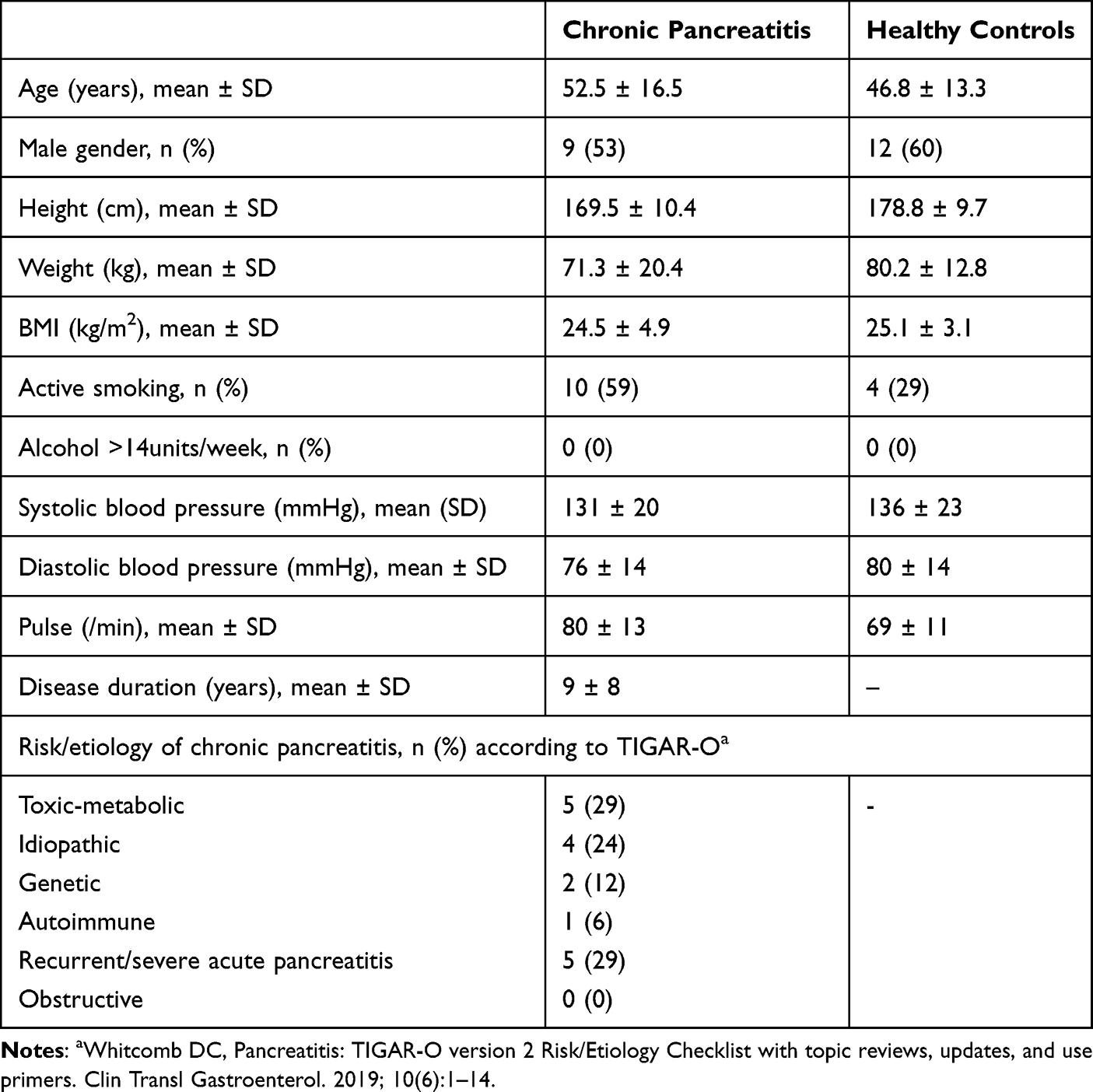 |
Table 1 Basic Demography of Included Chronic Pancreatitis Patients (n = 17) and Healthy Controls (n = 20) |
Quantitative Sensory Testing
Temporal Summation
The temporal summation scores did not differ between groups at either the control site (CP: 1 (IQR, 1–2); Healthy: 1 (IQR, 1–1); P = 0.78) or the pancreatic site (CP: 2 (IQR, 1–2); Healthy: 1 (IQR, 1–1.25); P = 0.31).
