Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Sex-Based Differences and Risk Factors for Comorbid Nonalcoholic Fatty Liver Disease in Patients with Bipolar Disorder: A Cross-Sectional Retrospective Study
Authors Wang Y, Liu Y ![]() , Zhang X
, Zhang X ![]() , Wu Q
, Wu Q
Received 29 August 2023
Accepted for publication 31 October 2023
Published 6 November 2023 Volume 2023:16 Pages 3533—3545
DOI https://doi.org/10.2147/DMSO.S428523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Ying Wang,1,2,* Yiyi Liu,1– 3,* Xun Zhang,1– 3 Qing Wu1– 3
1Department of Psychiatry, Affiliated Psychological Hospital of Anhui Medical University, Hefei, People’s Republic of China; 2Anhui Mental Health Center, Hefei Fourth People’s Hospital, Hefei, People’s Republic of China; 3School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qing Wu, Department of Psychiatry, Affiliated Psychological Hospital of Anhui Medical University, 316 Huangshan Road, Hefei, 230022, People’s Republic of China, Tel +8613856919530, Email [email protected]
Purpose: Sex-based differences in patients with bipolar disorders (BD) are well recognized, and it is well known that the prevalence and severity of nonalcoholic fatty liver disease (NAFLD) are both higher in men than in women. Although metabolic disorders such as NAFLD are common in patients with BD, sex differences and risk factors for NAFLD comorbidity in these patients have not been thoroughly explored. This study aimed to investigate sex differences in patients with comorbid NAFLD and BD and associated risk factors.
Methods: This retrospective cross-sectional study included 710 patients with BD. Clinical data of patients with BD, including information on fasting glucose, liver function-related enzymes, relevant lipid data, uric acid, the triglyceride-glucose index (TyG), and demographics, were derived from the hospital electronic medical record system from June 2020 to July 2022. We performed logistic regression analysis and calculated the odds ratios with 95% confidence intervals of factors using t-tests, χ²-tests, and receiver operating characteristic. NAFLD was diagnosed using liver ultrasonography.
Results: The prevalence of NAFLD was higher in male patients with BD than in female patients (50.9% vs 38.5%), and there were significant differences in the years of education and marital status (all P< 0.05). Regression analysis showed that the risk factors for comorbidities were the body mass index (BMI), fasting glucose, and apolipoprotein B levels in male patients and the BMI, bipolar disease course, glutamine transpeptidase levels, and the TyG in female patients.
Conclusion: Sex-based differences exist in risk factors and in the prevalence of comorbid NAFLD among patients with BD. BMI is a sex-independent risk factor, and clinical attention should be targeted to risk factors associated with comorbid NAFLD related to sex, especially in female patients with BD who presenting a high TyG index.
Keywords: sex differences, triglyceride-glucose index, metabolic disorders, prevalence
Corrigendum for this paper has been published.
Introduction
Bipolar disorder (BD) is a serious psychiatric disorder characterized by recurrent episodes of hypomania and depression.1 It has affected over 1% of the global population, regardless of ethnicity, nationality, or socioeconomic status, and generally leads to impaired social functioning, a reduced quality of life, and cognitive impairment.2 It is also one of the leading causes of disability in young people.3 Patients with BD are considerably more likely to develop metabolic syndrome than the general population owing to factors such as antipsychotic use, unhealthy lifestyle, increased obesity rates, and unknown pathogenesis of the disease itself.4,5 Additionally, patients with BD have a higher incidence of comorbid metabolic disorders such as nonalcoholic fatty liver disease (NAFLD) and obesity relative to the general population, and the risk in such patients is often insufficiently assessed, requiring early detection and intervention.5–7
NAFLD is a group of diseases closely associated with obesity and metabolic syndrome,8–10 the second most common liver disease after viral hepatitis,11 and the most common cause of chronic liver disease worldwide.12 The current global prevalence of NAFLD ranges from 6.3% to 45.0%, and the prevalence of NAFLD in Asia (27.4%) is slightly higher than the median (25.2%);13 previous Chinese reports have revealed that the prevalence of NAFLD among patients admitted to hospitals for psychiatric disorders increased yearly, increasing from 16.88% to 19.07% from 2014 to 2018 with an annual growth rate of 0.548%.14 The prevalence of NAFLD among Chinese adults is about 29.2%, with an annual incidence rate of about 5%, as found in a recent epidemiologic survey.15 NAFLD can develop into a form of nonalcoholic steatohepatitis (NASH), characterized by fat accumulation, hepatocellular damage, and oxidative stress. The prevalence of NAFLD is expected to increase annually as the prevalence of obesity, diabetes mellitus, and metabolic syndrome continues to increase globally.16 NAFLD is often observed in conjunction with metabolic disorders such as hypertension, insulin resistance, hyperlipidaemia, and diabetes mellitus.17 Numerous studies have suggested that these factors are closely associated with the development of cardiovascular diseases, such as cardiomyopathy, arrhythmias, and coronary atherosclerosis,18–20 greatly increasing the risk of patients developing multiple diseases and ultimately imposing a huge medical and economic burden on society.21
Significant sex differences in patients with BD have been widely recognized.22,23 Numerous studies have shown that women are more likely to suffer from bipolar II, hypomania, and rapid cycling, while male patients are more likely to be comorbidly substance dependent.24–26 In addition, BD occurs later in women who are more susceptible to the seasonal effects of mood disorders.26 There are also studies that reveal sex-based differences in their comorbidities, with women having a higher incidence of inflammatory diseases such as Crohn’s disease, multiple sclerosis, and asthma than male patients with BD,27 although risk factors for their comorbidities have not been further investigated. Some studies have shown sex-based differences in obesity and metabolic syndrome in patients with schizophrenia but not in bipolar patients,28,29 and some studies have shown sex-based differences in obesity rates in patients with BD.30 Most current studies have mainly investigated sex differences in terms of general demographics, clinical symptoms, and biochemical indicators in patients with BD, while some studies have also preliminarily elaborated on the prevalence of other disorders in patients with comorbidities.31 However, there is still a lack of research on sex differences in and risk factors for comorbid NAFLD in patients with BD. Therefore, the purpose of this large cross-sectional study was to understand the sex-based differences in patients with comorbid NAFLD and BD and to explore the associated risk factors.
