Back to Journals » Journal of Inflammation Research » Volume 17
Serum Proteomic Analysis Revealed Biomarkers for Eosinophilic Chronic Rhinosinusitis with Nasal Polyps Pathophysiology
Authors Chen Y ![]() , Gao R, Liu H, Ye M, Chu L, Wang T
, Gao R, Liu H, Ye M, Chu L, Wang T
Received 11 October 2023
Accepted for publication 1 February 2024
Published 7 February 2024 Volume 2024:17 Pages 805—821
DOI https://doi.org/10.2147/JIR.S444280
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Yu Chen,1 Ru Gao,1 Honghui Liu,1 Maoyu Ye,1 Ling Chu,2 Tiansheng Wang1
1Department of Otolaryngology-Head and Neck Surgery, the Third Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 2Department of Pathology, the Third Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China
Correspondence: Tiansheng Wang, Department of Otolaryngology-Head and Neck Surgery, the Third Xiangya Hospital, Central South University, 138 Tongzipo Road, Yuelu District, Changsha, People’s Republic of China, Email [email protected]
Background: Individuals with eosinophilic chronic rhinosinusitis with nasal polyps(eCRSwNP) exhibited worse outcomes and higher postoperative recurrence rates. This study aimed to identify biomarkers that can aid in the early differentiation of eCRSwNP and enhance our comprehension of its pathophysiology.
Methods: We recruited two independent cohorts. In the discovery cohort, CRSwNP was categorized into eCRSwNP and non-eosinophilic CRSwNP(neCRSwNP), and serum proteomics was performed to identify differentially expressed proteins between the two groups. These candidate proteins were chosen and confirmed in the validation cohort using an enzyme-linked immunosorbent assay (ELISA), Western blot (WB), quantitative real time-polymerase chain reaction (qRT-PCR), immunofluorescence (IF), and their predictive values and associations with tissue eosinophilic pathophysiology were evaluated.
Results: We identified a total of 39 differential proteins between the two groups, including 20 proteins upregulated and 19 downregulated in the eCRSwNP group. Further validation was conducted on the top 5 proteins that were up or down-regulated. Results from the ELISA showed that levels of serum MRC1, CDH13, and MMP2 were significantly higher, TRIM28 was lower in the eCRSwNP group compared to the neCRSwNP group (all P< 0.05), and serum MRC1 (AUC=0.742, P< 0.001) and MMP2 (AUC=0.766, P< 0.001) levels exhibited promising predicting values for eCRSwNP. Moreover, qRT-PCR and WB analysis found that MMP2 and MRC1 expressions were enhanced in the eCRSwNP group compared to the neCRSwNP group (all P< 0.01), and their levels were positively correlated with the number and percentages of tissue eosinophils (all P< 0.01). The IF suggested that MMP2 and MRC1 were overexpressed in the nasal polyps tissues of eCRSwNP patients, and MMP2 was mainly located on eosinophils.
Conclusion: Circulating proteins identified by proteomics could serve as potential preoperative biomarkers for distinguishing eCRSwNP. Among them, MMP2 was enhanced in eCRSwNP and correlated with tissue eosinophilia, which provided valuable insights into the pathophysiology of eCRSwNP.
Keywords: chronic rhinosinusitis with nasal polyps, endotype, eosinophilic, proteomics
Introduction
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a chronic inflammatory disease of the nasal and sinus mucosa characterized primarily by type 2 inflammation.1,2 As society evolves, the prevalence of CRSwNP has been steadily rising each year, affecting approximately 5–15% of the global population and 8% of the Chinese population.3,4 This has notable implications for individuals’ quality of life and imposes substantial economic and societal burdens.5–7 Currently, CRSwNP can be classified into two endotypes based on the extent of eosinophilic infiltration in the tissues: eosinophilic CRSwNP (eCRSwNP) and non-eosinophilic CRSwNP (neCRSwNP).8,9 Nevertheless, the coexistence of CRSwNP with conditions like asthma presents challenges in diagnosing eosinophilic and non-eosinophilic endotypes solely based on the extent of eosinophilic infiltration in tissues.10,11 In addition, prior research has revealed that in contrast to neCRSwNP, individuals with eCRSwNP exhibit suboptimal treatment responses and a higher susceptibility to postoperative recurrence. This poses a greater challenge in the realm of clinical management.12 Hence, comprehending the distinctive attributes of eCRSwNP and pinpointing relevant predictive markers will play a pivotal role in formulating tailored therapeutic strategies and enhancing the overall quality of life for affected patients.
Human serum harbors a wide spectrum of proteins that hold vital functions in upholding homeostasis and orchestrating responses to a range of physiological and pathological circumstances.13 Within this repertoire, one can find acute phase reactants, cytokines, enzymes, antibodies, and an array of other signaling molecules. Collectively, these elements contribute to the intricate and dynamic protein composition found in serum.14 Serum proteomics, as a subset of proteomics, offers a potent and all-encompassing method for investigating the complete protein landscape present in blood samples.13,15 The fundamental approach involves systematically analyzing alterations in the blood proteome throughout the progression of the disease to identify biomarkers specific to that particular condition.15 Its main objective is to discern, measure, and examine the array of proteins within the serum, thereby providing valuable insights into a wide range of physiological and pathological processes.13,16,17 The utilization of serum proteomics has played a pivotal role in advancing our comprehension of diseases, including cancer,18 cardiovascular disorders,19 autoimmune diseases,20 and inflammatory diseases.21 Zhou et al22 using serum proteomics identified the combination of SAA1 and CD248 as an early diagnostic marker for systemic lupus erythematosus. Through the comparison of serum protein profiles between healthy individuals and patients suffering from particular diseases, researchers can identify disease-specific biomarkers.23 These biomarkers have significant potential to contribute to early disease diagnosis, forecast disease progression, and support the development of personalized treatment approaches.24,25 In recent years, proteomics has been increasingly applied in the mechanistic studies of chronic rhinosinusitis.10,26 Researchers have discovered distinct disease-specific protein expression profiles in the nasal mucosa of chronic rhinosinusitis patients, and several proteins have been confirmed to play significant roles in its pathogenesis.10 However, limited studies have concentrated on the changes in circulating proteins among eCRSwNP patients, and a shortage of research employing serum proteomics to explore its underlying mechanisms is evident.
Hence, the present study seeks to explore unique shifts in protein expression associated with eCRSwNP by conducting a proteomic analysis of serum samples obtained from both eCRSwNP and neCRSwNP patients. Consequently, the objective is to attain a more comprehensive insight into the pathogenesis of eCRSwNP and its connection to serum protein components.
Materials and Methods
Participants and Settings
The present study was approved by the Ethics Committee of the Third Xiangya Hospital of Central South University (No. 23474). All participants signed written informed consent before their recruitment. We recruited two independent CRSwNP cohorts, including the discovery cohort and the validation cohort. The discovery cohort includes 8 neCRSwNP and 8 eCRSwNP patients. We enrolled 80 patients with CRSwNP in the validation cohort, comprising 40 cases of neCRSwNP and 40 cases of eCRSwNP. CRSwNP was diagnosed following the guidelines of the 2012 European Position Paper on Rhinitis and Nasal Polyps.27 We implemented distinct exclusion criteria, encompassing: (1) individuals aged below 18 years or above 70 years; (2) recent administration of antibiotics, oral or systemic corticosteroids, immunotherapy, or anti-allergy medication within 1 month before surgery; (3) coexistence of other nasal or sinus conditions; (4) confirmation of other inflammatory or autoimmune disorders; and (5) severe cardiac ailments, renal or other organ impairments, and pregnancy. The preoperative CT scores and nasal endoscopy scores were documented using the Lund-Mackay and Lund-Kennedy scoring systems, respectively.28 Demographic and clinical data were collected, including gender, age, body mass index (BMI), coexisting diseases, visual analog scale (VAS), tissue and blood eosinophil counts, and percentages.
Diagnosis of eCRSwNP and neCRSwNP
Nasal polyp tissues were taken from all patients during the surgery, then soaked in 10% formalin and embedded with paraffin wax. Paraffin-embedded samples were sectioned into 4-mm slices and subjected to hematoxylin and eosin (HE) staining. All stained specimens were examined at a high-power field (HPF) (×400) to evaluate the infiltration of inflammatory cells, including eosinophils. The eosinophil count was determined by averaging the counts from 5 randomly selected HPFs, and the eosinophil percentage was calculated as the ratio of the eosinophil count to the total number of inflammatory cells. The eosinophil counts were in 5 randomly selected fields. The diagnostic criterion for eCRSwNP was set at an eosinophil count exceeding 10 cells/HPF, otherwise defined as neCRSwNP.8
Serum Proteomics Analysis
Serum samples were collected from patients with CRSwNP in the discovery cohort, and serum proteomics analysis was conducted using liquid chromatography-tandem mass spectrometry (LC-MS/MS) as previously outlined.20,29 Briefly, serum samples were processed to extract total proteins, and their concentration was determined using the BCA assay. Subsequently, 100 μg of protein underwent acetone precipitation, followed by redissolution, reduction, alkylation, protein digestion, and final peptide desalting. For the LC-MS/MS experiment, the separation of tryptic peptides was carried out using an Ultimate 3000 nano-LC system coupled to a nano electrospray ionization (ESI) source. The ionized peptides were directed through a Q Exactive HF mass spectrometer from Thermo Fisher Scientific. A 2 μg protein digest was introduced into a trapping column and subsequently moved to an analytical column. Tryptic peptides were then separated at a flow rate of 250 nL/min, employing a gradient elution with solvent A (water containing 0.1% formic acid) and solvent B (80% acetonitrile with 0.1% FA). Data-dependent acquisition (DDA) was performed in positive mode using the Orbitrap analyzer, following the established protocol.21 Both MS1 and MS2 scans were executed, with the selection of the 20 most intense ions for subsequent fragmentation. A dynamic exclusion time window of 45 seconds was applied, and ions with a single charge or a charge exceeding 6 were excluded from the DDA process.