Pressure Stimulation
Overall, patients with CP detected pain at lower mechanical pressure intensity compared to healthy controls (P < 0.001). This was significant across all five dermatomes (all P ≤ 0.017) (Figure 2A). Likewise, patients with CP had lower overall pain tolerance thresholds during the pressure stimulations (P < 0.001). Again, this difference was significant between groups when comparing examination sites individually (all P ≤ 0.009) (Figure 2B).
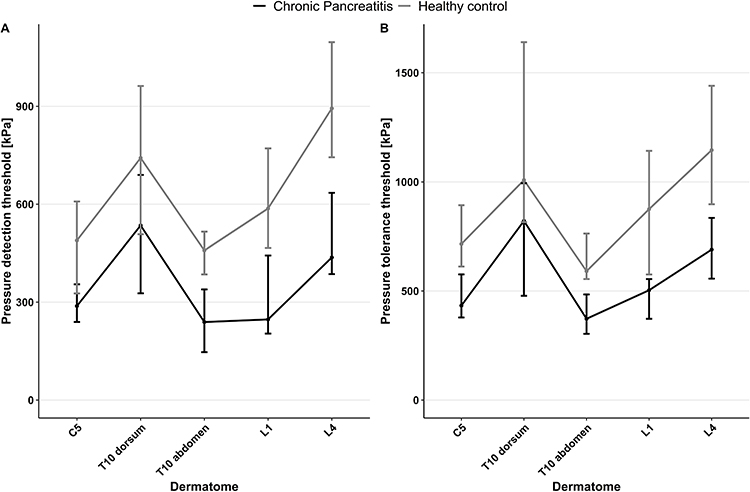 |
Figure 2 (A) Median pain detection thresholds in patients with chronic pancreatitis (n = 17) and healthy controls (n = 20), Whiskers mark interquartile range, (B) Median pain tolerance thresholds in patients with chronic pancreatitis (n = 17) and healthy controls (n = 20), Whiskers mark interquartile range. |
Cold Pressor Test and Conditioned Pain Modulation
During the cold pressor test, patients with CP reported overall higher VAS scores than healthy controls (P=0.03). The post-hoc analysis confirmed this was significant at all time points from 50 to 180 seconds except at 150 and 160 seconds (Figure 3A). Patients with CP had lower endurance time than healthy controls (CP: 120 seconds (IQR, 50–180); Healthy: 180 seconds (IQR, 180–180); P < 0.001) (Figure 3B). There were no differences in the conditioned pain modulation, which was 10% (IQR, 0–30%) in patients and 7.5% (IQR, 3.4–15%) in controls. In patients with CP, the median pPTT was 704 kPa (IQR, 449–945 kPa) before the cold pressor test and 772 kPa (IQR, 561–862 kPa) afterward. In healthy controls, median pPTT before the conditioning stimulus was 1045 kPa (IQR, 761–1427 kPa) and increased to 1159 kPa (IQR, 773–1615 kPa) afterward.
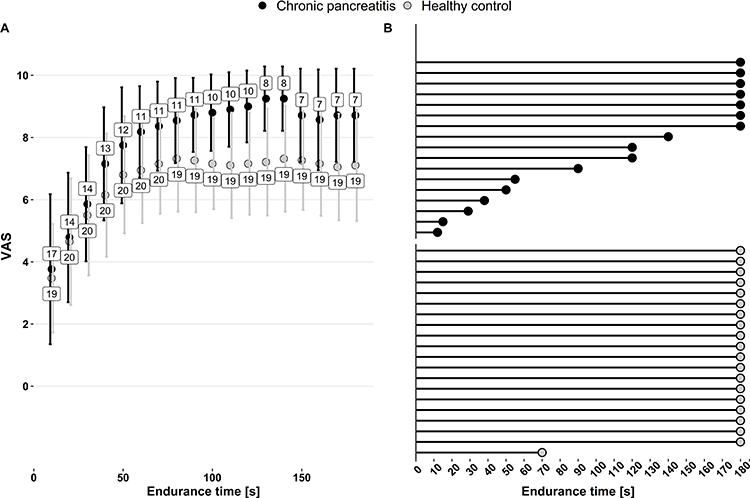 |
Figure 3 (A) Self-reported pain during cold pressor test in chronic pancreatitis patients (n = 17) and healthy controls (n = 20), VAS = visual analogue scale, (B) Coldpressor endurance time in chronic pancreatitis patients (n = 17) and healthy controls (n = 20). |
Nociceptive Withdrawal Reflex
The reflex threshold for eliciting NWR was lower in patients with CP compared to healthy controls (CP: 14 mA (IQR, 9.3–20); Healthy: 23 mA (IQR, 18.8–27.3); P = 0.02) (Figure 4A). The median number of reflexes elicited during stimulation per subject did not differ between groups (CP: 9 (IQR, 0–15.3); Healthy: 13 (IQR, 1–16.5); P = 0.54). The AUC of the EMG per subject was higher in CP patients compared to healthy controls, indicating spinal hyperexcitability (CP: 16.4 (IQR, 11.9–30.5); Healthy: 9.7 (IQR, 4.5–20.7); P = 0.045) (Figure 4B). The EMG latency per subject did not differ between groups (CP: 46.2 milliseconds (IQR, 0–80); Healthy: 60.8 milliseconds (IQR, 5.5–74.5); P = 0.72).
