Back to Journals » Psychology Research and Behavior Management » Volume 16
Social Support Mediates the Relationship Between Coping Styles and the Mental Health of Medical Students
Authors Dai P, Yi G ![]() , Qian D, Wu Z, Fu M, Peng H
, Qian D, Wu Z, Fu M, Peng H
Received 26 January 2023
Accepted for publication 23 March 2023
Published 19 April 2023 Volume 2023:16 Pages 1299—1313
DOI https://doi.org/10.2147/PRBM.S405580
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mei-Chun Cheung
Peilin Dai,1,2,* Guoguo Yi,3,4,* Dandan Qian,5,* Zhe Wu,2 Min Fu,6 Hui Peng1
1School of Nursing, Hunan University of Medicine, Huaihua, Hunan, People’s Republic of China; 2The Second School of Clinical Medicine, Southern Medical University, Guangzhou, People’s Republic of China; 3Department of Ophthalmology, The Sixth Affiliated Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 4Biomedical Innovation Center, The Sixth Affiliated Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 5Department of Clinical Skills Training Center, Zhujiang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 6Department of Ophthalmology, Zhujiang Hospital of Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Fu, Department of Ophthalmology, Zhujiang Hospital of Southern Medical University, No. 253, Industrial Avenue Middle, Haizhu, Guangzhou, People’s Republic of China, Tel +86 18665621066, Email [email protected] Hui Peng, School of Nursing, Hunan University of Medicine, No. 492, Jinxi South Road, Huaihua, Hunan, People’s Republic of China, Email [email protected]
Purpose: This study aimed to explore the impact that coping styles and social support have on the mental health of medical students by constructing a corresponding structural situation model that reveals the complex relationship between these three factors. In doing so, it seeks to help medication students better manage mental health problems.
Patients and Methods: The online study was conducted between March 6, 2021 and May 6, 2021. A total of 318 participants from multiple medical schools were involved. The general information questionnaire, simple coping style questionnaire (SCSQ), perceived social support scale (PSSS) and symptom checklist 90 (SCL-90) were used to collect relevant information from the subjects by snowball sampling. An independent t-test, ANOVA, Pearson correlation coefficient analysis, and intermediary effect analysis were all used to analyze the relevant data and construct the structural equation model.
Results: There was a significant difference in SCL-90 between medical students and national college students (1.78± 0.70, P < 0.001), and the positive rate of mental health status was as high as 40.3%. Sleep quality, regular diet, and positive coping style were positively correlated with mental health (P < 0.01), while negative coping styles and total scores of coping style as well as family, friends, and other sources of social support and total scores of social support were negatively correlated with mental health problems (P < 0.01). Positive and negative coping styles have an impact on mental health through the mediating effect of between social support and coping styles, as well as in the direct pathway.
Conclusion: The mental health status of medical students was significantly poor. Medical schools should thus pay close attention to the mental health status of students and encourage them to develop healthy living habits, optimize coping styles, and establish stable sources of social support to improve their psychological wellbeing.
Keywords: mediating effect, structural equation model, questionnaire investigation, psychological wellbeing
Introduction
Medical students are a distinct group that experience intense academic pressure and burnout due to the fact that their enrollment in professional courses and high-intensity practice make it difficult to balance their work, education, and personal lives.1,2 They face a variety of financial, social, and psychological challenges that can impact their mental health. For instance, medical students undergo a long training cycle and carry heavy economic burdens.3 They also have to contend with a widely-held social belief that doctors are the ones who shoulder the responsibility of saving lives and must grapple with the ethical and psychological pressure of facing death. Moreover, within the context of social networking, doctors feel the weight of public opinion like never before, and increasingly sophisticated medical technology has created stricter requirements for medical students. All of these factors jointly contribute to a tendency among medical students to strive for unrealistic perfectionism.4–7 Perfectionism is strongly positively correlated with mental health problems, and intense medical specialty and fierce employment competition pose career planning challenges to medical students.8–10 A tense doctor-patient relationship that often plays out in medical environments also contributes to the sense of uncertainty that medical students experience when considering their future work.11,12 A large number of studies that have taken place around the world show that medical students have more serious mental health problems than their peers and the general population;13–22 however, compared with a large number of studies on medical students’ mental health problems, research that investigates the coping styles and social support networks of medical students is limited. Exploring how coping styles and social support affect the mental health of medical students could help identify specific solutions that are likely to improve the situation and cultivate a new generation of doctors with strong levels of physical and mental health.23,24
Coping style refers to specific behavioral and psychological efforts to master, tolerate, reduce, or minimize stress events. Previous studies have shown that positive coping styles can improve outcomes by generating positive emotions and behaviors, while negative coping styles may cause mental health problems.25 Nevertheless, some studies have found that negative coping styles are beneficial in that they can relieve psychological stress and allow individuals to temporarily cope with adverse environments.26 Many studies indicate that coping style has a significant impact on mental health status and produces direct or intermediary effects,27,28 which means that targeting this factor may be an effective means of intervening in the mental health status of medical students. Social support refers to all types of spiritual and material support that individuals obtain through social relations. Strong social support can help people resist setbacks from work, study, and life, relieve pressure,29 and enhance their self-confidence when facing challenges or difficulties. Many studies have shown that social support positively impacts mental health.30,31 Medical students often confront strenuous work and course tasks, and they usually do not have enough free time to relax. They require strong social support that can provide them with spiritual motivation, encourage them to maintain a balanced psychological state, and ultimately allow them to realize the continuity of their work and study. Therefore, our study puts forward the following assumptions:
Hypothesis 1: Coping style and social support can significantly predict the mental health status of medical students.
According to previous study, coping style and social support contribute to an individual’s level of resilience to mental health problems.32 Assessment support can change an individual’s perception of threats and impact their coping abilities when they are experiencing psychological pain caused by stress.33 Generally speaking, emotional factors, such as the belief in social support, can predict behavior more effectively than cognitive factors.34,35 A study from Pakistan36 demonstrated that ineffective coping mechanisms and a lack of social support can lead to poor academic performance among medical students. For medical students who work in insular academic environments, perceived stress and low levels of social support are more common than they are in general populations.37 Medical students require more support than students of other majors,38 and social support can influence the way that they deal with difficulties and setbacks. According to existing research, social support can affect the relationship between health literacy and depression through mediating effects.39–41 For instance, Dunn et al42 proposed that both negative and positive inputs, including psychosocial support, would affect a student’s personal coping ability.43 Although we speculate that social support can affect the relationship between coping style and mental health, the exact role that it plays in this dynamic remains a mystery. Therefore, we also put forward the following assumption:
Hypothesis 2: Coping style affects the mental health status of medical students through the intermediary of social support.
Therefore, this online study establishes and verifies the model based on the above two hypotheses, aiming to explain the internal correlation and causal relationship between coping style, social support and mental health of medical students.
Materials and Methods
In this study, the general information questionnaire, simple coping style questionnaire (SCSQ), perceived social support scale (PSSS), and symptom checklist 90 (SCL-90) were used to analyze medical students. The purpose of this research was to better understand the coping style, social support, mental health status, and related influencing factors of this group and reveal their internal relationship through a structural equation model (SEM) to provide theoretical reference for the prevention and intervention of the mental health problems of medical students. After a manual screening and discarding the questionnaires of the abnormal value with high consistency of options and too short answer time (<5min), 318 valid questionnaires were retained. The effective rate of the questionnaire was 96.36%. In the course of receiving the data, the consent of the subjects is obtained, and the personal data and results are kept confidential.
Participants and Procedures
In this survey, the participants were medical students who were attending different medical colleges and universities dominated by Southern Medical University and Sun Yat-sen University and Nanchang University Medical School in China. The inclusion criteria was that students who were included in this study needed to be majoring in medicine and had to have been born after January 1, 2000. The exclusion criteria was that participants who selected the same choices to all of the questions in the questionnaire were excluded, as were participants who were suspended or dropped out of school. Considering that the survey period took place during the COVID-19 epidemic, all the questionnaires in this study were completed using a professional online questionnaire software called Questionnaire Star by snowball sampling. Advertisements in the form of linkage, QR codes and text messages were given in social platforms like WeChat and Tencent to invite medical students to participate in the study about mental health. The questionnaire consisted of two screens, with 135 questions in total. It took 6 minutes on average to complete the questionnaire, and people were given 1 to 2 yuan RMB for their participation at random. We prevented reduplicate participation by IP control. During the period from March 6, 2021 to May 6, 2021, 330 complete questionnaires were collected through the online platform after 360 questionnaires were started. Due to the mandatory completion before submission, all collected questionnaires had no missing values.
