Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Serum GDF-15 Levels in Pediatric ADHD: Associations with Symptom Severity and Stimulant Exposure
Authors Özkan S ![]() , Can F, Höbel A
, Can F, Höbel A
Received 20 May 2026
Accepted for publication 3 July 2026
Published 14 July 2026 Volume 2026:22 622224
DOI https://doi.org/10.2147/NDT.S622224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Selçuk Özkan,1 Fatmagül Can,2 Asiye Höbel2
1Department of Child and Adolescent Psychiatry, Faculty of Medicine, Kütahya Health Sciences University, Kütahya, Türkiye; 2Department of Biochemistry, Kütahya Health Sciences University, Kütahya, Türkiye
Correspondence: Selçuk Özkan, Department of Child and Adolescent Psychiatry, Faculty of Medicine, Kütahya Health Sciences University, Kütahya, Türkiye, Email [email protected]
Background: Growth differentiation factor-15 (GDF-15) is a stress-responsive cytokine involved in inflammatory signaling and metabolic regulation. Although inflammation has been implicated in attention-deficit/hyperactivity disorder (ADHD), the role of GDF-15 in pediatric ADHD has not been previously investigated.
Methods: This cross-sectional study included 72 children with ADHD. Participants were grouped as stimulant-treated (≥ 12 months, n=32) and treatment-naïve (n=40). Clinical symptoms were assessed using the Conners’ Parent Rating Scale and the Child Behavior Checklist (CBCL/6 − 18). Serum GDF-15 levels were measured using ELISA. Group comparisons and age-adjusted regression analyses were performed.
Results: Stimulant-treated participants were older and exhibited lower symptom severity across Conners and CBCL domains. Serum GDF-15 levels did not differ between groups and were not associated with medication status after age adjustment. Additionally, no significant correlations were observed between GDF-15 levels and clinical symptom measures.
Conclusion: Serum GDF-15 levels were not associated with symptom severity or stimulant exposure in children with ADHD. Although no significant associations were identified in this sample, further adequately powered longitudinal studies are needed to clarify the potential role of GDF-15 and inflammatory pathways in pediatric ADHD.
Keywords: attention-deficit/hyperactivity disorder, GDF-15, inflammation, methylphenidate
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is one of the most common neurodevelopmental disorders of childhood and adolescence and is characterized by significant difficulties in attention, impulsivity, and hyperactivity.1 The clinical presentation of ADHD is heterogeneous, and its etiology involves a complex interplay of genetic vulnerability, environmental risk factors, and multiple neurobiological mechanisms. Increasing evidence suggests that ADHD is not limited to alterations in neurotransmitter systems but may also be associated with neuroendocrine and systemic biological processes.2,3 In particular, meta-analytic studies focusing on the hypothalamic pituitary adrenal (HPA) axis and inflammatory markers have shown that certain neuroendocrine and inflammatory parameters may differ in children and adolescents with ADHD compared with healthy controls.3,4 Similarly, several studies have reported associations between inflammatory markers and ADHD symptom domains as well as symptom severity.3
Growth differentiation factor-15 (GDF-15) is a stress-responsive cytokine that increases in conditions of metabolic stress, inflammation, and cellular burden, and has recently emerged as an important biomarker associated with systemic stress responses and energy regulation.5,6 GDF-15 has been shown to exert appetite-suppressing effects through GFRAL receptors located in the brainstem and to play a role in the regulation of energy intake.5,7 Therefore, GDF-15 is thought to function as an integrated stress signal linking peripheral metabolic processes with the central nervous system and may play a role in the interaction between energy metabolism and behavioral processes.8 Evidence also suggests that biological signals involved in energy metabolism and appetite regulation may influence brain regions associated with attention and executive functions through dopaminergic systems.9 Although GDF-15 is not a direct marker of dopaminergic dysfunction, its role as a stress- and metabolism-responsive cytokine suggests that it may indirectly reflect biological processes relevant to ADHD. In this context, the fact that methylphenidate one of the most commonly used pharmacological treatments for ADHD is frequently associated with decreased appetite and weight loss suggests that biological mechanisms related to energy balance may be involved not only in the pathophysiology of the disorder but also in treatment-related physiological changes.10,11 Nevertheless, data regarding the long-term biological effects of methylphenidate remain limited and some long-term follow-up studies have reported that treatment does not lead to clinically significant changes in basic hematological or biochemical parameters.12,13
Emerging evidence indicates that the biological effects of GDF-15 are not limited to metabolic processes but may also involve the central nervous system. The presence of GDF-15 receptor subunits in brain regions associated with cognitive functions, such as the hippocampus and prefrontal cortex, suggests a potential link between this molecule and neurocognitive processes.8,14 Psychiatric studies have also shown that GDF-15 levels may vary in schizophrenia and other psychiatric disorders and may be associated with illness severity.15,16 In addition, several studies have reported associations between GDF-15 levels and cognitive performance as well as neuroprogressive processes.17,18 Experimental animal studies further suggest that modulation of GDF-15 levels may influence neuroinflammatory responses and behavioral symptoms.19 Moreover, the GDF-15 signaling pathway has been identified as a strong regulator of energy balance and appetite control and may therefore represent a pharmacologically targetable system.20,21
Despite these findings, studies examining GDF-15 in the field of child and adolescent psychiatry are extremely limited, and the role of this biomarker has not yet been investigated in ADHD samples. Considering the potential links of GDF-15 with energy metabolism, inflammation, and neurobiological processes, examining the possible role of this molecule in the pathophysiology of ADHD appears to be important.
