Back to Journals » Advances in Medical Education and Practice » Volume 17
Simulating the First Step: An Affordable ex vivo Tissue Model for Trocar Placement Training
Authors Sah Y ![]() , Garg A, Fisher B
, Garg A, Fisher B ![]() , Meshram P, Nigam A
, Meshram P, Nigam A ![]() , Onongaya C, Naaz R, Harmon JV Jr
, Onongaya C, Naaz R, Harmon JV Jr ![]()
Received 3 May 2026
Accepted for publication 3 July 2026
Published 10 July 2026 Volume 2026:17 621740
DOI https://doi.org/10.2147/AMEP.S621740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Yukti Sah, Anaya Garg, Benjamin Fisher, Pravin Meshram, Anmol Nigam, Chidiebere Onongaya, Rubeena Naaz, James V Harmon Jr
Department of Surgery, University of Minnesota, Minneapolis, MN, USA
*These authors contributed equally to this work
Correspondence: James V Harmon Jr, Department of Surgery, University of Minnesota, 420 Delaware Street SE, MMC 195, Minneapolis, MN, 55455, USA, Email [email protected]
Purpose: Trocar placement is a critical and potentially high-risk component of minimally invasive surgery. However, early hands-on training opportunities for surgical trainees are limited. Existing simulation models often lack realistic tactile fidelity or are constrained by cost and accessibility. We developed an affordable trocar placement training model using ex vivo animal tissue and assessed trainee perceptions of confidence, technical skills, and procedural risk awareness following its use.
Patients and Methods: Our tissue-based abdominal wall simulation model was evaluated during surgical skills acquisition workshops for medical students. To simulate abdominal wall tension, fresh porcine and ovine abdominal wall tissues were tightly stretched over a 5-gallon plastic container using elastic straps. After standardized didactic instruction, the participants placed multiple trocars using the simulation models. Model fidelity and educational efficacy were assessed using an anonymous, voluntary, 5-point Likert-scale survey. Procedural confidence, perceived realism, and educational value were also evaluated.
Results: According to the post-workshop survey analysis, 97% of the participants strongly agreed or agreed with the model’s educational value, and 93% reported that the simulation model improved their self-perceived confidence in performing laparoscopic entry. High levels of perceived realism were reported for tissue resistance (92%), abdominal wall layer simulation (85%), and tactile feedback (82%). Sixty-four percent of the participants reported feeling more prepared to recognize trocar- and Veress needle-related complications. The participants expressed strong support for curriculum integration; most indicated the model enhanced their anatomical understanding and had educational value.
Conclusion: Our ex vivo tissue-based trocar placement simulation model provided a realistic platform for elementary laparoscopic skill training. Following workshop participation, novice learners reported high confidence, perceived technical skill development, and awareness of procedural risks. Our model represents a simulation platform for hands-on surgical training that can help bridge the gap between theoretical knowledge and operative psychomotor skills.
Keywords: trocar placement, surgical simulation, medical education, minimally invasive surgery, ex vivo model, surgical training
Introduction
Laparoscopic and robotic approaches are standard contemporary surgical procedures that include cholecystectomies and appendectomies. Compared with open surgery, laparoscopic approaches are associated with reduced postoperative pain, shorter hospital stays, and faster recovery, contributing to their widespread adoption across surgical specialties.1 As minimally invasive surgery has expanded, proficiency in laparoscopic techniques has become a fundamental competency for modern surgeons. However, these procedures require distinct skills that are not emphasized in open surgery, such as visuospatial awareness, depth perception, and precise instrument handling under indirect visualization.2,3
Trocar placement is a critical and potentially high-risk step in laparoscopic and robotic surgeries because it establishes initial access to the abdominal cavity. Improper techniques during entry can result in serious complications, including bowel perforation, major vascular injury, and damage to intra-abdominal organs, as evidenced by a reported 37.9% incidence of laparoscopy-related bowel injuries caused by insertion of the primary trocar and 22% caused by the secondary trocar.4,5 Reported mortality rates for bowel and vascular injuries reach 2.5 to 5% and up to 15%, respectively. These rates emphasize the importance of safe and controlled entry techniques. However, structured opportunities to develop and practice these skills early in training remain limited because formal laparoscopic instruction is typically introduced during residency.6
Current training modalities, including synthetic simulators, cadaveric models, and low-fidelity task trainers, each have notable limitations: synthetic models lack realistic tissue feedback, cadaveric training is costly and logistically constrained, and existing low-cost trainers such as the Raj Model may not adequately replicate the physiological tissue resistance, tactile cues, and anatomical complexities of real procedures.7–10
Accessible, high-fidelity training tools that enable early learners to safely practice fundamental laparoscopic skills are therefore needed. To address this gap, we developed an affordable ex vivo tissue model for trocar placement. We hypothesized that the use of this model by medical student trainees during structured workshops would be educationally effective. The primary educational objectives assessed were perceived realism, learner confidence, and overall educational value, as measured by a post-workshop survey.
Materials and Methods
This educational evaluation was reviewed by the University of Minnesota IRB and granted exempt status (Study #00027053). Written informed consent was obtained from all participating trainees.
