Back to Journals » Nature and Science of Sleep » Volume 15
Sleep Reactivity and Related Factors in Adolescence: An Increased Risk for Insomnia? A Longitudinal Assessment
Authors Kater MJ ![]() , Werner A, Schlarb AA, Lohaus A
, Werner A, Schlarb AA, Lohaus A
Received 14 December 2022
Accepted for publication 25 March 2023
Published 11 April 2023 Volume 2023:15 Pages 207—216
DOI https://doi.org/10.2147/NSS.S401452
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Maren-Jo Kater,1 Anika Werner,1 Angelika Anita Schlarb,2 Arnold Lohaus1
1Faculty of Psychology and Sports Science, Department of Developmental Psychology and Developmental Psychopathology, Bielefeld University, Bielefeld, North Rhine Westphalia, Germany; 2Faculty of Psychology and Sports Science Clinical, Department of Psychology and Psychotherapy of Children and Adolescents, Bielefeld University, Bielefeld, North Rhine Westphalia, Germany
Correspondence: Maren-Jo Kater, Bielefeld University, Faculty of Psychology and Sports Science, Developmental Psychology and Developmental Psychopathology, P.O. Box 10 01 31, Bielefeld, 33501, Germany, Tel +49 0521 - 106 4461, Email [email protected]
Purpose: The individual vulnerability for stress-related sleep difficulties (eg, sleep reactivity) is known as a predisposing factor of insomnia in adults, yet relatively little is known about sleep reactivity in adolescence. The study goal is to determine factors related to sleep reactivity and to investigate whether sleep reactivity and related factors predict current and new incidents of insomnia in adolescents.
Patients and Methods: At baseline, 11-to-17-year-olds (N = 185, Mage = 14.3 years, SD = 1.8, 54% female) answered an age-appropriate version of the Ford Insomnia Response to Stress Test, questionnaires about sleep, stress, psychological symptoms, and resources, filled out a sleep diary and used actigraphy. Insomnia diagnoses according to ISCD-3 criteria were assessed at baseline, after 9 months and after one and a half years.
Results: Adolescents with high compared to low sleep reactivity had increased pre-sleep arousal, negative sleep-related cognitions, pre-sleep mobile phone use, stress experience, stress vulnerability, internalizing and externalizing symptoms, less social resources, and a later midpoint of bedtime. High sleep reactivity increased the likelihood for currently having insomnia, but not for the development of insomnia at subsequent assessments.
Conclusion: The findings suggest that high sleep reactivity is related to poor sleep health and mental health but cast doubt on sleep reactivity as a pivotal predisposing factor for the development of insomnia in adolescence.
Keywords: sleep vulnerability, sleep disorder, mental health, stress, resources, youth
Introduction
Insufficient sleep including difficulties initiating and maintaining sleep are common in adolescence as this developmental period is sensitive for the onset of insomnia.1 Prevalence rates range between 4% and 39%, depending on the diagnostic criteria, with strong sex differences emerging after puberty onset.2 According to the diathesis-stress model and Spielman’s three-factor (3P) model of insomnia, stressful events are a common precipitating factor triggering insomnia. How strongly stress impacts sleep is modulated by predisposing individual factors. One of them is the phenomenon known as sleep reactivity, which describes the individual vulnerability to react towards stress with acute sleep difficulties and is understood as a trait characteristic with a high situational stability.3 Individuals with high sleep reactivity are more vulnerable to having difficulties falling and staying asleep during stress periods, and also after the removal of stress, while those with low sleep reactivity experience mild sleep problems and mostly return to normal without persistent difficulties.3 Commonly measured by the Ford Insomnia Response to Stress Test (FIRST), previous research in adults has shown that sleep reactivity as a predisposing factor predicts not only the likelihood of current insomnia and the incidence of insomnia, but also the intensity of insomnia symptoms.4–6 In adult samples, high sleep reactivity was associated with negative sleep beliefs, mental health problems (eg, disordered-eating behaviors, social anxiety, and depression), personal characteristics and coping skills (eg, more emotion-oriented coping, rumination and neuroticism), and low resilience.7–11 Previous studies confirmed the sleep reactivity model for insomnia in adulthood, but little is known about adolescence as a challenging and rapidly changing developmental stage where social, personal, and cognitive changes, and a lack of adaptive coping and emotion regulation skills endanger positive trajectories.12,13 Exploring youth-specific predisposing and precipitating factors, including age, pubertal status, and sex, related to sleep reactivity might help to understand this stage’s contribution to the incidence of insomnia.
The degree of stressful experiences, stress vulnerability, internalizing and externalizing symptoms, sleep and bedtime behaviors (ie, mobile phone use and midpoint of time in bed), as well as resources were considered in this study with the objective to determine in adolescents (1) which of these risk factors are related in adolescents with high sleep reactivity, and (2) whether, as we hypothesize, high sleep reactivity and related factors predict the likelihood of current insomnia, (3) and the incidence of insomnia 9, respectively, 17 months later.
Materials and Methods
Sample and Procedure
The sample included 185 adolescents between 11 and 17 years of age (Mage = 14.3 years, SD = 1.8, 54% female) at baseline (T1). At the time of inclusion, the participants attended school in grades 5 to 12 (2% 5th grade, 12% 6th grade, 10% 7th grade, 16% 8th grade, 17% 9th grade, 25% 10th grade, 9% 11th grade, 9% 12th grade) and most often a grammar school (Gymnasium; 45%). They were mostly of German origin (92%) and lived in the district of North Rhine-Westphalia, Germany. All participants and their caregivers provided informed consent to participate in the study, after being recruited via social media, newspapers, flyers, or direct contact at school. Participation was not recommended in cases of (diagnosed) mental health disorder or heart disease and was monetarily incentivized by vouchers worth 140€ (for participation at all assessment waves). The study was funded by the German Research Foundation (DFG) and approved by the local ethics committee of the university.