Differential Protein Analysis and Bioinformatic Analysis
Principal component analysis (PCA) was utilized to explore the predominant latent serum proteins within the dataset. Proteins exhibiting differential expression, characterized by p values <0.05 and fold changes >1.5 or <2/3, were visualized using a heatmap generated by an R package. Differential expression analysis between the two groups was conducted using paired two-class analysis from the same R package, with a false discovery rate (FDR) threshold of 0.05. Differential expression of proteins between eCRSwNP and neCRSwNP patients was further examined through Reactome-based pathway enrichment analysis. The significance of pathway enrichment was determined using the Fisher exact test, and pathways with an FDR threshold of 0.05 were considered significantly modulated. To enhance understanding, Gene Ontology (GO) categories and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analyses were carried out using the OmicsBean database, accessible at http://www.omicsbean.cn.
Validation of Differentially Expressed Proteins by Enzyme-Linked Immunosorbent Assay (ELISA)
Enzyme-linked immunosorbent assay (ELISA) was performed in the validation cohort to examine the differentially expressed proteins detected by serum proteomics. To thoroughly validate differentially expressed proteins, we selected the top 5 up-regulated and down-regulated proteins for confirmation based on FC values. The serum concentrations of these proteins were quantified using commercially available ELISA kits following the manufacturer’s instructions. Mannose receptor C-type 1 (MRC1) kits (Cat: CSB-E09961h), cadherin 13 (CDH13) kits (Cat: CSB-E13817h), cluster of differentiation 5 antigen-like (CD5L) kits (Cat: CSB-E13423h), matrix metalloproteinase-2 (MMP2) kits (Cat: CSB-E04675h), plasma protease C1 inhibitor (SERPING1) kits (Cat: CSB-EL021086HU), insulin-like growth factor-binding protein 5 (IGFBP5) kits (Cat: CSB-EL010901HU), tripartite motif-containing protein 28 (TRIM28) kits (Cat: CSB-EL024502HU), and fatty acid-binding protein 5 (FABP5) kits (Cat: CSB-EL007946HU) were purchased from Cusabio (Wuhan, China). Neural cell adhesion molecule L1-like protein (CHL1) kits (Cat: IHUUCHL1KT) and leukotriene A-4 hydrolase (LTA4H) ELISA kits (Cat: IHULTA4HKT) were provided by Innov Research (Michigan, USA). To ensure objectivity, the assay operators were blinded to the detailed data of patients.
Western Blot (WB) Analysis
Polyp tissues were extracted from liquid nitrogen, and each sample was lysed with 1 mL of a lysing solution containing 1× protease inhibitor. Protein concentration was determined by the BCA method by adding an appropriate amount of Loading-buffer sampling buffer and mixing, followed by heating at 100°C for 5 min. A protein sample of 10 μg per well was taken and separated at a consistent current of 70 V in SDS-PAGE until the dye front reached the end of the separation gel. Subsequently, the electrophoresis gel was transferred to a PVDF membrane under 100 V conditions for 100 min. Following this step, the PVDF membrane was cut into strips based on molecular weight size and incubated in 5% skimmed milk for one hour at room temperature. After TBST washing, the strips of PVDF membranes were incubated overnight at 4°C with the following primary antibodies: MRC1 (Cat: DF4149, 1:1000), MMP2 (Cat: AF5330, 1:1000), CDH13 (Cat: AF5203, 1:1000), TRIM28 (Cat: DF7531, 1:1000), and β-actin (Cat: AF7018, 1:3000) (Affinity, China). The following day, the corresponding secondary antibody (Cat: #S0001, 1:3000) (Affinity, China) was allowed to incubate at room temperature for 1 hour. Protein signals were detected utilizing the ECL system. The protein grayscale was quantified using ImageJ software. The quantification of the target protein’s expression level was achieved by normalizing it against β-actin.
Quantitative Real-Time Polymerase Chain Reaction (qRT-PCR) Analysis
Total RNA was extracted from the tissue samples using Trizol reagent (Invitrogen, USA) following the manufacturer’s protocol. Subsequently, the RNA was reverse transcribed using a commercially available kit (US EVERBRIGHT, Suzhou, China). To perform qRT-PCR, we used a PCR system and SYBR Premix EX Taq (US EVERBRIGHT, Suzhou, China) with the following primers’ sequences (Table S1). We analyzed the relative mRNA levels of the target genes using the comparative threshold cycling (2-ΔΔCt) method. GAPDH was used as a loading control.
Immunofluorescence (IF)
IF was performed as described previously.30 Briefly, all nasal biopsy specimens embedded in paraffin were sectioned into 4-mm slices using a Leica microtome (Leica, Wetzlar, Germany). Sections were incubated with primary antibodies against MRC1 (Cat: DF4149, 1:100), MMP2 (Cat: AF5330, 1:100), CDH13 (Cat: AF5203, 1:100), and TRIM28 (Cat: DF7531, 1:100) (Affinity, China) overnight at 4 °C, and two rounds of staining were performed with 594-conjugated secondary antibodies (Cat: #S00019, 1:200) (Affinity, China). Finally, 30 μL DAPI solution was added to each slice to visualize the nuclei. Triple fluorescence staining was conducted as our previous study described with the Opal 6-Plex Detection Kit (Cat: NEL821001KT, PerkinElmer, USA).31 According to the instructions provided in the manual, sections were incubated with primary antibodies against MMP2, MRC1 (Cat: DF4149, 1:100), major basic protein (MBP) (Cat: AF4085, 1:200), and Siglec8 (Cat: DF14551, 1:200) (Affinity, China) for 2 h. Then, sections were incubated with the secondary antibody for 10 min with the Opal polymer horseradish peroxidase. Afterward, the Opal 6-Plex Detection Kit was employed for the visualization of Tyramide Signal Amplification, which includes Opal 520, Opal 550, and Opal 620. Then, 30 μL DAPI solution was added to each slice to visualize the nuclei. All slides were sealed with cover glass, and the images were observed and collected by fluorescence microscope in the dark room. In the final analysis, the recorded data included the relative fluorescence expression and the number of co-expressed positive cells, which were then subjected to comparison.
Statistical Analysis
Categorical data were displayed in a numerical format and subjected to comparison using the Chi-square test. For normally distributed data, the mean and standard deviation (SD) were presented, while non-normally distributed data were represented by the median and interquartile range. Receiver operating characteristic (ROC) curves were generated to assess and compare the discriminatory capabilities of various proteins for identifying eCRSwNP. Spearman correlation analysis was conducted to evaluate the associations between eosinophil counts and percentages and levels of different proteins. Statistical analyses were conducted utilizing SPSS (version 23.0), and graphical representations were generated using GraphPad Prism 8.0. Statistical significance was defined as P values < 0.05.
Result
Subject Characteristics in the Discovery Cohort
In the discovery cohort, 16 CRSwNP patients were recruited, including 8 eCRSwNP patients and 8 neCRSwNP patients. Table 1 demonstrates a notable increase in tissue and blood eosinophil count and percentage within the eCRSwNP group compared to the neCRSwNP group (P<0.05). Nevertheless, there were no statistically significant differences observed in terms of sex, age, BMI, allergic rhinitis, asthma, VAS score, Lund-MacKay score, and Lund-Kennedy score between the two groups (P>0.05).
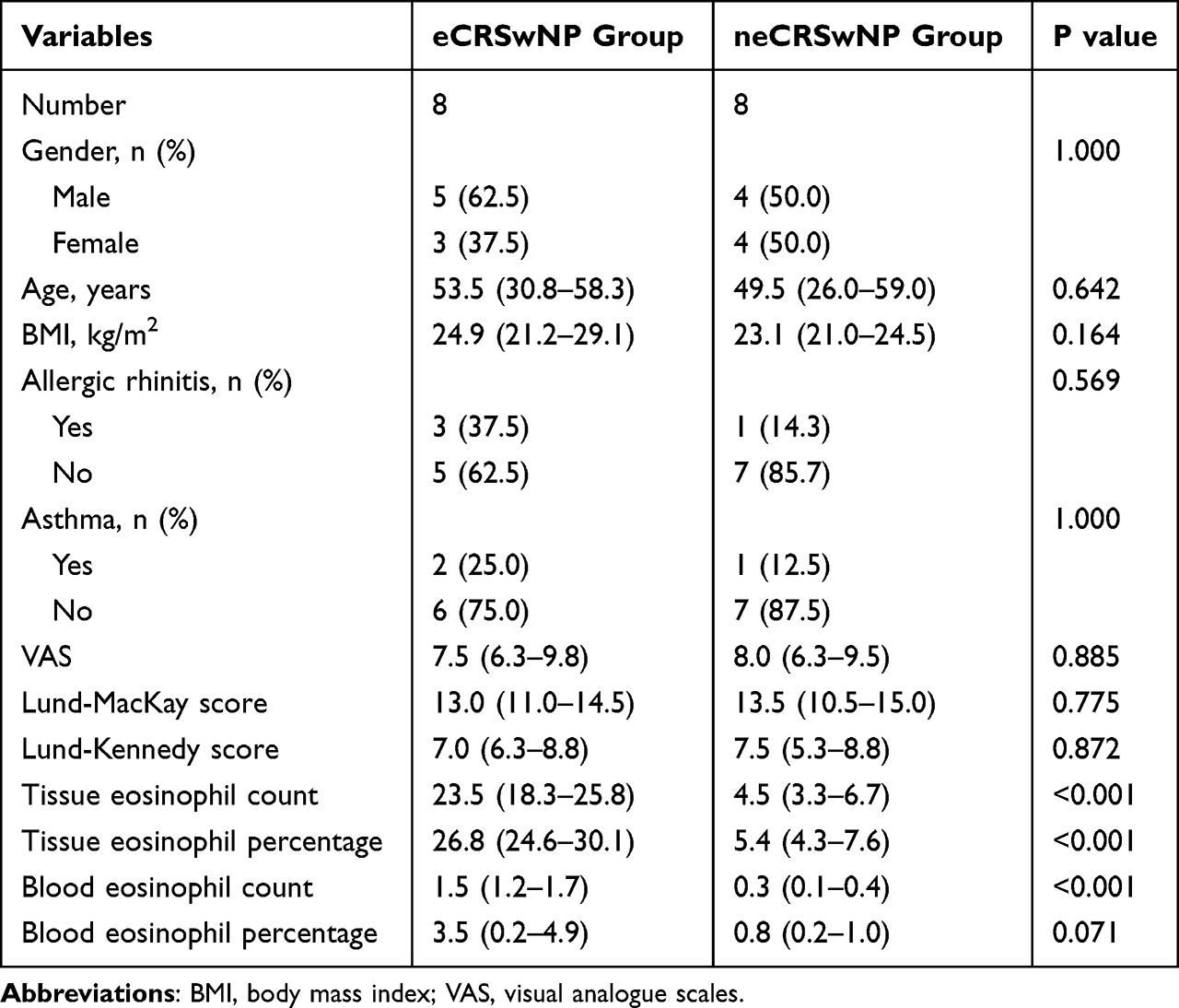 |
Table 1 Demographics and Clinical Characteristics of CRSwNP Patients |
Serum Protein Profiles Between eCRSwNP and neCRSwNP Groups
Figure 1A displays the outcomes of the identified and quantified proteins. Among these proteins, a total of 39 demonstrated distinct expression patterns between the two groups, with 20 exhibiting up-regulation and 19 showing down-regulation in the eCRSwNP group as compared to the neCRSwNP group. The application of PCA to the proteomics data of whole serum proteins displayed distinctive and separate clustering of samples from the eCRSwNP and neCRSwNP groups (Figure 1B). Further analysis using the heatmap and volcano plot depicted in Figure 1C and D revealed significant differences in protein expression patterns between the two groups. To enhance our understanding of the roles and associations of the differentially expressed proteins implicated in the pathological mechanisms of eCRSwNP, we performed GO and KEGG analyses. The GO analysis results revealed that the highest percentage of enriched differentially expressed proteins was associated with several cellular biological processes (Figure 2A). Moreover, the most prominently enriched KEGG pathways among the differentially expressed proteins encompassed complement, coagulation cascades, and matrix metalloproteinases (Figure 2B).