Materials and Methods
Research Population
This large cross-sectional study included 710 patients (male/female = 352/358) from June 2020 to July 2022 visiting the Anhui Provincial Mental Health Center. The general demographic data of the patients and the test results were collected anonymously from systematic electronic health records. The inclusion criteria were as followed: 1) diagnosis based on the Diagnostic Criteria of the International Classification of Diseases (ICD-10), 10th revision,32 confirmed by two psychiatrists with attending or higher titles; 2) age limit of 18–60 years; 3) no treatment with hepatoprotective drugs; 4) no history of hepatitis or other diseases that can cause fatty liver; 5) no use of psychiatric drugs and other drugs that could induce NAFLD within the last 3 months; and 6) no history of alcohol use disorder according to the diagnostic criteria. The exclusion criteria were as follows: 1) diagnosis of substance or drug abuse or history of such abuse; 2) pregnant women; 3) neurodegenerative diseases, including congenital neurodevelopmental delay and Alzheimer’s disease; and 4) combination of organic brain disease or severe physical illness. Based on these criteria, 710 patients were included in this study.
This study was performed in line with the principles of the Declaration of Helsinki. The study was approved by the Medical Ethics Committee (AMHC) of Anhui Mental Health Center. Because of the retrospective nature of the study and the fact that all data (including basic personal information and detailed medical records) were collected anonymously and encrypted, the Ethics Committee waived the requirement to obtain informed consent.
Definition and Ultrasound Diagnosis of NAFLD
NAFLD requires imaging or histological confirmation of hepatic steatosis and the absence of other causes of liver fat accumulation, such as genetic disorders, drug use, hepatitis C, or significant alcohol consumption.33 NAFLD was diagnosed by experienced medical personnel on the basis of liver ultrasound examination and medical history. In this research, the ICD-10 code for NAFLD was K76.0. After confirming the diagnosis of hospitalized patients using ICD-10 code K76.0, we further excluded patients with biliary cirrhosis (K74.3-K74.5), autoimmune hepatitis (K75.4), toxic liver disease (K71), viral hepatitis (B15-B19), and alcoholic liver disease (K70).
Blood Biochemistry Collection and Definition of the Triglyceride-Glucose Index
Blood samples were taken from the forearm vein of each patient on the morning of the first day of hospitalization (after 12 h of fasting) by a specialized medical staff. The blood test tubes used for the blood testing were evacuated sterile plastic or polypropylene tubes capable of automatically drawing 3 mL of blood. Sodium/potassium ethylenediaminetetraacetic acid potassium was used as an anticoagulant at a certain concentration (4.55±0.85 mmol/L) because it prevents coagulation by binding calcium. The samples were processed and analysed by flow cytometry within 30 min of collection by an independent laboratory test department. The triglyceride-glucose index (TyG) was then calculated from the test results using the formula TyG=LN [triglycerides (TG) (mg/dL) × plasma glucose (mg/dL)/2]. Several large studies including control groups have shown that the TyG index ranges from 4.62 ± 0.16 in healthy populations.34
Statistical Analysis
All analyses were performed using SPSS 27.0 (IBM Corp., Armonk, NY, USA). First, descriptive analyses were performed on the general demographic data and test results. Continuous variables that conformed to the normal distribution are expressed as mean±standard deviation (SD), and those that do not conform to the normal distribution were expressed as the median (interquartile range). Categorical variables are expressed as frequencies and percentages (%). A t-test was used for continuous variables that conformed to a normal distribution; otherwise, a Mann–Whitney U-test was used(z). A chi-square analysis was used for categorical variables(x2).
Patients with NAFLD were sub-grouped according to sex and compared to derive indicators of significant differences. A t-test was then performed for patients with or without NAFLD of the same sex, and indicators with significant differences were considered clinically significant and were entered in the multivariate regression analysis model, even if they were not significant in the univariate regression analysis. We performed univariate logistic regression analyses for each variable and then included meaningful variables in multivariate logistic regression analyses to derive possible influences and in this way examined the risk factors for NAFLD. The differences in statistical results between the sex groups were compared, and the analysis provided corrected ratios and established 95% confidence intervals. Data were visualized using GraphPad Prism version 8.0 (GraphPad Software Inc., San Diego, CA, USA). The clinical translational value of the identified risk factors was evaluated by receiver operating characteristic (ROC) curve analysis. The area under the curve (AUC) between 0.5 and 0.6 suggests bad discrimination of the diagnostic test, between 0.6 and 0.7 suggests sufficient discrimination, between 0.7 and 0.8 good discrimination. All statistical tests were two-tailed, and the alpha level was set at 0.05. At P<0.05, the results were considered statistically significant.
