Back to Journals » Advances in Medical Education and Practice » Volume 13
Simulation-Based Education Implementation in Pharmacy Curriculum: A Review of the Current Status
Authors Korayem GB ![]() , Alshaya OA
, Alshaya OA ![]() , Kurdi SM, Alnajjar LI
, Kurdi SM, Alnajjar LI ![]() , Badr AF
, Badr AF ![]() , Alfahed A, Cluntun A
, Alfahed A, Cluntun A
Received 17 March 2022
Accepted for publication 20 June 2022
Published 1 July 2022 Volume 2022:13 Pages 649—660
DOI https://doi.org/10.2147/AMEP.S366724
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Ghazwa B Korayem,1 Omar A Alshaya,2– 4 Sawsan M Kurdi,5 Lina I Alnajjar,1 Aisha F Badr,6 Amjaad Alfahed,1 Ameera Cluntun7
1Department of Pharmacy Practice, College of Pharmacy, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 2Department of Pharmacy Practice, College of Pharmacy, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 3Pharmaceutical Care Services, King Abdulaziz Medical City, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 4King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 5Department of Pharmacy Practice, College of Clinical Pharmacy, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 6Pharmacy Practice Department, Faculty of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabia; 7Curriculum and Training Department, Health Academy, Saudi Commission for Health Specialties, Riyadh, Saudi Arabia
Correspondence: Amjaad Alfahed, Department of Pharmacy Practice, College of Pharmacy, Princess Nourah bint Abdulrahman University, 11564 King Khalid International Airport, P.O. Box: 84428, Riyadh, Saudi Arabia, Tel +966 564321410, Email [email protected]; [email protected]
Abstract: Simulation-based education (SBE) is a fundamental teaching method that complements traditional teaching modalities. SBE has improved students’ knowledge, understanding, and numerous essential skills within undergraduate pharmacy education, similar to traditional teaching methods. However, SBE has become crucial for developing students’ teamwork, decision-making, and communication skills. Even though the Accreditation Council for Pharmacy Education (ACPE) has acknowledged the benefit of SBE in interprofessional education (IPE) and the introductory pharmacy practice experience (IPPE). This article provides evidence that SBE can be effective beyond that. This narrative review is focused on the literature related to SBE modalities and the assessment methods of student learning outcomes in the undergraduate pharmacy curriculum. The review illustrates that SBE is an effective teaching method that could be utilized within the pharmacy curriculum. The review also could help pharmacy educators decide on the best modality and placement of integrating patient simulation within the pharmacy curriculum. Combining multiple simulation techniques may be the best way to achieve the desired student learning outcomes.
Keywords: patient simulation, pharmacy, education, simulation-based education, pharmacy curriculum
Background
Pharmacy education has evolved with the progression of the pharmacist role.1 The emphasis on patient-centered care has become the core of the pharmacy curriculum.1 As clinical pharmacy continues to develop, pharmacy students are expected to play a vital role in direct patient care.2 Therefore, several innovative teaching approaches have been implemented to enhance students’ pharmaceutical knowledge and clinical skills.2 There is a massive shift in pharmacy education from traditional teaching methods into active learning methods.3 Active learning includes class discussions, project-based learning, problem-based learning, case studies, and simulation.4
Simulation-based education (SBE) is one of the teaching strategies that has been widely used in health profession education. Simulation-based learning is defined as “An array of structured activities representing actual or potential situations in education and practice„.5,6 These activities allow participants to develop or enhance their knowledge, skills, and attitudes or analyze and respond to realistic situations in a simulated environment.7 Patient simulation has been shown to be an effective teaching and assessment approach that replicates a patient within a clinical scenario in an educational setting.8 It offers a controlled teaching environment for learners that is equivalent to realistic experiences without compromising patients’ safety.9 Simulation application in health education is never limited to utilizing technologies. Instead, it is a technique used to replicate the real experience.10,11 Therefore, simulation techniques include all of the following: mannequins, part-task trainers, role-play (RP), standardized patients (SP), computer-based systems (CBS), virtual reality (VR), and gaming.11,12
Medical patient simulations originated in ancient times but advanced during the 1900s.13 Patient simulation was first presented in medical learning and then expanded to other health disciplines.13 Modern simulation was initially started using patient actors to teach medical students prior to the development of high-fidelity simulation.14 Medical and nursing schools mostly use manikins to help develop students’ clinical and communication skills.6 The first documented human patient simulation utilization in the pharmacy curriculum was at the University of Pittsburgh in 2006.15
In 2007, the Accreditation Council for Pharmacy Education (ACPE) revised its accreditation standards to recommend using a hybrid of didactic, simulation, and experiential methods in teaching the pharmacy curriculum.16 However, they encouraged simulation specifically in interprofessional education (IPE) and introductory pharmacy practice experience (IPPE).16 The ACPE limited the duration of simulated practice experience to no more than 20% of the total IPPE required hours.16 It also presented the types of simulation that pharmacy schools need to consider for IPPE and IPE, including virtual reality software, low- or high-fidelity manikins, role play, virtual environments, and standardized or virtual patients.17 Nonetheless, over the past decade, several pharmacy schools have implemented various SBE methodologies in advanced pharmacy practice experiences (APPE) courses and others in the pharmacy curriculum.18–22 During the COVID-19 pandemic, SBE emerged as an effective alternative teaching strategy due to its flexibility and the ability to train large numbers of students at various levels while maintaining students’ and patients’ safety.23–25 Nonetheless, SBE should not always be perceived as an alternative teaching strategy; instead, it is a fundamental teaching method that complements traditional teaching.
This article presents a review of the utilization of patient simulation, including the type of simulation utilized, location in the curriculum, topics, intended learning outcomes, and assessment methods. In addition, we reviewed the needed resources, opportunities,challenges, and the published articles in which patient simulations were performed. We also assessed the student learning outcomes within undergraduate pharmacy education between 2007 and May 2021. After the literature review, six experts in the field of pharmacy and simulation education gathered to summarize the current literature and provide recommendations about the best implementation of SBE technologies within the pharmacy curriculum based on the literature and their expertise.
