Back to Journals » Journal of Asthma and Allergy » Volume 16
Specific IgE Response and Omalizumab Responsiveness in Severe Allergic Asthma
Authors Tajiri T ![]() , Suzuki M, Kutsuna T, Nishiyama H, Ito K
, Suzuki M, Kutsuna T, Nishiyama H, Ito K ![]() , Takeda N, Fukumitsu K, Kanemitsu Y
, Takeda N, Fukumitsu K, Kanemitsu Y ![]() , Fukuda S, Umemura T, Ohkubo H, Maeno K, Ito Y
, Fukuda S, Umemura T, Ohkubo H, Maeno K, Ito Y ![]() , Oguri T, Takemura M, Yoshikawa K, Niimi A
, Oguri T, Takemura M, Yoshikawa K, Niimi A ![]()
Received 16 October 2022
Accepted for publication 4 January 2023
Published 22 January 2023 Volume 2023:16 Pages 149—157
DOI https://doi.org/10.2147/JAA.S393683
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Tomoko Tajiri,1 Motohiko Suzuki,2,3 Takeo Kutsuna,4 Hirono Nishiyama,1 Keima Ito,1 Norihisa Takeda,1 Kensuke Fukumitsu,1 Yoshihiro Kanemitsu,1 Satoshi Fukuda,1 Takehiro Umemura,1 Hirotsugu Ohkubo,1 Ken Maeno,1 Yutaka Ito,1 Tetsuya Oguri,1 Masaya Takemura,1 Kosho Yoshikawa,4 Akio Niimi1
1Department of Respiratory Medicine, Allergy and Clinical Immunology, Graduate School of Medical Sciences, Nagoya City University, Nagoya, Aichi, Japan; 2Department of Otorhinolaryngology, Graduate School of Medical Sciences, Nagoya City University, Nagoya, Aichi, Japan; 3Department of Otorhinolaryngology, Nagoya City East Medical Center, Nagoya, Aichi, Japan; 4Department of Respiratory Medicine, Daido Hospital, Nagoya, Aichi, Japan
Correspondence: Tomoko Tajiri, Department of Respiratory Medicine, Allergy and Clinical Immunology, Graduate School of Medical Sciences, Nagoya City University, 1 Kawasumi, Mizuho-cho, Mizuho-ku, Nagoya, Aichi, 467-8601, Japan, Tel +81-52-853-8216, Email [email protected]
Objective: Omalizumab has demonstrated clinical efficacy in patients with severe allergic asthma sensitized to perennial allergens and/or severe pollinosis through inhibition of IgE-dependent allergic response. When considering the “one airway, one disease” concept, sensitization to pollen could predict responsiveness to omalizumab. This study aimed to assess whether the pretreatment specific IgE response could be a predictor of responsiveness to omalizumab in severe allergic asthma sensitized to perennial allergens.
Methods: In this retrospective study, 41 adult patients with severe allergic asthma sensitized to perennial allergens (27 females; mean age 59 years) who had completed 52-week omalizumab treatment were enrolled. The Global Evaluation of Treatment Effectiveness was performed, and demographic characteristics and the positive ratios of specific IgE responses classified into five subgroups (pollen, dust mite, house dust, mold, and animal dander) were compared between responders and non-responders. Multivariate logistic regression analyses were performed to identify predictors of responsiveness to omalizumab.
Results: Thirty-one patients (76%) were identified as responders. The number of sensitized aeroallergen subgroups and sensitization to pollens were significantly higher in responders than in non-responders (both p< 0.05). Multivariate logistic regression analysis showed that sensitization to pollen (OR = 8.41, p = 0.02) was independently associated with the effectiveness of omalizumab.
Conclusion: Pretreatment serum pollen-specific IgE could be a predictor of responsiveness to omalizumab.
Keywords: omalizumab, antigen-specific IgE, pollen, allergic rhinitis, allergic asthma
Plain Language Summary
Given the existence of non-responders and the high cost of omalizumab, identifying predictors of responsiveness to omalizumab is needed. In this retrospective study, we showed that pretreatment sensitization to pollen could be a predictor of responsiveness to omalizumab in patients with severe allergic asthma sensitized to perennial allergens. This result would lead to more appropriate management of severe asthma.
Introduction
Asthma and allergic rhinitis often coexist and influence each other.1 Approximately 20% to 60% of patients with allergic rhinitis have asthma, whereas up to 70% of patients with asthma have allergic rhinitis.1–5 Allergic rhinitis is a risk factor for asthma onset.6,7 The presence of comorbid allergic rhinitis in asthmatic patients is related to worse asthma control8–10 and higher asthma severity.5 Treatment of allergic rhinitis with intranasal corticosteroids improves pulmonary function, airway hyperresponsiveness, asthma symptoms, and exacerbation frequency in patients with both asthma and allergic rhinitis.11 A pathophysiological, as well as a clinical, relationship between asthma and allergic rhinitis has also been reported. Nasal provocation with specific allergens increases lower airway eosinophilic inflammation12 and airway hyperresponsiveness to methacholine13 in asthmatic patients with allergic rhinitis. These interactions between asthma and allergic rhinitis have led to the concept of “one airway, one disease”.1,2 In both conditions, immunoglobulin (Ig) E plays a pivotal role.