Materials
General Information Questionnaire
The demographic information and basic living conditions of the subjects were investigated using self-made items that inquired about gender, age, whether they were an only child, whether their parents were alive, whether they were single, whether they had never been in love, how often they stay up late, their sleep quality, and whether they ate regularly and exercised (Supplementary Table 1). Staying up late was artificially defined as falling asleep after 12:00 am or staying up all night. The frequency of staying up late was divided into five different levels: almost every day, 3–5 times a week, 1–2 times a week, 1–3 times a month, and almost never. Sleep quality was scored on a four-point Likert scale (1 = excellent; 4 = insomnia), adapted from subjective sleep quality assessment in the Pittsburgh Sleep Quality Index. The design of exercise items referred to the method mentioned above.
Simple Coping Style Questionnaire
The Chinese version of the Simplified Coping Style Questionnaire (SCSQ) was used to evaluate the coping style tendency of subjects. Coping style is the cognitive and behavioral style that individuals adopt while under pressure or facing psychological distress. The scale was adapted from the foreign coping style scale and is considered to align with the characteristics of the local population. It shows high reliability and validity in other studies and constructs a two-dimensional model that includes positive and negative coping styles.44 The questionnaire contains 20 items. The combination of positive coping dimensions (items 1–12) and negative coping dimensions (items 13–20) reflect the characteristics of different coping styles and their relationship with mental health.45 This scale adopts multi-level scoring, and after each coping style item, there are four options: never, occasionally, sometimes, and often (the corresponding scores are 0, 1, 2, and 3). The subjects chose the corresponding options based on their own situation. The results were the respective average scores of positive and negative coping dimensions. The standard score is obtained by Z conversion between positive coping style and negative coping style; that is, the standard score Z = (actual score – sample average score) / sample standard deviation. The final result was as follows: coping tendency score = positive coping standard score – negative coping standard score. If the score of coping tendency is more than 0, the higher the score, the greater the possibility that the participants possessed positive coping styles. However, if the score is less than 0, the lower the score, the greater the likelihood that they are more inclined to negative coping styles. Due to its convenience and practicability, the scale has been widely used and is proven to have good reliability and validity.44,46–48 The Simple Coping Style Questionnaire showed high internal consistency (the Cronbach’s α = 0.807) in the study, The Kaiser–Meyer–Olkin Measure of Sampling Adequacy (KMO) was 0.816, with the significance of Bartlett’s test of sphericity <0.001. A total of 5 factors were obtained by rotation, with each factor including 3 to 5 items, and the factor load was between 0.527 and 0.899, larger than the acceptable value of 0.35.
Perceived Social Support Scale
Perceived Social Support scale (PSSS) is a social support scale used to reflect individual self-feeling. It is used to measure the various social support sources that individuals perceive, such as the level of support that they receive from family, friends, and others, and can reflect the total degree of social support that an individual experiences.49 Social support refers to psychological and material support or encouragement from family or friends while under stress. The support of social relations can affect the way that individuals understand their surroundings, play an essential role in formal and informal support networks,50 and reflect the closeness and quality of a person’s relationship with society. This domestic scale was revised in 1999 based on the perceived social support scale that Zimet complied in 1987.51 PSSS includes 12 self-assessment items. Each item adopts the seven-level scoring method of Likert scale 1–7 and is divided into seven levels: extremely disagree, strongly disagree, slightly disagree, neutral, slightly agree, very agree, and strongly agree. It also consists of three subscales: family support (items 3, 4, 8 and 11), friend support (items 6, 7, 9 and 12), and other sources of support (including teachers, classmates, and relatives). The total score of the scale is calculated by adding all the item scores. The higher the score, the higher an individual’s degree of social support. When the total score is between 12 and 36, it indicates a low support state. If the total score is between 37 and 60, it implies an intermediate support state, and a total score between 61 and 84 is considered to reflect a high support state. Similarly, because it is a simple scale suitable for domestic populations, PSSS is also widely used in various specific populations and shows excellent effects.52–54 The Cronbach’s α coefficient for PSSS was 0.952 in this study. The KMO was 0.936, with the significance of Bartlett’s test of sphericity <0.001, indicating that factor analysis suitable, and the factor load was between 0.657 and 0.879. The two factors had 4 and 8 items respectively.
Symptom Checklist-90
Symptom Checklist-90 (SCL-90) is one of the most famous mental health test scales in the world and contains 90 items that reflect on a subject’s somatization, obsessive-compulsive symptoms, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoia, psychosis, and other dimensions of their wellbeing, such as sleep and diet. The score of each item is 1–5, and the total score is the sum of the scores of all 90 items. The score of each dimension = (the sum of scores of subscales of this dimension) / (the number of items of this dimension). If the dimension score exceeds 2 points, it indicates that the dimension is positive. The number of positive items refers to the total number of items with a score greater than 1. SCL-90 positive means that the total score is more than 160, the number of positive items is over 43, or the score of any dimension is larger than 2. Positive results indicate that the subjects might have mental health problems in a certain dimension. The scale is widely used by researchers around the world55–57 because it can accurately reflect the multi-dimensional mental health status of subjects. The Cronbach’s α coefficient for SCL-90 was 0.987. The KMO was 0.970, with the significance of Bartlett’s test of sphericity <0.001.
Data Analysis
We used Amos 26.0, SPSS 26.0, and PROCESS 3.2 macro (IBM Crop) to examine and sort through the questionnaire data, conduct variable transformation and data analysis, and construct the structural equation model. The measurement data was represented by mean and standard deviation or median and interquartile range, and the counting data was represented by frequency and composition ratio (%). Pearson correlation analysis was used for bivariate normal distribution data whose independent variable was continuous, and Spearman correlation analysis was used for non-bivariate normal distribution data. According to the central limit theorem,58 when the sample size is large, t-test can be used even if the data does not meet the normal distribution. Thus, an independent sample t-test was applied to compare the data of this study with the national norm. ANOVA and mediation effect analysis were conducted between other variables in the questionnaire and the total score of SCL-90. After selecting appropriate variables, the feasibility of factor analysis was verified by KMO and Bartlett’s test of sphericity. The reliability and validity of the data were also tested using Cronbach’s α coefficient and multifactor confirmatory factor analysis (CFA). Finally, the SEM that can clearly show the internal correlation among the factors was constructed by Amos. P < 0.05 indicated that the difference was statistically significant.
Results
Descriptive Statistics and Sample Characteristics
This study investigated 318 medical students. The sample included 94 males (29.56%) and 224 females (70.44%) who were 17 to 21 years of age (mean = 19.88 years, SD = 1.01). Eighty-seven (27.36%) of participants had no siblings, 239 participants were single, 168 participants had never been in love, and 9 participants unfortunately suffered the death of their parents. With respect to living habits, only 20 participants said that they hardly stayed up late (staying up late was defined as falling asleep after 12:00 pm or staying up all night to study), while 112 participants (35.22%) said they stayed up almost every night and 56 people (17.61%) said that their sleep quality was poor, of which 9 had insomnia. Fifty-nine subjects admitted that they had an irregular diet, and 69 of the participants admitted that they hardly exercised. Through one-way ANOVA, significant statistical differences in sleep quality and diet were discovered. Table 1 shows the descriptive statistics of the sample.
 |
Table 1 The Descriptive Statistics of SCL-90, PSSS, and SCSQ |
There were 189 students’ SCL scores lower than 160, indicating that only 59.43% medical students were in a good mental health. Only 9 students (2.83%) in our study held low social support, and 39.62% students held middle social support. The students with high social support occupied 57.55%, similar to the proportion of students with good mental health. The proportion of negative coping style is 25.47%, and the one of positive coping style is 74.53%. Moreover, comparing the SCL-90 score of medical students obtained in this study with the national college student norm (Supplementary Table 2) revealed significant differences between medical students and other college students in the dimension of paranoia and the total score of SCL-90 (P < 0.001). The score of our subjects in the dimension of paranoia (1.66±0.73) was obviously lower than the national college student norm (1.84±0.63, t = −4.420). By contrast, the total score of SCL-90 of medical students (1.78±0.70) was apparently higher than the norm (1.63±0.51, t = 3.762). This study mainly determined the sample size based on mental health status. As the sample size of the national survey is 2685, our preset allocation ratio was 8:1. With an α of 0.05, 2-tailed testing, power of 0.80, and the effect size of d=0.5 in preset independent sample t-test, we estimated that 320 participants needed to be recruited by G*Power (3.1.9.7 for Windows XP, Vista.). Within the acceptable error range, the final actual sample size is 318.