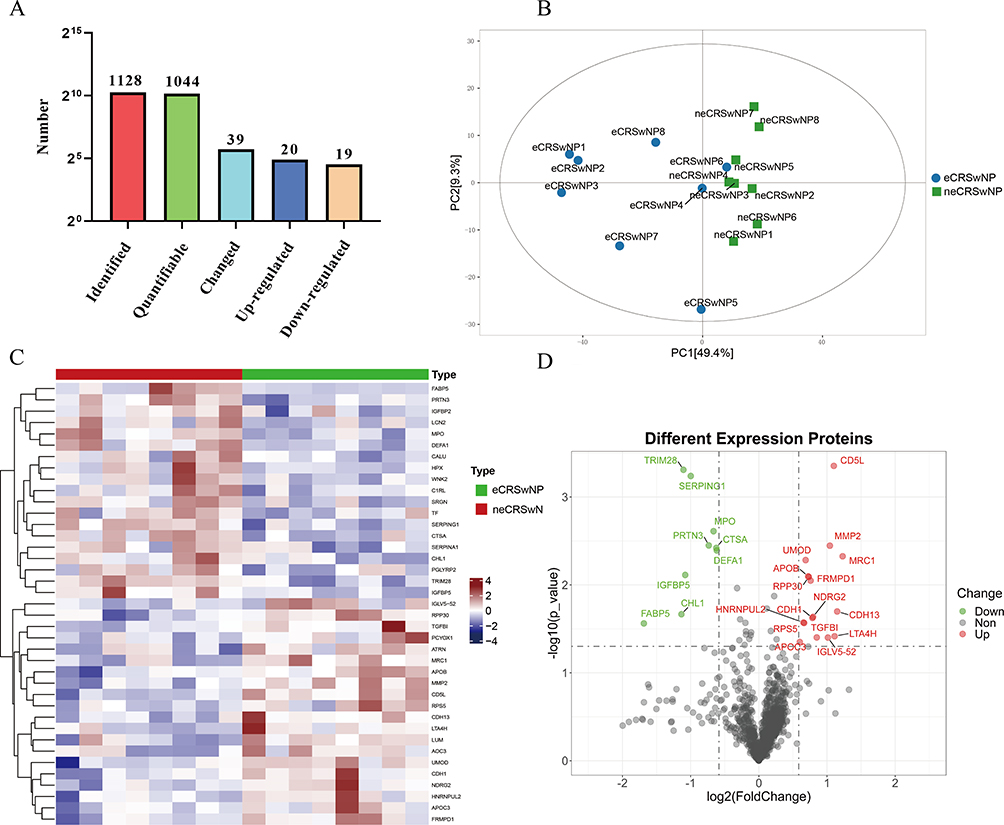 |
Figure 1 Differentially expressed proteins between the eCRSwNP and neCRSwNP groups were identified by serum proteomic. (A) The number of identified and quantified proteins; (B) PCA of total detected proteins. (C and D) Heatmap and volcano of overlapping proteins between the two groups. Abbreviations: eCRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; neCRSwNP, non-eosinophilic chronic rhinosinusitis with nasal polyps; PCA, principal component analysis. |
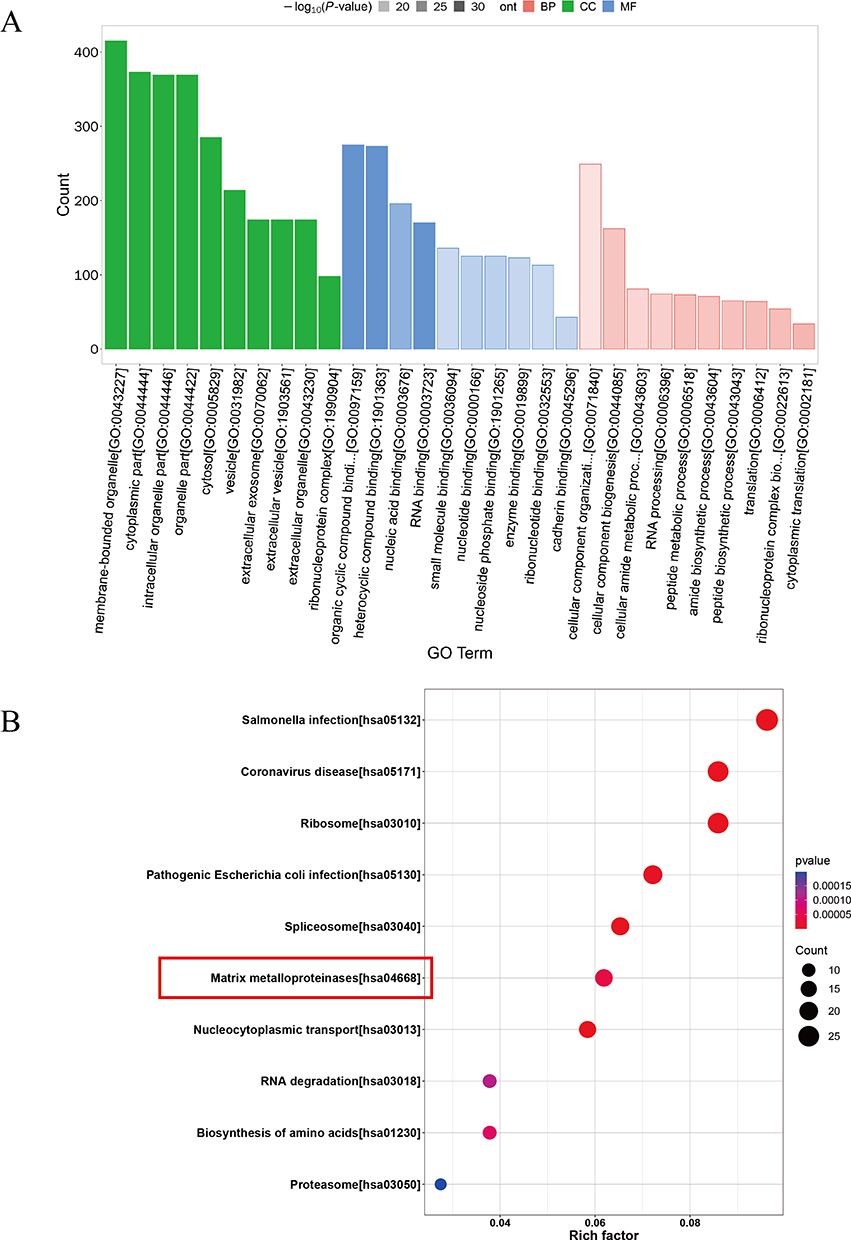 |
Figure 2 GO and KEGG analysis of differentially expressed proteins between eCRSwNP and neCRSwNP groups. Abbreviations: eCRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; neCRSwNP, non-eosinophilic chronic rhinosinusitis with nasal polyps. GO, Gene Ontology; KEGG, Kyoto Encyclopedia of Genes and Genomes. |
Validation of Differentially Expressed Proteins in the Validation Cohort
To corroborate the outcomes of the serum proteomics analysis, we evaluated the serum concentrations of the five most up-regulated and down-regulated differentially expressed proteins within the validation cohort (Table 2). The comparisons of protein abundances between the two groups are presented in Figure S1. The validation cohort consists of 80 patients with CRSwNP, including 40 patients with eCRSwNP and 40 patients with neCRSwNP. Their characteristics are summarized in Table 3. The eCRSwNP group exhibits elevated counts and percentages of eosinophils in both tissue and blood compared to the neCRSwNP group. However, no statistical differences are observed in other clinical variables between the two groups. The ELISA results shown in Figure 3 indicated notably elevated levels of serum MRC1, CDH13, and MMP2 within the eCRSwNP group, accompanied by decreased levels of TRIM28, in comparison to the neCRSwNP group (P<0.05). Interestingly, the serum MRC1 and MMP2 levels were positively correlated with tissue eosinophil count and percentage (P<0.05, Table S2). Furthermore, the ROC curves demonstrated that serum levels of MRC1 and MMP2 exhibited higher diagnostic efficacy for distinguishing eCRSwNP compared to the other proteins (Figure 4). The detailed parameters are listed in Table 4.