Omalizumab, a humanized anti-IgE monoclonal antibody, has been demonstrated to be efficacious in patients with severe allergic asthma sensitized to perennial allergens and/or severe pollinosis (seasonal allergic rhinitis caused by pollens),14 especially in patients with severe Japanese cedar pollinosis.15–17 Omalizumab has a number of clinical effects by binding serum free IgE and inhibiting the interaction between IgE and its high-affinity receptors. In a meta-analysis of the real-world effectiveness of omalizumab, 82% of patients with severe asthma achieved a good or excellent Global Evaluation of Treatment Effectiveness (GETE) at 12 months.25 In other words, not all patients responded to omalizumab. Given the existence of non-responders, the high cost of omalizumab, and appropriate use of type 2-targeted biologics including omalizumab in patients who most benefit from them, identifying predictors of responsiveness to omalizumab should lead to more appropriate management. However, predictive factors, including type 2 biomarkers, have been reported inconsistently. Based on the inhibitory effect of omalizumab on IgE-dependent allergic responses in both allergic asthma and pollinosis and the “one airway, one disease” concept, we hypothesized that serum aeroallergen-specific IgE, especially pollen-specific IgE, is a predictor of responsiveness to omalizumab. However, few studies have reported it.
In this retrospective study, the response rate and predicted responsiveness to omalizumab treatment were assessed by focusing on sensitization to aeroallergens in adult patients with severe allergic asthma sensitized to perennial allergens. The response rate as assessed by GETE was examined; and other important indicators of the response rate were not evaluated in this study.
Materials and Methods
Study Design and Subjects
This was a retrospective study that enrolled adult patients with severe allergic asthma sensitized to perennial allergens with Global Initiative for Asthma (GINA) Step 5 severity, who were sensitized to at least one perennial aeroallergen and had completed 52-week omalizumab treatment at Nagoya City University Hospital and Daido Hospital, Nagoya, Japan between October 2009 and June 2021. All asthma patients were treated by pulmonologists in respiratory departments at these tertiary hospitals on the basis of the GINA guideline.18
Measurements
For all patients, demographic characteristics, severe asthma-related comorbidities (allergic rhinitis, chronic rhinosinusitis, and gastroesophageal reflux disease), asthma control test (ACT), asthma exacerbation that required at least three days of systemic corticosteroids, asthma treatment, fractional exhaled nitric oxide (FeNO) levels, pulmonary function (forced vital capacity, FEV1), and blood test (eosinophil proportion, serum total IgE, and serum aeroallergen-specific IgE (ImmunoCAP® total IgE and ImmunoCAP® specific IgE, Phadia K.K., Tokyo, Japan)) results before and 52 weeks after omalizumab administration were extracted by reviewing medical records. Patients with allergic rhinitis were diagnosed by an otolaryngologist (M.S.) or pulmonologists (T.T., T.K., Y.K., M.T., K.Y., and A.N.) according to the guideline.19 Pretreatment serum aeroallergen-specific IgEs were classified into the following five groups:20 house dust; dust mite (Dermatophagoides); mold (mixed molds [Penicillium, Cladosporium, Aspergillus, Candida, and Alternaria] and Trichophyton); animal dander (cat dander, dog dander); pollen (Japanese cedar, mixed grass (orchard grass, vernal grass, Bermuda grass and timothy grass), and mixed weed (ragweed, mugwort, oxeye daisy, dandelion and goldenrod)). Positivity of serum aeroallergen-specific IgE was defined as ≥0.35 UA/mL.21 In all patients, serum specific IgEs against house dust and house dust mite were tested. The major component of house dust is house dust mite, though it includes house dust mite, animal dander, and mold.
Demographic characteristics and other variables listed above were assessed at baseline. Response to omalizumab treatment was then assessed in all patients. Demographic characteristics and other variables, including the positive ratio of serum specific IgE of each subgroup, were next compared between responders and non-responders. Univariate and multivariate logistic regression analyses were finally performed to clarify the predictors of responsiveness to omalizumab. Treatment responsiveness to omalizumab was determined by physicians’ overall evaluation according to the GETE scale at 52 weeks.22 GETE is a five-point scale: excellent (complete control of asthma), good (marked improvement), moderate (discernible, but limited improvement), poor (no appreciable change), and worsening (overall deterioration of asthma control). Patients with an “excellent” or “good” response were defined as responders.
This study was approved by the Ethics Committee of Nagoya City University (60-20-0174). Written informed consent was waived by the ethics committee due to the retrospective nature of this study. Instead, an opt-out document was posted on the hospital website to offer patients the opportunity to refuse participation.
Statistical Analysis
JMP Pro14.0 (SAS institute, Inc., Tokyo, Japan) was used for all statistical analyses. To compare demographic characteristics of patients between two groups (responders and non-responders), the Chi-squared test or the Wilcoxon rank-sum test was used as appropriate. Multivariate logistic regression analysis was performed to identify predictors of responsiveness to omalizumab. Variables with p <0.10 on univariate analysis of pretreatment indices were included in the multivariate logistic regression analysis, and p <0.05 was considered significant.
