")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Characteristics of Critical Care Pharmacy Services in Saudi Arabia
Authors Ismail NH , Alhammad AM , Alshaya AI , Alkhani N, Alenazi AO, Aljuhani O
Received 6 August 2023
Accepted for publication 24 October 2023
Published 1 November 2023 Volume 2023:16 Pages 3227—3234
DOI https://doi.org/10.2147/JMDH.S434116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nadia H Ismail,1,2,* Abdullah M Alhammad,3,* Abdulrahman I Alshaya,4– 6 Nada Alkhani,7 Ahmed O Alenazi,6,8 Ohoud Aljuhani9
1Department of Clinical Pharmacy Research, Institute for Research and Medical Consultations, Imam Abdulrahman Bin Faisal University (IAU), Dammam, Saudi Arabia; 2King Fahd Hospital of the University, Alkhobar, Saudi Arabia; 3Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 4Pharmaceutical Care Department, King Abdulaziz Medical City, Riyadh, Saudi Arabia; 5College of Pharmacy, King Saud Bin Abdulaziz University of Health Sciences, Riyadh, Saudi Arabia; 6King Abdullah International Medical Research Center-King Saud Bin Abdulaziz University for Health Sciences, Ministry of National Guard – Health Affairs, Riyadh, Saudi Arabia; 7Pharmacy Services Administration, King Fahad Medical City, Riyadh, Saudi Arabia; 8King Abdulaziz Medical City, National Guard Health Affairs, Pharmaceutical Care Department, Dammam, Saudi Arabia; 9Pharmacy Practice Department, Faculty of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Abdullah M Alhammad, Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia, Tel +996 114677486, Email [email protected]
Purpose: Critical care pharmacists (CCPs) in intensive care units (ICUs) are associated with improved patient outcomes, reduced adverse events (ADEs), and reduced mortality rates. This study aimed to describe the activities and pharmacy services provided by CCP in ICUs in hospitals in Saudi Arabia (SA).
Methods: In this cross-sectional prospective study, a questionnaire was electronically sent to CCPs practicing in SA between September 2022 and January 2023. A modified version of a previously published and validated survey was sent to the Saudi Critical Care and Emergency Specialty Network. The questionnaire focused on four CCP activities: clinical, educational, scholarly, and administrative. The level of services was similarly classified into three domains: fundamental, optimal, and desirable. The responses were analyzed using descriptive statistics.
Results: The study surveyed 44 CCPs in SA, with a response rate of 52.3%. These CCPs were predominantly located in the central (47.8%) and eastern (30.4%) regions. Hospitals’ ICU bed capacity ranged from 10 to 100, with 82% reporting mixed medical and surgical ICUs. Most CCPs had 4– 10 years of critical care experience, and 60% held advanced degrees, with a substantial portion having completed PGY-1 and PGY-2 pharmacy residencies. CCPs were actively involved in patient care, with 86.9% participating in multidisciplinary rounds five days a week. They were engaged in clinical, educational, and administrative activities, with 82.6% involved in retrospective research and educational activities. Furthermore, 78.2% were engaged in pharmacy and therapeutic committees, 56.5% in critical care committees, and 56.5% in pharmacy department policy development.
Conclusion: The study reveals that CCPs in SA play integral roles in ICU patient care and contribute significantly to clinical, educational, and administrative activities. The study highlights the need for standardized CCP-to-patient ratios and further support for CCPs to expand their services, thus contributing to enhanced healthcare quality.
