Back to Journals » International Medical Case Reports Journal » Volume 19
Severe Post-Measles ARDS with Multisystem Complications in an Unvaccinated Child in a Resource-Limited Setting: A Case Report
Authors Siyad AO ![]() , Hassan AM
, Hassan AM ![]() , Hassan RA
, Hassan RA ![]()
Received 11 March 2026
Accepted for publication 19 May 2026
Published 23 May 2026 Volume 2026:19 608541
DOI https://doi.org/10.2147/IMCRJ.S608541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Ahmed Omar Siyad,1 Abdukadir Mohamed Hassan,1 Rayan Abdirahman Hassan2
1Department of Intensive Care, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia; 2Department of Pediatrics, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia
Correspondence: Ahmed Omar Siyad, Email [email protected]; [email protected]
Background: Measles remains a major cause of preventable severe pediatric illness in low-resource settings where vaccination coverage is suboptimal and outbreaks continue to occur. Severe complications, particularly pneumonia, may be fatal, and in rare cases pulmonary involvement can progress to acute respiratory distress syndrome requiring intensive care support.
Case Presentation: A 2-year-old unvaccinated girl from a rural area presented with 1 week of fever and progressive respiratory distress after a recent clinically suspected measles illness characterized by fever and generalized rash during community measles circulation. She arrived critically ill with severe hypoxemia, tachypnea, hypotension, and depressed consciousness, requiring urgent intubation and pediatric intensive care. Chest imaging showed diffuse bilateral infiltrates consistent with severe pneumonia. In the setting of acute hypoxemic respiratory failure requiring invasive mechanical ventilation, together with the absence of a primary cardiogenic explanation on echocardiography, the clinical findings supported pediatric acute respiratory distress syndrome. Echocardiography showed mild pericardial effusion without hemodynamic compromise. She was managed with mechanical ventilation, broad-spectrum antimicrobials, age-appropriate vitamin A, sedation/analgesia, electrolyte correction, blood transfusion for severe anemia, diuresis for fluid overload, and enteral nutrition. She was extubated after 14 days, transferred out of intensive care on day 18, and discharged in good clinical condition after 27 days of hospitalization.
Conclusion: This case highlights the life-threatening course of post-measles acute respiratory distress syndrome in an unvaccinated child and shows that favorable outcomes are possible with early recognition, timely intensive supportive care, and close monitoring for multisystem complications. It also underscores the importance of strengthening routine immunization coverage and referral pathways in resource-limited settings.
Keywords: measles, acute respiratory distress syndrome, pediatric intensive care, unvaccinated child, pneumonia, resource-limited setting, case report
Introduction
Measles is an acute and highly contagious viral infection that continues to pose a major threat to child health worldwide.1 Although it is preventable through vaccination, measles remains an important cause of vaccine-preventable illness and death among children, particularly in populations where immunization coverage is incomplete.2 Despite the availability of a safe and effective vaccine, outbreaks continue to occur in settings with declining vaccine uptake and persistent gaps in routine immunization services.3
The burden of severe measles is greatest in low-resource and fragile health system settings, where limited access to preventive services, delayed care-seeking, and constrained hospital capacity increase the risk of complications and death.2 Children younger than 5 years of age are especially vulnerable, and a substantial proportion of measles-related deaths occur in this age group.1
Clinically, measles is commonly diagnosed on the basis of fever, generalized maculopapular rash, and associated respiratory or conjunctival symptoms.4 Although serologic or molecular confirmation may support diagnosis, such testing is not consistently available in resource-limited settings, where clinicians often rely on clinical findings and epidemiologic exposure to guide early management.
