Back to Journals » Psychology Research and Behavior Management » Volume 16
Short Video-Based Mental Health Intervention for Depressive Symptoms in Junior High School Students: A Cluster Randomized Controlled Trial
Authors Yang Y ![]() , Wang H, Sha W, Guo X, Deng W, Wang J, Fu C
, Wang H, Sha W, Guo X, Deng W, Wang J, Fu C ![]()
Received 2 August 2023
Accepted for publication 6 October 2023
Published 16 October 2023 Volume 2023:16 Pages 4169—4181
DOI https://doi.org/10.2147/PRBM.S433467
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Yuting Yang,1,* Hao Wang,1,* Wen Sha,2 Xiaoqin Guo,3 Wei Deng,1 Jingyi Wang,1 Chaowei Fu1
1School of Public Health; NHC Key Laboratory of Health Technology Assessment, Fudan University, Shanghai, People’s Republic of China; 2Shanghai Municipal Center for Health Promotion, Shanghai, People’s Republic of China; 3Songjiang District Center for Health Promotion, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chaowei Fu; Jingyi Wang, School of Public Health; NHC Key Laboratory of Health Technology Assessment, Fudan University, 446-2 Zhaojiabang Road, Shanghai, 200032, People’s Republic of China, Tel/Fax +86 21 3356 3933 ; +86 21 6416 9553, Email [email protected]; [email protected]
Purpose: Digital interventions for adolescent mental health are emerging in high-income countries, but have faced challenges and are scarce in China. This study investigated the effect of a short video-based mental health intervention on depressive symptoms in Chinese adolescents.
Methods: A three-arm cluster randomized controlled trial was conducted in four junior high schools in Shanghai from December 2020 to December 2021 with the measurement at baseline, 6 months after study entry, and 12 months. Outcomes were collected by self-completed questionnaires administered by teachers masked to allocation. The primary outcome was depressive symptoms assessed by the Depression Self-Rating Scale for Children (DSRSC). Mixed effects models were used to compare psychologist-led intervention (n=428 students) and teacher-led intervention (n=385) including six short video-based sessions to usual school provision (n=751).
Results: Using intention-to-treat analyses, psychologist-led intervention showed more reduction in depressive symptoms compared to usual school provision at 6 months (coefficient − 1.00, 95% CI − 1.94 to − 0.05), but not at 12 months. Using per-protocol analyses among participants who watched at least three video episodes, both psychologist-led (− 1.14, − 2.20 to − 0.09) and teacher-led intervention (− 1.23, − 2.45 to − 0.02) reduced depressive symptoms compared to usual school provision at 6 months, and the effect of teacher-led intervention persisted at 12 months (− 1.58, − 3.13 to − 0.03). Further exploration found that compared with urban students, the between-group differences for depressive symptoms in rural students were more significant (p< 0.05 for interaction) and the effects were maintained at 12 months.
Conclusion: The short video-based mental health intervention showed potential to reduce depressive symptoms among Chinese adolescents, and the effects were more significant if the minimum video viewing frequency was reached.
Keywords: short video-based intervention, adolescents, mental health, depressive symptoms, randomized controlled trial
Introduction
Since the beginning of the 21st century, adolescent mental health problems have been increasing.1–3 About 10 to 20% of children and adolescents worldwide have mental health problems.4 Before the COVID-19 pandemic, the prevalence of depressive symptoms was 15.4% in Chinese children and adolescents and 16.2% in junior high school students.5 The pandemic has further exacerbated this already challenging issue as the prevalence of depressive symptoms has increased in Chinese children.6,7 The distressing emotional problems that adolescents fail to address in time not only affect their current lives but also increase the risk of other psychiatric disorders in adolescence and adulthood.8–10 Long-term emotional problems also bring a huge burden to economic and societal costs.11,12
With more attention paid to adolescent mental health, there is growing evidence that symptoms can be reduced through public health interventions,2 especially those proactive preventive approaches with schools as a natural location to deliver such interventions.13,14 Traditional interventions are generally delivered by clinical professionals using materials that are often not straightforward for students to understand by themselves. The extreme scarcity of psychological resources in China makes it difficult to extend such interventions to a large number of schools.15 Although some Chinese schools have regular psychology lessons and psychological counselling offices staffed with full-time or part-time teachers, there are large discrepancies in terms of the provision of school-based mental health education and services between urban and rural areas and east and west of the country.16 Moreover, scholars are paying attention to the accessibility and scalability of prevention programs,17 and some have found that Internet-based depression prevention interventions are more standardized and cost-effective than face-to-face interventions.18
As a result, interventions based on digital technology gradually gained in popularity, and the number of practical applications began to surge.19,20 For example, an Australian study of SPARX-R, using online cognitive behavioral gamification intervention, showed that it was effective in reducing depressive symptoms in adolescents.21 A randomized controlled trial in America demonstrated the preventive effect of an Internet-based intervention, CATCH-IT, on adolescent depression.22 However, the results of digital interventions are inconsistent, and the effects were not significant in some other studies.23,24 In addition, a systematic review of interventions for adolescent mental health revealed that the existing evidence is mainly from high-income countries and that rigorous, high-quality evidence is urgently needed especially from low- and middle-income countries.25
Video is considered to be a cost-effective and easy to use tool which may create emotional response and enhance empathy alongside provision of information.26 Short videos (ie, ≤ 10 minutes) are more preferred by young people as they are engaging, flexible and convenient and can reduce extraneous cognitive load compared to longer videos.27 The positive role of short video in changing health-related outcomes among young people has been documented in some previous studies.28,29 However, evidence about effects of short video interventions on adolescent mental health is scarce. Given the increasing popularity of short videos in adolescents30 and their advantages of low cost, accessibility and scalability,28,31 it is of great academic and practical significance to design a short video-based intervention that can be widely accepted by Chinese adolescents and conduct a high-quality randomized controlled trial to evaluate its effectiveness and method of delivery. Therefore, our study conducted a three-arm randomized controlled trial among junior high school students in Shanghai using a short video-based psychoeducational intervention. We assessed the effectiveness of the intervention universally delivered by school psychologists and class teachers on the students’ mental health. Furthermore, we explored the difference in intervention effectiveness between students in urban and rural areas and the influence of the number of videos watched on the intervention effectiveness.
The primary hypotheses were that psychologist-led intervention and teacher-led intervention would demonstrate greater reductions in depressive symptoms from baseline to 6-month follow-up compared to usual school provision and that these effects would be maintained at 12-month follow-up. Secondary hypotheses were that being in the intervention groups rather than the control group would be associated with enhanced perceived social support and better health-related quality of life at 6-month and 12-month follow-ups.
Materials and Methods
Study Design and Participants
We did this three-arm cluster randomized controlled trial (the Chinese Clinical Trial Registry [ChiCTR2100041956]) from December 2020 to December 2021 with the measurement at baseline, 6 months after study entry (end of intervention), and 12 months (see Supplement Figure 1). Schools were used as the unit of allocation and individual participants as the unit of analysis. Five junior high schools in Songjiang District, Shanghai were invited to participate and four of them agreed. Three to four classes were randomly selected from each grade (grades 6 to 8) in participating schools to meet the need of sample size. To be eligible for the study, participants need to meet the following criteria: (1) be students in participating classes; (2) both children and their parents agreed to participate and signed an informed consent form; and (3) without long-term sickness which would prevent them from attending school.