Results
Demographic Characteristics of Subjects at Baseline
A total of 41 patients with severe allergic asthma sensitized to perennial allergens (27 females; median age 59 years (range 27−88 years, 19 patients ≥65 years); median serum total IgE 166 IU/mL) were analyzed (Table 1). All patients used high-dose inhaled corticosteroids (ICSs) and long-acting β2-agonists (LABAs). Thirty-four (83%) of 41 patients used leukotriene receptor antagonists, 22 (54%) used theophylline, 18 (44%) used long-acting muscarinic antagonists, and 14 (34%) used oral corticosteroids (OCSs). All patients had poorly controlled asthma (median ACT score: 16 (range 6−19)) despite GINA Step 5 treatment (Table 1). A total of 21 (51%) of 41 asthmatic patients were diagnosed with comorbid allergic rhinitis. Of these 21 patients, 14 were diagnosed with pollinosis, all of whom were sensitized to Japanese cedar pollen with or without other pollens.
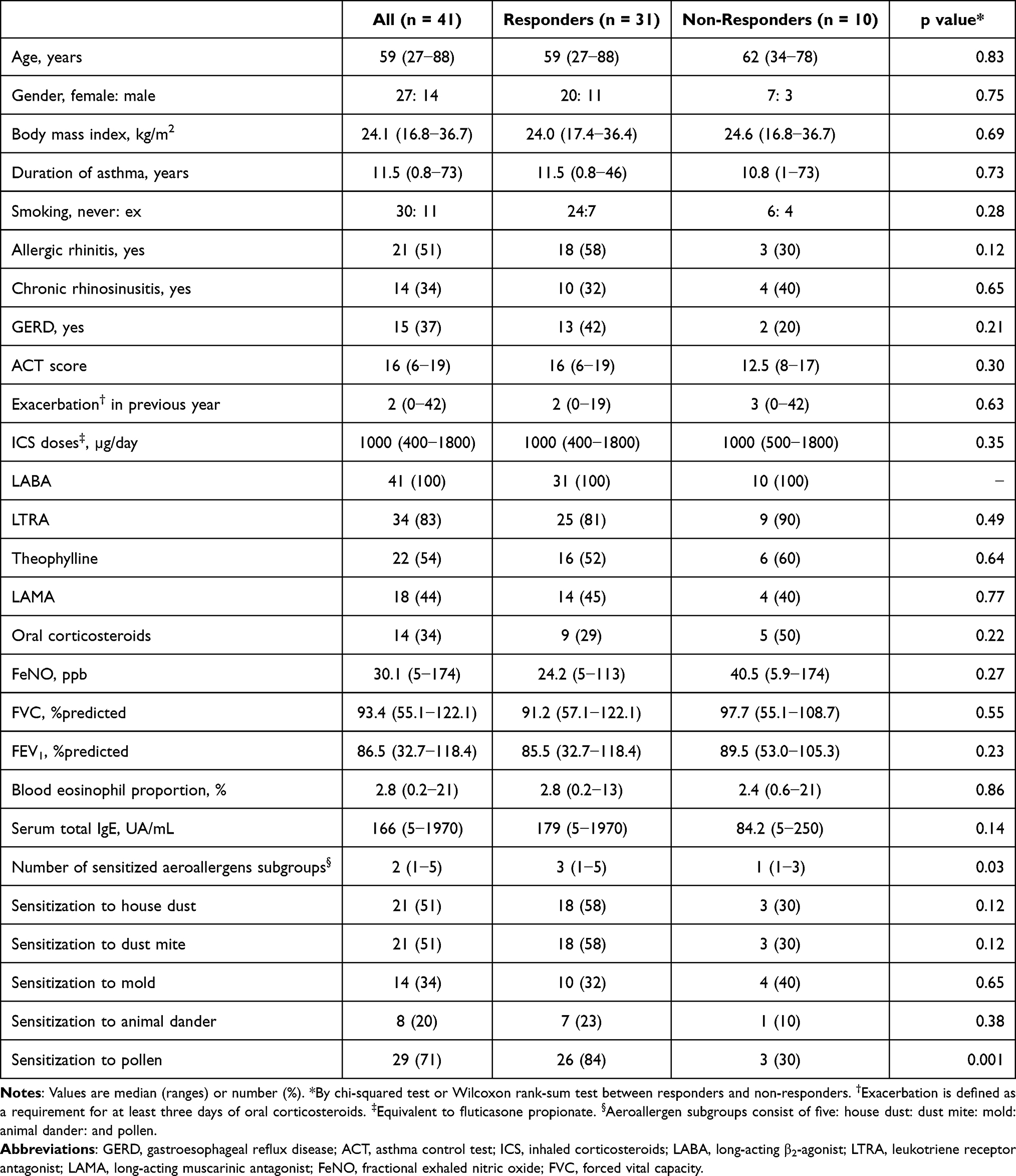 |
Table 1 Characteristics of Patients and Comparison of Responders with Non-Responders |
Regarding aeroallergen sensitization, all patients were sensitized to at least one perennial aeroallergen subgroup, and 24 (59%) patients were sensitized to two or more aeroallergen subgroups. The median number of sensitized aeroallergen subgroups was 2 (1−5). The positive ratio of serum aeroallergen-specific IgE of each subgroup was as follows: 29 (71%) patients were sensitized to pollen; 21 (51%) to house dust and dust mite; 14 (34%) to mold; and 8 (20%) to animal dander (Table 1). Of 29 patients with pollen sensitization, 28 were sensitized to Japanese cedar, 9 to mixed grass, and 6 to mixed weed.