While many cases resolve without long-term sequelae, severe complications can occur, particularly in unvaccinated children. Pneumonia remains the most common serious complication and a leading cause of measles-related death.5 Progressive pulmonary involvement may result in marked hypoxemia and respiratory failure. In rare but severe cases, this inflammatory lung injury may evolve into pediatric acute respiratory distress syndrome, a syndrome recognized in critically ill children with acute hypoxemia and diffuse pulmonary infiltrates.6
Although pediatric acute respiratory distress syndrome is well characterized in critical care literature, severe post-measles acute respiratory distress syndrome remains infrequently documented in resource-limited environments where diagnostic capacity and pediatric intensive care services may be limited.6 Reporting such cases is important to improve clinical recognition and to highlight the continuing public health consequences of incomplete vaccination coverage. We therefore describe a severe case of post-measles acute respiratory distress syndrome with multisystem complications in an unvaccinated child managed in a resource-limited setting.
Case Presentation
A 2-year-old unvaccinated girl weighing 9.4 kg from a rural area was brought to our hospital with a 1-week history of persistent fever and progressively worsening respiratory distress. Her father reported that she had recently experienced a febrile illness associated with a generalized rash while at home in a remote setting, where no medical evaluation had been sought. At the time of presentation, measles was circulating in the community and, given the absence of prior vaccination together with the characteristic rash history, a clinical diagnosis of recent measles infection was made. On examination, residual hyperpigmented rash lesions were present. Her weight was low for age, suggesting possible underlying undernutrition, which may have increased her vulnerability to severe measles-related complications.
On arrival, the child appeared critically ill and unconscious. Her temperature was 39°C, oxygen saturation was 70% on room air, respiratory rate was 60 breaths per minute, heart rate was 160 beats per minute, blood pressure was 80/45 mmHg, and random blood glucose was 102 mg/dL. Neurological assessment showed a Glasgow Coma Scale score of 8. Because of severe respiratory compromise and depressed consciousness, urgent endotracheal intubation was performed, and she was transferred to the intensive care unit for mechanical ventilation.
Initial laboratory workup included complete blood count, inflammatory markers, renal and liver function tests, serum electrolytes, and arterial blood gas analysis. Findings were significant for marked leukocytosis of 30 × 109/L, hemoglobin of 8 g/dL, C-reactive protein greater than 300 mg/L, and hypokalemia with a serum potassium level of 2.9 mmol/L. Arterial blood gas analysis demonstrated severe respiratory acidosis with metabolic compensation, consistent with ventilatory failure (Table 1). Chest radiography revealed diffuse bilateral pulmonary infiltrates (Figure 1). In the setting of acute severe hypoxemic respiratory failure requiring invasive mechanical ventilation, together with new bilateral chest infiltrates and the absence of a primary cardiogenic explanation on echocardiography, these findings supported a clinical diagnosis of pediatric acute respiratory distress syndrome complicating severe post-measles pneumonia. The PaO2/FiO2 ratio at presentation was approximately 96, supporting severe PARDS according to established pediatric consensus definitions. Transthoracic echocardiography showed mild pericardial effusion without tamponade or hemodynamic compromise (Figure 2).
 |
