")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
SGLT2 Inhibitors in the Management of Type 1 Diabetes (T1D): An Update on Current Evidence and Recommendations
Authors Maffei P, Bettini S, Busetto L , Dassie F
Received 25 May 2023
Accepted for publication 24 October 2023
Published 9 November 2023 Volume 2023:16 Pages 3579—3598
DOI https://doi.org/10.2147/DMSO.S240903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Pietro Maffei, Silvia Bettini, Luca Busetto, Francesca Dassie
Department of Medicine, Padua University, Padua, Italy
Correspondence: Pietro Maffei, Email [email protected]
Abstract: SGLT2i (sodium glucose transporter type 2 inhibitors) are pharmacological agents that act by inhibiting the SGLT2, by reducing the renal plasma glucose threshold and inducing glycosuria, resulting in a blood glucose lowering effect. In recent years, studies demonstrating some additional positive effects of SGLT2i also in the treatment of T1D have increased progressively. The SGLT2i dapagliflozin and sotagliflozin have been temporarily licensed for use by the European Medical Agency (EMA) as an adjunct to insulin therapy in adults with T1D with a body mass index of 27 kg/m2 or higher. However, in the meantime, the US Food and Drug Administration (FDA) Endocrinologic and Metabolic Drugs Advisory Committee was divided, citing concerns about the main side effects of SGLT2i, especially diabetic ketoacidosis (DKA). The aim of this manuscript was to conduct an update on current evidence and recommendations of the reported use of SGLT2i in the treatment of T1D in humans. Preclinical studies, clinical trial and real world data suggest benefits in glycaemia control and nefro-cardiovascular protection, even though several studies have documented an important increase in the risk of DKA, a serious and life-threatening adverse event of these agents. SGLT2i potentially addresses some of the unmet needs associated with T1D by improving glycaemic control with weight loss and without increasing hypoglycemia, by reducing glycaemic variability. However, due to side effects, EMA recommendation for SGLT2 use on T1D was withdrawn. Further studies will be needed to determine the safety of this therapy in T1D and to define the type of patient who can benefit most from these medications.
Keywords: dapagliflozin, canagliflozin, empagliflozin, ipragliflozin, mechanism, clinical studies
Introduction
Sodium glucose transporter type 2 inhibitors (SGLT2i) are a new class of oral glucose-lowering pharmacological agents that act by inhibiting the SGLT2, located in the proximal part of the kidney convoluted tubule and responsible for about 90% of glucose reabsorption. SGLT2i act by reducing the renal plasma glucose threshold and inducing glycosuria, resulting in a blood glucose lowering effect. With the advent of SGLT2i, the therapeutic possibilities available to diabetologists have increased, and clinical experience is in favor of their expanding use in the treatment of patients with type 2 diabetes mellitus (T2D).1,2
On the other hand, less known are the potential therapeutic actions of SGLT2i in the treatment of type 1 diabetes mellitus (T1D). In recent years, studies demonstrating some additional positive effects of SGLT2i also in the treatment of T1D have increased progressively. The SGLTi dapagliflozin (5 mg) and sotagliflozin (200 and 400 mg) have been temporarily licensed for use by the European Medical Agency (EMA) as an adjunct to insulin therapy in adults with T1D with a body mass index (BMI) of 27 kg/m2 or higher.1,2 Another SGLT2i, remogliflozin etabonate, has been studied in T1D, but it has never been licensed for these subgroups of patients. The SGLT2i ipragliflozin, canagliflozin and empagliflozin have also been investigated in T1D.
The aim of this manuscript was to conduct an update on current evidence and recommendations of the reported use of SGLT2i in the treatment of T1D in humans. Therefore, the studies carried out on preclinical experimental models were deliberately excluded from this update aside from for a brief general introduction to better understand the SGLT2i clinical implications.
Recommendations and Indications
In February 2019, the EMA provided an agreement on the clinical indication for both sotagliflozin 1 and dapagliflozin 2 as adjunctive treatments for T1D, in patients with a BMI of 27 kg/m² or higher. This new recommendation was based on data from phase three studies that included patients with T1D.3–5 However, in the meantime, the US Food and Drug Administration (FDA) Endocrinologic and Metabolic Drugs Advisory Committee was divided, citing concerns about the main side effects of SGLTi, especially diabetic ketoacidosis (DKA).
Dapagliflozin
The main advantage of dapagliflozin treatment in patients with T1D is a joint effect on glycaemia, weight and blood pressure and decrease in variability of glycaemia. The EMA emphasised that insulin therapy should be continuously adjusted to prevent ketosis and diabetic ketoacidosis and that SGLT2i therapy should be supervised by specialists. Later, the FDA announced its decision not to approve dapagliflozin6 on July 15, 2019. However, on 28 August 2019, the National Institute for Health and Care Excellence (NICE) published a guidance recommending dapagliflozin (Edistride®, Forxiga®), to treat T1D in adults with BMI more than 27 kg/m² and when insulin monotherapy does not provide adequate glycaemic control.7 The guidance also specified that dapagliflozin should be restricted to patients with T1D treated with insulin doses greater than 0.5 units per kg body weight per day. Furthermore, patients who receive adjunctive therapy with dapagliflozin should complete a structured education program and be trained to manage associated risks whose medical care is supervised by a consultant physician specialized in endocrinology and diabetes. The guidance also stated that people should stop dapagliflozin if they do not see a sustained improvement in glycaemic control when evaluated after 6 months and regularly thereafter. The recommended dose of dapagliflozin was 5 mg once daily administered orally, with or without food. On 29 October 2021, AstraZeneca, in agreement with the EMA and the National Competent Authority, informed that dapagliflozin 5 mg was no longer authorized for the treatment of patients with T1D and should no longer be used in this population.8 This fact was justified by the high frequency (occurring in at least 1 per 100 patients) of DKA in studies of T1D with dapagliflozin. The document added that the discontinuation of dapagliflozin in patients with T1D must be made by or in consultation with a physician specialized in diabetes care and be carried out as soon as clinically practical. After stopping dapagliflozin treatment, frequent blood glucose monitoring is recommended, and the insulin dose should be carefully increased to reduce the risk of hypoglycaemia. In November 2021, also NICE withdrew previous guidance because dapagliflozin with insulin is no longer licensed for treating T1D.7
Sotagliflozin
Sotagliflozin binds to and blocks both SGLT1 in the gastrointestinal (GI) tract and SGLT2 in the kidneys. SGLT1 is the primary transporter responsible for glucose absorption from the GI tract. EMA indicated Sotagliflozin (Zynquista®) “as an adjunct to insulin therapy to improve glycaemic control in adults with T1D, with a BMI ≥ 27 kg/m2, who have failed to achieve adequate glycaemic control despite optimal insulin therapy”.
Sotagliflozin therapy should have been initiated and supervised by a physician experienced in the treatment of T1D. The recommended dose was 200 mg of sotagliflozin once a day before the first meal of the day. After at least three months, if additional glycaemic control was needed, in patients tolerating 200 mg of Sotagliflozin, the dose could be increased to 400 mg once daily.9 Regarding special population, there were also other important recommendations. Due to the limited therapeutic experience in patients older than 75 years, initiation of sotagliflozin therapy was not recommended. In addition, the safety and efficacy of sotagliflozin in children and adolescents has not yet been established. Sotagliflozin should not be started in patients with an eGFR <60 mL/min and should be discontinued at an eGFR persistently below 45 mL/min. Due to side effects, the FDA announced that it would not approve sotagliflozin,10 while the EMA withdrew from use on August 16, 2022.11
Empagliflozin
The EASE Trials12 demonstrated an improved glycemic control and weight of empagliflozin 10 and 25 mg doses plus a unique lower dose (2.5 mg) as an adjunct to intensified insulin in patients with T1D. The ketoacidosis rate was comparable between empagliflozin 2.5 mg and placebo but increased with 10 mg and 25 mg. A very recent RCT (randomized control trial) showed that low-dose empagliflozin (2.5 mg and 5 mg) is enough to help patients with T1D who cannot achieve adequate glucose control with closed-loop insulin. However, future studies are required to evaluate its long-term efficacy and safety.13 A committee of the FDA has recommended against the approval of empagliflozin marketed under the trade name Jardiance®, for the treatment of T1D, due to limited data around safety, particularly an increased risk of DKA.14
Preclinical Studies
SGLT2 inhibitors’ chemical structure and main pharmacokinetic parameters are listed in Table 1.