Response Rate to Omalizumab
Based on the GETE scale, 31 (76%) of 41 patients were identified as responders after 52-week omalizumab treatment. All 31 responders had been identified as responders after 16 weeks. Of the 31 responders, nine and 22 patients achieved excellent and good GETE, respectively. Improvements in ACT, asthma exacerbation and airflow limitation were confirmed in responders. Of the 31 responders, 28 (90%) showed ≥3-point improvement in ACT scores from baseline to 52 weeks. Of the 16 responders who had asthma exacerbations in the previous 52 weeks, 14 (88%) showed a reduction in the asthma exacerbation rate from before to after 52 weeks. Of the 30 responders who had performed pulmonary function tests before and after treatment, 17 (57%) showed improvement in FEV1 (%predicted). All non-responders discontinued omalizumab after 52 weeks, and five of them switched to different biologics.
Regarding asthma medications, in seven (50%) of 14 patients with OCS-dependent asthma, OCS treatment was withdrawn at 52 weeks. In four (10%) of 41 patients, the ICS dose was stepped down at 52 weeks.
Comparisons of Demographic Characteristics and the Positive Ratio of Serum Aeroallergen-Specific IgE Between Responders and Non-Responders
The comparisons of demographic characteristics and other variables between responders and non-responders are shown in Table 1. There was no difference in the usage of concomitant asthma medications including leukotriene receptor antagonists, theophylline, long-acting muscarinic antagonists, and OCSs between responders and non-responders (p>0.10) (Table 1). The number of sensitized aeroallergen subgroups was significantly higher in responders than in non-responders (p = 0.03) (Table 1). The positive ratio of pretreatment pollen-specific IgE was significantly higher in responders than in non-responders (p = 0.001) (Table 1). No significant differences were observed in the positive ratio of dust mite, house dust, mold, and animal dander-specific IgEs between the two patients’ groups (all p>0.10). Regarding pollinosis, 13 of 14 patients with pollinosis responded to omalizumab treatment, whereas 5 of 12 patients with neither pollinosis nor pollen sensitization responded to omalizumab treatment (p = 0.004) (Figure 1). There were no significant differences in demographic characteristics, comorbidities, asthma control, asthma medication, type 2 biomarkers, and pulmonary functions between the two patients’ groups (all p>0.10) (Table 1).
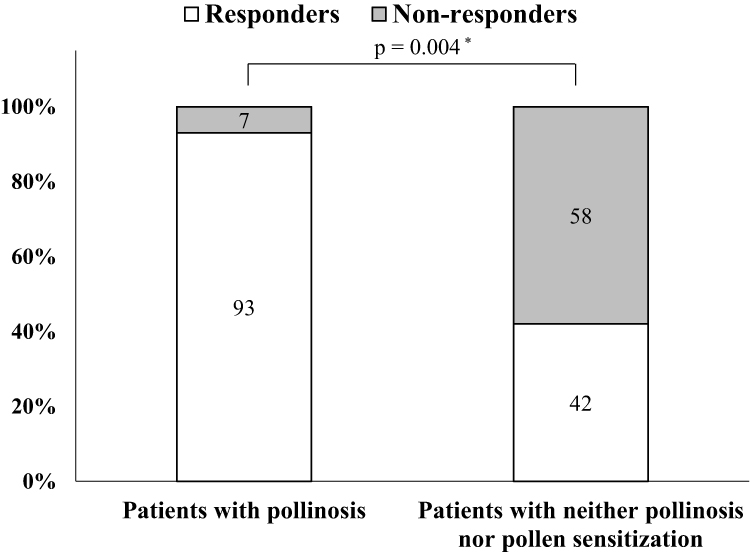 |
Figure 1 Comparison of omalizumab response rates between patients with pollinosis and patients with neither pollinosis nor pollen sensitization. *By the chi-squared test between patients with pollinosis and patients with neither pollinosis nor pollen sensitization. |
Predictors of Responsiveness to Omalizumab
To identify the predictors of responsiveness to omalizumab, univariate and multivariate logistic regression analyses were performed (Table 2). Multivariate logistic regression analysis of indices with p <0.10 on univariate analysis showed that sensitization to pollen (OR = 8.41, p = 0.02) was independently associated with the effectiveness of omalizumab treatment.