Results
Sex-Based Differences in General Demographics and Prevalence
The prevalence of NAFLD was significantly higher in male patients with BD than in female patients (50.9% vs 38.5%, P<0.001), and there was also a significant difference between male and female patients in terms of the years of education (11.34±3.49 vs 10.71±4.68, P<0.05) (Table 1). In terms of marital status, female patients also showed a significant difference compared to male patients (P<0.05), although there were no significant differences in terms of the age of onset and duration of the disease, or in the type of episode and the presence of psychotic symptoms.
 |
Table 1 Clinical Characteristics of the Study Participants |
Sex-Based Differences in Clinical Variables
Male bipolar patients had significantly higher systolic and diastolic blood pressure than female bipolar patients (P<0.001, P=0.016), and there were also significant differences between male and female patients in glutamine transpeptidase (GGT), alkaline phosphatase (ALP), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and TGs (all P<0.005), while high-density lipoprotein (HDL) levels were higher in female patients than in male patients [1.07(0.93, 1.25) vs 1.25(1.07, 1.46), P<0.001]. Our study also found that uric acid levels were significantly higher in male patients than in female patients with BD (396.42±103.97 vs 316.67±90.54, P<0.001); however, apolipoprotein A1 (ApoA1) levels were higher in female patients than in male patients [1.23(1.08, 1.42) vs 1.16(1, 1.36), P<0.005]. Finally, our study found that TyG index levels were higher in male patients with BD than in females [8.46(8.12, 8.89) vs 8.34(7.96, 8.78), P=0.006].
Differences in Patients with NAFLD by Sex
When patients with NAFLD were grouped and compared by sex, we found significant differences in the following indicators: years of education, duration of the disease, presence of psychotic symptoms, marital status, ALT, AST, triglycerides, HDL, and uric acid (as shown in Table 2).
 |
Table 2 Comparison of Parameter Differences Between Males and Females in Patients with BD Manifesting NAFLD |
Differences in NAFLD and Non-NAFLD Groups in Male/Female Patients with BD
When comparing the comorbid NAFLD group with the non-NAFLD group in men with BD, significant differences were found in the following indicators: BMI, glucose, ALP, GGT, TGs, ApoB, and TyG (as shown in Table 3). Significant differences were found for women in the following indicators: duration of the disease, marital status, BMI, glucose, ALT, GGT, TGs, HDL and TyG levels (Table 4).
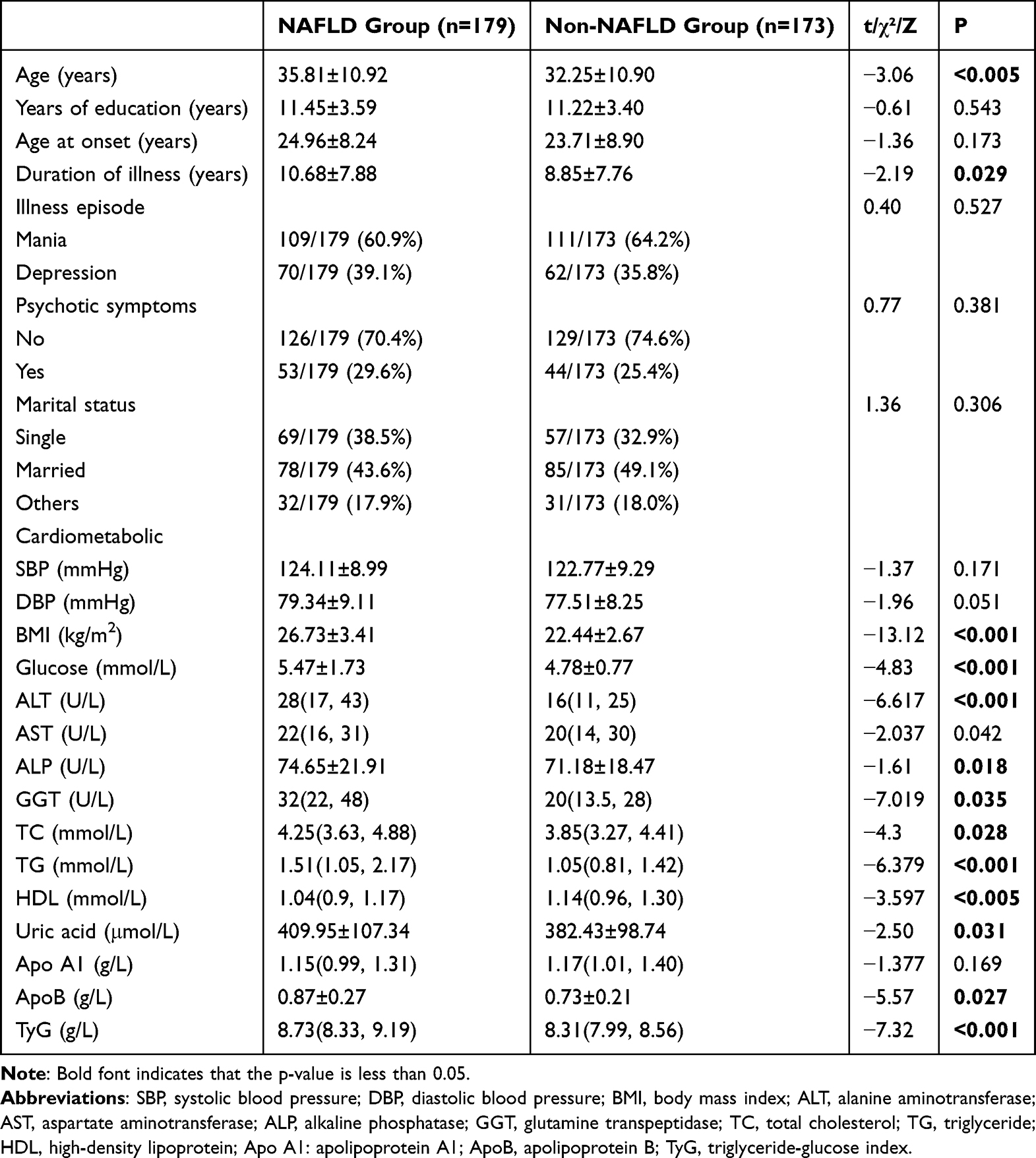 |
Table 3 Comparison of Parameters in Male Patients with BD |
 |
Table 4 Comparison of Parameters in Female Patients with BD |
Analysis of Risk Factors for NAFLD in Patients with BD
The indicators previously found to be significantly different in the t-tests were included in the regression equation analysis and the following results were obtained: in male patients with BD, the risk factors for nonalcoholic fatty liver were BMI (odds ratio [OR]=1.626, P<0.001), glucose (OR=1.644, P<0.001), and apolipoprotein B (OR=5.908, P<0.005) (as shown in Table 5). In contrast, the risk factors for comorbid NAFLD in female patients with BD were BMI (OR=1.284, P<0.001), disease duration (OR=1.039, P=0.017), GGT (OR=1.041, P<0.001), and TyG (OR=2.157, P<0.005) (Table 6).
 |
Table 5 Risk Factors for NAFLD in Male Patients with BD |
 |
Table 6 Risk Factors for NAFLD in Female Patients with BD |
Predictive Value of NAFLD Risk Factors
