Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Skipping Breakfast and Its Association with Health Risk Behaviour and Mental Health Among University Students in 28 Countries
Received 10 December 2019
Accepted for publication 2 April 2020
Published 18 August 2020 Volume 2020:13 Pages 2889—2897
DOI https://doi.org/10.2147/DMSO.S241670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Supa Pengpid,1,2 Karl Peltzer3
1ASEAN Institute for Health Development, Mahidol University, Salaya, Phutthamonthon, Nakhon Pathom, Thailand; 2Department of Research Administration and Development, University of Limpopo, Turfloop, South Africa; 3Department of Psychology, University of the Free State, Bloemfontein, South Africa
Correspondence: Karl Peltzer Email [email protected]
Introduction: The study aimed to investigate the associations between skipping breakfast and various health risk behaviours and mental health in university students in 28 countries.
Methods: Using a cross-sectional study design, 21,972 university students with a median age of 20 years from 28 countries in Africa, the Americas and Asia, replied to self-reported measures of breakfast consumption, health compromising behaviours, mental health measures and protective factors.
Results: In adjusted logistic regression analysis, infrequent and/or frequent breakfast skipping was associated with inadequate fruit and vegetable intake, frequent soft drink intake, not avoiding fat and cholesterol, current binge drinking, current tobacco use, gambling, not always wearing a seatbelt, inadequate physical activity, inadequate tooth brushing, not seeing a dentist in the past year and having been in a physical fight. In addition, infrequent and/or frequent breakfast skipping was associated with depression, lower happiness, posttraumatic stress disorder, loneliness, short sleep, long sleep, sleep problem, restless sleep, sleep problem due to traumatic event, and poor academic performance.
Discussion: We found evidence that skipping breakfast was associated with 10 of 15 health risk behaviours, all of nine poor mental health indicators and poor academic performance.
Keywords: skipping breakfast, health compromising behaviour, mental health, university students, multi-country
Introduction
In the adolescent period lifestyle patterns are developed, including breakfast consumption.1 Skipping breakfast is a common practice among university students, which has been shown in various studies, eg, in Barbados, Grenada and Jamaica, 48.2% of females and 41.6% of males,2 in Bahrain 50%,3 47.7% in Turkey,4 and significantly increases the risk of overweight/obesity, cardio metabolic risk factors, type 2 diabetes and heart disease.5–9 Most studies investigating the association between skipping breakfast and health compromising behaviours and mental health have been conducted with single health risk variables, among adolescents and in high-income countries. There is particularly a lack of studies investigating the effect of skipping breakfast on multiple health risk variables among university students from low- and middle-income countries and across a number of countries, which prompted this study.
Various studies among adolescents or emerging adults found associations between skipping breakfast and overweight/obesity,6,10-15 more negative body perception13 and unhealthy dietary behaviour,16 including low fruit and vegetable intake,1,13,16,17 higher sodium intake,16 lower consumption milk/dairy,1,11,16 higher consumption of sweets, sugary or soft drinks,1,13 and skipping other meals.11,13
Mental health correlates of skipping breakfast include stress or mentally distressed,18–20 depressive mood,10,18,21-23 lower happiness scores,24 suicidal behaviour,10,18 shorter sleep duration,1 nocturnal sleeping problems,25 and poor sleep quality.26 Skipping breakfast has among adolescents or emerging adults further been associated with substance use, such as smoking1,12,27 and alcohol use,1,10,12 physical inactivity1,11,15,28 and sedentary behaviour.1,11 Other effects included poor oral hygiene, such as less frequent tooth brushing29 and no dental care visit in the past year,30 and poor hand hygiene, such as no hand washing before meals,29 no seatbelt use,29 cardio metabolic risk factors, such as systolic blood pressure,5 and poorer academic performance.10,15,19 The study aimed to investigate the associations between skipping breakfast and various health compromising behaviours and mental health in university students in 28 countries.
Methods
The cross-sectional study comprised 21,858 college or university students with a median age of 20 years (interquartile range =3 years) with complete breakfast consumption data from 28 countries in Asia: Bangladesh, India, Indonesia, Kyrgyzstan, Laos, Malaysia, Myanmar, Pakistan, Philippines, Russia, Singapore, Thailand, Turkey, and Vietnam; in Africa: Cameroon, Egypt, Ivory Coast, Madagascar, Mauritius, Namibia, Nigeria, South Africa and Tunisia; and the Americas: Barbados, Columbia, Grenada, Jamaica and Venezuela. “In each study country one or two universities were purposefully selected.”31,31,31
In each university, research assistants administered a questionnaire and anthropometric measurements to all students in classrooms selected through a cluster random sample procedure in 2013.