Model Construction
An affordable high-fidelity abdominal wall model was developed for trocar placement training using ex vivo animal tissue. Fresh abdominal wall specimens were procured from porcine and ovine animals used in prior approved animal research studies following euthanasia. These tissue types were selected because their structural properties are comparable to those of the human abdominal wall, including layered fascia and resistance to penetration, which make them highly suitable for simulating trocar insertion. Tissues were obtained at no additional cost; the unit cost listed in Table 1 reflects the estimated commercial replacement value for laboratories that would need to purchase tissues.
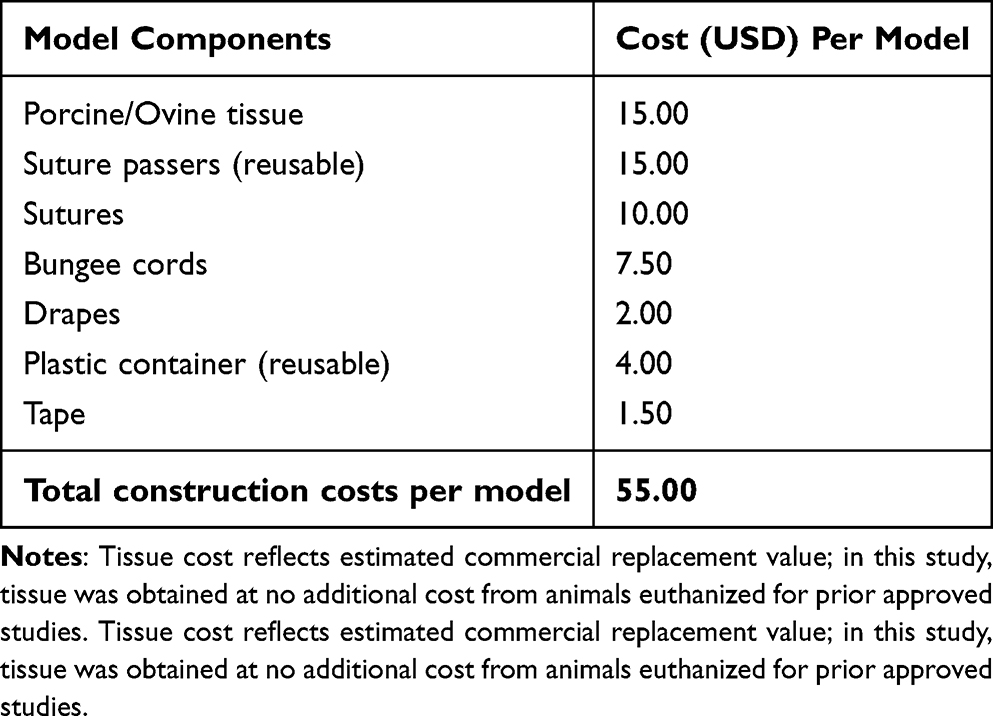 |
Table 1 Estimated Component Costs for Replicating the Trocar Simulation Model (per Unit, USD) |
The training models were constructed using standard 5-gallon plastic containers as foundational structures. Circular ports were created on the lateral aspects of each container to facilitate insertion of a laparoscopic camera and laparoscopic graspers. The abdominal wall tissue was tightly stretched using bungee cords positioned over the open top of the container to simulate the anterior abdomen.
To secure the tissue under physiological tension, small incisions were made along the peripheral edges of the specimen using a No. 11 surgical blade. Bungee cords with hook attachments were placed through these incisions and anchored to the container base, creating circumferential tension and maintaining a taut and stable surface. This step was critical for approximating the resistance encountered during real trocar placement (Figure 1).
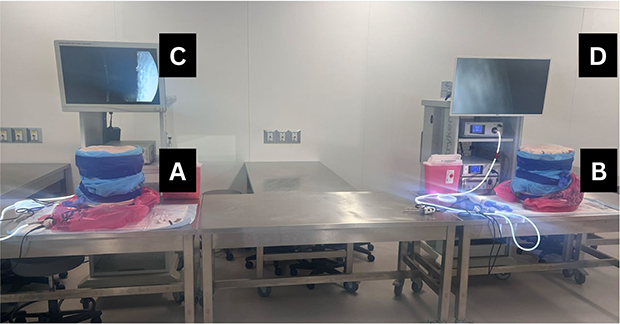 |
Figure 1 The completed abdominal wall simulation model. (A and B) Final assembled trocar placement simulation models, with porcine/ovine abdominal wall tissue stretched over a 5-gallon container and secured circumferentially with bungee cords. (C and D) Laparoscopic monitor display showing the intraperitoneal view through the model during trocar insertion. |
Workshop Design
Three medical student surgical skills workshops hosted from February through March of 2026 introduced medical trainees to laparoscopic entry techniques, with a specific focus on trocar placement. The workshop comprised a didactic demonstration, followed by supervised hands-on practice. The participants were provided with an educational handout that summarized the procedural steps and risks associated with trocar and Veress needle insertions (Figure 2). The faculty demonstrated the trocar placement technique, which emphasized the insertion angle, force control, and recognition of tissue layer transitions (Table 2). The participants performed hands-on practice using abdominal wall models and were given the opportunity to perform multiple trocar insertions under direct supervision, allowing for real-time feedback and iterative skill refinement (Figure 3). At the end, participants also used suture passers and performed laparoscopic guided closure of the abdominal wall fascia for the port sites. All the participants had repeated opportunities to practice the procedure in a controlled, low-risk environment.