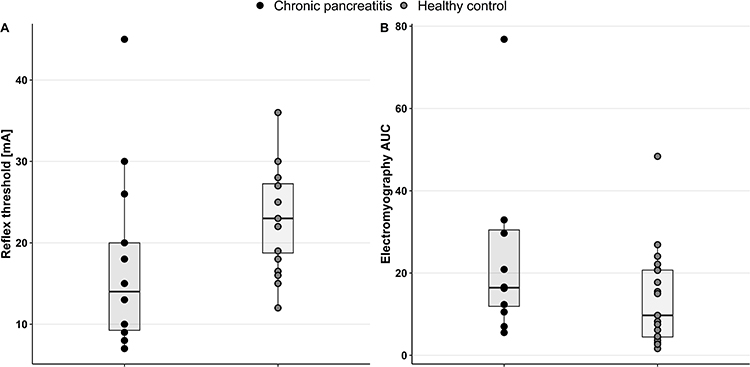 |
Figure 4 (A) Boxplot of reflex thresholds measured in mA during the nociceptive withdrawal reflex in patients with chronic pancreatitis (n = 14) and healthy controls (n = 20), (B) Boxplot of reflex AUC per subject measured using electromyography during elicitation of the nociceptive withdrawal reflex in patients with chronic pancreatitis (n = 12) and healthy controls (n = 19). Abbreviation: AUC, area under the curve. |
Evoked Brain Potentials
When comparing EEG recorded during NWR, we found no difference between groups on either peak-to-peak or individual peak amplitude and latency (Supplementary Figure 1A–C).
Correlation Between Quantitative Sensory Testing and Neurophysiological Measures
We found a positive correlation between reflex thresholds and cold pressor endurance time (ρ =0.71, P = 0.004) (Figure 5A). Furthermore, 6 out of the 7 CP patients who were unable to complete the cold pressor test had the lowest reflex threshold values within the complete CP cohort (Figure 5B). We also correlated other QST and clinical measures to NWR findings and found a positive correlation between reflex thresholds and Brief Pain Inventory pain severity score (ρ =0.70, P = 0.02), as well as disease duration (ρ = 0.61, P = 0.02) in CP patients (Table 2).
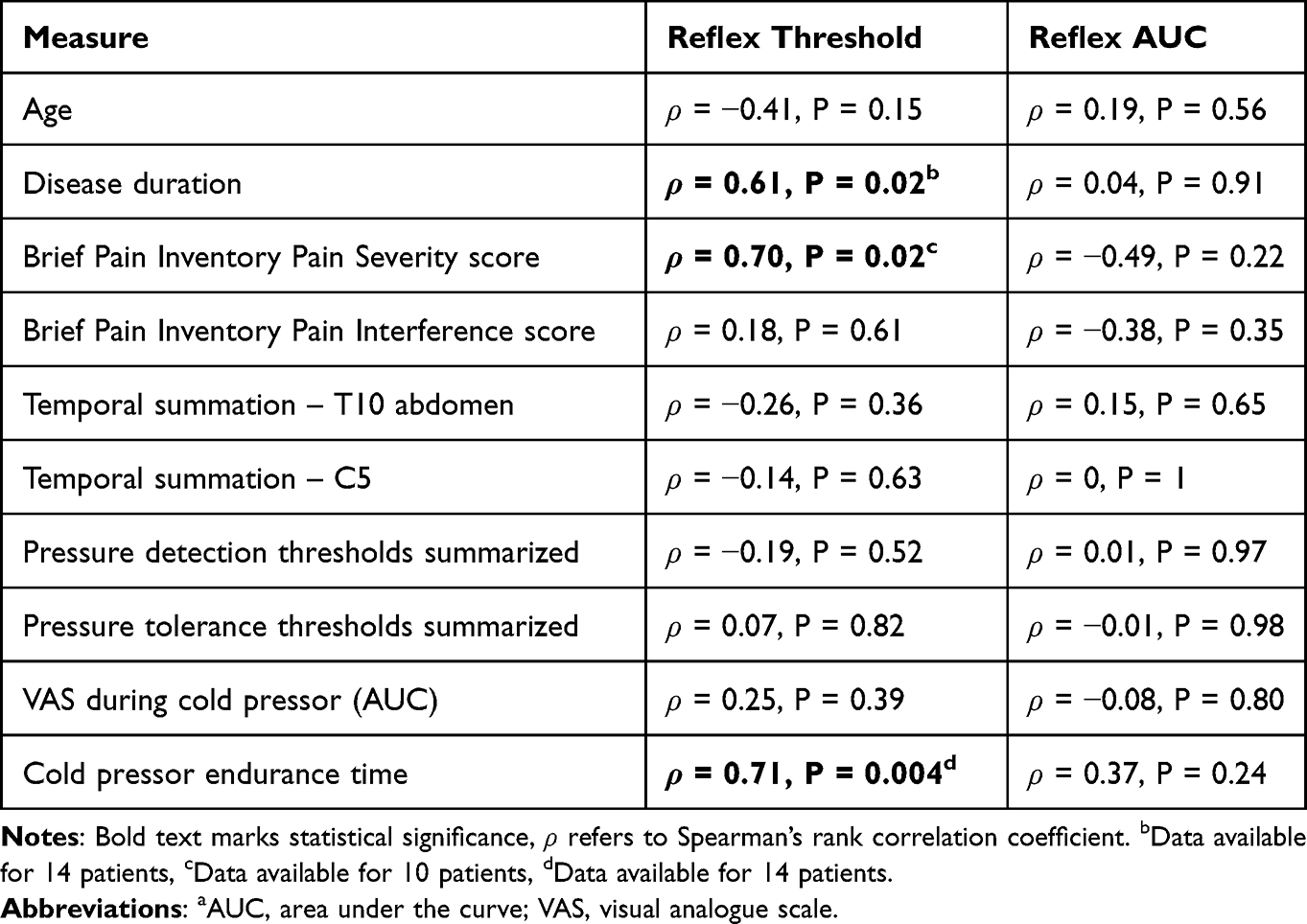 |
