")
Back to Journals » Clinical Epidemiology » Volume 12
Sixty-Day Mortality Among 520 Italian Hospitalized COVID-19 Patients According to the Adopted Ventilatory Strategy in the Context of an Integrated Multidisciplinary Clinical Organization: A Population-Based Cohort Study
Authors Potalivo A, Montomoli J , Facondini F, Sanson G , Lazzari Agli LA, Perin T, Cristini F , Cavagna E , De Giovanni R, Biagetti C, Panzini I, Ravaioli C, Bitondo MM, Guerra D, Giuliani G, Mosconi E , Guarino S, Marchionni E, Gangitano G , Valentini I, Giampaolo L , Muratore F, Nardi G
Received 25 August 2020
Accepted for publication 7 December 2020
Published 30 December 2020 Volume 2020:12 Pages 1421—1431
DOI https://doi.org/10.2147/CLEP.S278709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eyal Cohen
Antonella Potalivo,1,* Jonathan Montomoli,1,* Francesca Facondini,1 Gianfranco Sanson,2 Luigi Arcangelo Lazzari Agli,3,4 Tiziana Perin,5 Francesco Cristini,6 Enrico Cavagna,7 Raffaella De Giovanni,8 Carlo Biagetti,6 Ilaria Panzini,9 Cinzia Ravaioli,10 Maria Maddalena Bitondo,1 Daniela Guerra,1 Giovanni Giuliani,1 Elena Mosconi,1 Sonia Guarino,1 Elisa Marchionni,6 Gianfilippo Gangitano,5 Ilaria Valentini,3,4 Luca Giampaolo,8 Francesco Muratore,7 Giuseppe Nardi1
1Department of Anaesthesia and Intensive Care, Infermi Hospital, AUSL della Romagna, Rimini, Italy; 2Department of Medicine, Surgery and Health Sciences, University of Trieste, Trieste, Italy; 3Department of Pneumology, Infermi Hospital, Rimini, Italy; 4Ceccarini Hospital, AUSL della Romagna, Riccione, Italy; 5Department of Emergency Medicine, Infermi Hospital, AUSL Della Romagna, Rimini, Italy; 6Department of Infectious Diseases, Infermi Hospital, AUSL della Romagna, Rimini,Italy; 7Department of Radiology, Infermi Hospital, AUSL della Romagna, Rimini, Italy; 8Department of Internal Medicine, Cervesi Hospital, AUSL della Romagna, Cattolica, Italy; 9Department of Clinical Research, AUSL della Romagna, Ravenna, Italy; 10Ausl della Romagna Health Care Service Direction, Ravenna, Italy
*These authors contributed equally to this work
Correspondence: Giuseppe Nardi
Department of Anaesthesia and Intensive Care, Infermi Hospital, AUSL della Romagna, Viale Settembrini 2, Rimini 47921, Italy
Tel +39 0541-705254
Fax +39 0541 705886
Email [email protected]
Purpose: Although the decision of which ventilation strategy to adopt in COVID-19 patients is crucial, yet the most appropriate means of carrying out this undertaking is not supported by strong evidence. We therefore described the organization of a province-level healthcare system during the occurrence of the COVID-19 epidemic and the 60-day outcomes of the hospitalized COVID-19 patients according to the respiratory strategy adopted given the limited available resources.
Patients and Methods: All COVID-19 patients (26/02/2020– 18/04/2020) in the Rimini Province of Italy were included in this population-based cohort study. The hospitalized patients were classified according to the maximum level of respiratory support: oxygen supplementation (Oxygen group), non-invasive ventilation (NIV-only group), invasive mechanical ventilation (IMV-only group), and IMV after an NIV trial (IMV-after-NIV group). Sixty-day mortality risk was estimated with a Cox proportional hazard analysis adjusted by age, sex, and administration of steroids, canakinumab, and tocilizumab.
Results: We identified a total of 1,424 symptomatic patients: 520 (36.5%) were hospitalized, while 904 (63.5%) were treated at home with no 60-day deaths. Based on the respiratory support, 408 (78.5%) were assigned to the Oxygen group, 46 (8.8%) to the NIV-only group, 25 (4.8%) to the IMV-after-NIV group, and 41 (7.9%) to the IMV-only group. There was no significant difference in the PaO2/FiO2 at IMV inception in the IMV-after-NIV and IMV-only groups (p=0.9). Overall 60-day mortality was 24.2% (Oxygen: 23.0%; NIV-only: 19.6%; IMV-after-NIV: 32.0%; IMV-only: 36.6%; p=0.165). Compared with the Oxygen group, the adjusted 60-day mortality risk significantly increased in the IMV-after-NIV (HR 2.776; p=0.024) and IMV-only groups (HR 2.966; p=0.001).
Conclusion: This study provided a population-based estimate of the impact of the COVID-19 outbreak in a severely affected Italian province. A similar 60-day mortality risk was found for patients undergoing immediate IMV and those intubated after an NIV trial with favorable outcomes after prolonged IMV.
Keywords: COVID-19, mechanical ventilation, mortality, noninvasive ventilation, multidisciplinary team approach, ARDS
Introduction
By the end of October 2020, the coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been responsible for almost 1.2 million deaths worldwide. The percentage of COVID-19 patients requiring non-invasive (NIV) or invasive mechanical ventilation (IMV) remains unclear and is strongly affected by hospital organization and availability of resources. Three studies from China, the US, and Germany reported that the use of IMV in hospitalized COVID-19 patients is 2.3%, 12%, and 17%, respectively.1–3 Intensive care unit (ICU) mortality among mechanically ventilated COVID-19 patients varies from 25% to 97%.2–10 Such wide variations may have different explanations. First, only a few studies that included all patients hospitalized for COVID-19 are able to provide a complete overview of the characteristics and outcomes of COVID-19 patients who required hospitalization. Second, information regarding the respiratory management of COVID-19 patients has been mainly elicited from the setting of ICUs.4,8,9,11 Thus, the number of hospitalized COVID-19 patients treated with oxygen supplementation and NIV has been markedly underreported, leading to inaccurate information regarding the overall use of the different respiratory supports and the outcomes. Third, most previous reports included a percentage of patients still admitted at the ICU at the end of the follow-up, ranging from 2.3%8 to 71%,2 and this may have led to different degrees of inaccuracy in estimating ICU mortality. Finally, the availability of ICU beds and human resources is likely to vary across different areas; this aspect has not been generally described in clinical studies, thereby affecting the generalizability of the results.12
The Province of Rimini in Northern Italy was one of the areas severely affected by the COVID-19 outbreak. On March 7, Rimini Province was declared a “Red Zone” due to the high number of infected people. Thereafter, it was isolated, with no possibility of entry or exit. Using clinical and demographic information that were routinely collected in a unique database that included all residents in the entire province, we performed the present population-based cohort study with the following aims: 1) to describe the characteristics of hospitalized COVID-19 patients; 2) to examine patient outcomes overall and stratified by the adopted respiratory support; and 3) to describe the organization of the local healthcare system.