The aim of the present study was to investigate serum GDF-15 levels in school-aged children and adolescents diagnosed with ADHD, to compare individuals receiving regular stimulant treatment with treatment-naïve patients, and to evaluate the relationship between GDF-15 levels and symptom severity. In this regard, our study aims to contribute to the limited literature examining GDF-15 in pediatric ADHD samples and to provide a new perspective for biologic marker research focusing on inflammation-related mechanisms. We hypothesized that serum GDF-15 levels would differ according to stimulant treatment status and would be associated with ADHD symptom severity.
Methods
This cross-sectional, comparative, observational study was conducted at the Child and Adolescent Psychiatry Outpatient Clinic of a tertiary university hospital between April 2025 and December 2025. The study aimed to examine the association between serum growth differentiation factor-15 (GDF-15) levels and clinical symptom measures in children and adolescents with attention-deficit/hyperactivity disorder (ADHD) across different treatment statuses.
School-aged children and adolescents diagnosed with ADHD according to DSM-5 criteria were eligible for inclusion. Preschool children receiving ADHD treatment were not included. Participants were allocated into two groups: 1. Medicated group: participants receiving regular stimulant treatment (methylphenidate derivatives) for at least 12 months (n = 32). 2. Non-medicated group: newly diagnosed participants who had not yet initiated pharmacological treatment (n = 40). The total sample comprised 72 participants.
Inclusion criteria were DSM-5 diagnosis of ADHD, school-age status and for the medicated group, regular stimulant treatment for at least 12 months. Exclusion criteria were acute infection or systemic illness within the previous month, any chronic medical condition and use of any systemic medication other than stimulant treatment within the previous month. Learning disorders and other psychiatric comorbidities were not considered exclusion criteria.
All participants underwent standardized parent-report assessments: Child Behavior Checklist (CBCL/6-18)/Conners’ Parental Rating Scale-Short Form, Sociodemographic Form.22 In addition, the medicated group completed the Barkley Stimulant Side Effect Rating Scale.
Venous blood samples were collected in the morning after an 8 −10 hour overnight fast. Samples were drawn into gel-containing, additive-free serum separator tubes. After clot formation, samples were centrifuged at 1500 x g (3500 rpm) for 10 minutes to separate serum. Serum aliquots were transferred into Eppendorf tubes and stored at −80°C until analysis. Serum GDF-15 concentrations were measured using a commercially available sandwich enzyme-linked immunosorbent assay (ELISA) kit (Human GDF-15 ELISA Kit, Cat. No. E0037Hu; BT Laboratory, Shanghai, China) according to the manufacturer’s instructions. The assay had a measurement range of 10–3000 ng/L and a sensitivity of 5.57 ng/L. According to the manufacturer, the intra-assay coefficient of variation (CV) was <5% and the inter-assay CV was <10%. Absorbance was measured at 450 nm, and all analyses were performed in the same laboratory using standardized procedures. Sample concentrations were calculated from the standard calibration curve and expressed as ng/L.