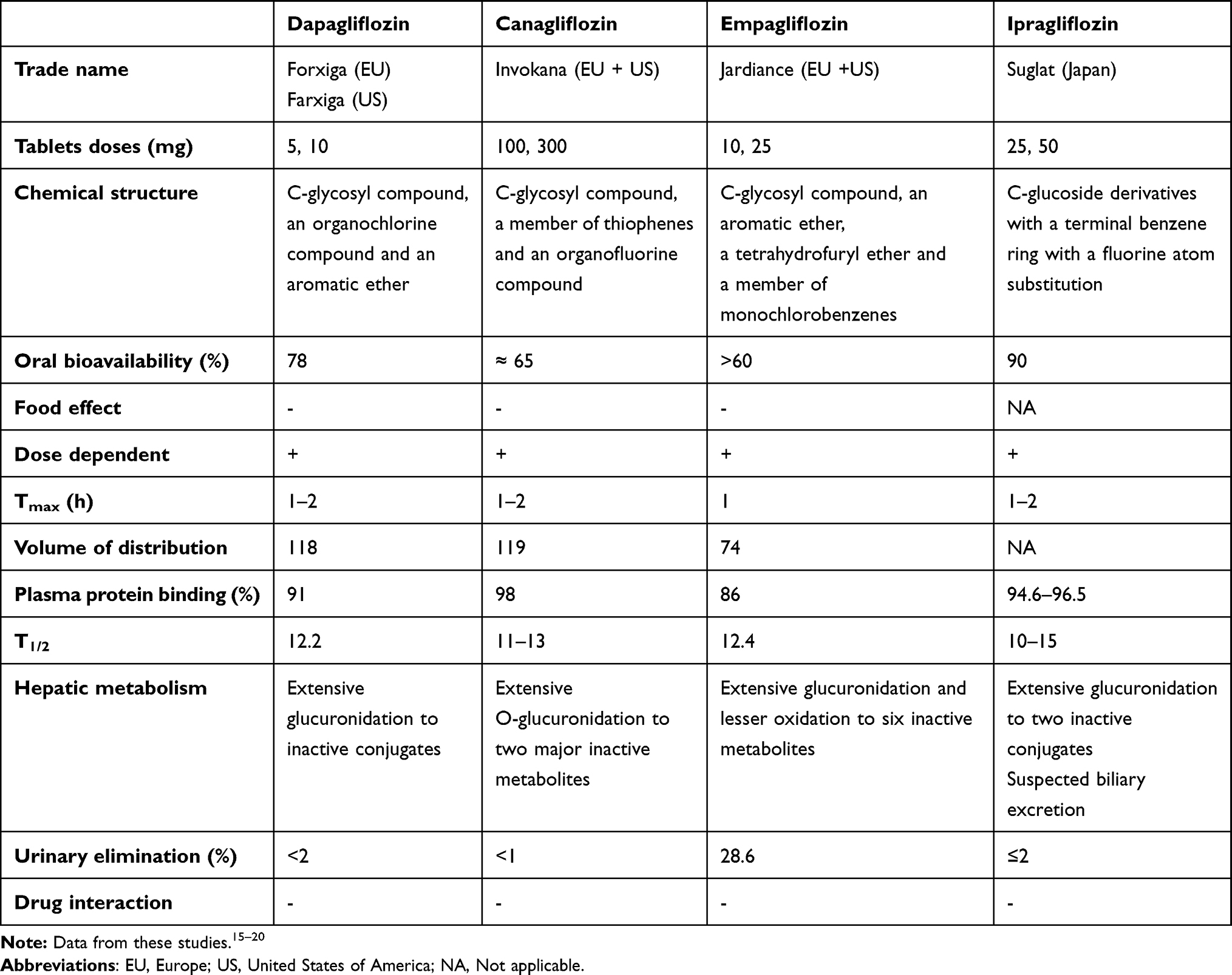 |
Table 1 SGLT2 Inhibitors Chemical Structure and Main Pharmacokinetic Parameters |
SGLT2i inhibits renal reabsorption of filtered glucose acting through SGLT2, which is localized in the early proximal tubule, and mediates the tubular glucose uptake through the apical membrane of the kidney. SGLT2 increase: 1) Na and fluid reabsorption in the proximal tubule of the early diabetic kidney; 2) proximal reabsorption that contributes to diabetic glomerular hyperfiltration by lowering Na-Cl-K concentrations at the macula densa and 3) glomerular filtration rate (GFR) through the physiology of tubulo-glomerular feedback. In early diabetic kidney, they also inhibit the SGLT2 mediated glucose uptake, which causes kidney growth, that has been linked to nephropathy. In a first paper, Vallon et al showed that gene knockout of the sodium-glucose cotransporter SGLT2 modestly lowered blood glucose in streptozotocin-diabetic mice (STZ mice) and prevented glomerular hyperfiltration but did not attenuate albuminuria or renal growth and inflammation.21 In a second paper, the authors showed in T1D Akita mice that empagliflozin attenuated/prevented the increase in systolic blood pressure, glomerular size, and molecular markers of kidney growth, inflammation, and gluconeogenesis. The authors speculated that inhibition of SGLT2 can lower GFR independent of reducing blood glucose (consistent with the tubular hypothesis of diabetic glomerular hyperfiltration), while attenuation of albuminuria, kidney growth, and inflammation in the early diabetic kidney may be secondary to lower blood glucose.22
Among the mechanisms beyond diabetic nephropathy, renal fibrosis plays an important role, and dapagliflozin seems to have an inhibitory effect on tubulo-interstitial fibrosis (TIF) with a possible impact on renal function. Huang et al studied this mechanism with an in vitro experiment in HK-2 cells derived from kidney biopsies from patients that were incubated in high glucose with dapagliflozin or fludarabine, and epithelial–mesenchymal transition cells and in vivo study in STZ mice treated with dapagliflozin for 16 weeks. The authors demonstrated that dapagliflozin not only improves hyperglycemia but also slows the progression of diabetes-associated renal TIF by improving hyperglycemia-induced activation of the STAT1/TGF-β1 pathway. In fact, in mice dapagliflozin improved blood glucose levels, renal function, and reduced TIF while in HK-2 cells; dapagliflozin, and fludarabine directly decreased aberrant STAT1 expression and reversed high glucose-induced downregulation of E-cadherin and α-SMA induction.23
Cheng and collaborators studied the role of empagliflozin in pancreatic cells in streptozotocin-induced T1D rats. Empagliflozin induced an improved glucose tolerance and increased insulin m-RNA expression, β-cell area, total pancreatic area and Ki-67 as a cell proliferation marker. These effects were probably due to a reduction in apoptosis and reactive oxygen species in pancreatic β-cells. Taken together, the results of this study indicate that empagliflozin may have a beneficial effect on preserving β-cell regeneration, thus improving blood glucose homeostasis in T1D, probably through protection of pancreatic β-cell from glucotoxicity-induced oxidative stress.24
SGLT2i acts also on diabetic cardiomyopathy with two pathways: in the first pathway, SGLT2i decreases oxidative stress activating SIRT1 mainly through the SIRT1/Nrf2 signaling and in the second pathway SGLT2i does not enhance autophagy.25 Empagliflozin regulated increased autophagy, which depended on the downregulation of NHE1 and NHE1-related genes that induce autophagy, such as Beclin 1 and autophagy-related protein 5.26
Although the association between atherosclerosis and hyperglycemia is still unclear, Terasaki et al studied the association between the amelioration of dapagliflozin or ipragliflozin induced glycemia and the macrophage-driven atherosclerosis in apolipoprotein E-null (Apoe-/-) mice, streptozotocin-induced diabetic Apoe-/- mice, and diabetic db/db mice. The authors found anti-atherogenic effects due to pure glucose lowering with a mechanism that is independent of insulin action in diabetic mice by suppressing macrophage foam cell formation, suggesting that foam cell formation is highly sensitive to glycemia ex vivo. Apoe-/- mice treated with dapagliflozin reduced aortic atherosclerotic lesions, atheromatous plaque size, and macrophage infiltration. In non-diabetic Apoe-/- mice, atherosclerosis was not affected by dapagliflozin. Ipragliflozin decreased foam cell formation in db/db mice. SGLT2i normalized gene expressions of the lectin-like ox-LDL receptor-1 and the acyl-coenzyme A:cholesterol acyltransferase 1.27 Al Sharea et al studied lipoprotein clearance in Ldlr−/− type 1 diabetic mice, and they found that the glycemic control secondary to SGLT2i treatment reduced monocytosis and atherosclerosis and improved plasma lipoprotein profile, which was mediated by heparin sulfate proteoglycan (HSPG)-dependent clearance mechanisms in the liver.28
Regarding the microvascular comorbidities, Eid et al investigated the role of empagliflozin in diabetic neuropathy, retinopathy, and kidney disease in STZ mice. Empagliflozin decreased blood glucose, with an improvement in diabetic neuropathy and a reduction in systemic oxidative stress, and also had a modest effect on retinopathy and had no effects on kidney disease.29
Clinical Studies on Presymptomatic T1D (Pre-T1D)
Recently, the ADA, JDRF, and Endocrine Society released a joint position statement for the staging of pre-T1D, a clinical condition where autoimmunity is present but there is no symptomatic clinical or metabolic impairment. In order to prevent T1D, several clinical trials on lifestyle interventions and medications (insulin, GLP1-rA, and immunotherapy) were conducted, but no final recommendations were made. No data are available on SGLT2i therapy in these subgroups of patients. Therefore, in patients with pre-T1D, the results of treatment with SGLT2i are inferred from pre-T2D studies. Dapagliflozin treatment of prediabetic insulin-resistant individuals for 14 days resulted in significant metabolic adaptations in whole-body and skeletal muscle substrate metabolism despite being weight neutral.30 On the contrary, in the paper of Clemmensen et al, the authors showed that in 120 patients with pre-T2D, 13 weeks of treatment with dapagliflozin, metformin or exercise was not associated with significant changes in fasting or post-OGTT glucagon concentrations.31
A recent meta-analysis of randomized controlled trials on new onset T2D patients with prediabetes showed that SGLT2i reduced the risk of new-onset T2D among adults with prediabetes, heart failure or chronic kidney disease.32
Clinical Studies in T1D
Remogliflozin
In a single-center, randomized, double-blinded, placebo-controlled trial, 10 individuals with T1D treated with continuous subcutaneous insulin infusion were enrolled. This clinical trial was the first to explore the feasibility of administering an SGLT2i with insulin to patients with T1D. In addition to basal insulin, subjects received five randomized treatments: placebo, prandial insulin, 50 mg, 150 mg or 500 mg of Remogliflozin etabonate. All Remogliflozin etabonate regimens significantly decreased glucose concentrations compared to placebo after a glucose load and glucose improvements were sustained for 10 h.33
Dapagliflozin
Dose-related trends in the magnitude of effect for fasting plasma glucose (FPG), diacylglycerol (DAG), SD of DAG, and mean amplitude of glucose excursion (MAGE) were suggested with dapagliflozin therapy in T1D. In 2015, a short pilot study among patients with T1D, dapagliflozin treatment resulted in dose-dependent urinary glucose excretion. A 2-week, dose-ranging, randomized, double-blind, placebo-controlled study randomly assigned 70 adults with T1D, who were receiving treatment with stable doses of insulin, to one of the four dapagliflozin doses (1, 2.5, 5, or 10 mg) or placebo. No differences between dapagliflozin and placebo were observed for the 7-point mean glucose measurements.34
A year later, in a single-center, randomized, placebo-controlled, double-blind, Phase IV study, the effect of triple therapy (dapagliflozin, liraglutide, and insulin) on T1D was tested. The authors observed marked improvements in hyperglycemic spikes. The patients received insulin therapy through continuous subcutaneous insulin infusion (CSII) or multiple (four or more) injections per day. All were on liraglutide therapy at maximum tolerated doses prior to the start of the study. Patients were randomized to receive 10 mg dapagliflozin or placebo daily for 12 weeks, and the primary end point of the study was the change in mean HbA1c after 12 weeks. HbA1c in the triple therapy group fell by 0.66%, whereas there was no significant change in the placebo group. The mean absolute total insulin dose remained unchanged in both groups.35
In 2018, a total of 12 male patients with T1D were randomized to receive either 10 mg of dapagliflozin or placebo for 3 days in a double- blind, cross-over design. The short-term addition of dapagliflozin to insulin influenced neither postprandial glucose excursions nor insulin sensitivity. Following oral glucose, total ketone bodies decreased in parallel with an increase in GLP-1 concentrations, which were higher under dapagliflozin treatment compared with placebo.36
Insulin dose reductions of more than 30% were observed in Japanese patients with T1D treated with dapagliflozin 5 or 10 mg. In a phase Ib randomized, single-blind, three-arm, placebo-controlled study has been assessed the pharmacokinetics/pharmacodynamics (PK/PD) of dapagliflozin and its main metabolite, dapagliflozin-3-O-glucuronide (D3OG), in Japanese patients with T1D and inadequate glycaemic control. Patients with inadequately controlled T1D were randomized to dapagliflozin 5 mg, 10 mg or placebo once daily for 7 days, with adjustable insulin.37