Correlation Analysis
Table 2 shows the mean, standard deviation, and binary correlation between the main variables. There was no significant correlation between the dimensions of social support (family support, friend support, and other sources of support) and negative coping styles; however, there was a significant correlation between the other main variables. SCL-90 score mainly reflects mental health status. In our analysis, there was a significant negative correlation between positive coping styles, an individual’s mental health status, and the three dimensions of social support and mental health status. There is a positive correlation between other relevant variables.
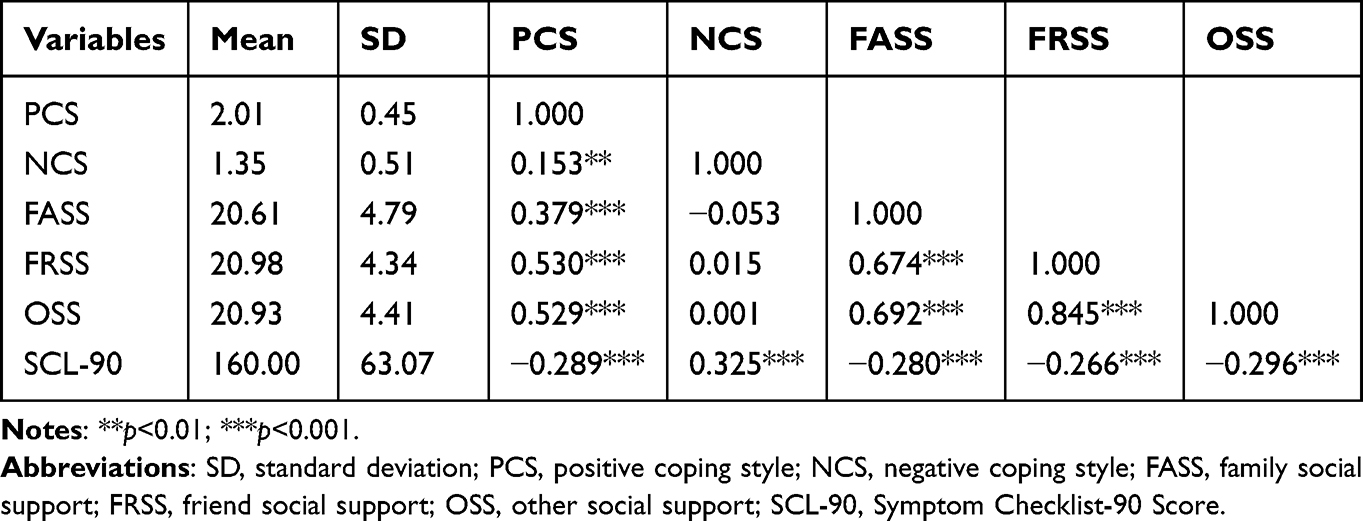 |
Table 2 Descriptive Statistics and Correlations Among the Main Variables |
Verification of Mediation Effect
In order to verify the mediation effect, this study applied Baron’s multiple linear regression to verify the mediation model.59 This study constructed three models to verify the mediating role of social support between coping style and mental health status. Similar to the previous study with Chinese college students with disabilities,60 model 1 also showed that coping style had a significant predictive effect on mental health (β = −0.470, P < 0.001). And model 2 demonstrated that coping style had a significant predictive effect on social support (β= 0.434, P < 0.001). Moreover, when social support and coping style were included in the regression model as predictors (model 3) just like the programme of a multicenter survey,61 the prediction effect of the model on mental health was still significant. Then, model 4 was established through SPSS-PROCESS macro, which was an intermediary model based on a bootstrap method. The result indicated that 95% CI did not contain 0 [95% CI = (−2.174, −1.002)], which meant that coping style was related to mental health status but did not indirectly affect mental health status through social support. Table 3 illustrates the details.
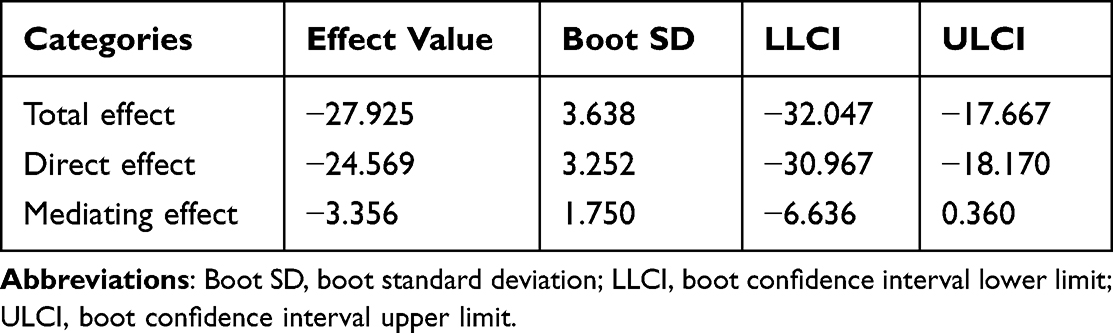 |
Table 3 Analysis of Mediating Effect of Social Support Between Coping Style and Mental Health |
Next, we used the previously mentioned sleep quality—which could significantly affect mental health status according to previous studies62,63 —as the mediator between coping style and mental health status and established a model for verification.64 Model 1 is the same as the model mentioned above and is used to predict SCL-90 score through SCSQ. Model 5 showed that sleep status had a notable impact on coping style (β = −0.246, P < 0.001). Zhang et al Indicated that coping style played a partial intermediary role in the relationship between sleep quality and depression symptoms of nursing students.65 After incorporating sleep status and coping style into the regression model as predictive variables (model 6), our result revealed that the prediction effect of the model on mental health status was still satisfactory. Coping style and social support are important mediating and regulating factors in the process of individual psychological stress, which have an important impact on individual mental health.66,67 Therefore, we applied the same method used to build model 4 to establish mediation model 7. The result indicated that coping style was not only directly related to mental health status but also indirectly affected mental health status through sleep status. After replacing coping style with social support, model 8–10 were established in the same way (as shown in Table 4). Similar to previous research results,68,69 our research also showed the beneficial roles of social support for mental health, and displayed that higher levels of social support are related to lower levels of mental health.
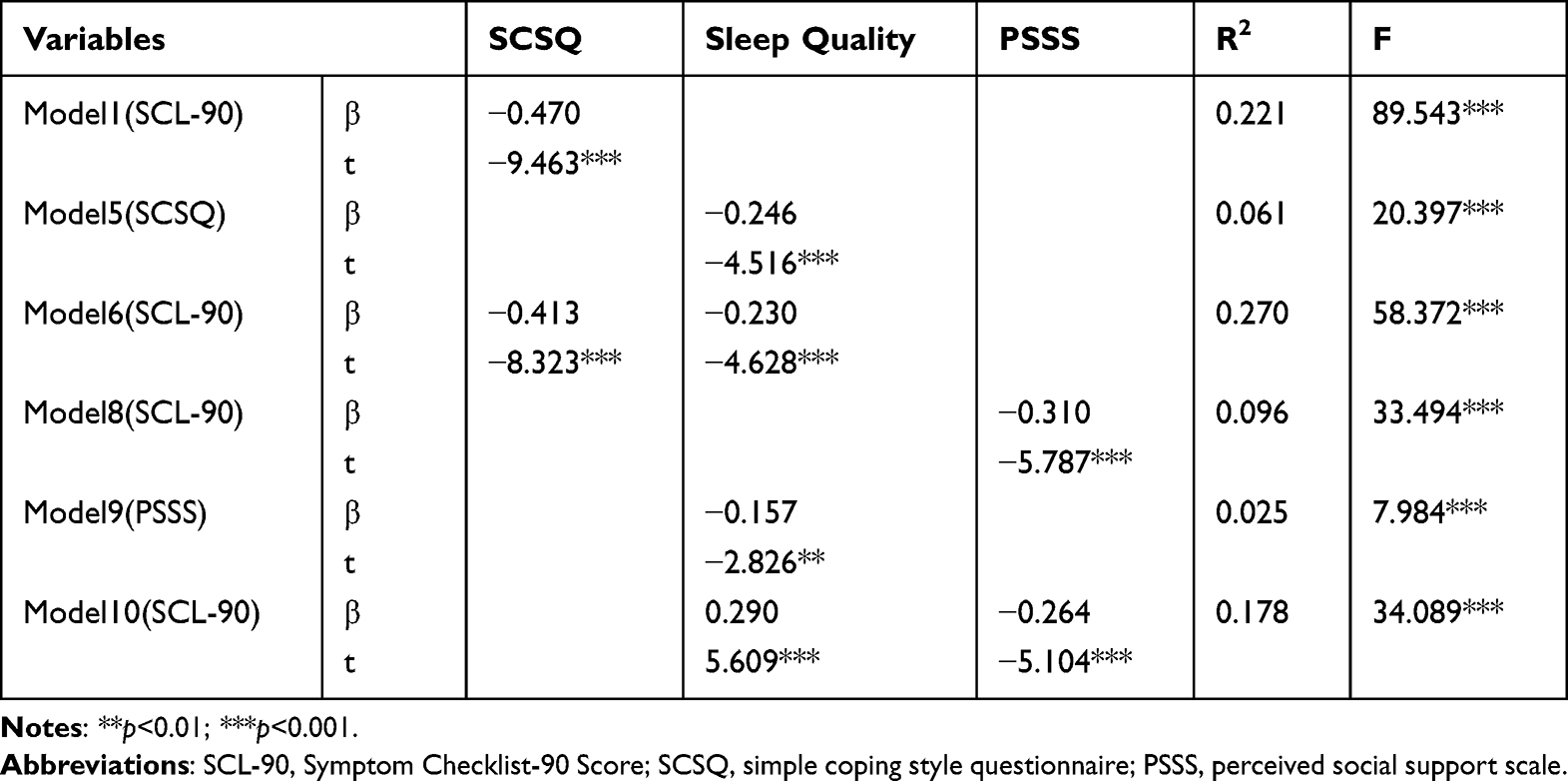 |
Table 4 Model Parameters Among Sleep Quality and the Main Variables |
The final results illustrated that sleep quality had a similar mediating effect between social support and mental health. Figure 1 displays the specific relationship network. Sleep quality had partial mediating effects between coping style and mental health and between social support and mental health, and the relative effects were 12.04% and 14.71%, respectively. Table 5 describes the details of the mediating effects of sleep quality.