Keywords: critical care, Saudi Arabia, education, pharmacy, research, pharmacy practice
Introduction
Critical care pharmacy services cater to a unique patient population that is prescribed numerous specialized procedures and a complex variety of treatment modalities. Critical care pharmacists (CCPs), with their advanced training in pharmacology, drug pharmacokinetics, and pharmacodynamics, have contributed to preventing adverse events, reducing prescription errors, decreasing drug-related costs, and reducing intensive care unit (ICU) length of stay and mortality. CCPs assist clinicians and physicians in pharmacotherapy decision-making, contributing to optimizing patient outcomes.1–4
In Saudi Arabia (SA), critical care pharmacy services were established in the early 2000s by pharmacists who obtained a Doctor of Pharmacy degree and residency training from universities in the United States of America (USA). Additionally, in 2010, more CCPs gained postgraduate training and education by completing specialized residencies or masters in clinical pharmacy.5–7 These pharmacists were the pioneers who established critical care pharmacy services and postgraduate training programs in SA. CCPs in SA have contributed to adverse event prevention and cost reduction in critically ill patients.8–10 Since 2019, CCPs in SA have contributed to delivering critical care pharmacy services during the Hajj Pilgrimage.10
Critical care pharmacy services are well-established in SA. However, the current level and status of critical care pharmacy services and CCP activities in the SA are not well-described in the literature.5 Only one survey that was carried out in the Western region of SA demonstrated that only 43% of responding hospitals had CCP as a member of the ICU team, and more than half of responding hospitals (54%) had CCP services with at least one dedicated pharmacist at the bedside and during medical rounds.11 Internationally, a 2004 survey of CCP conducted in 382 US institutions encompassing 1034 ICUs found that 62.2% of ICUs provided direct patient care, with a focus on clinical and administrative duties and varying involvement in education and scholarship. A 2020 follow-up survey of 493 ICUs indicated that 70.8% of ICUs offered direct clinical pharmacy services, with key tasks including drug history review, adverse event assessment, and drug therapy management, alongside educational services, such as in-services and training for students and residents.12,13
Describing the current level and scope of pharmacy services at SA hospitals is crucial for future projection and development. The purpose of this survey was to describe the pharmacy services and CCPs’ activities provided in the ICUs of SA hospitals.
Materials and Methods
Study Design
This cross-sectional study surveyed CCPs practicing in SA. The survey questions were adapted and formulated based on a previously published survey.12 We slightly modified the options for a few questions to reflect the updates in the field. We used the 2000 Society of Critical Care Medicine and American College of Clinical Pharmacy recommendations (SCCM/ACCP).14 Survey questions were designed using QuestionPro. All the survey questions were reviewed and approved by a panel of six CCP board members from the Critical Care and Emergency Medicine Pharmacy Specialty Network of the Saudi Society of Clinical Pharmacy. The survey was divided into two sections. For section one, the survey questions were designed to categorize responses according to practice site demographics and ICU characteristics (seven questions). Section two of the survey was designed to collect information regarding critical care pharmacy services and CCP activities across practices such as clinical, educational, scholarship, and administration (15 questions). All survey questions were closed-ended questions with predefined options except for one question related to the estimation of the percentage of time per week devoted to different activities. The survey questions were categorized to define CCP activities or services. For example, CCPs were adjudged to have provided fundamental services if the pharmacist prospectively evaluated all drug therapies for appropriateness, effectiveness, and safety. Optimal services were adjudged if CCPs developed residency and fellowship training programs. Desirable services were adjudged if CCPs were to attend regular rounds with a multidisciplinary team. Direct patient care was defined as providing full-time CCP with little to no commitment to non-critically ill patients. The research team nominated three CCPs to participate in the survey pilot to ensure clarity and presentation of the survey questions.
Data Collection
The electronic questionnaire assured confidentiality and consent was implied upon completion of the survey. A link to the electronic survey was sent to members and non-members of the Critical Care and Emergency Medicine Pharmacy Speciality Network, and participants were only authorized to complete the survey once for inclusion in the study. Periodic reminders were sent monthly to CCPs through a group list to complete the survey. The survey was conducted from September 2022 to January 2023, and the final survey responses were collected on January 10, 2023.
Statistical Analysis
Frequencies and percentages were used to describe the categorical variables. Means and standard deviations, or median and interquartile range (IQR), were used to describe continuous variables. Analyses were performed with the level of significance set at p < 0.05. The data were analyzed by SPSS version 20.0 (SPSS Inc., Chicago, US).
Results
The electronic survey link was received by 44 CCPs, of which 23 (52.3%) completed the survey.
Practice Site Information
CCPs who participated in this survey were mostly from the central and eastern regions of the Kingdom (47.8% and 30.4%, respectively). CCPs mainly worked in Ministry of Health hospitals (MOH), academic medical centers, and military hospitals (34.7%, 30.4%, and 26.1%, respectively). The total number of beds devoted to ICUs in all hospitals ranged from 10–100. The complete practice information is presented in Table 1. Concerning the type of ICU available at each institution, most respondents (82%) indicated mixed medical and surgical ICUs. Table 2 describes the medication-use systems available to pharmacists caring for critically ill patients.
 |
Table 1 Practice Site Information |
 |
Table 2 Types of Medication Use Systems Available to Pharmacists Caring for Critically Ill Patients |
Critical Care Pharmacist Experience, Education, and Training
Most CCPs (47.8%) had 4–10 years of experience in critical care practice. Regarding education, 43% held a master’s degree in clinical pharmacy, 39% held a Doctor of Pharmacy degree, 17% held a Bachelor of Pharmacy degree, and 52% held other degrees. Regarding postgraduate training, most of the surveyed CCPs had undergone PGY-1 and PGY-2 pharmacy residency. (60%), while the remaining had critical care fellowships (13%).