Adolescent’s self-reports on sleep reactivity, stress, sleep, and sleep-related behaviors were filled out online at home, while more sensitive questionnaires about mental health symptoms were completed at a personal university appointment along with a sleep interview (see Supporting Information for detailed information). After 8.9 ± 1.5 (T2) and 17.1 ± 2.0 (T3) months participants were invited again for a sleep interview.
Measurements
Sleep Reactivity
The German children and adolescent version of the Ford Insomnia Response to Stress Test (FIRST) assesses sleep reactivity, eg, the vulnerability for stress-related sleep disturbances.14 Nine items measure the probability of having difficulties to sleep due to specific and common stressful events or periods of stress occurring during this day or the next day (eg, after a bad school day, before an oral presentation in class) from (1) never to (4) always. Previous studies have demonstrated good psychometric properties in adults.14,15 For our adolescent sample, we found a good internal consistency (α = 0.84) and good fit for a one-factor solution (see Supporting Information). The resulting total score ranges from 9 to 36, with higher values showing greater vulnerability to stress-related insomnia. In this study, we applied the clinical cut-off of FIRST ≥ 18 proposed by Kalmbach et al,6 which reflects a high vulnerability for future insomnia.
Insomnia
In accordance with the International Classification of Sleep Disorders (3rd ed.; ICSD-3), insomnia was diagnosed if an adolescent reported difficulties falling asleep or staying asleep (despite having an adequate opportunity to sleep), resulting in significant distress and daytime consequences (eg, sleepiness, difficulties with concentration and memory, mood lability, social or school difficulties).16 Insomnia was diagnosed if the criteria were fulfilled for at least one month, indicating at least an acute insomnia of relative endurance.
Sleep
Continuous sleep was assessed by two-week of sleep diary and one-week of actigraphy (MotionWatch 8, CamTech, United Kingdom). At least four nights of measurements had to be available for the average total sleep time (TST) and sleep onset latency (SOL) to be extracted from actigraphy.
Moreover, the average perceived sleep quality was extracted from sleep diary evaluated from (1) very good to (6) very bad. (Pre-) sleep behavior was assessed by midpoint of time in bed (TIB), indicating the average bedtime schedule, and pre-sleep mobile phone use. The average midpoint of TIB was extracted from actigraphy calculated as the midpoint between bedtimes in the evening and rising times in the morning (time going to bed +(TIB/2)). The average duration of pre-sleep mobile phone use was captured via the sleep diary by the following item “Did you use your smartphone in bed at night? If yes, how long? (In minutes)”. The Pre-Sleep Arousal Scale (α = 0.87) is a 15-item measure assessing somatic and cognitive pre-sleep arousal on a response scale ranging from (1) not at all to (5) extremely (α = 0.89).17 The subscale negative sleep-related cognitions of the questionnaire on sleep-related cognitions measures catastrophizing thinking, sleep drug use, and sleep anxiety by 18 items answered on a scale ranging from (1) nearly never to (4) nearly always (α = 0.91).18
Stress
The intensity of stress experiences regarding potentially daily stressful experiences or situations was captured by the Adolescent Stress Questionnaire-S (ASQ-S) on nine domains.19 Twenty-seven items are rated on a response scale from (1) not stressful at all/did not occur to (5) very stressful (α = 0.92). The subscale stress vulnerability of the Stress and Coping Questionnaire for Children and Adolescents (SSKJ 3-8-R) measured the extent of stress vulnerability in everyday life situations of adolescents.20 Anticipated stress towards seven situations was evaluated on a response scale ranging from (1) no stress at all to (4) very much stress. A higher total sum score indicates higher vulnerability to potential stressors (α = 0.75).
Mental Health
Indicators of mental health were assessed by the internalizing and externalizing symptom scales of the Youth Self Report (YSR 11–18R; αinternalizing = 0.89; αexternalizing = 0.87).21
Resources
The Questionnaire on Resources in Childhood and Adolescence (FRKJ 8–16) provides an assessment of personal resources (eg, optimism, self-esteem) and social resources (eg, parental social and emotional support, peer group integration) with higher sum scores indicating more perceived social/personal resources (αsocial = 0.91, αpersonal = 0.87).22
Other Variables
At baseline, we obtained demographics including age and sex. The Puberty Development Scale (PDS) evaluated puberty status in five stages from (1) prepubertal to (5) postpubertal.23 The COVID-19-related overall burden was rated by the participants and will be considered as a covariate, as the SARs-CoV-2 pandemic began during the baseline data collection. The item “The current corona situation can trigger uncertainty or fear in people. How strongly do you feel burdened by the current situation?” was answered on a scale ranging from (0) not at all to (5) very much.
Statistical Analysis
At baseline, participants of whom an insomnia diagnosis was missing (n = 15), from whom more than 70% of items were missing (n = 1), and with an age older than 17 (n = 5) were excluded, leaving N = 185 adolescents. Missing values (3%) were replaced with multiple imputation (m = 10) using Multivariate Imputation by Chained Equations (MICE; in R v4.2.1) as a function of scale level (ie, logistic regression for nominal-scaled and predictive mean matching for interval-scaled variables). Only variables that correlated with at least 0.10 were utilized for an imputation. All variables were included in the multiple imputation, including the outcome variables insomnia T1, insomnia T2, and insomnia T3 following recommendations by von Hippel.24 The outcome variables were, however, not imputed themselves. The 10 data sets resulting from the imputation were aggregated and subsequently the total sum and mean scores were calculated for all participants.