Patients and Methods
Setting
The COVID-19 patients who were admitted to Rimini Hospital constituted the study cohort in the present historical observational population-based cohort study. The Italian National Public Healthcare System provides homogeneous and free access to any level of appropriate treatment for everyone, including irregular immigrants, through the hospital network, family doctors, and District Health Systems. The province of Rimini consists of approximately 340,000 inhabitants. It is served by a network of five public hospitals, with Rimini Hospital being the largest and providing up to 600 beds.
Since the beginning of the outbreak and for the entire duration of this study, Rimini Hospital was identified as a reference hospital for all COVID-19-positive or suspected patients. With the increase in the number of admitted patients, 340 hospital beds, including 80 beds in two newly opened wards, were progressively dedicated to infected subjects. Moreover, 28 negative pressure rooms—eight set up at the Emergency Department (ED) and 20 already available in the Infectious Diseases ward—were dedicated to patients requiring NIV. During the first 10 days of March, the number of ICU beds was progressively increased from 20 to 53, among which 48 were dedicated to COVID-19 patients and five to non-COVID-19 patients. Non-COVID-19 patients who were in excess of the local availability were transferred to another nearby hospital equipped with 10 ICU beds.
Study Population
All patients who were evaluated at one of the five EDs in the province from February 26 to April 18, 2020, presenting symptoms indicative of suspected COVID-19 (ie, fever and/or respiratory symptoms) and tested for the SARS-CoV-2 (real-time reverse transcriptase-polymerase chain reaction) were considered for inclusion.13 Patients with a positive swab, as well those with chest X-ray or CT scan presenting evidence of COVID-19-related pneumonia despite a negative swab, were included. The more stable patients were discharged and entrusted to primary care, while the patients identified to be at high risk for complications based on symptom severity and associated comorbidities were admitted at the hospital and represented the study population. All included patients with a first negative swab had at least a positive subsequent swab during the same hospitalization, except for the patients who died at the ED before a second swab was administered.
Organization
At the hospital level, an extremely strict prevention policy involving all facilities and healthcare providers was adopted to prevent possible viral transmission between the patients and the staff. Visitors were banned from the hospital, one-way “dirty-clean” paths were created within the care wards, and the use of gloves, FFP 2 or FFP3 masks (FFP2 for regular clinical activities and FFP3 for invasive aerosol generating procedures) masks, gowns, and protective goggles was made mandatory as appropriate. All staff involved in the COVID-19 patients’ care underwent an IgG/IgM rapid test every 30 days for screening and a nasopharyngeal swab. They were also quarantined in case of contact at risk (ie, not wearing adequate personal protective equipment), symptoms, or positivity during screening. Previously positive patients were considered no longer infected—and possibly no longer in need of isolation—after two negative swabs.
A daily meeting that was always attended by the heads of the Emergency, Infectious Disease, Pneumology, Radiology, and Intensive Care departments was set regardless of holidays or Sundays, with the above-described airborne and contact transmission precautions implemented to ensure homogeneous and standardized treatment for all COVID-19 patients. Every day, the relevant clinical information (eg, comorbidities, respiratory status, medical treatments, and active clinical conditions) of the critically ill cases were updated and the overall therapeutic stewardship to be adopted (eg, off-label medications, change in the respiratory support) was collegially discussed and agreed upon. Moreover, for each patient, the appropriate treatment to adopt in the event that his/her condition worsened was planned, taking into account the limitation of the available resources. All decisions were recorded and promptly communicated to the physicians and nurses working at all COVID-19 wards comprising the ICU.
Respiratory Support
Oxygen administration via a Venturi mask or a mask with reservoir was considered the standard of care for moderately/severely ill patients, while NIV (comprising continuous positive airway pressure, CPAP) and IMV following tracheal intubation were chosen for the most critical cases. To avoid airborne viral transmission, high-flow nasal cannulas were used only for respiratory weaning in patients who become negative, and a helmet was identified as the only interface to be used for NIV. As described above, the choice in the employed ventilatory strategy, such as the maximum level of intensity of care, was not defined a priori but was tailored for each patient, taking into consideration his/her general baseline conditions. In general, the conditions leading to the decision to start NIV or IMV were respiratory fatigue or worsening of gas exchange, notwithstanding oxygen/NIV. The prognostic criteria and resource availability (eg, ICU beds and mechanical ventilators) were also considered. Patients with one or more organ impairments other than respiratory failure were considered for IMV. For the patients who received IMV, protective ventilation was adopted following these general criteria: 6mL/kg VT that is reduced to 4mL/kg in the presence of low pulmonary compliance and positive end-expiratory pressure titration, taking into account the minimum driving pressure value and the delta PaCO2-ETCO2 to prevent possible over-distension. When necessary, the patients were administered a neuromuscular blocking agent to avoid the occurrence of the “fight the ventilator” phenomenon. The tracheal tube was replaced by percutaneous tracheostomy in cases of prolonged IMV. Extra-corporeal membrane oxygenation (ECMO) was considered for patients younger than 60 when less-than-marginal gas exchanges were achieved despite the maximal IMV support.
Based on the level of respiratory support, the study population was divided into the following subgroups: Oxygen (patients receiving no more than oxygen supplementation); NIV-only (patients receiving no more than NIV); IMV-after-NIV (patients undergoing IMV after a failed NIV trial); and IMV-only (patients starting IMV upon hospital admission or after a trial with oxygen).