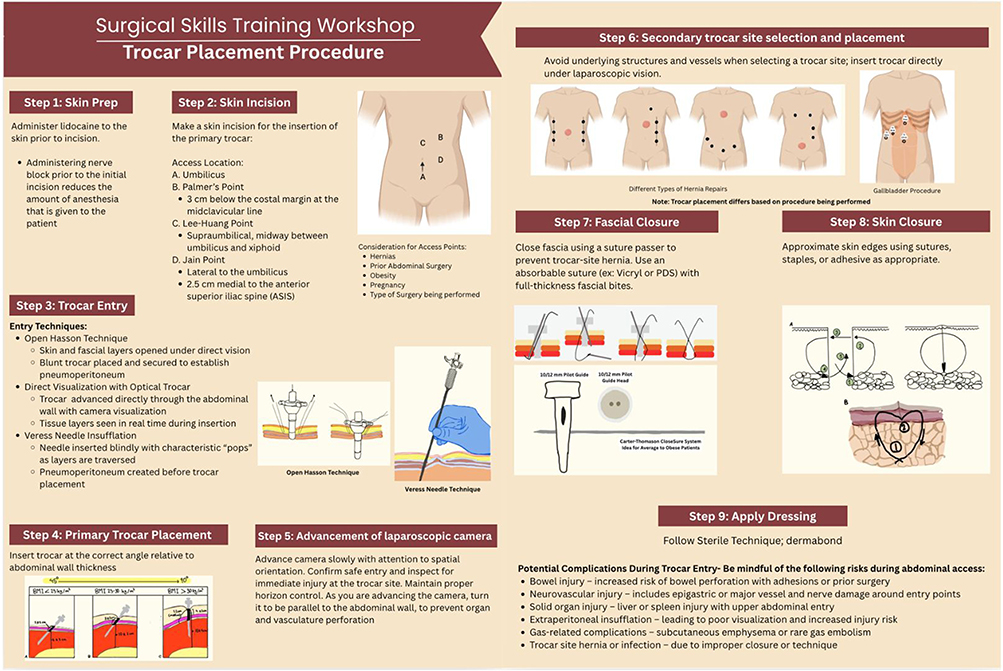 |
Figure 2 Educational handout materials regarding the trocar placement procedure provided to students before the workshops. The handout lists the ten steps of the trocar placement procedure, including skin preparation, skin incision, trocar entry, primary trocar placement, and advancement of the laparoscopic camera. The additional final four steps of trocar placement include secondary trocar site selection and placement, fascial closure, skin closure, and dressing application. Information on the potential complications during trocar entry is also provided. The illustration in Step 3 has been adapted from Kriener et al11 The illustration in Step 4 has been adapted from Hurd et al12. |
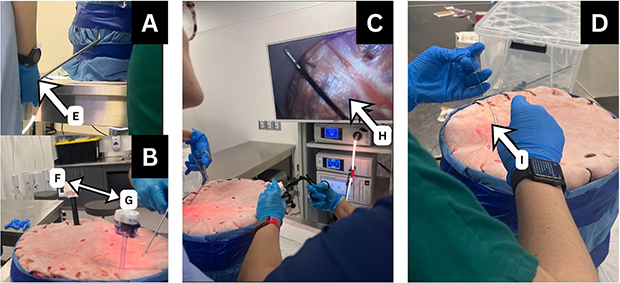 |
Figure 3 Trainees using the trocar placement simulation model. (A) A trainee stabilizes the laparoscopic camera through the access port (white arrow E). (B) Two trocars are placed within the model to demonstrate port positioning (double-headed arrows F and G). (C) A suture passer is advanced through a trocar with real-time visualization on the monitor (arrow H). (D) Fascial closure is completed using a hand-tied knot (arrow B). |
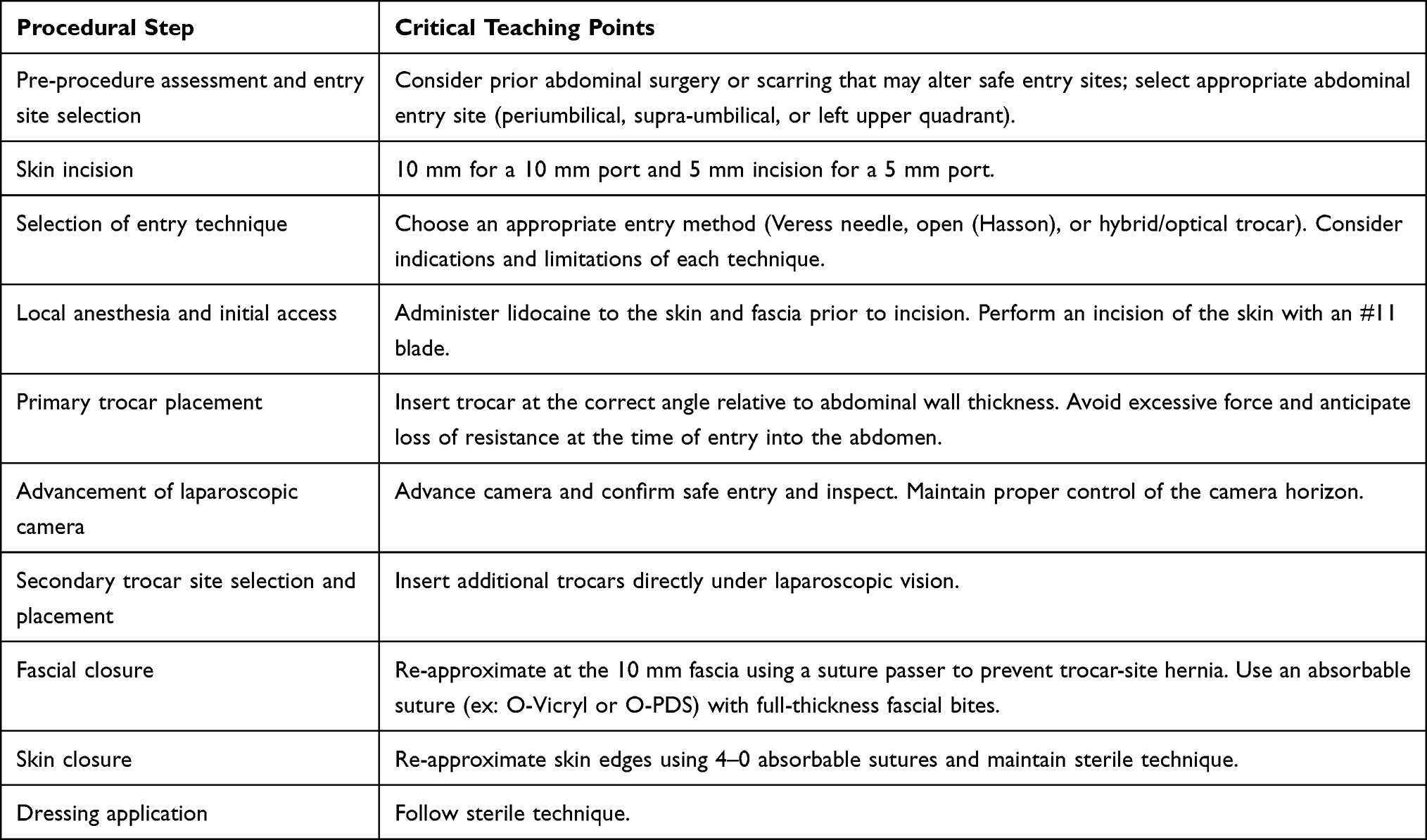 |
Table 2 Procedural Teaching Points Emphasized During the Trocar Placement Workshop |
Survey Instrument
We used a volunteer post-workshop survey to assess the effectiveness of a hands-on trocar placement training model implemented across three surgical skills acquisition workshops for medical student surgical trainees. A total of 60 students attended the three workshops (n = 20, 23, and 17), and 43 completed the post-workshop survey. Self-reported improvements in confidence and perceived technical skills were assessed using a 5-point Likert-scale survey (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree) in which participants rated their agreement with statements regarding confidence in performing laparoscopic entry, ability to use related instruments, and overall procedural preparedness. The outcomes include awareness of the risks and complications associated