Table 2 Correlations Between Nociceptive Withdrawal Reflex Findings (Reflex Threshold, Reflex Area Under the Curve), Clinical Characteristics and Quantitative Sensory Testing Measures in Patients with Painful CPa |
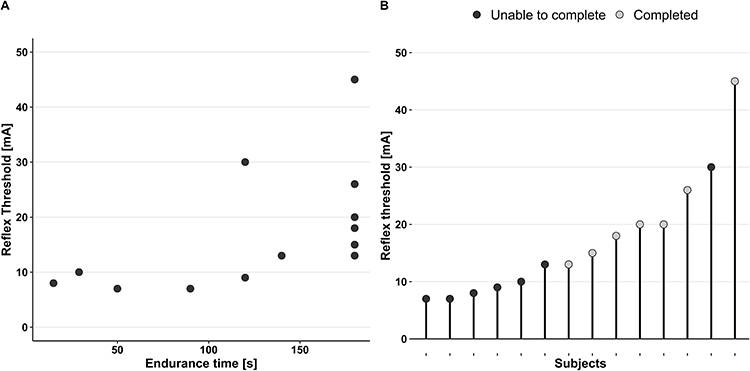 |
Figure 5 (A) Scatterplot of reflex thresholds and cold pressor endurance time in patients with painful chronic pancreatitis (n=14), (B) Reflex thresholds in patients with painful chronic pancreatitis colored according to whether they were able to endure the cold pressor test for 180 seconds (n=7) or less (n=7). |
Opioid Stratification
Because it is well-known that opioid treatment affects experimental pain testing, we chose to stratify patients according to whether they were on permanent opioid treatment or not at the time of testing. We conducted this analysis for all measures separating CP patients and healthy controls. However, we found no differences between patient groups in pressure pain detection or tolerance thresholds, subjective sensation of pain or endurance time during cold pressor tests, or reflex thresholds or sizes during the NWR.
Discussion
This study demonstrated hyperalgesia to pressure and tonic exposure to cold temperatures in patients with painful CP compared with healthy controls. Patients with CP also had lower reflex thresholds and higher EMG activity, indicating predominantly spinal hyperexcitability. We found a positive correlation between reflex thresholds and cold pressor endurance, indicating that spinal hyperexcitability is related to clinical pain.