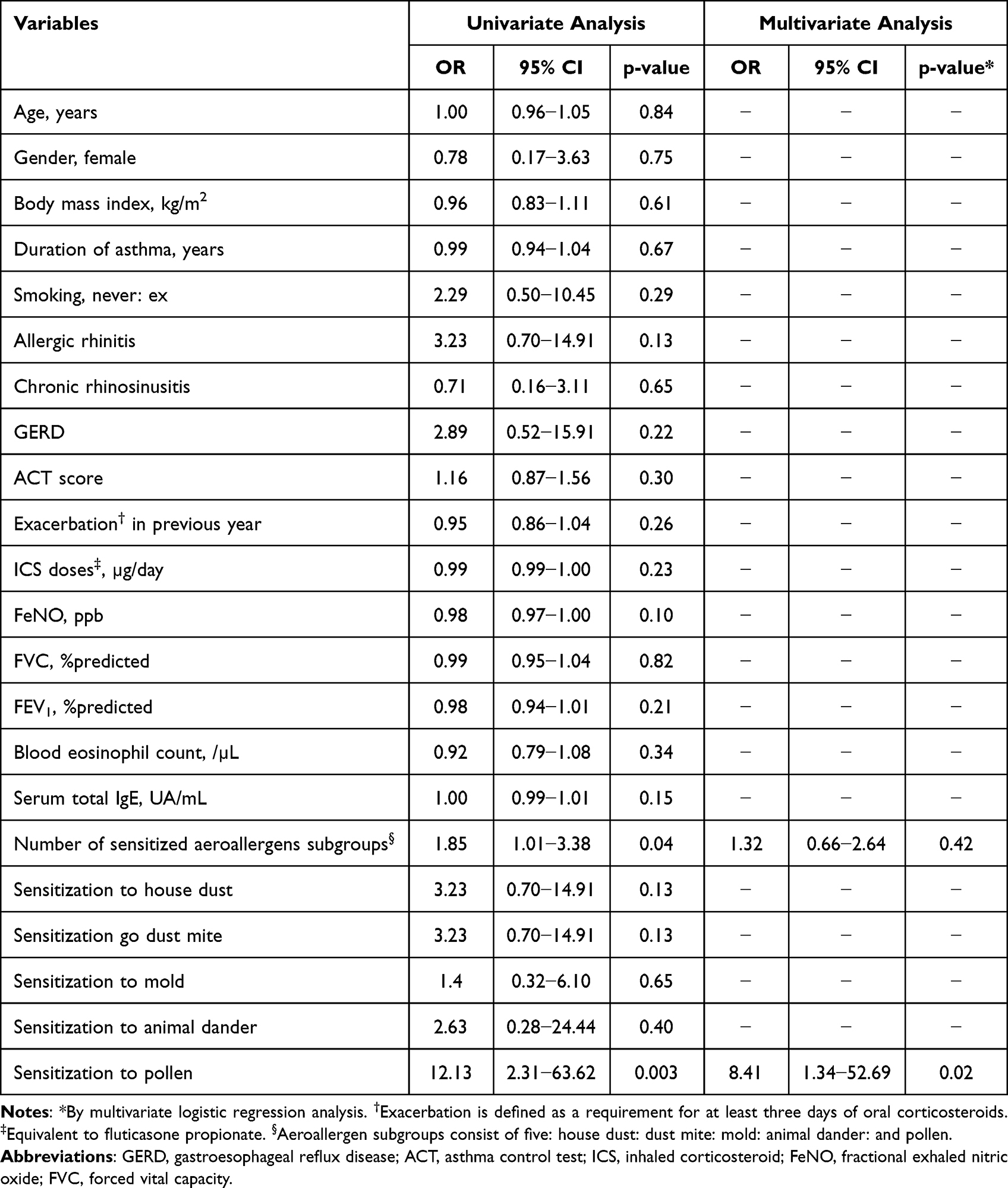 |
Table 2 OR and Associated 95% CIs for the Effectiveness of Omalizumab |
Discussion
In this study, it was shown that 1) 76% of patients with severe allergic asthma responded to 52-week omalizumab treatment; 2) 71% of patients were sensitized to pollen; and 3) sensitization to pollen was independently associated with the effectiveness of omalizumab treatment. Sensitization to pollen, especially Japanese cedar pollen, could be a predictor of responsiveness to omalizumab in patients with severe allergic asthma sensitized to perennial allergens.
Omalizumab, a humanized monoclonal anti-IgE antibody, has been approved for the treatment of severe allergic asthma patients sensitized to perennial allergens, chronic spontaneous urticaria, and severe seasonal allergic rhinitis, and it has been shown to significantly improve these conditions.14 Meta-analyses of randomized, controlled trials (RCTs)23,24 and real-world studies25,26 showed that omalizumab had several clinical effects in severe allergic asthma23,25,26 and in allergic rhinitis inadequately controlled with conventional treatment.24 The proportion of GETE responders after 12 months of omalizumab treatment in severe allergic asthma patients was 82% in the real-world meta-analysis of observational studies.26 Consistent with these analyses, the present study confirmed that 76% of patients with severe allergic asthma sensitized to perennial allergens responded to 52-week omalizumab treatment in the real-world setting.
As mentioned above, not all patients respond to omalizumab treatment. Given the existence of non-responders and the appropriate choice of type 2-targeted biologics, including omalizumab, mepolizumab, benralizumab, and dupilumab, identifying factors predictive of responsiveness is needed. So far, several studies reported factors predictive of omalizumab responsiveness. Initially, post hoc studies of RCTs suggested that the efficacy of omalizumab may be greater in patients with high type 2 biomarkers. The EXTRA omalizumab study reported that patients with higher levels of FeNO, blood eosinophils and serum periostin were more responsive to omalizumab treatment than those with lower levels in terms of the reduction in asthma exacerbations during the first year of treatment.14,27 We confirmed this previously, showing that higher FeNO levels were the best predictor of improvement in asthma control after 16 weeks of treatment and that higher serum periostin levels were the best predictor of reduction in severe asthma exacerbations after 1 year of treatment.14,28 Meanwhile, the STELLAIR study29 and the PROSPERO study30 recently showed that omalizumab was effective in patients with severe allergic asthma irrespective of pre-treatment type 2 biomarkers, including blood eosinophil29,30 or FeNO levels.30 In the present study, there were no significant differences in FeNO levels and blood eosinophils between the two patients’ groups. Type 2 biomarkers as predictors of responsiveness to omalizumab treatment remain controversial.
