Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 14
Sick Leave and Costs in Active Workers with Chronic Osteoarthritis Pain in Spain: Outcomes of the OPIOIDS Real World Study
Authors Sicras-Mainar A ![]() , Tornero-Tornero JC, Vargas-Negrín F
, Tornero-Tornero JC, Vargas-Negrín F ![]() , Lizarraga I, Sicras-Navarro A, Rejas-Gutierrez J
, Lizarraga I, Sicras-Navarro A, Rejas-Gutierrez J
Received 29 October 2021
Accepted for publication 24 February 2022
Published 15 March 2022 Volume 2022:14 Pages 25—38
DOI https://doi.org/10.2147/OARRR.S346746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Natasha Hodgkinson
Antoni Sicras-Mainar,1 Juan Carlos Tornero-Tornero,2 Francisco Vargas-Negrín,3 Isabel Lizarraga,4 Aram Sicras-Navarro,1 Javier Rejas-Gutierrez5
1Health Economics and Outcomes Research Department, Atrys Health, Barcelona, Spain; 2Department of Anesthesiology, Hospital Clínico Universitario of Valencia, Valencia, Spain; 3Healthcare Center Dr. Guigou, Canary Islands Health Service, Tenerife, Spain; 4Medical Department, Pfizer, SLU, Alcobendas, Madrid, Spain; 5Health Economics and Outcomes Research Department, Pfizer, SLU, Alcobendas, Madrid, Spain
Correspondence: Antoni Sicras-Mainar, Health Economics and Outcomes Research Department, Atrys Health, C/ Provença 392, bajos, Barcelona, 08025, Spain, Tel +34 934 581 561, Fax +34 93 458 73 03, Email [email protected]
Purpose: To estimate the number of sick leave days and productivity costs in active workers with osteoarthritis (OA) who initiated opioid treatment for moderate/severe chronic pain in clinical practice in Spain.
Patients and Methods: This is a secondary analysis of the longitudinal, retrospective OPIOIDS study, using electronic medical records (EMR) of patients aged ≥ 18 years, who started an opioid treatment for moderate/severe chronic OA pain between 2010 and 2015 after treatment failure with ≥ 1 first-line drugs (acetaminophen, metamizole and/or nonsteroidal anti-inflammatory drugs [NSAIDs]). The number of days of sick leave and productivity costs were analyzed during a follow-up period of 36 months.
Results: A total of 5089 patients with moderate/severe chronic OA pain, aged 56.8 years (standard deviation [SD]: 4.6) (56.6% were female), were analyzed: 73.3% of them started a treatment with weak opioids and 26.7% of them were treated with strong opioids. At 36 months, adherence was 21.0% (strong opioids: 15.4%; weak opioids: 23.0%; p< 0.001), and 77% of patients had at least one sick leave related with chronic OA pain, with an average of 93 days off work in all working patients (120.5 days in patients with sick leaves). Besides, 16.9% of the study population had sick leave periods that lasted at least 6 months. Pain reduction was modest (− 1.2 points; − 4.0%, p< 0.001). The cost of sick leave was € 2594 patient/year, and factors such as older age (β=0.043), female sex (β=0.036), comorbidities (β=0.035) and strong opioid use (β=0.031) were associated with higher productivity costs (p< 0.05 in all associations).
Conclusion: Active workers who started opioid treatment for moderate/severe chronic OA pain showed an increased frequency of sick leave and productivity cost, with a modest effect on pain relief. Older age, female sex, comorbidities, and strong opioids were associated with higher costs for society.
Keywords: analgesics, arthritis, disability, sick days, observational study
Introduction
Osteoarthritis (OA) is a degenerative joint pathology characterized by cartilage deterioration, with a proliferative reaction of the subchondral bone and inflammation of the synovial membrane but also meniscal degeneration and inflammation and fibrosis of the infrapatellar fat pad.1,2 It is estimated that 6–24% of adults have chronic OA pain, and the incidence increases with age.3 In Spain, according to the EPISER study,4 the prevalence of OA in people aged >40 years is 29.4%. Therapeutic approaches include non-pharmacological measures, drug treatments and joint replacement surgery for the most disabled patients.5 Drug treatments include nonsteroidal anti-inflammatory drugs (NSAIDs), which are often used in patients who do not respond to first-choice analgesics such as acetaminophen.6 Tramadol is the weak opioid with the greatest evidence on efficacy and safety, while strong opioids are used for treating moderate to severe pain with an unsatisfactory response to other treatments.7,8 The analgesic efficacy of strong opioids was estimated in cancer patients, but their efficacy to relieve chronic non-cancer pain is unclear.5,7,8 Furthermore, some scientific societies, such as the Osteoarthritis Research Society International (OARSI) or the American College of Rheumatology (ACR) discourage their use in OA treatment.1,9
The chronic pain and disability associated with OA have a negative impact on the patients’ quality of life and are some of the main causes of days off work due to sick leave. In addition, these patients have lower productivity, which increases social costs.1,8,10–15 It has been estimated that one out of four active workers with OA leave the workplace before the normal retirement age.16 The mechanisms underlying the effects of OA in occupational performance are not entirely evident.15 Most studies have found that pain and/or functional joint deterioration are the main factors that reduce labor productivity.10 Joint pain may have a direct effect on labor productivity, regardless of comorbidities or other associated factors, but it may also have an indirect effect, as it causes physical limitations, depression, poor adaptation and poor sleep quality.17 On the other hand, the use of opioids in patients with OA has increased, but its connection with the number of days off work due to sick leave and productivity costs are not clear.18,19 The OPIOIDS (Outcomes in Patients usIng Opioids In Painful Disorders in Spain) study, carried out under conditions of routine medical practice in Spain, collected information on the impact of opioids in OA patients who had failed the first-line treatment of chronic pain with analgesics such as acetaminophen, metamizole and/or NSAIDs. The OPIOIDS was a non-interventional, multicenter, longitudinal retrospective study, with a new user design, based on the review of electronic medical records (EMR) of OA patients included in the database of health providers in seven regions of Spain.20 However, the consequences of the use of opioids on the number of sick leave days and costs in the subset of active workers were not estimated. Therefore, the objective of this Research was to carry out a secondary analysis of the OPIOIDS study to estimate the number of sick leave days and productivity costs in active workers with OA, who initiated an opioid treatment for moderate/severe chronic pain in clinical practice in Spain.