Quantitative Sensory Testing
Overall, patients with CP in this study exhibited hyperalgesia during QST, keeping with previous findings.11,34,35 Nonetheless, it seems most patients did not have hyperalgesia to dynamic testing (conditioning pain modulation and temporal summation). This might be due to the reliability of these measures, since our previous study on CP patients found high variability and low reproducibility of conditioned pain modulation compared to static measures such as pain thresholds.36 We found no significant differences in temporal summation between groups, in contrast to previous findings of increased temporal summation in patients with CP.37 Temporal summation has mainly been used to characterize hyperalgesia as part of QST-regimens13,36 and might be less sensitive as a stand-alone measure. The method used for the evaluation of temporal summation in this study was also different than what has been used in previous studies of CP patients, limiting direct comparisons. Previous findings that not all patients with painful CP have evidence of generalized hyperalgesia may also partly explain this.38
The Nociceptive Reflex
Lower reflex thresholds using NWR have been found in patients with, eg, headache, musculoskeletal pain, whiplash, and fibromyalgia.19–22 Furthermore, we have shown that treatment with venlafaxine and tapentadol decreased the reflex activity in healthy controls.28,39 Together, these findings indicate that both pain and analgesics may alter the thresholds for eliciting the NWR. In this context, we found no difference in reflex thresholds between patients stratified according to whether they were on permanent opioid treatment or not, which may be a type II error. We found a positive correlation between the NWR threshold and cold pressor endurance time, in agreement with previous findings that tonic pain during the cold pressor test offers a valid experimental model for subjective pain assessment.40 The NWR works at a lower spinal level than the location of the pancreas. Still, previous studies show that visceral afferents terminate diffusively and with little spatial discrimination at the spinal level.41 Thus, the NWR may still represent segmental central pain processes in painful CP. A positive correlation between the NWR threshold and cold pressor endurance time also speaks to the feasibility of QST using the cold pressor test as a bedside evaluation of complex neuronal processing in patients with painful CP. We found a positive correlation between reflex thresholds and self-reported pain severity and disease duration, which seems counterintuitive. However, co-morbidity and co-medication can modulate the reflex threshold and influence our findings.42 Furthermore, as subjective pain intensity is determined by supraspinal networks and complex psychological mechanisms, it is not directly associated with spinal hyperexcitability.
Clinical Implications
Spinal hyperexcitability in patients with painful CP is in keeping with the suboptimal pain relief with current therapies and further supports the use of alternative management strategies.1,43 In this context, pregabalin reduces pain in patients with CP compared to placebo – possibly through subcortical mechanisms.44,45 Tapentadol and venlafaxine also affect the NWR, whereas oxycodone does not,28,39 supporting the use of serotonin and norepinephrine reuptake inhibitors in patients with painful CP.46 Of that note, non-opioid analgesics are recommended over opioid treatment in guidelines for pain management of CP.47 Patients with painful CP are most likely a very heterogenous group, and pancreatic pain is often multifactorial. Hence, we would expect patients within this group to vary substantially in pain processing mechanisms and therapy responses. Quantification of the NWR or QST may be used to predict which patients respond to different therapies and thus individualize treatment. This notion is supported by our previous finding where QST predicted response to pregabalin treatment in patients with painful CP.15 This is an essential field for future research on new treatment modalities and personalization of treatment for these patients. By individualizing treatment according to central neuronal changes in CP patients, we may improve the effectiveness of pain management while avoiding adverse effects associated with ineffective management strategies.48
Limitations
Patients in this study were highly selected from the heterogeneous group of individuals with CP and may represent those with a higher disease burden as they were originally selected for a drug trial. In this regard, there are several potential confounders for the neurophysiological testing (eg, NWR) including diabetes and analgesics that may influence our results such as recently shown by our group.28,49,50 We did, however, take this partly into account since we stratified for opioid use in our analysis. Due to the relatively small sample size, the validity of the correlation analyses may be limited, and there was an overall increased risk of type 2 errors. As the examinations involved detailed investigations of nociceptive processes and subjective pain, they were comprehensive. Hence, some patients could not complete all evaluations, resulting in missing data that could also have influenced the results. Nevertheless, the tendency in our study was clear, and it is unlikely that more patients would have changed the overall findings.
Conclusion
We showed that hyperalgesia in patients with painful CP might be related to changes in central pain processing, predominantly at the spinal level. Furthermore, we showed that QST provides a feasible bedside tool for evaluating the magnitude of these changes, potentially allowing clinicians to personalize treatment. This may improve outcomes and quality of life for patients with painful CP.
Data Sharing Statement
No further data will be shared.
Acknowledgments
The study was supported by “INPAIN, Aalborg University Hospital” and The NovoNordisk Foundation, grant#NNF19OC0057331.