ROC analysis was used to assess the threshold value of the identified risk factors for predicting the development of NAFLD in patients with BD. The following three risk factors predicted NAFLD: For male patients, a BMI at a cut-off value of 24.05 kg/m² (AUC: 0.828, 95% CI: 0.809–0.888, sensitivity: 79.9%, and specificity: 77.5%); glucose levels at a cut-off value of 4.945 mmol/L (AUC: 0.653, 95% CI: 0.595–0.710, sensitivity: 54.2%, and specificity: 72.4%); and ApoB levels at a cut-off value of 0.765 g/L (AUC: 0.666, 95% CI: 0.610–0.722, sensitivity: 65.4%, and specificity: 60.7%) (Figure 1). For female patients, a BMI at a cut-off value of 24.19 kg/m² (area under the curve [AUC]: 0.814, 95% CI: 0.767–0.862, sensitivity: 77.5%, and specificity: 78.2%); duration of illness at a cut-off value of 11.5 years (AUC: 0.657, 95% CI: 0.599–0.715, sensitivity: 47.1%, and specificity: 76.4%); GGT level at a cut-off value of 19.5 U/L (AUC: 0.699, 95% CI: 0.643–0.756, sensitivity: 45.7%, and specificity: 84.1%); and TyG index at a cut-off value of 8.20 (AUC: 0.737, 95% CI: 0.685–0.789, sensitivity: 83.3%, and specificity: 53.2%) (Figure 2).
 |
Figure 1 The predictive value of influencing factors on NAFLD in male patients with BD. (A) ROC curve of BMI in predicting NAFLD; (B) ROC curve of Glucose in predicting NAFLD; (C) ROC curve of ApoB in predicting NAFLD. |
 |
Figure 2 The predictive value of influencing factors on NAFLD in female patients with BD. (A) ROC curve of BMI in predicting NAFLD; (B) ROC curve of Duration of illness in predicting NAFLD; (C) ROC curve of GGT in predicting NAFLD; (D) ROC curve of TyG in predicting NAFLD. |
Discussion
This study investigated sex differences and risk factors and the prevalence of NAFLD in Chinese patients with BD for which limited information is available. The major findings of our research are the following: 1) the prevalence of NAFLD was significantly higher in men and there were significant differences in the years of education, marital status, and metabolic indicators; 2) there were sex differences in metabolic and biochemical indicators between patients with NAFLD and differences in metabolic and biochemical indicators between patients of the same sex with and without NAFLD; and 3.) risk factors for comorbid NAFLD in patients with BD differed according to sex. BMI was a common risk factor for both sexes, and the risk factors for female patients with BD included disease duration, GGT, and TyG, whereas those for male patients with BD included blood glucose and apolipoprotein B in addition to BMI.
BD is a serious and common psychiatric disorder that imposes a heavy burden on society and families and seriously affects the daily lives of patients. This effect manifests itself not only in the impairment of social functioning and cognitive abilities, but also in the tendency to have comorbidities of many complex somatic disorders.14,35,36 Furthermore, studies have shown that patients with BD have a significantly increased risk of NAFLD, hyperlipidaemia, and ischemic heart disease.35,37–39 NAFLD, a common comorbidity in bipolar patients, is a liver disease characterized by an excessive accumulation of fat in hepatocytes. Existing studies have shown sex differences in the duration and type of attacks in male and female patients with BD,26 but little is known about the presence of comorbid NAFLD, making it particularly important to investigate risk factors for comorbid NAFLD in different sexes. Our previous study find significantly higher rates of comorbid obesity in patients with BD and higher plasma levels of ALT, blood glucose, uric acid and TG in obese patients;7 building on this finding, we take it a step further to examine sex differences in comorbid NAFLD in patients with BD, targeting sex-specific risk factors.