Omalizumab was originally approved for severe allergic asthma patients sensitized to at least one perennial allergen. Nonetheless, a previous study showed that omalizumab was also effective in severe asthma caused by seasonal allergens.31 A high prevalence of sensitization to seasonal allergens was observed in previous omalizumab studies.20,32 From 41.3% to 61.7% of severe asthmatic patients were sensitized to pollens.20,32 Pollens are major seasonal allergens and trigger the allergic cascade in both pollinosis and allergic asthma. When considering the efficacy of omalizumab through inhibition of IgE-dependent allergic responses in both pollinosis and allergic asthma, the high prevalence of sensitization to pollen in allergic asthma, and the “one airway, one disease” concept, sensitization to pollen could be assumed to be a predictor of responsiveness to omalizumab. So far, three studies33–35 have evaluated the association between type of aeroallergen sensitization and omalizumab responsiveness. A post hoc analysis of the INNOVATE study35 showed that patients with high values of D. pteronyssinus- or D. farinae-specific IgE, but with these making a relatively low contribution to total specific IgE load, appeared to achieve the most benefit from omalizumab; though not statistically significantly. This study assessed the levels of specific IgE against perennial allergens as predictive of responsiveness to omalizumab. Another post hoc analysis of longitudinal data33 showed that polysensitized patients who were sensitized to all perennial allergens (mites, molds, and pets) had a higher tendency to be responders than non-polysensitized patients. This study assessed the effect of sensitization to perennial allergens (including mites, molds, and pets), but not seasonal allergens on the responsiveness to omalizumab. Another post hoc analysis of a real-world study34 evaluated the effects of number and type of allergen sensitizations (non-sensitized, seasonal, perennial, or both) on omalizumab response. This study showed that response to omalizumab evaluated by exacerbation rates, lung function, and quality of life was not different, regardless of the number and type of allergen sensitization. In contrast to the previous studies, the present study was the first to show that sensitization to pollen could be a predictor of responsiveness to omalizumab. The reason for the different results among studies remains unclear, but differences in antigenicity, especially Japanese cedar pollen and other pollens, may partly explain it. Allergen sensitization in a population depends on the climate or environment, and the different biological features of sensitized allergens may affect the clinical characteristics of patients.36 Interestingly, the real-world omalizumab studies20,37 showed that severe allergic asthmatic patients with concomitant allergic rhinitis were more responsive to omalizumab than those without. In the present study as well, patients with pollinosis responded to omalizumab more frequently than those with neither pollinosis nor pollen sensitization. Omalizumab exerted profound efficacy in patients with allergic asthma and comorbid pollinosis by inhibiting allergen-specific IgE-dependent allergic responses in both upper and lower airways.
This study has several limitations. First, it was a retrospective study. Second, the sample size was small. Third, the patient population was composed mainly of Japanese patients with cedar sensitization. Fourth, skin-prick tests were not performed in all patients. According to the guidelines,19 a diagnosis of allergic rhinitis is made based on nasal symptoms, together with positive nasal eosinophil tests in the season, and identified causative allergens, based on skin reactions or serum specific IgE antibody measurement. Despite these limitations, the present finding is noteworthy from the perspective of the “one airway, one disease” concept. Omalizumab indications may have to be extended to include patients with severe allergic asthma who are sensitized to seasonal allergens, as well as perennial allergens. Future prospective studies with larger sample sizes and with different patient populations and sensitization are needed to examine if seasonal IgE response could be a predictive marker of omalizumab responsiveness.
In conclusion, this study was the first to show that sensitization to pollen could be a predictor of responsiveness to omalizumab treatment in adult patients with severe allergic asthma sensitized to perennial allergens. From the perspective of “one airway, one disease”, omalizumab could be a promising treatment in severe asthmatic patients with allergic rhinitis. To further examine the present finding, prospective studies are needed.
Abbreviations
GINA, Global Initiative for Asthma; ACT, asthma control test; FeNO, fractional exhaled nitric oxide; GETE, the Global Evaluation of Treatment Effectiveness; RCTs, randomized, controlled trials; Pts, patients; GERD, gastroesophageal reflux disease.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Nagoya City University (60-20-0174). Written informed consent was waived by the ethics committee due to the retrospective nature of this study. Instead, an opt-out document was posted on the hospital website to offer patients the opportunity to refuse participation. This study complied with the Declaration of Helsinki.
Acknowledgment
The authors thank Dr. Hiroya Hashimoto for advice on statistical analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Dr Kensuke Fukumitsu reports grants from Novartis Pharma, GSK; personal fees from AstraZeneca, Boehringer Ingelheim, Novartis Pharma, and Kyorin, outside the submitted work. The authors declared neither financial nor non-financial competing interests with respect to the research, authorship, and/or publication of this article.