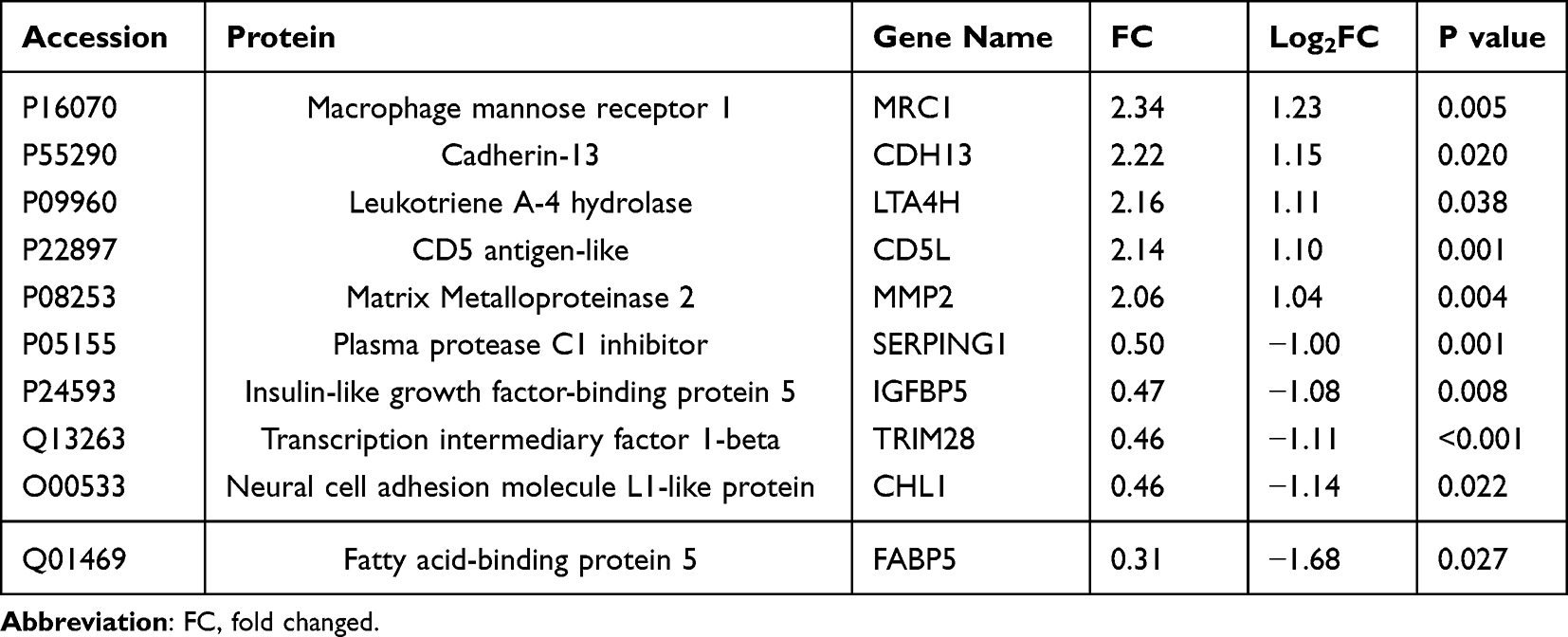 |
Table 2 The Up-Regulated and Down-Regulated Top 5 Proteins Between the Two Groups |
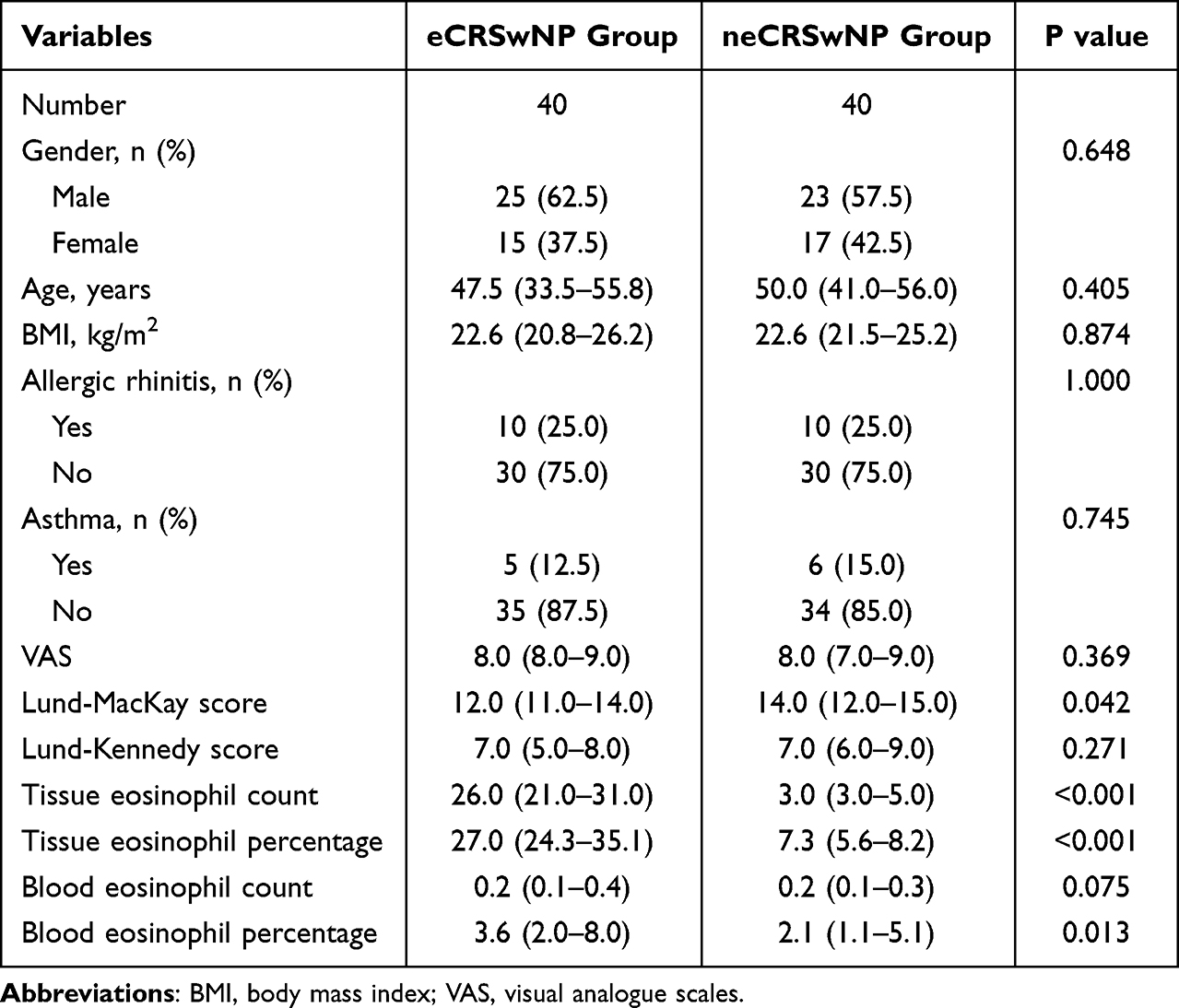 |
Table 3 The Characteristics of CRSwNP Patients in the Validation Cohort |
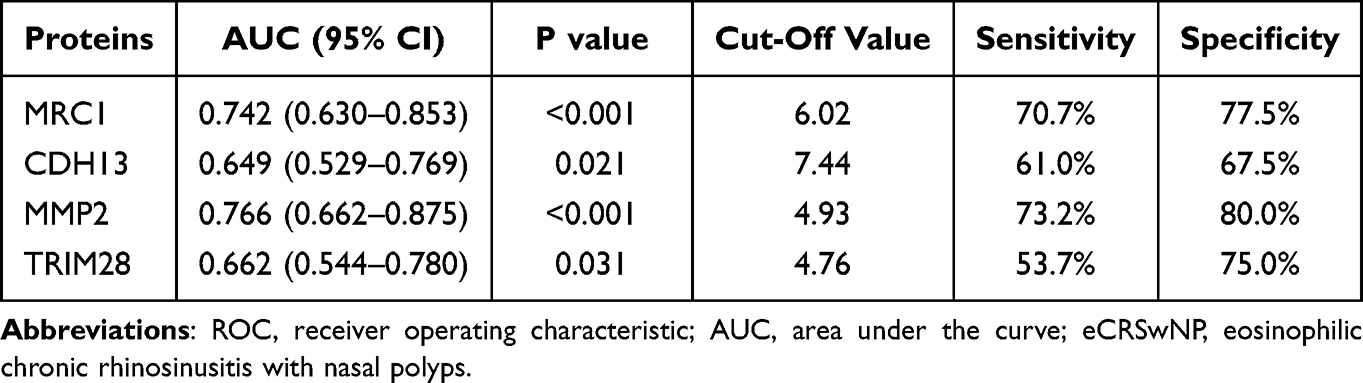 |
Table 4 ROC Curves of Serum Proteins in Predicting eCRSwNP |
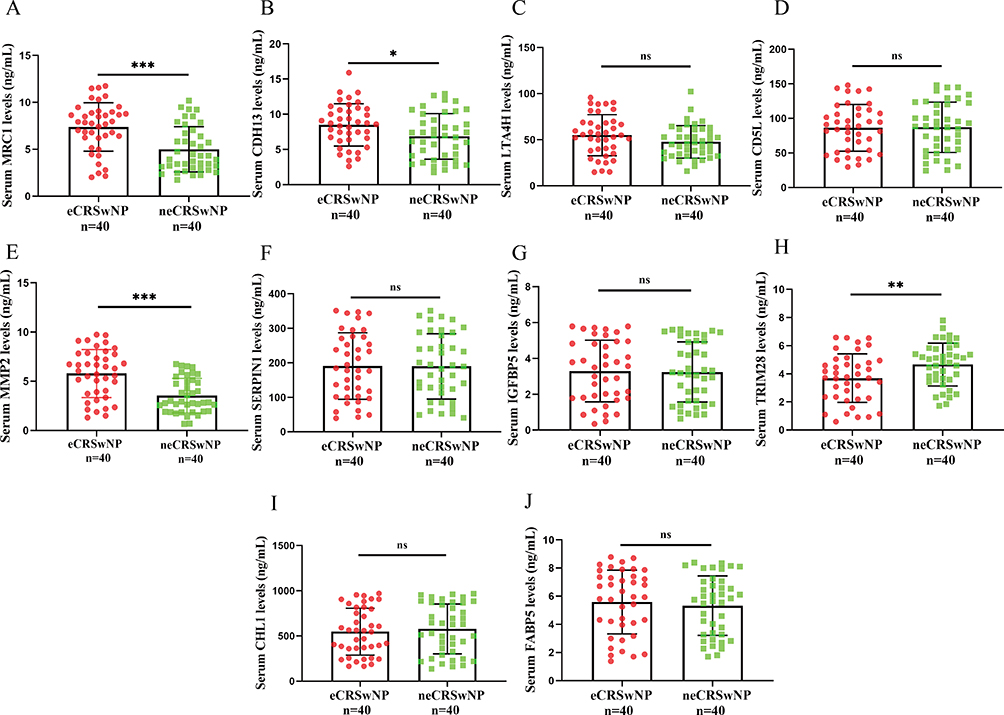 |
Figure 3 Validation of the top 5 up and down-regulated proteins in an independent validation cohort. (A–E) comparison of serum MRC1, CDH13, LTA4H, CD5L and MMP2 concentrations between the eCRSwNP and neCRSwNP groups. (F–J) comparison of serum SERPING1, IGFBP5, TRIM28, CHL1 and FABP5 levels between the eCRSwNP and neCRSwNP groups. *P<0.05; **P<0.01; ***P<0.001. Abbreviations: eCRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; neCRSwNP, non-eosinophilic chronic rhinosinusitis with nasal polyps; ns, no significance. |
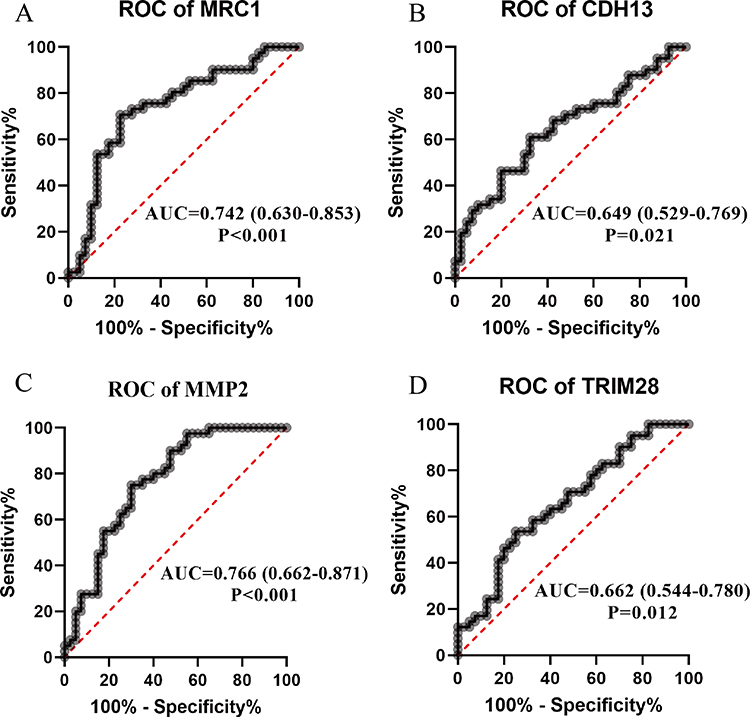 |
Figure 4 ROC curves evaluating the discriminative abilities of candidate proteins for eCRSwNP. (A) MRC1, (B) CDH13, (C) MMP2, (D) TRIM28. Abbreviations: ROC, receiver operator characteristic; eCRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps. |
Tissue Expression of Differentially Expressed Proteins in Validation Cohort
To further investigate the roles of differentially expressed proteins in the pathophysiology of eCRSwNP, we conducted additional validation within nasal polyps tissues. Both qRT-PCR (Figure 5) and WB analysis results (Figure 6) revealed notable overexpression of MMP2 and MRC1 in eCRSwNP patients compared to neCRSwNP patients (P<0.05). Moreover, the IF results provided further evidence that MRC1 and MMP2 were overexpressed in the tissues of eCRSwNP patients compared to neCRSwNP patients (Figure 7). To gain a deeper understanding of the connections between tissue MRC1 and MMP2 expressions and the presence of eosinophils, we conducted multiplexed immunofluorescence staining using two eosinophil markers (MBP and Siglec8). We observed extensive co-staining among MMP2, MBP, and Siglec8 in the eCRSwNP group compared to the neCRSwNP group. However, this phenomenon was not observed in MRC1 between the two groups (Figures 8 and 9).