The DEPICT-1 (Dapagliflozin Evaluation in Patients With Inadequately Controlled Type 1 Diabetes) was a double-blind, randomised, parallel-controlled, three-arm, Phase 3, multicentre study carried out at 143 sites in 17 countries. Patients were randomly assigned (1:1:1) to dapagliflozin 5 mg or 10 mg once daily, administered orally or matched placebo. The mean difference in HbA1c from baseline to week 24 for dapagliflozin 5 mg versus placebo was −0.42%, and for dapagliflozin 10 mg versus placebo was −0.45%. HbA1c reduction with dapagliflozin occurred in the first 4 weeks, with the effect maintained throughout the duration of the study. Additionally, the mean difference in the total daily insulin dose from baseline to week 24 was −8.8% for dapagliflozin 5 mg versus placebo and −13.2% for dapagliflozin 10 mg versus placebo.3 The long-term safety and efficacy of DEPICT-1 was also evaluated in the long term after 52 weeks. The DEPICT-1 study showed that dapagliflozin as an adjunct to adjustable insulin leads to a clinically relevant decrease in HbA1c and total daily insulin dose reductions between patient groups stratified by baseline characteristics (HbA1c, continuous glucose monitoring [CGM] use, and insulin administration method).3
The DEPICT-2 was a randomized, double-blind, parallel-controlled, three-arm, multicenter, phase 3 study that evaluated the efficacy and safety of dapagliflozin 5 mg and 10 mg as an adjunct therapy to adjustable insulin in adult patients with T1D and inadequate glycemic control. The DEPICT-2 study included patients from North America, Latin America, Europe, and Japan, and the primary efficacy outcome was the change in HbA1c from baseline after 24 weeks. At week 24, there were significant reductions in HbA1c with both dapagliflozin doses versus placebo. Mean changes in HbA1c from baseline to week 24 versus placebo were - 0.37% and - 0.42% for dapagliflozin 5 mg and 10 mg. The initial reduction in HbA1c was observed in the first 4 weeks, and the effect was maintained throughout the study.4 The DEPICT-2 study also aimed to assess the long-term efficacy and safety of dapagliflozin in people with T1D. From baseline to 52 weeks (24-week short-term period plus a 28-week extension), dapagliflozin 5 and 10 mg were associated with a significant reduction in HbA1c and an adjusted mean percentage change in body weight.4 These results support the long-term benefit of dapagliflozin in people with T1D of different ethnicities and countries of origin.
To quantitatively describe the relationship between dapagliflozin systemic exposure and HbA1c response among patients with T1D and to assess the possible impact of covariate effects, the data were pooled from DEPICT-1 and DEPICT-2 who received dapagliflozin 5 or 10 mg or placebo for 24 weeks.3,4 The results of the DEPICT studies showed that the adjunct of dapagliflozin therapy resulted in improved HbA1c and reduced body weight, without an increase in the risk of hypoglycemia. Baseline HbA1c was predicted to have an impact on dapagliflozin efficacy; however, the efficacy was not impacted to a clinically relevant extent.38 DEPICT-1 and DEPICT-2 studies had almost identical designs, which allowed a pooled analysis at 52 weeks, confirming that dapagliflozin provided glycaemic and weight benefits, with no increased frequency of severe hypoglycemia compared with placebo.39 The aim of this analysis was to report the safety and efficacy of adjunct dapagliflozin therapy in a pooled population from DEPICT-1 and −2 studies. Furthermore, the aim was to explore whether the efficacy and safety of dapagliflozin treatment differs between subgroups of patients according to baseline HbA1c (<75 mmol/mol [<9.0%] or ≥75 mmol/mol [≥9.0%]) or the method of insulin administration (continuous subcutaneous insulin infusion or multiple daily injections [MDI]). Both studies included an 8-week lead-in period to optimize diabetes management; a 24-week, double-blind treatment period (short-term period); a 28-week subject- and site-blinded extension (long-term period); and a 4-week follow-up period. Dapagliflozin treatment provided glycaemic and weight benefits, along with reductions in insulin dose over 52 weeks. The safety and efficacy of adjunct dapagliflozin therapy was consistent across baseline HbA1c subgroups and by the method of insulin administration. The subgroup analyses showed comparable efficacy results with the overall DEPICT population. Dapagliflozin was well tolerated and led to clinically relevant improvements in glycaemic control and weight reduction, without an increased risk of severe hypoglycemia. Compared to placebo, the risk of DKA was higher in patients treated with dapagliflozin. The authors suggested that this risk may be mitigated by appropriate patient selection and education.
In participants with BMI ≥27 kg/m2 coming from the pooled DEPICT 1 and 2 population, the efficacy and safety of dapagliflozin 5 mg compared to placebo, both used as an adjunct to insulin, were evaluated. Efficacy outcomes were analyzed at weeks 24 and 52 and included changes from baseline in HbA1c and body weight, percentage change from baseline in daily insulin dose, and proportion of participants who achieved HbA1c reduction ≥0.5% with no severe hypoglycemia. The adjusted mean change in week 52 from baseline for HbA1c was −0.26% with dapagliflozin versus +0.08% with placebo and for body weight was −2.74 kg with dapagliflozin versus +0.81 kg with placebo. The mean percentage change in daily insulin dose was −10.5% with dapagliflozin versus −1.4% with placebo. The time spent in the target glycaemic range increased by 2.2 h/day versus placebo.4
Also, in Japanese patients with inadequately controlled T1D, long-term dapagliflozin adjunct to insulin therapy improved HbA1c, reduced body weight, and reduced total daily insulin dose, and these improvements in efficacy were maintained for up to 52 weeks 37,40. However, there were no differences in the efficacy parameters when stratified by BMI.37
Araki et al studied the efficacy and safety of dapagliflozin as an adjunct to insulin in Japanese patients enrolled in the DEPICT-2 study. This was a multicentre, randomized, double-blind, parallel-group, three-arm, placebo-controlled phase 3 study to evaluate the efficacy and safety of two doses of dapagliflozin (5 and 10 mg) as an adjunct to insulin in patients with T1D and inadequate glycaemic control. The study confirmed that dapagliflozin treatment improved HbA1c, reduced body weight, and reduced the total daily insulin dose at 24 weeks and that these efficacies were maintained for up to 52 weeks.41
The safest method of instructing the reduction of insulin dose in combination with SGLT2i, dapagliflozin, for patients with T1D has not been already clarified. Hamaguchi et al conducted a stratified, 2-arm, parallel comparative study with the primary endpoint of decreasing the frequency of hypoglycemia by instructing basal insulin dose reduction. The authors of the RISING-STAR study hypothesized that the frequency of hypoglycemia per day would increase after the administration of an SGLT2i, provided the dose of basal insulin was not titrated. This study will be conducted in 7 research institutions and total 350 patients with T1D are being treated in these institutions. From the previous survey, 30% of these patients are assumed to be eligible for the use of the SGLT2i, meaning that approximately 100 patients can use the SGLT2i with insulin.42
The effects of Dapagliflozin on glucose levels overnight and during the following day after two unannounced meals were investigated also under full closed loop (FCL) conditions. A combination of AID (Automated Insulin Delivery) with Dapagliflozin adjunct may constitute a novel approach to maximize TIR (Time in range) of glucose during insulin therapy, potentially helping individuals with T1D to achieve meaningful clinical benefits beyond reductions in HbA1c.40
Recently, the efficacy of the SGLT2i dapagliflozin was evaluated as an adjunct to insulin therapy in young Japanese T1D subjects diagnosed before 15 years old who were overweight and had inadequate glycemic control despite intensive insulin therapy.43 These results corroborate those reported in previous Caucasian studies and show a beneficial effect of adjunct dapagliflozin therapy in young people with type 1 diabetes. Twenty-two patients participated in the study. Body weight and BMIs were significantly reduced, insulin dose was significantly decreased (−0.17 units/kg), and glycaemic control improved significantly (fasting plasma glucose: −18.7 mg/dL, HbA1 c: −0.62%) during the study period.
Sotagliflozin
Sotagliflozin is a dual inhibitor of SGLT1 and SGLT2. In Phase 2 studies, sotagliflozin administration improved glycemic control and decreased body weight among patients with T1D or T2D; it also reduced glycemia, despite a decrease in insulin bolus dose, among patients with T1D.44,45
Sotagliflozin was studied in T1D in a randomized, multicenter, placebo-controlled, double-blind evaluation of 29 days of treatment in 33 adult patients who used their previous insulin delivery regimen: either CSII or MDI. In the sotagliflozin-treated group, the percent reduction from baseline in the primary end point of the bolus insulin dose was 32.1%, accompanied by a lower mean daily glucose measured by CGM and a reduction of 0.55% (5.9 mmol/mol) in HbA1c. The percentage of time in the target glucose range increased from baseline with sotagliflozin compared to placebo, to 68.2% vs 54.0%.44
The North American inTandem1 Study is a phase 3, multicenter, randomized, double-blind, placebo-controlled, parallel-group study conducted at 75 sites in the US and Canada that evaluated the safety and efficacy of oral sotagliflozin 200 or 400 mg combined with insulin in adult patients with inadequately controlled T1D. The study consisted of two double-blind periods: a 24-week treatment period (the primary end-point assessment) followed by a 28-week double-blind extension. The placebo-adjusted reductions in HbA1c were 0.36% and 0.41% with sotagliflozin 200 and 400 mg, respectively, at 24 weeks and 0.25% and 0.31% at 52 weeks. At 52 weeks, mean treatment differences between sotagliflozin 400 mg and placebo were −1.08 mmol/L for fasting plasma glucose, −4.32 kg for weight, and −15.63% for bolus insulin dose and −11.87% for basal insulin dose.46 Sotagliflozin 400 mg was associated with lower insulin doses, FPG, weight, and SBP, as well as improved glycaemic variability with less hypoglycemia. Sotagliflozin 200 mg did not reduce bolus insulin doses; however, significant reductions in total insulin dose, FPG, and weight were reported.