Clinical Activities
Most surveyed CCPs indicated that 86.9% of their time was dedicated to caring for critically ill patients. Nearly all respondents (95%) indicated that they had prospectively evaluated all drug therapies for appropriateness. A typical CCP workweek included providing direct patient care (71.7%), teaching and education (38.9%), administration and management (28.6%), non-direct ICU patient care (21.6%), scholarly activities (21.5%), and drug distribution (21.2%). Nearly all CCPs provided direct patient care, defined as dedicating one or two CCPs to critically ill patients. In addition, 86.9% of the respondents indicated that they were involved in identifying and managing adverse drug events. Most of the surveyed pharmacists (86.9%) also indicated attending multidisciplinary rounds 5 days per week. Most pharmacists (82%) were actively involved in documenting clinical activities (eg, disease management, therapeutic monitoring, and adverse drug events). Most respondents (91.3%) indicated they were actively involved in liaisons between pharmacy, nursing, and medical staff to educate healthcare professionals on current drug-related policies, guidelines, and clinical pathways. More details about the clinical activities are listed in Table 3.
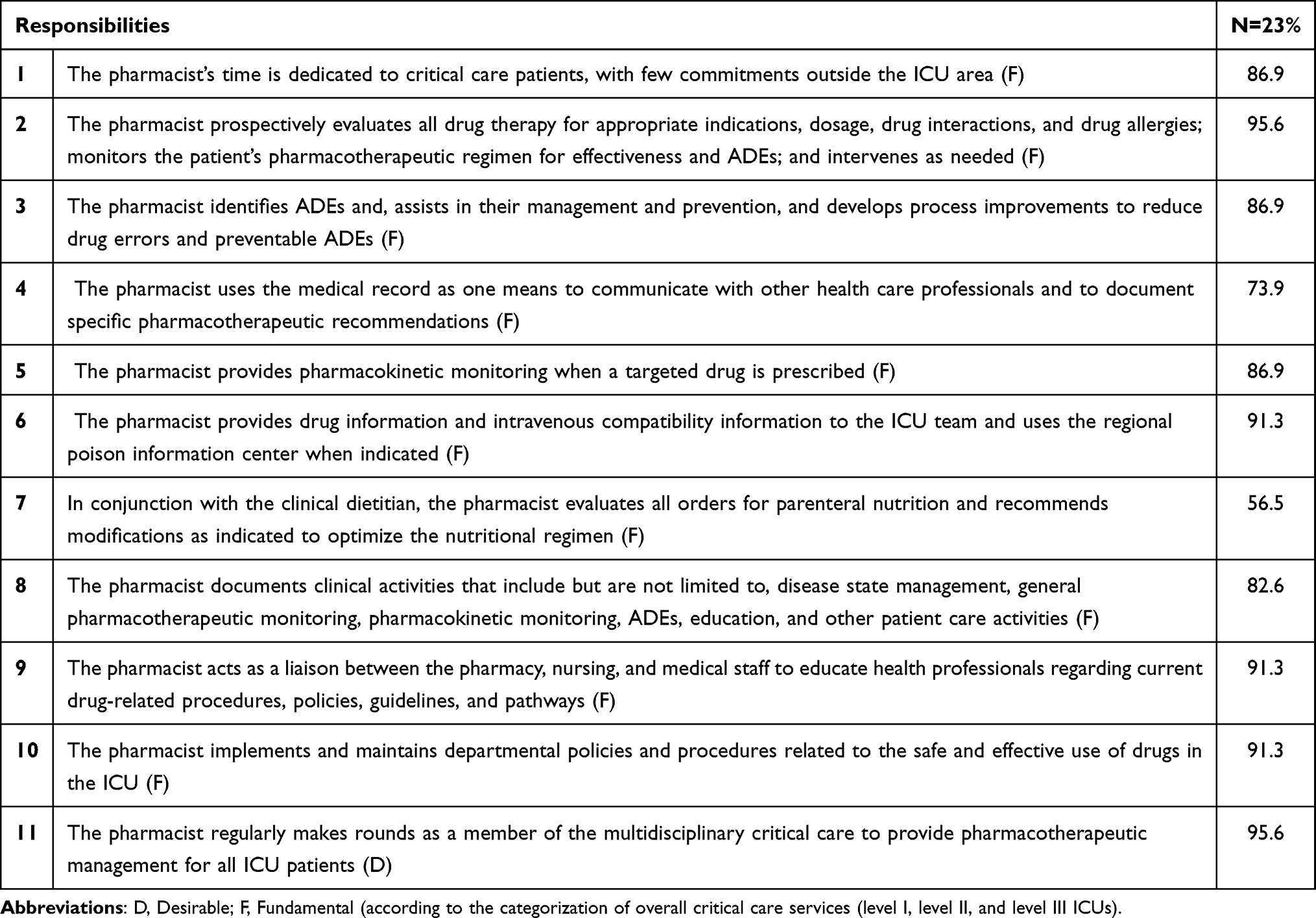 |
Table 3 Types of Clinical Activities Performed by Critical Care Pharmacists |
Scholarly and Educational Activities
When CCPs were asked about their involvement in research, most (82.6%) were involved in retrospective research. When CCPs were asked about their involvement in educational activities, most (82.6%) indicated that they had provided informal instructions to pharmacists and other ICU healthcare professionals.
Administrative Activities
When CCPs were asked about their involvement in systems and processes that contributed to the improved care of critically ill patients, over 78.2% stated that they were involved in pharmacy and therapeutic committees, critical care committees (56.5%), and pharmacy department policy development (56.5%).
Discussion
This is the first nationwide study to outline the activities and services that CCPs provide to ICUs in SA. We found that most CCPs devoted their time to critically ill patients, with little commitment outside the intensive care area. Nearly all CCPs provided direct patient care, defined as having 1–2 CCPs per critically ill patient. Additionally, our study highlights that CCPs in SA are actively involved in services beyond direct patient care, such as education, training, and administrative activities. Regarding our study findings about CCPs’ provision of direct patient care, our results are comparable to those reported by Maclaren et al13 who showed that more than 70% of CCPs in ICUs in the USA offered direct patient care.
