Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Skeletal Muscle Function in Relation to COPD Severity and Its Predictive Significance for Disease Progression
Authors He Z, Cao B, Liu K, Wei Q
Received 5 December 2024
Accepted for publication 17 February 2025
Published 21 February 2025 Volume 2025:20 Pages 389—397
DOI https://doi.org/10.2147/COPD.S510425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Zemin He,1 Boxiong Cao,1 Keting Liu,2 Qiang Wei1
1Department of Thoracic Surgery, The First People’s Hospital of Shuangliu District, Chendu, Sichuan Province, People’s Republic of China; 2Department of Neurology, Chengdu Seventh People’s Hospital, Chendu, Sichuan Province, People’s Republic of China
Correspondence: Qiang Wei, Department of Thoracic Surgery, The First People’s Hospital of Shuangliu District, 120 Chengbei Upper Street, Dongsheng Town, Shuangliu District, Chengdu City, Sichuan Province, People’s Republic of China, Tel +86 13778533702, Email [email protected]
Purpose: To compare skeletal muscle function levels in different COPD severities and explore their relationship with COPD severity and progression.
Patients and Methods: The study included COPD patients from the First People’s Hospital of Shuangliu District, Chengdu between May 2021 and May 2022, categorized into mild, moderate, severe and very severe groups based on FEV1%. Skeletal muscle function (quadriceps strength, respiratory muscle strength, 6MWD) was compared among these groups. Patients were followed up to assess disease progression, and logistic regression was used to analyze the predictive value of skeletal muscle function for COPD progression.
Results: Among the 400 subjects, respiratory muscle strength, quadriceps strength, and 6MWD were all higher in the nonsmoking group than in the smoking group, with the mild group better than the moderate group, the moderate group better than the severe group, males stronger than females, the MMRC score ≤ 2 group better than the > 2 group, and strength greater in the age ≤ 70 group than in the age > 70 group. The mild group had a higher 6MWD than the moderate group, the moderate group was better than the severe group, non-smokers had a higher 6MWD than smokers, and the difference between males and females was greater with statistical significance. There are differences in quadriceps strength, respiratory strength, and 6MWD within the progression group. Logistic regression analysis showed that respiratory muscle strength, quadriceps strength, 6MWD, and COPD severity were risk factors for COPD progression (P < 0.05).
Conclusion: COPD patients show skeletal muscle dysfunction that worsens with disease severity. Respiratory muscle strength, quadriceps strength, 6MWD, and COPD severity predict COPD prognosis.
Keywords: COPD, chronic obstructive pulmonary disease, skeletal muscle function, disease progression, predictive value
Introduction
Chronic obstructive pulmonary disease (COPD) is a common chronic respiratory disease with a high incidence rate and high disease burden. Once established, the disease is progressive and cannot be reversed. Skeletal muscle dysfunction is one of the most common comorbidities of COPD and the main cause of reduced exercise tolerance in patients.1,2 Research has shown that systemic factors such as smoking, systemic inflammation, exercise intolerance, exacerbations, nutritional deficiencies, anabolic insufficiency, comorbidities, and certain medications can affect muscle function by altering the local muscle microenvironment. These factors can lead to imbalances in protein metabolism, oxidative stress, inflammatory events and muscle injury, ultimately affecting muscle structure and function.3 It seriously affects the quality of life and prognosis of patients, but it is still unclear whether skeletal muscle function testing can predict the prognosis of COPD patients. This study investigates the relationship between COPD severity and skeletal muscle function and the predictive value of skeletal muscle function for COPD progression by comparing the levels of skeletal muscle function in patients with different degrees of COPD. The research hypothesis is that assessment of skeletal muscle function can serve as an effective indicator of prognosis in COPD. This finding may have significant implications for the clinical management of COPD patients, particularly in the early identification of risk of disease progression and the development of personalized treatment plans.
Materials and Methods
Ethical Considerations
This study has been approved by the ethics committee of the First People’s Hospital of Shuangliu District, Chengdu (batch number: 2021–02-01). Written informed consent was obtained from all patients.