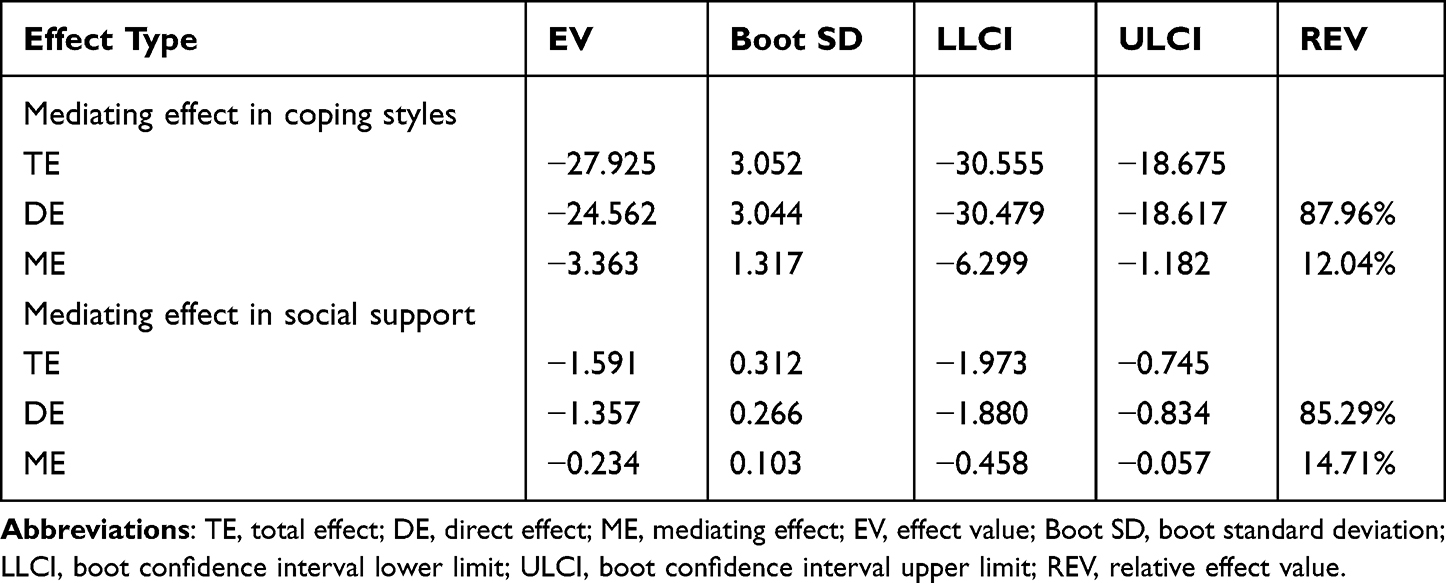 |
Table 5 Decomposition Table of Mediating Effects of Sleep Quality |
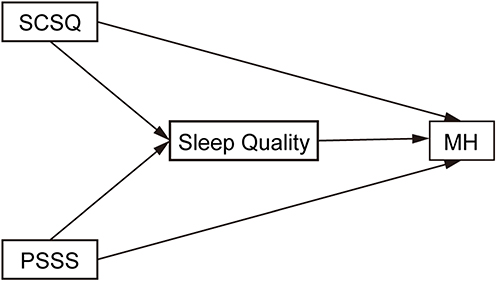 |
Figure 1 Theoretical framework for the mediating effect of sleep quality. Abbreviations: SCSQ, simple coping style questionnaire; PSSS, perceived social support scale; MH, mental health. |
Construction of Structural Equation Model
According to the regression analysis of model 1, 2, 3 and 8, there were significant correlations between (positive and negative) coping styles and mental health and between social support and mental health in regression analysis, similar to previous studies.46,61,70 We constructed several SEMs between coping style, social support and mental health, but the attempts failed. Subsequently we further analyzed the internal structure of latent variables. Ultimately, we included PCS, NCS, social support and mental health into SEM. In line with the rule-of-thumb of 10 cases per variable, the number of participants was deemed sufficient for SEM. Subsequent analysis revealed that taking the two dimensions of positive coping and negative coping as potential variables alone could realize the construction of the structural equation model. After analysis, the KMO value was 0.900, and Bartlett’s test of sphericity significance was < 0.001, which indicated that the data was suitable for factor analysis. Concurrently, considering the limitation of the number of items of sleep quality and other variables (not enough to build SEM), they were not included in the SEM. We used SEM to verify the model shown in Figures 2 and 3. The path coefficient of the link between positive copying style and negative copying style was not significant enough. At this point, we reviewed the model by changing the path. The factor loading of the items is demonstrated in Table 6.