However, we could not assess the CCP-to-patient ratio owing to the lack of national standards for an optimal CCP-to-patient ratio. Several international societies have suggested CCP-to-patient ratios ranging from a minimum of one pharmacist per 10 patients to a maximum of one pharmacist per 30 patients.15 It is worth noting that the impact of increased workload on CCPs raises concerns about optimizing critically ill patient safety.16
In addition to direct patient care, we reported that a typical workweek for CCPs in SA involves other activities. Among them, involvement in teaching and education was the highest, followed by administrative and management tasks and other non-ICU patient care and drug distribution to a lesser extent. The absence of a national unified CCP performance evaluation matrix may increase heterogeneity in the time allocation for different activities among CCPs. These findings are similar to those reported by Maclaren et al13 who found that a typical workweek for CCPs consisted of 50% direct ICU patient care, 10% teaching, 8% order processing, 5% direct non-ICU patient care, and 5% scholarships.
Most CCPs in SA provide fundamental clinical pharmacy services and, to some extent, desirable and optimal clinical pharmacy services for critically ill patients. These findings are consistent with those reported by Aljuhani,11 who showed that most CCPs in the western region of SA mainly provided fundamental clinical services with little engagement in desirable and optimal clinical services. One of the reasons for the minimal involvement in optimal and desirable services might be related to the limited number of CCPs in SA. Thus, revising the optimal CCP-to-patient ratio, increasing residency-training sites, and unifying the performance evaluation of critical care pharmacy services and CCP activities that affect patient clinical outcomes are key factors in improving CCP service provision in SA.
Additionally, we found that most CCPs were heavily involved in research. These findings are consistent with those reported by Maclaren et al12 who observed that more than half of critical care pharmacists were engaged in all research activities, such as retrospective design, data collection and analysis, and abstract and article writing. This study’s survey questions were not tailored to report whether CCPs in SA were leading multidisciplinary research or co-investigators. In addition, we could not report the percentage of CCPs who participated in or led randomized control trials in SA.