Patients Simulation Implemented in Pharmacy Curriculum
Standardized Patients (SPs)
Description
SPs refer to well-trained specialists who portray the case of a real-life patient in a consistent and replicable performance to different students and provide responses that vary based on the students’ performance.7,26 The SP portrayal should involve all aspects of the presented patient case, including but not limited to medical history, signs and symptoms, physical findings, emotional and personal characteristics, and body language. SPs may also assess students and provide feedback on their performance.7,26
Implementation in the Pharmacy Curriculum
Utilizing SPs in pharmacy education has been widely reported in the literature as an effective complementary teaching modality to advance clinical pharmacy education.27–33 Many learning outcomes can be achieved using this modality, ranging from advancing patient interviewing and history-taking skills to the optimal implementation and monitoring of a pharmacotherapy plan.34 The SP modality can be utilized in various courses throughout the pharmacy curriculum and at various student levels, especially when the learning objectives are aimed to boost students’ confidence and develop the students’ professional skills, such as patient interviews and communication skills, clinical knowledge, and practice, cultural and emotional competence, and team-based skills. Courses that focus on pharmacotherapy, immunization, medication therapy management, and psychiatry are some examples where SP could be utilized. In addition, the standardization in the SP modality makes it an excellent modality to use in high-stake assessments where the responses to students are standardized among all participating students.
Pharmacy schools could recruit paid or volunteer actors to play the role of the SP, train their faculty members to play this role, or utilize student peers. Each strategy carries some advantages and disadvantages that should be weighed when choosing between them for specific learning experiences. Paid or volunteer actors are mostly flexible and available when needed and unfamiliar with students; however, they require more training time and may be costly on some occasions. Faculty members are a great resource to play this role, as they need less training and provide high-quality assessments and feedback; however, their availability is not guaranteed all the time.
Using simulation through SPs has been proven to improve students’ knowledge, perception,30–32 cultural skills, and communication skills.27,28 Tailoring the SP experience to the student’s specific areas of improvement in communication skills showed better performance and satisfaction when compared to a non-tailored standardized patient group.35 Although simulation through SPs did improve the attainment of various learning outcomes, it does hold some limitations, such as high cost, the need for well-structured training, and the scarcity of validated and reliable assessment tools, as shown in Table 1. The process of recruiting, training, and preparing SPs is expensive, despite the literature showing its cost-effectiveness.26,28,36
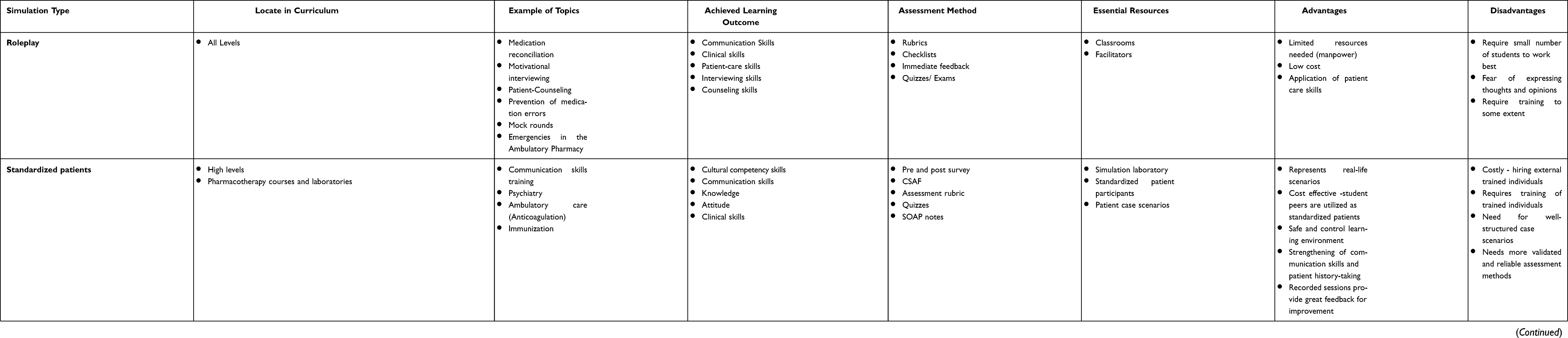 |
Table 1 Summary of the Features of Various Types of Patient Simulation Utilized in the Pharmacy Curriculum |
Recommendation
The SP modality should be incorporated throughout the pharmacy curriculum in courses that involve higher-level skills with the utilization of faculty members or student peers to perform the SP role, given the high cost associated with recruiting outside performers. Assessments of student encounters with SPs can be performed through immediate feedback, rubrics, pre and post surveys, SOAP notes, and quizzes.
Role-Play (RP)
Description
Role-play (RP) is a well-known learning practice in which students perform various roles in a simulation of real-life situations.37 During role-play, a peer student (co-learner) may impersonate a patient, caregiver, or health care provider within a clinical scenario.38 If the role is played with an individual who is trained to act as a patient or a family member, this can fall under an SP, as discussed earlier in this review.38 This allows students to practice realistic experiences while remaining in a controlled environment.
Implementation in the Pharmacy Curriculum
Many pharmacy programs have reported successfully using RP to teach a wide range of skills in several core or elective courses and laboratories.9,39–48 Moreover, it can be used in all levels of the pharmacy curriculum, including APPE.9,39–48 Despite the variations in the application method, several researchers have reported positive outcomes regarding students’ communication skills,9,42–48 motivational interviewing skills47,48 medication reconciliation,46 patient presentation skills,45 patient and self-care,43 and patient counseling.41 Furthermore, students have reported increased confidence,41 knowledge,44 and engagement.48 All of these outcomes have been assessed using various methods, such as rubrics, checklists, immediate feedback, and exams.41,43–46,48
RP is considered one of the simplest simulation methods due to the ease of its application. It does not require many resources other than sufficient space, human resources, and sometimes money. However, training the faculty, students, or paid actors to play the role needed is time consuming. Furthermore, finding enough instructors is sometimes challenging when there are many students.45 Language barriers have also been reported to be a drawback of this method, as it can result in a lack of understanding and fear of expression.46 More details are presented about the advantages and disadvantages in Table 1.