References
1. Brożek JL, Bousquet J, Agache I, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. 2017;140:950–958. doi:10.1016/j.jaci.2017.03.050
2. Niimi A. Redefining “one airway, one disease”: broader classification considering specific pathophysiology and treatment. Respir Invest. 2021;59(5):573–575. doi:10.1016/j.resinv.2021.04.008
3. Yamauchi K, Tamura G, Akasaka T, et al. Analysis of the comorbidity of bronchial asthma and allergic rhinitis by questionnaire in 10,009 patients. Allergol Int. 2009;58:55–61. doi:10.2332/allergolint.08-OA-0004
4. Ohta K, Bousquet PJ, Aizawa H, et al. Prevalence and impact of rhinitis in asthma. SACRA, a cross-sectional nation-wide study in Japan. Allergy. 2011;66:1287–1295. doi:10.1111/j.1398-9995.2011.02676.x
5. Tajiri T, Niimi A, Matsumoto H, et al. Prevalence and clinical relevance of allergic rhinitis in patients with classic asthma and cough variant asthma. Respiration. 2014;87:211–218. doi:10.1159/000355706
6. Burgess JA, Walters EH, Byrnes GB, et al. Childhood allergic rhinitis predicts asthma incidence and persistence to middle age: a longitudinal study. J Allergy Clin Immunol. 2007;120:863–869. doi:10.1016/j.jaci.2007.07.020
7. Shaaban R, Zureik M, Soussan D, et al. Rhinitis and onset of asthma: a longitudinal population-based study. Lancet. 2008;372:1049–1057. doi:10.1016/S0140-6736(08)61446-4
8. Bousquet J, Gaugris S, Kocevar VS, et al. Increased risk of asthma attacks and emergency visits among asthma patients with allergic rhinitis: a subgroup analysis of the investigation of montelukast as a partner agent for complementary therapy [corrected]. Clin Exp Allergy. 2005;35:723–727. doi:10.1111/j.1365-2222.2005.02251.x
9. Price D, Zhang Q, Kocevar VS, Yin DD, Thomas M. Effect of a concomitant diagnosis of allergic rhinitis on asthma-related health care use by adults. Clin Exp Allergy. 2005;35:282–287. doi:10.1111/j.1365-2222.2005.02182.x
10. Halpern MT, Schmier JK, Richner R, Guo C, Togias A. Allergic rhinitis: a potential cause of increased asthma medication use, costs, and morbidity. J Asthma. 2004;41:117–126. doi:10.1081/JAS-120026069
11. Lohia S, Schlosser RJ, Soler ZM. Impact of intranasal corticosteroids on asthma outcomes in allergic rhinitis: a meta-analysis. Allergy. 2013;68:569–579. doi:10.1111/all.12124
12. Braunstahl GJ, Overbeek SE, Kleinjan A, Prins JB, Hoogsteden HC, Fokkens WJ. Nasal allergen provocation induces adhesion molecule expression and tissue eosinophilia in upper and lower airways. J Allergy Clin Immunol. 2001;107:469–476. doi:10.1067/mai.2001.113046
13. Corren J, Adinoff AD, Irvin CG. Changes in bronchial responsiveness following nasal provocation with allergen. J Allergy Clin Immunol. 1992;89:611–618. doi:10.1016/0091-6749(92)90329-Z
14. Okayama Y, Matsumoto H, Odajima H, Takahagi S, Hide M, Okubo K. Roles of omalizumab in various allergic diseases. Allergol Int. 2020;69(2):167–177. doi:10.1016/j.alit.2020.01.004
15. Okubo K, Ogino S, Nagakura T, Ishikawa T. Omalizumab is effective and safe in the treatment of Japanese cedar pollen-induced seasonal allergic rhinitis. Allergol Int. 2006;55:379–386. doi:10.2332/allergolint.55.379
16. Nagakura T, Ogino S, Okubo K, Sato N, Takahashi M, Ishikawa T. Omalizumab is more effective than suplatast tosilate in the treatment of Japanese cedar pollen-induced seasonal allergic rhinitis. Clin Exp Allergy. 2008;38:329–337. doi:10.1111/j.1365-2222.2007.02894.x
17. Okubo K, Okano M, Sato N, et al. Add-on omalizumab for inadequately controlled severe pollinosis despite standard-of-care: a randomized study. J Allergy Clin Immunol Pract. 2020;8:3130–3140.e2. doi:10.1016/j.jaip.2020.04.068
18. Reddel HK, Bacharier LB, Bateman ED, et al. Global initiative for asthma strategy 2021: executive summary and rationale for key changes. Am J Respir Crit Care Med. 2022;205:17–35. doi:10.1164/rccm.202109-2205PP
19. Okubo K, Kurono Y, Ichimura K, et al. Japanese guidelines for allergic rhinitis 2020. Allergol Int. 2020;69:331–345. doi:10.1016/j.alit.2020.04.001
20. Adachi M, Kozawa M, Yoshisue H, et al. Real-world safety and efficacy of omalizumab in patients with severe allergic asthma: a long-term post-marketing study in Japan. Respir Med. 2018;141:56–63. doi:10.1016/j.rmed.2018.06.021
21. Takemura M, Niimi A, Matsumoto H, et al. Atopic features of cough variant asthma and classic asthma with wheezing. Clin Exp Allergy. 2007;(37):1833–1839. doi:10.1111/j.1365-2222.2007.02848.x
22. Bousquet J, Siergiejko Z, Swiebocka E, et al. Persistency of response to omalizumab therapy in severe allergic (IgE-mediated) asthma. Allergy. 2011;66:671–678. doi:10.1111/j.1398-9995.2010.02522.x
23. Rodrigo GJ, Neffen H, Castro-Rodriguez JA. Efficacy and safety of subcutaneous omalizumab vs placebo as add-on therapy to corticosteroids for children and adults with asthma: a systematic review. Chest. 2011;139:28–35. doi:10.1378/chest.10-1194