with trocar insertion, perceived realism of tissue resistance, tactile feedback, and anatomical fidelity. These measures captured both the technical and cognitive components of procedural learning. The surveys were completed at the conclusion of each workshop to obtain immediate perceptions of learning and skill development.
The survey items included statements such as “The model improved my confidence in performing laparoscopic entry”, “The model realistically simulated abdominal wall resistance”, and “I feel more prepared to recognize complications associated with trocar placement”.
Statistical Analysis
As this was an initial descriptive assessment of our model, the analyses were limited to frequencies and proportions; inferential statistics were not performed. For key outcome measures, the proportion of participants who selected “strongly agree” or “agree” was calculated to assess the overall positive response trends using Microsoft Excel.
Results
Of the 60 medical students who attended the workshops, 43 (72%) completed the post-workshop survey, of whom 38 (88%) responded to the prior-experience item. Among these 38 respondents, 93.0% reported 0 to 1 years of prior surgical-simulation exposure (Figure 4). Following the workshop, the survey participants reported high levels of confidence in laparoscopic procedures, with over 90% selecting “strongly agree” or “agree”. Sixty-four percent of the participants (28/43) reported feeling more prepared to recognize trocar- and Veress needle-related complications, selecting “agree” or “strongly agree”. The participants rated the simulation model as realistic, with 92% (40/43), 85% (37/43), and 82% (35/43) endorsing abdominal wall resistance, anatomical layer representation, and tactile feedback, respectively (Figure 5). Ninety-seven percent of the participants rated the educational value of the model favorably, and 93% reported improved self-perceived confidence in laparoscopic procedures. Additionally, most respondents expressed willingness to recommend the model to peers, with strong support for incorporation into formal surgical curricula (Figure 6).