Firstly, to address the question of whether and how adolescents with a high sleep reactivity (SR) differed from adolescents with low SR on demographic, sleep, stress, health, and resource parameters, a profile analysis by group (using profileR) tested differences in the profiles of the two groups (high/low SR using the clinical cut-off score of the FIRST) at baseline.25 The profile analysis was calculated based on difference values of the normalized dependent variables. In case of significant profile deviations, these were subsequently investigated using a one-factor multivariate analysis of covariance (MANCOVA) and subsequent post-hoc ANCOVAs based on the raw values (the dichotomous variable sex was examined using Chi-squared tests). COVID-19-related burden was included as covariate. To address the variance heterogeneity, Pillai trace is reported.26
Secondly, to clarify whether SR (low/high) and the related risk factors predict the likelihood of having a current insomnia diagnosis hierarchical logistic binomial regressions were calculated. Therefore, insomnia diagnose (no/yes) at baseline was used as outcome variable. In step 1, sleep reactivity (low/high) was entered. In step 2, all significant variables of the profile analysis were added stepwise to extract the most important predictors.
Thirdly, regarding the longitudinal prediction of new occurrences of insomnia, the second logistic hierarchical regression analysis included the insomnia diagnoses at T2/T3 to test whether sleep reactivity (low/high) and the significant profile variables predict the likelihood of suffering from an insomnia 9/17 months later, when insomnia was not experienced at baseline. For this reason, only adolescents without initial insomnia diagnosis at baseline and completed sleep interviews at T2/T3 were included, resulting in a sample size of N = 93. The outcome variable insomnia T2/T3 was coded as follows: 0 indicated that the participant had no insomnia at T2 nor at T3 (ie, adolescents who did not developed insomnia), 1 indicated an insomnia diagnosis either at T2, at T3 or at both assessments (ie, adolescents who did develop insomnia). The same model steps as outlined for the cross-sectional analysis were performed.
In all analyses, p-values < 0.05 indicate significant results. In analyses of variance, partial η2 indicates a small effect at >0.01, a medium effect at >0.06, and a large effect at >0.14. Regarding the logistic regression models, the odds ratio (OR) coefficient is reported. Nagelkerke’s R² indicates small effect at <0.1, modest effect at 0.1 to 0.3, a moderate effect at 0.3 to 0.5, and a strong improvement at >0.5.27
Results
Inspection of Sleep Reactivity
In the total sample, the average SR was 19.14 (SD = 5.31). The discrimination by the cut-off of 18 resulted in significant higher mean SR in those over the cut-off (high SR, n = 111, M = 22.61, SD = 3.60) than those under the cut-off (low SR, n = 74, M = 13.83, SD = 2.33), t (183) = 18.51, p < 0.001, d = 3.16. Sleep reactivity was not associated with COVID-19 related burden, but particularly with pre-sleep arousal, negative sleep-related cognitions, and stress vulnerability (all r > 0.39, p < 0.05).