All analyses were two-tailed, and p < 0.05 was considered statistically significant. Distributional properties of continuous variables were evaluated using histograms, Q-Q plots, and the Shapiro–Wilk test. When normality assumptions were not met, non-parametric methods were preferred; to demonstrate robustness, parametric and non-parametric results were reported together where appropriate. Between-group comparisons for continuous variables were performed using Welch’s independent samples t-test; when normality was not satisfied, Mann–Whitney U-tests were used as confirmatory analyses. Categorical variables were compared using the chi-square test. Welch’s t-test was preferred because it provides more robust estimates when variances between groups may be unequal. Non-parametric analyses were additionally performed when distributional assumptions were violated to ensure the robustness of the findings.
Because serum GDF-15 values showed a right-skewed distribution, analyses were conducted using both raw values and natural log-transformed values. Group comparisons and multivariable linear regression models were performed using log-transformed GDF-15. Associations between GDF-15 and clinical scale scores were examined using Spearman’s rank correlation coefficients. Multiple comparisons were controlled using the Benjamini-Hochberg false discovery rate (FDR) procedure. To evaluate the independent effect of medication status on clinical scale scores while accounting for the potential confounding effect of age, multivariable linear regression analyses were conducted. In each model, the dependent variable was the relevant scale score, and the independent variables were medication status (0 = non-medicated, 1 = medicated) and age (months). Regression results were reported as β coefficients with standard errors, 95% confidence intervals, and model explained variance (R2).
Results
The study included 72 participants, of whom 32 were receiving stimulant treatment and 40 were treatment-naive. The medicated group was significantly older than the non-medicated group (122.9 ± 27.3 vs 101.2 ± 25.9 months; Welch’s t = 3.43, p = 0.001, Cohen’s d = 0.82), indicating a large effect size. Sex distribution did not differ between groups (84.4% vs 85.0% male; χ2 = 0.00, p = 1.00) (Table 1).
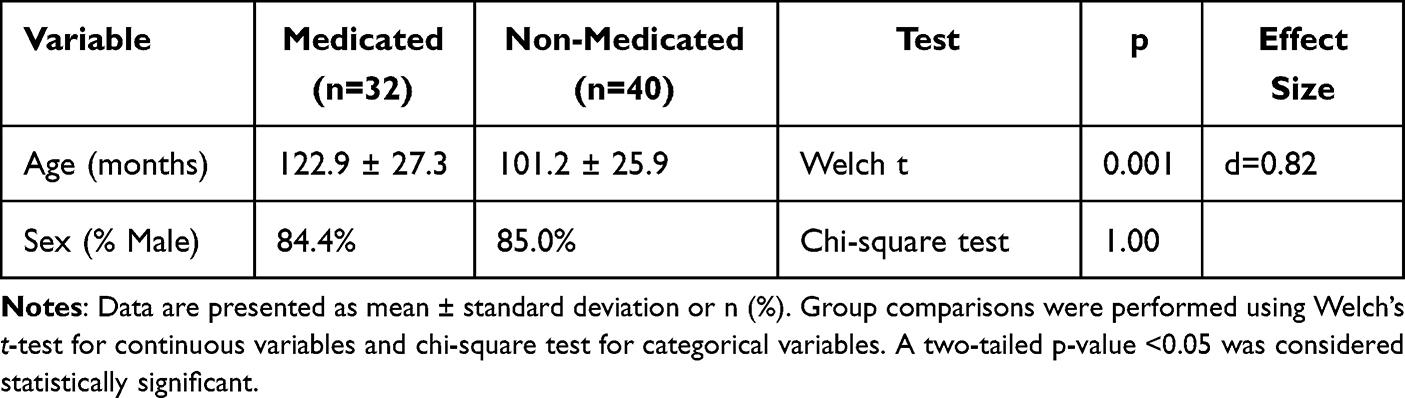 |
Table 1 Sociodemographic Characteristics of the Study Sample According to Treatment Status |
Among the medicated participants (n = 32), all were receiving long-acting methylphenidate formulations (Concerta or extended-release Medikinet) and had been on regular treatment for at least 12 months. The mean daily methylphenidate dose was 26.97 ± 8.79 mg (range 10–54 mg). Correlation analyses showed no significant association between methylphenidate dose and serum GDF-15 levels (Pearson r = −0.004, p = 0.983; Spearman r = 0.055, p = 0.766).