Table 1 Laboratory Investigation Results |
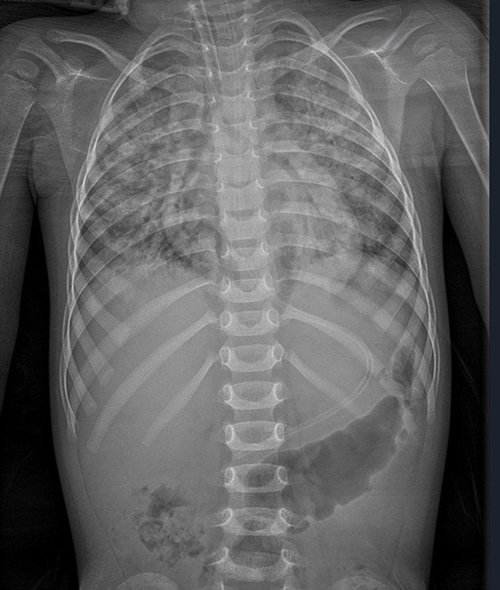 |
Figure 1 Initial chest radiograph showing diffuse bilateral pulmonary infiltrates. |
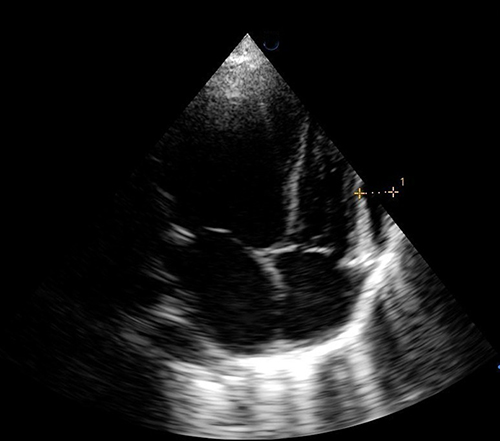 |
Figure 2 Echocardiography showing mild pericardial effusion without tamponade or hemodynamic compromise. |
Alternative diagnostic considerations included severe bacterial pneumonia, sepsis-related acute respiratory distress syndrome, and other viral pneumonias. However, the combination of recent febrile generalized rash illness during community measles circulation, absence of measles vaccination, residual hyperpigmented rash lesions, and the overall clinical course strongly supported recent measles infection complicated by severe pneumonia and pediatric acute respiratory distress syndrome. No primary cardiac cause of respiratory failure was identified on echocardiography.
Broad-spectrum antimicrobial therapy with meropenem and vancomycin was started along with supportive management, including reduced-maintenance intravenous fluids, electrolyte supplementation, gastric protection, and nebulized bronchodilator therapy. Age-appropriate vitamin A supplementation was administered as part of supportive measles management. Corticosteroids were given as adjunctive treatment in the setting of severe airway and pulmonary inflammation. Adrenaline nebulization was administered during the first 48 hours because of concern for upper airway edema and to help maintain airway patency. Anticoagulation was also given according to local intensive care prophylaxis practice during prolonged immobilization and central venous access. In our setting, measles IgM testing and polymerase chain reaction were not available during admission, and microbiological culture capacity was limited. As a result, diagnosis and management relied on clinical assessment, serial laboratory monitoring, and the patient’s bedside response to treatment.
Sedation, analgesia, and ventilator synchrony were maintained with continuous infusions of midazolam, ketamine, fentanyl, and atracurium. The patient was ventilated using synchronized intermittent mandatory ventilation with pressure control, with an FiO2 of 50%, positive end-expiratory pressure of 4 cmH2O, respiratory rate of 30 breaths per minute, inspiratory pressure of 20 cmH2O, and pressure support of 10 cmH2O. On day 3 of intensive care admission, peripheral venous access became difficult because of generalized edema and the ongoing need for antimicrobial therapy and supportive care, so a central venous line was inserted. During this period, laboratory monitoring showed worsening leukocytosis, increasing to 35 × 109/L, and subsequent arterial blood gas analysis demonstrated metabolic acidosis during the course of critical illness, suggesting evolving systemic involvement (Table 1). In response to persistent fever, worsening leukocytosis, evolving metabolic acidosis, prolonged ventilator dependence, and concern for resistant nosocomial gram-negative infection in the setting of limited microbiologic diagnostic capacity, antimicrobial therapy was escalated by replacing meropenem with ceftazidime-avibactam and adding clarithromycin.
Enteral feeding through a nasogastric tube was started on day 3 while intravenous fluids were gradually reduced. As the admission progressed, the child developed signs of fluid overload, and furosemide was initiated to optimize fluid balance. On day 4, hemoglobin dropped to 6.1 g/dL, necessitating transfusion of 141 mL of packed red blood cells over 3 hours, after which hemoglobin improved to 9.4 g/dL. Hypernatremia developed (Table 1) during the same period, prompting adjustment of intravenous fluids to a mixture of two-thirds 5% dextrose and one-third normal saline.