Materials and Methods
Design of the Study
We conducted a secondary analysis of the longitudinal, multicenter, retrospective OPIOIDS study,20 which used electronic medical records (EMR) from the BIG-PAC database,21 including the records of 1.8 million people from seven Spanish autonomous communities.22 EMRs were anonymized according to Organic Law 3/2018, of December 5, on the Protection of Personal Data and guarantee of digital rights.23 EMRs of patients who started a new treatment (index date) with any weak or strong opioid drug in monotherapy or in combination with other analgesics between January 1st, 2010 and December 12th, 2015 (recruitment period) were included. Patients were followed from the index date for a maximum of 3 years and/or until discontinuation of opioid treatment (follow-up period), change to another analgesic, loss to follow-up and/or until any-cause death. The OPIOIDS study was classified by the Spanish Agency for Medicines and Health Products as EPA-OD and subsequently approved by the Ethics Committee of the Hospital of Terrassa (Barcelona) (Code: PFI-OP-2018-01) on March 11, 2019. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines for reporting observational studies were followed.24
Study Population
We included the EMR of patients who started a new treatment with strong or weak opioids, alone or combined with other analgesics, for the treatment of moderate to severe (≥ 5 points on the numeric rating scale [NRS] of pain) chronic (≥ 3 months) nociceptive pain in any site due to OA between 1/01/2010 and 31/12/2015.25 Diagnoses were analyzed using the International Classification of Diseases (10th edition) Clinical Modification (ICD-10-CM) coding system.26 The site of pain was a) hip and knee (M16, M17), b) lumbar (M54.5), and other sites (M15, M18, M19, M40, M41) according to medical criteria.
Patients had previously been treated with ≥1 first-line drugs such as acetaminophen, metamizole and/or NSAIDs. EMRs were obtained during the 12 months before the index date and over the next 36 months. The index date was that of the initiation of the new opioid treatment and two study cohorts were considered, according to the type of opioid administered (weak or strong).
Additional inclusion criteria for the study population were (a) age ≥18 years, (b) being occupationally active, c) being active in the database (≥2 health records in the computer system) a minimum of 12 months before the start of the study, (d) having regular monitoring (≥2 health records in the computer system from the index date), and (c) being included in the chronic prescription program (with a record of the daily dose, time interval and duration of each treatment administered (≥2 prescriptions during the follow-up period). Exclusion criteria were (a) being displaced or out-of-area; (b) being permanently institutionalized, (c) having terminal illness and/or dialysis (ICD-10-CM: N18), (d) neuropathic pain/radiculopathy (ICD-10-CM: G50-65) or cancer (ICD-10-CM: G89.6), and (e) not being occupationally active (retired, unemployed, permanent work disability, early retirement and/or maternity leave).
Demographic Variables, Comorbidities and Medication
Demographic and comorbidity variables, such as age (continuous and by range: 18–44, 45–54 and ≥55 years on the index date), sex and body mass index (BMI), along with medical history were recorded at the index date (baseline characteristics). The Charlson comorbidity index and the number of chronic comorbidities were used as a summary variable of general comorbidity and an approximation of patient severity.27
The medications (active ingredients) indicated for chronic OA pain were analyzed using the Anatomical Therapeutic Chemical Classification System (ATC codes: N02AA01 to N02AX06) from prescription records. The prescription of treatments was the physician’s discretion. The medical specialty that initiated the prescription and the type of opioid prescribed were determined. Adherence, persistence, medication possession ratio (MPR) and discontinuation definitions were as previously described in the OPIOIDS study.20 The requirement of rehabilitation sessions was also estimated in the study population.
Cost of Days of Sick Leave (Productivity Costs)
The cost of days of temporary work disability from the social perspective was determined by the human capital method. It was considered that the mean salary of the replacement of the active patient amounted to €119.44 per day not worked, according to the Spanish National Statistics Institute (INE).28 The number of days of sick leave were expressed as absolute and relative values (patients with sick leave), and as the mean days of sick leave per patient (patients with/without sick leave).
Clinical Effectiveness
Clinical effectiveness was estimated as pain intensity using the 11-point NRS (5–7: moderate pain; >7: severe pain) at the closest date before the index date (baseline value) and at the end of the study.25 Variations were assessed as percentages from the baseline value.
Statistical Analysis
The data were validated by computer sentences (specific scripts). Descriptive, univariate statistical analyses were made. Qualitative data were analysed using absolute and relative frequencies. The 95% confidence intervals (CI) for parameter estimation were based on the total number of subjects with no missing values. ANOVA and the chi-square tests for independent groups were used in the bivariate analysis. Paired tests were also used to evaluate the before-after differences for each subgroup (McNemar’s and the Student’s t tests). A survival analysis was made by estimating the Kaplan-Meier curves (log rank test) to analyze the persistence to the opioid treatment, applying a Cox proportional risk model (corrected by covariates) to determine the hazard ratio (HR) and its 95% CI between strong and weak opioids. Covariate analysis was used to correct the cost per patient of days of sick leave. The covariates considered were sex, age, general comorbidity (Charlson index), time from diagnosis, treatment persistence and the MPR. A multiple linear regression model (procedure: consecutive steps) was constructed to examine the variables associated with sick leave (dependent variable: cost per patient [all] of sick leave). The analyses used IBM SPSS, version 23.0, NY, USA software.
Results
Study Population, Treatments and Rehabilitation Sessions
Out of an initial selection of 1,280,684 subjects aged ≥18 years who sought care during the recruitment period, 124,798 were diagnosed with OA in any site with chronic nociceptive pain. It was estimated that 34.0% of them initiated a new opioid treatment (n=42,429) and were included in the OPIOIDS study. For the present analysis, 37,340 subjects (77.2%) were excluded, as they were not active workers. Finally, 5089 patients met the study selection criteria (Figure 1). Table 1 shows the demographic characteristics and comorbidities; the mean age was 56.8 (standard deviation [SD]: 4.6) years and 56.6% were female. Only 14 patients were aged ≥ 65 years.