Recommendation
Simulation using RP should be implemented at all levels within the pharmacy curriculum, especially when teaching and practicing patient-care skills. Most RP simulations can be assessed using rubrics and immediate feedback.
Manikin-Based Simulation (MBS)
Description
Manikins are classified according to their levels of physiologic function; the simulation replicates real life with low-fidelity, medium-fidelity, and high-fidelity mannequins.7 Low fidelity refers to part-task trainers, static mannequins, or dolls.49 Medium fidelity utilizes manikins or task trainers with limited physiological functions.31 In contrast, high-fidelity mannequin simulators present a full-body mannequin that physiologically reacts like a “real” patient and has a voice based on computer programs.31 Manikin-based simulations (MBSs) combined with other simulation types, such as SPs or RP, have been widely implemented in the pharmacy curriculum, especially in experiential training.9,21,50
Implementations in the Pharmacy Curriculum
Several pharmacy schools have utilized and assessed MBSs in pharmacy curriculum in core and elective pharmacotherapy courses,18,31 pharmacotherapy practice laboratories,26 and certification programs,33 in addition to mannequin-based simulator integration in IPPE and APPE.21,33 Overall, MBSs have more frequently been used for advanced level pharmacy students.26,32,34 This is expected, as pharmacotherapy courses and parallel laboratories are usually delivered at high pharmacy student levels. Moreover, many elective and certificate programs were built on preexisting knowledge from fundamental courses offered early in the pharmacy curriculum.
Nonetheless, most pharmacy schools have implemented MBSs in managing acutely ill patients with arrhythmia, decompensated heart failure, hypertensive crisis, or coronary syndrome.15,18,51 Only a few schools have used MBSs in ambulatory care or non-acute settings,33,52 as shown in Table 1. Evidence has shown that implementing SBE using MBSs within the pharmacy curriculum has improved students’ learning, critical thinking, problem-solving, communication, clinical skills,18,26,33,34 and information retention.21,32 The use of mannequins in SBE can expose the students to high-risk and rare medical diseases. The benefit of MBSs has been evaluated through exams and OSCEs.15,18,53–55 MBS has been shown to significantly benefit pharmacy learners through connecting didactic coursework with actual experiences.26,33,34 However, it still has several drawbacks, as presented in Table 1. Some major disadvantages include the extensive resources needed to apply such a simulation, including equipment, facilities, and advanced technical skills.18,52,56 Moreover, the costs for resource acquisition, implementation, maintenance, and training are high.53 MBS also may require many facilitators for a small group of learners,53,56 is labor-intensive and requires extensive logistics and time for arrangement and preparation.19,55,57
Recommendation
- MBS should be implemented as an active teaching method for high-level students within the pharmacy curriculum for acute and primary care situations, and formative or summative assessment methods should be used.
Computer-Based Simulation (CBS)
Description
Advancements in technology have allowed pharmacy students to experience patient care without stepping into an actual pharmacy. Computer-based simulation (CBS) software and applications bring the experience into the classroom setting in an innovative and engaging manner.57,58 Virtual reality (VR), also known as augmented reality, is a type of CBS where simulation software is utilized to aid pharmacy students in learning specialized tasks or situations.59,60 It combines multimedia elements, such as audio, graphics, and animation, with textual information. VR simulation software mimics reality by modeling a clinical setting, outpatient/community pharmacy, or how to deal with a virtual patient.6,61 Some examples of these simulation programs include Mydispense®, Pharmacy Simulator,36,49 DecisionSim™, and virtual patients software.54,55
Implementation in the Pharmacy Curriculum
Many pharmacy colleges have applied VR simulation as a teaching method in various courses at different points of the pharmacy curriculum.62–64 For instance, software programs such as Cyber Patient and Virtual Organ Bath have been used in pharmacokinetics and pharmacodynamics lectures.62 This has led to higher learning and understanding when compared to traditional lecture-based teaching.62 MyDispense, developed at Monash University, Australia, is another popular software program that simulates an authentic community pharmacy.63 MyDispense software has been integrated into IPPE and therapeutic courses.64,65 The use of such software has had positive effects on exam scores.64 However, a randomized, parallel-group design was conducted at a private college of pharmacy to compare problem-based learning (PBL) and virtual simulated patient cases and found that the post-experience PBL scores were higher.66 This suggests that a varied approach to simulated patient cases in education may lead to greater learning outcomes.66
CBS offers many advantages in providing an adaptable, flexible, and accessible virtual pharmacy environment that maximizes the realism of actual patient-centered care at a low level of risk and relatively low cost compared to SP or manikins simulation.57,58 It allows a high level of interactivity57,67 and immediate feedback49,57,58 and simultaneously caters to a large number of students.58,61 Virtual patients’ demographic characteristics and comorbidities can be easily changed in virtual scenarios to follow the curricula and achieve the intended learning outcomes, as presented in Table 1.68 These learning outcomes include critical thinking, decision making, problem solving, communication skills, and information retention.55,68 However, CBS still has its limitations related to the management of hardware and software, technical support, and unreliable internet connections, as presented in Table 1.
Generally, published reports exploring the application of CBS in the pharmacy school curriculum are limited. However, the previous applications have been mainly used for higher-level students in comprehensive courses, therapeutic courses, and preparation before IPPE. Moreover, further studies are needed to assess the achievement of intended learning outcomes and integration into the curriculum.
Recommendation
CBS should be implemented in combination with other simulation techniques at all levels of the pharmacy curriculum along with pre and post-examinations and performance tests to help assess whether the desired learning outcomes have been achieved.