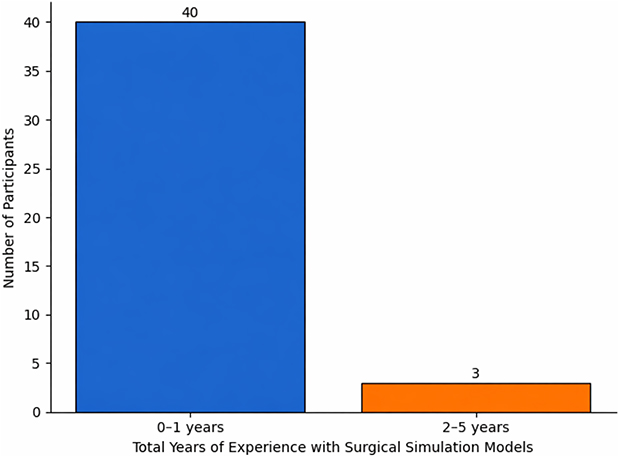 |
Figure 4 Prior experience with surgical simulation models. This figure illustrates that most participants reported minimal experience with surgical simulation models. |
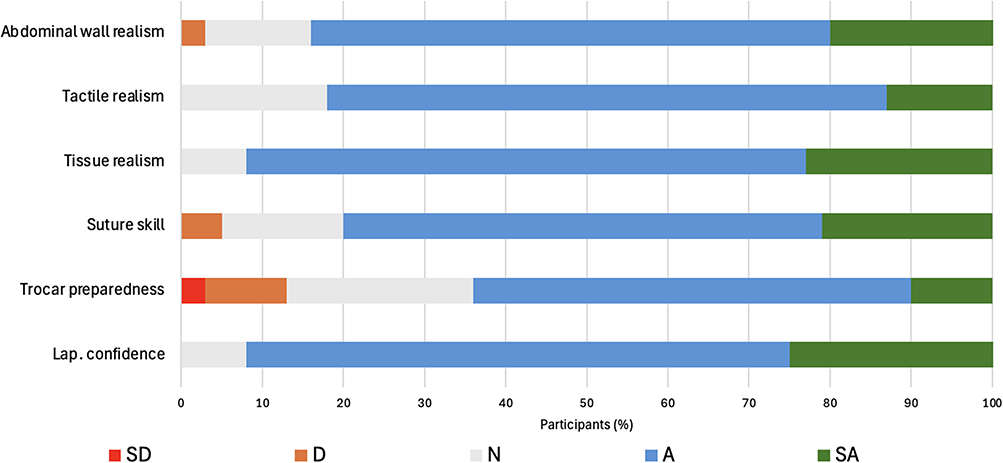 |
Figure 5 Distribution of participant responses to survey items. The survey items assessed confidence in laparoscopic procedures, preparedness to recognize trocar and Veress needle related complications, suture passer skill development, and perceived realism of the simulation model (n = 43). Responses were predominantly in the “strongly agree” or “agree” categories across all domains. Abbreviations: SD, strongly disagree; D, disagree; N, neutral; A, agree; SA, strongly agree. |
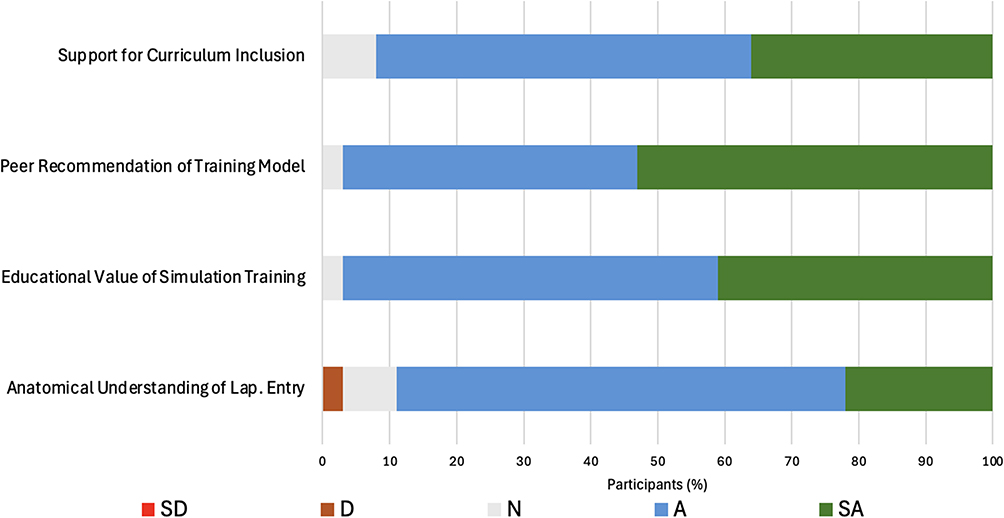 |
Figure 6 Participant responses for model utility. The participant responses were assessed for perceived anatomical understanding of laparoscopic entry, educational value of the simulation model, willingness to recommend the model to peers, and support for its inclusion in surgical training curricula (n = 43). Responses were predominantly “strongly agree” and “agree”. Abbreviations: SD, strongly disagree; D, disagree; N, neutral; A, agree; SA, strongly agree. |
Discussion
This study evaluated medical student reactions (Kirkpatrick Level 1) regarding perceived confidence, preparedness, and realism and did not assess objective skill acquisition, behavioral transfer, or long-term retention.13 Throughout this discussion, terms such as “improved” and “enhanced” refer to participants’ self-perception following the workshop and should be interpreted as Kirkpatrick Level 1 outcomes only. Following exposure to the model, the trainees reported high self-rated confidence, procedural preparedness, and perceived technical skill development. Most participants reported an increased sense of confidence in laparoscopic procedures, as 93% selected “strongly agree” or “agree” (Figure 5). This is particularly notable because most participants had minimal exposure to surgical simulations (Figure 4). The model appeared to have been effective even for early learners, which suggests its utility as an introductory training platform. Skill development was further supported for suture passer use (Figure 5). The models supported hands-on practice of related procedural skills (eg, trocar placement, Veress needle insertion, suture passer use, fascial closure) within a single training environment; this integration of multiple skill components may enhance overall procedural fluency. Participants also reported an enhanced sense of preparedness for recognizing trocar- and Veress needle-related complications, as 64% selected “agree” or “strongly agree” (Figure 5). This indicates that the model contributes not only to helping trainees develop situational awareness and anticipate procedural challenges but also to the acquisition of the cognitive aspects of surgical training, including risk recognition and procedural planning.