Conners Scale Comparisons
Children receiving stimulant treatment demonstrated significantly lower symptom severity across all Conners domains.
The ADHD Index was significantly lower in the medicated group (14.63 ± 5.16) compared to the non-medicated group (20.20 ± 5.36; t = −4.48, p < 0.001, d = −1.06).
Similarly, oppositional symptoms (t = −2.92, p = 0.005, d = −0.68), cognitive problems (t = −4.64, p < 0.001, d = −1.10), and hyperactivity (t = −5.69, p < 0.001, d = −1.32) were all significantly reduced in the medicated group (Table 2).
 |
Table 2 Comparison of Conners and CBCL Scale Scores According to Treatment Status |
Age-adjusted linear regression analyses confirmed that medication status independently predicted lower ADHD Index (β = −5.52, p < 0.001), oppositional symptoms (β = −1.93, p = 0.020), cognitive problems (β = −3.19, p < 0.001), and hyperactivity (β = −2.61, p < 0.001). Age was independently associated only with hyperactivity (β = −0.022, p = 0.039).
CBCL Comparisons
In the CBCL 6–18 scales, no significant differences were observed in internalizing domains, including withdrawn behavior, somatic complaints, anxious/depressed symptoms, and total internalizing scores (all p > 0.10).
However, significant reductions were observed in the medicated group for aggressive behavior (t = −2.63, p = 0.011, d = −0.64), externalizing problems (t = −2.75, p = 0.008, d = −0.65), and attention problems (t = −2.81, p = 0.006, d = −0.67).
Age-adjusted regression analyses confirmed that medication independently predicted lower aggressive behavior (β = −3.40, p = 0.015), externalizing problems (β = −5.19, p = 0.012), and attention problems (β = −2.47, p = 0.005). No significant associations were observed in internalizing domains.
Serum GDF-15 Levels
Raw serum GDF-15 values demonstrated a right-skewed distribution in both groups (Shapiro–Wilk p < 0.01). Therefore, both raw and log-transformed values were analyzed.
Mean GDF-15 levels were 269.99 ± 161.75 ng/L in the medicated group and 282.32 ± 135.54 ng/L in the non-medicated group. Median values were 231.70 (213.85–302.94) and 254.32 (210.91–327.92), respectively.
No significant difference was observed between groups using Welch’s t-test (p = 0.731) or Mann–Whitney U-test (p = 0.533). Log-transformed GDF-15 values also did not differ between groups (5.41 ± 0.72 vs 5.51 ± 0.59; p = 0.530) (Table 3).
 |
Table 3 Comparison of GDF-15 Levels According to Treatment Status |
Age-adjusted linear regression analysis showed that medication status was not associated with log-GDF-15 levels (β = −0.137, p = 0.417). Age was also not a significant predictor (p = 0.561). The overall model explained only 1.1% of the variance (R2 = 0.011).
Correlation Analyses
Across the entire sample (n = 72), log-GDF-15 levels were not significantly correlated with any CBCL subscale (all |ρ| < 0.12, all p > 0.30). False discovery rate correction did not alter these findings.
Within the medicated subgroup (n = 32), log-GDF-15 was not associated with any CBCL subscale (all p > 0.30) or with individual items of the Barkley side-effect scale after FDR correction (all q > 0.05).
Sex-Based Analyses
Serum GDF-15 levels did not differ between males and females in the total sample (log-GDF-15 p = 0.479). Similarly, no sex-specific differences were observed within treatment groups (all p > 0.50).
Additional Laboratory Parameters
Comparisons of additional laboratory parameters revealed no significant differences between groups after FDR correction (all q > 0.05) (Supplementary Table 1). GDF-15 remained non-significant in this multivariate laboratory context.
Discussion
In this study, we provide the first evidence examining serum GDF-15 levels in children and adolescents with ADHD in relation to symptom severity and stimulant treatment status. Our findings indicate that, although stimulant treatment was associated with expected reductions in behavioral symptom scores, GDF-15 levels did not vary according to treatment status or clinical symptom severity. Our findings highlight two main points. First, as expected, the stimulant-treated group showed significant reductions in all Conners domains and in several externalizing/attention domains of the CBCL.23 Second, GDF-15 levels were not associated with treatment status or symptom severity and did not differ significantly according to age or sex. In addition, no clinically meaningful differences were observed between groups in other laboratory parameters.