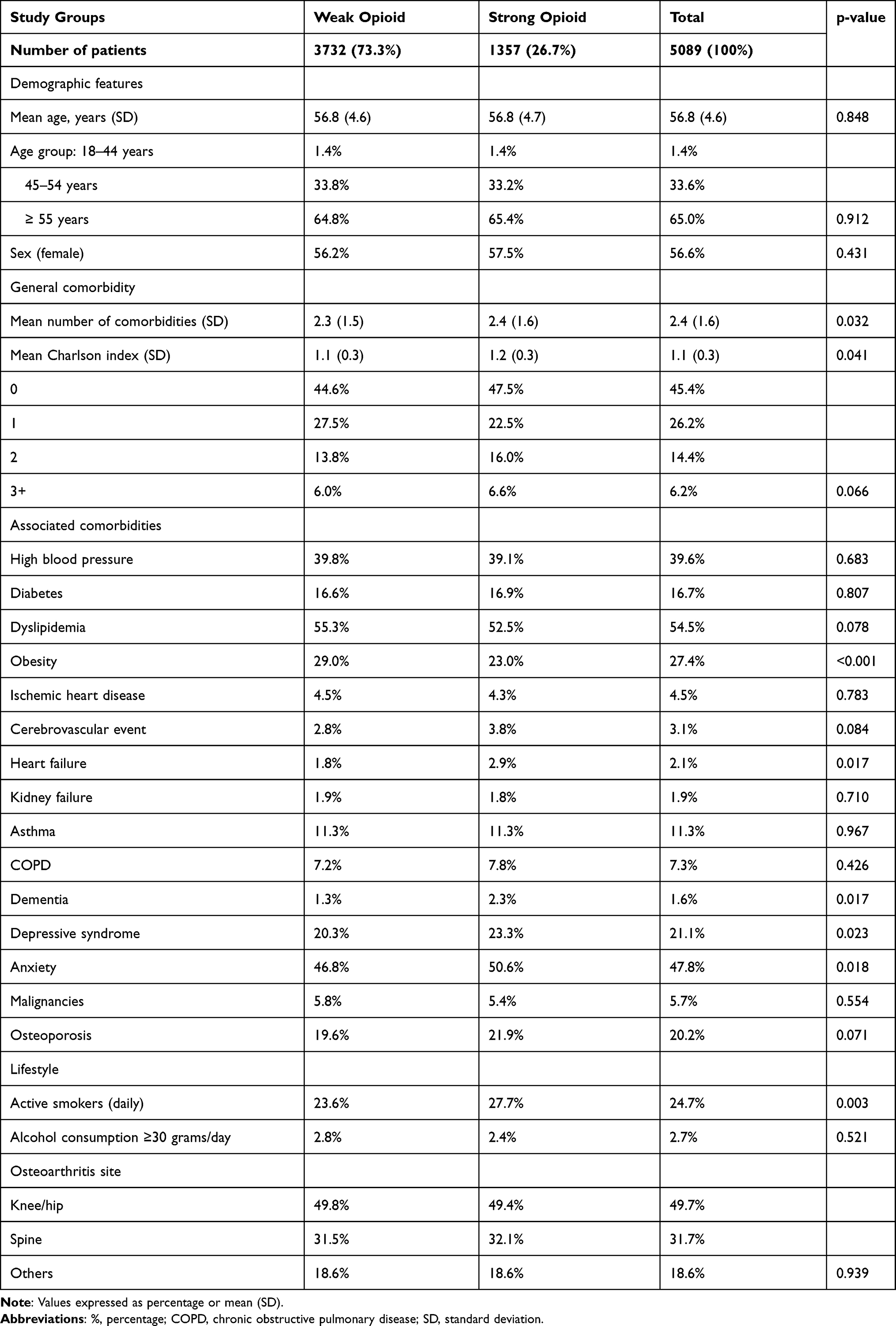 |
Table 1 Baseline Characteristics (Demographic and Morbidity) of Patients by Study Groups |
 |
Figure 1 Study flow diagram. Abbreviation: NRS, numeric rating scale. |
Most of the study population (73.3% [n=3732]) initiated their analgesic treatment with a weak opioid and 26.7% (n=1357) with a strong opioid. Patients receiving strong opioids had more comorbidities (Charlson index: 1.2 vs 1.1; p=0.041) (Table 1). The medical department that prescribed the opioid and the kind of opioid prescribed can be seen in Supplementary Table S1. Almost all prescriptions for weak opioids were for tramadol or tramadol + acetaminophen (98.1%) while fentanyl, tapentadol and oxycodone-naloxone were the most frequently prescribed strong opioids (76.4%). Strong opioids were proportionately more frequently prescribed by specialists than by GPs (40.6% vs 22.6%; p<0.001). Supplementary Table S2 shows the concomitant medication prescribed by group and follow-up periods. During the 12 months before initiation of opioids, mean concomitant medication was 1.4 analgesics per patient compared with 1.2 at 36 months (p<0.001). This reduction in the average concomitant medication administered was mainly due to the lower use of acetaminophen (73.0% vs 38.9%, p<0.001), which was offset by the significant increase in the use of NSAIDs and metamizole (Supplementary Table S2).
Treatment adherence, persistence, MPR, reasons for discontinuation and mortality by study group (strong/weak opioids) are shown in Table 2. The median duration of opioid treatment was 187 days (interquartile range: 84–738 days). At 36 months, overall treatment adherence was 21% (95% CI: 19.9–22.1%), being 23% (95% CI: 21.6–24.4%) for weak opioids and 15.4% (95% CI: 13.5–17.3%) for strong opioids (p<0.001). Supplementary Figure S1 shows the Kaplan-Meier curves for the persistence of opioid treatment, with a corrected mean that was 27% higher for weak compared with strong opioids (HR=1.27 [1.17–1.34], p=0.001). Pain intensity decreased moderately (−1.2 points [−14%]; p<0.001) and only 6.8% of patients could stop the treatment with opioids as they had no moderate or severe pain (Supplementary Table S3). Pain reduction was greater in patients on weak opioids in comparison with those receiving strong opioids.