Randomization and Masking
Once all schools had been enrolled, a computer-generated list of random numbers was used to allocate the schools to one of the study arms. Schools (1: 1: 2) were randomly allocated to psychologist-led intervention, teacher-led intervention, or usual school provision. Unequal allocation was used to reduce financial costs as the intervention was more expensive than the control, which is a common situation where unequal randomization can be useful.32 Randomization was undertaken at school and not the class level to avoid possible contamination within schools. The sample size remained roughly the same at each school for each grade level. Students were not masked to treatment allocation. Outcomes were collected by self-completed online questionnaires and administered by teachers who were not informed of participants’ treatment allocation. A statistician who helped with data analysis was also masked to the allocation.
Intervention and Procedure
The intervention was based on the Authier psychoeducation model33 and included six short videos and following discussion. The short videos were jointly produced by the School of Public Health of Fudan University and the Shanghai Municipal Center for Health Promotion. They involved techniques derived from classic psychoeducation,33 interpersonal psychotherapy34 and cognitive behavioral therapy.35 The videos focused on six themes of emotional and relationship problems frequently encountered by adolescents, including depression, stress, emotion regulation and self-harm, peer relationship problems, parent-child communication, and internet addiction. They presented causes of the problem, adverse impact on health and functioning, coping strategies, communication skills, problem-solving skills and help-seeking resources. Each episode is about 10 minutes long and is presented in the form of melodrama and expert explanation. The content of the videos was based on literature, expert consultations and interviews with junior high school students. Before reaching out to experts, the research team had collected, sorted out and initially analyzed the literature related to this study. Child and adolescent psychiatrists from Shanghai Mental Health Center, junior high school psychologists, public health experts, and the video director from Shanghai Municipal Center for Health Promotion participated in several meetings to decide and check the content of the intervention videos. Interviews with adolescents were used to find out the influential factors of their psychological health and their expectations and preferences for the intervention. The short videos aimed to help children develop emotional awareness and regulation strategies, enhance positive interactions, and learn more functional ways of thinking and problem-solving skills to cope with situations that may provoke emotional problems.
In the psychologist-led group, each session was led by a school psychologist who had professional psychology background and experience of working with children. The students in each participating class watched the videos together during psychology lessons followed by discussions and activities related to the theme of each video. The videos were uploaded to Chaoxing platform (https://mooc1-gray.chaoxing.com/course/220663028.html). Each participant was given an account and a password which allowed them to log in and watch the videos multiple times. Students were strongly encouraged to watch the videos again at home and the videos were also recommended to their parents. In the teacher-led group, the procedures were similar to psychologist-led intervention, but sessions were led by class teachers and the videos were played at weekly class meetings. The class teachers were individuals who were in charge of the class and familiar with each student in the class but did not have psychology background. Interventions in both groups were implemented from March to May 2021 and were delivered to the entire classes. The frequency of intervention was determined by the schools’ curriculum, with an average of 30 to 45 minutes per session and once every 1 to 2 weeks. Each session included one episode of the videos followed by discussion. School psychologists and class teachers were given a session plan which specified key learning points, discussion outlines, and core activities for each session. The implementation in both intervention groups was supported and supervised by two trained facilitators.
In the usual school provision group, existing psychological supporting measures, such as psychology lectures and psychology class meetings, were maintained. They were planned and provided solely by the teachers and did not include the short videos or any other external input from the research team.
Measures
Outcomes
Student outcomes were collected through self-completed electronic questionnaires on Wenjuanxing platform at baseline, 6 months after study entry (end of intervention), and 12 months.
The primary outcome was depressive symptoms assessed by total score on the Depression Self-Rating Scale for Children (DSRSC),36,37 an 18-item measure of depressive symptoms in children aged 8 to 14 years. The possible total score ranges from 0 to 36, with higher scores indicate higher levels of depressive symptoms. The Chinese version of the scale had adequate content validity and criterion validity, and showed good internal consistency (Cronbach’s alpha 0.73).36
Secondary outcomes were social support as assessed by the Multidimensional Scale of Perceived Social Support (MSPSS),38,39 a 12-item measure of perceived social support from family, friends, and significant other (scores of the scale range from 12 to 84, with higher scores indicating better social support); health-related quality of life as assessed by the EuroQol five-dimension questionnaire-young (EQ-5D-Y),40,41 a five-item measure of health status in children (summary index of the scale range from 0 to 1, higher scores indicate better quality of life).
Basic Characteristics
The basic characteristics included sex, grade, only child or non-only child family, household registration in an urban or rural area, family economic status, whether having difficulty in studying, fathers’ education, and mothers’ education.
Ethical Considerations
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the School of Public Health, Fudan University (IRB#2020040817). Moreover, before commencing, the trail was registered with ClinicalTrials.gov (ChiCTR2100041956).
Statistical Analysis
We powered the study to detect a small difference of 1.5 points in mean DSRSC total scores between intervention and control groups. The standard deviations of the DSRSC change scores were assumed to be equal in each group and were estimated to be 5 from previous research.42 Based on a standard deviation of 5 points, an intracluster correlation coefficient of 0.03,43,44 40 students per class, 80% power, 5% significance, and 1:1:2 allocation, we required a sample size of 320 in psychologist-led intervention, 320 in teacher-led intervention, and 600 in usual school provision (a total of 1240 assenting participants). A standardized treatment effect size of 0.3 is equivalent to an estimated difference on the DSRSC of 1.5 points based on an SD of 5.
We used descriptive statistics to assess the balance between the trial groups at baseline. The primary outcome was assessed by intention-to-treat analysis with the intervention groups including all participants as originally allocated after randomization. Given the hierarchical nature of the data, multivariable mixed effects models were used to compare DSRSC total score at 6 and 12 months for psychologist-led intervention and teacher-led intervention with usual school provision, with adjustment for baseline DSRSC score, sex, grade, only-child family, household registration, family economic status, whether having difficulty in studying, fathers’ education, and mothers’ education. The models examined fixed effects for randomization group and baseline covariates, while random intercepts were used to account for clustering by class and baseline DSRSC score was allowed to vary randomly (random slopes). These mixed effects analyses which accounted for clustering by class were repeated for secondary outcomes, controlling for the baseline value of the outcome and the other covariates. There were no missing data for participants who completed the questionnaires as the Wenjuanxing platform automatically checked for missing values and reminded the participants before submission.
We did sensitivity analyses to compare the primary and secondary outcomes between randomization groups using per-protocol analysis. This approach included only those participants in the intervention groups who watched at least three episodes of the videos both at school and at home to investigate whether the intervention would have effect if the minimum video viewing frequency was reached.
In further analysis of the DSRSC, we tested interaction terms in the regression models between the randomized group and the baseline variables in Table 1. Associations between the randomized group and DSRSC score at 6 and 12 months differed by household registration when tested as an interaction (p < 0.05), and thus subgroup analyses were conducted for participants from urban and rural areas separately.