This study found significant differences in general demographic data, blood biochemical parameters, and liver enzymes in BD patients by sex and also found a higher prevalence of NAFLD in men with BD than in women. Since a high BMI suggests the accumulation of fat in internal organs such as the liver, which in turn can cause hepatocellular steatosis and a variety of metabolic conditions, studies have confirmed that obesity is an independent risk factor for NAFLD.40 It is not difficult to explain why BMI is a risk factor for comorbid NAFLD, shared by different sexes. Furthermore, although some studies have found that higher educational attainment leads to a lower risk of NAFLD,41 our study found that although male BD patients had higher educational level than female BD patients, their prevalence of NAFLD was not lower than that in women. This may be due to the fact that the mean age of the study subjects was lower than the age of female menopause, and for this age group, men were more likely to develop NAFLD.42,43
In our study, ApoB, which is synthesized in the liver, directly reflected low-density lipoprotein cholesterol (LDL-CHOL) levels and is the major structural protein of LDL-CHOL. It has also been found to be a risk factor in men. Increased ApoB levels have been found in clinical studies to be a risk factor for coronary heart disease and represents a better marker of atherosclerosis among all lipid markers.44 Elevated ApoB levels can also indicate an increased risk of diabetes, renal impairment, and obstructive jaundice,45–47 and higher ApoB levels in male patients imply a greater susceptibility to liver involvement that may be influenced by these diseases, ultimately increasing the odds of comorbid NAFLD. This may, to some extent, explain why ApoB is a risk factor for male patients with BD, but not for women.
We found that the duration of biphasic disease was on average longer in women than in men in the different sex groups with NAFLD, and there is no doubt that a longer duration of BD has a greater impact on the lifestyles of patients. Lifestyle has been shown to have a significant effect on the prevalence of NAFLD.48,49 Therefore, as a risk factor for female patients with BD, the duration of the disease can increase the odds of comorbid NAFLD. GGT levels are lower in women than in male BD patients. However, some studies have found that GGT may be more sensitive in female patients, suggesting atherosclerosis and cardiovascular risks.50,51 Furthermore, GGT in the blood is significantly higher when the liver is affected, such as in obstructive jaundice, acute hepatitis, active chronic hepatitis, biliary tract infection, and cirrhosis.52,53 This may be due to increased cellular production of GGT and the inflammatory stimulating effect in and around injured tissue, which increases the permeability of the hepatocyte membrane, resulting in an increase in blood GGT. Our findings suggest that not only can high GGT levels indicate the risk of disease, but low GGT levels are also a risk factor of concern in sex-specific and disease-specific conditions such as comorbid NAFLD in female patients with BD.
A high TyG index is a risk factor for comorbid NAFLD in female patients, while higher blood glucose is a risk factor for comorbid NAFLD in male patients. The current study showed that the determination of TyG is a simple and effective method for the early evaluation of NAFLD54 and that the TyG index is significantly and positively correlated with the severity of cirrhosis and the presence of liver fibrosis in patients with NAFLD.55 A previous study that included 1969 participants also observed that the association between the TyG index and NAFLD in Asian populations was more pronounced in women than in men.56 Some studies have suggested that TyG is more clinically significant in the prediction of cardiovascular risks, such as hypertension, diabetes, and atherosclerosis, in women than in men.57–59 Our findings also suggest that a higher TyG index is a more significant risk factor for comorbid NAFLD in women with BD, while for men, focusing on fasting glucose levels may be a better marker.
We identified three limitations of this study. First, as this study was a retrospective cross-sectional study, the inherent limitations of cross-sectional and retrospective studies prevent us from drawing definitive conclusions of a causal nature from the observed differences. Second, it was not possible to completely exclude the effect of the medications because although we strictly limited the participants by selecting patients who had not taken psychiatric medications or medications that could induce NAFLD in the last three months. Therefore, we could not quantify the association between medications and NAFLD. Further exploration in this area is required for future research. Finally, the information collected on the study population is not fully exhaustive, specifically risk factors that can be associated with NAFLD, such as low-density lipoprotein, smoking history, and patient lifestyle prior to hospital admission. These factors that were not included in the analysis may have influenced the results of the risk factors associated with NAFLD in our research. This is important information to consider, collect, and analyse in future studies.
Conclusion
This study identified sex differences in general demographics, clinical indicators, and prevalence of NAFLD in patients with BD. The higher prevalence of NAFLD in male patients than in female patients may make them more susceptible to a multitude of chronic diseases including hypertension, cardiovascular disease, diabetes, and stroke.60,61 Although several biopsychosocial causes, such as estrogenic effects, neurodevelopmental differences, and genetic susceptibility, have been proposed to explain this sex-based difference, clinicians should pay closer attention to sex differences between male and female patients in the course of treatment and continuously monitor their respective risk factors. At the same time, psychiatrists should be aware of the differences between male and female patients and encourage them to exercise, lead a healthy lifestyle, control sugar intake, fat intake, and increase physical activity, and body weight according to their respective characteristics to prevent the development of NAFLD. This study has important implications for the therapeutic management of comorbid NAFLD in patients with BD, particularly with regard to the further reduction of the incidence of cardiovascular diseases, improvement of long-term prognosis, and facilitation of individualized treatment for patients of different sexes with BD.