Data Sources, Follow-Up, and Outcomes
For the whole population, the demographic data and hospital length of stay (LOS) were retrieved from an administrative and clinical database (Maria DB, Log 80, Forlì-Italy), while information about the administered off-label medications related to the COVID-19 treatment (ie, hydroxychloroquine, antivirals, steroids, canakinumab, and tocilizumab) were collected through clinical documentation. For patients treated with NIV and/or IMV, the Charlson comorbidity index was computed.14 The SpO2 upon hospital admission, the PaO2/FiO2 (P/F) ratio at the inception of NIV and IMV, and the duration of ventilatory supports were also collected. For those patients, the extent of lung damage was estimated from the chest radiogram using the Brixia score. Each lung was transversally divided into three sectors, and for each sector, a score ranging from zero (no alteration) to three (interstitial-alveolar infiltrates) was assigned (total score range: 0–18).15,16
For patients admitted to the ICU (ie, IMV-after-NIV and IMV-only), the Simplified Acute Physiology Score II (SAPS 2)17 and the Sequential Organ Failure Assessment (SOFA) score18 upon ICU admission were computed. In addition, the possible implementation of tracheostomy, ECMO, and renal replacement therapy was documented.
All patients were followed up to 60 days from hospital admission. The condition of being dead or alive after 30 and 60 days from hospital admission constituted the main study endpoints. Accordingly, data collection was concluded on June 18, 2020, to ensure at least 60 days of observation for the patients who were included last.
Ethical Aspects
The investigation conforms to the principles outlined in the Declaration of Helsinki. The AUSL della Romagna Institutional Review Board approved the project (Registration No. NCT04348448), with a waiver of informed consent, as the data included in the present study are routinely collected in everyday patient care and the treatments described represent the standard of care with no additional procedures or investigations requested or provided. All sensitive data were anonymized, stored, and processed in full compliance with the current legislation to guarantee patient data confidentiality.
Statistics
Continuous variables were described as mean ± standard deviation. The differences between the means were analyzed by paired or unpaired Student’s t-test as appropriate after considering whether the subgroups had equal variance using Levene’s test. One-way analysis of variance was applied for all comparisons between the subgroups. The nominal variables were presented as numbers and percentages and compared either through Χ2 test or Fisher’s exact test as appropriate.
The ability of the P/F measured before an NIV trial to predict NIV failure (ie, death or need for IMV) was tested by calculating the area under the receiver operating characteristics curve (AUC). The maximum Youden index (J) was considered as the optimal P/F cut-off value. Sixty-day mortality was computed using Kaplan–Meier technique overall and among groups. The Mantel-Cox Log rank test was adopted to assess differences among the survival rates. A multivariate Cox proportional hazard analysis was used to estimate 30-day and 60-day mortality risks among the study groups in comparison to the