Patients and Study Design
This study selected patients diagnosed with chronic obstructive pulmonary disease (COPD) in our hospital from May 2021 to May 2022. According to the GOLD classification of lung function,4 patients were divided into mild group: FEV1% pred ≥ 80%; moderate group: 50% ≤ FEV1% pred<80%; severe group: 30% ≤ FEV1% pred<50%; Extremely severe group: FEV1% pred<30% or FEV1% pred<50% with respiratory failure, with 100 cases included in each group. If any subjects were excluded, additional subjects were included, for a total of 400 subjects. All subjects signed an informed consent form before the study. Inclusion criteria: (1) age ≥ 18 years; (2) diagnosed with chronic obstructive pulmonary disease according to the GOLD diagnostic criteria;4 (3) complete medical records; (4) all subjects enrolled voluntarily. Exclusion criteria: (1) Those meeting one or more of the following criteria: bronchiectasis, active tuberculosis, severe interstitial lung disease, bronchiolitis, malignant tumours, or others deemed inappropriate for inclusion; (2) history of previous thoracic surgery; (3) contraindications to skeletal muscle function testing, such as cognitive impairment, severe osteoarthritis, and recent myocardial infarction. (4) During enrolment, subjects were found not to meet the inclusion criteria or were unwilling to cooperate; (5) Patients suffering from other serious illnesses or dying from other illnesses; (6) The patient is lost to follow-up or voluntarily requests to withdraw from the study.
The clinical data of all subjects were recorded, including sex, age, smoking history, alcohol consumption history, duration of chronic obstructive pulmonary disease (≤5 years/>5 years), and respiratory distress index score (mMRC score),5 and the lung function of all subjects was measured. Patients’ quadriceps muscle strength was measured using a WDF-50 digital push-pull force meter (Wenzhou Weidu Electronics Co., Ltd)., and respiratory muscle strength was measured using a portable lung function tester (Saike Xiamen Medical Equipment Co., Ltd., Min Qi Zhuzhun 20172070241). The patient’s 6-minute walk test (6MWD) was performed according to the 6MWD expert consensus protocol.6,7 All subjects completed a 6-minute walking distance test on the same ward floor, with uniform distance markings on the ward floor. The test was administered by a dedicated person and the pre-test preparation was consistent. All subjects were followed up for 12 months. During the follow-up period, any acute exacerbation of chronic obstructive pulmonary disease (COPD), hospitalization for COPD, or death from COPD was considered disease progression and defined as the disease progression group. Specifically, acute exacerbation of COPD (AECOPD) refers to an acute event, so we defined the disease progression group as patients who experienced at least one AECOPD, were hospitalized for COPD, or died for COPD during the follow-up period, while the remainder were considered as the disease stability group. To reduce human error, all detection indicators were operated by the same person.
Statistical Analyses
SPSS 19.0 was used for data analysis, with quantitative data expressed as (x ± s). Independent samples t-test was used for comparison between two groups, one-way analysis of variance for comparison between three or more groups, percentage (%) for count data and chi-squared test for comparison between groups; risk factors for progression of chronic obstructive pulmonary disease were analysed using binary logistic regression, and a p-value of less than 0.05 was considered statistically significant.
Results
Basic Information
Among the 400 research subjects, there were 245 males (61.3%) and 155 females (38.7%); Age range: 51–88 years; Among them, there were 100 cases each in the mild group, moderate group, severe group, and extremely severe group; There were 135 cases (33.8%) in the disease progression group, including 99 cases of worsening, 33 cases of hospitalisation due to chronic obstructive pulmonary disease, 3 cases of death, and 265 cases (66.2%) in the stable condition group; There were 240 cases (60. There were 240 cases (60.0%) in the group with a history of smoking and 160 cases (40.0%) in the group without a history of smoking; 159 cases (39.8%) of chronic obstructive pulmonary disease had a duration of ≤5 years, whereas 241 cases (60.2%) had a duration of >5 years; 255 cases (63.7%) were aged 70 years and under, and 145 cases (16.3%) were aged 70 years and over; 210 cases (52.5%) had a score of 2 or less in the mMRC, and 190 cases (47.5%) had a score of 3–4. See Table 1.
 |
Table 1 Comparison of Testing Results for Various Indicators |
Respiratory Muscle Strength Test
Among the 400 subjects, respiratory muscle strength was greater in the non-smoking group than in the smoking group. There were differences in respiratory muscle strength between groups according to the severity of chronic obstructive pulmonary disease. Respiratory muscle strength was greater in men than in women, and the mMRC score was ≤ 2. Respiratory muscle strength was greater in the >2 group and the difference was statistically significant (P<0.05). Further comparisons between groups showed that the respiratory muscle strength of the mild group was greater than that of the moderate group, and the respiratory muscle strength of the moderate group was greater than that of the severe group; the respiratory muscle strength of the severe group was greater than that of the extremely severe group, and the differences were statistically significant (P<0.05). See Table 1 for details.