Over the following days, laboratory parameters gradually improved, with declining leukocytosis and inflammatory markers (Table 1). Follow-up chest radiography showed improvement in the bilateral pulmonary infiltrates (Figure 3). Her neurological status also improved steadily, allowing gradual reduction of sedation. She remained intubated and mechanically ventilated for 14 days. After successful extubation, repeat arterial blood gas analysis confirmed normalization of acid-base status. She remained in the intensive care unit for a further 4 days, during which respiratory support was progressively reduced from face-mask oxygen to nasal cannula. Once clinically stable, she was transferred to the pediatric ward for ongoing care.
 |
Figure 3 Follow-up chest radiograph showing improvement in the bilateral pulmonary infiltrates. |
After transfer to the pediatric ward on day 18, the central venous line was removed and peripheral venous access was re-established. Following discontinuation of sedation infusions, diazepam was prescribed in a tapering regimen to reduce the risk of withdrawal symptoms. Additional supportive therapy included oral iron supplementation and continued nutritional rehabilitation. Laboratory results continued to normalize during the ward stay. After a total hospital stay of 27 days, the patient was discharged in good clinical condition, maintaining oxygen saturation on room air and tolerating oral feeding.
Discussion
This case shows how measles, a vaccine-preventable illness that is often initially recognized as a febrile rash disease, can progress rapidly to critical respiratory failure in an unvaccinated child. In this patient, the illness evolved into severe hypoxemia requiring prolonged invasive mechanical ventilation and intensive care support. The case is particularly important because it reflects the clinical reality of managing life-threatening measles complications in a resource-limited setting, where advanced diagnostics and pediatric critical care resources may be constrained.1,4
Pneumonia remains the most common serious complication of measles and the leading direct cause of measles-related death, especially among young children, unvaccinated populations, and those with delayed access to care.2,3 In the present case, the child came from a rural setting, had not received measles vaccination, and presented only after a week of persistent fever and worsening respiratory distress. Her low body weight for age may also have increased her susceptibility to severe infection. These overlapping vulnerabilities likely contributed to the aggressive course of illness.
The pulmonary findings in this case were strongly compatible with pediatric acute respiratory distress syndrome complicating severe post-measles pneumonia. Current pediatric consensus definitions describe PARDS as acute hypoxemic respiratory failure associated with new pulmonary infiltrates that cannot be fully explained by cardiac dysfunction or fluid overload.6,7 Our patient fit this clinical pattern, with profound hypoxemia at presentation, diffuse bilateral chest radiographic infiltrates, and the need for invasive mechanical ventilation. Echocardiography did not show a primary cardiac cause for the respiratory failure, instead demonstrating only mild pericardial effusion without tamponade or hemodynamic compromise. Taken together, these features support the diagnosis of PARDS in the context of recent measles and severe pneumonia.
Compared with the established clinical literature on severe measles pneumonia and PARDS, this case demonstrates a similar pattern of diffuse pulmonary involvement, profound hypoxemia, and need for intensive respiratory support.5–7 Its distinguishing contribution is the combination of clinically diagnosed recent measles, severe PARDS physiology, multisystem complications, and survival after prolonged invasive ventilation in a setting where confirmatory virologic testing and microbiologic culture support were limited.