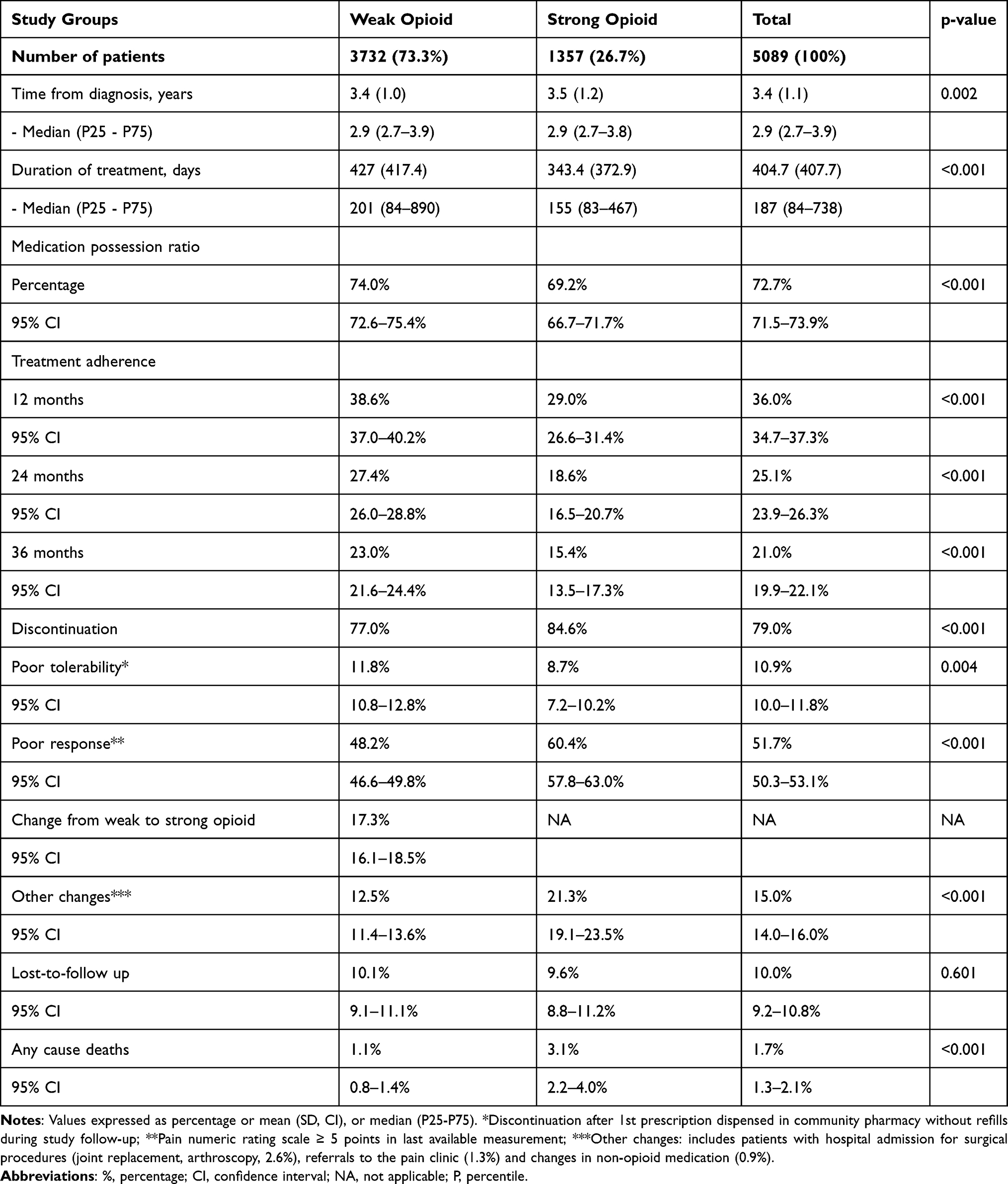 |
Table 2 Treatment Persistence and Adherence, Medication Possession Ratio and Discontinuation by Study Groups |
Rehabilitation sessions showed no significant changes 12-months after opioid initiation in the percentage of patients using this resource or in the mean number of rehabilitation sessions per patient according to both the period of the study or the type of opioid medications used (Supplementary Figure S2), although a numerical increase in the percentage of rehabilitation users was observed throughout the follow-up of the study.
Sick Leave Days and Productivity Costs
Table 3 shows the distribution of days of sick leave and productivity costs by type of opioid and period of study. During the first year of opioid treatment, 37.9% of patients had ≥1 days of sick leave (6.1% ≥ 6 months), with a mean of 57.1 (SD: 55.3) days/year in patients with sick leave and 21.7 (SD: 43.9) days/year overall. The productivity costs in patients with sick leave and the overall sample amounted to €6837 and €2594, respectively. Patients receiving strong opioids had a longer duration of sick leave and a higher productivity cost per patient than those receiving weak opioids.
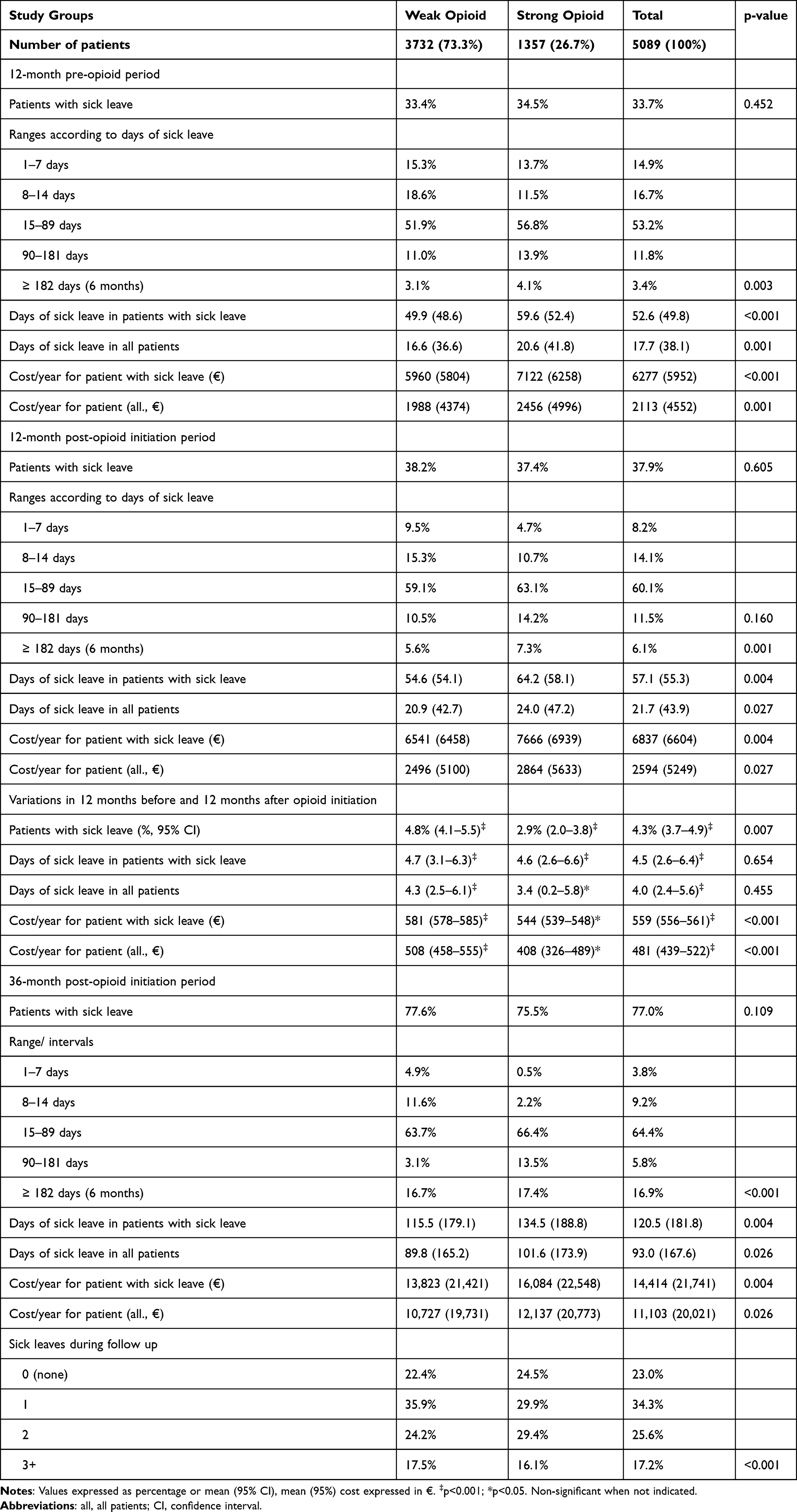 |
Table 3 Days of Sick Leave and Annual Cost Due to Lost Productivity |
Comparing the 12 months before and after the initiation of the opioid treatment, there was an increase of 4.3% of patients with sick leave (p<0.001) and sick leaves were longer, both in patients on sick leave and in the overall sample (4.5 and 4.0 days, respectively [p<0.001]). Therefore, a significant increase in the cost of lost productivity was recorded in the first 12 months of opioid treatment in patients with sick leave and the overall sample (€559 and €481, respectively [p<0.001]). The increase in productivity costs was slightly higher in patients treated with weak opioids (Table 3).