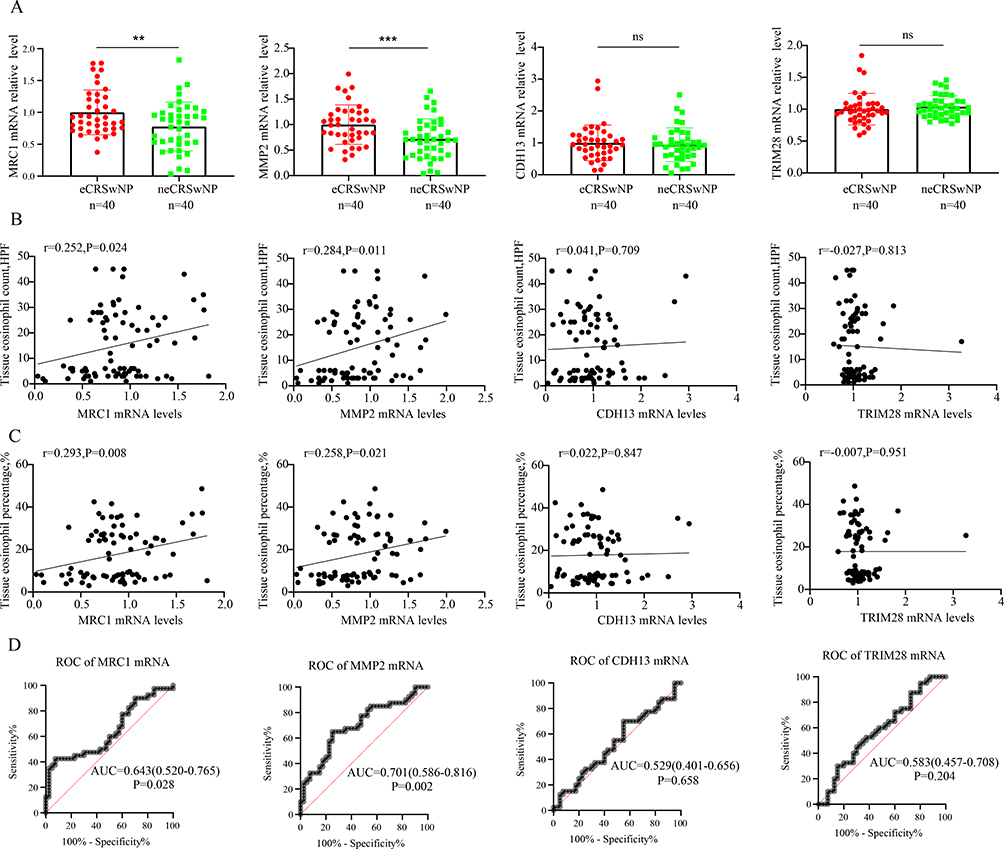 |
Figure 5 Tissue mRNA expressions of four candidate biomarkers and their associations with the degree of tissue eosinophilic inflammation between the two groups. (A) Tissue mRNA expressions between the two groups. (B and C) The correlations between tissue mRNA expressions and tissue eosinophil count and percentage. (D) ROC curves evaluate the discriminative abilities of four candidate biomarkers for eCRSwNP. **P<0.01; ***P<0.001. Abbreviations: eCRSwNP, eosinophilic chronic rhinosinusitis with nasal polyps; ROC, receiver operator characteristic; ns, no significance. |
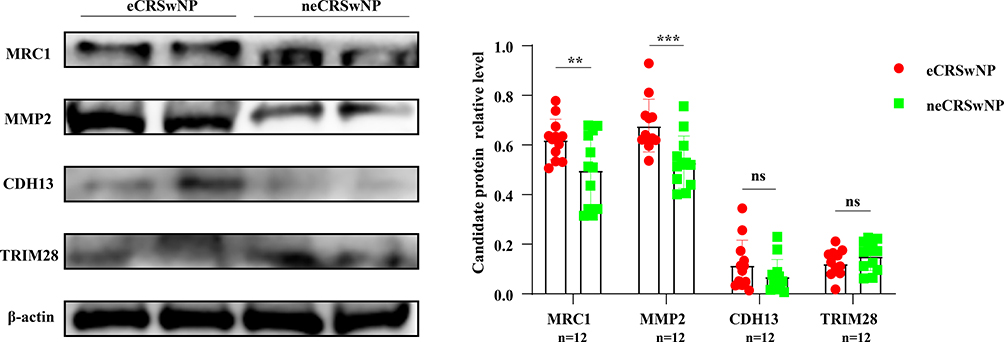 |
Figure 6 WB evaluates the tissue proteins of four biomarkers between the two groups. **P<0.01; ***P<0.001. Abbreviations: WB, Western blot; ns, no significance. |
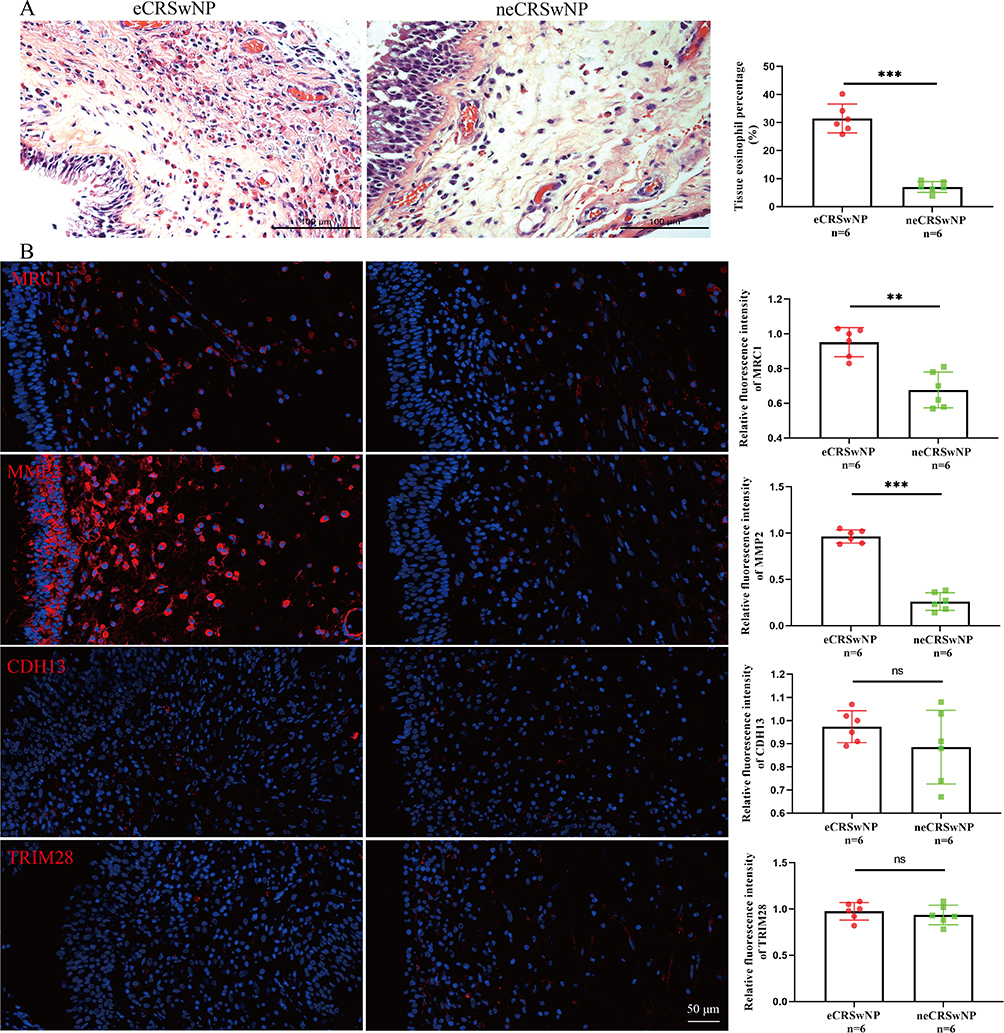 |
Figure 7 HE and immunofluorescence staining in the tissues between the two groups. (A) HE staining of nasal polyp samples and comparison of tissue eosinophil percentage between the two groups. (B) immunofluorescence staining of four proteins and their relative fluorescence intensities between the two groups. **P<0.01; ***P<0.001. Abbreviations: HE, hematoxylin, and eosin; ns, no significance. |
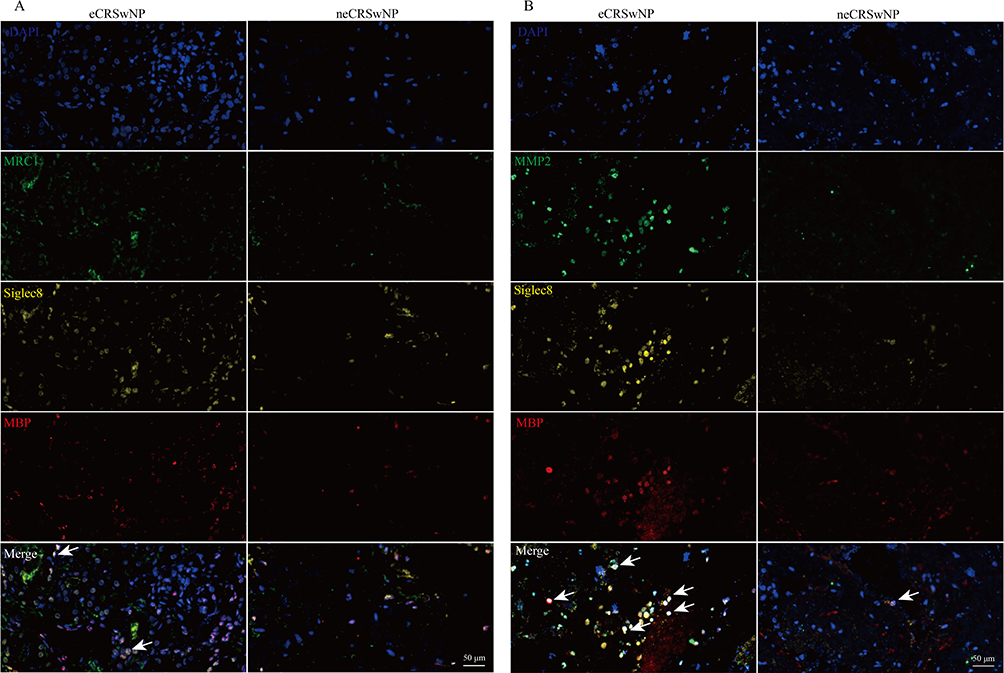 |
Figure 8 Multiplex immunofluorescence staining exploring the co-expressions of MRC1 (A), MMP2 (B), and eosinophil markers. Cells with evident co-expression are indicated by white arrows. |
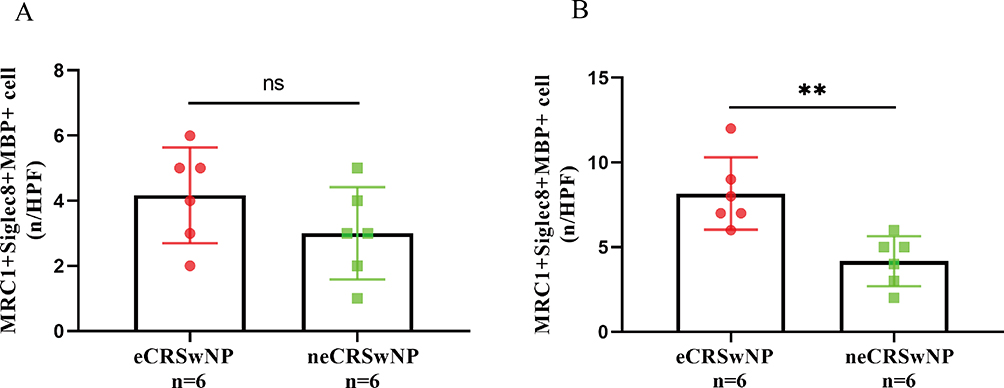 |
Figure 9 Comparison of the number of positive co-staining cells between the two groups. **P<0.01. Abbreviation: ns, no significance. |
Discussion
eCRSwNP is a complex inflammatory disorder characterized by persistent eosinophilic inflammation, poor prognosis, and a high risk of postoperative recurrence.32,33 Currently, the pathological and physiological mechanisms of eCRSwNP remain unclear. Its diagnosis primarily relies on pathological tissue section examination and eosinophil count, which is invasive and subject to certain subjectivity.34,35 Although previous studies have identified several potential biomarkers for predicting eCRSwNP, such as serum