Not surprisingly, all the CCPs surveyed were board-certified in critical care. The number of board-certified CCPs in SA has risen from 18 in 2018 to 55 in 2023.17 Compared to other countries in the Middle East, these numbers signify the dedication and commitment of CCPs working in SA and highlight their ability to attain higher qualifications to sustain their competencies in caring for critically ill patients.5
Advanced degrees and postgraduate residency training attained by CCPs in SA qualify them for direct patient care because they possess advanced knowledge and expertise in critical care pharmacotherapy. These findings are similar to those reported by Maclaren et al13 who observed that advanced training of CCPs contributed to the expansion of direct patient care services in ICUs in the USA. It is worth mentioning that the official classification and registration of CCPs in SA does not account for an equivalent clinical experience to be classified as a consultant CCP, which is the main classification title for CCPs with a specialty residency according to the Saudi Commission for Health Specialties (SCFHS) licensing bylaws.
Implementing advanced technology, such as physician order entry systems, also improves CCPs’ ability to provide direct patient care. Less than half (43.4%) of Saudi CCPs indicated the availability of direct provider order entry into their ICUs, which also contributed to the ability of CCPs to allocate more time to direct patient care activities.
These findings are consistent with those reported by Maclaren et al13 who observed that the implementation of provider order entry systems in ICUs in the USA contributed largely to the ability of CCPs to provide more direct patient care in hospitals in the USA. Furthermore, in 2017, guidelines for medication safety in ICU were published, which included a recommendation to implement computerized provider order entry systems in ICUs as part of multiple strategies for preventing medication errors in critically ill patients.18
Although this was the first national survey aimed to delineate CCP services in SA, several limitations are notable The survey was exclusively distributed through the Critical Care and Emergency Medicine Pharmacy Specialty Network of the Saudi Society of Clinical Pharmacy, which might not encompass all CCPs, including those who are board-certified or graduates of residency programs. As a result, the respondents may not comprehensively represent all active CCPs and their practices in SA. Nevertheless, the response rate was 52.3%, and all participants represented various institutions and geographical regions in the SA. The approach of having one pharmacist per institution complete the survey could have restricted the number of CCP representatives participating in the study. Importantly, it should be noted that the survey did not stipulate a specific CCP within each institution to complete it; rather, invitations were extended to all CCPs, encouraging a broader perspective. Furthermore, it is possible that respondents were more inclined to participate when their pharmacy departments offered well-established clinical pharmacy services, potentially introducing response bias.
Future perspectives in the field of critical care pharmacy services in SA are promising. This national survey sets the stage for several key developments. First, standardizing CCP-to-patient ratios is essential for ensuring patient safety, with collaboration with international societies playing a vital role. Standardization of CCP performance evaluation can lead to a more balanced allocation of time among CCPs for various activities. Encouraging CCPs to engage in desirable and optimal clinical services, expanding involvement in research, and promoting the qualification and registration of experienced practitioners are vital for growth. Integrating advanced technologies is pivotal for enhancing direct patient care.
Conclusion
The study provides insights into the role and activities of Clinical Care Pharmacists (CCPs) in SA. The majority of CCPs in SA dedicate a significant portion of their time to providing direct patient care for critically ill patients, engage in educational activities, and actively participate in research. Many CCPs hold advanced degrees and have completed postgraduate training, which enhances their qualifications for patient care. However, there is a need for standardization in CCP-to-patient ratios and technology implementation to optimize their services. While CCPs primarily offer fundamental clinical pharmacy services, efforts to increase their numbers and standardize services could lead to the expansion of desirable and optimal clinical pharmacy services. The study highlights both the strengths and areas for improvement in the role of CCPs in SA, offering valuable insights for future research and healthcare practice.
Data Sharing Statement
The dataset supporting the conclusions of this article is available by request from the corresponding author.
Ethics Approval and Informed Consent
This research followed the relevant guidelines and regulations of the Helsinki Declaration. This study was approved by the Institutional Review Boards of Imam Abdulrahman bin Faisal University and King Fahad Hospital of the University (IRB-2021-11-280).