Which Factors are Concurrent with High Sleep Reactivity?
Profile analysis with group (low/high SR) as the between-subjects factor and possible risk factors (ie, sleep, stress, psychological health, resources, age, pubertal status, and sex) as dependent variables showed that profiles differed significantly between SR groups: There were significant group differences, F (1, 183) = 88.82, p < 0.001, as well as differences between the risk factors, F (15, 169) = 326.70, p < 0.001. A significant interaction of group × risk factors, F (15, 169) =7.31, p < 0.001, Pillai trace = 0.39, indicates that the profiles are not parallel, ie, the groups vary in their profiles. These findings were examined in more detail using post-hoc MANCOVA as well as ANCOVAs controlling for COVID-19-related burden. MANCOVA confirmed the main group effect for sleep reactivity on the set of dependent variables, F (15, 168) = 8.77, p < 0.001, Pillai trace = 0.44, partial η2 = 0.44, 95% CI[0.30, 0.51], but not for COVID-19-related burden as covariate, F (15, 168) = 0.73, p = 0.75, Pillai trace = 0.06, partial η2 = 0.06, 95% CI[0.00, 0.06]. Significant differences (see Table 1) found by sequential ANCOVAs indicated more sleep disturbances, pre-sleep arousal, negative sleep-related cognitions, pre-sleep mobile phone use, stress experience, stress vulnerability, internalizing and externalizing symptoms, as well as less social resources in adolescents with high compared to low sleep reactivity (all p < 0.05). Participants with high SR were more likely to be female, were older, and had higher pubertal status (all p < 0.05).
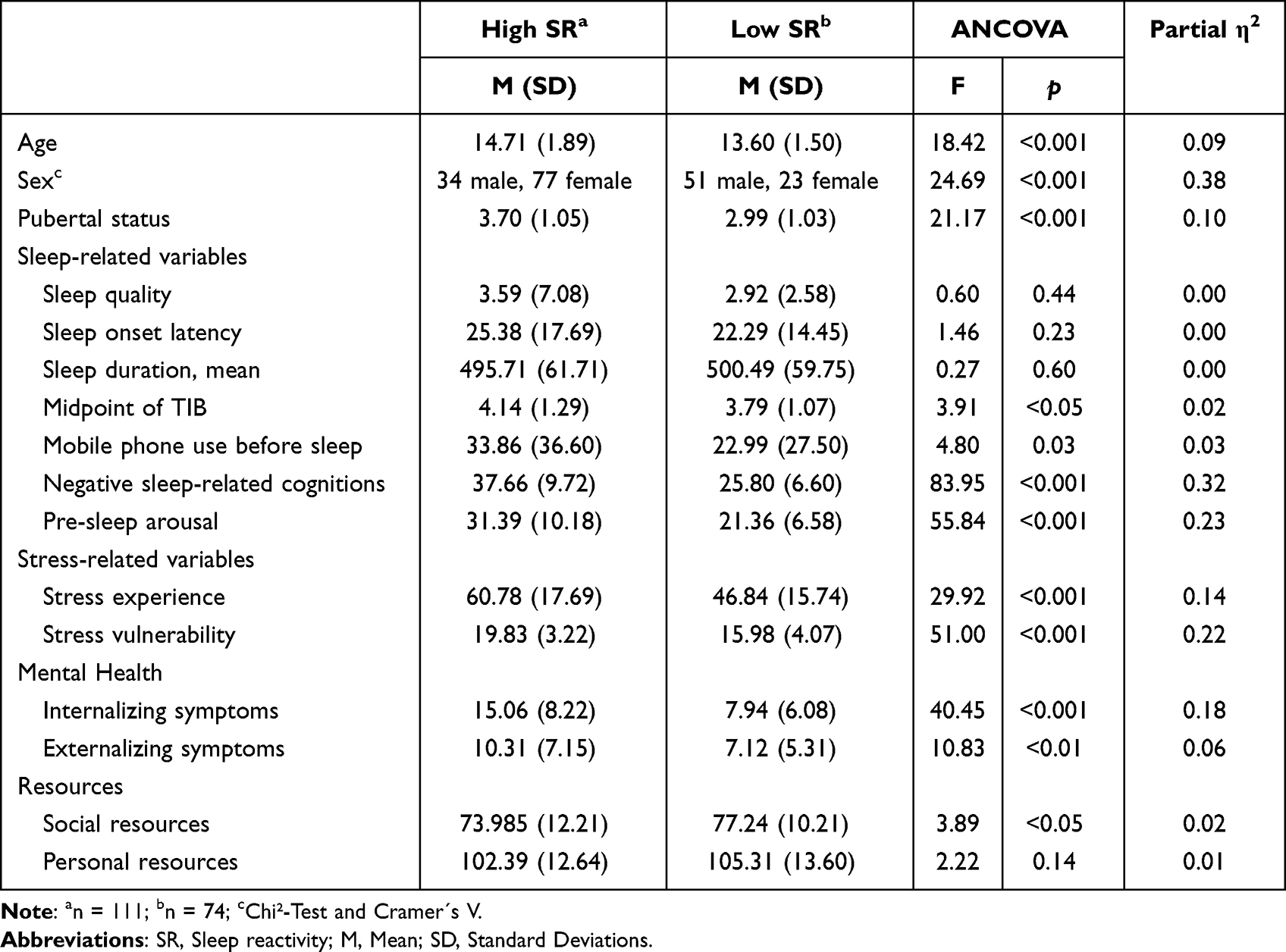 |
Table 1 Means and Standard Deviations for Adolescents with High and Low Sleep Reactivity and Results of the Post-Hoc ANCOVAs for Sleep Reactivity |
Does High Sleep Reactivity Increase the Likelihood of Having a Current Insomnia?
A hierarchical logistic regression analysis was conducted to determine the likelihood of current insomnia for sleep reactivity (high/low) and potential risk factors (ie, age, pubertal status, gender, pre-sleep arousal, negative sleep-related cognitions, pre-sleep mobile phone use, midpoint of TIB, stress experiences, stress vulnerability, internalizing symptoms, externalizing symptoms, and social resources). The results of step 2 showed a significant model (χ²(4) = 42.60, p < 0.001, Nagelkerke’s R² = 0.29; see Table 2). Goodness-of-fit was assessed using the Hosmer-Lemeshow-Test, which indicated a good model fit, χ²(8) = 13.21, p = 0.11. The likelihood of current insomnia increased with high compared to low SR (OR = 2.95; 95% CI[1.19, 7.28], p <. 05), and more negative sleep-related cognitions (OR = 1.05; 95% CI[1.00, 1.09], p < 0.05). In this sample, 12% of adolescents with low SR and 48% of adolescents with high SR had a current insomnia.
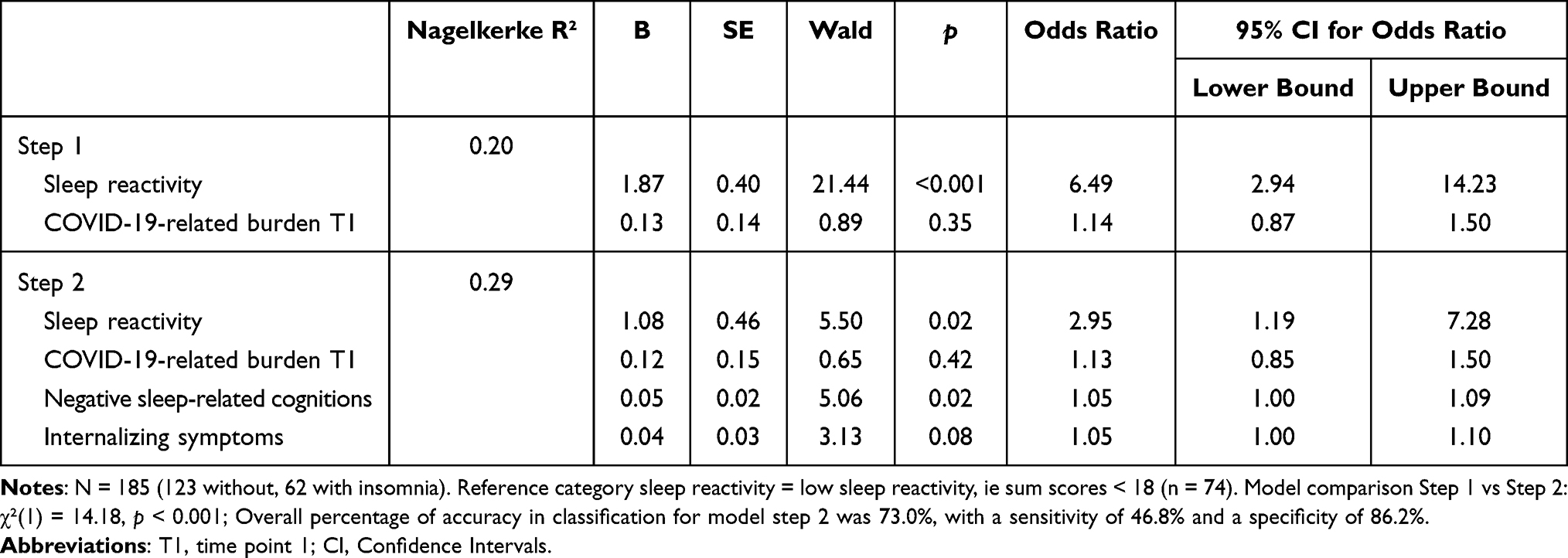 |
Table 2 Results of Hierarchical Binomial Logistic Regression Analyses Predicting Current Insomnia at T1 |
Does High Sleep Reactivity Increase the Likelihood for a Future Incident of Insomnia?