A major strength of the model was its perceived realism, with high agreement reported for tissue resistance (92%), tactile feedback (82%), and abdominal wall layer simulation (85%) among the participants (Figure 5). These findings suggest that porcine and ovine tissues successfully replicated the key physical characteristics of laparoscopic entry, which are often lacking in synthetic or low-fidelity models. The realistic tactile environment likely allowed participants to practice under conditions that approximated clinical experience.
Collectively, these results highlight the model’s efficacy as a hands-on and accessible training platform that enhances confidence, technical skill development, and awareness of procedural challenges. Its ability to provide realistic tactile feedback while remaining feasible for repeated use is a valuable adjunct to existing surgical education methods. A key advantage of this model is its practical accessibility. Tissue procurement relied on abdominal walls procured from animals already euthanized for unrelated approved studies, eliminating additional animal use and substantially reducing cost compared with cadaveric or live-animal training applications. Assembly and workshop facilitation required no specialized infrastructure, making the model readily scalable across institutions with varying resources. This is particularly relevant for programs in resource-limited settings where high-fidelity commercial simulators and cadaveric labs are often unavailable. The low per-session cost, straightforward preparation, and absence of equipment maintenance burdens make this model a viable option for integration for surgical trainees.
Laparoscopic trocar training methods range from in vivo animal models to low-cost synthetic and haptic simulators. Live animal models, such as those used by Moreno et al14 and Van Sickle et al, 15 offer high anatomical fidelity and allow quantification of insertion mechanics and fascial integrity; however, they focus primarily on the biomechanical assessment rather than trainee skill acquisition and do not address insertion angle, applied force, or suture placement in an educational context. Low-fidelity synthetic models such as the Raj Model and table-based cardboard trainers allow repeated, portable practice and demonstrate moderate user satisfaction but lack realistic anatomical layering, physiological tissue resistance, and tactile cues critical for accurate trocar placement.16 Haptic simulators replicate force-displacement profiles but are limited by simplified one-dimensional resistance profiles and absence of anatomical layering.17 AI-based optical detection systems, such as YOLOv8, show promise for real-time tissue layer identification but do not provide the tactile resistance or force cues necessary to guide safe trocar placement.18 Ebina et al also utilized animal tissues to increase the fidelity in their training model designed for motion analysis in psychomotor skills training. Similar to our study, their research included early learners.19
Our porcine abdominal wall training model addresses these limitations by providing a reproducible platform that combines the tactile fidelity of real tissue with the accessibility and low-risk practice of synthetic trainers. The procured porcine abdominal walls replicated the heterogeneous multilayered structure of the human abdominal wall, offering realistic resistance, spatial orientation, and force feedback. Unlike live-animal models, this approach uses tissue from animals already euthanized for unrelated approved studies, avoiding additional animal use and reducing cost. It also allows repeated practice without direct risks. Compared to other modalities, our approach exposes trainees to authentic tissue mechanics and dynamic feedback during insertion, thereby enhancing skill acquisition and technique refinement (Figure 5). By bridging the gap between purely mechanical simulations and live-tissue experiences, our model offers an educationally robust platform for deliberate practice.
Our simulation model achieved a high degree of perceived realism without the resource burden associated with cadaver-based training. Although advanced simulators may offer additional features, the consistently strong ratings across the realism domains in this study indicate that the model provided sufficient fidelity to support effective training.