The finding that the treated group showed lower symptom severity across all subscales of the Conners scale, and that treatment status remained an independent predictor in age-adjusted models, is clinically expected and consistent with previous literature.23 Similarly, the absence of significant differences in the internalizing domains of the CBCL, alongside lower scores in aggression, externalizing behavior, and attention problems in favor of the treatment group, suggests that stimulant treatment may exert more pronounced effects on outward behavioral patterns and attention-related domains. Although behavioral changes and side effects associated with methylphenidate have been described in the literature, data regarding their frequency and long-term course remain limited, and many studies emphasize that adverse effects have not been systematically assessed using standardized scales.10,13,23 Therefore, monitoring long-term treatment effects not only through symptom scores but also through broader behavioral and biological outcomes remains important.
The primary aim of this study was to explore whether GDF-15, a molecule associated with cellular stress and inflammatory signaling, could serve as a biomarker reflecting clinical features of ADHD. Although we hypothesized that serum GDF-15 levels might vary according to symptom severity, no significant associations were observed in the present study. Therefore, our findings did not support this hypothesis. In recent years, appetite-regulating hormones have been suggested to be related not only to metabolic processes but also to neuropsychological performance, and methylphenidate use has been reported to alter certain hormonal profiles.16 Within this framework, the positioning of GDF-15 as a hormone/signal molecule that conveys energy balance and stress signaling to the brain theoretically raises the expectation that it could show changes parallel to symptom dynamics in ADHD.5,7 However, our findings did not demonstrate an association between serum GDF-15 levels and treatment status or scale-based symptom severity.
This finding does not exclude the involvement of inflammatory mechanisms in ADHD; rather, it suggests that peripheral inflammatory signals may not show simple or linear relationships with symptom domains. Indeed, systematic reviews and meta-analyses examining cortisol dynamics and various inflammatory markers in ADHD report heterogeneous results, even when certain parameters differ between patients and controls.3,4 Similarly, meta-analytic evaluations of peripheral inflammatory markers emphasize that sample characteristics, comorbidities, and methodological differences may substantially influence findings, and that single markers are unlikely to serve as specific stand-alone diagnostic biomarkers but should instead be interpreted as indicators reflecting biological heterogeneity.4 The absence of an association between GDF-15 and symptom domains in our sample is consistent with this broader framework.
The biological characteristics of GDF-15 position it not merely as a metabolic marker but as a more integrative stress signal. GDF-15 has been proposed to act as a “somatic distress” signal that conveys peripheral stress responses to the central nervous system, particularly through the GFRAL receptor in the brainstem, where it suppresses energy intake.5,8 Experimental findings examining the relationship between GDF-15 and stress-related behavioral responses also suggest that this axis may be context-dependent and multi-layered. For example, studies showing that GDF-15 increases mediated through adrenergic activation and lipolysis can modulate anxiety-like behaviors position GDF-15 as a mediator linking metabolic responses and behavioral processes.24 In neuropsychiatric populations, several studies have reported associations between GDF-15 levels, illness burden, and cognitive performance.15–18,25 Taken together, these findings suggest that GDF-15 may reflect broader biological processes related to systemic stress and metabolic regulation rather than momentary clinical symptom severity. However, given the cross-sectional design and single-time-point measurement of the present study, no conclusions can be drawn regarding whether GDF-15 represents a state- or trait-related biomarker in ADHD.
On the other hand, it has been suggested that in pediatric populations GDF-15 levels may vary substantially in relation to age, growth, and metabolic processes, and that developmental factors should therefore be considered when interpreting such biomarkers.26 For this reason, capturing a direct relationship between clinical state and biomarker levels through single time-point measurements may be more challenging in children and adolescents compared with adult populations. Moreover, in some neurodevelopmental disorders, elevated GDF-15 levels have been reported alongside heterogeneous relationships with clinical severity, supporting the possibility that GDF-15 may relate to phenotypic indicators in a non-linear manner.27 Similarly, experimental findings suggesting that GDF-15 may not exert a direct determining influence on dopaminergic system integrity raise the possibility that its role in certain neurobiological pathways may be context-specific.28
Increasing attention has been given to the interaction between peripheral inflammatory mediators and central nervous system processes in neurodevelopmental disorders, including potential effects mediated through the blood–brain barrier, microglial activation, and neuroinflammatory pathways.29 Within this broader framework, inflammation in ADHD may be more prominent in certain subgroups or biological subtypes, suggesting that a “single marker–single clinical measure” approach may be insufficient to capture the underlying heterogeneity. Although some studies have reported significant associations between inflammatory markers and symptom domains, the literature also emphasizes that findings are not always consistent.3,4,30 Our findings align with this perspective, suggesting that GDF-15 does not emerge as a universal peripheral biomarker reflecting ADHD symptom severity.