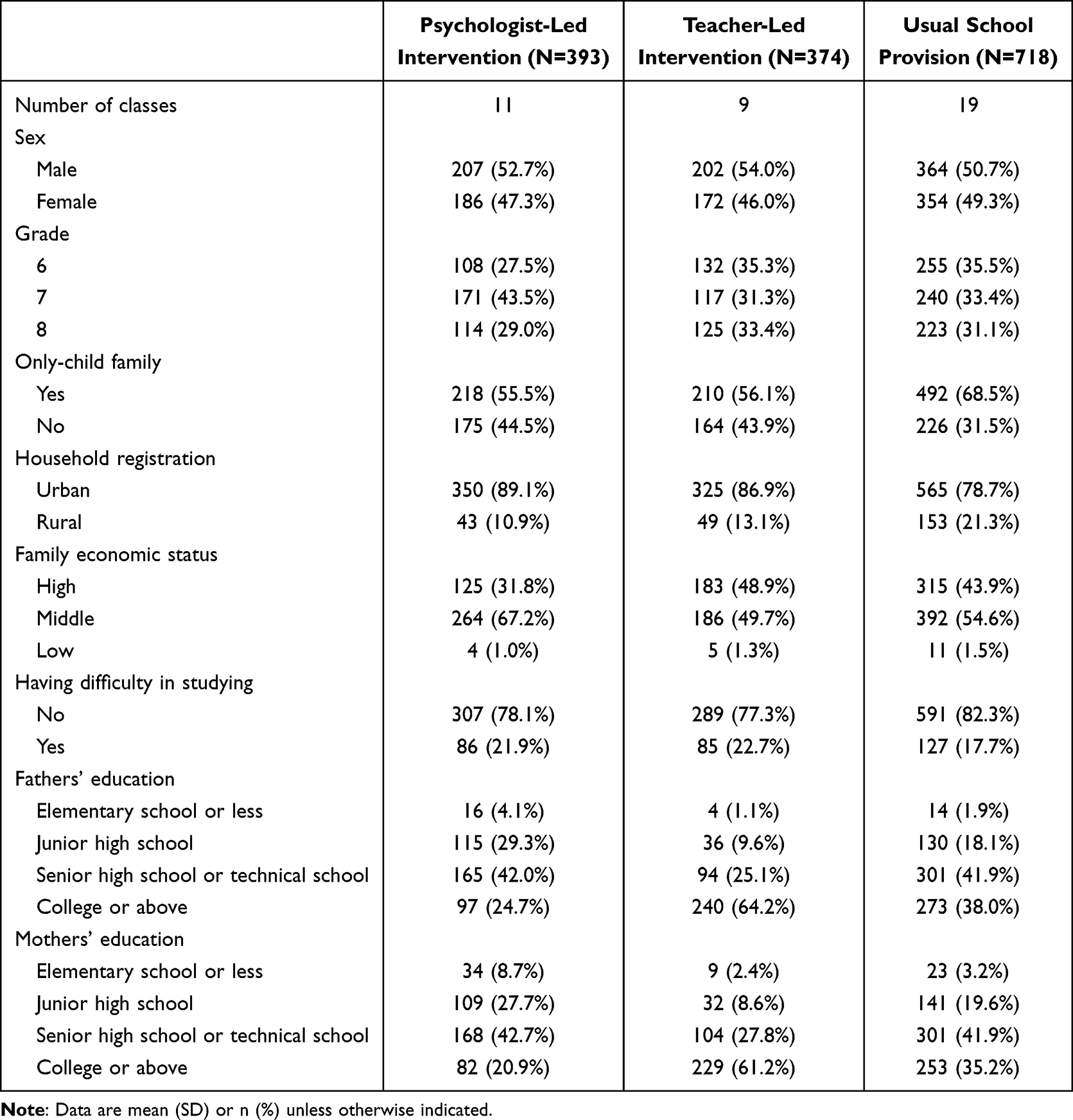 |
Table 1 Baseline Characteristics of Participants |
In addition, multivariable mixed effects models were used to analyze the effect of intervention process variables (including the number of videos watched by students at school and at home, the number of videos watched by parents, and whether students communicated with parents about the videos) on the primary outcome (DSRSC at 6-month follow-up), with adjustment for baseline DSRSC score and the other relevant baseline covariates (sex, grade, only-child family, household registration, family economic status, study hours per day, relationships with mother and father).
We conducted all analyses using Stata 16.0 (Stata Corp LP, College Station, TX) with the level of significance determined at 0.05 p-value.
Results
Figure 1 demonstrates the recruitment and retention of participants during the course of the study. Between December 2020 and March 2021, four schools were enrolled and one declined to participate. The four schools which consented to participate were randomly assigned: one (n=428 students) to psychologist-led intervention, one (n=385) to teacher-led intervention, and two (n=751) to usual school provision.
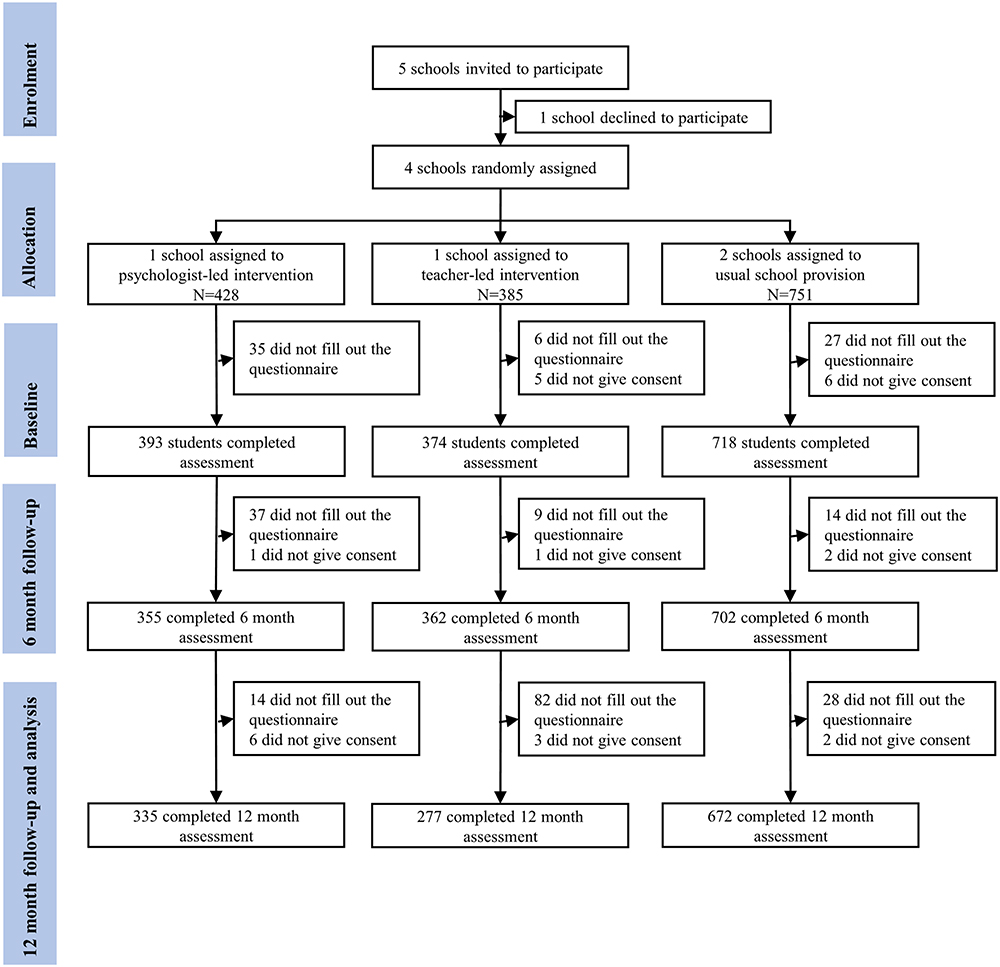 |
Figure 1 CONSORT diagram of participant flow through the trial. |
Of the 1564 eligible participants, 1553 (99%) consented to participate in the study, of whom 1485 (96%) completed baseline assessments. The baseline characteristics of participants are presented in Table 1. More parents of students in teacher-led intervention had a college or above education degree than in the other two groups, otherwise, the groups were well-balanced. We collected primary outcome data at 6 months from 1419 (96%) of the 1485 students who completed baseline assessments (355 [90%] in psychologist-led intervention, 362 [97%] in teacher-led intervention, and 702 [98%] in usual school provision) and at 12 months from 1284 (86%) of 1485 baseline participants (335 [85%], 277 [74%] and 672 [94%], respectively).