An additional hierarchical logistic regression analysis was conducted to determine the predictive effect of sleep reactivity (low/high) and related risk factors (see above) on the likelihood of developing insomnia 9 or 17 months later.
Predicting insomnia at T2/T3, the results of step 2 showed a significant model (χ²(4) =25.45, p < 0.001, Nagelkerke’s R² = 0.36; see Table 3) with a good model fit (χ²(8) = 4.54, p = 0.81). The likelihood of the development of a new insomnia at T2/T3 increases with female sex (OR = 4.06; 95% CI[1.13, 14.62], p = 0.03) and the level of internalizing symptoms (OR = 1.18; 95% CI[1.07, 1.30], p < 0.001). SR failed to reach significance in predicting the development of insomnia (OR = 0.26; 95% CI[0.06, 1.06], p = 0.06) as in this sample 23% of adolescents with low SR and 26% of adolescents with high SR developed insomnia. In other words, only 52% of participants who developed insomnia had high SR.
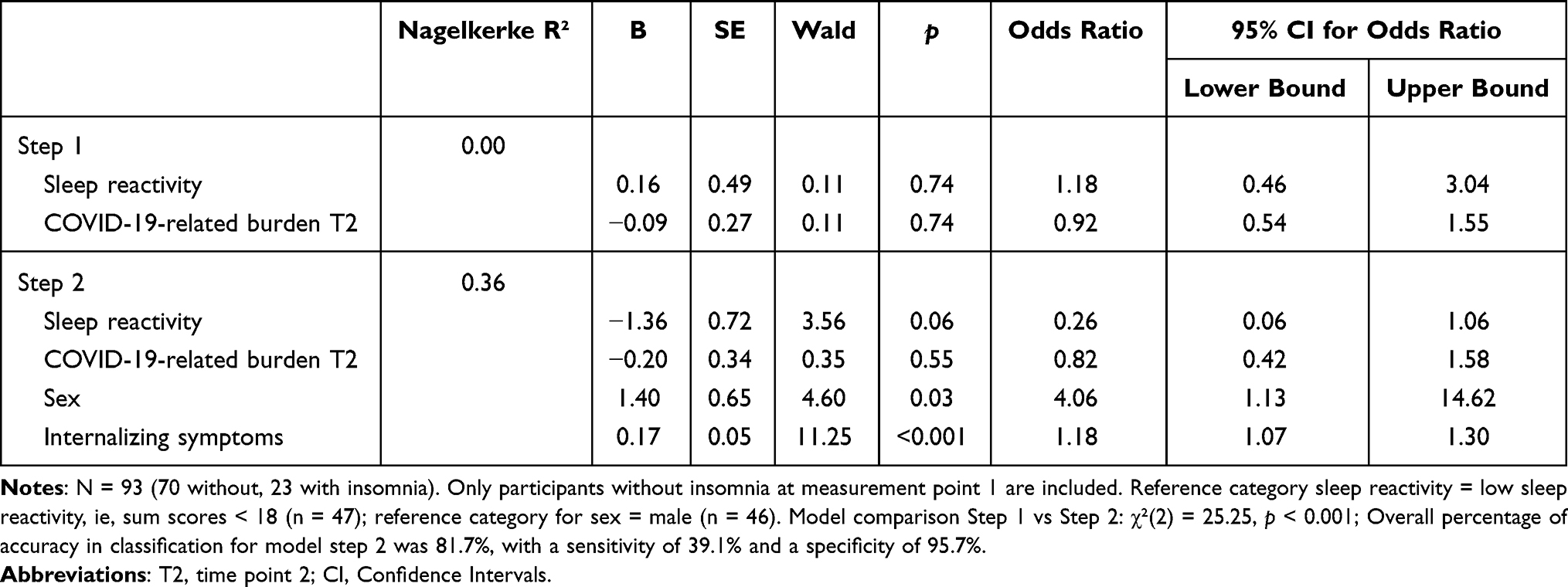 |
Table 3 Results of Hierarchical Binomial Logistic Regression Analyses Predicting the Development of Insomnia T2/T3 |
Discussion
The goals of the present study were to investigate 1) related risk factors for high sleep reactivity, 2) whether high sleep reactivity predicts the likelihood of having current insomnia, and 3) an incident of insomnia 9 or 17 months later in adolescents. Adolescents with high and low SR were found to differ in terms of their age, pre-sleep mobile phone use, midpoint of TIB, negative sleep-related cognitions, pre-sleep arousal, stress experience, stress vulnerability, internalizing and externalizing symptoms, and social resources, with increased difficulties and lower social resources at high sleep reactivity. As expected, the odds for an adolescent with high SR to have a current insomnia were 2.95 times higher than the odds for an adolescent with low SR. Surprisingly, the risk for an insomnia incident 9 or 17 months later did not increase with higher SR levels.
Regarding the related risk factors, as SR is discussed as a sleep-specific facet of stress reactivity, it is not surprising and in line with previous studies in adults that adolescent’s SR is accompanied by more stress vulnerability, by increased stress experiences, and by more internalizing and externalizing symptoms.3,9 Regarding age and gender differences, we found the prevalence of high SR to be more pronounced in older adolescents with a higher pubertal status, and in girls. It may be assumed that older adolescents are more perceptive and aware of the impact of stressful events on their sleep, as older adolescents are more able to consider problems from multiple angles.28 Especially from puberty onwards, gender differences occur, with a pronounced development of rumination and depression (starting age 12 resp. 13) and a greater assignment of importance to stressful situations in girls, which could contribute to high SR particularly in female adolescents.29,30 Although the relationship between SR and sex hormones has so far not been directly investigated, insomnia symptoms, sleep changes, and depressive symptoms are known to be linked to abnormal (high and low) levels and changes in estrogen and progesterone. As progesterone and estrogen are regulators of cortisol secretion,31 and heightened and blunted cortisol levels are related with high SR and insomnia,32,33 sex and stress hormones might interact in their neurobiological contribution to higher SR in females particularly in later pubertal stages. Yet, future research is needed to explore this assumption.