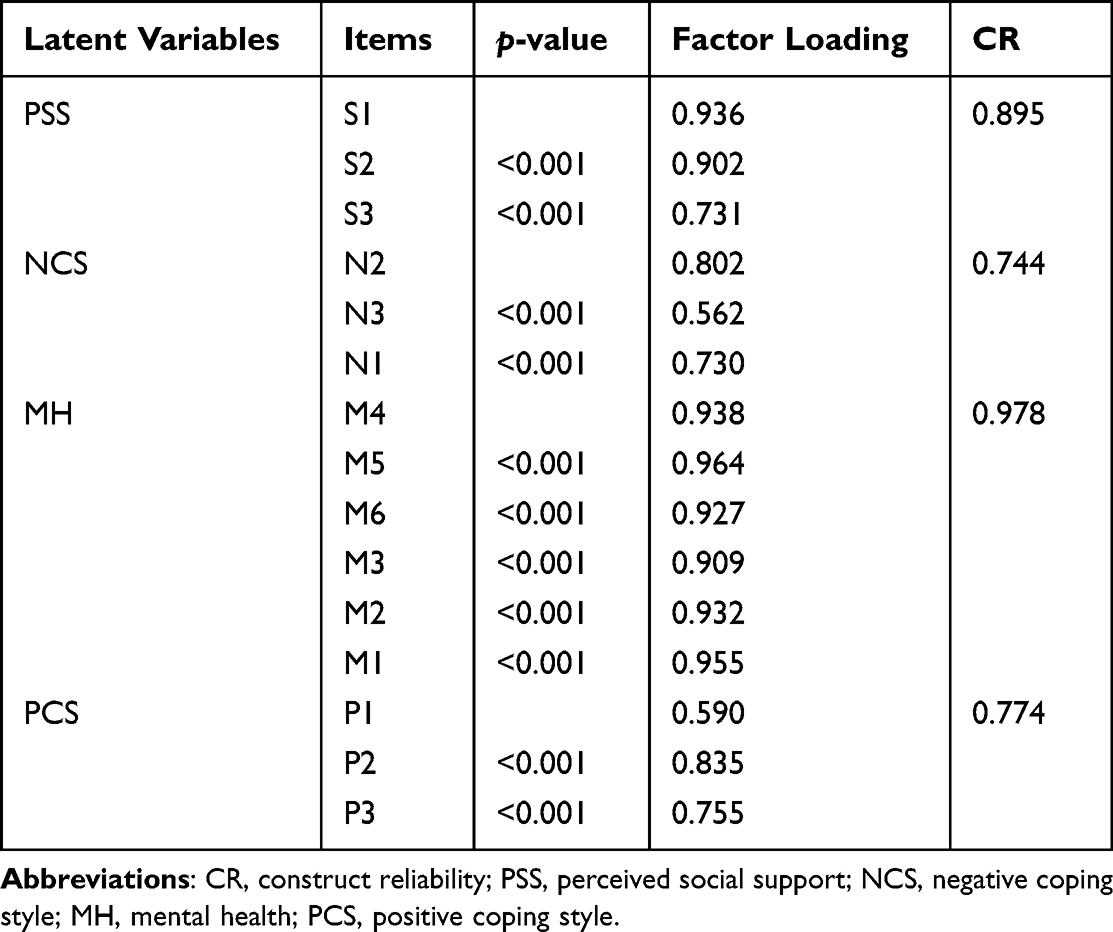 |
Table 6 The Related Parameters of the Final SEM Items |
 |
Figure 2 Envisaged structural equation model framework. Abbreviations: PCS, positive coping style; PSS, perceived social support; NCS, negative coping style; MH, mental health. |
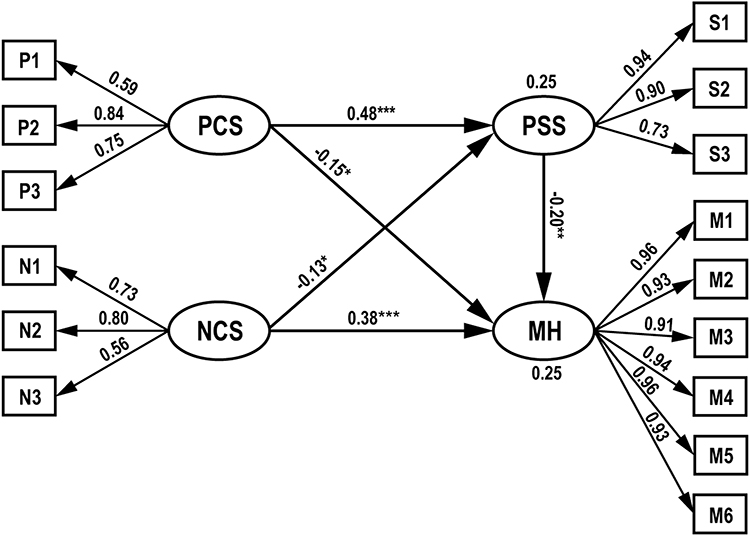 |
Figure 3 Final structural equation model framework. Abbreviations: PCS, positive coping style; PSS, perceived social support; NCS, negative coping style; MH, mental health. Notes: *p<0.05; **p<0.01; ***p<0.001. |
After maximum likelihood estimation, multi factor CFA was performed, and the model performed excellently: GFI=0.932; AGFI=0.904; NFI=0.958; IFI=0.977; CFI=0.977; TLI=0.972; RMSEA = 0.059. Positive and negative coping style accounted for 25% of the variance of social support. Positive coping style, negative coping style, and social support accounted for 25% of the variance of mental health problems. Social support and positive coping style were significantly negatively correlated with mental health problems (γ = −0.20 and −0.15, P < 0.01 and < 0.05). There was a significant positive correlation between negative coping styles and mental health problems (γ = 0.38, P<0.001). Negative coping style was negatively associated with social support (γ = −0.13, P < 0.05), while positive coping style was positively connected with social support (γ = 0.48, P < 0.001).
Discussion
Mental health is an important factor that affects the careers of medical students. Many medical students cannot successfully complete their studies or interrupt their medical career because of mental health problems that emerged before they officially became doctors.71 Therefore, mental health management and intervention of medical students plays an essential role in the cultivation of future doctors. Compared with the national norm for college students, the overall mental health status of medical students was worse, which was consistent with a large number of previous research findings. Though the dimension of paranoia was significantly better for medical students than the general college student population according to the SCL-90 scale, there was no significant difference in the other dimensions; however, from the perspective of the total score and average score of this scale, the situation was not optimistic. It is acknowledged that the threshold of SCL-90 scale to determine the positive mental health status is 160, and if the score exceeds 160, the subject can be considered to have mental health problems. The average value of the total score obtained in this study was exactly equal to 160, which means that there is an urgent need to improve the mental health of medical students.
Medical students generally have poor sleep quality, and there is a trend towards sleep deterioration that has emerged in recent years.72,73 This study revealed that sleep quality can significantly predict the mental health status of medical students. It is worth mentioning that the effect is mutual, and mental health can also obviously predict an individual’s quality of life, including sleep quality. There was a two-way predictive relationship between poor sleep quality and mental health problems. Methods to improve sleep quality, such as taking sleeping pills or other effective interventions, may promote mental health. Conversely, mental health treatment may also improve sleep quality.74 In our study, sleep quality had partial mediating effects between coping style and mental health and between social support and mental health. In other words, coping style and social support can not only directly affect mental health but also have the ability to further affect mental health by impacting individual sleep quality, though our data showed that their relative effect values were not very high (12.04%, 14.71%). With respect to the relationship between sleep quality and mental health, previous studies have shown that an increase of glucocorticoid is linked to mental health problems. The operation of human endocrine system is affected by circadian rhythm. Poor sleep quality interferes with normal hormone secretion and regulation of the body, which affects the content of glucocorticoid in blood and impacts mental health.75,76 This suggests that improving sleep quality could bolster the mental health of medical students and that ensuring they have adequate amounts of sleep is the first step towards helping this particular student group.
Unhealthy eating patterns are also common among medical students, despite the fact that they are knowledgeable about the harm these habits can have on their health. Resolving this particular situation seems more possible in recent years, however, due to a shift in the general public’s attitudes towards eating and living habits.77,78 An unhealthy diet can manifest as skipping meals, eating snacks instead of dinner, low intake of fruits and vegetables, and high intake of fast food or carbonated drinks. The research suggested that the eating habits of female medical students were worse than those of male students.79 Although this study analyzed gender as an independent variable within mental health status, the results show that gender has no significant impact on mental health status. A study in Japan80 showed that serum albumin content was linked to psychological distress, which means that unhealthy diet may affect the content of nutrients in the human body, thereby increasing the risk of mental health problems. A separate review81 also extensively collected evidence that diet plays an important role in emotional and mental health and also found that diet can affect mental states by changing the content of nutrients in the body and altering hormone levels. For instance, excessive intake of sodium salt can increase the ratio of sodium to potassium, lead to progesterone secretion, change brain nerve activity, and result in emotional deterioration.82,83 Hence, encouraging medical students to eat in the school canteen, balance their diet, and adjust their eating habits may be a solution worth pursuing to optimize their mental health.
Coping styles are divided into two dimensions: positive coping and negative coping. Individuals often deal with stress events and manage the corresponding emotional states through coping styles.84 In the current study, the mental health status of medical students was significantly regulated by coping styles, especially negative coping styles, which can obviously increase the risk of mental health problems. Among college students, life stress is related to the increase of negative coping styles. Negative coping styles are often risk factors for mental health problems, such as suicidal ideation and depression.85–87 Thus, a vicious circle can emerge between negative coping styles and adverse life stress events, ultimately worsening mental health. Positive coping style was a protective factor of mental health, which is consistent with previous research results.88
As predicted in hypothesis 2, we discovered that coping styles can indirectly affect the mental health of medical students through the intermediary effect of perceived social support. The intermediary effect of social support played a greater role in positive coping styles than in negative coping styles. The results suggested that positive coping styles can alleviate the pressure and negative emotions caused by adverse life events through high-level social support, which can reduce the risk of mental health problems. Medical students’ perceptions of social support come from interpersonal relationships and a sense of belonging. Improving the humanistic atmosphere in their learning workplace is more likely to promote the positive development of their social support,89 thereby reducing the probability of mental health problems. Social support was the protective factor of mental health in this study. Previous studies have illustrated that the lack of social support is often closely related to mental health problems, such as anxiety disorders, depression,84,90 and schizophrenia.91 In addition, as other studies have demonstrated, social support not only contributes to the mental health of the general population but also plays a role in helping patients with respiratory diseases cope with dyspnea crisis.92 Moreover, this study adopted the perceived social support scale that reflects the subjective perceived physical and mental support from others, which may differ from objective social support. We believe that perceived social support has a more accurate predictive effect on mental health than objective social support because mental health is closely related to personal subjective feelings logistically, but more research is needed to confirm this idea.