Acknowledgments
The authors would like to express their gratitude to the Anhui Mental Health Center for their valuable support in providing the data for this study. The authors acknowledge that without the assistance and collaboration of the hospital, this research would not have been feasible.
Funding
This work was supported by the Hospital Project of Hefei Fourth People’s Hospital (grant numbers HFSY2022ZD11, HFSY2022YB08 and 2019001) and the Hefei Health Applied Medicine Research Project (grant number Hwk2021yb015).
Disclosure
The authors declare no conflicts of interest associated with this research and affirm that the study was conducted without any commercial or financial relationships that could be perceived as potential conflicts of interest.
References
1. Martinez-Aran A, Vieta E, Torrent C, et al. Functional outcome in bipolar disorder: the role of clinical and cognitive factors. Bipolar Disord. 2007;9(1–2):103–113. doi:10.1111/j.1399-5618.2007.00327.x
2. Bauer MS. Bipolar Disorder. Ann Intern Med. 2022;175(7):Itc97–itc112. doi:10.7326/AITC202207190
3. Alonso J, Petukhova M, Vilagut G, et al. Days out of role due to common physical and mental conditions: results from the WHO World Mental Health surveys. Mol Psychiatry. 2011;16(12):1234–1246. doi:10.1038/mp.2010.101
4. Silarova B, Giltay EJ, Van Reedt Dortland A, et al. Metabolic syndrome in patients with bipolar disorder: comparison with major depressive disorder and non-psychiatric controls. J Psychosom Res. 2015;78(4):391–398. doi:10.1016/j.jpsychores.2015.02.010
5. Vancampfort D, Vansteelandt K, Correll CU, et al. Metabolic syndrome and metabolic abnormalities in bipolar disorder: a meta-analysis of prevalence rates and moderators. Am J Psychiatry. 2013;170(3):265–274. doi:10.1176/appi.ajp.2012.12050620
6. Godin O, Leboyer M, Belzeaux R, et al. Non-alcoholic fatty liver disease in a sample of individuals with bipolar disorders: results from the FACE-BD cohort. Acta Psychiatr Scand. 2021;143(1):82–91. doi:10.1111/acps.13239
7. Wu Q, Zhang X, Liu Y, Wang Y. Prevalence and Risk Factors of Comorbid Obesity in Chinese Patients with Bipolar Disorder. Diabetes Metab Syndr Obes. 2023;16:1459–1469. doi:10.2147/DMSO.S404127
8. Fiedorowicz JG, Palagummi NM, Forman-Hoffman VL, Miller DD, Haynes WG. Elevated prevalence of obesity, metabolic syndrome, and cardiovascular risk factors in bipolar disorder. Ann Clin Psychiatry. 2008;20(3):131–137. doi:10.1080/10401230802177722
9. Yki-Järvinen H. Non-alcoholic fatty liver disease as a cause and a consequence of metabolic syndrome. Lancet Diabetes Endocrinol. 2014;2(11):901–910. doi:10.1016/S2213-8587(14)70032-4
10. Eslam M, George J. Reply to: correspondence regarding “A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement”: bringing evidence to the NAFLD-MAFLD debate. J Hepatol. 2020;73(6):1575. doi:10.1016/j.jhep.2020.07.045
11. Younossi Z, Anstee QM, Marietti M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11–20. doi:10.1038/nrgastro.2017.109
12. Younossi Z, Stepanova M, Ong JP, et al. Nonalcoholic Steatohepatitis Is the Fastest Growing Cause of Hepatocellular Carcinoma in Liver Transplant Candidates. Clin Gastroenterol Hepatol. 2019;17(4):748–755 e743. doi:10.1016/j.cgh.2018.05.057
13. Younossi ZM. Non-alcoholic fatty liver disease - A global public health perspective. J Hepatol. 2019;70(3):531–544. doi:10.1016/j.jhep.2018.10.033
14. Ma Q, Yang F, Ma B, et al. Prevalence of nonalcoholic fatty liver disease in mental disorder inpatients in China: an observational study. Hepatol Int. 2021;15(1):127–136. doi:10.1007/s12072-020-10132-z
15. Zhou F, Zhou J, Wang W, et al. Unexpected Rapid Increase in the Burden of NAFLD in China From 2008 to 2018: a Systematic Review and Meta-Analysis. Hepatology. 2019;70(4):1119–1133. doi:10.1002/hep.30702
16. Estes C, Razavi H, Loomba R, Younossi Z, Sanyal AJ. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology. 2018;67(1):123–133. doi:10.1002/hep.29466
17. Buzzetti E, Pinzani M, Tsochatzis EA. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism. 2016;65(8):1038–1048. doi:10.1016/j.metabol.2015.12.012
18. Sinn DH, Kang D, Chang Y, et al. Non-alcoholic fatty liver disease and progression of coronary artery calcium score: a retrospective cohort study. Gut. 2017;66(2):323–329. doi:10.1136/gutjnl-2016-311854
19. Anstee QM, Mantovani A, Tilg H, Targher G. Risk of cardiomyopathy and cardiac arrhythmias in patients with nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol. 2018;15(7):425–439. doi:10.1038/s41575-018-0010-0