24. Tsabouri S, Ntritsos G, Koskeridis F, Evangelou E, Olsson P, Kostikas K. Omalizumab for the treatment of allergic rhinitis: a systematic review and meta-analysis. Rhinology. 2021;59:501–510. doi:10.4193/Rhin21.159
25. Alhossan A, Lee CS, MacDonald K, Abraham I. “Real-life” effectiveness studies of omalizumab in adult patients with severe allergic asthma: meta-analysis. J Allergy Clin Immunol Pract. 2017;5:1362–1370.e2. doi:10.1016/j.jaip.2017.02.002
26. Bousquet J, Humbert M, Gibson PG, et al. Real-world effectiveness of omalizumab in severe allergic asthma: a meta-analysis of observational studies. J Allergy Clin Immunol Pract. 2021;9:2702–2714. doi:10.1016/j.jaip.2021.01.011
27. Hanania NA, Wenzel S, Rosén K, et al. Exploring the effects of omalizumab in allergic asthma: an analysis of biomarkers in the EXTRA study. Am J Respir Crit Care Med. 2013;187:804–811. doi:10.1164/rccm.201208-1414OC
28. Tajiri T, Matsumoto H, Gon Y, et al. Utility of serum periostin and free IgE levels in evaluating responsiveness to omalizumab in patients with severe asthma. Allergy. 2016;71:1472–1479. doi:10.1111/all.12922
29. Humbert M, Taillé C, Mala L, Le Gros V, Just J, Molimard M. Omalizumab effectiveness in patients with severe allergic asthma according to blood eosinophil count: the STELLAIR study. Eur Respir J. 2018;51:1702523. doi:10.1183/13993003.02523-2017
30. Casale TB, Luskin AT, Busse W, et al. Omalizumab effectiveness by biomarker status in patients with asthma: evidence from PROSPERO, A prospective real-world study. J Allergy Clin Immunol Pract. 2019;7:156–164.e1. doi:10.1016/j.jaip.2018.04.043
31. Domingo C, Pomares X, Navarro A, et al. Omalizumab is equally effective in persistent allergic oral corticosteroid-dependent asthma caused by either seasonal or perennial allergens: a pilot study. Int J Mol Sci. 2017;18:521. doi:10.3390/ijms18030521
32. Mizuma H, Tanaka A, Uchida Y, et al. Influence of omalizumab on allergen-specific ige in patients with adult asthma. Int Arch Allergy Immunol. 2015;168:165–172. doi:10.1159/000442668
33. Vaník P, Novosad J, Kirchnerová O, Krčmová I, Teřl M. Effect of individual allergen sensitization on omalizumab treatment outcomes in patients with severe allergic asthma determined using data from the Czech Anti-IgE Registry. Allergy Asthma Clin Immunol. 2020;16:81. doi:10.1186/s13223-020-00479-1
34. Soong W, Yoo B, Pazwash H, Holweg CTJ, Casale TB. Omalizumab response in patients with asthma by number and type of allergen. Ann Allergy Asthma Immunol. 2021;127:223–231. doi:10.1016/j.anai.2021.04.002
35. Wahn U, Martin C, Freeman P, Blogg M, Jimenez P, Relationship between pretreatment specific IgE and the response to omalizumab therapy. Allergy. 2009;64:1780–1787. doi:10.1111/j.1398-9995.2009.02119.x
36. Lombardi C, Savi E, Ridolo E, Passalacqua G, Canonica GW. Is allergic sensitization relevant in severe asthma? Which allergens may be culprit? World Allergy Organ J. 2017;10:2. doi:10.1186/s40413-016-0138-8
37. Sposato B, Scalese M, Milanese M, et al. Factors reducing omalizumab response in severe asthma. Eur J Intern Med. 2018;52:78–85. doi:10.1016/j.ejim.2018.01.026
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Allergic Sensitivity and Pollination in Allergic Respiratory Disease: The Role of Pollution
Pavón-Romero GF, Calderón-Ezquerro MDC, Rodríguez-Cervantes MA, Fernández-Villanueva D, Melgoza-Ruiz E, Ramírez-Jiménez F, Teran LM
Journal of Asthma and Allergy 2022, 15:1227-1243
Published Date: 1 September 2022
Role of Chemokines and Inflammatory Cells in Respiratory Allergy
Bao Y, Zhu X
Journal of Asthma and Allergy 2022, 15:1805-1822
Published Date: 21 December 2022
Dupilumab Efficacy in Patients with Uncontrolled Moderate-to-Severe Type 2 Asthma Regardless of Perennial Aeroallergen Sensitization
Corren J, Jackson DJ, Casale TB, Borish L, Rabe KF, Busse WW, Maspero JF, Jackson DJ, Daizadeh N, Altincatal A, Radwan A, Khodzhayev A, Djandji M, Jacob-Nara JA, Rowe PJ, Deniz Y
Journal of Asthma and Allergy 2023, 16:249-260
Published Date: 7 March 2023
Real-World Safety and Effectiveness of Omalizumab in Moderate to Severe Allergic Asthma Patients in China: A Post-Authorization Study
Su N, Zhi L, Liu F, Wang Y, Zhang Q, Liu X, Wang X, Hao G, Zhang X, Hu Q, Ligueros-Saylan M, Uddin A, Yang J, Liang T, Ding L, Li R, Wang C
Journal of Asthma and Allergy 2023, 16:625-636
Published Date: 19 June 2023
Antitussive Use in Patients with Inadequately Controlled Moderate-to-Severe Asthma: A Post Hoc Analysis of the Omalizumab EXTRA Trial
Rutland CJ, Iweala OI, Anders K, Ko J, Mital P, Gupta S, Mohan A
Journal of Asthma and Allergy 2023, 16:661-665
Published Date: 24 June 2023