Written informed consent was attained from all participating students, and ethics approvals were obtained from all participating universities (see supplementary file). The study was conducted in accordance with the Declaration of Helsinki. Participation rates were in most countries over 90%.
Measures
Breakfast consumption was measured with the item, “How often do you eat breakfast?” (“Almost every day, sometimes, rarely or never”).32 Skipping breakfast was defined as sometimes, rarely or never having breakfast.
Socio-demographic information comprised gender, age, residence status, subjective wealth status and country income.
Overweight or obesity was determined based on measured body mass index (BMI) and defined as ≥23.0 kg/m2 in South and East Asian countries33 (WHO, 2004) and ≥25.0 kg/m2 in the other countries.34 “Standing height was measured to the nearest 0.1 cm without shoes, using a stadiometer. Participants, wearing light clothes were weighed to the nearest 0.01 kg on a load-cell-operated digital scale, which was first calibrated using a standard weight and re-checked daily”.2
Fruit and vegetable intake was measured with two questions, 1) “How many servings [80 grams] of fruit do you eat on a typical day?” and 2)”How many servings [80 grams] of vegetables do you eat on a typical day?”35 Inadequate fruit and vegetable intake was defined as “less than 5 servings a day.”36
Other dietary items comprised: 1) “avoiding foods containing fat and cholesterol”, 2) “frequency of eating red meat” 3) adding salt to food (“usually, sometimes, occasionally, never”).36
Binge drinking (past-month) was assessed with the item, “How often do you have (for men) five or more and (for women) four or more drinks on one occasion?”37
Tobacco use was defined as currently using “tobacco products (cigarettes, snuff, chewing tobacco, cigars, etc.).”38
Gambling behaviour was measured with 5 different gambling behaviours, eg, “Played cards for money,” from the “South Oaks Gambling Screen (SOGS).”39 Gambling in the past week was defined as any of the five assessed gambling behaviours once a week or more. (Cronbach alpha 0.78)
Seatbelt use was measured with the item, “When driving or riding in the front seat of a car do you wear a seat belt?” (“1 = all of the time, 2 = some of the time, 3 = never and 4 = I don’t ride in cars”).36
Physical activity was measured using the “International Physical Activity Questionnaire (IPAQ) short form,”40 and physical activity levels were defined following IPAQ guidelines.41
Sedentary behaviour was assessed with one item from the IPAQ40 and defined as eight or more hours per day.
Oral health risk behaviour was measured with two items, 1) “Do you brush your teeth? … Twice or more a day, about once a day, less than once a day, and seldom or never.”36 and 2) “How frequently do you go for dental check-ups? … Twice a year, once a year, rarely and never.”42
Having been in a physical fight was defined as one or more times in the past 12 months.43
The “Centres for Epidemiologic Studies Depression Scale (CES-D: Ten items)” measured with 15 or more scores severe depressive symptoms.44 (Cronbach’s alpha = 0.76).
“Post-traumatic stress disorder (PTSD)” was measured with “Breslau’s 7-item screener”.45
Loneliness was defined as most (5–7 days) feeling lonely in the past week.44
Happiness was measured with a four-item “Subjective Happiness Scale (SHS),”46 a score of 13 and above was used to describe high happiness. (Cronbach’s alpha 0.94)
Sleep duration: “On average, how many hours of sleep do you get in a 24 h period?” “Responses were divided into three categories: short sleep (≤6 h), reference category (7–8 h), and long sleep (≥9 h).”24
Sleep quality was assessed with the question, overall in the last 30 days, how much of a problem did you have with sleeping, such as falling asleep, waking up frequently during the night, or waking up too early in the morning? Response options ranged from 1 (none) to 5 (extreme/cannot do),47 Restless sleep. ”Much of the time in the past week, your sleep was restless?” Response option ranged from “1=rarely (<1 day) to 4= most (5–7 days)”. Restless sleep was defined as “much (3–4 days) or most (5–7 days).”44
Sleep problem due to traumatic event. “In your life, have you ever had any experience that was so frightening, horrible, or upsetting that, in the past 30 days you had more trouble than usual falling asleep or staying asleep? (Yes/No)45
Poor academic performance was self-reported as “not satisfactory academic performance.”48
Social support was sourced from three questions of the “Social Support Questionnaire.”49 (Cronbach’s alpha 0.94).
Religiosity was assessed with two dimensions (one item organized religious activity and three items intrinsic religiosity) from the “Duke University Religion Index.”50 (Cronbach’s alpha = 0.80).