This study demonstrated that our trocar placement training model is well-suited for integration into preclinical curricula and surgical skills laboratories, which provides a structured platform for students to gain hands-on experience with laparoscopic entry. This skill is crucial to learn in a structured training environment because, in many traditional surgical education curricula, trocar placement is often introduced through observation rather than hands-on practice.20–24 Trainees often observe abdominal entry without dedicated hands-on practice, and their first attempt frequently occurs in the operating room under clinical pressure.20,24 This “see one, do one” approach introduces real clinical risk because entry with a Veress needle or trocar is associated with a disproportionate share of laparoscopic complications, including bowel and vascular injuries, which can lead to significant morbidity and mortality.20–23 Estimates indicate that a substantial portion of major laparoscopic injuries occur during initial entry and that such events are more common when performed without direct supervision.20,21 Such injuries highlight the narrow safety margin inherent in blind trocar insertion and underscore the need for earlier, deliberate training outside of the clinical setting.23–25 By allowing trainees to engage with tactile cues, force modulation, spatial orientation, and recognition of tissue transitions, our model promotes acquisition of nuanced procedural skills that are difficult to learn through observation alone.15,26
The results presented in Figure 6 further emphasize the educational value and feasibility of the model for integration into surgical training. Most participants agreed or strongly agreed that the model enhanced their anatomical understanding of laparoscopic entry and provided substantial educational benefits. Notably, a strong endorsement of peer recommendations and curriculum inclusion reflect both learner satisfaction and perceived utility within a broader educational framework (Figure 6). The observed improvements in confidence and complication awareness are particularly important, given that laparoscopic entry remains a high-risk step despite its routine nature.20–23 The integration of this model into structured curricula could take multiple forms, including preclinical anatomy courses, procedural skills workshops, and existing simulation-based curricula.25,27,28,29
Our study has several limitations. First, the study used a post-only survey design without a pre-workshop comparator; the reported gains in confidence and preparedness reflect retrospective self-perception rather than measured changes. Second, our evaluations relied on subjective participant assessments, without any assessment of objective performance metrics. The absence of pre-intervention measurements and objective performance metric evaluations limits the strength of the educational conclusions that can be drawn from this study. Therefore, the statistical analyses remained largely descriptive. Third, the study was conducted at a single institution with a small convenience sample, limiting the generalizability of the findings. Fourth, a comparison group was not included, making it difficult to isolate the effects of the simulation model from concurrent didactic instruction or attention effects. Fifth, immediate educational outcomes were assessed without longitudinal follow-up; skill transfer to clinical settings was not evaluated. Sixth, biological tissue variability across sessions was not quantified and may have influenced participant experience and perceived realism. Future work should incorporate pre/post-workshop assessments, objective skill metrics (eg, time-to-completion, force tracking, fascial layer recognition), comparison against synthetic and cadaveric models, and follow-up assessment of skill transfer to live operative settings.
Conclusion
Our findings indicate that an affordable ex vivo tissue model is feasible for early-learner trocar placement training and is rated favorably for realism, educational value, and confidence-building. Participants reported high post-workshop confidence, perceived technical skill, and recognition of procedural risks. Because data were collected post-only and at the reaction level (Kirkpatrick Level 1), these findings reflect learner perception rather than objective skill acquisition or transfer. By providing structured, low-risk exposure to a high-stakes procedural step, this model addresses a gap in medical education and represents a promising and scalable candidate for early surgical training. Longitudinal follow-up and validation against objective skill metrics and assessment of clinical transfer remain prospective next steps to establish educational impact beyond learner satisfaction.
Data Sharing Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
The IRB of the University of Minnesota provided an exemption (IRB Study number: 00027053). Written informed consent was obtained from all the trainees involved in the study.
Acknowledgments
We are grateful to the University of Minnesota Experimental Surgery Services for their assistance and support during the assembly of the models prior to the workshops. We also thank the University of Minnesota M-Simulation Center for providing their simulation expertise and the realistic educational environment for the surgical skills workshops. We sincerely appreciate the trainees who consented to participate in the surgical skills acquisition workshop. Finally, we are thankful to Mark Wille, clinical research project manager at the University of Minnesota, for administrative support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The William Harmon Fund for Surgical Education and Research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Morales-Conde S, Peeters A, Meyer YM, et al. European association for endoscopic surgery (EAES) consensus statement on single-incision endoscopic surgery. Surg Endosc. 2019;33(4):996–11. doi:10.1007/s00464-019-06693-2
2. Fried GM, Feldman LS, Vassiliou MC, et al. Proving the value of simulation in laparoscopic surgery. Ann Surg. 2004;240(3):518–525. doi:10.1097/01.sla.0000136941.46529.56
3. Rahimi AM, Hardon SF, Uluç E, Bonjer HJ, Daams F. Prediction of laparoscopic skills: objective learning curve analysis. Surg Endosc. 2023;37(1):282–289. doi:10.1007/s00464-022-09473-7
4. Krishnakumar S, Tambe P. Entry complications in laparoscopic surgery. J Gynecol Endosc Surg. 2009;1(1):4–11. doi:10.4103/0974-1216.51902
5. Molloy D, Kaloo PD, Cooper M, Nguyen TV. Laparoscopic entry: a literature review and analysis of techniques and complications of primary port entry. Aust N Z J Obstet Gynaecol. 2002;42(3):246–254. doi:10.1111/j.0004-8666.2002.00246.x
6. Gawad N, Zevin B, Bonrath EM, Dedy NJ, Louridas M, Grantcharov TP. Introduction of a comprehensive training curriculum in laparoscopic surgery for medical students: a randomized trial. Surgery. 2014;156(3):698–706. doi:10.1016/j.surg.2014.04.046
7. Costello DM, Huntington I, Burke G, et al. A review of simulation training and new 3D computer-generated synthetic organs for robotic surgery education. J Robot Surg. 2022;16(4):749–763. doi:10.1007/s11701-021-01302-8
8. James HK, Chapman AW, Pattison GTR, Griffin DR, Fisher JD. Systematic review of the current status of cadaveric simulation for surgical training. Br J Surg. 2019;106(13):1726–1734. doi:10.1002/bjs.11325
9. de Montbrun SL, MacRae H. Simulation in surgical education. Clin Colon Rect Surg. 2012;25(3):156–165. doi:10.1055/s-0032-1322553
10. Panait L, Akkary E, Bell RL, Roberts KE, Dudrick SJ, Duffy AJ. The role of haptic feedback in laparoscopic simulation training. J Surg Res. 2009;156(2):312–316. doi:10.1016/j.jss.2009.04.018
11. Kriener K, Lala R, Homes RAP, et al. Mechanical characterization of the human abdominal wall using uniaxial tensile testing. Bioengineering. 2023;10(10):1213. doi:10.3390/bioengineering10101213
12. Hurd WH, Bude RO, DeLancey JO, Gauvin JM, Aisen AM. Abdominal wall characterization with magnetic resonance imaging and computed tomography. The effect of obesity on the laparoscopic approach. J Reprod Med. 1991;36(7):473–476.