Serious Gaming (SG)
Description
Serious gaming (SG) is a relatively new concept of teaching that incorporates simulation.69 Even though SG itself is not a simulation modality, it encompasses simulation activities using play for problem solving instead of entertainment.69 SG is designed for educational purposes rather than entertainment.7 Within SG, real-world events or processes are simulated to solve problems.7
Implementation in Pharmacy Curriculum
The 2013–2014 Academic Affairs Committee of the American Association of Colleges of Pharmacy (AACP) recommended that SG be incorporated in pharmacy education.70 Faculty and student innovation in designing and implementing SG can be used to prepare future health care leaders.70 As a result, the use of SG in pharmacy education has gained popularity in the past decade, particularly in in-patient simulations. Although most published research on gamification has aimed to assess student perceptions of these games, some have also assessed pre-and post-knowledge gain. For instance, the use of escape rooms resulted in a significant difference in knowledge and cognitive learning outcomes.71–81 Escape rooms are a popular simulated gamification tool utilized in the enhancement of pharmacy student learning outcomes.74,81 The rooms are used for groups or individuals who work to resolve several clues to “escape” simulated scenarios in a designated time frame.76
Most researchers have described the utilization of simulated SG in the early years of pharmacy education, including the first, second, and third years. Simulated gamification can be implemented to help students examine various pharmacotherapy topics, including diabetes,75,81 heart failure,80 cancer,78 toxicology,73 non-sterile compounding,74 geriatrics,82 and others, such as disaster preparedness,79 skill-based leadership,76 opioid medication safety, medication history taking,71 and APPE readiness.77 Moreover, in past experiences, SG has proven to be impactful on students’ knowledge and learning experiences.73,74
The apparent advantage of using SG is that students find it fun and engaging,73–83 but these games also aim to build leadership, communication, problem-solving, and teamwork skills.76 More details about the advantages, disadvantages, and essential resources for SG are presented in Table 1. Several studies have highlighted the great potential of IPE using SG 67,68,72,74,76, and the remarkable adaptability of the game to use for any subject and in classes of any size.71,75,77,81 However, these published studies lacked validity and reliability of the methods used since they mainly were pilot studies.71–81 One of the drawbacks with SG was the fluctuating costs reported in these studies, which ranged from $0 to $400, and its dependence on available resources and funds.74,75,77,79
Although positive outcomes have been reported, SG is still considered a relatively new concept to pharmacy educators and may require further studies to assess its use in simulation practice in the pharmacy curriculum.83 SG helps build extracurricular skills such as leadership, communication, problem-solving, and teamwork.
Recommendation
SG should be incorporated into various courses and within different levels of pharmacy education. The use of pre- and post-knowledge assessments is mandated to test the validity of the SG implemented.
Hybrid Simulation
Description
This describes the use of two or more simulation modalities in the same scenario to enhance the reality of the experience.7 Primarily, this involves the use of MBS with supporting techniques to mimic real-life scenarios. These supporting methods include RP (involving another member of the health team or a caregiver), SPs, or CBS. Even though each of the mentioned simulation modalities has its advantages and disadvantages, the choice of the best SBE fit within the course depends on the desired learning outcomes.
Implications in the Pharmacy Curriculum
Numerous previous experiences in pharmacy education have involved the use of MBS with RP or SP.21,74,84 Using hybrid SBE methods may be the best way to achieve the intended student learning outcomes. Hybrid simulation has proven to help students improve their knowledge, understanding, communication, and psychomotor skills.19,21,34,54,55,84 However, its implementation may require extra resources, time, and workforce members. Previous reports have indicated the use of hybrid simulation in advanced pharmacy levels, including APPE. Various assessment methods have been used to evaluate student achievement, including summative and formative assessments, depending on the simulation modalities used and the intended learning outcome of the scenario.
Recommendation
Hybrid simulation is the best method to implement simulation scenarios to mimic real-world experiences for high-level pharmacy students and can be assessed using either summative or formative methods.
Future Recommendations About Patients-Simulation Implementation in the Pharmacy Curriculum
- Further studies are needed to assess the use of MBS within the pharmacy curriculum in non-acute care settings.
- Cost-effectiveness studies about patient simulation implementation within the pharmacy curriculum are needed given the high cost of some simulation methods.
- The integration of RP, SP, SG, and CBS should be explored for advanced pharmacotherapy courses, disease management, and care implementation within pharmacy school curricula.
Simulation Implemented in Interprofessional Education
IPE is defined as an experience involving two or more health care professionals who work collaboratively and learn from, with, and about each other to improve patient care.85 This educational strategy has improved communication and the learning experience between pharmacy students and other health care professionals. The ACPE accreditation standards were establish to enforce the implementation of IPE in pharmacy curricula so that students can learn to be an active members of an interprofessional team.16 The ACPE also encourages pharmacy schools to implement interprofessional simulation (sim-IPE) experiences and the utilization of simulation into IPE so that students can understand the scope of practice of team members.16
The researchers who have previously applied sim-IPE for pharmacy students have mostly used hybrid simulations using human patients and MBS with SPs and/or RP.20,86,87 They have demonstrated the possibility of enhancing students’ attitudes, teamwork skills, confidence, and communication with other healthcare professionals.87–90 Most IPE experiences have involved high-level pharmacy students or APPE.85,88–90 IPE primarily uses high-fidelity simulation within its activities to help students better understand the pharmacist’s role on the interdisciplinary team.
The major challenge in applying IPE within the pharmacy curriculum is finding the best course that fits its implementation and the arrangement with other health discipline schools.87,90 In addition, IPE activities usually include a limited number of students in each session to achieve the desired outcomes.87 Sim-IPE also carries the drawbacks of the types of simulation it utilizes, such as the need for resources, logistic arrangements, and extra cost. Thus, we suggest incorporating IPE within the pharmacotherapy laboratories of high-level pharmacy students, and advanced experiential training may be the best fit for IPE in the pharmacy curriculum.