Data Analysis
Data analysis was conducted with “STATA software version 15.0 (Stata Corporation, College Station, TX, USA)”. Unadjusted and adjusted logistic regression analyses were used to assess the associations between skipping breakfast categories (sometimes and never or rarely having breakfast), with almost daily having breakfast as reference category, relevant confounders (age, sex, subjective economic status, residence status, country, social support, and religiosity) and dependent variables (15 health risk behaviours, nine poor mental health indicators and academic performance). Due to the clustered nature of the data, country was entered in the survey command. Missing data were excluded from the analysis. P values <0.05 were considered significant.
Results
The sample consisted of 21,972 university students (median age 20 years, interquartile range 3 years), 58.4% were females and 41.6% males, 51.2% rated their economic status as high, 53.9% were living away from parents (on their own or in university residences), 53.9% were residing in low- or lower middle-income countries, 63.8% had high social support, 39.8% high organized religiosity and 33.0% high intrinsic religiosity. In all, 13.8% of university students had rarely or never, 34.2% sometimes and 51.9% had almost every day breakfast (see Table 1).
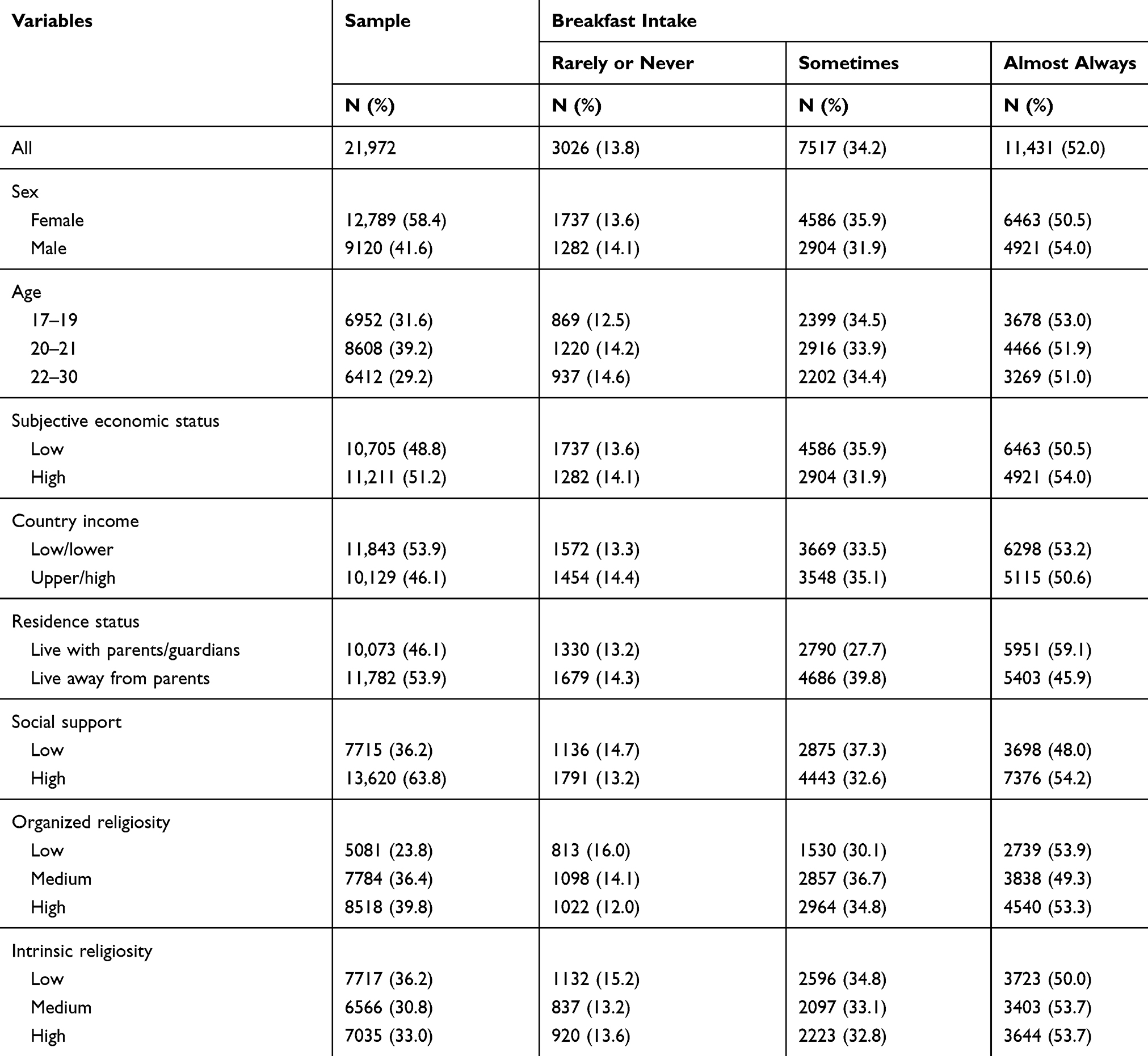 |
Table 1 Sample and Breakfast Intake Characteristics |
Associations Between Skipping Breakfast and Health Risk Behaviour and Mental Health
In adjusted logistic regression analysis, infrequent and/or frequent breakfast skipping was associated with inadequate fruit and vegetable intake, frequent soft drink intake, not avoiding fat and cholesterol, current binge drinking, current tobacco use, gambling, not always wearing a seatbelt, inadequate physical activity, inadequate tooth brushing, not seeing a dentist in the past year and having been in a physical fight. In addition, infrequent and/or frequent breakfast skipping was associated with depression, lower happiness, PTSD, loneliness, short sleep, long sleep, sleep problem, restless sleep, sleep problem due to traumatic event, and poor academic performance (see Tables 2 and 3).