Measurement of Quadriceps Muscle Strength
In all subjects, quadriceps strength was greater in the non-smoking patients than in the smoking group. There were differences in the severity of chronic obstructive pulmonary disease between the groups, with men having greater quadriceps strength than women and mMRC scores ≤ 2 points. Quadriceps strength was greater in patients aged ≤70 years than in those aged >70 years, and the difference was statistically significant (P<0.05). Further comparisons between groups showed that there was no statistically significant difference between the mild and moderate groups (P>0.05); the quadriceps muscle strength of the moderate group was greater than that of the severe group, and the quadriceps muscle strength of the severe group was greater than that of the extremely severe group, with statistical significance (P<0.05), as shown in Table 1.
6-minute Walk Test results
The 6MWD of non-smoking patients was greater than that of the smoking group, and there were differences in the severity of chronic obstructive pulmonary disease between the groups. The 6MWD of men was greater than that of women and the differences between the groups were statistically significant (P<0.05). Further comparisons between groups showed that the mild group was greater than the moderate group and the moderate group was greater than the severe group, and the differences were statistically significant (P<0.05). The difference between the severe group and the extremely severe group was not statistically significant (P>0.05). See Table 1.
Comparison of Disease Progression Groups
Comparison between the disease progression group and the disease stability group revealed significant differences in quadriceps muscle strength, respiratory muscle strength and 6MWD between the two groups (P<0.05), as shown in Table 2. Select the indicators with a single factor analysis P<0.05 in Table 2, and perform logistic regression analysis on the factors that can be considered to have an impact on the exacerbation of chronic obstructive pulmonary disease in clinical practice, with the progression of chronic obstructive pulmonary disease as the dependent variable: 1 for the COPD progression group and 2 for the stable condition group; the severity of the condition is mild at 1, moderate at 2, severe at 3, and extremely severe at 4; smoking history is 1, and no smoking history is 2; 1 has a history of drinking alcohol, 2 has