Acknowledgment
The authors thank the Researchers Supporting Project number (RSPD2023R919), King Saud University, Riyadh, Saudi Arabia, for their support.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, analysis, and interpretation of data and/or took part in drafting the article or revising it critically for important intellectual content. All authors agreed to submit it to the current journal, gave final approval to the version to be published, and agreed to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Preslaski CR, Lat I, MacLaren R, Poston J. Pharmacist contributions as members of the multidisciplinary ICU team. Chest. 2013;144(5):1687–1695. doi:10.1378/chest.12-1615
2. MacLaren R, Devlin JW. The bedside critical care pharmacist: a mandatory ICU team member essential for patient care. Crit Care Med. 2019;47(9):1276–1278. doi:10.1097/CCM.0000000000003888
3. Bauer SR, Kane-Gill SL. Outcome assessment of critical care pharmacist services. Hosp Pharm. 2016;51(7):507–513. doi:10.1310/hpj5107-507
4. Rech MA, Adams W, Smetana KS, et al. PHarmacist avoidance or reductions in medical costs in patients presenting the EMergency department: PHARM-EM study. Crit Care Explor. 2021;3(4):e0406. doi:10.1097/CCE.0000000000000406
5. Alshaya AI, Alhammad AM, Ismail N, et al. Critical care pharmacy in Saudi Arabia: historical evolution and future directions—a review by the critical care and emergency medicine pharmacy specialty network at the Saudi society of clinical pharmacy. J Am Coll Clin Pharm. 2021;4(11):1428–1437. doi:10.1002/jac5.1518
6. Alshaya A, Aljuhani O, Alghadeer S, et al. Critical care pharmacy program accreditation standards framework and core competencies in Saudi Arabia: an opinion paper by the SSCP critical care and emergency medicine pharmacy specialty network. Saudi J Clin Pharm. 2022;1(2):57. doi:10.4103/sjcp.SJCP_7_22
7. Badreldin HA, Alosaimy S, Al-jedai A. Clinical pharmacy practice in Saudi Arabia: historical evolution and future perspective. J Am Coll Clin Pharm. 2020;3(5):920–929. doi:10.1002/jac5.1239
8. Al-Jazairi AS, Al-Agil AA, Asiri YA, Al-Kholi TA, Akhras NS, Horanieh BK. The impact of clinical pharmacist in a cardiac-surgery intensive care unit. Saudi Med J. 2008;29(2):277–281.
9. Alomi YA, Almudaiheem HY. Clinical and economic outcomes of pharmacist intervention during therapeutic drug monitoring program in Saudi Arabia. Value Health. 2016;19(7):A465–A466. doi:10.1016/j.jval.2016.09.691
10. Al Sulaiman K, Aljuhani O, Al Harbi M, et al. Clinical pharmacist interventions in intensive care units during Hajj: a multicenter retrospective study. Saudi J Clin Pharm. 2022;1(4):134. doi:10.4103/sjcp.sjcp_18_22
11. Aljuhani O. Critical care pharmacy services in the Western Region of Saudi Arabia. Saudi Crit Care J. 2020;4(2):66. doi:10.4103/sccj.sccj_2_20
12. MacLaren R, Devlin JW, Martin SJ, Dasta JF, Rudis MI, Bond CA. Critical care pharmacy services in United States hospitals. Ann Pharmacother. 2006;40(4):612–618. doi:10.1345/aph.1G590
13. MacLaren R, Roberts RJ, Dzierba AL, Buckley M, Lat I, Lam SW. Characterizing critical care pharmacy services across the United States. Crit Care Explor. 2021;3(1):e0323. doi:10.1097/CCE.0000000000000323
14. Rudis MI, Brandl KM. Position paper on critical care pharmacy services. Society of critical care medicine and American college of clinical pharmacy task force on critical care pharmacy services. Crit Care Med. 2000;28(11):3746–3750. doi:10.1097/00003246-200011000-00037
15. Horn E, Jacobi J. The critical care clinical pharmacist: evolution of an essential team member. Crit Care Med. 2006;34(3):S46–S51. doi:10.1097/01.CCM.0000199990.68341.33
16. Newsome AS, Smith SE, Jones TW, Taylor A, Van Berkel MA, Rabinovich M. A survey of critical care pharmacists to patient ratios and practice characteristics in intensive care units. J Am Coll Clin Pharm. 2020;3(1):68–74. doi:10.1002/jac5.1163
17. Board of Pharmacy Specialties. Available from: https://www.bpsweb.org/find-a-board-certified-pharmacist.
18. Kane-Gill SL, Dasta JF, Buckley MS, et al. Executive summary: clinical practice guideline: safe medication use in the ICU. Crit Care Med. 2017;45(9):1546–1551. doi:10.1097/CCM.0000000000002519
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.