The European inTandem2 study is a phase 3 multicenter, randomized, double-blind, placebo-controlled, parallel-group study that evaluated the safety and efficacy of 200 or 400 mg oral sotagliflozin once-daily in combination with insulin in adults with T1D who had inadequate glycemic control. The double-blind treatment continued for 52 weeks and the primary end point was assessed at week 24. After 24 weeks, the difference from placebo for the primary end point of HbA1c was - 0.37% and - 0.35% with sotagliflozin 200 and 400 mg. After 52 weeks with 200 mg and sotagliflozin 400 mg of sotagliflozin, the difference in HbA1c from placebo was −0.21 and −0.32%, respectively. Furthermore, FPG decreased significantly in both sotagliflozin groups.47 Additionally, the glycemic variability of the CGM subgroup, measured on the basis of the mean amplitude of glycemic excursions, improved with both doses of sotagliflozin.48
InTandem3, is a phase 3, multicenter, randomized, double-blind, placebo-controlled trial, conducted at 133 sites in 19 countries, which evaluated the safety and efficacy of sotagliflozin in combination with insulin therapy (pump or injections) in patients with T1D. In the sotagliflozin group, patients received the 400 mg dose of sotagliflozin and continued their existing insulin regimens. A significantly higher proportion of patients in the sotagliflozin group than in the placebo group achieved the primary end point of HbA1c lower than 7.0% at week 24 with a difference of 13.4 percentage points. Furthermore, in the subgroup analysis based on type of insulin therapy (pump vs no pump), approximately twice as many patients in the sotagliflozin group as in the placebo group, both among those who used an insulin pump and those who did not, achieved the primary end point.5
The inTandem4 trial is a phase 2 dose-ranging study that evaluated the effects of three doses of sotagliflozin combined with stable doses of insulin administered as MDI or CSII in adults with T1D. The primary outcome was the change in HbA1c over 12 weeks. Sotagliflozin 200 and 400 mg in combination with stable insulin doses improved glycaemic control and reduced weight in people with T1D who had an eGFR ≥60 mL/min/1.73 m2 and normal beta-hydroxybutyrate levels at screening.49
Canagliflozin
Canagliflozin was investigated in an 18-week, double-blind, phase 2 study that randomized 351 T1D patients on multiple daily insulin injections or continuous subcutaneous insulin infusion to canagliflozin 100 or 300 mg or placebo. At week 18, a greater proportion of patients reached the primary endpoint and had HbA1c reduction >0.4% (>4.4 mmol/mol) and no increase in body weight with canagliflozin 100 and 300 mg compared to placebo (36.9%, 41.4%, and 14.5%, respectively). Both canagliflozin doses provided reductions in insulin dose over 18 weeks.50
The effects of canagliflozin on T1D were studied in a randomized, double-blind, treat-to-target, placebo-controlled, multicenter, phase 2 study consisting of a 2-week pre-randomization period followed by an 18-week double-blind treatment phase and 2 weeks of post-treatment follow-up. The patients were randomized to receive canagliflozin 100 or 300 mg or placebo once daily. Measures of glucose variability assessed by 9-point self-monitoring blood glucose (SMBG) and CGM profiles were assessed. More patients met the primary end point of HbA1c reduction of - 0.4% (- 4.4 mmol/mol) and no increase in body weight with canagliflozin 100 and 300 mg versus placebo at week 18 (36.9%, 41.4%, and 14.5%, respectively). The changes in daily mean glucose assessed by 9-point SMBG at week 18 with canagliflozin 100 and 300 mg and placebo were 21.2, 21.1, and 0.2 mmol/L, respectively. HbA1c reductions were also observed in the CGM sub-study.51
Ipragliflozin
Ipragliflozin is an SGLT2i approved for the treatment of T2D in Japan since 2014. The pharmacodynamics, pharmacokinetics, and safety of Ipragliflozin 25, 50, and 100 mg administered once daily for 2 weeks in Japanese patients with T1D who have inadequate glycaemic control with insulin therapy were evaluated in a phase 2 study. Ipragliflozin induced dose-dependent improvements in plasma glucose Cmax and AUC24h. Furthermore, there was a concomitant dose- dependent increase in mean renal glucose clearance.52 Afterwards, a phase 3 study aimed at evaluating the efficacy and safety of once-daily oral Ipragliflozin 50 mg was compared to placebo over 24 weeks in people with T1D inadequately controlled with insulin therapy. Treatment with ipragliflozin significantly reduced HbA1c, insulin dose, and body weight from baseline versus placebo in T1D.53
Shimoda et al aimed to retrospectively study patients with T1D who had received Ipragliflozin during the period from April 1, 2019, to August 21, 2020, in the Division of Diabetes, Endocrinology and Metabolism of Kawasaki Medical School Hospital. The primary endpoint was the level of HbA1c at 24 weeks. The percentage reduction in insulin dose at the start of the Ipragliflozin administration was the following: 0–9% reduction, 8%; 10%–19% reduction, 58%; ≥20%, 33%. HbA1c levels 8 weeks after the start of ipragliflozin administration were decreased by –0.78 ± 0.72%, and the daily insulin dose was reduced by 18.2 ± 8.5%. Ipragliflozin decreased HbA1c levels to 8.2 ± 1.2% and reduced the insulin dose to 0.52 ± 0.17 units/kg after 24 weeks. The value of HbA1c was particularly reduced in subjects with a preserved C-peptide index. Ipragliflozin significantly reduced body weight by –1.4 ± 1.4 kg 16 weeks after starting treatment, without additional weight loss after 24 weeks.54
Empagliflozin
The glycemic efficacy and safety of empagliflozin 25 mg daily was evaluated in 40 patients with T1D treated for 8 weeks in a single-arm open-label proof-of-concept trial. HbA1C decreased from 8.0 (64 mmol/mol) to 7.6 (60 mmol/mol), fasting glucose from 9.0 to 7.0 mmol/L, and daily insulin dose from 54.7 to 45.8 units/day at the end of treatment.55
EASE 1 (Empagliflozin as Adjunctive to inSulin thErapy) was a randomized, double-blind, placebo-controlled, parallel-group, phase 2 study conducted in one centre in Germany and one centre in Austria. Patients with T1D received 2.5 mg, 10 mg, 25 mg, or placebo as a supplement to insulin for 28 days. Empagliflozin significantly decreased HbA1c concentrations compared to placebo on day 28 and significantly decreased weekly mean total recorded insulin doses compared with placebo.56
The totality of the phase 3 data on empagliflozin as an adjunctive to insulin in T1D including the characterization of a unique lower dose was evaluated. The EASE program in patients with T1D included two international, multi-center, phase 3, randomized, double- blind, placebo-controlled, parallel-group trials of once-daily oral empagliflozin doses conducted over 52 weeks (EASE-2) and 26 weeks (EASE-3). Empagliflozin 10 mg and 25 mg versus placebo was studied in both trials, and an additional arm (empagliflozin 2.5 mg) was included in EASE-3. The EASE program showed that empagliflozin improved glycemic control, as assessed by placebo-corrected HbA1c change after 26 weeks of treatment. The maximum effect of HbA1c was observed from week 12 of treatment, it was dose-dependent, and greatest with empagliflozin 10 and 25 mg doses.12
In a phase 2, double-blind, randomized, placebo-controlled, parallel-group trial, 3 doses of empagliflozin taken once daily for 4 weeks as an adjunct to insulin therapy were studied in Japanese participants with T1D. Empagliflozin resulted in a dose-dependent significant increase in 24-hour urinary glucose excretion (UGE) compared to placebo, which was associated with improved glycaemic control, reduced body weight, and decreased insulin needs.57
Haidar A. et al aimed to assess whether adding empagliflozin to closed-loop automated insulin delivery systems, can reduce the need for carbohydrate counting without degrading glucose control. In an open-label, crossover, non-inferiority trial, 30 adult participants with T1D, Empagliflozin added to automated insulin delivery has the potential to eliminate the need for carbohydrate counting and improves glycaemic control in conjunction with carbohydrate counting, but does not allow for the elimination of meal announcement.58 Johnston et al aimed to investigate by a semi-mechanistic model the interplay between empagliflozin exposures, changes in insulin dose and mean daily glucose, and their joint effect on HbA1c lowering. Such a framework allowed for the evaluation of insulin titration on changes in HbA1c time course. As expected, a greater magnitude of the percentage change from baseline HbA1c resulted from a stable insulin regimen (30% greater decrease), relative to an adjusted insulin regimen. The semi-mechanistic model provided comparable efficacy predictions for a 2.5-mg dose of empagliflozin relative to the descriptive model and the effect observed in EASE-3. Using the models to simulate the outcome of a 2.5 mg dose in the EASE-2 study population provided supportive evidence of the efficacy of a low dose of empagliflozin. 2.5 mg in patients with T1D, illustrating how pharmacometric analyses can support efficacy assessments in the context of limited data.59
Added Benefits
In recent years, the treatment goals of patients with diabetes have been broadened from mere glycaemia control to cardiovascular protection. Tight glucose control has been shown to reduce the risk of renal complications in T1D. No specific interventions that can reduce the progression of kidney disease have been approved since 2001, when angiotensin-converting enzyme inhibitors and angiotensin-II receptor blockers were recommended for this purpose.