Conclusion
Similar to traditional teaching methods, SBE has improved students’ knowledge, understanding, and numerous essential skills within undergraduate pharmacy education. This review highlights various modalities of simulation and their incorporation into pharmacy curricula. It can help pharmacy educators identify the best type and placement of integrating patient simulation within the pharmacy curriculum to achieve the intended student learning outcomes. The SBE method is crucial for developing skills (eg, teamwork, decision making, and communication) that are difficult to achieve by conventional methods.
Even though the ACPE acknowledged SBE benefits in IPE and IPPE, this article provides evidence that they are effective within all pharmacy curricula. Combining multiple simulation techniques may be the best way to achieve the desired student learning outcomes. Some gaps in the literature involving the use of SBE in pharmacy education have been identified and need to be further investigated in future studies.
Abbreviations
ACPE, Accreditation Council for Pharmacy Education; APPE, Advanced pharmacy practice experience; CBS, Computer-based simulation; COVID-19, Coronavirus 2019; CSAF, Communication Skills Assessment Form; IPE, Interprofessional education; Sim-IPE, Interprofessional simulation; IPPE, Introductory pharmacy practice experience; MBS, Manikin based simulators; OSCE, Objective Structured Clinical Examination; RP, Role-play; SBE, Simulation-based education; SP, Standardized patient; SG, Serious Gaming; SOAP, Subjective, Objective, Assessment, Plan; SWOC, Strengths, Weaknesses, Opportunities, Challenges.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Wolters M, van Paassen JG, Minjon L, Hempenius M, Blokzijl MR, Blom L. Design of a Pharmacy Curriculum on Patient Centered Communication Skills. Pharmacy. 2021;9(1):22. doi:10.3390/pharmacy9010022
2. Seybert AL. Patient Simulation in Pharmacy Education. Am J Pharm Educ. 2011;75(9):187. doi:10.5688/ajpe759187
3. Meng X, Yang L, Sun H, Du X, Yang B, Guo H. Using a novel student-centered teaching method to improve pharmacy student learning. Am J Pharm Educ. 2019;83(2):6505. doi:10.5688/ajpe6505
4. Mesquita AR, Souza WM, Boaventura TC, et al. The effect of active learning methodologies on the teaching of pharmaceutical care in a Brazilian pharmacy faculty. PLoS One. 2015;10(5):e0123141. doi:10.1371/journal.pone.0123141
5. Bradley P. The history of simulation in medical education and possible future directions. Med Edu. 2006;40(3):254–262. doi:10.1111/j.1365-2929.2006.02394.x
6. Lin K, Travlos D, Wadelin JW, Vlasses PH. Simulation and Introductory Pharmacy Practice Experiences. Am J Pharm Educ. 2011;75(10):209. doi:10.5688/ajpe7510209
7. Lopreiato JOH. Healthcare Simulation Dictionary. Vol. 16. Rockville, MD:: Agency for Healthcare Research and Quality; 2016. doi:10.23970/simulationv2
8. So HY, Chen PP, Wong GKC, Chan TTN. Simulation in medical education. J Royal Coll Phys Edinburgh. 2019;49(1):52–57. doi:10.4997/JRCPE.2019.112
9. Robinson JD, Bray BS, Willson MN, Weeks DL. Using Human Patient Simulation to Prepare Student Pharmacists to Manage Medical Emergencies in an Ambulatory Setting. Am J Pharm Educ. 2011;75(1):3. doi:10.5688/ajpe7513
10. Gaba DM. The future vision of simulation in health care. Qual Saf Health Care. 2004;13(SUPPL. 1):i2–i10. doi:10.1136/qshc.2004.009878
11. Seybert AL, Smithburger PL, Benedict NJ, Kobulinsky LR, Kane-Gill SL, Coons JC. Evidence for simulation in pharmacy education. J Am Coll Clin Pharmacy. 2019;2(6):686–692. doi:10.1002/jac5.1167
12. Ferguson J, Astbury J, Willis S, Silverthorne J, Schafheutle E. Implementing, embedding and sustaining simulation-based education: what helps, what hinders. Med Edu. 2020;54(10):915–924. doi:10.1111/medu.14182
13. Rosen KR. The history of medical simulation. J Crit Care. 2008;23(2):157–166. doi:10.1016/j.jcrc.2007.12.004
14. Wallace P. Following the threads of an innovation: the history of standardized patients in medical education. Caduceus. 1997;13(2):5–28.
15. Seybert AL, Kobulinsky LR, McKaveney TP. Human Patient Simulation in a Pharmacotherapy Course. Am J Pharm Educ. 2008;72(2):37. doi:10.5688/aj720237
16. Accredetation Council for Pharmacy Education. Accreditation standards and key elements for the professional program in pharmacy leading to the doctor of pharmacy; 2015. Available from: https://www.acpe-accredit.org/pdf/Standards2016FINAL.pdf.
17. Accredition Coucil for Pharmacy Education. Policies and Procedures for ACPE Accreditation of Professional Degree Programs; 2020. Available from: https://www.acpe-accredit.org/pdf/CS_PoliciesandProcedures.pdf.
18. Seybert AL, Smithburger PL, Kobulinsky LR, Kane-Gill SL. Simulation-based learning versus problem-based learning in an acute care pharmacotherapy course. Simulation Healthcare. 2012;7(3):162–165. doi:10.1097/SIH.0b013e31825159e3
19. Korayem GB, Alboghdadly AM. Integrating simulation into advanced pharmacy practice experience curriculum: an innovative approach to training. Saudi Pharmaceutical J. 2020;28(7):837–843. doi:10.1016/j.jsps.2020.06.004
20. Marken PA, Zimmerman C, Kennedy C, Schremmer R. Human simulators and standardized patients to teach difficult conversations to interprofessional health care teams; 2010. Available from: http://www.ajpe.org.