Analysis of mean DSRSC at 6 months showed an adjusted difference between psychologist-led intervention and usual school provision (coefficient −1.00, 95% CI −1.94 to −0.05; p=0.040), but not between teacher-led intervention and usual school provision (−0.44, −1.43 to 0.54; p=0.376). For the primary outcome at 12 months, the difference favored teacher-led intervention but it was marginally significant (−1.06, −2.31 to 0.19; p=0.097). Analysis of other secondary outcomes identified no differences at 6 and 12 months for psychologist-led intervention and teacher-led intervention compared with usual school provision (Table 2).
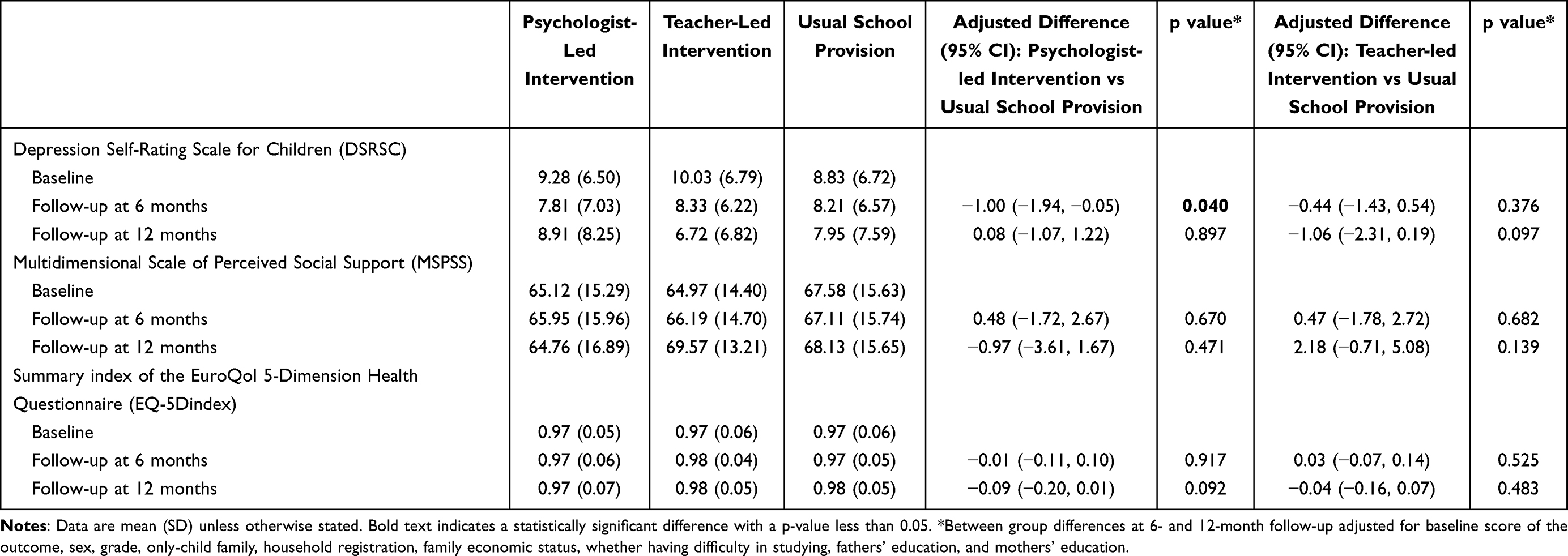 |
Table 2 Analysis of Primary (DSRSC) and Secondary Outcomes for All Students at 6- and 12-Months Follow-Up for Psychologist-Led Intervention and Teacher-Led Intervention Vs Usual School Provision |
In sensitivity analyses among participants in the intervention groups who watched at least three episodes of the videos both at school and at home, we recorded significant differences in adjusted mean DSRSC at 6 months for psychologist-led (−1.14, −2.20 to −0.09; p=0.033) and teacher-led intervention (−1.23, −2.45 to −0.02; p=0.047) compared with usual school provision. The effect of teacher-led intervention persisted at 12 months (−1.58, −3.13 to −0.03; p=0.046). There was little evidence of any effect for secondary outcomes (Table 3).