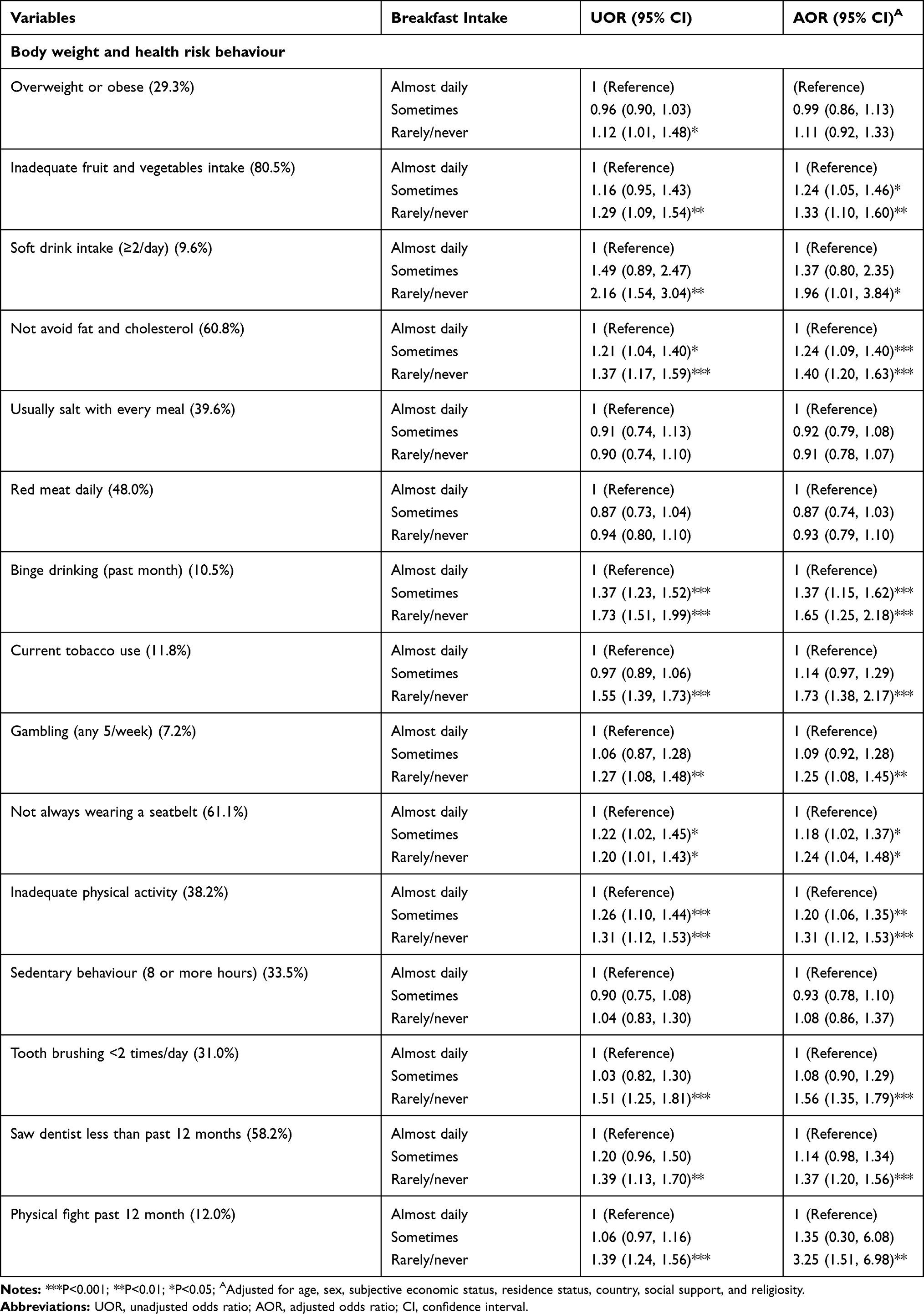 |
Table 2 Breakfast Consumption and Its Associations with Body Weight and Health Risk Behaviours |
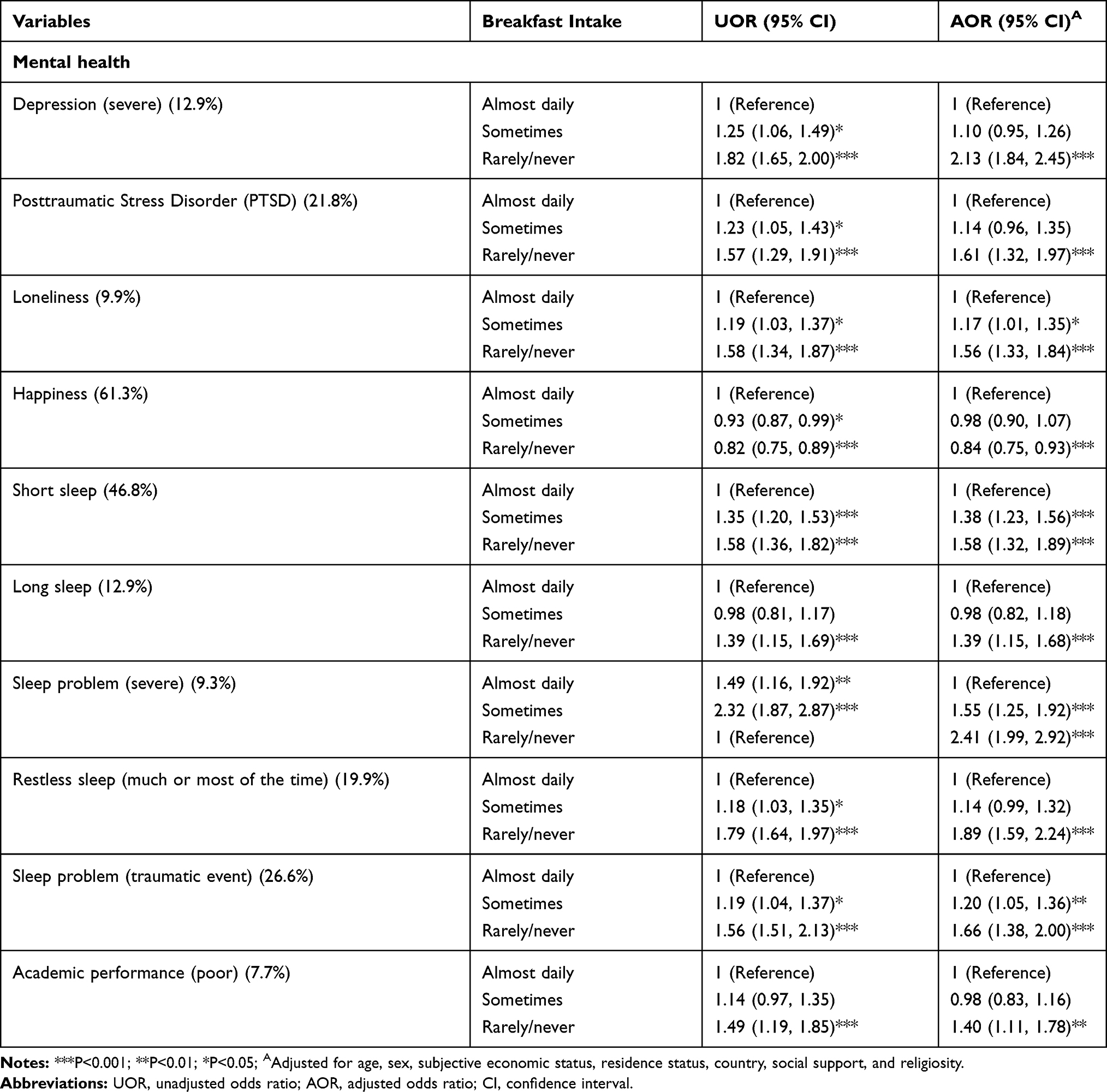 |
Table 3 Breakfast Consumption and Its Associations with Mental Health and Academic Performance |
Discussion
In agreement with a number of previous studies,1,10,11,13,15-30 this study found that skipping breakfast increased the likelihood of 11 of 15 health risk behaviours, all of nine poor mental health indicators and poor academic performance. These findings replicate earlier results showing the wide range of possible effects of skipping breakfast on various health risk behaviours and poor mental indicators.16,18,20,29
Possible mechanisms to explain the effects of skipping breakfast on health risk behaviours and mental health, may be that having breakfast assists university students to “function better cognitively and psychosocially.”18,51 University students who had almost daily or daily breakfast tended to make healthier food choices throughout the day, as found in an earlier study among Chinese adolescents.1 Some mechanisms through which breakfast contributes to reducing poor mental health have been proposed.52 For example, after eating breakfast, carbohydrates are converted into glucose which is essential for the formation of tryptophan, a precursor protein for the synthesis of serotonin, which regulates depressive symptoms, irritable mood and cognitive functioning.51–53
This study suggests that skipping breakfast is part of an unhealthy behaviour pattern, including poor mental health, which clusters in the form of multiple risk behaviours.16,29 However, various previous studies found an association between skipping breakfast and overweight or obesity,6,10-15 while this study only found such an association in unadjusted analysis. This study did also not find an association between skipping breakfast and sedentary behaviour and high sodium intake, as this was found in previous investigations.1,11,16