After 36 months, most of the study population (77.0%) had at least one sick leave related with OA chronic pain, with an average of 93 days off work in all actively working patients, being 120.5 days in patients with sick leave (Table 3).
Table 4 shows the cost per patient during the 36-month follow-up period in different scenarios, according to the location of OA, the pain reduction after opioid administration and the concomitant use of NSAIDs. Patients with a relevant reduction in pain (≥50% in NRS) had lower productivity costs in comparison to those who did not have such relief. However, patients treated with strong opioids, regardless of whether they received concomitant NSAIDs, had a higher mean productivity cost.
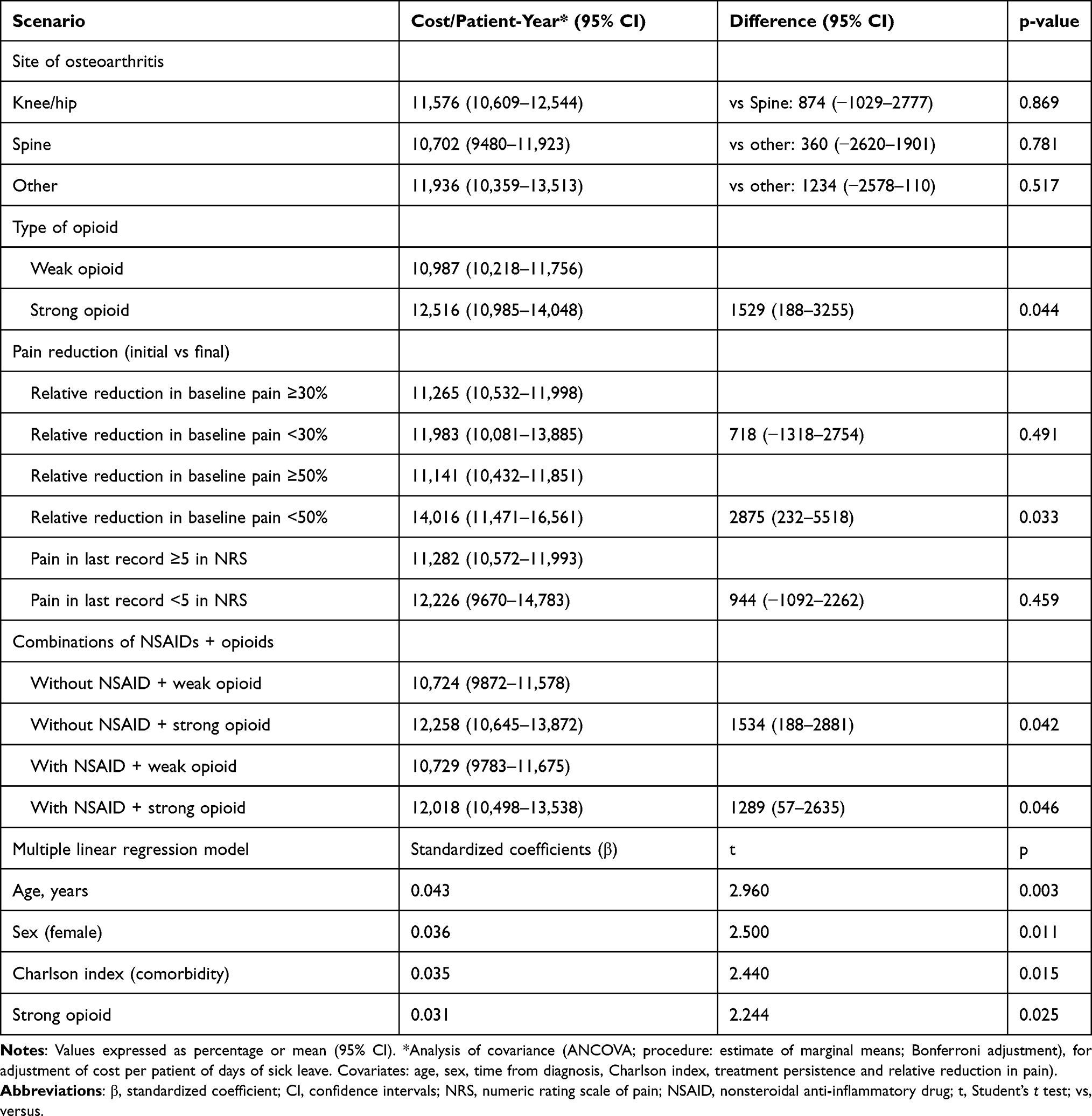 |
Table 4 Mean Adjusted Productivity Costs (€/Patient) During the Follow-Up Period in Different Scenarios |
In the multiple linear regression model, the mean cost of days of sick leave was associated with age (β=0.043, p=0.003), female sex (β=0.036, p=0.011), the severity of comorbidities (β=0.035, p=0.015) and treatment with strong opioids (β=0.031, p=0.025) (Table 4). Figure 2 shows the mean cost per patient of days of sick leave adjusted by covariates during the follow-up period according to sex and age group. The cost of sick leave was significantly higher in women and in individuals aging 55 years or more in comparison with men or younger patients, either receiving weak or strong opioids. In all subgroups, patients treated with strong opioids, regardless of sex or age group, showed higher cost per patient.