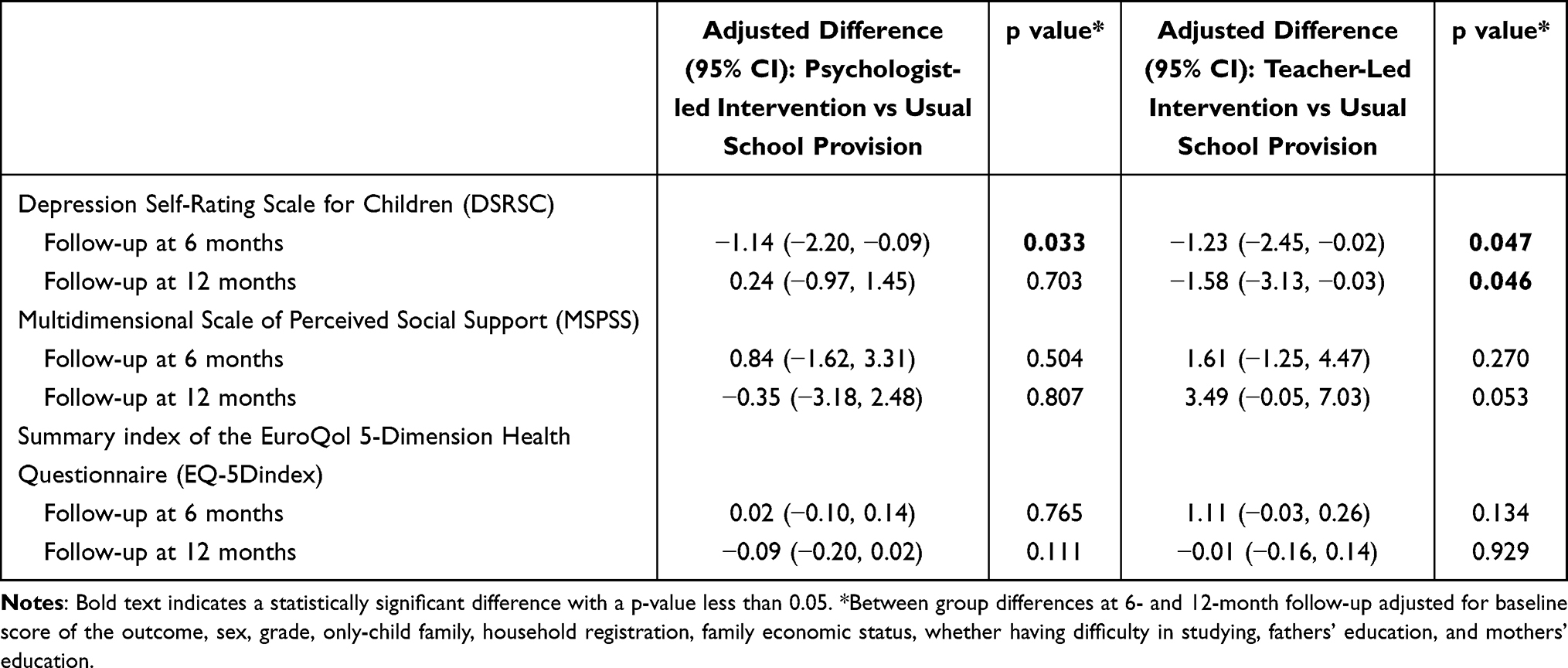 |
Table 3 Sensitivity Analyses: Analysis of Primary (DSRSC) and Secondary Outcomes for Students Who Watched at Least Three Episodes of the Videos Both at School and Home at 6- and 12-Month Follow-Up for Psychologist-Led Intervention and Teacher-Led Intervention Vs Usual School Provision |
In subgroup analyses (Table 4) among students with household registration in urban area and rural area, we found between-group differences in mean DSRSC at 6 months for the rural group. Adjusted differences showed an effect for psychologist-led intervention versus usual school provision (−4.16, −6.28 to −2.04; p<0.001) and teacher-led intervention versus usual school provision (−2.13, −4.04 to −0.22; p=0.028). The effect for psychologist-led intervention was maintained at 12-month follow-up (−2.78, −5.47 to −0.09; p=0.043), but not for teacher-led intervention (−2.09, −4.78 to 0.60; p=0.128). In the rural household registration group, the standardized effect size of psychologist-led intervention compared with usual school provision at 6 months (Cohen’s d corrected for uneven groups=−0.53) was medium, while the other between-group differences were small to medium (Cohen’s d −0.25 to −0.47). In the urban household registration group, we recorded within-group reductions for mean DSRSC at 6 and 12 months but no effects between groups.
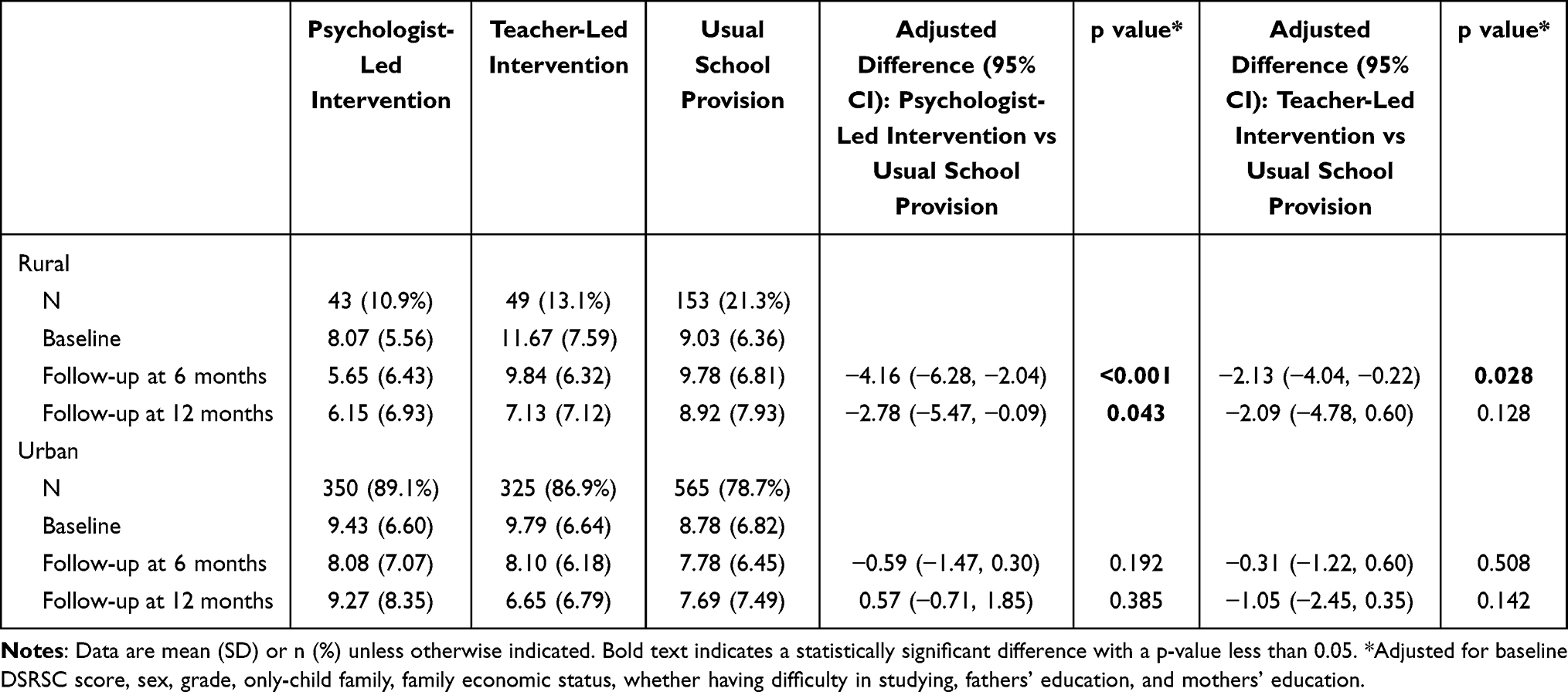 |
Table 4 Subgroup Analysis of Primary Outcome (DSRSC) for Students with Rural and Urban Household Registration |
All six intervention sessions were delivered to classes assigned to both the psychologist-led and teacher-led conditions. Most (n=675, 94%) of 717 participants perceived the intervention as helpful, of whom around 80% reported effects on improving their psychological health knowledge, strategies to cope with emotional problems, and confidence in addressing adversities. Over 50% reported that the intervention improved their relationships with parents, classmates, friends, and teachers, increased their parents’ psychological health knowledge, and helped their parents understand them. Regarding uptake of the intervention, 430 (60%) of 717 participants attended all six sessions offered. Majority (n=339, 95%) of 355 participants in psychologist-led intervention attended at least three sessions at school and 286 (81%) watched at least three episodes of the videos at home, compared with 72% (259 of 362 at school) and 51% (184 of 362 at home) of teacher-led group. Parents of students in psychologist-led group watched more episodes (mean [SD] 4.28 [2.45] vs 2.53 [2.52]) and more students reported communicating with their parents about the videos (71% vs 44%) than in teacher-led group. In addition, this study found that more episodes of videos watched by students at school and at home, more episodes watched by parents, and the fact that students communicated with their parents about the videos were all associated with a larger reduction in DSRSC scores at 6 months in both psychologist-led and teacher-led groups (Supplement Table 1).