20. Lonardo A, Nascimbeni F, Mantovani A, Targher G. Hypertension, diabetes, atherosclerosis and NASH: cause or consequence? J Hepatol. 2018;68(2):335–352. doi:10.1016/j.jhep.2017.09.021
21. Mahady SE, George J. Predicting the future burden of NAFLD and NASH. J Hepatol. 2018;69(4):774–775. doi:10.1016/j.jhep.2018.06.025
22. Buoli M, Cesana BM, Dell’Osso B, et al. Gender-related differences in patients with bipolar disorder: a nationwide study. CNS Spectr. 2019;24(6):589–596. doi:10.1017/S1092852918001529
23. Suominen K, Mantere O, Valtonen H, Arvilommi P, Leppämäki S, Isometsä E. Gender differences in bipolar disorder type I and II. Acta Psychiatr Scand. 2009;120(6):464–473. doi:10.1111/j.1600-0447.2009.01407.x
24. Cotton SM, Lambert M, Schimmelmann BG, et al. Gender differences in premorbid, entry, treatment, and outcome characteristics in a treated epidemiological sample of 661 patients with first episode psychosis. Schizophr Res. 2009;114(1–3):17–24. doi:10.1016/j.schres.2009.07.002
25. Rietschel L, Lambert M, Karow A, et al. Clinical high risk for psychosis: gender differences in symptoms and social functioning. Early Interv Psychiatry. 2017;11(4):306–313. doi:10.1111/eip.12240
26. Menculini G, Steardo L Jr, Sciarma T, et al. Sex Differences in Bipolar Disorders: impact on Psychopathological Features and Treatment Response. Front Psychiatry. 2022;13:926594. doi:10.3389/fpsyt.2022.926594
27. Patel RS, Virani S, Saeed H, Nimmagadda S, Talukdar J, Youssef NA. Gender Differences and Comorbidities in U.S. Adults with Bipolar Disorder. Brain Sci. 2018;8(9):168. doi:10.3390/brainsci8090168
28. Afzal M, Siddiqi N, Ahmad B, et al. Prevalence of Overweight and Obesity in People With Severe Mental Illness: systematic Review and Meta-Analysis. Front Endocrinol (Lausanne). 2021;12:769309. doi:10.3389/fendo.2021.769309
29. Li Q, Chen D, Liu T, et al. Sex Differences in Body Mass Index and Obesity in Chinese Patients With Chronic Schizophrenia. J Clin Psychopharmacol. 2016;36(6):643–648. doi:10.1097/JCP.0000000000000594
30. Baskaran A, Cha DS, Powell AM, Jalil D, McIntyre RS. Sex differences in rates of obesity in bipolar disorder: postulated mechanisms. Bipolar Disord. 2014;16(1):83–92. doi:10.1111/bdi.12141
31. Li X, Gao Y, Wang Y, Wang Y, Wu Q. Prevalence and Influence Factors for Non-Alcoholic Fatty Liver Disease in Long-Term Hospitalized Patients with Schizophrenia: a Cross-Sectional Retrospective Study. Neuropsychiatr Dis Treat. 2023;19:379–389. doi:10.2147/NDT.S398385
32. Dilling H, Dittmann V. Psychiatric diagnosis following the 10th revision of the International Classification of Diseases (ICD-10). Nervenarzt. 1990;61(5):259–270.
33. Wong VW, Chan WK, Chitturi S, et al. Asia-Pacific Working Party on Non-alcoholic Fatty Liver Disease guidelines 2017-Part 1: definition, risk factors and assessment. J Gastroenterol Hepatol. 2018;33(1):70–85. doi:10.1111/jgh.13857
34. Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299–304. doi:10.1089/met.2008.0034
35. Hsu JH, Chien IC, Lin CH. Increased risk of hyperlipidemia in patients with bipolar disorder: a population-based study. Gen Hosp Psychiatry. 2015;37(4):294–298. doi:10.1016/j.genhosppsych.2015.04.003
36. Hsu JH, Chien IC, Lin CH. Increased risk of ischemic heart disease in patients with bipolar disorder: a population-based study. J Affect Disord. 2021;281:721–726. doi:10.1016/j.jad.2020.11.083
37. Soto-Angona O, Anmella G, Valdes-Florido MJ, et al. Non-alcoholic fatty liver disease (NAFLD) as a neglected metabolic companion of psychiatric disorders: common pathways and future approaches. BMC Med. 2020;18(1):261. doi:10.1186/s12916-020-01713-8
38. Mosolov SN, Fedorova EY. The risk of developing cardiovascular disease in bipolar disorder. Clinical and social factors. Ter Arkh. 2021;93(12):1556–1561. doi:10.26442/00403660.2021.12.201175
39. Rossom RC, Hooker SA, O’Connor PJ, Crain AL, Sperl-Hillen JM. Cardiovascular Risk for Patients With and Without Schizophrenia, Schizoaffective Disorder, or Bipolar Disorder. J Am Heart Assoc. 2022;11(6):e021444. doi:10.1161/JAHA.121.021444
40. Samuel VT, Shulman GI. Nonalcoholic Fatty Liver Disease as a Nexus of Metabolic and Hepatic Diseases. Cell Metab. 2018;27(1):22–41. doi:10.1016/j.cmet.2017.08.002
41. Xie J, Huang H, Liu Z, et al. The associations between modifiable risk factors and nonalcoholic fatty liver disease: a comprehensive Mendelian randomization study. Hepatology. 2022.