Among non-glycaemic benefits, in subjects with T2D, both cardiovascular and renal outcomes have been established to improve with SGLT2i.60 In a recent American and European consensus, it was established that, nevertheless, there are very few data on people with T1D, and SGLT2i have shown benefits in renal and heart failure in people without diabetes, suggesting that patients with T1D harboring these comorbidities could also be helped by this therapy.61 Additionally, a meta-analysis demonstrated both kidney and eye protection related to SGLT2i, with a reduction in albuminuria and risk of diabetic eye disorders. These positive benefits were associated with an improvement in continuous glucose monitoring rather than in HbA1c.62
Kidney and Systemic Complications
The effect of 24 weeks of empagliflozin treatment on urine albumin-to-creatinine ratio (UACR) in patients with T2D and either microalbuminuria or macroalbuminuria was evaluated in patients who participated in one of the five phase 3 randomized placebo-controlled clinical trials with primary endpoints related to glucose lowering. Treatment with empagliflozin significantly reduced UACR in patients with microalbuminuria (−32% vs placebo) or macroalbuminuria (−41% vs placebo). Most of the UACR-lowering effects were not explained by improvements in HbA1c, SBP, or weight.63 In the post-hoc pooled analysis of the DEPICT studies, the effect of dapagliflozin as an adjunct to insulin on the UACR and the estimated glomerular filtration rate (eGFR) was investigated in a subgroup of participants with T1D and albuminuria (UACR ≥30 mg/g) at baseline. In this study, dapagliflozin used as an adjunct to insulin resulted in a reduction in UACR in individuals with T1D and baseline albuminuria, and this effect appeared to be dose dependent.64 Laursen et al aimed to evaluate the acute effects of SGLT2 inhibition on renal oxygenation evaluated by MRI in individuals with T1D and albuminuria. The authors hypothesised that renal oxygenation could be improved within six hours, as previous studies have demonstrated rapid plasma uptake of dapagliflozin and subsequent dose-dependent induction of glucosuria. Dapagliflozin significantly reduced at MRI the renal cortical R2* (corresponding to an improved oxygenation) compared to placebo after six hours. This occurred without differences between dapagliflozin and placebo in blood oxygenation, renal tissue perfusion, renal blood flow, autonomic nerve function, or mitochondrial energy production. These findings are consistent with the hypothesis that acute inhibition of SGLT2 improves renal cortical oxygenation by reducing energy expenditure by inhibiting oxygen-demanding glucose and sodium cotransport in the renal proximal tubule. This improved oxygenation may contribute to the long-term renal beneficial effects of SGLT2i.65 Sotagliflozin, in addition to renal inhibition of SGLT2 and its effect on UGE, reduces postprandial hyperglycemia by reducing glucose absorption via local SGLT1 in the gut.66 In a 52-week pooled analysis, 1575 adults enrolled in the Tandem1 and Tandem2 trials were randomized to Sotagliflozin 200 mg, 400 mg, or placebo in addition to optimized insulin therapy.67 Sotagliflozin showed beneficial effects on clinical parameters of cardiorenal health such as GFR, UACR, blood pressure, hematocrit, serum albumin, and uric acid.64 Stougaard et al performed a simulation analysis to estimate the risk of CVD and ESKD in persons with T1D with and without SGLTi treatment using the Steno T1 Risk Engines. The engines are based on detailed clinical data from Danish electronic health records of approximately 5000 individuals with T1D treated at Steno Diabetes Centre Copenhagen in combination with data from the Danish National Patient Register and Cause of Death Register. The authors found a significant reduction in CVD and ESKD risk, especially in the subgroup with albuminuria.68
In a 12-week, prospective, double-blind randomized clinical study, 40 male patients with T1D have been studied for the possible effects of empagliflozin on top of metformin treatment on endothelial function and arterial stiffness parameters. Empagliflozin, metformin and empagliflozin/metformin significantly improved endothelial function and to a comparable level. Arterial stiffness was maximally decreased in the group treated with the empagliflozin/metformin.69
The EASE (Empagliflozin as Adjunctive to inSulin thErapy) program in patients with T1D showed at 26 weeks (EASE-2) and 52 weeks (EASE-3) a weight loss (up to 23.4 kg), an increased glucose time in range (up to +3 h/day), and reductions in insulin need (up to 213%) and blood pressure (up to 23.9 mmHg for systolic).12
Liu et al performed a post hoc metabolomic analysis on plasma and urine samples from participants in the ATIMRA trial. This 8-week, single-armed open-label pilot study was designed to determine the effect of empagliflozin on renal hyperfiltration in subjects with T1D. The tricarboxylic acid (TCA) cycle, the biosynthesis of unsaturated fatty acids, butanoate, propanoate, and alanine, aspartate, and glutamate metabolites increased after empagliflozin treatment under clamped euglycemia. In addition, plasma pyruvate levels were significantly reduced after empagliflozin treatment. Empagliflozin significantly affected metabolites associated with the TCA cycle and lipid metabolism, while altering metabolic responses to hyperglycemia, indicating a potential change in the use of metabolic substrates.70
Iatrogenic hypoglycemia (IAH) is the most common acute complication of insulin therapy in T1D. Fifteen patients with T1D and IAH were included in a randomized double-blind, placebo-controlled cross-over trial.71 The patients were treated with dapagliflozin 10 mg once a day or matching placebo, with a washout period of 2 weeks. At the end of each treatment period, participants underwent a modified hyperinsulinaemic normoglycemic- hypoglycemic glucose clamp. Blinded continuous glucose monitors were used in the final treatment weeks. Eight weeks of dapagliflozin treatment did not restore hypoglycemic awareness in people with T1D and impaired awareness of hypoglycemia but improved some clinical aspects.72 However, it reduced the need for exogenous glucose to maintain hypoglycemia during the clamp.72 Dapagliflozin also reduced HbA1c and improved glucose variability without increasing the frequency of hypoglycaemia or the time spent below the range of normoglycaemia. Shaffer et al73 studied by a euglycemia-hypoglycemia clamp procedure the effects of SGLT2 inhibition on the counterregulatory response to hypoglycemia. Although they found a 32% higher basal glucagon concentration after dapagliflozin treatment, SGLT2 did not restore the glucagon counterregulatory response of glucagon to hypoglycemia. In a randomized, double-blind, crossover design trial, the effects of SGLT2 inhibition on the counterregulatory response to hypoglycemia were evaluated in 22 participants with T1D who received 4 weeks of dapagliflozin 5 mg daily and 4 weeks of placebo. The authors provide evidence that SGLT2 inhibition does not alter the physiological response to hypoglycemia, improve recovery from hypoglycemia, or improve cognitive function during episodes of hypoglycemia.73
Baba et al aimed to elucidate the effects of SGLT2i on the body composition and blood glucose variability of Japanese patients with T1D in a 52-week single-center, open-label, single-arm interventional study. Participants received a 50 mg daily dose of ipragliflozin, and their insulin dose was reduced by 10–20% prior to ipragliflozin administration to avoid hypoglycemia. In this study, body weight decreased rapidly after the administration of the SGLT2i, and this reduction was maintained for a long time. Glycaemic variability, represented by standard deviation and mean amplitude of glucose excursion (MAGE), also decreased with the administration of the SGLT2i. There were no notable changes in total body water between 12 and 52 weeks. Ipragliflozin decreased fat mass, muscle mass, and bone mineral content. Compared to baseline, the reduction ratio indicates that total fat mass is the dominant factor, which is affected by the use of SGLT2i.74
In a recent meta-analysis, no differences were observed for cardiovascular, metabolic, and safety outcomes between SGLT1/2 inhibitors and SGLT2 inhibitors in patients with T1D.75
Real-World Data
The Diabetes Prospective Follow-up Registry DPV (Diabetes-Patienten-Verlaufsdokumentation) has followed patients with diabetes since 1995. DPV data on patients with all T1D (regardless of their disease stage and treatment strategy) are collected every 6 months from centres in Germany, Austria and Switzerland using DPV software, and the anonymized data are sent to the University of Ulm. In this observational trial in clinical practice, the selection of patients with T1D for SGLT2i treatment appears to be triggered primarily by the presence of higher HbA1c and BMI in combination with the requirement for higher insulin doses, higher blood pressure, and the presence of microalbuminuria. This pre-selection of patients may also explain in part the somewhat larger reductions in HbA1c in this real-world evidence study compared to the results of controlled licensing trials of SGLT2is in T1D. The authors concluded that the overall use of SGLT2is in adults with T1D is rare in real-world clinical practice.72
A retrospective cohort study in two European centers evaluated the efficacy and safety of SGLT2i treatment in T1D.76 During 12 months, the use of SGLT2i was associated with significant reductions in HbA1c, body weight, and daily insulin requirements among individuals with baseline HbA1c >8.0%. Fifty-seven individuals (28.6%) reported adverse events: 45 with genital infections (22.6%), 5 ketosis episodes (2.5%), and 7 DKA (3.5%).76
Fallatah et al reported a real-world clinical experience in the off-label use of empagliflozin in Saudi patients with T1D. They have shown a significant reduction in HbA1c of 0.8% from baseline after a mean follow-up duration of treatment of 15 months. Moreover, there was an average non-significant weight reduction of 1.7 kg, but a significant reduction in the total daily insulin dose of 2.9 units.77
Edwards et al recently conducted a retrospective cohort study of all instances of GLP-1 RA and SGLT2i use as adjuvant therapy by people with T1D in a single, large academic institution. While SGLT2i demonstrated efficacy in improving HbA1c and reducing the basal insulin dose, no weight reductions or the total daily dose of insulin demonstrated in clinical trials were observed in this real-world cohort. GLP-1RAs were initiated most frequently for weight loss and improved glycemic control, while SGLT2i were initiated most frequently for improved glycemic control, reduced insulin dose, and reduced glucose variability.78
Adverse Events
Although SGLTi therapy has shown improvements in glycaemic control, weight loss, and other risk reductions, several studies have documented an important increase in the risk of DKA,3–5 a serious and life-threatening adverse event of these drugs. Ketosis is defined as increased levels of ketones (b-hydroxybutyrate and acetoacetate) in the blood or urine, and ketoacidosis is ketosis associated with anion gap metabolic acidosis. DKA is generally associated with hyperglycemia in individuals with diabetes and serum ketones >3.0 mmol/L.