In this study, we creatively analyzed the relationship between the mental health and social support and coping styles of medical students, filling the gap of relevant researches, and putting forward targeted strategies to improve the current situation. There are also some limitations in our study: The number of samples is limited, which may affect the results and conclusions. The study is a cross-sectional study, and the sample is not nationally representative. For our study, the females occupied the majority of the sample (70.44%), and it mainly represented the mental health of women. Due to the excessive number of questions in the questionnaire, we did not fully include the authoritative sleep quality scale. Therefore, the sleep quality results we have evaluated are only indicative and further research is needed to confirm our conclusions about sleep quality. A potential deficiency of this study is that when the questionnaire was issued, the COVID-19 epidemic was still ongoing. By the time students filled out this questionnaire, they had returned to medical colleges or practice bases for normal study or practice; however, the impact of COVID-19 on medical students was not taken into account in the design of this study, though this unusual social environment would inevitably affect the mental health status of medical students to a certain extent. This aspect needs to be supplemented by follow-up research.
Conclusion
We found that mental health status was severe among medical students and that these poor results were linked to sleep quality and unhealthy diet. In addition, we discovered that sleep quality was the mediator between coping style and mental health and between social support and mental health. Positive and negative coping styles could significantly predict mental health status and also had an impact on mental health status through the mediating effect of social support. Our findings provided a valuable theoretical reference for improving the mental health of medical students. Future clinical practice could formulate intervention strategies based on these findings to improve the mental health of medical students and help cultivate future doctors with healthy psychological characteristics.
Human Ethnics Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Zhujiang Hospital (protocol code 2021-KY-005-01 and date of approval February 10, 2021). Informed Consent Statement: Informed consent was obtained from all subjects involved in the study.
Acknowledgments
Thank all colleagues, relatives and friends who helped distribute the questionnaire. Thank Maoyuan Wang, Ziyi Tang, Wen Fang and all the students for their valuable suggestions and feedback on the questionnaire design, and all participants for their active cooperation. Wish you all the best.
Funding
This work was supported by Education Reform Research Fund of Higher Education of Hunan Province (grant number HNJG-2021-1219) and Science and Technology Program of Guangzhou (grant number 202002020046).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hill MR, Goicochea S, Merlo LJ. In their own words: stressors facing medical students in the millennial generation. Med Educ Online. 2018;23(1):1530558. PubMed: 30286698. doi:10.1080/10872981.2018.1530558
2. Slavin SJ, Schindler DL, Chibnall JT. Medical student mental health 3.0: improving student wellness through curricular changes. Acad Med. 2014;89(4):573–577. PubMed: 24556765. doi:10.1097/ACM.0000000000000166
3. Pisaniello MS, Asahina AT, Bacchi S, et al. Effect of medical student debt on mental health, academic performance and specialty choice: a systematic review. BMJ Open. 2019;9(7):e029980. PubMed: 31270123. doi:10.1136/bmjopen-2019-029980
4. Heiman N, Davis R, Rothberg B. A deeper understanding of depression and suicidality among medical students. Med Teach. 2019;41(6):711–713. doi:10.1080/0142159X.2018.1467559
5. Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among US. and Canadian medical students. Acad Med. 2006;81(4):354–373. PubMed: 16565188. doi:10.1097/00001888-200604000-00009
6. Bond KS, Jorm AF, Kitchener BA, Reavley NJ. Mental health first aid training for Australian medical and nursing students: an evaluation study. BMC Psychol. 2015;3(1):11. PubMed: 25914827. doi:10.1186/s40359-015-0069-0
7. Fletcher I, Castle M, Scarpa A, Myers O, Lawrence E. An exploration of medical student attitudes towards disclosure of mental illness. Med Educ Online. 2020;25(1):1727713. PubMed: 32054420. doi:10.1080/10872981.2020.1727713
8. Eley DS, Bansal V, Leung J. Perfectionism as a mediator of psychological distress: implications for addressing underlying vulnerabilities to the mental health of medical students. Med Teach. 2020;42(11):1301–1307. doi:10.1080/0142159X.2020.1805101
9. AlFaris E, Irfan F, Qureshi R, et al. Health professions’ students have an alarming prevalence of depressive symptoms: exploration of the associated factors. Bmc Med Educ. 2016;16(1):279. PubMed: 27769235. doi:10.1186/s12909-016-0794-y
10. Moutinho I, Lucchetti A, Ezequiel O, Lucchetti G. Mental health and quality of life of Brazilian medical students: incidence, prevalence, and associated factors within two years of follow-up. Psychiatry Res. 2019;274:306–312. PubMed: 30831455. doi:10.1016/j.psychres.2019.02.041
11. Fond G, Bourbon A, Boucekine M, et al. First-year French medical students consume antidepressants and anxiolytics while second-years consume non-medical drugs. J Affect Disord. 2020;265:71–76. PubMed: 31957694. doi:10.1016/j.jad.2020.01.035
12. Fond G, Bourbon A, Micoulaud-Franchi JA, Auquier P, Boyer L, Lançon C. Psychiatry: a discipline at specific risk of mental health issues and addictive behavior? Results from the national BOURBON study. J Affect Disord. 2018;238:534–538. PubMed: 29936392. doi:10.1016/j.jad.2018.05.074
13. Brazeau CM, Shanafelt T, Durning SJ, et al. Distress among matriculating medical students relative to the general population. Acad Med. 2014;89(11):1520–1525. PubMed: 25250752. doi:10.1097/ACM.0000000000000482
14. Worobetz A, Retief PJ, Loughran S, et al. A feasibility study of an exercise intervention to educate and promote health and well-being among medical students: the ‘MED-WELL’ programme. Bmc Med Educ. 2020;20(1):183. PubMed: 32493427. doi:10.1186/s12909-020-02097-2
15. Burger P, Scholz M. Gender as an underestimated factor in mental health of medical students. Ann Anat. 2018;218:1–6. PubMed: 29551695. doi:10.1016/j.aanat.2018.02.005
16. Seera G, Arya S, Sethi S, Nimmawitt N, Ratta-Apha W. Help-seeking behaviors for mental health problems in medical students: studies in Thailand and India. Asian J Psychiatr. 2020;54:102453. PubMed: 33271732. doi:10.1016/j.ajp.2020.102453
17. Cook AF, Arora VM, Rasinski KA, Curlin FA, Yoon JD. The prevalence of medical student mistreatment and its association with burnout. Acad Med. 2014;89(5):749–754. PubMed: 24667503. doi:10.1097/ACM.0000000000000204
18. Dyrbye L, Shanafelt T. A narrative review on burnout experienced by medical students and residents. Med Educ. 2016;50(1):132–149. PubMed: 26695473. doi:10.1111/medu.12927
19. Cuttilan AN, Sayampanathan AA, Ho RC. Mental health issues amongst medical students in Asia: a systematic review [2000–2015]. Ann Transl Med. 2016;4(4):72. PubMed: 27004219. doi:10.3978/j.issn.2305-5839.2016.02.07
20. Gold JA, Hu X, Huang G, et al. Medical student depression and its correlates across three international medical schools. World J Psychiatry. 2019;9(4):65–77. PubMed: 31799151. doi:10.5498/wjp.v9.i4.65
21. Zeng W, Chen R, Wang X, Zhang Q, Deng W. Prevalence of mental health problems among medical students in China: a meta-analysis. Medicine. 2019;98(18):e15337. PubMed: 31045774. doi:10.1097/MD.0000000000015337
22. Maser B, Danilewitz M, Guérin E, Findlay L, Frank E. Medical student psychological distress and mental illness relative to the general population: a Canadian cross-sectional survey. Acad Med. 2019;94(11):1781–1791. PubMed: 31436626. doi:10.1097/ACM.0000000000002958
23. Manfro GG, Graeff-Martins AS, Biolo A, Leitão C, Kliemann L. Mental health initiatives for medical students in Brazil. Lancet Psychiatry. 2019;6(11):e26. PubMed:31631878. doi:10.1016/S2215-0366(19)30391-8
24. Chen X, Liu T, Luo J, Ren S. Data for teenagers’ stressor, mental health, coping style, social support, parenting style and self-efficacy in South China. Data Brief. 2020;29:105202. PubMed: 32071981. doi:10.1016/j.dib.2020.105202
25. Benyamini Y, Gefen-Bardarian Y, Gozlan M, Tabiv G, Shiloh S, Kokia E. Coping specificity: the case of women coping with infertility treatments. Psychol Health. 2008;23(2):221–241. PubMed: 25160052. doi:10.1080/14768320601154706
26. Li Z, Yi X, Zhong M, et al. Psychological distress, social support, coping style, and perceived stress among medical staff and medical students in the early stages of the COVID-19 epidemic in China. Front Psychiatry. 2021;12:664808. PubMed: 34140903. doi:10.3389/fpsyt.2021.664808
27. Wu S, Xu Z, Zhang Y, Liu X. Relationship among psychological capital, coping style and anxiety of Chinese college students. Riv Psichiatr. 2019;54(6):264–268. PubMed: 31909753. doi:10.1708/3281.32545
28. Zhao L, Sznajder K, Cheng D, Wang S, Cui C, Yang X. Coping styles for mediating the effect of resilience on depression among medical students in web-based classes during the COVID-19 pandemic: cross-sectional questionnaire study. J Med Internet Res. 2021;23(6):e25259. PubMed: 34033579. doi:10.2196/25259
29. Reeve KL, Shumaker CJ, Yearwood EL, Crowell NA, Riley JB. Perceived stress and social support in undergraduate nursing students’ educational experiences. Nurse Educ Today. 2013;33(4):419–424. PubMed: 23246284. doi:10.1016/j.nedt.2012.11.009
30. Yalçın İ. Relationships between well-being and social support: a meta analysis of studies conducted in Turkey. Turk Psikiyatri Derg. 2015;26(1):21–32. PubMed:25742034.