42. Ballestri S, Nascimbeni F, Baldelli E, Marrazzo A, Romagnoli D, Lonardo A. NAFLD as a Sexual Dimorphic Disease: role of Gender and Reproductive Status in the Development and Progression of Nonalcoholic Fatty Liver Disease and Inherent Cardiovascular Risk. Adv Ther. 2017;34(6):1291–1326. doi:10.1007/s12325-017-0556-1
43. Burra P, Bizzaro D, Gonta A, et al. Clinical impact of sexual dimorphism in non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH). Liver Int. 2021;41(8):1713–1733. doi:10.1111/liv.14943
44. Purcell-Huynh DA, Farese RV Jr, Johnson DF, et al. Transgenic mice expressing high levels of human apolipoprotein B develop severe atherosclerotic lesions in response to a high-fat diet. J Clin Invest. 1995;95(5):2246–2257. doi:10.1172/JCI117915
45. Zhao W, Li J, Zhang X, et al. Apolipoprotein B and renal function: across-sectional study from the China health and nutrition survey. Lipids Health Dis. 2020;19(1):110. doi:10.1186/s12944-020-01241-7
46. Han SJ, Fujimoto WY, Kahn SE, Leonetti DL, Boyko EJ. Apolipoprotein B Levels Predict Future Development of Hypertension Independent of Visceral Adiposity and Insulin Sensitivity. Endocrinol Metab. 2020;35(2):351–358. doi:10.3803/EnM.2020.35.2.351
47. Koskinen J, Magnussen CG, Wurtz P, et al. Apolipoprotein B, oxidized low-density lipoprotein, and LDL particle size in predicting the incidence of metabolic syndrome: the Cardiovascular Risk in Young Finns study. Eur J Prev Cardiol. 2012;19(6):1296–1303. doi:10.1177/1741826711425343
48. Zhang XL, Wang TY, Targher G, Byrne CD, Zheng MH. Lifestyle Interventions for Non-Obese Patients Both with, and at Risk, of Non-Alcoholic Fatty Liver Disease. Diabetes Metab J. 2022;46(3):391–401. doi:10.4093/dmj.2022.0048
49. Mascaró CM, Bouzas C, Tur JA. Association between Non-Alcoholic Fatty Liver Disease and Mediterranean Lifestyle: a Systematic Review. Nutrients. 2021;14(1):49. doi:10.3390/nu14010049
50. Jung CH, Yu JH, Bae SJ, et al. Serum gamma-glutamyltransferase is associated with arterial stiffness in healthy individuals. Clin Endocrinol (Oxf). 2011;75(3):328–334. doi:10.1111/j.1365-2265.2011.04060.x
51. Ren J, Sun J, Ning F, et al. Gender differences in the association of hypertension with gamma-glutamyltransferase and alanine aminotransferase levels in Chinese adults in Qingdao, China. J Am Soc Hypertens. 2015;9(12):951–958. doi:10.1016/j.jash.2015.09.014
52. Cho HS, Lee SW, Kim ES, et al. Clinical significance of serum bilirubin and gamma-glutamyltransferase levels on coronary atherosclerosis assessed by multidetector computed tomography. Nutr Metab Cardiovasc Dis. 2015;25(7):677–685. doi:10.1016/j.numecd.2015.03.014
53. Onat A, Can G, Cakr H, et al. Sex-Specific Predictors of Metabolic Syndrome Independent of Its Components. J Investig Med. 2015;63(6):796–801. doi:10.1097/JIM.0000000000000203
54. Hu H, Han Y, Cao C, He Y. The triglyceride glucose-body mass index: a non-invasive index that identifies non-alcoholic fatty liver disease in the general Japanese population. J Transl Med. 2022;20(1):398. doi:10.1186/s12967-022-03611-4
55. Guo W, Lu J, Qin P, et al. The triglyceride-glucose index is associated with the severity of hepatic steatosis and the presence of liver fibrosis in non-alcoholic fatty liver disease: a cross-sectional study in Chinese adults. Lipids Health Dis. 2020;19(1):218. doi:10.1186/s12944-020-01393-6
56. Lin IT, Lee MY, Wang CW, Wu DW, Chen SC. Gender Differences in the Relationships among Metabolic Syndrome and Various Obesity-Related Indices with Nonalcoholic Fatty Liver Disease in a Taiwanese Population. Int J Environ Res Public Health. 2021;18(3). doi:10.3390/ijerph18030857
57. Park K, Ahn CW, Lee SB, et al. Elevated TyG Index Predicts Progression of Coronary Artery Calcification. Diabetes Care. 2019;42(8):1569–1573. doi:10.2337/dc18-1920
58. Tai S, Fu L, Zhang N, et al. Association of the cumulative triglyceride-glucose index with major adverse cardiovascular events in patients with type 2 diabetes. Cardiovasc Diabetol. 2022;21(1):161. doi:10.1186/s12933-022-01599-1
59. Wang X, Xu W, Song Q, et al. Association between the triglyceride-glucose index and severity of coronary artery disease. Cardiovasc Diabetol. 2022;21(1):168. doi:10.1186/s12933-022-01606-5
60. Sanyal AJ. Past, present and future perspectives in nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol. 2019;16(6):377–386. doi:10.1038/s41575-019-0144-8
61. Xiao J, Wang F, Wong NK, et al. Global liver disease burdens and research trends: analysis from a Chinese perspective. J Hepatol. 2019;71(1):212–221. doi:10.1016/j.jhep.2019.03.004
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between TyG Index, Liver Steatosis and Immunosenescence in People Living with HIV
Yan H, Chen S, Gao X, Jiang Y, Liang G, Peng J, Cai S
Infection and Drug Resistance 2024, 17:5049-5059
Published Date: 13 November 2024