Based on the pharmacology and physiology of SGLT2i, some mechanisms involved in the development of DKA can be suggested. On the one hand, the reduction of total daily insulin doses may cause a decrease in inhibiting lipolysis and ketogenesis. On the other hand, SGLT2i induces an increase in glucagon, which increases lipolysis and ketogenesis. SGLT2i has also been proposed to decrease the excretion of ketone bodies.48,79 In a recent meta-analysis and meta-regression, it has been demonstrated that the risk of DKA was determined by four independent predictors: BMI and baseline insulin resistance (defined by an estimated glucose disposal rate) explained 86% of the variance. In particular, the risk of DKA began with BMI more than 27 kg/m², which coincides with the cut-off of the indication for SGLT2i. Furthermore, during insulin dose down-titration, the risk of DKA was related to individual insulin sensitivity at baseline: the higher the insulin resistance, the more cautious the reduction in total insulin dose should be to prevent inhibition of lipolysis and ketogenesis. Finally, volume depletion, together with insulin reduction, represented a trigger for DKA, through the activation of the catecholamine and corticosterone axis and increased lipolysis of adipose tissue.62 Other recognized risk factors for DKA associated with SGLT2i therapy were reduced or inconsistent carbohydrate intake, excessive alcohol use, illicit drugs, viral or bacterial infection, vomiting, insulin pump or infusion site failure.48 Thus, patients to candidate to SGLT2i therapy needed to be adequately selected to mitigate the associated risk of DKA. Briefly, it was recommended to adjust the appropriate insulin dose to avoid insulinopaenia, starting with a low dose of SGLT2i, and to measure ketone levels with prompt action to address elevated values as sensible precautions.48 Recently, Stougaard et al calculated the incidence of DKA in people with T1D treated with SGLT2i in Denmark. From a population of 10.500, they observed 134 people treated with SGLT2i over a total period of 222 patient-years and median duration of treatment was 12 months. They found that none of the participants developed DKA during treatment.68
Beyond DKA, other adverse events have been demonstrated with SGLTi therapy. Both dapagliflozin and sotagliflozin can cause intravascular volume depletion, which may sometimes manifest as symptomatic hypotension or acute transient changes in creatinine. This effect is particularly evident in patients with renal failure, the elderly, in patients with low systolic blood pressure, and in patients on diuretics. Serious urinary tract infections, including urosepsis and pyelonephritis, that require hospitalization have been reported in patients receiving SGLT2i, including dapagliflozin and sotagliflozin. In addition, genital mycotic infections are higher with this therapy. Dapagliflozin can increase the risk of hypoglycemia when combined with insulin or an insulin secretagogue. Therefore, a lower dose of insulin or insulin secretagogue may be required to minimize the risk of hypoglycemia when these agents are used in combination with dapagliflozin. Common adverse reactions to sotagliflozin are gastrointestinal disorders, such as diarrhoea and flatulence, and serum lipids increased. One of the most common adverse reactions associated with dapagliflozin was nasopharyngitis. Reports of necrotizing fasciitis of the perineum (Fournier’s Gangrene), a rare but serious and life-threatening necrotizing infection that requires urgent surgical intervention, have been identified in post-marketing surveillance in patients with diabetes mellitus receiving SGLT2i, including dapagliflozin and sotagliflozin. To prevent serious outcomes, including hospitalization, multiple surgeries, and death, it has been indicated to evaluate patients who present with pain or tenderness, erythema, or swelling in the genital or perineal area, and with fever. Finally, an increase in cases of lower limb amputation (primarily of the toe) has been observed in clinical studies with sotagliflozin.80,81
Recently, Zou et al studied by a meta-analysis the safety of sotagliflozin in patients with T1D and T2D. They confirmed that in T1D sotagliflozin could increase the risk of genital mycotic infection, acidosis-related adverse events, diarrhoea, and volume depletion. Table 2 shows a resume of all adverse events of dapagliflozin and sotagliflozin. Speculatively, the use of a dose of 200 mg instead of 400 mg for sotagliflozin and a 5-mg rather 10-mg dose of 5 mg instead of 10 mg for dapagliflozin could help limit unwanted effects.82
 |
Table 2 Clinical Characteristics of Dapagliflozin and Sotagliflozin |
Association Therapy
Since both GLP-1RA and SGLT2i show efficacy in improving glycaemic controls as adjunctive treatment in T1D, very few studies investigated the combination of the two therapies in addition to insulin.
Two large multicentre phase three trials, ADJUNCT ONE and ADJUNCT TWO, investigated the long-term effects and safety of adding a Glucagon-like peptide 1 receptor agonists (GLP-1RA), liraglutide to insulin for the treatment of T1D.17,18 In ADJUNCT ONE, after 20 weeks Hb1Ac was of 0.8% in the liraglutide 1.8 mg versus the placebo group with a corresponding mean reduction in body weight reduction of 4.9 kg. In ADJUNCT TWO, there was a statistically significant reduction in mean HbA1c in the liraglutide groups versus placebo (placebo-corrected reduction −0.35%, for dose 1.8 mg), at week 26 and a mean body weight reduction in a dose-dependent manner (−5.1 Kg for dose 1.8 mg) versus placebo (−0.2 kg).83,84
In an RCT that enrolled 26 patients for 12 weeks, it was investigated whether dapagliflozin addition to an already established regimen of insulin and liraglutide results in a significant improvement in glycemia and body weight. In the triple therapy group, HbA1c decreases by 0.66%, versus the placebo group, with an unchanged incidence of hypoglycemia and a body weight decrease in 1.9 kg versus placebo.35
Further studies are currently being conducted with a combination of exenatide and dapagliflozin and a combination of semaglutide and dapagliflozin to determine whether this approach would yield better outcomes. These trials could also settle the DKA risk in patients undergoing triple therapy. Incoming and ongoing clinical trials are shown in Table 3.
 |
Table 3 Ongoing Clinical Trial on SGLT2 Inhibitors in T1D |
Conclusion
SGLT2i potentially addresses some of the unmet needs associated with T1D by improving glycaemic control with weight loss and without increasing hypoglycemia, by reducing glycaemic variability. Further studies will be needed to determine the safety of this therapy in T1D or pre-T1D and to define the type of patient who can benefit most from these medications. In the project of next clinical trials, patients’ inclusion criteria should be carefully defined in order to reduce the adverse events. Treatment of T1D has to consider all the available medications and introduces a risk-benefit estimation tool that permits 1) to select patients that benefit most from SGLT2i therapy (ie, individuals with higher glycated haemoglobin and higher body mass index); 2) to weigh carefully risk and benefits on cardiovascular, renal and metabolic comorbidities and 3) to exclude groups at greatest risk. The trial design also has to consider the use of the lowest dose of SGLT2i and the possible combination with other glucose-lowering agents. The introduction of new trial designs of personalized medicine concepts will allow a reduction in adverse events and an increase in confidence in prescribing SGLT2i in T1D patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funds were used to write this manuscript.
Disclosure
Professor Luca Busetto reports personal fees from Novonordisk, Ely Lilly, Pfizer, Rhythm Pharmaceuticals, Bruno Farmaceutici, and Pronokal, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. EMA. New add-on treatment to insulin for treatment of certain patients with type 1 diabetes. Available from: https://www.ema.europa.eu/en/news/new-add-treatment-insulin-treatment-certain-patients-type-1-diabetes.
2. EMA. First oral add-on treatment to insulin for the treatment of certain patients with type 1 diabetes. Available from: https://www.ema.europa.eu/en/documents/press-release/first-oral-add-treatment-insulin-treatment-certain-patients-type-1-diabetes_.
3. Dandona P, Mathieu C, Philip M, et al. Efficacy and safety of dapagliflozin in patients with inadequately controlled type 1 diabetes (DEPICT-1): 24 week results from a multicentre, double-blind, phase 3, randomised controlled trial. Lancet Diabetes Endocrinol. 2017;11(5):864–876. doi:10.1016/S2213-8587(17)30308-X
4. Mathieu C, Dandona P, Gillard P, et al. Efficacy and safety of dapagliflozin in patients with inadequately controlled type 1 diabetes (the DEPICT-2 Study): 24-week results from a randomized controlled trial. Diabetes Care. 2018;41(9):1938–1946. doi:10.2337/dc18-0623
5. Garg SK, Henry RR, Banks P. Effects of sotagliflozin added to insulin in patients with type 1 diabetes. N Engl J Med. 2017;377(24):2337–2348. doi:10.1056/NEJMoa1708337
6. AstraZeneca. Update on US regulatory decision for Forxiga in type-1 diabetes. Available from: https://www.astrazeneca.com.
7. NICE. NICE technology appraisal guidance TA597. Dapagliflozin with insulin for treating type 1 diabetes. Available from: https://www.nice.org.uk/guidance/ta597.
8. AIFA. Forxiga (dapagliflozin) 5mg should no longer be used for the treatment of Type 1 Diabetes Mellitus. Available from: https://www.aifa.gov.it/documents/20142/1313724/2021.10.29_NII_FORXIGA-dapagliflozin_EN.pdf.
9. EMA. Zynquista (sotagliflozin) An overview of Zynquista and why it is authorised in the EU; 2019. Available from: https://www.ema.europa.eu/en/documents/overview/zynquista-epar-medicine-overview_en.pdf.
10. Sanofi. FDA issues Complete Response Letter for Zynquista (sotagliflozin). Available from: http://www.news.sanofi.us/2019-03-22-FDA-issues-Complete-Response-Letter-for-Zynquista-TM-sotagliflozin.
11. EMA. Zynquista. Withdrawal of the marketing authorisation in the European Union. Available from: https://www.ema.europa.eu/en/documents/public-statement/public-statement-zynquista-withdrawal-marketing-authorisation-european-union_en.pdf.