Study Limitations
The study survey was limited to a cross-sectional design, participants attending university and most of the questionnaire administered was by self-report. In order to identify causal associations, further longitudinal research is indicated. It is possible, for example, that students with poor mental health adopt skipping breakfast because of their poor mental health. Skipping breakfast was only assessed with one question and did not include diet quality and information about other meals, and future studies should consider several questions, including diet quality, information about other meals, provide definitions of terminology, such as what constitutes breakfast, and reasons or explanations of skipping breakfast. Further, some health risk behaviours, such as fast food consumption, and poor mental health indicators, such as suicidal behaviour, were not assessed in this investigation and should be included in further research.
Conclusion
This investigation added evidence for a large university population from 28 countries that skipping breakfast was associated with 10 of 15 health risk behaviours, all of nine poor mental health indicators, and poor academic performance. Interventions programmes targeting breakfast consumption in this population should address health risk behaviours and poor mental health linked with skipping breakfast identified in this survey.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Wang M, Zhong JM, Wang H, et al. Breakfast consumption and its associations with health-related behaviors among school-aged adolescents: A cross-sectional study in Zhejiang Province, China. Int J Environ Res Public Health. 2016;13(8):
2. Wright M, Adair L, James C, et al. The association of nutrition behaviors and physical activity with general and central obesity in Caribbean undergraduate students. Rev Panam Salud Publica. 2015;38(4):278–285.
3. Musaiger AO, Awadhalla MS, Al-Mannai M, AlSawad M, Asokan GV. Dietary habits and sedentary behaviors among health science university students in Bahrain. Int J Adolesc Med Health. 2017;29(2). doi:10.1515/ijamh-2015-0038
4. Neslişah R, Emine AY. Energy and nutrient intake and food patterns among Turkish university students. Nutr Res Pract. 2011;5(2):117–123. doi:10.4162/nrp.2011.5.2.117
5. Cayres SU, Júnior IF, Barbosa MF, Christofaro DG, Fernandes RA. Breakfast frequency, adiposity, and cardiovascular risk factors as markers in adolescents. Cardiol Young. 2016;26(2):244–249. doi:10.1017/S1047951115000050
6. Nurul-Fadhilah A, Teo PS, Huybrechts I, Foo LH. Infrequent breakfast consumption is associated with higher body adiposity and abdominal obesity in Malaysian school-aged adolescents. PLoS One. 2013;8(3):e59297. doi:10.1371/journal.pone.0059297
7. Ballon A, Neuenschwander M, Schlesinger S. Breakfast skipping is associated with increased risk of type 2 diabetes among adults: A systematic review and meta-analysis of prospective cohort studies. J Nutr. 2019;149(1):106–113. doi:10.1093/jn/nxy194
8. Monzani A, Ricotti R, Caputo M, et al. A systematic review of the association of skipping breakfast with weight and cardiometabolic risk factors in children and adolescents. What should we better investigate in the future? Nutrients. 2019;11(2):
9. Takagi H, Hari Y, Nakashima K, Kuno T, Ando T. ALICE (All-Literature Investigation of Cardiovascular Evidence) Group. Meta-analysis of relation of skipping breakfast with heart disease. Am J Cardiol. 2019;124(6):978–986. doi:10.1016/j.amjcard.2019.06.016
10. Lee HJ, Kim CH, Han I, Kim SH. Emotional state according to breakfast consumption in 62276 South Korean adolescents. Iran J Pediatric. 2019;29(6):e92193.