Disclosure
Dr Rasmus Bach Nedergaard reports grants from Grünenthal GmbH, grants from The Danish Cancer Society, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Olesen SS, Poulsen JL, Drewes AM, et al. The Scandinavian Baltic Pancreatic Club (SBPC) database: design, rationale and characterisation of the study cohort. Scand J Gastroenterol. 2017;52(8):909–915. doi:10.1080/00365521.2017.1322138
2. Wilcox CM, Yadav D, Ye T, et al. Chronic pancreatitis pain pattern and severity are independent of abdominal imaging findings. Clin Gastroenterol Hepatol. 2015;13(3):552–560. doi:10.1016/j.cgh.2014.10.015
3. Olesen SS, Poulsen JL, Broberg MCH, Madzak A, Drewes AM. Opioid treatment and hypoalbuminemia are associated with increased hospitalisation rates in chronic pancreatitis outpatients. Pancreatology. 2016;16(5):807–813. doi:10.1016/j.pan.2016.06.004
4. Ceyhan GO, Bergmann F, Kadihasanoglu M, et al. Pancreatic neuropathy and neuropathic pain-a comprehensive pathomorphological study of 546 cases. Gastroenterology. 2009;136(1):177–186.e1. doi:10.1053/j.gastro.2008.09.029
5. Muthulingam JA, Hansen TM, Olesen SS, Drewes AM, Frøkjær JB. Altered brain morphology in chronic pancreatitis patients and its association with pain and other disease characteristics. Eur J Gastroenterol Hepatol. 2019;31(9):1092–1098. doi:10.1097/MEG.0000000000001470
6. Lelic D, Olesen SS, Hansen TM, Valeriani M, Drewes AM. Functional reorganization of brain networks in patients with painful chronic pancreatitis. Eur J Pain. 2014;18(7):968–977.
7. Olesen SS, Hansen TM, Graversen C, Valeriani M, Drewes AM. Cerebral excitability is abnormal in patients with painful chronic pancreatitis. Eur J Pain. 2013;17(1):46–54.
8. Frøkjær JB, Bouwense SAW, Olesen SS, et al. Reduced cortical thickness of brain areas involved in pain processing in patients with chronic pancreatitis. Clin Gastroenterol Hepatol. 2012;10(4):434–438.e1. doi:10.1016/j.cgh.2011.11.024
9. Olesen SS, Frøkjær JB, Lelic D, Valeriani M, Drewes AM. Pain-associated adaptive cortical reorganisation in chronic pancreatitis. Pancreatology. 2011;10(6):742–751. doi:10.1159/000321644
10. Dimcevski G, Sami SAK, Funch-Jensen P, et al. Pain in chronic pancreatitis: the role of reorganization in the central nervous system. Gastroenterology. 2007;132(4):1546–1556. doi:10.1053/j.gastro.2007.01.037
11. Olesen SS, Kuhlmann L, Novovic S, et al. Association of multiple patient and disease characteristics with the presence and type of pain in chronic pancreatitis. J Gastroenterol Hepatol. 2020;35(2):326–333. doi:10.1111/jgh.14783
12. Olesen SS, Juel J, Nielsen AK, Frøkjær JB, Wilder-Smith OHG, Drewes AM. Pain severity reduces life quality in chronic pancreatitis: implications for design of future outcome trials. Pancreatology. 2014;14(6):497–502. doi:10.1016/j.pan.2014.09.009
13. Phillips AE, Faghih M, Kuhlmann L, et al. A clinically feasible method for the assessment and characterization of pain in patients with chronic pancreatitis: pain phenotyping in chronic pancreatitis. Pancreatology. 2020;20(1):25–34. doi:10.1016/j.pan.2019.11.007
14. Phillips AE, Faghih M, Singh VK, et al. Rationale for and development of the pancreatic quantitative sensory testing consortium to study pain in chronic pancreatitis. Pancreas. 2021;50(9):1298–1304. doi:10.1097/MPA.0000000000001912
15. Olesen SS, Graversen C, Bouwense SAW, van Goor H, Wilder-Smith OHG, Drewes AM. Quantitative sensory testing predicts pregabalin efficacy in painful chronic pancreatitis. PLoS One. 2013;8(3):1–9. doi:10.1371/journal.pone.0057963
16. Kuhlmann L, Olesen SS, Olesen AE, Arendt-Nielsen L, Drewes AM. Mechanism-based pain management in chronic pancreatitis–is it time for a paradigm shift? Expert Rev Clin Pharmacol. 2019;12(3):249–258. doi:10.1080/17512433.2019.1571409