Discussion
This is a randomized controlled trial in China, comparing a universally provided short video-based mental health intervention for adolescents led by school psychologists and class teachers with usual school provisions. The effect of primary outcome at 6 months suggested that the intervention reduced depressive symptoms, partially confirming the primary hypotheses, although the confidence intervals were wide for teacher-led intervention. This trial addresses the need for evidence on how to reduce depressive symptoms in adolescents and provides promising evidence for the effectiveness of short video-based intervention in Chinese schools. If our finding is replicated in routine settings, adolescents would have greater opportunities for emotional well-being, and the burden on school psychological services might be reduced.
We noted that the improvement of depressive symptoms was not maintained at 12 months. Consistent with the findings of a meta-analysis, online interventions to prevent depression can reduce depressive symptoms in the short and medium term, but not in the long term.45 Future research needs to further examine the factors that influence the effectiveness of digital interventions and explore how to maintain the effects over a longer period.
We found that psychologist-led intervention was effective in reducing depressive symptoms at 6 months, but teacher-led intervention had smaller effect sizes and wider confidence intervals, suggesting that the intervention fidelity might be better in the psychologist-led group. Our results are consistent with previous research that found psychologist-led intervention to be superior to teacher-led intervention.43,46,47 This may be due to differences in expertise, attitude, and practical skills of the intervention facilitators. Although class teachers are more competent in some areas such as classroom management, they have less psychological knowledge and more routine teaching tasks than school psychologists, which might have compromised intervention delivery.43 The percentages of students who watched at least three episodes of the videos at school (72%) and at home (51%) in the teacher-led group were lower than those in the psychologist-led group (95%; 81%). In sensitivity analyses including only participants who watched at least three episodes both at school and at home, we found significant differences in depressive symptoms at 6 months for teacher-led intervention compared with usual school provision, and the effect persisted at 12 months. Class teachers have opportunities to intensively consolidate intervention skills through their daily contact with students. If facilitators’ enthusiasm, confidence, and ability to motivate students could be enhanced, teacher-led intervention might be as effective as psychologist-led intervention. Therefore, additional training and supervision for intervention facilitators should be considered in future research to increase relevant knowledge and skills.48,49
We recorded no differences between groups for any secondary outcomes, suggesting that the intervention effects were specific to depressive symptoms. The short videos were specifically designed to improve knowledge and develop coping strategies known to reduce emotional problems. Therefore, the effect that we identified is consistent with the trial focus. However, additional measures of potential mechanisms, such as confidence in addressing adversities, might be more informative.
Compared with urban students, the between-group differences in depressive symptoms among rural students were more significant. In the rural group, there were small to medium effects of both psychologist-led intervention (where effects were maintained at 12-month follow-up) and teacher-led intervention compared with usual school provision. Some studies suggest that Internet-based mental health interventions, such as computerized cognitive behavioral therapy, can be used effectively to improve depressive symptoms and may be particularly useful in rural settings.50 People living in rural communities have greater difficulty accessing mental health services and factors influencing depressive symptoms differ between urban and rural adolescents.51–53 Our intervention might have addressed factors that are particularly important to rural students. Therefore, it is necessary to report differential effects of mental health interventions for socioeconomic status and geographic settings as the impact might vary according to various contextual factors. Future interventions should take into account contextual differences and develop tailored strategies for various subgroups to optimize their effectiveness. In addition, in future studies, it would be interesting to assess potential variations in outcomes between different interventions among both genders.
Regarding the intervention process, we found that the number of videos watched by students and parents, and whether students communicated with parents about the videos were significantly associated with the reduction in depressive symptoms. Family is a very important factor affecting the mental health of junior high school students.54,55 Studies have shown that parents’ attitudes and upbringing toward their children play a major role in influencing adolescents’ emotional status, and good parent-child relationships have a positive impact on children’s mental health.56,57 Therefore, how to encourage parents to watch videos and interact with their children should be considered in the future.
One strength of this trial was that the intervention mainly took place in the school setting, thus increasing ecological validity. Although the intervention facilitators received some training and supervision, participants were not given any direct guidance by the research team during treatment or when responding to assessments. The intervention was designed to be broadly applicable to Chinese adolescents, and the short videos uploaded to the Chaoxing platform are free and easily accessible to adolescents, parents and teachers, thereby increasing generalizability. Additional strengths were that recruitment and retention were high and the design and procedures were robust with oversight from a registered clinical trials unit.
This study also had several limitations. First, the primary outcomes were based on self-report measures rather than diagnostic interviews. It is unclear whether the reduction in depressive symptoms was indicative of changes in diagnostic status. Additionally, the study did not collect the information about current diagnosis of depression or use of medication with antidepressants or mood stabilizers. Future studies could explore the impact of the intervention on different levels of depressive symptoms. Second, our study only included schools from one district in Shanghai. Whether consistent results would be obtained with adolescents in other areas is unclear. Third, although the psychologist-led and teacher-led intervention facilitators had the same intervention material, we did not directly assess how the intervention was delivered. The differences between these groups might be caused by different intervention fidelity and different attitudes and ability of the facilitators. Fourth, there are potentially unmeasured differences in school characteristics, although individual factors were controlled for. Future studies should enrol more intervention sites to reduce the possibility that school-level factors colinear with the intervention arm. Finally, although the uptake of the intervention was fairly good, the number of episodes of videos watched by students and parents at home needs to be further improved.
Conclusion
In conclusion, the short video-based mental health intervention for junior high school students did reduce depressive symptoms at 6 months. The findings suggest that video viewing frequency is important and the effects were more significant if at least three episodes of the videos were watched both at school and at home. The finding that rural adolescents benefited from the intervention supports its application in schools and areas short of psychological services. This study should be replicated in different contexts to confirm our findings. Further research is also needed to explore the potential mediators and moderators of the intervention, assess cost-effectiveness, and investigate participant and facilitator experiences.
Data Sharing Statement
The database of the current study is not publicly available.
Informed Consent
All participants and parents or legal guardians of the children participating in our study provided informed consent prior to study participation. Informed consent procedures were used to collect all study data.