Regarding pre-sleep behaviors, high SR was accompanied by later midpoint of TIB, and more pre-sleep mobile phone use. One might expect the later midpoint of TIB in adolescents with high SR could be driven by a later chronotype conveyed by the higher average age in this group.34 It might also be possible that individuals with higher SR procrastinate more before bedtime, in the assumption that they will then be able to sleep better after a longer time to relax from the day and after having some “me time” before sleep.35 As bedtime procrastination is also associated with evening media consumption, this assumption also fits with our findings that adolescents with high SR use their mobile phones longer before bedtime.36 Other studies suggest pre-sleep mobile phone usage as a technique for stress reduction and avoidance of brooding that seems to be used primarily by adolescents with high SR.37 Furthermore, more social resources, such as peer group integration and parental support were reported in the group of adolescents with low SR compared to adolescents with high SR. Thus, it might be assumed that the adolescents with high SR may less rely on their social network to overcame stressful situations. The adolescents with low SR, on the other hand, were apparently capable of utilizing the protective effect, which social resources can have on stress and sleep.38–40
As previously reported for adults, our findings showed an increased risk for a current insomnia in adolescents with high SR.3 However, contrary to the 3P model of insomnia and findings in adults, high SR did not increase the risk for an insomnia incident 9 or 17 months later in this sample.3,41 As mentioned, only 52% of participants, who developed insomnia had high SR, while 48% belonged to the group with low SR. It is possible that during the developmental phase of almost 2 years, sleep reactivity is a less stable (trait) disposition than anticipated and/or less influential on insomnia symptoms compared to other risk factors (in line with various studies our results highlight also the increased risk by female gender and internalizing symptoms for the incidence of insomnia symptoms).42 Moreover, within the diathesis-stress model, sleep reactivity is often understood as a moderator between (early) life stress and insomnia, increasing the likelihood of developing insomnia when stress has been experienced.³ Because this study did not consider previous stressful life events, we cannot exclude the possibility that an absence of these events reduces the effects of sleep reactivity. Yet another possible explanation could be that study participation had an enhanced motivational effect to reflect on and change one`s own unhealthy sleep behavior and thus reduce the risk of future insomnia. Perhaps such beneficial changes are more likely in adolescents with high SR, as reflection allows them to consciously attribute their sleep problems to acute stress rather than to other long-term internal causes, thus providing a subjective explanatory model for their poor sleep. In this regard, Jamieson et al43 showed that changing one’s mindset about stress can have an impact on stress-related health outcomes. Further research is needed to clarify this assumption.
Strengths and Limitations
The strengths of this study include: (1) a nearly balanced gender ratio, (2) the inclusion of acute insomnia depicting the early developmental phase of insomnia, (3) the coverage of a period of almost two years for a possible insomnia incident.
The current study also has limitations with implications for future research. Based on the relative sample size (n = 93) for predicting insomnia incidents, this study could only consider a limited number of predisposing and precipitating factors. In addition, our logistic regression models included all profile risk factors, but to reduce the number of independent predictors due the small sample size, we used the stepwise approach to only incorporate the most important factors. To expand knowledge about predisposing and precipitating factors, future research should examine additional physiological factors (eg, diet and obesity), parental factors (eg, SES), and personal characteristics (ie, perfectionism, chronotype), which are considered to influence mental health including sleep, in a bigger sample.44–48
Most of the data was collected during the COVID-19 pandemic. Although the perceived COVID-19 related burden was included as covariate and did not show significance, differential impacts on insomnia symptoms during different phases of the pandemic cannot be completely ruled out. For example, online learning at home was found to increase sleep duration and to provide more sufficient sleep opportunity.49
Even though this study investigated SR profiles and their association with insomnia in a prospective approach, it would be informative to examine potential bi-directional associations in studies with multiple time points to gain insight into whether sleep reactivity changes as a function of insomnia symptom intensity. Hence, future studies should consider state and trait proportions of sleep reactivity and related temporal and additive effects of environmental factors. In this vein, a distinction between acute and chronic insomnia would shed light on how sleep reactivity affects the early developmental phase and the chronification process of insomnia.
Conclusion
Our findings suggest that in adolescence high sleep reactivity is accompanied by various predisposing and precipitating factors, with girls and older adolescents at later pubertal stages being particularly affected by high SR. Although a current insomnia is 2.95 times more likely in adolescents with high sleep reactivity, surprisingly our results did not reveal sleep reactivity as a predisposing determinant of future insomnia in adolescence. More research is needed to determine the causal role of sleep reactivity for the emergence of insomnia in this age group. Further longitudinal studies should therefore compare the role of sleep reactivity on the development of insomnia throughout different age groups under consideration of the interindividual variability.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval and Informed Consent
The study was approved by the local ethics committee of Bielefeld University [EUB 2017-203]. All participants and their caregivers gave informed consent. We confirm that our study complies with the Declaration of Helsinki.
Funding
This work was supported by the German Research [funding codes LO 337/30-1 and SCHL 1909/8-1]. We acknowledge support for the publication costs by the Open Access Publication Fund of Bielefeld University and the Deutsche Forschungsgemeinschaft (DFG). The funders had no role in study design and administration, data analysis or interpretation, manuscript writing, or the decision to submit the paper for publication.