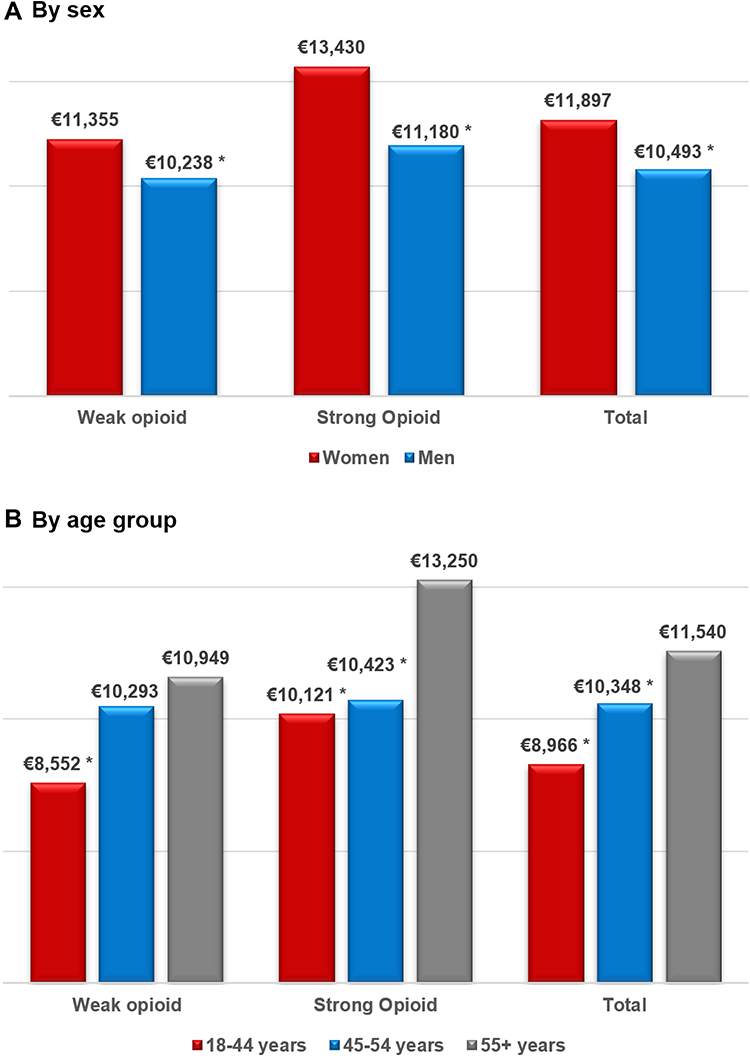 |
Figure 2 Mean cost per patient (€) of sick leaves adjusted by covariates during follow up (36 months) by sex (A) and age group (B). Notes: Values expressed as means. *p <0.05 (reference cohort: females and 55+ years, respectively). Not significant when not indicated. |
Discussion
This study is a secondary analysis of the OPIOIDS study, which was carried out in usual medical practice in Spain.20 Active workers with OA who started opioid treatment for moderate/severe chronic pain showed high productivity losses due to days of temporary occupational disability. In the present research, patients on treatment with opioids showed a low treatment adherence and discontinued the therapy prematurely. Opioids had a modest impact on pain reduction and did not reduce the number of days on sick leave. Furthermore, no significant differences were seen in the use of rehabilitation sessions by workers with sick leave compared to those without, highlighting the need for rehabilitation resources in these patients.29 In addition, older age, female sex, the severity of comorbidities, and the use of strong opioids were associated with greater occupational costs because of a higher number of workdays off due to temporary disability. There is a scarcity of observational studies in real-world conditions, which makes it difficult to compare our results, but it enhances the singularity of the study and may help health authorities and opinion leaders to make healthcare decisions for OA patients. Standard randomized clinical trials should be used with caution to justify political, medico-legal, and economic decisions. On the other hand, outcomes obtained under routine medical care, like the ones included here, could be of help for healthcare decision makers in OA. This is because naturalistic, non-interventional studies may be complementary to evidence-based medicine supported by traditional clinical trial research.30,31 In addition, the large number of patients included, and the monitoring period analyzed, may support the degree of external validity of the results in Spain, and may be considered as a strength of the study.
Our study considered active workers, with a mean age of around 57 years, and 56.6% of them were female, in line with other studies carried out in patients with common musculoskeletal disorders.14,16,17 After 36 months of follow-up, treatment adherence was low (21.0%). Kostev et al found that in a large cohort of patients (n=32,158) with chronic pain,32 adherence to opioids was low; 69% of patients discontinued treatment per year of follow up, similar to our study (64%). In the series analyzed in this research, opioid use did not result in a substantial reduction in pain and had no direct effect in reducing days of sick leave. Our results show a close relationship between pain intensity and days of sick leave. Reducing days of sick leave would require a multidisciplinary approach, including improvements in pain (new treatments), associated comorbidities (obesity, psychological states), lifestyle and/or occupational conditions (occupational risk of certain jobs). We found that, in one-third of patients, there was a significant impact of lost productivity per follow-up year, which increased to 77.0% at the end of the follow up. These results are in line with other reports.14 For each follow-up year, there was an average of 57.1 days of sick leave in patients on sick leave; in 8.2% of patients, the mean was 1–7 days and in 6.1% it was ≥ 6 months while, in all patients, the mean was 21.7 days/year at a cost of €2594/year/patient. At 36 months, 77.0% of patients had taken some days of sick leave, with a mean of 93 lost working days (16.9% of patients had at least 6 months of sick leave), while the average productivity cost amounted to €11,103/patient.