Funding
This work was supported by the China Medical Board (grant number #22-472), Shanghai Health Commission (grant number 202240115), and Shanghai Pujiang Program (grant number 2020PJC005).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bor W, Dean AJ, Najman J, Hayatbakhsh R. Are child and adolescent mental health problems increasing in the 21st century? A systematic review. Aust N Z J Psychiatry. 2014;48(7):606–616. doi:10.1177/0004867414533834
2. Collishaw S. Annual research review: secular trends in child and adolescent mental health. J Child Psychol Psychiatry. 2015;56(3):370–393. doi:10.1111/jcpp.12372
3. Patalay P, Gage SH. Changes in millennial adolescent mental health and health-related behaviours over 10 years: a population cohort comparison study. Int J Epidemiol. 2019;48(5):1650–1664. doi:10.1093/ije/dyz006
4. Kieling C, Baker-Henningham H, Belfer M, et al. Child and adolescent mental health worldwide: evidence for action. Lancet. 2011;378(9801):1515–1525. doi:10.1016/S0140-6736(11)60827-1
5. Li J, Chen X, Zhao C, Hong Y. Prevalence of depression in Chinese children and adolescents: a Meta-analysis. Chin J Child Health Care. 2016;24(03):295–298.
6. Xie X, Xue Q, Zhou Y, et al. Mental health status among children in home confinement during the coronavirus disease 2019 outbreak in Hubei Province, China. JAMA Pediatr. 2020;174(9):898–900. doi:10.1001/jamapediatrics.2020.1619
7. Zhou SJ, Zhang LG, Wang LL, et al. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur Child Adolesc Psychiatry. 2020;29(6):749–758. doi:10.1007/s00787-020-01541-4
8. Kim-Cohen J, Caspi A, Moffitt TE, Harrington H, Milne BJ, Poulton R. Prior juvenile diagnoses in adults with mental disorder: developmental follow-back of a prospective-longitudinal cohort. Arch Gen Psychiatry. 2003;60(7):709–717. doi:10.1001/archpsyc.60.7.709
9. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62(6):593–602. doi:10.1001/archpsyc.62.6.593
10. Colman I, Murray J, Abbott RA, et al. Outcomes of conduct problems in adolescence: 40 year follow-up of national cohort. BMJ. 2009;338:a2981. doi:10.1136/bmj.a2981
11. Smith JP, Smith GC. Long-term economic costs of psychological problems during childhood. Soc Sci Med. 2010;71(1):110–115. doi:10.1016/j.socscimed.2010.02.046
12. Hu TW, He Y, Zhang M, Chen N. Economic costs of depression in China. Soc Psychiatry Psychiatr Epidemiol. 2007;42(2):110–116. doi:10.1007/s00127-006-0151-2
13. Davies SC, Lemer C, Strelitz J, Weil L. Our children deserve better: prevention pays. Lancet. 2013;382(9902):1383–1384. doi:10.1016/s0140-6736(13)62004-8
14. Shepherd J, Pickett K, Dewhirst S, et al. Training teachers for the public health workforce: systematic mapping and synthesis of effectiveness and processes. Lancet. 2013;382:S90. doi:10.1016/S0140-6736(13)62515-5
15. Xiang YT, Ng CH, Yu X, Wang G. Rethinking progress and challenges of mental health care in China. World Psychiatry. 2018;17(2):231–232. doi:10.1002/wps.20500
16. Zhang H, Du Y. Chinese school curricula should include mental health education. Lancet Psychiatry. 2018;5(8):e18. doi:10.1016/s2215-0366(18)30217-7
17. McGorry PD, Mei C. Early intervention in youth mental health: progress and future directions. Evid Based Ment Health. 2018;21(4):182–184. doi:10.1136/ebmental-2018-300060
18. Andersson G, Titov N. Advantages and limitations of Internet-based interventions for common mental disorders. World Psychiatry. 2014;13(1):4–11. doi:10.1002/wps.20083
19. Naslund JA, Aschbrenner KA, Araya R, et al. Digital technology for treating and preventing mental disorders in low-income and middle-income countries: a narrative review of the literature. Lancet Psychiatry. 2017;4(6):486–500. doi:10.1016/S2215-0366(17)30096-2
20. Uhlhaas P, Torous J. Digital tools for youth mental health. NPJ Digit Med. 2019;2:104. doi:10.1038/s41746-019-0181-2
21. Perry Y, Werner-Seidler A, Calear A, et al. Preventing depression in final year secondary students: school-based randomized controlled trial. J Med Internet Res. 2017;19(11):e369. doi:10.2196/jmir.8241
22. Van Voorhees B, Gladstone TRG, Sobowale K, et al. 24-month outcomes of primary care web-based depression prevention intervention in adolescents: randomized clinical trial. J Med Internet Res. 2020;22(10):e16802. doi:10.2196/16802
23. Burckhardt R, Manicavasagar V, Batterham PJ, Miller LM, Talbot E, Lum A. A web-based adolescent positive psychology program in schools: randomized controlled trial. J Med Internet Res. 2015;17(7):e187. doi:10.2196/jmir.4329
24. Lillevoll KR, Vangberg HC, Griffiths KM, Waterloo K, Eisemann MR. Uptake and adherence of a self-directed internet-based mental health intervention with tailored e-mail reminders in senior high schools in Norway. BMC Psychiatry. 2014;14:14. doi:10.1186/1471-244X-14-14
25. Das JK, Salam RA, Lassi ZS, et al. Interventions for adolescent mental health: an overview of systematic reviews. J Adolesc Health. 2016;59(4s):S49–s60. doi:10.1016/j.jadohealth.2016.06.020
26. Janoušková M, Tušková E, Weissová A, et al. Can video interventions be used to effectively destigmatize mental illness among young people? A systematic review. Eur Psychiatry. 2017;41:1–9. doi:10.1016/j.eurpsy.2016.09.008
27. Slemmons K, Anyanwu K, Hames J, et al. The impact of video length on learning in a middle-level flipped science setting: implications for diversity inclusion. J Sci Educ Technol. 2018;27(5):469–479. doi:10.1007/s10956-018-9736-2
28. Winkler P, Janoušková M, Kožený J, et al. Short video interventions to reduce mental health stigma: a multi-centre randomised controlled trial in nursing high schools. Soc Psychiatry Psychiatr Epidemiol. 2017;52(12):1549–1557. doi:10.1007/s00127-017-1449-y
29. Cowdery JE, Powell JH, Fleming YA, Brown DL. Effectiveness of a short video-based educational intervention on factors related to clinical trial participation in adolescents and young adults: a pre-test/post-test design. Trials. 2019;20(1):7. doi:10.1186/s13063-018-3097-2
30. Kaye DBV, Chen X, Zeng J. The co-evolution of two Chinese mobile short video apps: parallel platformization of Douyin and TikTok. Mob Media Commun. 2021;9(2):229–253. doi:10.1177/2050157920952120
31. Ito-Jaeger S, Perez Vallejos E, Curran T, et al. Digital video interventions and mental health literacy among young people: a scoping review. J Mental Health. 2022;31(6):873–883. doi:10.1080/09638237.2021.1922642
32. Dumville JC, Hahn S, Miles JN, Torgerson DJ. The use of unequal randomisation ratios in clinical trials: a review. Contemp Clin Trials. 2006;27(1):1–12. doi:10.1016/j.cct.2005.08.003
33. Authier J. The psychoeducation model: definition, contemporary roots and content. Canad J Counsell Psychoth. 2012;12:1.