11. Tin SP, Ho SY, Mak KH, Wan KL, Lam TH. Lifestyle and socioeconomic correlates of breakfast skipping in Hong Kong primary 4 schoolchildren. Prev Med. 2011;52(3–4):250–253. doi:10.1016/j.ypmed.2010.12.012
12. Kapantais E, Chala E, Kaklamanou D, Lanaras L, Kaklamanou M, Tzotzas T. Breakfast skipping and its relation to BMI and health-compromising behaviours among Greek adolescents. Public Health Nutr. 2011;14(1):101–108. doi:10.1017/S1368980010000765
13. van Vliet JS, Gustafsson PA, Nelson N. Feeling ‘too fat’ rather than being ‘too fat’ increases unhealthy eating habits among adolescents - even in boys. Food Nutr Res. 2016;60(1):29530. doi:10.3402/fnr.v60.29530
14. Yang RJ, Wang EK, Hsieh YS, Chen MY. Irregular breakfast eating and health status among adolescents in Taiwan. BMC Public Health. 2006;6(1):295. doi:10.1186/1471-2458-6-295
15. Sa J, Heimdal J, Sbrocco T, Seo DC, Nelson B. Overweight and Physical Inactivity Among African American Students at a Historically Black University. J Natl Med Assoc. 2016;108(1):77–85. doi:10.1016/j.jnma.2015.12.010
16. Rodrigues PRM, Luiz RR, Monteiro LS, Ferreira MG, Gonçalves-Silva RMV, Pereira RA. Adolescents’ unhealthy eating habits are associated with meal skipping. Nutrition. 2017;42:114–120.e1. doi:10.1016/j.nut.2017.03.011
17. Pedersen TP, Meilstrup C, Holstein BE, Rasmussen M. Fruit and vegetable intake is associated with frequency of breakfast, lunch and evening meal: cross-sectional study of 11-, 13-, and 15-year-olds. Int J Behav Nutr Phys Act. 2012;9(1):9. doi:10.1186/1479-5868-9-9
18. Lee G, Han K, Kim H. Risk of mental health problems in adolescents skipping meals: the Korean National Health and Nutrition Examination Survey 2010 to 2012. Nurs Outlook. 2017;65(4):411–419. doi:10.1016/j.outlook.2017.01.007
19. Lien L. Is breakfast consumption related to mental distress and academic performance in adolescents? Public Health Nutr. 2007;10(4):422–428. doi:10.1017/S1368980007258550
20. Tajik E, Latiffah AL, Awang H, et al. Unhealthy diet practice and symptoms of stress and depression among adolescents in Pasir Gudang, Malaysia. Obes Res Clin Pract. 2016;10(2):114–123. doi:10.1016/j.orcp.2015.06.001
21. Perveen A, Hamzah HB, Ramlee F, Morgul E, Govindasamy P. Skipping breakfast and lack of physical activity; contributing factors of depressive symptoms among university students. Inter J Aca Res Business Soc Sci. 2018;8(8):12–23.
22. Khan A, Ahmed R, Burton NW. Prevalence and correlates of depressive symptoms in secondary school children in Dhaka City, Bangladesh. Ethn Health. 2017;1–13. doi:10.1080/13557858.2017.1398313
23. Zhu Z, Cui Y, Gong Q, et al. Frequency of breakfast consumption is inversely associated with the risk of depressive symptoms among Chinese university students: A cross-sectional study. PLoS One. 2019;14(8):e0222014. doi:10.1371/journal.pone.0222014
24. Peltzer K, Pengpid S. Nocturnal sleep problems among university students from 26 countries. Sleep Breath. 2015;19(2):499–508. doi:10.1007/s11325-014-1036-3
25. Lesani A, Mohammadpoorasl A, Javadi M, Esfeh JM, Fakhari A. Eating breakfast, fruit and vegetable intake and their relation with happiness in college students. Eat Weight Disord. 2016;21(4):645–651. doi:10.1007/s40519-016-0261-0
26. Wang L, Qin P, Zhao Y, et al. Prevalence and risk factors of poor sleep quality among Inner Mongolia Medical University students: A cross-sectional survey. Psychiatry Res. 2016;244:243–248. doi:10.1016/j.psychres.2016.04.011
27. Smith KJ, McNaughton SA, Cleland VJ, Crawford D, Ball K. Health, behavioral, cognitive, and social correlates of breakfast skipping among women living in socioeconomically disadvantaged neighborhoods. J Nutr. 2013;143(11):1774–1784. doi:10.3945/jn.113.181396
28. Pengpid S, Peltzer K, Kassean HK, Tsala Tsala JP, Sychareun V, Müller-Riemenschneider F. Physical inactivity and associated factors among university students in 23 low-, middle- and high-income countries. Int J Public Health. 2015;60(5):539–549. doi:10.1007/s00038-015-0680-0
29. Jordão LMR, Malta DC, Freire MDCM. Clustering patterns of oral and general health-risk behaviours in Brazilian adolescents: findings from a national survey. Community Dent Oral Epidemiol. 2018;46(2):194–202. doi:10.1111/cdoe.12354