no history of drinking alcohol; disease duration ≤ 5 years is 1, and>5 years is 2; MMRC ≤ 2 points is 1, >2 points is 2; respiratory muscle strength, quadriceps muscle strength, and 6MWD are included based on actual values. The results showed that respiratory muscle strength, quadriceps strength, 6MWD and COPD severity were risk factors for COPD progression (P<0.05). See Table 3.
 |
Table 2 Comparison of Various Items in the Disease Progression Group |
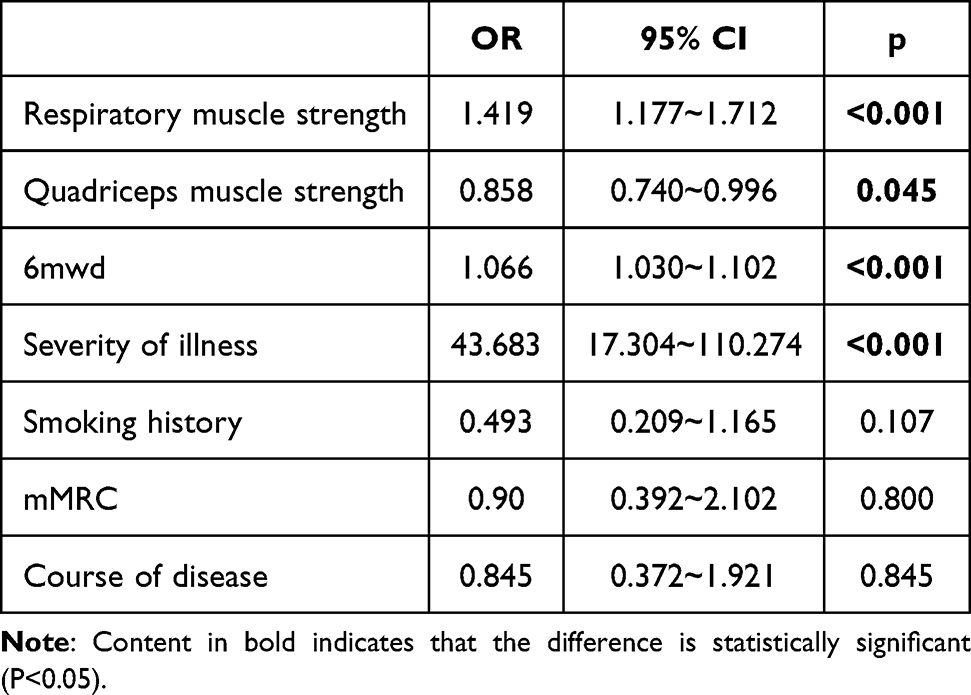 |
Table 3 Analysis of Risk Factors for Worsening of the Condition |
ROC Curve Analysis
Respiratory muscle strength, quadriceps muscle strength and 6WMD can effectively predict the progression of chronic obstructive pulmonary disease. The area under the ROC curve (AUC) of respiratory muscle strength is (0.816, 95% CI (0.775~0.858, P<0.001, critical value 38.04), and the area under the ROC curve of quadriceps muscle is (0. 718, 5% CI (0.669~0.768), P<0.01, critical value 15.47), and the area under the ROC curve of 6WMD is (0.810, 5% CI (0.768~0.851), P<0.01, critical value 199.45), as shown in Figure 1 and Table 4. This indicates that when the respiratory muscle strength of patients with chronic obstructive pulmonary disease is less than 38.04, the quadriceps muscle strength is less than 15.47 and the 6WMD is less than 199.45, their condition is more severe and may lead to the progression of chronic obstructive pulmonary disease.
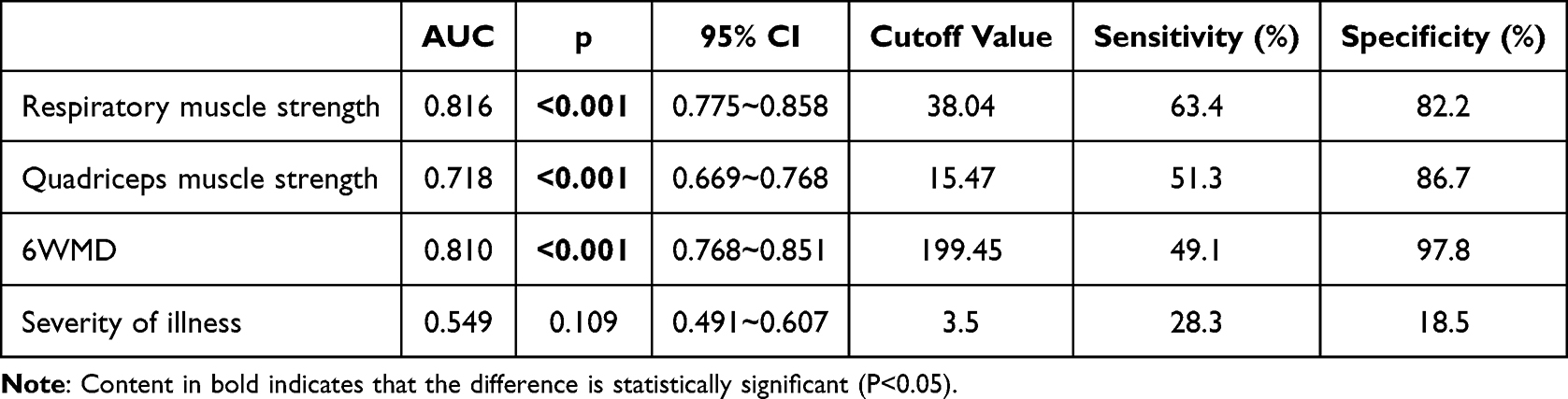 |
Table 4 Area Under the ROC Curve for Each Indicator |
 |
Figure 1 ROC curves and results for each indicator. |
Discussion
Chronic obstructive pulmonary disease (COPD) is highly prevalent in China and has a significant impact on patients’ quality of life. Once established, the disease progresses continuously and is irreversible. Early intervention can effectively slow the progression of the disease8. Therefore, it is important to identify effective early predictors of COPD prognosis. Studies have shown that 15–20% of stable COPD patients have skeletal muscle dysfunction,4 which forms a vicious cycle with the progression of COPD, accelerating its deterioration and severely affecting patient outcomes. Our study compared the skeletal muscle function levels of COPD patients with different severity levels and found that skeletal muscle function is related to the severity of chronic obstructive pulmonary disease and can predict the prognosis of COPD patients.