12. Rosenstock J, Marquard J, Laffel LM, et al. Empagliflozin as adjunctive to insulin therapy in type 1 diabetes: the EASE trials. Diabetes Care. 2018;12(41):2560–2569. doi:10.2337/dc18-1749
13. Pasqua MR, Jafar A, Kobayati A, et al. Low-dose empagliflozin as adjunct to hybrid closed-loop insulin therapy in adults with suboptimally controlled type 1 diabetes: a randomized crossover controlled trial. Diabetes Care. 2023;1(46):165–172. doi:10.2337/dc22-0490
14. Diabetes.co.uk, FDA rejects approval of empagliflozin for type 1 diabetes. Available from: https://www.diabetes.co.uk/news/2019/Nov/fda-rejects-approval-of-empagliflozin-for-type-1-diabetes.html.
15. Scheen AJ. Pharmacodynamics, efficacy and safety of sodium–glucose co-transporter type 2 (SGLT2) Inhibitors for the Treatment of Type 2 Diabetes Mellitus. Drugs. 2015;75(1):33–59. doi:10.1007/s40265-014-0337-y
16. A.j S. Pharmacokinetics, Pharmacodynamics and Clinical Use of SGLT2 Inhibitors in Patients with Type 2 Diabetes Mellitus and Chronic Kidney Disease. Clin Pharmacokinet. 2015;54(7):691–708. doi:10.1007/s40262-015-0264-4
17. Dapaglifozin Compound summary PubChem. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Dapagliflozin.
18. Canaglifozin compound summary pubchem. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Canagliflozin.
19. Empaglifozin Compound summary Pubchem. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Empagliflozin#:~:text=Empagliflozin%20is%20a%20C%2Dglycosyl,group%20at%20the%20anomeric%20centre.
20. Alkabbani W, Gamble JM. Profile of Ipragliflozin, an oral SGLT-2 inhibitor for the treatment of type 2 diabetes: the evidence to date drug design. Dev Ther. 2021;5:3057–3069. doi:10.2147/DDDT.S281602
21. Vallon V, Gerasimova M, Rose MA, et al. SGLT2 inhibitor empagliflozin reduces renal growth and albuminuria in proportion to hyperglycemia and prevents glomerular hyperfiltration in diabetic Akita mice. Am J Physiol Renal Physiol. 2014;306(2):194–204. doi:10.1152/ajprenal.00520.2013
22. Song P, Huang W, Onishi A, et al. Knockout of Na+-glucose cotransporter SGLT1 mitigates diabetes-induced upregulation of nitric oxide synthase NOS1 in the macula densa and glomerular hyperfiltration. Am J Physiol Renal Physiol. 2019;1(317):207–217. doi:10.1152/ajprenal.00120.2019
23. Huang F, Zhao Y, Wang Q, et al. Dapagliflozin attenuates renal tubulointerstitial fibrosis associated with type 1 diabetes by regulating STAT1/TGFβ1 signaling. Front Endocrinol. 2019;10(441). doi:10.3389/fendo.2019.00441
24. Cheng ST, Chen L, Li SY, et al. The Effects of Empagliflozin, an sglt2 inhibitor, on pancreatic β-cell mass and glucose homeostasis in type 1 diabetes. PLoS One. 2016;11(1). doi:10.1371/journal.pone.0147391
25. Zhang B, Zhai M, Li B, et al. Honokiol ameliorates myocardial ischemia/reperfusion injury in type 1 diabetic rats by reducing oxidative stress and apoptosis through activating the SIRT1-Nrf2 signaling pathway. Oxid Med Cell Longev. 2018;2018. doi:10.1155/2018/3159801
26. Jiang K, Xu Y, Wang D, et al. Cardioprotective mechanism of SGLT2 inhibitor against myocardial infarction is through reduction of autosis. Protein Cell. 2022;13(5):336–359. doi:10.1007/s13238-020-00809-4
27. Terasaki M, Hiromura M, Mori Y. Amelioration of hyperglycemia with a sodium-glucose cotransporter 2 inhibitor prevents macrophage-driven atherosclerosis through macrophage foam cell formation suppression in type 1 and type 2 diabetic mice. PLoS One. 2015;10(11):e0143396. doi:10.1371/journal.pone.0143396
28. Yang L, Zhang X, Wang Q, et al. Effects and mechanisms of SGLT2 inhibitors on the NLRP3 inflammasome, with a focus on atherosclerosis. Front Endocrinol. 2022;13. doi:10.3389/fendo.2022.992937
29. Eid SA, O’Brien PD, Hinder LM, et al. Differential effects of empagliflozin on microvascular complications in murine models of type 1 and type 2 diabetes. Biology. 2020;9(11):347. doi:10.3390/biology9110347
30. Veelen A, Andriessen C, Op den Kamp Y. “Effects of the sodium-glucose cotransporter 2 inhibitor dapagliflozin on substrate metabolism in prediabetic insulin resistant individuals: a randomized, double-blind crossover trial”. Metabolism. 2023;140:155396. PMID: 36592688. doi:10.1016/j.metabol.2022.155396
31. Clemmensen KKB, Blond MB, Amadid H, et al. No effects of dapagliflozin, metformin or exercise on plasma glucagon concentrations in individuals with prediabetes: a post hoc analysis from the randomized controlled PRE-D trial. Diabetes Obes Metab. 2021;23(2):530–539. PMID: 33146457.
32. Mori Y, Duru OK, Et Al TKR. Sodium-glucose cotransporter 2 inhibitors and new-onset type 2 diabetes in adults with prediabetes: systematic review and meta-analysis of randomized controlled trials. J Clin Endocrinol Metab. 2022;108(1):221–231. PMID: 36217306. doi:10.1210/clinem/dgac591
33. Mudaliar S, Armstrong DA, Mavian AA, et al. Remogliflozin etabonate, a selective inhibitor of the sodium-glucose transporter 2, improves serum glucose profiles in type 1 diabetes. Diabetes Care. 2012;35(11):2198–2200. doi:10.2337/dc12-0508
34. Henry RR, Rosenstock J, s E, et al. Exploring the potential of the SGLT2 inhibitor dapagliflozin in type 1 diabetes: a randomized, double-blind, placebo-controlled pilot study. Diabetes Care. 2015;38(3):412–419. doi:10.2337/dc13-2955
35. Kuhadiya ND, Ghanim H, Mehta A, et al. Dapagliflozin as additional treatment to liraglutide and insulin in patients with type 1 diabetes. J Clin Endocrinol Metab. 2016;101(9):3506–3515. doi:10.1210/jc.2016-1451
36. Melmer A, Kempf P, Lungen L, et al. Short-term effects of dapagliflozin on insulin sensitivity, postprandial glucose excursion and ketogenesis in type 1 diabetes mellitus: a randomized, placebo-controlled, double blind, cross-over pilot study. Diabetes Obes Metab. 2018;20(11):2685–2689. doi:10.1111/dom.13439
37. Watada H, Shiramoto M, Ueda S, et al. Pharmacokinetics and pharmacodynamics of dapagliflozin in combination with insulin in Japanese patients with type 1 diabetes. Diabetes Obes Metab. 2019;21(4):876–882. doi:10.1111/dom.13593
38. Parkinson J, Weifeng T, Magnus A, et al. Model-based characterization of the relationship between dapagliflozin systemic exposure and HbA1c response in patients with type 1 diabetes mellitus. Diabetes Obes Metab. 2018;2018:1.
39. Phillip M, Mathieu C, Lind M, et al. Long-term efficacy and safety of dapagliflozin in patients with inadequately controlled type 1 diabetes: pooled 52-week outcomes from the DEPICT-1 and −2 studies. Diabetes Obes Metab. 2021;23(2):549–560. doi:10.1111/dom.14248
40. Biester T, Muller I, von Dem Berge T, et al. Add-on therapy with dapagliflozin under full closed loop control improves time in range in adolescents and young adults with type 1 diabetes: the DAPADream study. Diabetes Obes Metab. 2021;23(2):599–608. doi:10.1111/dom.14258
41. Araki E, Watada H, Uchigata Y, et al. Efficacy and safety of dapagliflozin in Japanese patients with inadequately controlled type 1 diabetes (DEPICT-5): 52-week results from a randomized, open-label, Phase III clinical trial. Diabetes Obes Metab. 2020;22(4):540–548. doi:10.1111/dom.13922
42. Hamaguchi M, Hashimoto Y, Tanaka T, et al. multicenter, open-label, 2-arm, pilot trial for safe reduction of basal insulin dose combined with SGLT2 inhibitor in type 1 diabetes mellitus: study protocol for a RISING-STAR trial. Clin Med Insights Endocrinol Diabetes. 2021;14:117955142110405. doi:10.1177/11795514211040539
43. Urakami T, Yoshida K, Suzuki J. Efficacy of low-dose dapagliflozin in young people with type 1 diabetes. Intern Med. 2023;62(2):177–186. doi:10.2169/internalmedicine.9632-22
44. Sands AT, Zambrowicz BP, Rosenstock J, et al. Sotagliflozin, a dual SGLT1 and SGLT2 inhibitor, as adjunct therapy to insulin in type 1 diabetes. Diabetes Care. 2015;38(7):1181–1188. doi:10.2337/dc14-2806
45. Zambrowicz B, Freiman J, Brown PM. LX4211, a dual SGLT1/SGLT2 inhibitor, improved glycemic control in patients with type 2 diabetes in a randomized, placebo-controlled trial. Clin Pharmacol Ther. 2012;92(2):158–169. doi:10.1038/clpt.2012.58
46. Buse JB, Garg SK, Rosenstock J, et al. Sotagliflozin in combination with optimized insulin therapy in adults with type 1 diabetes: the North American inTandem1 study. Diabetes Care. 2018;41(9):1970–1980. doi:10.2337/dc18-0343
47. Danne T, Cariou B, Buse JB, et al. HbA1c and hypoglycemia reductions at 24 and 52 weeks with sotagliflozin in combination with insulin in adults with type 1 diabetes: the European inTandem2 study. Diabetes Care. 2018;41(9):1981–1990. doi:10.2337/dc18-0342
48. Danne T, Cariou B, Buse P, et al. Improved time in range and glycemic variability with sotagliflozin in combination with insulin in adults with type 1 diabetes: a pooled analysis of 24-week continuous glucose monitoring data from the inTandem program. Diabetes Care. 2019;42(5):919–930. doi:10.2337/dc18-2149