Oxygen group (reference group), adjusted by age, sex, and administration of steroids, canakinumab, and tocilizumab. The results were presented as a proportional hazard ratio (HR) with 95% CI and adjusted cumulative survival curves. Finally, in order to examine the potential impact of survival bias among the patients treated with IMV, especially among the patients intubated after NIV (a patient had to survive until endotracheal intubation), we computed the adjusted HRs for 10-day and 11- to 60-day mortality separately for sensitivity analysis. Moreover, minimally to fully adjusted HRs were reported in the Supplementary Materials (e-Figures 1 and 2, Table S1).
For all tests, statistical significance was set at an alpha level of p=0.05. All statistical analyses were performed using the software IBM SPSS Statistics version 24.0 (Armonk, NY, US: IBM Corp.).
Results
During the study period, 1,424 symptomatic patients were evaluated at the EDs in the province and had a positive swab and/or chest imaging that was indicative of suspected COVID-19. Nine-hundred and four (63.5%) were treated at home without further ED access, while the remaining 520 (36.5%) were hospitalized and constituted the study population (males 350, 67.3%; mean age 70.7 ± 14.1, range 19–98). Among the hospitalized patients, 440 (84.6%) were treated with oxygen supplementation at the time of hospital admission, while the remaining ones received either NIV or IMV. During the subsequent days, 57 patients (11.0%) required an upgrade of the ventilatory support. Almost all patients were treated with hydroxychloroquine and antiviral drugs. Table 1 presents the demographic characteristics, hospital LOS, and the administered medications of the study population overall and by groups. Figure 1 shows a complete synthesis of the respiratory support adopted and the 60-day mortality for each group.
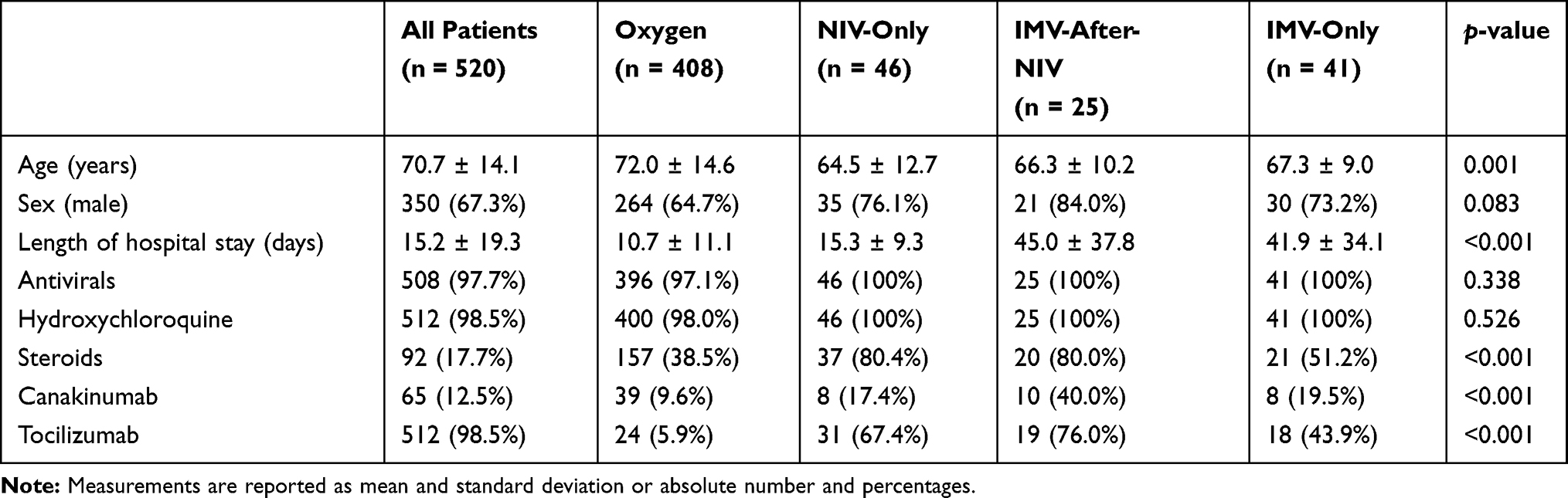 |
Table 1 Comparison of Demographic Characteristics and Administered Medications Among the Study Subgroups |
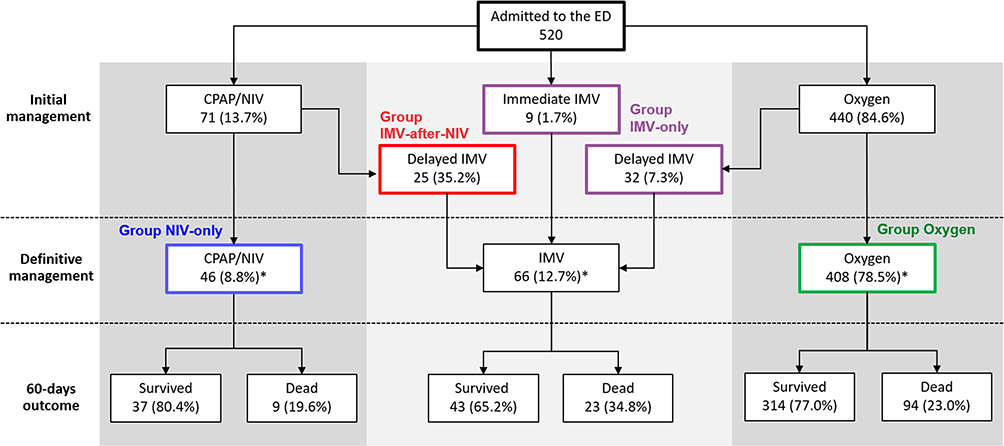 |
Figure 1 Flow chart synthesizing the clinical pathways of the COVID-19 patients, the respiratory support provided at each step of their hospital stay, and their 60-day mortality. Percentages refer to the previous level in the flow chart, unless otherwise indicated. *With respect to total hospital admissions. Abbreviations: CPAP, continuous positive airway pressure; NIV, non-invasive ventilation; IMV, invasive mechanical ventilation; ED, emergency department. |
Ventilatory Support
The main clinical characteristics of the 112 (21.5%) patients who received ventilatory support (NIV and/or IMV, mean age 66.9 ± 9.4 years) are reported in Table 2. Among them, 71 (63.4%) patients received at least one trial of NIV (mean age 65.1 ± 11.8) with a mean duration of 3.8 ± 2.2 days (range 1–10, Figure 2A) and a mean P/F ratio of 105.9 ± 40.6 at the beginning of NIV. Thirty-eight (53.5%) of the patients treated with NIV improved and were transferred to a COVID-19 ward, while 25 (35.2%) were intubated and admitted to the ICU to undergo IMV. The P/F ratio before starting NIV differed significantly between the patients with a successful trial and those who failed (successful: 119.4 ± 46.2; failing: 92.1 ± 23.8; p=0.003). For the patients who needed IMV, a statistically