metabolomics,36 nasal microbiota,37 and the peripheral blood lymphocyte-to-eosinophil ratio,38 their sensitivity and specificity remain relatively constrained, hindering their adoption in clinical settings. Therefore, the exploration of objective biomarkers for eCRSwNP is still a current research focus, which will contribute to achieving personalized precision treatment.
Serum proteomics is a scientific field that studies the comprehensive composition of proteins in serum and their changes.13,16,39 Alterations in circulating proteins have been documented in a variety of inflammatory diseases, and serum proteomics offers insights into the pathophysiology of the disease, aids in disease diagnosis, tracks disease advancement, and predict the prognosis.20,40,41 Diorio et al42 identified fms-like tyrosine kinase 3 and mast cell immunoglobulin-like receptor 1 as predictive biomarkers of severe cytokine release syndrome and found IL18 as a possible targetable cytokine in immune effector cell–associated neurotoxicity syndrome by serum proteomics. However, there are no clear results regarding serum protein expression profiles of eCRSwNP patients and the association between differentially expressed proteins and eosinophilic inflammation. In this study, we performed a novel application of serum proteomic analysis to identify and validate potential serum proteins for the preoperative diagnosis of eCRSwNP and exploration of its pathophysiology. Our results revealed discernible variations in serum protein expression patterns between the eCRSwNP and neCRSwNP groups, and the differentially expressed proteins encompassed complement, coagulation cascades, and matrix metalloproteinases. Specifically, heightened serum levels of MRC1, MMP2, and CDH13 were observed in eCRSwNP patients, accompanied by diminished TRIM28 levels. Remarkably, ROC curves demonstrated that these four biomarkers showcased promising diagnostic precision in distinguishing eCRSwNP, particularly serum MRC1, and MMP2. These findings underscore the significance of serum proteomics as an invaluable tool for preoperative eCRSwNP diagnosis, thereby contributing to personalized treatment strategies and enhanced disease prognosis.