49. Baker C, Wason S, Banks P, et al. ”Dose-dependent glycometabolic effects of sotagliflozin on type 1 diabetes over 12 weeks: the inTandem4 trial. Diabetes Obes Metab. 2019;21(11):2440–2449. doi:10.1111/dom.13825
50. Henry RR, Thakkar P, Tang C, et al. Efficacy and safety of canagliflozin, a sodium-glucose cotransporter 2 inhibitor, as add-on to insulin in patients with type 1 diabetes. Diabetes Care. 2015;38(12):2258–2265. doi:10.2337/dc15-1730
51. Rodbard HW, Peters AL, Slee A, et al. The effect of canagliflozin, a sodium glucose cotransporter 2 inhibitor, on glycemic end points assessed by continuous glucose monitoring and patient-reported outcomes among people with type 1 diabetes. Diabetes Care. 2017;40(2):171–180. doi:10.2337/dc16-1353
52. Kaku K, Isaka H, Toyoshima J, et al. Clinical pharmacology study of ipragliflozin in Japanese patients with type 1 diabetes mellitus: a phase 2, randomized, placebo-controlled trial. Diabetes Obes Metab. 2019;21(6):1445–1454. doi:10.1111/dom.13679
53. Kaku K, Isaka H, Sakatani T, et al. Efficacy and safety of ipragliflozin add-on therapy to insulin in Japanese patients with type 1 diabetes mellitus: a randomized, double-blind, phase 3 trial. Diabetes Obes Metab. 2019;21(10):2284–2293. doi:10.1111/dom.13807
54. Shimoda M, Mashiko A, Katakura Y, et al. Efficacy and safety of adding ipragliflozin to insulin in Japanese patients with type 1 diabetes mellitus: a retrospective study. Endocr J. 2021;68(12):1455–1461. doi:10.1507/endocrj.EJ21-0161
55. Perkins BA, Cherney DZ, Partridge H, et al. Sodium-glucose cotransporter 2 inhibition and glycemic control in type 1 diabetes: results of an 8-week open-label proof-of-concept trial. Diabetes Care. 2014;37(5):1480–1483. doi:10.2337/dc13-2338
56. Pieber TR, Famulla S, Eilbracht J, et al. Empagliflozin as adjunct to insulin in patients with type 1 diabetes: a 4-week, randomized, placebo-controlled trial (EASE-1. Diabetes Obes Metab. 2015;17(10):928–935. doi:10.1111/dom.12494
57. Shimada A, Hanafusa T, Yasui A, et al. Empagliflozin as adjunct to insulin in Japanese participants with type 1 diabetes: results of a 4-week, double-blind, randomized, placebo-controlled phase 2 trial. Diabetes Obes Metab. 2018;20(9):2190–2199. doi:10.1111/dom.13351
58. Haidar A, Yale JF, Lovblom LE, et al. Reducing the need for carbohydrate counting in type 1 diabetes using closed-loop automated insulin delivery (artificial pancreas) and empagliflozin: a randomized, controlled, non-inferiority, crossover pilot trial. Diabetes Obes Metab. 2021;23(6):1272–1281. doi:10.1111/dom.14335
59. Johnston CK, Eudy-Byrne RJ, Elmokaden A, et al. A Model-Informed Drug Development (MIDD) approach for a low dose of empagliflozin in patients with type 1 diabetes. Pharmaceutics. 2021;13(4):485. doi:10.3390/pharmaceutics13040485
60. Zelniker TA, Wiviott SD, Roz I, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019;393(10166):31–39. doi:10.1016/S0140-6736(18)32590-X
61. Holt RIG, DeVnes JH. The management of type 1 diabetes in adults. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2021;64(12):2609–2652. doi:10.1007/s00125-021-05568-3
62. Musso G, Sircana A, Saba F, et al. Assessing the risk of ketoacidosis due to sodium-glucose cotransporter (SGLT)-2 inhibitors in patients with type 1 diabetes: a meta-analysis and meta-regression. PLoS Med. 2020;17(12):e1003461. doi:10.1371/journal.pmed.1003461
63. Cherney D, Lund SS, Perkins BA, et al. The effect of sodium glucose cotransporter 2 inhibition with empagliflozin on microalbuminuria and macroalbuminuria in patients with type 2 diabetes. Diabetologia. 2016;59(9):1860–1870. doi:10.1007/s00125-016-4008-2
64. Groop PH, Phillip M DP, Phillip M, et al. Effect of dapagliflozin as an adjunct to insulin over 52 weeks in individuals with type 1 diabetes: post-hoc renal analysis of the DEPICT randomised controlled trials. Lancet Diabetes Endocrinol. 2020;8(10):845–854. doi:10.1016/S2213-8587(20)30280-1
65. Laursen JC, Søndergaard-Heinrich N, de Melo JML, et al. Acute effects of dapagliflozin on renal oxygenation and perfusion in type 1 diabetes with albuminuria: a randomised, double-blind, placebo-controlled crossover trial. EClinicalMedicine. 2021;37:100895. doi:10.1016/j.eclinm.2021.100895
66. Lapuerta P, Zambrowicz B, Strumph P, et al. Development of sotagliflozin, a dual sodium-dependent glucose transporter 1/2 inhibitor. Diab Vasc Dis Res. 2015;12(2):101–110. doi:10.1177/1479164114563304
67. van Raalte DH, Bjornstand P, Persson F, et al. The impact of sotagliflozin on renal function, albuminuria, blood pressure, and hematocrit in adults with type 1 diabetes. Diabetes Care. 2019;42(10):1921–1929. doi:10.2337/dc19-0937
68. Stougaard EB, Rossing P, Cherney D, et al. Sodium-glucose cotransporter 2 inhibitors as adjunct therapy for type 1 diabetes and the benefit on cardiovascular and renal disease evaluated by Steno risk engines. J Diabetes Complications. 2022;36(8):108257. doi:10.1016/j.jdiacomp.2022.108257
69. Lunder M, Janić M, Japelj M, et al. Empagliflozin on top of metformin treatment improves arterial function in patients with type 1 diabetes mellitus. Cardiovasc Diabetol. 2018;17(1):153. doi:10.1186/s12933-018-0797-6
70. Liu H, Shidhar VS, Montemayor D, et al. Changes in plasma and urine metabolites associated with empagliflozin in patients with type 1 diabetes. Diabetes Obes Metab. 2021;23(11):2466–2475. doi:10.1111/dom.14489
71. van Meiel L, Skidhar VS, Montemayor D. Effect of short-term use of dapagliflozin on impaired awareness of hypoglycaemia in people with type 1 diabetes. Diabetes Obes Metab. 2021;2021:3.
72. Seufert J, Lanzinger S, Danne T, et al. Real-world data of 12-month adjunct sodium-glucose co-transporter-2 inhibitor treatment in type 1 diabetes from the German/Austrian DPV registry: improved HbA1c without diabetic ketoacidosis. Diabetes Obes Metab. 2022;24(4):742–746. doi:10.1111/dom.14620
73. Shafer B, Gregory J, Giovanetti E, et al. SGLT2 inhibition increases fasting glucagon but does not restore the counterregulatory hormone response to hypoglycemia in participants with type 1 diabetes. Diabetes. 2022;2022:4.
74. Baba Y, Ishibashi R, Takasaki A, et al. Effects of sodium glucose co-transporter 2 inhibitors in type 1 diabetes mellitus on body composition and glucose variabilities: single-arm, exploratory trial. Diabetes Ther. 2021;12(5):1415–1427. doi:10.1007/s13300-021-01047-5
75. Teo YN, Ting AZH, Teo YH, et al. Effects of Sodium/Glucose Cotransporter 2 (SGLT2) Inhibitors and Combined SGLT1/2 Inhibitors on cardiovascular, metabolic, renal, and safety outcomes in patients with diabetes: a network meta-analysis of 111 randomized controlled trials. Am J Cardiovasc Drugs. 2022;22(3):299–323. doi:10.1007/s40256-022-00528-7
76. Palanca A, van Nes F, Pardo F, et al. Real-world evidence of efficacy and safety of SGLT2 inhibitors as adjunctive therapy in adults with type 1 diabetes: a European two-center experience. Diabetes Care. 2022;45(3):650–658. doi:10.2337/dc21-1584
77. Fallatah W, Brema I, Abbedallah A, et al. Efficacy and Safety of SGLT2 inhibitors as adjunctive treatment in type 1 diabetes in a tertiary care center in Saudi Arabia. Avicenna J Med. 2022;12(1):10–15. doi:10.1055/s-0041-1742196
78. Edwards K, Li X, Lingvay I. Clinical and safety outcomes with GLP-1 receptor agonists and SGLT2 inhibitors in type 1 diabetes: a real-world study. J Clin Endocrinol Metab. 2023;108(4):920–930. doi:10.1210/clinem/dgac618
79. Taylor SI, Blau JE, Rother KI, et al. SGLT2 Inhibitors May Predispose to Ketoacidosis. J Clin Endocrinol Metab. 2015;100(8):2849–2852. doi:10.1210/jc.2015-1884
80. PDF of HIGHLIGHTS OF PRESCRIBING INFORMATION Farxiga. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/202293s020lbl.pdf.
81. Available from: https://www.ema.europa.eu/en/documents/product-information/zynquista-epar-product-information_en.pdf.
82. Zou H, Liu L, Guo J, et al. Sodium–glucose cotransporter inhibitors as add-on therapy in addition to insulin for type 1 diabetes mellitus: a meta-analysis of randomized controlled trials. J Diabetes Investig. 2021;12:546–556.
83. Mathieu C, Zinman B, Hemmingsson JU, et al. Efficacy and safety of liraglutide added to insulin treatment in type 1 diabetes: the ADJUNCT ONE treat-to-target randomized trial. Diabetes Care. 2016;39(10):1702–1710. doi:10.2337/dc16-0691
84. Ahrén B, Hirsh IB, Pieber TR, et al. Efficacy and safety of liraglutide added to capped insulin treatment in subjects with type 1 diabetes: the ADJUNCT TWO randomized trial. Diabetes Care. 2016;39(10):1693–1701. doi:10.2337/dc16-0690
85. Clinicaltrial.gov. Available from: https://clinicaltrials.gov/search?cond=Type%201%20Diabetes%20Mellitus&term=SGLT2-Inhibitors.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.