This study shows that a decline in respiratory muscle strength occurs early in the course of chronic obstructive pulmonary disease (COPD), progressively worsens as COPD severity increases, and persists throughout the disease process. Our research has shown that the respiratory muscles weaken earlier than the quadriceps femoris muscles. Some studies9 suggest that this is mainly due to the respiratory muscles being in a state of long-term high stress, which leads to structural and functional changes, as well as systemic factors such as hypoxemia, malnutrition, electrolyte imbalance, and the effects of mechanical ventilation. Weakness of the quadriceps muscle is often associated with trauma, local nerve compression, hip or knee disease, and prolonged inactivity. Quadriceps strength begins to manifest in patients with moderately impaired lung function due to COPD and also gradually decreases as the disease progresses. The 6-minute walk distance (6MWD) also decreases as the severity of COPD increases, although the difference between the severe and very severe groups is not significant. Research has shown that the age-related decline in skeletal muscle mass is more pronounced in people with COPD than in the general population, leading to poor health outcomes, including an increased risk of death.8 The reasons for this accelerated loss of muscle mass have been debated. Some researchers have found that static hyperinflation in COPD patients alters ventilatory mechanics, leading to changes in thoracic geometry and displacement of muscles from their optimal length.10 In addition, respiratory muscles face increased elastic, resistance and threshold inspiratory loads due to airflow limitation, which may contribute to early respiratory muscle weakness. The majority of researchers agree that sedentary behaviour and long-term smoking in COPD patients are significant factors leading to these outcomes.11 Studies have shown that as COPD progresses, there are changes in various pathophysiological aspects such as hypercapnia, hypoxia and inflammation.12 Following inflammation, the inflammatory mediator TNF-α can directly stimulate total muscle protein, leading to muscle protein loss, and the binding of TNF-α to its receptor can induce muscle cell apoptosis. Chronic hypoxia leads to an imbalance between oxidation and antioxidation, enhancing oxidative stress responses and increasing skeletal muscle consumption, thereby reducing the maximal contractile force of skeletal muscle,13 which contributes to the exacerbation of muscle atrophy. Some studies have performed muscle biopsies in COPD patients on the fourth day of hospitalisation and found that local IL-6 and IL-8 levels are inversely proportional to quadriceps strength, suggesting that local and systemic inflammatory responses are involved in the impairment of skeletal muscle function in COPD.14
Our research also found significant differences in skeletal muscle function between COPD patients of different sexes, with female COPD patients typically having poorer muscle mass and function than male patients. However, these differences were not statistically significant after multiple factor analysis. Other studies15 have shown significant differences in skeletal muscle function between the sexes in COPD patients, with female COPD patients typically having poorer muscle mass and function than male patients. This may be due to several factors, including metabolic differences, inflammatory responses, lifestyle and behavioral factors. In addition, studies have shown that the incidence of muscle wasting syndrome in male COPD patients is 18.3%, while in female patients it is 30.3%,16 indicating a significant difference between the two. In the absence of further statistics on the decline in skeletal muscle function within the same time period for different sexes, it cannot be concluded that these differences have an impact on our research.
This study found differences in quadriceps muscle strength, respiratory muscle strength and 6MWD between the disease progression group and the disease stability group. Further binary logistic regression analysis showed that respiratory muscle strength, quadriceps muscle strength, 6MWD and chronic obstructive pulmonary disease severity can effectively predict whether the disease will worsen and have predictive value for the prognosis of chronic obstructive pulmonary disease patients. Some studies show that17 the decline in skeletal muscle function in COPD patients is more severe than in normal people. About 4–39% of COPD patients have skeletal muscle dysfunction, which will have a negative impact on the quality of life, morbidity and mortality of COPD patients. Another study18 found that the respiratory muscle group index has some predictive value for the severity of lung ventilatory impairment in elderly patients with chronic obstructive pulmonary disease. Taivassalo et al believe that changes in mitochondrial function in patients with chronic obstructive pulmonary disease, including decreased mitochondrial enzyme activity, decreased muscle respiratory capacity, increased mitochondrial reactive oxygen species emissions, and denervation reinnervation of skeletal muscles, exacerbate muscle atrophy. This study also found that skeletal muscle dysfunction is associated with smoking. Studies have shown19 that patients with chronic obstructive pulmonary disease often have a history of smoking, and chronic activation of aromatic hydrocarbon receptors induced by tobacco smoke may be an important factor leading to mitochondrial damage, muscle atrophy and the denervation phenotype in patients with chronic obstructive pulmonary disease. A study17 曾 showed that during hospitalisation, the average daily walking time of COPD patients was less than 10 minutes, and the decrease in activity was a major cause of disuse atrophy of muscles, especially in the elderly. Muscle wasting and strength loss are more pronounced in the legs. In elderly COPD patients, quadriceps muscle strength and cross-sectional area decrease by 5% within 5 days of hospitalisation. The decrease in quadriceps muscle strength and cross-sectional area is associated with acute exacerbation, readmission and increased mortality in elderly COPD.