significant but clinically irrelevant improvement in the P/F ratio was documented (before NIV: 93.1± 23.8; before IMV: 113.8 ± 41.5; p=0.041). The remaining eight patients (11.3%) died without being intubated (P/F ratio before NIV 85.3 ± 36.5). The length of NIV did not differ among the patients with successful or failed trial (Table 2). The ability of the P/F ratio obtained before NIV to predict the failure of an NIV trial showed an AUC of 0.71 (95% CI 0.59–0.83; p-value 0.002) and provided a best cut-off of 115.5 (sensitivity 52.6%, specificity 81.8%; J 0.353).
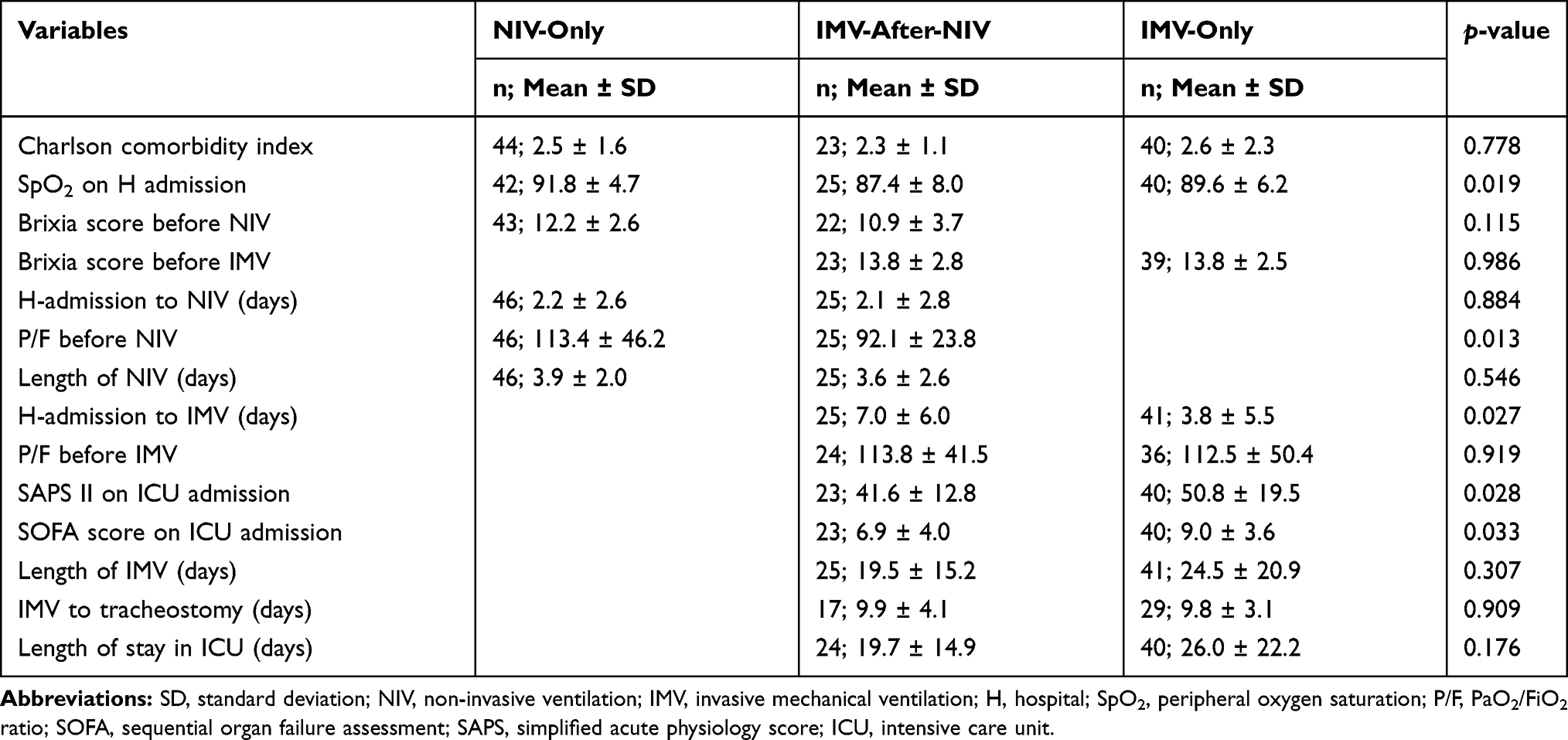 |
Table 2 Characteristics of Patients Receiving Either Invasive or Non-Invasive Mechanical Ventilation |
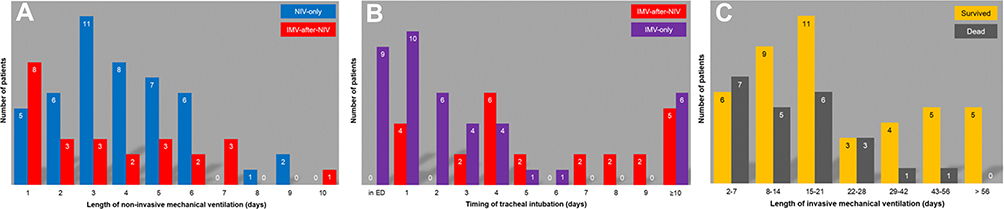 |
Figure 2 (A) Duration of continuous non-invasive ventilation (NIV) for patients who received at least one trial of NIV (n=71). (B) Interval between hospital admission and the onset of invasive mechanical ventilation (IMV) for patients admitted to the intensive care unit (n=66). (C) Length of IMV in patients who survived or died at the 60-day follow-up. |
Overall, 66 patients (Groups IMV-after-NIV and IMV-only, mean age 66.9 ± 9.4 years) were admitted to the ICU and treated with IMV (Figure 1). The mean interval between hospital admission and the onset of IMV was 5.0 ± 5.9 days (range 0–26) (Figure 2B). Eleven (15.2%) patients were intubated after 10 or more days from hospital admission (P/F before intubation: 113.0 ± 46.7). No difference in the P/F ratio at the time of the definitive ventilation support was found among the three study groups (p=0.993).
Patients who failed the NIV trial (n=21) had a Brixia score of 10.6 ± 3.4 before NIV, which worsened to 13.4 ± 2.5 (p=0.002) before IMV. A similar Brixia score was obtained at the time of endotracheal intubation among patients who failed an NIV trial and among patients who were treated with IMV without an NIV trial (Table 2).
Among the 66 patients admitted to the ICU, the mean duration of IMV was 22.6 ± 19.0 days (range 2–87). One patient underwent ECMO due to hypoxemia and hypercapnia incompatible with survival. Forty-six ICU patients (69.7%) received percutaneous tracheostomy (time from intubation: 9.8 ± 3.5 days). Renal replacement therapy was performed in 19 (28.8%) patients, with a mean duration of 21.7 ± 18.7 days.
Outcome
None of the 904 patients treated at home died during the follow-up. For the hospitalized patients the overall 30-day mortality was 22.5% (Oxygen: n=88, 21.6%; NIV-only: n=9, 19.6%; IMV-after-NIV: n=7, 28.0%; IMV-only: n=13, 31.7%; p=0.414, eFigure 1A) and the 60-day mortality was 24.2% (Oxygen: n=94, 23.0%; NIV-only: n=9, 19.6%; IMV-after-NIV: n=8, 32.0%; IMV-only: n=15, 36.6%; p=0.165, Figure 3A). Mortality among the 112 patients who received ventilatory support (NIV and/or IMV) was 25.9% and 27.7% after 30 and 60 days from hospital admission, respectively. No between-group difference either in the 30- (Log rank test: p=0.639, eFigure 1B) or in the 60-day (Log rank test: p=0.343, Figure 3A) mortality was found by comparing the crude Kaplan–Meier curves. Age was a risk factor for death in Groups Oxygen and NIV-only, but not for patients undergoing IMV. The relationships between some characteristics of the study groups and mortality are described in Table 3.