The absence of significant differences between groups not only in GDF-15 but also in other laboratory parameters provides preliminary evidence that long-term stimulant treatment is not associated with measurable alterations in this stress-responsive biomarker or the general biochemical profile. This observation is consistent with findings from a two-year open-label study in which children treated with OROS methylphenidate did not show clinically meaningful changes in hematological or biochemical parameters, and no treatment discontinuations were required due to laboratory abnormalities.12 Nevertheless, these findings should be interpreted cautiously given the cross-sectional design and relatively modest sample size of the present study.
Although interest in biomarkers capable of predicting treatment response or clinical course in ADHD has increased, none of the proposed neuroimaging, electrophysiological, or peripheral biomarkers have yet demonstrated sufficient sensitivity, specificity, and reproducibility for routine clinical use.31 The negative findings of the present study are consistent with this broader picture and underscore the need for larger samples, better-defined subgroups, multi-biomarker panels, and longitudinal designs in future biomarker research.
Several limitations should be considered. First, the study has a cross-sectional design; therefore, temporal variability of GDF-15 and its relationship with symptom fluctuations could not be evaluated. Second, the treated group was older; although statistical adjustments were made for age in months, developmental and puberty-related physiological variability cannot be entirely excluded, as pubertal stage was not systematically assessed.26 Third, the absence of a healthy control group prevented comparisons of GDF-15 levels between children with ADHD and typically developing peers, limiting the interpretation of whether GDF-15 levels are altered in ADHD itself. Fourth, because comorbidities were not excluded, clinical heterogeneity may have increased; this may have attenuated potential biomarker–symptom relationships present in specific subgroups.4 Additionally, body mass index was not systematically recorded. Given the established role of GDF-15 in energy metabolism and appetite regulation, future studies should include anthropometric measures such as BMI when evaluating this biomarker.
Finally, GDF-15 was examined as a single biomarker. Future studies incorporating cortisol/HPA axis markers, hematological inflammatory indices, other metabolic appetite-related hormones, and ideally multi-omics approaches may provide more comprehensive insights.2,9,30 In addition, considering evidence that GDF-15 can be induced by acute psychosocial stress, longitudinal designs incorporating contextual variables such as stress, sleep, and physical activity may be particularly informative.32 Furthermore, GDF-15 was measured in fasting serum at a single time point. Recent studies suggest that salivary GDF-15 may provide a non-invasive measure of dynamic stress responses. Future studies comparing serum and salivary GDF-15, particularly under stress-challenge paradigms, may further clarify the biological relevance of this marker in ADHD.
Conclusion
In conclusion, although we hypothesized that serum GDF-15 levels would differ according to stimulant treatment status and be associated with ADHD symptom severity, our findings did not support this hypothesis. Stimulant treatment was associated with expected improvements in behavioral symptoms, whereas serum GDF-15 levels were not significantly associated with treatment status or symptom severity in pediatric ADHD. Although no significant associations were identified in the present sample, larger adequately powered longitudinal studies are needed to clarify the potential role of GDF-15 in pediatric ADHD. However, it may still reflect broader biological processes related to systemic stress or metabolic regulation. Further longitudinal and multi-biomarker studies are needed to clarify its potential role in ADHD.
AI Use Statement
The authors did not use artificial intelligence tools to generate the scientific content of this manuscript. However, OpenAI ChatGPT (GPT-5.5) was used for language editing and final technical checks during manuscript preparation. All interpretations, analyses, and conclusions remain the sole responsibility of the authors.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Considerations
The study protocol was approved by the Kütahya Health Sciences University Non-Interventional Clinical Research Ethics Committee (Decision No: 2025/03-23). Written informed consent was obtained from the parents or legal guardians of all participants. All procedures contributing to this work complied with the ethical standards of the relevant national and institutional committees on human experimentation and with the principles of the Declaration of Helsinki (1975, revised in 2008).