An important strength of this case is that it highlights how syndromic but well-reasoned diagnosis remains essential in low-resource practice. In our setting, measles IgM, polymerase chain reaction testing, and full microbiologic culture support were not available during admission. Because of these limitations, the diagnosis of recent measles infection was made clinically, based on the epidemiologic context, the absence of vaccination, the recent history of febrile generalized rash illness, and the residual cutaneous findings on examination. Although laboratory confirmation would have strengthened etiologic certainty, lack of such testing should not delay recognition of severe disease or initiation of life-saving treatment, especially in settings where clinicians must act on the best available evidence at the bedside.4,8 Evidence from multiplex polymerase chain reaction-based acute respiratory infection surveillance in a comparable hospital context further illustrates how expanded molecular testing can improve pathogen detection, while limited access to such testing can constrain etiologic certainty in severe respiratory infections.9
This case also underlines the multisystem burden of severe measles-associated critical illness. Beyond respiratory failure, the child developed marked leukocytosis, severe anemia requiring transfusion, hypokalemia, hypernatremia, generalized edema, difficult venous access, fluid overload requiring diuresis, and mild pericardial effusion. These findings remind us that severe measles is not simply a respiratory infection. In critically ill children, it may be accompanied by systemic inflammation, metabolic disturbances, hemodynamic instability, and complications related both to the disease itself and to prolonged intensive care management. Close serial monitoring was therefore a key part of successful management in this patient. This approach is consistent with pediatric clinical literature emphasizing careful clinico-investigative assessment of acute severe presentations in young children, particularly when systemic complications evolve during admission.10
Another notable feature of this case is the length and complexity of the recovery process. The child required 14 days of invasive mechanical ventilation, followed by gradual weaning of respiratory support, stabilization in intensive care, and later ward-based rehabilitation. Despite the severity of illness, her condition improved progressively with sustained supportive care, radiographic recovery, correction of metabolic abnormalities, nutritional support, and close reassessment. This favorable outcome is clinically meaningful because it shows that survival is possible even in very severe pediatric presentations when timely airway support, careful monitoring, and adaptive treatment strategies are maintained throughout the admission.
From a broader public health perspective, this case reinforces the continuing consequences of incomplete immunization coverage. A preventable infection in an unvaccinated child progressed to prolonged critical illness, exposing both the patient and the healthcare system to major avoidable burden. This has particular relevance in fragile and underserved settings, where missed vaccination opportunities, delayed referral, and limited pediatric intensive care capacity may combine to worsen outcomes.1,2 Strengthening routine immunization programs, improving early recognition of danger signs at community level, and expanding timely referral pathways remain essential to reduce severe measles complications and prevent similar life-threatening presentations. Consistent with evidence on delayed routine immunization among children in underserved settings, this case reinforces how missed vaccination opportunities can translate into preventable severe disease and avoidable critical care burden.11
Overall, this case adds useful clinical evidence from a resource-limited setting by documenting severe post-measles PARDS with multisystem complications in a young unvaccinated child who ultimately recovered after prolonged intensive care management. Its value lies not only in the severity of the presentation, but also in illustrating how careful bedside assessment and sustained supportive care can still lead to a good outcome, even when confirmatory testing and advanced monitoring are limited.
Conclusion
This case demonstrates that measles in an unvaccinated child can progress beyond a self-limited febrile rash illness to severe respiratory failure with multisystem complications requiring prolonged intensive care. In resource-limited settings, where delayed presentation and restricted diagnostic capacity are common, early clinical recognition, timely referral, and sustained supportive management remain critical to survival. It also illustrates that severe post-measles PARDS can remain survivable even in resource-limited settings when early recognition, sustained intensive supportive care, and close monitoring are available. Furthermore, it highlights the continuing importance of clinical bedside diagnosis in environments where confirmatory virologic testing may not be accessible. The case also reinforces the public health importance of strengthening routine immunization coverage, caregiver awareness, and access to pediatric critical care services in fragile health systems.
Abbreviations
ARDS, acute respiratory distress syndrome; PARDS, pediatric acute respiratory distress syndrome; ABG, arterial blood gas; ICU, intensive care unit; CRD, Center of Research and Development.
Data Sharing Statement
All relevant data supporting the findings of this case report are included in the manuscript. No additional data are available due to patient confidentiality.
Ethics Approval and Informed Consent
Written informed consent was obtained from the patient’s parent for publication of the case details and accompanying images. In our institution, ethical approval is not required for case reports.
Acknowledgments
This article was supported by the Center of Research and Development (CRD), SIMAD University, Mogadishu, Somalia. The authors also acknowledge the frontline clinicians and families at Dr. Sumait Hospital, whose experiences continue to inform efforts to improve context-responsive and patient-centered critical care delivery.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This article was supported by the Center of Research and Development (CRD), SIMAD University, Mogadishu, Somalia.
Disclosure
The authors declare no conflicts of interest related to this work.
References
1. World Health Organization. Measles. [updated November 14, 2024]. Available from: https://www.who.int/news-room/fact-sheets/detail/measles.