21. Vyas D, Wombwell E, Russell E, Caligiuri F. High-Fidelity Patient Simulation Series to Supplement Introductory Pharmacy Practice Experiences. Am J Pharm Educ. 2010;74(9):169. doi:10.5688/aj7409169
22. Fernandez R, Parker D, Kalus JS, Miller D, Compton S. Using a Human Patient Simulation Mannequin to Teach Interdisciplinary Team Skills to Pharmacy Students. Am J Pharm Educ. 2007;71(3):51. doi:10.5688/aj710351
23. Khalil R, Mansour AE, Fadda WA, et al. The sudden transition to synchronized online learning during the COVID-19 pandemic in Saudi Arabia: a qualitative study exploring medical students’ perspectives. BMC Med Educ. 2020;20(1):285. doi:10.1186/s12909-020-02208-z
24. Badreldin HA, Alshaya O. Restructuring the inpatient advanced pharmacy practice experience to reduce the risk of contracting coronavirus disease 2019: lessons from Saudi Arabia. J Am Coll Clin Pharmacy. 2020;3(4):771–777. doi:10.1002/jac5.1237
25. Sara A, David E. The Use of Simulation in Health-Care Response to COVID-19. Saudi Critical Care J. 2020;4(5):28–30.
26. Beck DE. Performance-Based Assessment: using Pre-Established Criteria and Continuous Feedback to Enhance a Student’s Ability to Perform Practice Tasks. J Pharm Pract. 2000;13(5):347–364. doi:10.1106/LGR5-3C3N-NTEG-B9VH
27. Gillette C, Rudolph M, Rockich-Winston N, Stanton R, Anderson HG. Improving Pharmacy Student Communication Outcomes Using Standardized Patients. Am J Pharm Educ. 2017;81(6):548. doi:10.5688/ajpe816110
28. Sales I, Jonkman L, Connor S, Hall D. A Comparison of Educational Interventions to Enhance Cultural Competency in Pharmacy Students. Am J Pharm Educ. 2013;77(4):76. doi:10.5688/ajpe77476
29. Cobb BT, Bowen JF, Pontiggia L, Koffer KF, Scholtz JM. Evaluation of an individualized vs non-specific standardized patient activity in improving communication skills amongst pharmacy students. Curr Pharm Teach Learn. 2019;11(6):603–608. doi:10.1016/j.cptl.2019.02.022
30. Serag-Bolos ES, Chudow M, Perkins J, Patel R. Enhancing Student Knowledge Through a Comprehensive Oncology Simulation. Am J Pharm Educ. 2018;82(3):6245. doi:10.5688/ajpe6245
31. Ledbetter E, Lau S, Enterline A, Sibbitt B, Chen AMH. A Simulation Activity to Assess Student Pharmacists’ Knowledge and Perceptions of Oncology Pharmacy. Am J Pharm Educ. 2020;84(5):7474. doi:10.5688/ajpe7474
32. Patel R, Chudow M, Vo TT, Serag-Bolos ES. Evaluation of pharmacy students’ knowledge and perceptions of pharmacogenetics before and after a simulation activity. Curr Pharm Teach Learn. 2018;10(1):96–101. doi:10.1016/j.cptl.2017.09.012
33. Vyas D, Galal SM, Rogan EL, Boyce EG. Training Students to Address Vaccine Hesitancy and/or Refusal. Am J Pharm Educ. 2018;82(8):6338. doi:10.5688/ajpe6338
34. Smithson J, Bellingan M, Glass B, Mills J. Standardized patients in pharmacy education: an integrative literature review. Curr Pharm Teach Learn. 2015;7(6):851–863. doi:10.1016/j.cptl.2015.08.002
35. Cobb P, Bowers J. Cognitive and Situated Learning Perspectives in Theory and Practice. Educ Res. 1999;28(2):4–15. doi:10.3102/0013189X028002004
36. Sibbald D. Using first-year students as standardized patients for an objective structured clinical exam for third-year pharmacy students. Am J Pharmaceutical Educ. 2001;64(4):404.
37. University of Hong Kong. Assessment: role play, Assessment Resource Centre. Available from: https://ar.cetl.hku.hk/am_rp.htm.
38. STATPEARLS. Types of standardized patients and recruitment in medical simulation. Available from: https://www.statpearls.com/ArticleLibrary/viewarticle/63906.