17. Sandrini G, Serrao M, Rossi P, Romaniello A, Cruccu G, Willer JC. The lower limb flexion reflex in humans. Prog Neurobiol. 2005;77(6):353–395. doi:10.1016/j.pneurobio.2005.11.003
18. Andersen OK. Studies of the organization of the human nociceptive withdrawal reflex: focus on sensory convergence and stimulation site dependency. Acta Physiol. 2007;189(SUPPL. 654):1–35. doi:10.1111/j.1748-1716.2007.01706.x
19. Banic B, Petersen-Felix S, Andersen OK, et al. Evidence for spinal cord hypersensitivity in chronic pain after whiplash injury and in fibromyalgia. Pain. 2004;107(1–2):7–15. doi:10.1016/j.pain.2003.05.001
20. Biurrun Manresa JA, Neziri AY, Curatolo M, Arendt-Nielsen L, Andersen OK. Reflex receptive fields are enlarged in patients with musculoskeletal low back and neck pain. Pain. 2013;154(8):1318–1324. doi:10.1016/j.pain.2013.04.013
21. Filatova E, Latysheva N, Kurenkov A. Evidence of persistent central sensitization in chronic headaches: a multi-method study. J Headache Pain. 2008;9(5):295–300. doi:10.1007/s10194-008-0061-7
22. Lim ECW, Sterling M, Pedler A, Coombes BK, Vicenzino B. Evidence of spinal cord hyperexcitability as measured with nociceptive flexion reflex (NFR) threshold in chronic lateral epicondylalgia with or without a positive neurodynamic test. J Pain. 2012;13(7):676–684. doi:10.1016/j.jpain.2012.04.005
23. Juel J, Olesen SS, Olesen AE, et al. Study protocol for a randomised, double-blinded, placebo-controlled, clinical trial of S-ketamine for pain treatment in patients with chronic pancreatitis (RESET trial). BMJ Open. 2015;5(3):1–7. doi:10.1136/bmjopen-2014-007087
24. Layer P, Yamamoto H, Kalthoff L, Clain JE, Bakken LJ, Dimagno EP. The different courses of early- and late-onset idiopathic and alcoholic chronic pancreatitis. Gastroenterology. 1994;107(5):1481–1487. doi:10.1016/0016-5085(94)90553-3
25. Mendoza T, Mayne T, Rublee D, Cleeland C. Reliability and validity of a modified Brief Pain Inventory short form in patients with osteoarthritis. Eur J Pain. 2006;10(4):353–361. doi:10.1016/j.ejpain.2005.06.002
26. Arendt-Nielsen L, Morlion B, Perrot S, et al. Assessment and manifestation of central sensitisation across different chronic pain conditions. Eur J Pain. 2018;22(2):216–241.
27. Kuhlmann L, Olesen SS, Grønlund D, et al. Patient and disease characteristics associate with sensory testing results in chronic pancreatitis. Clin J Pain. 2019;35(9):786–793. doi:10.1097/AJP.0000000000000740
28. Nedergaard RB, Hansen TM, Mørch CD, Niesters M, Dahan A, Drewes AM. Influence of tapentadol and oxycodone on the spinal cord and brain using electrophysiology - a randomized, placebo-controlled trial. Br J Clin Pharmacol. 2022;20:1–10.
29. Jensen MB, Biurrun Manresa J, Andersen OK. Reliable estimation of nociceptive withdrawal reflex thresholds. J Neurosci Methods. 2015;253:110–115. doi:10.1016/j.jneumeth.2015.06.014
30. Rhudy JL, France CR. Defining the nociceptive flexion reflex (NFR) threshold in human participants: a comparison of different scoring criteria. Pain. 2007;128(3):244–253. doi:10.1016/j.pain.2006.09.024
31. France CR, Rhudy JL, McGlone S. Using normalized EMG to define the nociceptive flexion reflex (NFR) threshold: further evaluation of standardized NFR scoring criteria. Pain. 2009;145(1–2):211–218. doi:10.1016/j.pain.2009.06.022
32. Herm C, Silbereisen V, Graf BM, Lassen CL. Long term reliability of nociceptive withdrawal reflex thresholds. J Neurosci Methods. 2019;320:44–49. doi:10.1016/j.jneumeth.2019.03.009
33. Pion-Tonachini L, Kreutz-Delgado K, Makeig S. ICLabel: an automated electroencephalographic independent component classifier, dataset, and website. Neuroimage. 2019;198:181–197. doi:10.1016/j.neuroimage.2019.05.026
34. Buscher HC, Wilder-Smith OHG, Van Goor H. Chronic pancreatitis patients show hyperalgesia of central origin: a pilot study. Eur J Pain. 2006;10(4):363. doi:10.1016/j.ejpain.2005.06.006