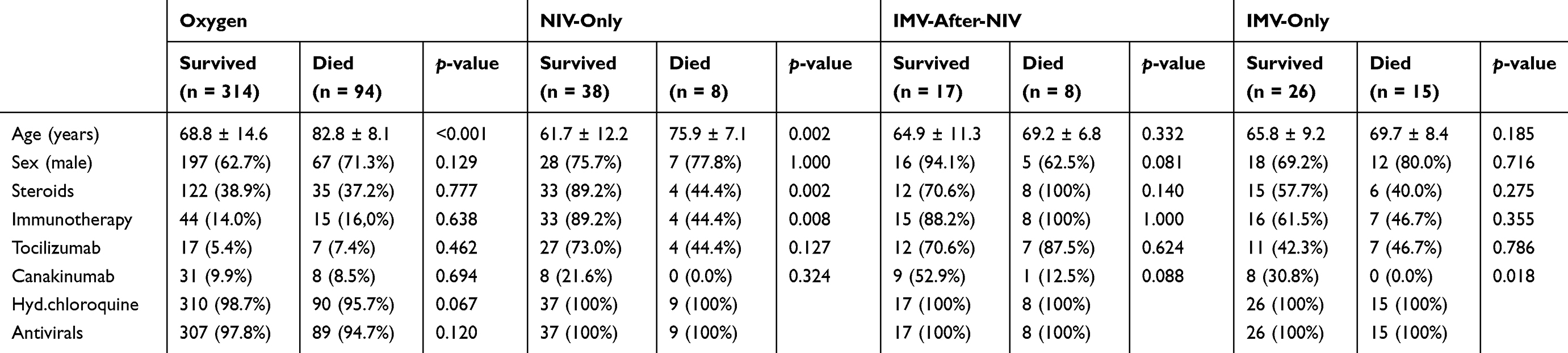 |
Table 3 Comparison of Mortality Rate Among Study Subgroups |
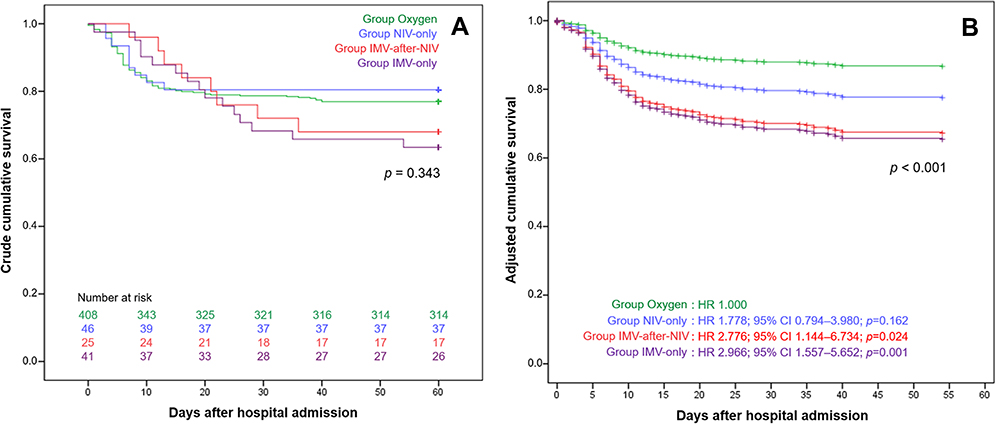 |
Figure 3 Crude (A) and adjusted (B) Kaplan–Meier curves for the risk of 60-day mortality in patients belonging to the study groups according to the provided respiratory support. |
The mean duration of IMV was 26.5 ± 21.1 days for the 43 patients who were alive at the end of the follow-up (range: 6–70) and 15.3 ± 11.5 days for the 23 non-survivors (range: 2–51). Among the 43 who survived, 14 patients (32.6%) underwent IMV for more than four weeks (Figure 2C). Two patients (one belonging to the IMV-after-NIV group and one to the IMV-only group) were still on IMV at the end of the follow-up period, with an IMV duration of 70 and 63 days, respectively. Interestingly, among the patients treated with IMV after NIV, the survivors showed on the average a lower number of days of NIV than the non-survivors, both for 30-day (non-survivors: 5.0 ± 2.8 days; survivors: 3.0 ± 2.3 days; p=0.078) and 60-day mortality (non-survivors: 5.0 ± 2.6 days; survivors: 2.9 ± 2.3 days; p=0.051). However, the difference did not reach statistical significance.
Compared with the Oxygen group, the multivariate Cox regression analysis showed both 30-day and 60-day mortality risks progressively increasing in the other groups, demonstrating statistical significant in the IMV-after-NIV group (30 days: HR 2.798; 95% CI 1.091–7.180; p=0.032; 60 days: HR 2.776; 95% CI 1.144–6.734; p=0.024) and the IMV-only group (30 days: HR 2.791; 95% CI 1.404–5.551; p=0.003; 60 days: HR 2.966; 95% CI 1.557–5.652; p=0.001), but not for the NIV-only group (30 days: HR 2.008, 95% CI 0.896–4.551; p=0.095; 60 days: HR 1.778; 95% CI 0.794–3.980; p=0.162) (eFigure 1B and Figure 3B). Among the explored covariates, only older age (30 days: HR 1.099, 955 CI 1.074–1.124, p < 0.001; 60 days: HR 1.097, 95% CI 1.073–1.120; p < 0.001) and male sex (30 days: HR 1.680, 1.105–2.555, p=0.015; 60 days: HR 1.597, 95% CI 1.072–2.379, p=0.021) showed statistically significant association with mortality. As expected, the sensitivity analysis showed a higher risk for 10-day mortality in the only-NIV group, but not in the patients receiving IMV compared to the patients treated with oxygen. Similar results to the main analysis were obtained for the 11- to 60-day mortality (e-Figure 2).
Discussion
Mortality According to Breathing Support
The present study showed how an integrated multidisciplinary clinical organization was able to optimize the allocation of the available resources among 520 hospitalized COVID-19 patients. The overall 30- and 60-day mortality were 22.5% and 24.2%, respectively. Approximately 21% of the patients were mechanically ventilated, with a mortality ranging from 19.6% in the patients treated with NIV-only to 36.6% in the patients undergoing IMV without an NIV trial. To our knowledge, this is the first study reporting 60-day mortality in a cohort of hospitalized patients diagnosed with COVID-19 overall and according to all adopted ventilatory strategies. A Chinese multicentric study enrolling 258 ICU patients reported an overall 60-day mortality of 64.3%, with 19 patients deceased within 48h after ICU admission.19 Among 165 mechanically ventilated patients, the 60-day mortality was 83%, 56%, and 94% for those treated with IMV, with NIV, and receiving both treatments, respectively. The median P/F ratio in the Chinese population was 91 (IQR 67–134) with a SOFA score of 6 (IQR 5–7). It should be noted that, in our study, we documented results for patients treated with NIV and/or IMV despite a similar P/F ratio (median 98.0; IQR 84.0–124.5) and a higher SOFA score (median 8; IQR 6–10), with a considerably lower 60-day mortality rate overall and in individual groups.