13. Kirkpatrick DL. Techniques for evaluating training programs. J Am Soc Train Dir. 1959;13:3–9.
14. Moreno DG, Pereira CAM, Sant Anna RK, et al. Laparoscopic insertion of various shaped trocars in a porcine model. JSLS. 2019;23(2):e201900002. doi:10.4293/JSLS.2019.00002
15. Van Sickle KR, Nanda Kumar HR, Parikh A, Ayon AA, Cohn SM. Development of an animal model to investigate optimal laparoscopic trocar site fascial closure. J Surg Res. 2013;184(1):126–131. doi:10.1016/j.jss.2013.05.025
16. Kailavasan M, Berridge C, Kandaswamy G, et al. A low-cost synthetic abdominal wall model (“raj model”) for the training of laparoscopic port insertion. World J Surg. 2020;44(5):1431–1435. doi:10.1007/s00268-019-05354-8
17. Galvan A, Da Costa AK, Shields J, Kho K, Fey AM. Haptic simulator for trocar insertion training.
18. Jearanai S, Wangkulangkul P, Sae-Lim W, et al. Development of a deep learning model for safe direct optical trocar insertion in minimally invasive surgery: an innovative method to prevent trocar injuries. Surg Endosc. 2023;37(9):7295–7304. doi:10.1007/s00464-023-10309-1
19. Alkatout I. Complications of laparoscopy in connection with entry techniques. J Gynecol Surg. 2017;33(3):81–91. doi:10.1089/gyn.2016.0111
20. Jansen FW, Kapiteyn K, Trimbos-Kemper T, Hermans J, Trimbos JB. Complications of laparoscopy: a prospective multicentre observational study. Br J Obstet Gynaecol. 1997;104(5):595–600. doi:10.1111/j.1471-0528.1997.tb11539.x
21. Vilos GA, Ternamian A, Dempster J, Laberge PY; Society of Obstetricians and Gynaecologists of Canada. Laparoscopic entry: a review of techniques, technologies, and complications. J Obstet Gynecol Can. 2007;29(5):433–447. doi:10.1016/s1701-2163(16)35496-2
22. Chapron CM, Pierre F, Lacroix S, Querleu D, Lansac J, Dubuisson JB. Major vascular injuries during gynecologic laparoscopy. J Am Coll Surg. 1997;185(5):461–465. doi:10.1016/S1072-7515(01)00958-9
23. Sutherland LM, Middleton PF, Anthony A, et al. Surgical simulation: a systematic review. Ann Surg. 2006;243(3):291–300. doi:10.1097/01.sla.0000200839.93965.26
24. American College of Surgeons, Association of Program Directors in Surgery. ACS/APDS Surgical Skills Curriculum for Residents. American College of Surgeons; 2008.
25. Issenberg SB, McGaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ. Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Med Teach. 2005;27(1):10–28. doi:10.1080/01421590500046924
26. Dawe SR, Pena GN, Windsor JA, et al. Systematic review of skills transfer after surgical simulation-based training. Br J Surg. 2014;101(9):1063–1076. doi:10.1002/bjs.9482
27. McGaghie WC, Issenberg SB, Cohen ER, Barsuk JH, Wayne DB. Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review. Med Educ. 2011;45(6):534–544.
28. Ziv A, Wolpe PR, Small SD, Glick S. Simulation-based medical education: an ethical imperative. Acad Med. 2003;78(8):783–788. doi:10.1097/00001888-200308000-00006
29. Seymour NE, Gallagher AG, Roman SA, et al. Virtual reality training improves operating room performance: results of a randomized, double-blinded study. Ann Surg. 2002;236(4):458–463. doi:10.1097/00000658-200210000-00008
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Outcomes of Non-Penetrating Deep Sclerectomy for Primary Congenital Glaucoma Performed by Experienced versus Trainee Surgeons: A Cohort Study

Khan OA, Sesma G, Alawi A, AlWazae M
Clinical Ophthalmology 2023, 17:897-906
Published Date: 16 March 2023
A Comparative Study of Traditional Technique Guide versus Virtual Reality in Orthopedic Trauma Training
Lamb A, McKinney B, Frousiakis P, Diaz G, Sweet S
Advances in Medical Education and Practice 2023, 14:947-955
Published Date: 4 September 2023