The limitations of this study are as follows: This study is a single-center study, which may limit the generalizability of the research results. Future research should adopt a multicenter design to increase the external validity of the results. This study used a cross-sectional design, which limits causal inference and lacks longitudinal data to track changes in skeletal muscle function over time. Although we performed sample size calculations during the research design phase, the lack of a formal power analysis may affect the reliability of the results. In addition, this study conducted multiple statistical comparisons without adjusting for multiple comparisons, which increased the risk of false-positive results. Future studies should adopt a longitudinal design, conduct a detailed efficacy analysis, and use appropriate statistical methods to control for errors caused by multiple comparisons. We will gradually improve these aspects in future research to enhance the scientific validity and clinical application value of the study.
Conclusion
In conclusion, our research indicates that patients with chronic obstructive pulmonary disease have skeletal muscle dysfunction, and skeletal muscle function progressively declines with the severity of chronic obstructive pulmonary disease; the weakening of respiratory muscle strength occurs earlier than the weakening of quadriceps muscle strength. Respiratory muscle strength, quadriceps strength, 6MWD and the severity of chronic obstructive pulmonary disease have some predictive value for the prognosis of patients with chronic obstructive pulmonary disease.
Data Sharing Statement
The data will be available upon reasonable request to the corresponding authors.
Ethics Approval and Informed Consent
Ethical approval was obtained from the human research ethics committee of the First People’s Hospital of Shuangliu District, Chengdu (batch number: 2021-02-01). We confirmed this study complied with the Declaration of Helsinki. All participants had signed the informed consent form.
Funding
This work was supported by grants from the Chengdu Medical Scientific Research Project (2021068, 2022103).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marklund S, Bui KL, Nyberg A. Measuring and monitoring skeletal muscle function in COPD: current perspectives. Int J Chron Obstruct Pulmon Dis. 2019;14:1825–1838. doi:10.2147/COPD.S178948
2. Taivassalo T, Hepple RT. Integrating mechanisms of exacerbated atrophy and other adverse skeletal muscle impact in COPD. Front Physiol. 2022;13:861617. doi:10.3389/fphys.2022.861617
3. McKee BJ, Regis SM, McKee AB, Flacke S, Wald C. Performance of ACR lung-RADS in a clinical CT lung screening program. J Am Coll Radiol. 2016;13(2 Suppl):R25–9. doi:10.1016/j.jacr.2015.12.009
4. Jaitovich A, Barreiro E. Skeletal muscle dysfunction in chronic obstructive pulmonary disease. what we know and can do for our patients. Am J Respir Crit Care Med. 2018;198(2):175–186. doi:10.1164/rccm.201710-2140CI
5. Lemmers J, Vonk MC, van den Ende C. Patient-reported outcomes to assess dyspnoea in interstitial lung disease and pulmonary hypertension: a systematic literature review of measurement properties. Eur Respir Rev. 2022;31:220091. doi:10.1183/16000617.0091-2022
6. Zou H, Zhang J, Chen X, et al. Reference equations for the six-minute walk distance in the healthy Chinese han population, aged 18-30 years. BMC Pulm Med. 2017;17:119. doi:10.1186/s12890-017-0461-z
7. Zou H, Zhang J, Zou Y, et al. Six-minute walking distance in healthy Chinese people older than 60 years. BMC Pulm Med. 2020;20:177. doi:10.1186/s12890-020-01211-w
8. Martinez FJ, Agusti A, Celli BR, et al. Treatment trials in young patients with chronic obstructive pulmonary disease and pre-chronic obstructive pulmonary disease patients: time to move forward. Am J Respir Crit Care Med. 2022;205:275–287. doi:10.1164/rccm.202107-1663SO