31. Karaca A, Yildirim N, Cangur S, Acikgoz F, Akkus D. Relationship between mental health of nursing students and coping, self-esteem and social support. Nurse Educ Today. 2019;76:44–50. PubMed: 30769177. doi:10.1016/j.nedt.2019.01.029
32. Thompson G, McBride RB, Hosford CC, Halaas G. Resilience among medical students: the role of coping style and social support. Teach Learn Med. 2016;28(2):174–182. PubMed: 27064719. doi:10.1080/10401334.2016.1146611
33. Yamada Y, Klugar M, Ivanova K, Oborna I. Psychological distress and academic self-perception among international medical students: the role of peer social support. Bmc Med Educ. 2014;14:256. PubMed: 25430069. doi:10.1186/s12909-014-0256-3
34. Lawton R, Conner M, Parker D. Beyond cognition: predicting health risk behaviors from instrumental and affective beliefs. Health Psychol. 2007;26(3):259–267. PubMed: 17500612. doi:10.1037/0278-6133.26.3.259
35. Blake H, Stanulewicz N, Mcgill F. Predictors of physical activity and barriers to exercise in nursing and medical students. J Adv Nurs. 2017;73(4):917–929. PubMed: 27731886. doi:10.1111/jan.13181
36. Kiran F, Javaid A. Students’ perceptions of factors for academic failure in pre-clinical years of a medical school. J Pak Med Assoc. 2020;70(5):803–808. PubMed: 32400731. doi:10.5455/JPMA.19548
37. Popa-Velea O, Diaconescu L, Mihăilescu A, Jidveian PM, Macarie G. Burnout and its relationships with alexithymia, stress, and social support among Romanian medical students: a cross-sectional study. Int J Environ Res Public Health. 2017;14(6):560. PubMed: 28587094. doi:10.3390/ijerph14060560
38. Masten R, Tusak M, Zalar B, Ziherl S. Stress, coping and social support in three groups of university students. Psychiatr Danub. 2009;21(1):41–48. PubMed:19270620.
39. Gazmararian J, Baker D, Parker R, Blazer DG. A multivariate analysis of factors associated with depression: evaluating the role of health literacy as a potential contributor. Arch Intern Med. 2000;160(21):3307–3314. PubMed: 11088094. doi:10.1001/archinte.160.21.3307
40. Stewart DW, Reitzel LR, Correa-Fernández V, et al. Social support mediates the association of health literacy and depression among racially/ethnically diverse smokers with low socioeconomic status. J Behav Med. 2014;37(6):105202–105279. PubMed: 25391450. doi:10.1007/s10865-014-9566-5
41. Zhong Y, Schroeder E, Gao Y, Guo X, Gu Y. Social support, health literacy and depressive symptoms among medical students: an analysis of mediating effects. Int J Environ Res Public Health. 2021;18(2):633. PubMed: 33451118. doi:10.3390/ijerph18020633
42. Dunn LB, Iglewicz A, Moutier C. A conceptual model of medical student well-being: promoting resilience and preventing burnout. Acad Psychiatry. 2008;32(1):44–53. PubMed: 18270280. doi:10.1176/appi.ap.32.1.44
43. Heinen I, Bullinger M, Kocalevent RD. Perceived stress in first year medical students - associations with personal resources and emotional distress. Bmc Med Educ. 2017;17(1):4. PubMed: 28056972. doi:10.1186/s12909-016-0841-8
44. Zhu Y, Guo J, Luo S, Li M, Hu S, Dong Y. Revision, reliability and validity of simplified coping style questionnaire in the elderly. Chin J Health Stat. 2016;4(33):660–664.
45. Xie Y. A preliminary study on the reliability and validity of the simplified coping style questionnaire. Chin J Clin Psychol. 1998;2(6):114–115.
46. Nie A, Su X, Zhang S, Guan W, Li J. Psychological impact of COVID-19 outbreak on frontline nurses: a cross-sectional survey study. J Clin Nurs. 2020;29(21–22):4217–4226. PubMed: 32786150. doi:10.1111/jocn.15454
47. Yan F, Tang S, Goldsamt L, Wang H, Chen J, Li X. Interrelationships between intimate partner violence, coping style, depression, and quality of life among the regular female sexual partners of men who have sex with men. J Interpers Violence. 2020:886260520917519. PubMed: 32390497. doi:10.1177/0886260520917519
48. Wu W, Zhang Y, Goldsamt L, Yan F, Wang H, Li X. The mediating role of coping style: associations between intimate partner violence and suicide risks among Chinese wives of men who have sex with men. J Interpers Violence. 2021;36(11–12):NP6304–NP6322. PubMed: 30484367. doi:10.1177/0886260518814264
49. Huang L, Jiang Q. Correlation between coping style, social support and psychosomatic symptoms of cancer patients. Chin Mental Health J. 1996;4(10):160–161.
50. Choi AMK, Moon JE, Friedman RA. Meeting the challenges of medical student mental health and well-being today. Med Educ. 2020;54(3):183–185. doi:10.1111/medu.14064
51. Blumenthal JA, Burg MM, Barefoot J, Williams RB, Haney T, Zimet G. Social support, type A behavior, and coronary artery disease. Psychosom Med. 1987;49(4):331–340. PubMed: 3615762. doi:10.1097/00006842-198707000-00002
52. Li Y, Long Z, Cao D, Cao F. Social support and depression across the perinatal period: a longitudinal study. J Clin Nurs. 2017;26(17–18):2776–2783. PubMed: 28334472. doi:10.1111/jocn.13817
53. Yu M, Qiu T, Liu C, Cui Q, Wu H. The mediating role of perceived social support between anxiety symptoms and life satisfaction in pregnant women: a cross-sectional study. Health Qual Life Outcomes. 2020;18(1):223. PubMed: 32650793. doi:10.1186/s12955-020-01479-w
54. Gan SW, Ong LS, Lee CH, Lin YS. Perceived social support and life satisfaction of Malaysian Chinese young adults: the mediating effect of loneliness. J Genet Psychol. 2020;181(6):458–469. PubMed: 32787705. doi:10.1080/00221325.2020.1803196
55. Judd LL, Schettler PJ, Rush AJ. A brief clinical tool to estimate individual patients’ risk of depressive relapse following remission: proof of concept. Am J Psychiatry. 2016;173(11):1140–1146. PubMed: 27418380. doi:10.1176/appi.ajp.2016.15111462
56. Grabe HJ, Frommer J, Ankerhold A, et al. Alexithymia and outcome in psychotherapy. Psychother Psychosom. 2008;77(3):189–194. PubMed: 18332617. doi:10.1159/000119739
57. Hou H, Feng X, Li Y, et al. Suboptimal health status and psychological symptoms among Chinese college students: a perspective of predictive, preventive and personalised health. Epma J. 2018;9(4):367–377. PubMed: 30538788. doi:10.1007/s13167-018-0148-4
58. Kwak SG, Kim JH. Central limit theorem: the cornerstone of modern statistics. Korean J Anesthesiol. 2017;70(2):144–156. PubMed: 28367284. doi:10.4097/kjae.2017.70.2.144
59. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. PubMed: 3806354. doi:10.1037//0022-3514.51.6.1173
60. Xu N, Liu Y. Coping strategy mediates the relationship between body image evaluation and mental health: a study with Chinese college students with disabilities. Disabil Health J. 2020;13(1):100830. PubMed: 31399346. doi:10.1016/j.dhjo.2019.100830
61. Huang Y, Su X, Si M, et al. The impacts of coping style and perceived social support on the mental health of undergraduate students during the early phases of the COVID-19 pandemic in China: a multicenter survey. Bmc Psychiatry. 2021;21(1):530. PubMed: 34706690. doi:10.1186/s12888-021-03546-y
62. João K, Jesus SN, Carmo C, Pinto P. The impact of sleep quality on the mental health of a non-clinical population. Sleep Med. 2018;46:69–73. PubMed: 29773214. doi:10.1016/j.sleep.2018.02.010