35. Bouwense SAW, Olesen SS, Drewes AM, Frøkjær JB, van Goor H, Wilder-Smith OHG. Is altered central pain processing related to disease stage in chronic pancreatitis patients with pain? An exploratory study. PLoS One. 2013;8(2):e55460. doi:10.1371/journal.pone.0055460
36. Olesen SS, Van Goor H, Bouwense SAW, Wilder-Smith OHG, Drewes AM. Reliability of static and dynamic quantitative sensory testing in patients with painful chronic pancreatitis. Reg Anesth Pain Med. 2012;37(5):530–536. doi:10.1097/AAP.0b013e3182632c40
37. Dimcevski G, Staahl C, Andersen SD, et al. Assessment of experimental pain from skin, muscle, and esophagus in patients with chronic pancreatitis. Pancreas. 2007;35(1):22–29. doi:10.1097/mpa.0b013e31805c1762
38. Faghih M, Phillips AE, Kuhlmann L, et al. Pancreatic QST differentiates chronic pancreatitis patients into distinct pain phenotypes independent of psychiatric comorbidities. Clin Gastroenterol Hepatol. 2022;20(1):153–161.e2. doi:10.1016/j.cgh.2020.10.036
39. Lelic D, Fischer IWD, Olesen AE, et al. Venlafaxine and oxycodone effects on human spinal and supraspinal pain processing: a randomized cross-over trial. Eur J Neurosci. 2016;44(11):2966–2974. doi:10.1111/ejn.13443
40. Gram M, Graversen C, Olesen SS, Drewes AM. Dynamic spectral indices of the electroencephalogram provide new insights into tonic pain. Clin Neurophysiol. 2015;126(4):763–771. doi:10.1016/j.clinph.2014.07.027
41. Drewes AM, Olesen AE, Farmer AD, Szigethy E, Rebours V, Olesen SS. Gastrointestinal pain. Nat Rev Dis Prim. 2020;6(1). doi:10.1038/s41572-019-0135-7
42. Skljarevski V, Ramadan NM. The nociceptive flexion reflex in humans - review article. Pain. 2002;96(1–2):3–8. doi:10.1016/S0304-3959(02)00018-0
43. Drewes AM, Kempeneers MA, Andersen DK, et al. Controversies on the endoscopic and surgical management of pain in patients with chronic pancreatitis: pros and cons! Gut. 2019;68(8):1343–1351.
44. Olesen SS, Graversen C, Olesen AE, et al. Randomised clinical trial: pregabalin attenuates experimental visceral pain through sub-cortical mechanisms in patients with painful chronic pancreatitis. Aliment Pharmacol Ther. 2011;34(8):878–887. doi:10.1111/j.1365-2036.2011.04802.x
45. Olesen SS, Bouwense SAW, Wildersmith OHG, Van Goor H, Drewes AM. Pregabalin reduces pain in patients with chronic pancreatitis in a randomized, controlled trial. Gastroenterology. 2011;141(2):536–543. doi:10.1053/j.gastro.2011.04.003
46. Kothari D, Ketwaroo G, Kee WS, Anderson AJ, Kothari D, Tarca AJ. Building a quality practice in chronic pancreatitis. Cardiology in the Young. 2023;1–4. doi:10.1017/S1047951123001105
47. Gardner TB, Adler DG, Forsmark CE, Sauer BG, Taylor JR, Whitcomb DC. ACG clinical guideline: chronic pancreatitis. Am J Gastroenterol. 2020;115(3):322–339. doi:10.14309/ajg.0000000000000535
48. Drewes AM, Bouwense SAW, Campbell CM, et al. Guidelines for the understanding and management of pain in chronic pancreatitis. Pancreatology. 2017;17(5):720–731. doi:10.1016/j.pan.2017.07.006
49. Lelic D, Valeriani M, Fischer IWD, Dahan A, Drewes AM. Venlafaxine and oxycodone have different effects on spinal and supraspinal activity in man: a somatosensory evoked potential study. Br J Clin Pharmacol. 2017;83(4):764–776. doi:10.1111/bcp.13177
50. Fischer IW, Gram M, Hansen TM, et al. Cortical and spinal assessment - a comparative study using encephalography and the nociceptive withdrawal reflex. J Pharmacol Toxicol Methods. 2017;84:37–43. doi:10.1016/j.vascn.2016.10.008
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Antioxidant Therapy Reverses Sound Stress-Induced Opioid Resistance in a Mouse Model of Mechanical Allodynia
Kasai S, Furuta A, Kuroda J, Takagi M, Sawai T, Yamada D, Saitoh A, Yoshizawa K
Journal of Pain Research 2026, 19:550094
Published Date: 25 June 2026