A study from six COVID-19 ICUs from the US enrolled 217 patients, 165 of whom (76.0%) received IMV, with a median IMV length of 9 days (IQR 4–13).4 Among the IMV subjects, ICU mortality was 33.9%, without any difference in IMV days between the deceased and the survivors. At the end of the follow-up (median observation time 15 [IQR: 9–24] days), hospital mortality was 35.7% (59/165), with eight patients still on IMV in the ICU. However, no information was provided either about the adopted respiratory support or the outcome for the patients not undergoing IMV. Although the mortality reported by Auld et al is similar to the mortality reported in our study in the IMV-only group, they reported a much shorter follow-up (maximum follow-up of 60 days), with 4.8% of the patients still at the ICU. Therefore, the 60-day mortality among those patients is likely to be higher than the reported hospital mortality. Recently, a nationwide study in Germany that included more than 10,000 hospitalized COVID-19 patients was published. Interestingly, although the Germany healthcare system has not been overwhelmed by the pandemic, the reported in-hospital mortality was markedly higher among patients treated with NIV (45% in patients with successful NIV, 50% in patients with failed NIV) and IMV (53% in patients treated with IMV). Meanwhile, it was lower in patients without mechanical ventilation (16%).3
Two other studies that considered ICU patients reported on all of the adopted breathing support strategies. An Italian multicentric study enrolling a cohort of 3,355 critically ill patients (median follow-up: 69 days; ventilatory support: IMV 87%, NIV 10%, CPAP/oxygen 2.3%) reported a mortality rate at the censoring (median observation time 70 [range, 38–112] days) of 17%, 36%, and 52% among patients treated with oxygen, NIV, and IMV, respectively.8 Accordingly, NIV and IMV were associated with an increased risk of death compared with patients treated only with oxygen (HR 2.36, 95% CI 1.33–4.17 and HR 3.77, 95% CI 2.19–6.51, respectively). Moreover, a study based on the RISC-19-ICU registry reported an ICU mortality of 9.5% (8/84), 25.0% (3/12), and 31.4% (86/274) among patients undergoing oxygen therapy, NIV, and IMV, respectively.9 Again, the mortalities reported in previous studies are likely to have underestimated the 60-day mortality. However, the mortality reported in the NIV and IMV groups in our study is lower than the mortality in the Italian study and similar to the mortality from the RISC-19-ICU registry. It should be noted that in all of the above-cited studies, the reported mortality for patients treated with standard oxygen and NIV was clearly conditioned by the reduced size of these subgroups, which is related to the study setting that is limited to the ICU.
Compared with the previously reported literature, the mortality reported in our study is generally lower. The centralized multidisciplinary approach adopted at Rimini Hospital may partially explain the difference with the existing literature. The sensitivity analysis and the differences between the crude and the adjusted HRs reported in the Supplementary Materials may help with the interpretation of the study findings. Interestingly, in the present investigation, mortality was higher in the oxygen and NIV-only groups in the first 10 days compared to the other two groups. This is partially explained by the survival bias among the mechanically ventilated patients, especially among the patients who were intubated after failing an NIV trial. Indeed, although the HRs for the 10-day mortality risk did not reach statistical significance, mortality risk was lower for patients intubated after a failed NIV trial only in the first 10 days of follow-up and not in the 11- to 60-day mortality. On the other hand, the fact that the oldest patients and those with severe coexisting diseases treated only with oxygen recorded a higher early mortality was clearly described by the differences between the crude HRs and the HRs adjusted only for age. This finding, together with the information of a mean IMV length of almost 20 days, may support the idea that those patients would not have survived to the IMV anyway and, therefore, endorse the decisions taken by the multidisciplinary team. Moreover, our results suggest that initial management of severe hypoxemia by oxygen or NIV might be a valuable alternative to immediate IMV in the event of limited available resources.
Thoughts on the Shared Decision-Making Process
The decision about the best breathing support to be provided to COVID-19 patients is anything but simple. Although often severely hypoxic, they tend to present less severe dyspnea than expected, probably because many patients, at least in the early stages of the disease, have normal pulmonary compliance and exert limited inspiratory efforts. In patients whose lung compliance tends to progressively decrease, the inspiratory effort increases and vigorous inspiratory effort can contribute to lung injury (Patient Self-Inflicted Lung Injury–P-SILI).20 This feature has been posited to increase morbidity and mortality. Therefore, early mechanical ventilatory support has been advocated for COVID-19-associated respiratory distress.21 Unfortunately, the criteria to intubate COVID-19 patients are controversial, and the decision may locally reflect the available resources.22
Older age and the comorbidity burden have been largely reported as the two main conditions associated with increased mortality risk,4,8,23 so prioritization of younger patients has been advised in case of shortage of resources.24 Notably, in the present investigation, although the non-survivors were older than the survivors in each of the four groups and each calendar year was associated with a 10% increased risk for mortality, the age difference was smaller and not statistically significant among survivors and non-survivors undergoing IMV. Moreover, the median age of patients submitted to IMV in our study (69 years) was slightly higher than that reported by other authors (59 to 64 years),2,4,8 suggesting that the adopted criteria at our institution were less restrictive in terms of age. Furthermore, once a patient was considered as potentially salvageable upon ICU admission and IMV, the length of IMV was not a criterion for treatment withdrawal. We strongly think that this ethically crucial decision could be widely considered.
Another interesting finding of our study was that a similar P/F ratio was found among patients treated with NIV-only or with IMV, either preceded by an NIV trial or not. Therefore, we speculated that a low P/F ratio should not be the only criterion to decide which patient would benefit from IMV. It should be noted that among the patients intubated after an NIV trial or receiving immediate IMV, the latter group had a higher SOFA score and SAPS (Table 2). These findings highlight the fundamental role played by our organizational strategy, which ensured a tailored treatment for each patient by taking into account the level of care that would better benefit her/him, and the daily re-discussion of each decision in light of new clinical reasons or changes in the resource availability. For example, during the very early phase of the outbreak, not all patients with appropriate indications were treated with NIV due to the scarcity of helmets. The subsequent increase in their availability allowed more targeted choices in the following days. Due to the scarcity of resources, especially in the initial phase of the emergency, for some patients, endotracheal intubation may have been postponed depending on their prognosis. Indeed, although without reaching statistical significance, our findings suggested that patients intubated after a longer NIV trial were less likely to survive compared to patients with a shorter NIV trial. On the other hand, many patients treated with NIV survived without undergoing IMV despite a low P/F ratio upon hospital admission.