63. Hertenstein E, Feige B, Gmeiner T, et al. Insomnia as a predictor of mental disorders: a systematic review and meta-analysis. Sleep Med Rev. 2019;43:96–105. PubMed: 30537570. doi:10.1016/j.smrv.2018.10.006
64. Wang Q, Zhang J, Wang R, et al. Sleep quality as a mediator of the association between coping styles and mental health: a population-based ten-year comparative study in a Chinese population. J Affect Disord. 2021;283:147–155. doi:10.1016/j.jad.2021.01.045
65. Zhang Y, Peters A, Bradstreet J. Relationships among sleep quality, coping styles, and depressive symptoms among college nursing students: a multiple mediator model. J Prof Nurs. 2018;34(4):320–325. doi:10.1016/j.profnurs.2017.12.004
66. Ando M. Relationships among mental health, coping styles, and mood. Psychol Rep. 2002;90(2):606–612. PubMed: 12061603. doi:10.2466/pr0.2002.90.2.606
67. Lakey B, Orehek E. Relational regulation theory: a new approach to explain the link between perceived social support and mental health. Psychol Rev. 2011;118(3):482–495. PubMed: 21534704. doi:10.1037/a0023477
68. Ozaki A, Horiuchi S, Kobayashi Y, et al. Beneficial roles of social support for mental health vary in the Japanese population depending on disaster experience: a nationwide cross-sectional study. Tohoku J Exp Med. 2018;246(4):213–223. PubMed: 30542048. doi:10.1620/tjem.246.213
69. Sengoelge M, Solberg Ø, Nissen A, Saboonchi F. Exploring social and financial hardship, mental health problems and the role of social support in asylum seekers using structural equation modelling. Int J Environ Res Public Health. 2020;17(19):6948. PubMed: 32977521. doi:10.3390/ijerph17196948
70. Wang Y, Wang P. Perceived stress and psychological distress among Chinese physicians: the mediating role of coping style. Medicine. 2019;98(23):e15950. PubMed: 31169719. doi:10.1097/MD.0000000000015950
71. Yussuf AD, Issa BA, Ajiboye PO, Buhari OI. The correlates of stress, coping styles and psychiatric morbidity in the first year of medical education at a Nigerian University. Afr J Psychiatry. 2013;16(3):206–215. PubMed: 23739824. doi:10.4314/ajpsy.v16i3.28
72. Zou P, Wang X, Sun L, et al. Poorer sleep quality correlated with mental health problems in college students: a longitudinal observational study among 686 males. J Psychosom Res. 2020;136:110177. PubMed: 32623194. doi:10.1016/j.jpsychores.2020.110177
73. Tao S, Wu X, Zhang Y, Zhang S, Tong S, Tao F. Effects of sleep quality on the association between problematic mobile phone use and mental health symptoms in Chinese college students. Int J Environ Res Public Health. 2017;14(2):185. PubMed: 28216583. doi:10.3390/ijerph14020185
74. Pacheco JP, Giacomin HT, Tam WW, et al. Mental health problems among medical students in Brazil: a systematic review and meta-analysis. Braz J Psychiatry. 2017;39(4):369–378. PubMed: 28876408. doi:10.1590/1516-4446-2017-2223
75. Slavish DC, Taylor DJ, Lichstein KL. Intraindividual variability in sleep and comorbid medical and mental health conditions. Sleep. 2019;42(6). PubMed: 30843059. doi:10.1093/sleep/zsz052
76. Bah TM, Goodman J, Iliff JJ. Sleep as a therapeutic target in the aging brain. Neurotherapeutics. 2019;16(3):554–568. PubMed: 31376067. doi:10.1007/s13311-019-00769-6
77. Sakamaki R, Toyama K, Amamoto R, Liu CJ, Shinfuku N. Nutritional knowledge, food habits and health attitude of Chinese university students--a cross sectional study. Nutr J. 2005;4:4. PubMed: 15703071. doi:10.1186/1475-2891-4-4
78. Ul HI, Mariyam Z, Li M, et al. A comparative study of nutritional status, Knowledge Attitude and Practices (KAP) and dietary intake between international and Chinese Students in Nanjing, China. Int J Environ Res Public Health. 2018;15(9). PubMed: 30177588. doi:10.3390/ijerph15091910
79. Bede F, Cumber SN, Nkfusai CN, et al. Dietary habits and nutritional status of medical school students: the case of three state universities in Cameroon. Pan Afr Med J. 2020;35(15). PubMed: 32341736. doi:10.11604/pamj.2020.35.15.18818
80. Fukushima K, Fukushima N, Sato H, Yokota J, Uchida K. Association between nutritional level, menstrual-related symptoms, and mental health in female medical students. PLoS One. 2020;15(7):e0235909. PubMed: 32658906. doi:10.1371/journal.pone.0235909
81. Arab A, Mehrabani S, Moradi S, Amani R. The association between diet and mood: a systematic review of current literature. Psychiatry Res. 2019;271:428–437. PubMed: 30537665. doi:10.1016/j.psychres.2018.12.014
82. O’Brien PM, Selby C, Symonds EM. Progesterone, fluid, and electrolytes in premenstrual syndrome. Br Med J. 1980;280(6224):1161–1163. PubMed: 7190047. doi:10.1136/bmj.280.6224.1161
83. Toffoletto S, Lanzenberger R, Gingnell M, Sundström-Poromaa I, Comasco E. Emotional and cognitive functional imaging of estrogen and progesterone effects in the female human brain: a systematic review. Psychoneuroendocrino. 2014;50:28–52. PubMed: 25222701. doi:10.1016/j.psyneuen.2014.07.025
84. Lin J, Su Y, Lv X, et al. Perceived stressfulness mediates the effects of subjective social support and negative coping style on suicide risk in Chinese patients with major depressive disorder. J Affect Disord. 2020;265:32–38. PubMed: 31959583. doi:10.1016/j.jad.2020.01.026
85. Zhang X, Wang H, Xia Y, Liu X, Jung E. Stress, coping and suicide ideation in Chinese college students. J Adolesc. 2012;35(3):683–690. PubMed: 22032975. doi:10.1016/j.adolescence.2011.10.003
86. Zhang C, Ye M, Fu Y, et al. The psychological impact of the COVID-19 pandemic on teenagers in China. J Adolesc Health. 2020;67(6):747–755. PubMed: 33041204. doi:10.1016/j.jadohealth.2020.08.026
87. Zheng Z, Han W, Zhou Y, Zhang N. Childhood maltreatment and depression in adulthood in Chinese female college students: the mediating effect of coping style. Front Psychiatry. 2020;11:581564. PubMed: 33240133. doi:10.3389/fpsyt.2020.581564
88. Hollifield M, Hewage C, Gunawardena CN, Kodituwakku P, Bopagoda K, Weerarathnege K. Symptoms and coping in Sri Lanka 20–21 months after the 2004 tsunami. Br J Psychiatry. 2008;192(1):39–44. PubMed: 18174508. doi:10.1192/bjp.bp.107.038422
89. Carrieri D, Mattick K, Pearson M, et al. Optimising strategies to address mental ill-health in doctors and medical students: ‘care under pressure’ realist review and implementation guidance. Bmc Med. 2020;18(1). doi:10.1186/s12916-020-01532-x
90. Bell CM, Ridley JA, Overholser JC, et al. The role of perceived burden and social support in suicide and depression. Suicide Life Threat Behav. 2018;48(1):87–94. PubMed: 28093796. doi:10.1111/sltb.12327
91. Wang J, Mann F, Lloyd-Evans B, Ma R, Johnson S. Associations between loneliness and perceived social support and outcomes of mental health problems: a systematic review. Bmc Psychiatry. 2018;18(1):156. PubMed: 29843662. doi:10.1186/s12888-018-1736-5
92. Garcia MV, Luckett T, Johnson M, Hutchinson A, Lal S, Phillips JL. The roles of dispositional coping style and social support in helping people with respiratory disease cope with a breathlessness crisis. J Adv Nurs. 2019;75(9):1953–1965. PubMed: 31012133. doi:10.1111/jan.14039
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.