34. Markowitz JC, Weissman MM. Interpersonal psychotherapy: principles and applications. World Psychiatry. 2004;3(3):136–139.
35. Hofmann SG, Asnaani A, Vonk IJ, Sawyer AT, Fang A. The efficacy of cognitive behavioral therapy: a review of meta-analyses. Cognit Ther Res. 2012;36(5):427–440. doi:10.1007/s10608-012-9476-1
36. Su L, Wang K, Zhu Y. Norm of the depression self-rating scale for children in Chinese urban children. Chin Mental Health J. 2003;2003:547–549.
37. Birleson P. The validity of depressive disorder in childhood and the development of a self-rating scale: a research report. J Child Psychol Psychiatry. 1981;22(1):73–88. doi:10.1111/j.1469-7610.1981.tb00533.x
38. Hu T. Development of perceived social support scale for youths. J Guizhou Educ Univer. 2010;26(03):71–75. doi:10.13391/j.cnki.issn.1674-7798.2010.03.002
39. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
40. Devlin NJ, Brooks R. EQ-5D and the EuroQol group: past, present and future. Appl Health Econ Health Policy. 2017;15(2):127–137. doi:10.1007/s40258-017-0310-5
41. Zhuo L, Xu L, Ye J, et al. Time trade-off value set for EQ-5D-3L based on a nationally representative Chinese population survey. Value Health. 2018;21(11):1330–1337. doi:10.1016/j.jval.2018.04.1370
42. Jordans MJ, Tol WA, Ndayisaba A, Komproe IH. A controlled evaluation of a brief parenting psychoeducation intervention in Burundi. Soc Psychiatry Psychiatr Epidemiol. 2013;48(11):1851–1859. doi:10.1007/s00127-012-0630-6
43. Stallard P, Skryabina E, Taylor G, et al. Classroom-based cognitive behaviour therapy (FRIENDS): a cluster randomised controlled trial to Prevent Anxiety in Children through Education in Schools (PACES). Lancet Psychiatry. 2014;1(3):185–192. doi:10.1016/s2215-0366(14)70244-5
44. Prencipe L, Houweling TAJ, van Lenthe FJ, Kajula L, Palermo T. Tanzania adolescent cash plus evaluation T. effects of adolescent-focused integrated social protection on depression: a pragmatic cluster-randomized controlled trial of tanzania’s cash plus intervention. Am J Epidemiol. 2022;191(9):1601–1613. doi:10.1093/aje/kwac093
45. Sander L, Rausch L, Baumeister H. Effectiveness of Internet-based interventions for the prevention of mental disorders: a systematic review and meta-analysis. JMIR Ment Health. 2016;3(3):e38. doi:10.2196/mental.6061
46. Gillham JE, Reivich KJ, Freres DR, et al. School-based prevention of depression and anxiety symptoms in early adolescence: a pilot of a parent intervention component. Sch Psychol Quart. 2006;21(3):323–348. doi:10.1521/scpq.2006.21.3.323
47. Brunwasser SM, Garber J. Programs for the prevention of youth depression: evaluation of efficacy, effectiveness, and readiness for dissemination. J Clin Child Adolesc Psychol. 2016;45(6):763–783. doi:10.1080/15374416.2015.1020541
48. Fisak BJ, Richard D, Mann A. The prevention of child and adolescent anxiety: a meta-analytic review. Prev Sci. 2011;12(3):255–268. doi:10.1007/s11121-011-0210-0
49. Calear AL, Christensen H. Systematic review of school-based prevention and early intervention programs for depression. J Adolesc. 2010;33(3):429–438. doi:10.1016/j.adolescence.2009.07.004
50. Vallury KD, Jones M, Oosterbroek C. Computerized cognitive behavior therapy for anxiety and depression in rural areas: a systematic review. J Med Internet Res. 2015;17(6):e139. doi:10.2196/jmir.4145
51. Lee G, Ham OK, Lee BG, Kim AM. Differences in factors associated with depressive symptoms between urban and rural female adolescents in Korea. J Korean Acad Nurs. 2018;48(4):475–484. doi:10.4040/jkan.2018.48.4.475
52. Li G, Mei JH, You J, et al. Sociodemographic characteristics associated with adolescent depression in urban and rural areas of Hubei province: a cross-sectional analysis. BMC Psychiatry. 2019;19(1):386. doi:10.1186/s12888-019-2380-4
53. Hesketh T, Ding QJ. Anxiety and depression in adolescents in urban and rural China. Psychol Rep. 2005;96(2):435–444. doi:10.2466/pr0.96.2.435-444
54. Yu XY, Liu YY, Zheng HY, Zhao Y. Influence of family environment on mental health; 2012:111–116.
55. Chi XL, Liu XF, Huang QM, Huang LY, Zhang PC, Chen XC. Depressive symptoms among junior high school students in southern china: prevalence, changes, and psychosocial correlates. J Affect Disord. 2020;274:1191–1200. doi:10.1016/j.jad.2020.05.034
56. Gao YJ, Xie SH, Frost CJ. An ecological investigation of resilience among rural-urban migrant adolescents of low socioeconomic status families in China. J Community Psychol. 2020;48(3):862–878. doi:10.1002/jcop.22303
57. Somrongthong R, Wongchalee S, Laosee O. Depression among adolescents: a study in a Bangkok slum community. Scand J Caring Sci. 2013;27(2):327–334. doi:10.1111/j.1471-6712.2012.01037.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Immersive Virtual Therapy as a Method Supporting Recovery of Depressive Symptoms in Post-Stroke Rehabilitation: Randomized Controlled Trial
Kiper P, Przysiężna E, Cieślik B, Broniec-Siekaniec K, Kucińska A, Szczygieł J, Turek K, Gajda R, Szczepańska-Gieracha J
Clinical Interventions in Aging 2022, 17:1673-1685
Published Date: 23 November 2022
Adaptation of the Mental Health Inventory (MHI-38) for Adolescents - Indonesian Version
Parombean AC, Abidin FA, Qodariah L, Novita S
Psychology Research and Behavior Management 2023, 16:2655-2665
Published Date: 13 July 2023
Differential Impact of Emotional and Contextual Factors Associated with COVID-19 on Adolescent Mental Health
Sánchez-López MT, Llamas-Díaz D, Megías-Robles A, Gómez-Leal R, Gutiérrez-Cobo MJ, Fernández-Berrocal P, Cabello R
Psychology Research and Behavior Management 2024, 17:147-156
Published Date: 10 January 2024
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Academic Pressure and Psychological Imbalance in High School Students: Predictors of Depression via Polynomial Regression and Response Surface Analysis
Ye Y, Zhang Z, Tao Z, Liping C, Wang Y, Chen H, Li S, Chen X, Tang H, Zhou J, Zhou J
Psychology Research and Behavior Management 2025, 18:15-23
Published Date: 7 January 2025