Different designs and time periods and the lack of specific studies difficult the comparison of our results with previous research. Hubertsson et al, analyzed patients aged 16–64 years and found that sick leave was more frequent in the 50–64 years age group and differed between males and females.17 For lower back pain and myalgia, 27% and 26% of all sick leaves were short (8–14 days) and only 11% and 13% were long (≥90 days), respectively. Berger et al found that private sector employees with OA had a mean of 62.9 days of sick leave compared with 36.7 days in a control group without OA.16 Mean total indirect costs were twice as high in patients with OA ($5002 vs $2120). Pekkala et al highlighted the hierarchical differences in occupational classes between different musculoskeletal disorders,33 with large discrepancies in back and shoulder disorders. Rabenda et al34 analyzed a cohort of active workers and underlined the high burden of direct and indirect costs of patients with OA (€15.2 and €23.8, respectively, per active subject per month; equivalent to 0.8 days of sick leave per patient per month), which were predominantly productivity-related costs. Mather et al found that 10.8% of days of sick leave were ≥90 days/year.35 Some reports have concluded that an increase in sick leave days and lost productivity cost as a result of OA is expected in forthcoming years.14 Taking methodological differences into account, our results are broadly in line with these studies. The association with strong opioids may be motivated by a greater degree of severity of OA or associated comorbidities. Some authors studied the association of opioid use and days off work and found a relationship between taking opioids, either weak or strong, and disability to work. Lalic et al36 found that among the 6.9% of patients initiating strong opioids, 12.5% had persistent high sickness absence and disability pension (estimated 320 days/year) before and after opioid initiation and 72.9% had persistent low/minimum sickness absence and disability pension (estimated 30 days/year). Tao et al reported a significant association between the use of opioids and psychotropic medications and workers’ compensation claim costs and prolonged disability. In general, it is assumed that opioid abuse/dependence impose a substantial economic burden for society.37,38
The possible limitations of the study are those inherent to retrospective observational studies (under recording, coding errors, variations in professionals and patients and possible classification bias). In addition, the severity of OA and the interactions among different comorbidities were not considered. Besides, the association between the intensity of chronic pain and days of sick leave was not assessed because these data were not available in the database (occupational risk control, work adaptation, flexibility of schedules, etc.). Finally, other possible limitations were that the study could not obtain the number of joints with OA or whether the origin of OA was traumatic.
Conclusion
In Spain, the management of active workers who started an opioid treatment for moderate to severe chronic OA pain, in conditions of usual clinical practice, implied high costs due to days of sick leave, with a modest reduction in pain. Older age, female sex, the severity of comorbidities and the use of strong opioids were significantly associated with higher productivity costs.
Abbreviations
ACR, American College of Rheumatology; ATC, Anatomical Therapeutic Chemical Classification System; BMI, body mass index; CI, confidence intervals; EMR, electronic medical records; HR, hazard ratio; ICD-10-CM, International Classification of Diseases (10th edition) Clinical Modification; INE, Spanish National Statistics Institute; MPR, medication possession ratio; NRS, numeric rating scale; NSAIDs, nonsteroidal anti-inflammatory drugs; OA, osteoarthritis; OARSI, Osteoarthritis Research Society International; OPIOIDS, Outcomes in Patients usIng Opioids In Painful Disorders in Spain; SD, standard deviation; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The OPIOIDS study was classified by the Spanish Agency for Medicines and Health Products and approved by the Ethics Committee of the Hospital of Terrassa (Barcelona). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines for reporting observational studies were followed.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by Pfizer, SLU.
Disclosure
Antoni Sicras-Mainar is employee of Atrys Health SA and is a paid consultant to Pfizer in connection with this manuscript. Juan Carlos Tornero-Tornero and Francisco Vargas-Negrín declare no competing interests. Isabel Lizarraga is employee of Pfizer, SLU. Aram Sicras-Navarro is employee of Atrys Health SA and is a paid consultant to Pfizer in connection with this manuscript. Javier Rejas-Gutiérrez is employee of Pfizer, SLU. The authors report no other conflicts of interest in this work.
References
1. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2020;72(2):149–162. doi:10.1002/acr.24131
2. Belluzzi E, Stocco E, Pozzuoli A, et al. Contribution of infrapatellar fat pad and synovial membrane to knee osteoarthritis pain. Biomed Res Int. 2019;2019:6390182. doi:10.1155/2019/6390182
3. O’Neill TW, McCabe PS, McBeth J. Update on the epidemiology, risk factors and disease outcomes of osteoarthritis. Best Pract Res Clin Rheumatol. 2018;32(2):312–326. doi:10.1016/j.berh.2018.10.007
4. Blanco FJ, Silva-Díaz M, Quevedo Vila V, et al. Prevalence of symptomatic osteoarthritis in Spain: EPISER2016 study. Reumatol Clínica Engl Ed. 2020:
5. Kroon FPB, Carmona L, Schoones JW, Kloppenburg M. Efficacy and safety of non-pharmacological, pharmacological and surgical treatment for hand osteoarthritis: a systematic literature review informing the 2018 update of the EULAR recommendations for the management of hand osteoarthritis. RMD Open. 2018;4(2):e000734. doi:10.1136/rmdopen-2018-000734
6. Majeed MH, Sherazi SAA, Bacon D, Bajwa ZH. Pharmacological treatment of pain in osteoarthritis: a descriptive review. Curr Rheumatol Rep. 2018;20(12):88. doi:10.1007/s11926-018-0794-5
7. O’Neil CK, Hanlon JT, Marcum ZA. Adverse effects of analgesics commonly used by older adults with osteoarthritis: focus on non-opioid and opioid analgesics. Am J Geriatr Pharmacother. 2012;10(6):331–342. doi:10.1016/j.amjopharm.2012.09.004
8. Yip K, Oettinger J. Why are we still using opioids for osteoarthritis? Int J Clin Pract. 2020;74(1):e13416. doi:10.1111/ijcp.13416
9. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
10. McDonough CM, Jette AM. The contribution of osteoarthritis to functional limitations and disability. Clin Geriatr Med. 2010;26(3):387–399. doi:10.1016/j.cger.2010.04.001
11. Xie F, Kovic B, Jin X, He X, Wang M, Silvestre C. Economic and humanistic burden of osteoarthritis: a systematic review of large sample studies. PharmacoEconomics. 2016;34(11):1087–1100. doi:10.1007/s40273-016-0424-x
12. Hermans J, Koopmanschap MA, Bierma-Zeinstra SMA, et al. Productivity costs and medical costs among working patients with knee osteoarthritis. Arthritis Care Res. 2012;64(6):853–861. doi:10.1002/acr.21617
13. Puig-Junoy J, Ruiz Zamora A. Socio-economic costs of osteoarthritis: a systematic review of cost-of-illness studies. Semin Arthritis Rheum. 2015;44(5):531–541. doi:10.1016/j.semarthrit.2014.10.012
14. Sharif B, Garner R, Hennessy D, Sanmartin C, Flanagan WM, Marshall DA. Productivity costs of work loss associated with osteoarthritis in Canada from 2010 to 2031. Osteoarthritis Cartilage. 2017;25(2):249–258. doi:10.1016/j.joca.2016.09.011
15. Wilkie R, Hay EM, Croft P, Pransky G. Exploring how pain leads to productivity loss in primary care consulters for osteoarthritis: a prospective cohort study. PLoS One. 2015;10(4):e0120042. doi:10.1371/journal.pone.0120042
16. Berger A, Hartrick C, Edelsberg J, Sadosky A, Oster G. Direct and indirect economic costs among private-sector employees with osteoarthritis. J Occup Environ Med. 2011;53(11):1228–1235. doi:10.1097/JOM.0b013e3182337620
17. Hubertsson J, Englund M, Hallgårde U, Lidwall U, Löfvendahl S, Petersson IF. Sick leave patterns in common musculoskeletal disorders–a study of doctor prescribed sick leave. BMC Musculoskelet Disord. 2014;15:176. doi:10.1186/1471-2474-15-176
18. Alamanda VK, Wally MK, Seymour RB, Springer BD, Hsu JR. Prescription reporting with immediate medication utilization mapping group. prevalence of opioid and benzodiazepine prescriptions for osteoarthritis. Arthritis Care Res. 2020;72(8):1081–1086. doi:10.1002/acr.23933
19. Spanish Agency of Medicines and Sanitary Products. Use of opioid medicines in Spain during the period 2010–2019. Available from: https://www.aemps.gob.es/medicamentos-de-uso-humano/observatorio-de-uso-de-medicamentos/utilizacion-de-medicamentos-opioides-en-espana-durante-el-periodo-2010-2018/.