Disclosure
Ms Maren-Jo Kater reports grants from Deutsche Forschungsgemeinschaft (DFG), publication funding from Open Access Publication Fund of Bielefeld University, before and after the conduction of the study. Dr Arnold Lohaus reports grants from German Research Foundation (Deutsche Forschungsgemeinschaft, DFG), before the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Franco P, Putois B, Guyon A, et al. Sleep during development: sex and gender differences. Sleep Med Rev. 2020;51:101276. doi:10.1016/j.smrv.2020.101276
2. Zambotti M, De, Goldstone A, Colrain IM, Baker FC. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. 2018;39:12–24. doi:10.1016/j.smrv.2017.06.009
3. Kalmbach DA, Cuamatzi-Castelan AS, Tonnu CV, et al. Hyperarousal and sleep reactivity in insomnia: current insights. Nat Sci Sleep. 2018;10:193–201. doi:10.2147/NSS.S138823
4. Drake C, Richardson G, Roehrs T, Scofield H, Roth T. Vulnerability to stress-related sleep disturbance and hyperarousal. Sleep. 2004;27(2):285–291. doi:10.1093/sleep/27.2.285
5. Jarrin DC, Chen IY, Ivers H, Morin CM. The role of vulnerability in stress‐related insomnia, social support and coping styles on incidence and persistence of insomnia. J Sleep Res. 2014;23:681–688. doi:10.1111/jsr.12172
6. Kalmbach DA, Pillai V, Arnedt JT, Drake CL. Identifying at-risk individuals for insomnia using the ford insomnia response to stress test. Sleep. 2016;39(2):449–456. doi:10.5665/sleep.5462
7. Yang C-M, Chou CP-W, Hsiao F-C. The association of dysfunctional beliefs about sleep with vulnerability to stress-related sleep disturbance in young adults. Behav Sleep Med. 2011;9(2):86–91. doi:10.1080/15402002.2011.557990
8. Dougherty EN, Johnson NK, Badillo K, Alissa A. Sleep reactivity is associated with social anxiety and disordered-eating behaviors in college students. J Am Coll Health. 2021;1–6. doi:10.1080/07448481.2021.1967359
9. Ellis JG, Allen S, Perlis M, Grandner M, Gardani M, Espie C. Sleep Reactivity and Psychological Health in Normal Sleepers: The Moderating Role of Stress. Center for Open Science; 2018.
10. Fernández-Mendoza J, Vela-Bueno A, Vgontzas AN, et al. Cognitive-emotional hyperarousal as a premorbid characteristic of individuals vulnerable to insomnia. Psychosom Med. 2010;72(4):397–403. doi:10.1097/PSY.0b013e3181d75319
11. Palagini L, Moretto U, Novi M, et al. Lack of resilience is related to stress-related sleep reactivity, hyperarousal, and emotion Dysregulation in Insomnia disorder. J Clin Sleep Med. 2018;14(5):759–766. doi:10.5664/jcsm.7100
12. Walker JL, Vargas I, Drake CL, Ellis JG, Muench A, Perlis ML. The natural history of insomnia: high sleep reactivity interacts with greater life stress to predict the onset of acute insomnia. Sleep. 2022;45:9. doi:10.1093/sleep/zsac149
13. Luong G, Arredondo CM, Wrzus C. Age differences in emotion regulation dynamics: anticipatory, reactivity, and recovery processes. In: Cole PM, Hollenstein T, editors. Emotion Regulation: A Matter of Time. Routledge; 2018:226–249.
14. Dieck A, Helbig S, Drake CL, Backhaus J. Validation of the German version of the Ford Insomnia response to stress test. J Sleep Res. 2018;27:e12621. doi:10.1111/jsr.12621
15. Nakajima S, Okajima I, Sasai T, et al. Validation of the Japanese version of the Ford Insomnia response to stress test and the association of sleep reactivity with trait anxiety and insomnia. Sleep Med. 2014;15(2):196–202. doi:10.1016/j.sleep.2013.09.022
16. American Academy of Sleep Medicine. International Classification of Sleep Disorders.
17. Gieselmann A, Jong-Meyer R, de Pietrowsky R. PSAS – Pre-Sleep Arousal Scale – German Version. Leipzig: ZPID (Leibniz Institute for Psychology Information) – Testarchiv; 2014.
18. Scharfenstein A. Der Fragebogen zu schlafbezogenen Kognitionen (FB-SK), ein änderungssensitives instrument für diagnostik und therapie [The questionnaire on sleep-related cognitions (FB-SK), a change-sensitive instrument for diagnostics and therapy]. Göttingen. 1995;41:203–220. German.
19. Anniko MK, Boersma K, van Wijk NPL, Byrne D, Tillfors M. Development of a shortened version of the Adolescent Stress Questionnaire (ASQ-S): construct validity and sex invariance in a large sample of Swedish adolescents. Scand J Child Adolesc Psychiatr Psychol. 2018;6(1):4–15. doi:10.21307/sjcapp-2018-001
20. Lohaus A, Eschenbeck H, Kohlmann C-W, Klein-Heßling J. Fragebogen Zur Erhebung von Stress Und Stressbewältigung Im Kindes- Und Jugendalter-Revision (SSKJ 3-8 R) [Stress and Coping Questionnaire for Children and Adolescents]. Göttingen: Hogrefe; 2018. German.
21. Döpfner M, Görtz-Dorten A. Diagnostik-System Für Psychische Störungen Nach ICD-10 Und DSM-5 Für Kinder Und Jugendliche-III. [Diagnostic System for Mental Disorders According to ICD-10 and DSM-5 for Children and Adolescents – III]. Göttingen: Hogrefe; 2017.
22. Lohaus A, Nussbeck FW. Fragebogen Zu Ressourcen Im Kindes- Und Jugendalter (FRKJ 8–16) [Questionnaire on Resources in Childhood and Adolescence]. Göttingen: Hogrefe; 2016. German.