2. World Health Organization. Measles vaccines: WHO position paper, April 2017. Wkly Epidemiol Rec. 2017;92(17):205–8.
3. Paules CI, Marston HD, Fauci AS. Measles in 2019: going backward. JAMA. 2019;322(7):599–600. doi:10.1001/jama.2019.1118
4. Centers for Disease Control and Prevention. Measles (Rubeola): for healthcare professionals. Available from: https://www.cdc.gov/measles/hcp/index.html.
5. Moss WJ. Measles. Lancet. 2017;390(10111):2490–2502. doi:10.1016/S0140-6736(17)31463-0
6. Khemani RG, Smith LS, Zimmerman JJ, Erickson S; Pediatric Acute Lung Injury Consensus Conference Group. Pediatric acute respiratory distress syndrome: definition, incidence, and epidemiology: proceedings from the pediatric acute lung injury consensus conference. Pediatr Crit Care Med. 2015;16(suppl 1):S23–S40. doi:10.1097/PCC.0000000000000432
7. Pediatric Acute Lung Injury Consensus Conference Group. Pediatric acute respiratory distress syndrome: consensus recommendations from the pediatric acute lung injury consensus conference. Pediatr Crit Care Med. 2015;16(5):428–439. doi:10.1097/PCC.0000000000000350
8. World Health Organization. Pocket Book of Hospital Care for Children: Guidelines for the Management of Common Childhood Illnesses.
9. Muneeswaran S, Naik A, Basu S, et al. Enhancing acute respiratory infection surveillance with multiplex polymerase chain reaction testing: findings from a 3-year (post-COVID-19) retrospective observational study from an Indian hospital. Prev Med Res Rev. 2026;3(2):66–69. doi:10.4103/PMRR.PMRR_99_25
10. Soni GS, Jadhav JP, Sharma P, Mohandas A, Kapadia JR, Pundkar R. Clinico-investigative profile of the first episode of seizure in children aged 2 months to 5 years in Western Rural Maharashtra, India: a descriptive observational study. Prev Med Res Rev. 2026;3(2):141–144. doi:10.4103/PMRR.PMRR_6_25
11. Sawant DA, Rane S, Shah AK, Raul MU. Factors associated with delayed routine immunisation in children under 5 years of age in an urban slum area. Prev Med Res Rev. 2026;3(Suppl 1):S25–S28. doi:10.4103/PMRR.PMRR_163_24
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Metagenomic Next-Generation Sequencing Contributes to the Diagnosis of Pneumonia Caused by Chlamydia abortus in a Male Patient: Case Report and Literature Review
Gong F, Chen Z, Chang J, Liu J, Wang X, Mo W, Tan M, Jiang T
Infection and Drug Resistance 2023, 16:3463-3468
Published Date: 2 June 2023
Chlamydia Psittaci Pneumonia-Induced Myocarditis: A Case Report
Yang X, Liu Z, Liu X, Li Q, Huang H, Li R, He M
Infection and Drug Resistance 2023, 16:4259-4264
Published Date: 29 June 2023
A Nomogram for Predicting Mortality in Patients with Pneumonia-Associated Acute Respiratory Distress Syndrome (ARDS)
Huang D, He D, Gong L, Jiang W, Yao R, Liang Z
Journal of Inflammation Research 2024, 17:1549-1560
Published Date: 8 March 2024
Coxiella burnetii Should Not Be Ignored: Two Cases of Q Fever Pneumonia Diagnosed by Metagenomic Next-Generation Sequencing
Yao J, Zhang J, Zheng L, Fang W, Lang Y
Infection and Drug Resistance 2025, 18:6227-6239
Published Date: 27 November 2025
Severe Mitral Stenosis in Term Pregnancy Presenting During Labor in a Resource-Limited Setting: A Case Report from Borama, Awdal Region of Somalia

Jama AM, Osman AA, Deria HM, Mousa MM, Jama AM, Ali AO
International Medical Case Reports Journal 2026, 19:564292
Published Date: 26 February 2026