39. Rao D. Skills Development Using Role-Play in a First-Year Pharmacy Practice Course. Am J Pharm Educ. 2011;75(5):84. doi:10.5688/ajpe75584
40. Kiersma ME, Darbishire PL, Plake KS, Oswald C, Walters BM. Laboratory Session to Improve First-year Pharmacy Students’ Knowledge and Confidence Concerning the Prevention of Medication Errors. Am J Pharm Educ. 2009;73(6):99. doi:10.5688/aj730699
41. Rogers ER, King SR. The Influence of a Patient-Counseling Course on the Communication Apprehension, Outcome Expectations, and Self-Efficacy of First-Year Pharmacy Students. Am J Pharm Educ. 2012;76(8):152. doi:10.5688/ajpe768152
42. Luiz Adrian JA, Zeszotarski P, Ma C. Developing Pharmacy Student Communication Skills through Role-Playing and Active Learning. Am J Pharm Educ. 2015;79(3):44. doi:10.5688/ajpe79344
43. Buring SM, Kirby J, Conrad WF, Structured A. Approach for Teaching Students to Counsel Self-care Patients. Am J Pharm Educ. 2007;71(1):08. doi:10.5688/aj710108
44. Lupu AM, Stewart AL, O’Neil C. Comparison of Active-Learning Strategies for Motivational Interviewing Skills, Knowledge, and Confidence in First-Year Pharmacy Students. Am J Pharm Educ. 2012;76(2):28. doi:10.5688/ajpe76228
45. Bond R, Donohoe KL, Jakeman B, Davis HT, Morgan L. Combining rhetoric and role-play to introduce and develop patient presentation skills in third year pharmacy students. Curr Pharm Teach Learn. 2017;9(6):1164–1169. doi:10.1016/j.cptl.2017.07.029
46. Bajis D, Chaar B, Basheti IA, Moles R. Pharmacy students’ medication history taking competency: simulation and feedback learning intervention. Curr Pharm Teach Learn. 2019;11(10):1002–1015. doi:10.1016/j.cptl.2019.06.007
47. Jin HK, Park SH, Kang JE, et al. The influence of a patient counseling training session on pharmacy students’ self-perceived communication skills, confidence levels, and attitudes about communication skills training. BMC Med Educ. 2019;19(1). doi:10.1186/s12909-019-1607-x
48. Jacob SA, Larter J, Blair A, Boyter AC. Using forum theatre to teach communication skills within an undergraduate pharmacy curriculum: a qualitative evaluation of students’ feedback. Curr Pharm Teach Learn. 2019;11(4):373–381. doi:10.1016/j.cptl.2019.01.015
49. Datta R, Upadhyay KK, Jaideep CN. Simulation and its role in medical education. Med J Armed Forces India. 2012;68(2):167–172. doi:10.1016/S0377-1237(12
50. Patel R, Butler K, Garrett D, Badger N, Cheoun D, Hallman L. The Impact of a Pharmacist’s Participation on Hospitalists’ Rounds. Hosp Pharm. 2010;45(2):129–134. doi:10.1310/hpj4502-129
51. Lee Chin K, Ling Yap Y, Leng Lee W, Chang Soh Y. Comparing Effectiveness of High-Fidelity Human Patient Simulation vs Case-Based Learning in Pharmacy Education. Am J Pharm Educ. 2014;78(8):153. doi:10.5688/ajpe788153
52. Seybert AL, Barton CM. Simulation-Based Learning to Teach Blood Pressure Assessment to Doctor of Pharmacy Students. Am J Pharm Educ. 2007;71(3):48. doi:10.5688/aj710348
53. Grice GR, Wenger P, Brooks N, Berry TM. Comparison of Patient Simulation Methods Used in a Physical Assessment Course. American Journal of Pharmaceutical Education. 2013;77(4):77. doi:10.5688/ajpe77477
54. Bushell M, Frost J, Deeks L, Kosari S, Hussain Z, Naunton M. Evaluation of Vaccination Training in Pharmacy Curriculum: preparing Students for Workforce Needs. Pharmacy. 2020;8(3):151. doi:10.3390/pharmacy8030151
55. Curtin LB, Finn LA, Czosnowski QA, Whitman CB, Cawley MJ. Computer-based Simulation Training to Improve Learning Outcomes in Mannequin-based Simulation Exercises. Am J Pharm Educ. 2011;75(6):113. doi:10.5688/ajpe756113
56. Nicholas H, Lyn H, Marjorie W, Denise T. The use of a high-fidelity simulation manikin in teaching clinical skills to fourth year undergraduate pharmacy students. Pharmacy Educ. 2013;13(1):54–60.
57. Bernaitis N, Baumann-Birkbeck L, Alcorn S, Powell M, Arora D, Anoopkumar-Dukie S. Simulated patient cases using DecisionSimTM improves student performance and satisfaction in pharmacotherapeutics education. Curr Pharm Teach Learn. 2018;10(6):730–735. doi:10.1016/j.cptl.2018.03.020
58. Cavaco AM, Madeira F. European Pharmacy Students’ Experience With Virtual Patient Technology. Am J Pharm Educ. 2012;76(6):106. doi:10.5688/ajpe766106
59. Salem S, Cooper J, Schneider J, Croft H, Munro I. Student Acceptance of Using Augmented Reality Applications for Learning in Pharmacy: a Pilot Study. Pharmacy. 2020;8(3):122. doi:10.3390/pharmacy8030122
60. Schneider J, Patfield M, Croft H, Salem S, Munro I. Introducing Augmented Reality Technology to Enhance Learning in Pharmacy Education: a Pilot Study. Pharmacy. 2020;8(3):109. doi:10.3390/pharmacy8030109
61. Coyne L, Merritt TA, Parmentier BL, Sharpton RA, Takemoto JK. The Past, Present, and Future of Virtual Reality in Pharmacy Education. Am J Pharm Educ. 2019;83(3):7456. doi:10.5688/ajpe7456
62. Ezeala CC, Ram AA, Vulakouvaki N. Learning gain of pharmacy students after introducing guided inquiry learning with computer simulation in a pharmacology class in Fiji. J Educ Eval Health Prof. 2012;10:9. doi:10.3352/jeehp.2013.10.9
63. McDowell J, Styles K, Sewell K, et al. A Simulated Learning Environment for Teaching Medicine Dispensing Skills. Am J Pharm Educ. 2016;80(1):11. doi:10.5688/ajpe80111
64. Shin J, Tabatabai D, Boscardin C, Ferrone M, Brock T. Integration of a Community Pharmacy Simulation Program into a Therapeutics Course. Am J Pharm Educ. 2018;82(1):6189. doi:10.5688/ajpe6189