23. Watzlawik M. Die Erfassung des pubertätsstatus anhand der pubertal development scale: erste schritte zur evaluation einer deutschen übersetzung. [Assessing pubertal status using the Pubertal development scale: first steps towards evaluating a German translation]. Diagnostica. 2009;55(1):55–65. German. doi:10.1026/0012-1924.55.1.55
24. Von Hippel PT. Regression with missing Ys: an improved strategy for analyzing multiply imputed data. Sociol Methodol. 2007;37:83–117. doi:10.1111/j.1467-9531.2007.00180.x
25. Desjardins CD, Bulut O. profileR: an R package for profile analysis. J Open Source Softw. 2020;5:1941. doi:10.21105/joss.019411
26. Ateş C, Kaymaz Ö, Kale HE, Tekindal MA. Comparison of test statistics of nonnormal and unbalanced samples for multivariate analysis of variance in terms of type-I error rates. Comput Math Methods Med. 2019;2019:2173638. doi:10.1155/2019/2173638
27. Muijs D. Doing Quantitative Research in Education with SPSS. Thousand Oaks: SAGE Publications; 2010.
28. Seiffge-Krenke I. Causal links between stressful events, coping style, and adolescent symptomatology. J Adolesc. 2000;23(6):675–691. doi:10.1006/jado.2000.0352
29. Jose PE, Brown I. When does the gender difference in rumination begin? Gender and age differences in the use of rumination by adolescents. J Youth Adolescence. 2008;37(2):180–192. doi:10.1007/s10964-006-9166-y
30. Govaerts S, Grégoire J. Stressful academic situations: study on appraisal variables in adolescence. Eur Rev Appl Psychol. 2004;2004(54):261–271. doi:10.1016/j.erap.2004.05.001
31. Hamidovic A, Karapetyan K, Serdarevic F, Choi SH, Eisenlohr-Moul T, Pinna G. Higher circulating cortisol in the follicular vs. luteal phase of the menstrual cycle: a meta-analysis. Front Endocrinol. 2020;11:311. doi:10.3389/fendo.2020.00311
32. Reffi AN, Cheng P, Kalmbach DA, et al. Is a blunted cortisol response to stress a premorbid risk for insomnia? Psychoneuroendocrinology. 2022;144:105873. doi:10.1016/j.psyneuen.2022.105873
33. Asarnow LD. Depression and sleep: what has the treatment research revealed and could the HPA axis be a potential mechanism? Curr Opin Psychol. 2020;34:112–116. doi:10.1016/j.copsyc.2019.12.002
34. Karan M, Bai S, Almeida DM, Irwin MR, McCreath H, Fuligni AJ. Sleep–wake timings in adolescence: chronotype development and associations with adjustment. J Youth Adolesc. 2021;50:628–640. doi:10.1007/s10964-021-01407-1
35. Bernecker K, Job V. Too exhausted to go to bed: implicit theories about willpower and stress predict bedtime procrastination. Br J Psychol. 2020;111:126–147. doi:10.1111/bjop.12382
36. Chung SJ, An H, Suh S. What do people do before going to bed? A study of bedtime procrastination using time use surveys. Sleep. 2020;43:zsz267. doi:10.1093/sleep/zsz267
37. Kater M-J, Schlarb AA. Smartphone usage in adolescents – motives and link to sleep disturbances, stress and sleep reactivity. Somnologie. 2020;24:245–252. doi:10.1007/s11818-020-00272-7
38. Camara M, Bacigalupe G, Padilla P. The role of social support in adolescents: are you helping me or stressing me out? Int J Adolesc Youth. 2017;22:123–136. doi:10.1080/02673843.2013.875480
39. Rueger SY, Malecki CK, Pyun Y, Aycock C, Coyle S. A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychol Bull. 2016;142(10):1017–1067. doi:10.1037/bul0000058
40. Werner A, Kater M-J, Kerkhoff D, Schlarb AA, Lohaus A. Personal and social resources in the context of adolescent sleep. Psychol Health. 2022;1–17. doi:10.1080/08870446.2022.2121396
41. Spielman AJ, Caruso LS, Glovinsky PB. A behavioral perspective on insomnia treatment. Psychiatr Clin North Am. 1987;10:541–553. doi:10.1016/S0193-953X(18)30532-X
42. Marver JE, McGlinchey EA. Sex differences in insomnia and risk for psychopathology in adolescence. Curr Opin Psychol. 2020;34:63–67. doi:10.1016/j.copsyc.2019.09.004
43. Jamieson JP, Crum AJ, Goyer JP, Marotta ME, Akinola M. Optimizing stress responses with reappraisal and mindset interventions: an integrated model. Anxiety Stress Coping. 2018;31:245–261. doi:10.1080/10615806.2018.1442615
44. El-Sheikh M, Shimizu M, Philbrook LE, Erath SA, Buckhalt JA. Sleep and development in adolescence in the context of socioeconomic disadvantage. J Adolesc. 2020;83:1–11. doi:10.1016/j.adolescence.2020.06.006
45. Khan MKA, Chu YL, Kirk SFL, Veugelers PJ. Are sleep duration and sleep quality associated with diet quality, physical activity, and body weight status? A population-based study of Canadian children. Can J Public Health. 2015;106(5):e277–82. doi:10.17269/cjph.106.4892
46. Richardson C, Gradisar M. Perfectionism and insomnia in adolescents: the role of vulnerability to stress and gender. J Adolesc. 2020;85:70–79. doi:10.1016/j.adolescence.2020.10.003
47. Van Sluijs EMF, Ekelund U, Crochemore-Silva I, et al. Physical activity behaviours in adolescence: current evidence and opportunities for intervention. Lancet. 2021;398(10298):429–442. doi:10.1016/S0140-6736(21)01259-9
48. Li SX, Chan NY, Yu MWM, et al. Eveningness chronotype, insomnia symptoms, and emotional and behavioural problems in adolescents. Sleep Med. 2018;47:93–99. doi:10.1016/j.sleep.2018.03.025
49. Meltzer LJ, Saletin JM, Honaker SM, et al. COVID-19 instructional approaches (in-person, online, hybrid), school start times, and sleep in over 5000 US adolescents. Sleep. 2021;44(12):zsab180. doi:10.1093/sleep/zsab180
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.