Our results demonstrated a substantial elevation in serum MMP2 levels among eCRSwNP patients, exhibiting a positive correlation with both tissue and circulating eosinophilic inflammation levels. Additionally, serum MMP2 levels displayed robust predictive potential for eCRSwNP. Notably, tissue analysis revealed heightened MMP2 expression in eCRSwNP tissues, aligning with tissue eosinophil counts and percentages. Furthermore, a significant portion of MMP2-positive cells co-localized with eosinophils. These findings strongly implied that MMP2 could hold a pivotal role in the pathogenesis of eCRSwNP. MMP2 plays a crucial role as an enzymatic protein in regulating the degradation and remodeling of the extracellular matrix.43,44 Consequently, it influences cell migration, tissue repair, and the inflammatory process.45,46 Furthermore, MMP2 is implicated in the migration and infiltration of eosinophils, indicating that its activity can hold significance in modulating the eosinophilic inflammatory response.47,48 It was found that MMP2 possessed the capability to enhance the infiltration and aggregation of eosinophils at the inflammation site through its control over the degradation of the extracellular matrix and the dissociation of extracellular matrix molecules.49 Moreover, a prior study revealed that the increased expression of MMP-2 and MMP13 in allergic nasal mucosa could expedite eosinophil migration to the nasal mucosa among patients with allergic rhinitis. This observation underscored the dynamic participation of MMPs in the pathogenesis of allergic rhinitis.50 Furthermore, MMP-2 promotes eosinophil migration and inflammation by enhancing microvessel permeability, resulting in edema formation at the site of inflammation.51 It was widely recognized that nasal mucosal tissue remodeling and extensive eosinophil infiltration were significant pathological characteristics of eCRSwNP.52,53 Overwhelming inflammatory reactions could lead to the impairment of nasal mucosa epithelial and basal cells, ultimately fostering increased cell migration and synthesis of the extracellular matrix. This cascade exacerbated tissue fibrosis, eosinophil chemotaxis, and recruitment, then contributes to the formation of nasal polyps.54 Despite previous studies confirming the upregulation of MMP2 expression in both neCRSwNP and eCRSwNP, an increasing body of evidence suggests that MMP2 plays a more significant role in tissue remodeling mediated by eosinophils.49,55 Hence, building upon prior investigations and our study outcomes, we posit that heightened MMP2 levels can facilitate extracellular matrix degradation and initiate tissue remodeling by modifying nasal epithelial architecture. Furthermore, MMP2 is presumed to play a role in directing eosinophils toward infiltrating the epithelial tissue, thereby initiating eosinophilic inflammation within the nasal epithelium. These dual influences collectively contribute to the underlying pathology of eCRSwNP. However, a more comprehensive understanding of the exact mechanism behind these interactions requires further exploration.
Another important finding was that both circulating and tissue MRC1 were highly expressed in patients with eCRSwNP, and positively correlated with the number and percentage of tissue eosinophils. ROC results suggested that serum MRC1 could be used as a biomarker for distinguishing eCRSwNP. MRC1 is also known as CD206, which is a marker of macrophage M2 polarization.56 Importantly, macrophage M2 polarization exhibits a notable connection with the activation of eosinophil migration. Research has demonstrated that in allergic conditions, activated M2 macrophages release substantial quantities of type 2 chemokines, including C-C motif chemokine ligand (CCL)-17 and eosinophil chemotactic proteins. These chemokines serve to intensify eosinophilic inflammation, thereby contributing to the exacerbation of inflammatory diseases.57,58 In addition, Peterson et al found that the accumulation and activation of M2 macrophages in CRSwNP may further enhance tissue eosinophilia through the production of eosinophilic chemokines, thereby promoting an eosinophilic inflammatory response.59 Furthermore, an elevated polarization of M2 macrophages was prominently observed in CRSwNP. This heightened polarization was shown to exert control over cytokine production and chemokine release, subsequently exerting an influence on the severity and duration of the inflammatory process.60 Hence, amalgamating prior literature with our findings, we postulate that MRC1 plays a significant role in the pathology of eCRSwNP by fostering the migratory infiltration of eosinophils, thereby contributing to the escalation of eosinophilic inflammation.
However, it is essential to acknowledge several limitations of this study. Firstly, this research is based on a single center with a restricted sample size, potentially impacting the generalizability of the findings. Hence, additional validation in larger and more diverse populations is necessary. Secondly, there is a lack of standardized criteria for the diagnosis of eCRSwNP, leading to possible discrepancies in determining endophenotypes. Finally, our investigation solely focused on examining the expressions of candidate proteins in both circulating and tissue samples, along with their correlation with eosinophilic inflammatory pathology in eCRSwNP. However, we did not delve into cellular mechanisms to explore how these proteins might affect the functionality of eosinophils. In subsequent studies, we will further confirm our results and related pathological mechanisms by performing multicenter validation, in vitro/in vivo functional studies, and epigenetic perspectives.
Conclusion
This study pioneered the use of serum proteomics to identify potential biomarkers for the preoperative diagnosis of eCRSwNP. Our findings highlight several circulating proteins as promising biomarkers for preoperative distinguishing eCRSwNP, and MMP2 was demonstrated to be augmented in eCRSwNP and correlated with tissue eosinophilia. These findings enhance our comprehension of how circulating proteins impact the progression of eCRSwNP and offer insights into potential therapeutic mechanisms for this condition.
Ethics and Consent Statements
This study was approved by the ethical committee of the Third Xiangya Hospital of Central South University (No.23474). All experiments involving human participants adhered to the institutional ethical guidelines and followed the principles of the Declaration of Helsinki. All participants signed informed consent.
Funding
This research was supported by the National Natural Science Foundation of China (No. 82270003), the Natural Science Foundation of Hunan Province (No. 2022JJ70153), and the Natural Science Foundation of Changsha (No. kq2202429).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Scadding GK, Scadding GW. Biologics for chronic rhinosinusitis with nasal polyps (CRSwNP). J Allergy Clin Immunol. 2022;149:895–897. doi:10.1016/j.jaci.2021.10.029
2. Gelardi M, Bocciolini C, Notargiacomo M, et al. Chronic rhinosinusitis with nasal polyps: how to identify eligible patients for biologics in clinical practice. Acta Otorhinolaryngol Ital. 2022;42:75–81. doi:10.14639/0392-100X-N1699
3. Xie S, Zhang C, Xie Z, et al. Serum metabolomics identifies uric acid as a possible novel biomarker for predicting recurrence of chronic rhinosinusitis with nasal polyps. Rhinology. 2023;61:541–551. doi:10.4193/Rhin23.236
4. Xu X, Seet JE, Yap QV, et al. Latent class analysis of structured histopathology in prognosticating surgical outcomes of chronic rhinosinusitis with nasal polyps in Singapore. Rhinology. 2023;61:358–367. doi:10.4193/Rhin22.455
5. Sedaghat AR, Singerman KM, Phillips KM. Discordance of chronic rhinosinusitis disease control between EPOS guidelines and patient perspectives identifies utility of patient-rated control assessment. Rhinology. 2022;60:444–452. doi:10.4193/Rhin22.160
6. Fokkens WJ, Viskens AS, Backer V, et al. EPOS/EUFOREA update on indication and evaluation of biologics in chronic rhinosinusitis with nasal polyps 2023. Rhinology. 2023;61:194–202. doi:10.4193/Rhin22.489
7. La Mantia I, Ragusa M, Grigaliute E, et al. Sensibility, specificity, and accuracy of the sinonasal outcome test 8 (SNOT-8) in patients with chronic rhinosinusitis (CRS): a cross-sectional cohort study. Europ Archiv Oto Rhin Laryngol. 2023;280:3259–3264. doi:10.1007/s00405-023-07855-8
8. Abbas EE, Li C, Xie A, et al. Distinct clinical pathology and microbiota in chronic rhinosinusitis with nasal polyps endotypes. Laryngoscope. 2021;131:E34–E44.
9. Wu PW, Chiu CH, Huang YL, et al. Tissue eosinophilia and computed tomography features in paediatric chronic rhinosinusitis with nasal polyps requiring revision surgery. Rhinology. 2023;61:246–254.
10. Maspero JF, Katelaris CH, Busse WW, et al. Dupilumab efficacy in uncontrolled, moderate-to-severe asthma with self-reported chronic rhinosinusitis. J Aller Clin Immunol Pract. 2020;8:527–539.e529. doi:10.1016/j.jaip.2019.07.016
11. Jo S, Lee SH, Jo HR, et al. Eosinophil-derived TGFβ1 controls the new bone formation in chronic rhinosinusitis with nasal polyps. Rhinology. 2023;61:338–347. doi:10.4193/Rhin22.439
12. Lou H, Zhang N, Bachert C, et al. Highlights of eosinophilic chronic rhinosinusitis with nasal polyps in definition, prognosis, and advancement. Int Forum Allergy Rhinol. 2018;8:1218–1225. doi:10.1002/alr.22214
13. Dayon L, Cominetti O, Affolter M. Proteomics of human biological fluids for biomarker discoveries: technical advances and recent applications. Expert Rev Proteomics. 2022;19:131–151. doi:10.1080/14789450.2022.2070477
14. Utkarsh K, Kumar A, Khan A, et al. Circulating and non-circulating proteins and nucleic acids as biomarkers and therapeutic molecules in ovarian cancer. Genes Dis. 2023;10:1005–1018. doi:10.1016/j.gendis.2022.07.004
15. Zhao Y, Xue Q, Wang M, et al. Evolution of mass spectrometry instruments and techniques for blood proteomics. J Proteome Res. 2023;22:1009–1023. doi:10.1021/acs.jproteome.3c00102
16. Deutsch EW, Omenn GS, Sun Z, et al. Advances and utility of the human plasma proteome. J Proteome Res. 2021;20:5241–5263. doi:10.1021/acs.jproteome.1c00657
17. Tremlett H, Dai DL, Hollander Z, et al. Serum proteomics in multiple sclerosis disease progression. J Proteomics. 2015;118:2–11. doi:10.1016/j.jprot.2015.02.018
18. Astradsson T, Sellberg F, Ehrsson YT, et al. Serum proteomics in patients with head and neck cancer: peripheral blood immune response to treatment. Int J Mol Sci. 2022;23:6304. doi:10.3390/ijms23116304
19. Brunner PM, Suarez-Farinas M, He H, et al. The atopic dermatitis blood signature is characterized by increases in inflammatory and cardiovascular risk proteins. Sci Rep. 2017;7:8707. doi:10.1038/s41598-017-09207-z
20. Hu C, Dai Z, Xu J, et al. Proteome Profiling Identifies Serum Biomarkers in Rheumatoid Arthritis. Front Immunol. 2022;13:865425. doi:10.3389/fimmu.2022.865425
21. Mayo S, Benito-Leon J, Pena-Bautista C, et al. Recent evidence in epigenomics and proteomics biomarkers for early and minimally invasive diagnosis of alzheimer’s and parkinson’s diseases. Curr Neuropharmacol. 2021;19:1273–1303. doi:10.2174/1570159X19666201223154009
22. Zhou G, Wei P, Lan J, et al. TMT-based quantitative proteomics analysis and potential serum protein biomarkers for systemic lupus erythematosus. Clin Chim Acta. 2022;534:43–49. doi:10.1016/j.cca.2022.06.031
23. Geyer PE, Voytik E, Treit PV, et al. Plasma proteome profiling to detect and avoid sample-related biases in biomarker studies. EMBO Mol Med. 2019;11:e10427.