Acknowledgments
The authors thank all participants and their families for their involvement in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Danielson ML, Claussen AH, Bitsko RH, et al. ADHD prevalence among US children and adolescents in 2022: diagnosis, severity, co-occurring disorders, and treatment. J Clin Child Adolesc Psychol. 2024;53(3):343–9. doi:10.1080/15374416.2024.2335625
2. Chang JPC, Su KP, Mondelli V, Pariante CM. Cortisol and inflammatory biomarker levels in youths with attention deficit hyperactivity disorder (ADHD): evidence from a systematic review with meta-analysis. Transl Psychiatry. 2021;11(1):430. doi:10.1038/s41398-021-01550-0
3. Abdel Samei AM, Mahmoud DAM, Salem Boshra B, Abd El Moneam MHED. The interplay between blood inflammatory markers, symptom domains, and severity of ADHD disorder in children. J Atten Disord. 2024;28(1):66–76. doi:10.1177/10870547231197213
4. Misiak B, Wojta-Kempa M, Samochowiec J, et al. Peripheral blood inflammatory markers in ADHD: a systematic review and meta-analysis. Prog Neuropsychopharmacol Biol Psychiatry. 2022;118:110581. doi:10.1016/j.pnpbp.2022.110581
5. Lockhart SM, Saudek V, O’Rahilly S. GDF15: a hormone conveying somatic distress to the brain. Endocr Rev. 2020;41(4):bnaa007. doi:10.1210/endrev/bnaa007
6. Li J, Hu X, Xie Z, Li J, Huang C, Huang Y. Overview of growth differentiation factor 15 (GDF15) in metabolic diseases. Biomed Pharmacother. 2024;176:116809. doi:10.1016/j.biopha.2024.116809
7. Klein AB, Kleinert M, Richter EA, Clemmensen C. GDF15 in appetite and exercise: essential player or coincidental bystander? Endocrinology. 2022;163(1):bqab242. doi:10.1210/endocr/bqab242
8. Seo M, Pyeon SY, Kim MS. Molecular links between metabolism and mental health: integrative pathways from GDF15-mediated stress signaling to brain energy homeostasis. Int J Mol Sci. 2025;26(15):7611. doi:10.3390/ijms26157611
9. Lai KY, Li CJ, Tsai CS, et al. Appetite hormones, neuropsychological function and methylphenidate use in children with ADHD. Psychoneuroendocrinology. 2024;170:107169. doi:10.1016/j.psyneuen.2024.107169
10. Konrad-Bindl DS, Gresser U, Richartz BM. Changes in behavior as side effects in methylphenidate treatment: review of the literature. Neuropsychiatr Dis Treat. 2016;12:2635–2647. doi:10.2147/NDT.S114185
11. Chordia A, Karia S, Shah N, De Sousa A. A study of safety and efficacy of methylphenidate in children and adolescents: an observational clinical study. Indian J Private Psychiatr. 2022;16(2):56–60. doi:10.5005/jp-journals-10067-0115
12. Wigal SB, Wilens TE, Wolraich M, Lerner M. Hematologic and blood biochemistry monitoring during methylphenidate treatment in children with ADHD: 2-year open-label study results. Pediatrics. 2007;120(1):e120–e128. doi:10.1542/peds.2006-1402
13. Moran LV. Long-term safety of methylphenidate in children with ADHD. Lancet Psychiatry. 2023;10(5):306–307. doi:10.1016/S2215-0366(23)00092-5
14. Jackson TC, Gorse K, Herrmann JR, Kochanek PM. Hippocampal and prefrontal cortical brain tissue levels of irisin and GDF15 receptor subunits in children. Mol Neurobiol. 2021;58(5):2145–2157. doi:10.1007/s12035-020-02250-4
15. Kumar P, Millischer V, Villaescusa JC, et al. Plasma GDF15 level is elevated in psychosis and inversely correlated with severity. Sci Rep. 2017;7(1):7906. doi:10.1038/s41598-017-07503-2
16. Costanzi M, Goularte JF, da Silva LHT, et al. The effect of psychiatric hospitalizations and diagnosis on serum CCL11 and GDF15 levels in schizophrenia, bipolar disorder, and major depressive disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2025;141:111446. doi:10.1016/j.pnpbp.2025.111446