The adopted strategy contributed in the creation of a more collaborative way to approach difficult decisions, thereby supporting healthcare professionals, especially the younger ones, in making such ethically and emotionally demanding decisions.22
Strength and Limitations
The main strength of the study consisted in having described the impact of the SARS-CoV-2 epidemic in an entire province. Since all patients with moderate to severe COVID-19 were managed at the same hospital, a shared and homogeneous standard of care was guaranteed. Moreover, in addition to the often-reported 30-day outcome, a further follow-up was established at 60 days, taking into account all respiratory supports and without patient loss. As many COVID-19 patients require prolonged IMV, a short follow-up time is a major limitation for the majority of reports published thus far.
Limitations are mainly related to the historical observational study design. Indeed, patient assignment to different ventilatory strategies was not at random but based on different conditions, such as the severity of the disease, pre-existing patient conditions, and available resources. As a consequence, the main study findings are not intended to explore causal relation between different ventilatory strategies and mortality, but rather, aims to provide an overview of how the adopted multidisciplinary centralized strategy affected patients’ outcomes in comparison with the existing literature. Moreover, the lack of information in the group of patients treated only with oxygen in terms of comorbidity, Brixia score, lung exchanges (such as P/F ratio and oxygen saturation), and other scores assessing patient severity prevented us from providing a mortality risk adjusted based on those conditions. Furthermore, previous information would have provided relevant knowledge for a more accurate interpretation of our findings. Finally, the number of patients requiring invasive mechanical ventilatory support was smaller compared to that in other studies.2,3,10 Consequently, the generalizability of our findings should be considered with caution.
Conclusion
The COVID-19 outbreak has strongly challenged the healthcare systems of many countries. A multidisciplinary panel in charge of the decision of the individualized breathing approach to adopt for hospitalized COVID-19 patients maybe be a valuable option to maximize 60-day survival, dealing with the imbalance between the available resources and the clinical needs. Our findings highlight the need for high-quality follow-up data that could support decision-making for the appropriate ventilatory support strategy for COVID-19 patients.
Disclosure
Jonathan Montomoli reports personal fees from Active Medical BV, outside the submitted work. The authors report no other potential conflicts of interest for this work.
References
1. Guan W, Ni Z, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
2. Richardson S, Hirsch JS, Narasimhan M, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City Area. JAMA. 2020;323(20):2052. doi:10.1001/jama.2020.6775
3. Karagiannidis C, Mostert C, Hentschker C, et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: an observational study. Lancet Respirat Med. 2020;8(9):853–862. doi:10.1016/S2213-2600(20)30316-7
4. Auld SC, Caridi-Scheible M, Blum JM, et al. ICU and ventilator mortality among critically ill adults with coronavirus disease 2019. Crit Care Med. 2020. doi:10.1097/CCM.0000000000004457
5. ICNARC. Intensive Care National Audit & Research Centre (ICNARC) report on COVID-19 in critical care - 17 July 2020. Available from: https://www.icnarc.org/Our-Audit/Audits/Cmp/Reports.
6. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respirat Med. 2020;8(5):475–481. doi:10.1016/S2213-2600(20)30079-5
7. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
8. Grasselli G, Greco M, Zanella A, et al. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern Med. 2020;180(10):1345. doi:10.1001/jamainternmed.2020.3539
9. Wendel Garcia PD, Fumeaux T, Guerci P, et al. Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: initial report of the international RISC-19-ICU prospective observational cohort. EClinicalMedicine. 2020;25:100449. doi:10.1016/j.eclinm.2020.100449
10. Cummings MJ, Baldwin MR, Abrams D, et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study. Lancet. 2020;395(10239):1763–1770. doi:10.1016/S0140-6736(20)31189-2
11. Quah P, Li A, Phua J. Mortality rates of patients with COVID-19 in the intensive care unit: a systematic review of the emerging literature. Crit Care. 2020;24:1. doi:10.1186/s13054-020-03006-1
12. Qian Z, Alaa AM, van der Schaar M, Ercole A. Between-centre differences for COVID-19 ICU mortality from early data in England. Intensive Care Med. 2020;46(9):1779–1780. doi:10.1007/s00134-020-06150-y
13. Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance. 2020;25(3). doi:10.2807/1560-7917.ES.2020.25.3.2000045
14. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
15. Borghesi A, Zigliani A, Masciullo R, et al. Radiographic severity index in COVID-19 pneumonia: relationship to age and sex in 783 Italian patients. Radiol Med. 2020;125(5):461–464. doi:10.1007/s11547-020-01202-1
16. University of Brescia. Data mining and machine learning for the development of risk-predicting models in patients with Covid-19 pneumonia, based on the chest x-ray Brixia-severity score and lab tests. Available from: https://bodai.unibs.it/covid19brixia/.
17. Le Gall JR, Lemeshow S, Saulnier F. A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. JAMA. 1993;270(24):2957–2963. doi:10.1001/jama.270.24.2957
18. Vincent JL, de Mendonça A, Cantraine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit Care Med. 1998;26(11):1793–1800. doi:10.1097/00003246-199811000-00016
19. Xu J, Yang X, Yang L, et al. Clinical course and predictors of 60-day mortality in 239 critically ill patients with COVID-19: a multicenter retrospective study from Wuhan, China. Crit Care. 2020;24(1). doi:10.1186/s13054-020-03098-9
20. Gattinoni L, Chiumello D, Rossi S. COVID-19 pneumonia: ARDS or not? Crit Care. 2020;24(1). doi:10.1186/s13054-020-02880-z
21. Gattinoni L, Chiumello D, Caironi P, et al. COVID-19 pneumonia: different respiratory treatments for different phenotypes? Intensive Care Med. 2020;46(6):1099–1102. doi:10.1007/s00134-020-06033-2
22. Vergano M, Bertolini G, Giannini A, et al. Clinical ethics recommendations for the allocation of intensive care treatments in exceptional, resource-limited circumstances: the Italian perspective during the COVID-19 epidemic. Crit Care. 2020;24(1). doi:10.1186/s13054-020-02891-w
23. Reilev M, Kristensen KB, Pottegaard A, et al. Characteristics and predictors of hospitalization and death in the first 9,519 cases with a positive RT-PCR test for SARS-CoV-2 in Denmark: a nationwide cohort. Epidemiology. 2020. doi:10.1101/2020.05.24.20111823
24. Haas LEM, de Lange DW, van Dijk D, van Delden JJM. Should we deny ICU admission to the elderly? Ethical considerations in times of COVID-19. Crit Care. 2020;24(1). doi:10.1186/s13054-020-03050-x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.