30. Peltzer K, Pengpid S. Oral health behaviour and social and health factors in university students from 26 low, middle and high income countries. Int J Environ Res Public Health. 2014;11(12):12247–12260. doi:10.3390/ijerph111212247
31. Pengpid S, Peltzer K. Correlates of sedentary behaviour among university students with depression from 22 low- and middle-income countries. J Hum Behav Soc Environ. 2019;29(7):833–839. doi:10.1080/10911359.2019.1610134
32. Wardle J, Haase AM, Steptoe A. Body image and weight control in young adults: international comparisons in university students from 22 countries. Int J Obes. 2006;30(4):644–651. doi:10.1038/sj.ijo.0803050
33. World Health Organization (WHO). WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. doi:10.1016/S0140-6736(03)15268-3
34. World Health Organization (WHO). The International Classification of Adult Underweight, Overweight and Obesity according to BMI, 2018. Available online: http://apps.who.int/bmi/index.jsp?introPage=intro_3.html. (
35. Hall JN, Moore S, Harper SB, Lynch JW. Global variability in fruit and vegetable consumption. Am J Prev Med. 2009;36(5):402–409.e5. doi:10.1016/j.amepre.2009.01.029
36. World Health Organization (WHO). Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation. Geneva, Switzerland: WHO; 2003.
37. Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med. 1998;158(16):1789–1795. doi:10.1001/archinte.158.16.1789
38. World Health Organization (WHO). Guidelines for Controlling and Monitoring the Tobacco Epidemic. Geneva, Switzerland: WHO; 1998.
39. Lesieur HR, Blume SB. The South Oaks Gambling Screen (SOGS): a new instrument for the identification of pathological gamblers. Am J Psychiatry. 1987;144(9):1184–1188. doi:10.1176/ajp.144.9.1184
40. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
41. International Physical Activity Questionnaire (IPAQ) Research Committee. International Physical Activity Questionnaire. 2016. Available online: https://sites.google.com/site/theipaq/scoring-protocol. (
42. Åstrøm AN, Masalu JR. Oral health behavior patterns among Tanzanian university students: a repeat cross-sectional survey. BMC Oral Health. 2001;1(1):2. doi:10.1186/1472-6831-1-2
43. Centers for Disease Control (CDC) The Global School and Health Survey background, 2013. Available from http://www.cdc.gov/gshs/background/index.htm. (
44. Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am J Prev Med. 1994;10(2):77–84. doi:10.1016/S0749-3797(18)30622-6
45. Breslau N, Peterson EL, Kessler RC, Schultz LR. Short screening scale for DSM-IV posttraumatic stress disorder. Am J Psychiatry. 1999;156(6):908–911. doi:10.1176/ajp.156.6.908
46. Lyubomirsky S, Lepper HS. A measure of subjective happiness: preliminary reliability and construct validation. Soc Indic Res. 1999;46(2):137–155. doi:10.1023/A:1006824100041
47. Peltzer K, Pengpid S. Sleep duration and health correlates among university students in 26 countries. Psychol Health Med. 2016;21(2):208–220. doi:10.1080/13548506.2014.998687
48. Peltzer K, Pengpid S. Health behaviour and self-reported academic performance among university students: an international study. Mediterr J Soc Sci. 2014;5(27):998–1005. doi:10.5901/mjss.2014.v5n27p998
49. Brock D, Sarason I, Sarason B, Pierce G. Simultaneous assessment of perceived global and relationship-specific support. J Soc Pers Relatsh. 1996;13(1):143–152. doi:10.1177/0265407596131008
50. Koenig HG, Bussing A. The Duke University Religion Index (DUREL): A five-item measure for use in epidemiological studies. Religions. 2010;1(1):78–85. doi:10.3390/rel1010078
51. O’Sullivan TA, Robinson M, Kendall GE, et al. A good-quality breakfast is associated with better mental health in adolescence. Public Health Nutr. 2009;12(2):249–258. doi:10.1017/S1368980008003935
52. Ferrer-Cascales R, Sánchez-SanSegundo M, Ruiz-Robledillo N, Albaladejo-Blázquez N, Laguna-Pérez A, Zaragoza-Martí A. Eat or skip breakfast? The important role of breakfast quality for health-related quality of life, stress and depression in spanish adolescents. Int J Environ Res Public Health. 2018;15(8):1781. doi:10.3390/ijerph15081781
53. Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. 2009;65(9):732–741. doi:10.1016/j.biopsych.2008.11.029
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.