17. Beydoun MA, Hooten NN, Weiss J, et al. GDF15 and its association with cognitive performance over time in a longitudinal study of middle-aged urban adults. Brain Behav Immun. 2023;108:340–349. doi:10.1016/j.bbi.2022.12.015
18. Guo T, Chen L, Sun W, et al. Increased GDF-15 in chronic male patients with schizophrenia: correlation with body mass index and cognitive impairment. Schizophrenia. 2024;10(1):117. doi:10.1038/s41537-024-00541-6
19. Arda DB, Tunç KC, Bozkurt MF, Bora ES, Çiğel A, Erbaş O. Intranasal insulin eases autism in rats via GDF-15 and anti-inflammatory pathways. Curr Issues Mol Biol. 2024;46(9):10530–10544. doi:10.3390/cimb46090624
20. Benichou O, Coskun T, Gonciarz MD, et al. Discovery, development, and clinical proof of mechanism of LY3463251, a long-acting GDF15 receptor agonist. Cell Metab. 2023;35(2):274–286. doi:10.1016/j.cmet.2022.12.011
21. Wang D, Jabile MJT, Lu J, et al. Fatty acids increase GDF15 and reduce food intake through a GFRAL signaling axis. Diabetes. 2024;73(1):51–56. doi:10.2337/db23-0495
22. Peterson BS, Trampush J, Brown M, et al. Tools for the diagnosis of ADHD in children and adolescents: a systematic review. Pediatrics. 2024;153(4).
23. Storebø OJ, Storm MRO, Ribeiro JP, et al. Methylphenidate for children and adolescents with attention deficit hyperactivity disorder (ADHD). Cochrane Database Syst Rev. 2023;3(3). doi:10.1002/14651858.CD009885.pub3
24. Townsend LK, Wang D, Knuth CM, et al. GDF15 links adipose tissue lipolysis with anxiety. Nat Metab. 2025;7(5):1004–1017. doi:10.1038/s42255-025-01264-3
25. Azarsız YD, Kahve AC, Üstün ESA, et al. Serum FGF21 and GDF15 levels and their association with cognitive function in bipolar disorder. J Affect Disord. 2025;397:120979. doi:10.1016/j.jad.2025.120979
26. Kronenberger DW, Zimmers TA, Ralston RK, Runco DV. Circulating growth differentiation factor 15 (GDF15) in paediatric disease: a systematic review. J Cachexia Sarcopenia Muscle. 2025;16(2):e13712. doi:10.1002/jcsm.13712
27. Hertzog A, Tolun AA, Wykes AD, et al. Evaluating the utility of GDF15 and FGF21 as blood biomarkers for Rett syndrome. Sci Rep. 2025;15(1):36017. doi:10.1038/s41598-025-20005-w
28. Machado V, Gilsbach R, Das R, et al. Gdf-15 deficiency does not alter vulnerability of nigrostriatal dopaminergic system in MPTP-intoxicated mice. Cell Tissue Res. 2016;365(2):209–223. doi:10.1007/s00441-016-2406-x
29. Than UTT, Nguyen LT, Nguyen PH, et al. Inflammatory mediators drive neuroinflammation in autism spectrum disorder and cerebral palsy. Sci Rep. 2023;13(1):22587. doi:10.1038/s41598-023-49902-8
30. Kaşak M, Günal Okumuş H, Çelik YS, Kırşan FZ, Öztürk Y, Efe A. Novel hematologic ratios and systemic inflammation index in ADHD: effects of methylphenidate treatment. Front Psychiatry. 2025;16:1621767. doi:10.3389/fpsyt.2025.1621767
31. Michelini G, Norman LJ, Shaw P, Loo SK. Treatment biomarkers for ADHD: taking stock and moving forward. Transl Psychiatry. 2022;12(1):1–30. doi:10.1038/s41398-022-02207-2
32. Huang Q, Trumpff C, Monzel AS, et al. The mitochondrial disease biomarker GDF15 is dynamic, quantifiable in saliva, and correlates with disease severity. Mol Genet Metab. 2025;145(4):109179. doi:10.1016/j.ymgme.2025.109179
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Role and Mechanism of Growth Differentiation Factor 15 in Chronic Kidney Disease
Tang Y, Liu T, Sun S, Peng Y, Huang X, Wang S, Zhou Z
Journal of Inflammation Research 2024, 17:2861-2871
Published Date: 9 May 2024