9. de Souza Y, Suzana ME, Medeiros S, Macedo J, da Costa CH. Respiratory muscle weakness and its association with exercise capacity in patients with chronic obstructive pulmonary disease. Clin Respir J. 2022;16(2):162–166. doi:10.1111/crj.13449
10. Cavalcanti JD, Fregonezi G, Sarmento AJ, et al. Electrical activity and fatigue of respiratory and locomotor muscles in obstructive respiratory diseases during field walking test. PLoS One. 2022;17:e0266365. doi:10.1371/journal.pone.0266365
11. Thome T, Miguez K, Willms AJ, et al. Chronic aryl hydrocarbon receptor activity phenocopies smoking-induced skeletal muscle impairment[J]. J Cachexia, Sarcopenia Muscle. 2022;13(1):589–604. doi:10.1002/jcsm.12826
12. Zhang L, Sun Y. Muscle-bone crosstalk in chronic obstructive pulmonary disease. Front Endocrinol. 2021;12:724911. doi:10.3389/fendo.2021.724911
13. Adami A, Corvino RB, Calmelat RA, et al. Muscle oxidative capacity is reduced in both upper and lower limbs in COPD. Med Sci Sports Exerc. 2020;52(10):2061–2068. doi:10.1249/MSS.0000000000002364
14. Ito A, Hashimoto M, Tanihata J, et al. Involvement of parkin-mediated mitophagy in the pathogenesis of chronic obstructive pulmonary disease-related sarcopenia. J Cachexia, Sarcopenia Muscle. 2022;13:1864–1882. doi:10.1002/jcsm.12988
15. Engelen M, Kirschner SK, Coyle KS, et al. Sex related differences in muscle health and metabolism in chronic obstructive pulmonary disease. Clin Nutr. 2023;42(9):1737–1746. doi:10.1016/j.clnu.2023.06.031
16. Li W, Wu Y, Yang X, et al. Association between muscular atrophy and mortality risk in patients with COPD: a systematic review. Ther Adv Respir Dis. 2024;18:17534666241304626. doi:10.1177/17534666241304626
17. Abdulai RM, Jensen TJ, Patel NR, et al. Deterioration of limb muscle function during acute exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197:433–449. doi:10.1164/rccm.201703-0615CI
18. Ammous O, Feki W, Lotfi T, et al. Inspiratory muscle training, with or without concomitant pulmonary rehabilitation, for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2023;1:CD013778.
19. Su J, Li J, Lu Y, et al. The rat model of COPD skeletal muscle dysfunction induced by progressive cigarette smoke exposure: a pilot study[J]. BMC Pulm Med. 2020;20(1):74. doi:10.1186/s12890-020-1109-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Disease Progression and Age as Factors Underlying Multimorbidity in Patients with COPD: Results from COSYCONET
Alter P, Kahnert K, Trudzinski FC, Bals R, Watz H, Speicher T, Söhler S, Andreas S, Welte T, Rabe KF, Wouters EFM, Sassmann-Schweda A, Wirtz H, Ficker JH, Vogelmeier CF, Jörres RA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1703-1713
Published Date: 29 July 2022
Phenotyping COPD Patients with Emphysema Distribution Using Quantitative CT Measurement; More Severe Airway Involvement in Lower Dominant Emphysema
Park J, Kim EK, Lee SH, Kim MA, Kim JH, Lee SM, Lee JS, Oh YM, Lee SD, Lee JH
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2013-2025
Published Date: 31 August 2022
Chronic Obstructive Pulmonary Disease Prevalence and Associated Risk Factors in Adults Aged 40 Years and Older in Southeast China: A Cross-Sectional Study During 2019–2020
Chen J, Yin Y, Zhang Y, Lin X, Chen T, Yang Z, Wang D, Zhong W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2317-2328
Published Date: 17 September 2022
Prevalence of Chronic Obstructive Pulmonary Disease in England from 2000 to 2019
Stone PW, Osen M, Ellis A, Coaker R, Quint JK
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1565-1574
Published Date: 21 July 2023
A Long-Term Study of Adverse Outcomes Associated With Oral Corticosteroid Use in COPD

Tse G, Emmanuel B, Ariti C, Bafadhel M, Papi A, Carter V, Zhou J, Skinner D, Xu X, Müllerová H, Price D
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2565-2580
Published Date: 15 November 2023