24. Zainal NHM, Abas R, Mohamad Asri SF. Childhood allergy disease, early diagnosis, and the potential of salivary protein biomarkers. Mediators Inflamm. 2021;2021:9198249. doi:10.1155/2021/9198249
25. Dyball S, Rodziewicz M, Mendoza-Pinto C, et al. Predicting progression from undifferentiated connective tissue disease to definite connective tissue disease: a systematic review and meta-analysis. Autoimmun Rev. 2022;21:103184. doi:10.1016/j.autrev.2022.103184
26. Kao SS, Bassiouni A, Ramezanpour M, et al. Scoping review of chronic rhinosinusitis proteomics. Rhinology. 2020;58:418–429. doi:10.4193/Rhin20.034
27. Fokkens WJ, Lund VJ, Mullol J, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology. 2012;50:1–12. doi:10.4193/Rhino12.000
28. Greguric T, Prokopakis E, Vlastos I, et al. Imaging in chronic rhinosinusitis: a systematic review of MRI and CT diagnostic accuracy and reliability in severity staging. J Neuroradiol. 2021;48:277–281. doi:10.1016/j.neurad.2021.01.010
29. Yu J, Hu C, Dai Z, et al. Dipeptidyl peptidase 4 as a potential serum biomarker for disease activity and treatment response in rheumatoid arthritis. Int Immunopharmacol. 2023;119:110203. doi:10.1016/j.intimp.2023.110203
30. Chen CL, Yao Y, Pan L, et al. Common fibrin deposition and tissue plasminogen activator downregulation in nasal polyps with distinct inflammatory endotypes. J Allergy Clin Immunol. 2020;146:677–681. doi:10.1016/j.jaci.2020.02.010
31. Wang T, Chen Y, Gao R, et al. Overexpression of AXL on macrophages associates with disease severity and recurrence in chronic rhinosinusitis with nasal polyps. Int Immunopharmacol. 2023;121:110449. doi:10.1016/j.intimp.2023.110449
32. Wang C, Zhang L. Determining a cut-off value for eosinophilic chronic rhinosinusitis. Rhinology. 2022;60:318–319. doi:10.4193/Rhin22.090
33. Tsai PC, Lee TJ, Chang PH, et al. Role of serum eosinophil cationic protein in distinct endotypes of chronic rhinosinusitis. Rhinology. 2023;2023:1.
34. Zhang H, Xie S, Fan R, et al. Elevated ALCAM expression associated with endotypes and postoperative recurrence in chronic rhinosinusitis with nasal polyps. J Inflamm Res. 2022;15:1063–1077. doi:10.2147/JIR.S350609
35. Zhu KZ, He C, Li Z, et al. Development and multicenter validation of a novel radiomics-based model for identifying eosinophilic chronic rhinosinusitis with nasal polyps. Rhinology. 2023;61:132–143. doi:10.4193/Rhin22.361
36. Xie S, Zhang H, Liu Y, et al. The role of serum metabolomics in distinguishing chronic rhinosinusitis with nasal polyp phenotypes. Front Mol Biosci. 2020;7:593976. doi:10.3389/fmolb.2020.593976
37. Liang Y, Xie R, Xiong X, et al. Alterations of nasal microbiome in eosinophilic chronic rhinosinusitis. J Allergy Clin Immunol. 2023;151:1286–1295.e1282. doi:10.1016/j.jaci.2022.11.031
38. Wang J, Yang Y, Guo J, et al. The tissue lymphocyte-to-eosinophil ratio predicted long-term recurrence of eosinophilic CRSwNP. Am J Rhinol Allergy. 2023;37:563–570. doi:10.1177/19458924231179615
39. Pappa E, Vougas K, Zoidakis J, et al. Proteomic advances in salivary diagnostics. Bioch Bioph Acta Prote Prot. 2020;1868:140494. doi:10.1016/j.bbapap.2020.140494
40. Kessel C, Lavric M, Weinhage T, et al. Serum biomarkers confirming stable remission in inflammatory bowel disease. Sci Rep. 2021;11:6690. doi:10.1038/s41598-021-86251-w
41. Bakker DS, Nierkens S, Knol EF, et al. Confirmation of multiple endotypes in atopic dermatitis based on serum biomarkers. J Allergy Clin Immunol. 2021;147:189–198. doi:10.1016/j.jaci.2020.04.062
42. Diorio C, Shraim R, Myers R, et al. Comprehensive serum proteome profiling of cytokine release syndrome and immune effector cell-associated neurotoxicity syndrome patients with B-Cell ALL receiving CAR T19. Clin Cancer Res. 2022;28:3804–3813. doi:10.1158/1078-0432.CCR-22-0822
43. Ribeiro Vitorino T, Ferraz Do Prado A, Bruno de Assis Cau S, et al. MMP-2 and its implications on cardiac function and structure: interplay with inflammation in hypertension. Biochem Pharmacol. 2023;215:115684. doi:10.1016/j.bcp.2023.115684
44. Wang X, Sima Y, Zhao Y, et al. Endotypes of chronic rhinosinusitis based on inflammatory and remodeling factors. J Allergy Clin Immunol. 2023;151:458–468. doi:10.1016/j.jaci.2022.10.010
45. Kessenbrock K, Plaks V, Werb Z. Matrix metalloproteinases: regulators of the tumor microenvironment. Cell. 2010;141:52–67. doi:10.1016/j.cell.2010.03.015
46. Jia R, Li T, Wang N. Long noncoding RNA HOTAIR functions as ceRNA to regulate MMP2 in paraquat induced lung epithelial-mesenchymal transition. Toxicology. 2021;461:152891. doi:10.1016/j.tox.2021.152891
47. Corry DB, Kiss A, Song LZ, et al. Overlapping and independent contributions of MMP2 and MMP9 to lung allergic inflammatory cell egression through decreased CC chemokines. FASEB J. 2004;18:995–997. doi:10.1096/fj.03-1412fje
48. Kuwabara Y, Kobayashi T, D’Alessandro-Gabazza CN, et al. Role of matrix metalloproteinase-2 in eosinophil-mediated airway remodeling. Front Immunol. 2018;9:2163. doi:10.3389/fimmu.2018.02163
49. Janulaityte I, Januskevicius A, Rimkunas A, et al. Asthmatic eosinophils alter the gene expression of extracellular matrix proteins in airway smooth muscle cells and pulmonary fibroblasts. Int J Mol Sci. 2022;23:4086. doi:10.3390/ijms23084086
50. Mori S, Pawankar R, Ozu C, et al. Expression and Roles of MMP-2, MMP-9, MMP-13, TIMP-1, and TIMP-2 in allergic nasal mucosa. Allergy Asthma Immunol Res. 2012;4:231–239. doi:10.4168/aair.2012.4.4.231
51. Rimkunas A, Januskevicius A, Vasyle E, et al. Blood inflammatory-like and lung resident-like eosinophils affect migration of airway smooth muscle cells and their ECM-related proliferation in asthma. Int J Mol Sci. 2023;25:24. doi:10.3390/ijms25010024
52. Pan X, Zhang Y, Wang C, et al. Evaluation of nasal symptoms to distinguish eosinophilic from noneosinophilic nasal polyps based on peripheral blood. Allergy Asthma Proc. 2021;42:214–221. doi:10.2500/aap.2021.42.210004
53. Wang C, Zhou ML, Liu YC, et al. The roles of autophagy, mitophagy, and the Akt/mTOR pathway in the pathogenesis of chronic rhinosinusitis with nasal polyps. J Immunol Res. 2022;2022:2273121. doi:10.1155/2022/2273121
54. Zhu Z, Wang W, Zhang X, et al. Nasal fluid cytology and cytokine profiles of eosinophilic and non-eosinophilic chronic rhinosinusitis with nasal polyps. Rhinology. 2020;58:314–322. doi:10.4193/Rhin19.275
55. Shi LL, Ma J, Deng YK, et al. Cold-inducible RNA-binding protein contributes to tissue remodeling in chronic rhinosinusitis with nasal polyps. Allergy. 2021;76:497–509. doi:10.1111/all.14287
56. Abdelaziz MH, Abdelwahab SF, Wan J, et al. Alternatively activated macrophages; a double-edged sword in allergic asthma. J Transl Med. 2020;18:18. doi:10.1186/s12967-019-02169-y
57. Sokulsky LA, Goggins B, Sherwin S, et al. GSTO1-1 is an upstream suppressor of M2 macrophage skewing and HIF-1α-induced eosinophilic airway inflammation. Clin Exp Allergy. 2020;50:609–624. doi:10.1111/cea.13582
58. Lee SH, Chaves MM, Kamenyeva O, et al. M2-like, dermal macrophages are maintained via IL-4/CCL24-mediated cooperative interaction with eosinophils in cutaneous leishmaniasis. Sci Immunol. 2020;2020:5.
59. Peterson S, Poposki JA, Nagarkar DR, et al. Increased expression of CC chemokine ligand 18 in patients with chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol. 2012;129:119–127. doi:10.1016/j.jaci.2011.08.021
60. Yao Y, Wang ZC, Liu JX, et al. Increased expression of TIPE2 in alternatively activated macrophages is associated with eosinophilic inflammation and disease severity in chronic rhinosinusitis with nasal polyps. Int Forum Allergy Rh. 2017;7:963–972. doi:10.1002/alr.21984
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Integrated Analysis of Inflammatory Endotypes and Clinical Characteristics in Chronic Rhinosinusitis with Nasal Polyps
Hao D, Wu Y, Li P, Li C, Jiang T, Zhang Q, Liu S, Shi L
Journal of Inflammation Research 2022, 15:5557-5565
Published Date: 24 September 2022