65. Johnson AE, Barrack J, Fitzgerald JM, Sobieraj DM, Holle LM. Integration of a Virtual Dispensing Simulator “MyDispense” in an Experiential Education Program to Prepare Students for Community Introductory Pharmacy Practice Experience. Pharmacy. 2021;9((1):48):48. doi:10.3390/pharmacy9010048
66. Al-Dahir S, Bryant K, Kennedy KB, Robinson DS. Online Virtual-Patient Cases Versus Traditional Problem-Based Learning in Advanced Pharmacy Practice Experiences. Am J Pharm Educ. 2014;78(4):76. doi:10.5688/ajpe78476
67. Bindoff I, Ling T, Bereznicki L, et al. A Computer Simulation of Community Pharmacy Practice for Educational Use. Am J Pharm Educ. 2014;78(9):168. doi:10.5688/ajpe789168
68. Douglass MA, Casale JP, Skirvin JA, DiVall MV. A Virtual Patient Software Program to Improve Pharmacy Student Learning in a Comprehensive Disease Management Course. Am J Pharm Educ. 2013;77(8):172. doi:10.5688/ajpe778172
69. Pilote B, Chiniara G. The Many Faces of Simulation. Elsevier; 2019; doi:10.1016/B978-0-12-815657-5.00002-4
70. Cain J, Conway JM, DiVall MV. Report of the 2013-2014 Academic Affairs Committee. Am J Pharm Educ. 2014;78(10):S23. doi:10.5688/ajpe7810S23
71. Sando KR, Elliott J, Stanton ML, Doty R. An Educational Tool for Teaching Medication History Taking to Pharmacy Students. Am J Pharm Educ. 2013;77(5):105. doi:10.5688/ajpe775105
72. Abraham O, Tidd M, Buechel M, Thakur T, Brown R. Student Pharmacists’ Assessment of a Serious Game on Opioid Medication Safety. Inov Pharm. 2020;11(4):19. doi:10.24926/iip.v11i4.2937
73. Korenoski AS, Ginn TR, Seybert AL. Use of an immersive, simulated learning game to teach pharmacy students clinical concepts of toxicology. Curr Pharm Teach Learn. 2021;13(5):556–559. doi:10.1016/j.cptl.2021.01.018
74. Caldas LM, Eukel HN, Matulewicz AT, Fernández EV, Donohoe KL. Applying educational gaming success to a nonsterile compounding escape room. Curr Pharm Teach Learn. 2019;11(10):1049–1054. doi:10.1016/j.cptl.2019.06.012
75. Eukel HN, Frenzel JE, Cernusca D. Educational Gaming for Pharmacy Students – design and Evaluation of a Diabetes-themed Escape Room. Am J Pharm Educ. 2017;81(7):6265. doi:10.5688/ajpe8176265
76. Baker CM, Crabtree G, Anderson K. Student pharmacist perceptions of learning after strengths-based leadership skills lab and escape room in pharmacy practice skills laboratory. Curr Pharm Teach Learn. 2020;12(6):724–727. doi:10.1016/j.cptl.2020.01.021
77. Clauson A, Hahn L, Frame T, et al. An innovative escape room activity to assess student readiness for advanced pharmacy practice experiences (APPEs). Curr Pharm Teach Learn. 2019;11(7):723–728. doi:10.1016/j.cptl.2019.03.011
78. Wilby KJ, Kremer LJ. Development of a cancer-themed escape room learning activity for undergraduate pharmacy students. Int J Pharmacy Practice. 2020;28(5):541–543. doi:10.1111/ijpp.12622
79. Nybo SE, Klepser SA, Klepser M. Design of a disaster preparedness escape room for first and second-year pharmacy students. Curr Pharm Teach Learn. 2020;12(6):716–723. doi:10.1016/j.cptl.2020.01.037
80. Plakogiannis R, Stefanidis A, Hernandez N, Nogid A. A heart failure themed escape room approach to enhance pharmacy student learning. Curr Pharm Teach Learn. 2020;12(8):940–944. doi:10.1016/j.cptl.2020.04.014
81. Kavanaugh R, George S, Lamberton N, Frenzel JE, Cernusca D, Eukel HN. Transferability of a diabetes escape room into an accelerated pharmacy program. Curr Pharm Teach Learn. 2020;12(6):709–715. doi:10.1016/j.cptl.2020.01.022
82. Badr AF. The Geriatric Virtual Escape Room in Pharmacy Education: female Students Escape Significantly Faster than Male Students. Pharmacy. 2022;10(2):36. doi:10.3390/pharmacy10020036
83. Cain J, Piascik P. Are Serious Games a Good Strategy for Pharmacy Education? Am J Pharm Educ. 2015;79(4):47. doi:10.5688/ajpe79447
84. Tofil NM, Benner KW, Worthington MA, Zinkan L, Lee White M. Use of Simulation to Enhance Learning in a Pediatric Elective. Am J Pharm Educ. 2010;74(2):21. doi:10.5688/aj740221
85. Smithburger PL, Kane-Gill SL, Kloet MA, Lohr B, Seybert AL. Advancing interprofessional education through the use of high fidelity human patient simulators. Pharmacy Practice. 2013;11(2):61–65. doi:10.4321/S1886-36552013000200001
86. Kane-Gill SL, Smithburger PL PATIENT SIMULATION transitioning knowledge gained from simulation to pharmacy practice; 2011. Available from: http://www.ajpe.org.
87. Bolesta S, Chmil J. Interprofessional Education Among Student Health Professionals Using Human Patient Simulation. Am J Pharm Educ. 2014;78(5):94. doi:10.5688/ajpe78594
88. Hodgkins SR, Marian KM, Shrader S, et al. A case of anaphylaxis: IPE simulation as a tool to enhance communication and collaboration. J Interprofessional Educ Practice. 2020;18:100303. doi:10.1016/j.xjep.2019.100303
89. Clinard VB, Kearney TE, Repplinger DJ, Smollin CG, Youmans SL. An interprofessional clinical toxicology advanced pharmacy practice experience. Curr Pharm Teach Learn. 2019;11(5):505–512. doi:10.1016/j.cptl.2019.02.002
90. Pillow MT, Hatfield CL, Aulbach R, et al. Using a Resuscitation-Based Simulation Activity to Create an Interprofessional Education Activity for Medical, Nursing, and Pharmacy Students. MedEdPORTAL. 2020;16(1). doi:10.15766/mep_2374-8265.11054
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Characteristics of Critical Care Pharmacy Services in Saudi Arabia
Ismail NH, Alhammad AM, Alshaya AI, Alkhani N, Alenazi AO, Aljuhani O
Journal of Multidisciplinary Healthcare 2023, 16:3227-3234
Published Date: 1 November 2023