20. Sicras-Mainar A, Tornero-Tornero C, Vargas-Negrín F, Lizarraga I, Rejas-Gutierrez J. Health outcomes and costs in patients with osteoarthritis and chronic pain treated with opioids in Spain: the OPIOIDS real-world study. Ther Adv Musculoskelet Dis. 2020;12:1–18. doi:10.1177/1759720X20942000
21. Big-Pac. European network of centres for pharmacoepidemiology and pharmacovigilance; 2021. Available from: http://www.encepp.eu/encepp/viewResource.htm?id=29236.
22. Sicras-Mainar A, Enriquez JL, Hernández I, Sicras-Navarro A, Aymerich T, Leon M. PMU146 Validation and representativeness of the Spanish BIG-PAC database: integrated computerized medical records for research into epidemiology, medicines and health resource use (real world evidence). Value Health. 2019;22:S734. doi:10.1016/j.jval.2019.09.1764
23. Boletín Oficial del Estado [National Official Bulletin]. Ley Orgánica 3/2018, de 5 de Diciembre, de Protección de Datos Personales y Garantía de Los Derechos Digitales; 2018. Available from: https://www.boe.es/buscar/doc.php?id=BOE-A-2018-16673.
24. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
25. Vicente-Herrero MT, Delgado-Bueno S, Bandrés-Moyá F, et al. Pain assessment: Comparative review of scales and questionnaires. Rev Soc Esp Dolor. 2018;25(4):228–236. doi:10.20986/resed.2018.3632/2017
26. Ministry of Health, Consume and Societal Welfare. International Classification of Diseases (ICD); 2020. Available from: https://eciemaps.mscbs.gob.es/ecieMaps/browser/metabuscador.html.
27. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):73–383. doi:10.1016/0021-9681(87)90171-8
28. National Institute on Statistics. Average employment earnings by age and sex. 2018. https://www.ine.es/dynt3/inebase/index.htm?padre=4563&capsel=4563.
29. Gobelet C, Luthi F, Al-Khodairy AT, Chamberlain MA. Work in inflammatory and degenerative joint diseases. Disabil Rehabil. 2007;29(17):1331–1339. doi:10.1080/09638280701315094
30. Mielke D, Rohde V. Randomized controlled trials-a critical re-appraisal. Neurosurg Rev. 2021;44(4):2085–2089. doi:10.1007/s10143-020-01401-4
31. Bothwell LE, Greene JA, Podolsky SH, Jones DS. Assessing the gold standard — lessons from the history of RCTs. N Engl J Med. 2016;374(22):2175–2181. doi:10.1056/NEJMms1604593
32. Kostev K, Wartenberg F, Richter H, Reinwald M, Heilmaier C. Persistence with opioid treatment in Germany in patients suffering from chronic non-malignant or cancer pain. Curr Med Res Opin. 2015;31(6):1157–1163. doi:10.1185/03007995.2015.1034095
33. Pekkala J, Rahkonen O, Pietiläinen O, Lahelma E, Blomgren J. Sickness absence due to different musculoskeletal diagnoses by occupational class: a register-based study among 1.2 million Finnish employees. Occup Environ Med. 2018;75(4):296–302. doi:10.1136/oemed-2017-104571
34. Rabenda V, Manette C, Lemmens R, Mariani A-M, Struvay N, Reginster J-Y. Direct and indirect costs attributable to osteoarthritis in active subjects. J Rheumatol. 2006;33(6):1152–1158.
35. Mather L, Ropponen A, Mittendorfer-Rutz E, Narusyte J, Svedberg P. Health, work and demographic factors associated with a lower risk of work disability and unemployment in employees with lower back, neck and shoulder pain. BMC Musculoskelet Disord. 2019;20:622. doi:10.1186/s12891-019-2999-9
36. Lalic S, Bell JS, Gyllensten H, et al. Trajectories of sickness absence and disability pension before and after opioid initiation for noncancer pain: a 10-year population-based study. Pain. 2019;160(5):1224–1233. doi:10.1097/j.pain.0000000000001500
37. Tao XG, Lavin RA, Yuspeh L, Weaver VM, Bernacki EJ. The association of the use of opioid and psychotropic medications with workers’ compensation claim costs and lost work time. J Occup Environ Med. 2015;57(2):196–201. doi:10.1097/JOM.0000000000000333
38. Rice JB, Kirson NY, Shei A, et al. Estimating the costs of opioid abuse and dependence from an employer perspective: a retrospective analysis using administrative claims data. Appl Health Econ Health Policy. 2014;12(4):435–436. doi:10.1007/s40258-014-0102-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.