")
Back to Journals » Infection and Drug Resistance » Volume 16
Seroprevalence and Associated Risk Factors of Brucellosis Among Human Population in Duhok City, Iraq
Authors Khalid HM
Received 18 February 2023
Accepted for publication 29 April 2023
Published 8 May 2023 Volume 2023:16 Pages 2805—2811
DOI https://doi.org/10.2147/IDR.S407263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Haval Mohammed Khalid
Department of Biology, Faculty of Science, University of Zakho, Zakho, Kurdistan Region, Iraq
Correspondence: Haval Mohammed Khalid, Tel +9647504508093, Email [email protected]
Purpose: Brucellosis is a zoonotic disease that contributes to severe global health and economic issues. In this study, the Rose Bengal Test (RBT), a crucial diagnostic tool for brucellosis in Duhok city, was evaluated in order to offer updated epidemiological data on this disease.
Patients and Methods: A total of 339 patients suffered from fever and seeking medical attention in the private medical health center in Duhok city, Iraq, were enrolled after taking ethical approval from committee at Faculty of Sciences, University of Zakho and a verbal consent from each enrolled patient for using his/her blood and data. The blood specimens were tested for Brucella spp. Antibodies using the RBT and blood cultures, followed by spp. determination. A questionnaire form was designed to detect the associated risk factors.
Results: Prevalence of brucellosis was 12.6% among participants with a probable diagnosis and 10.3% among those with a confirmed diagnosis (positive blood culture). Most of the positive cases were between the ages of 20 to 40 years. A highly significant (P < 0.0001) association was found between brucellosis with both consuming raw milk and having contact with cattle. The most common species identified were Brucella melitensis (57.1%) and Brucella abortus (42.7%).
Conclusion: Brucellosis is a significant cause of fever in the current study and can be detected using the RBT. Human brucellosis can be reduced by minimizing the chances of contact with cattle and consuming boiled or pasteurized milk.
Keywords: Brucella species, risk factors, serology, blood culture
A Letter to the Editor has been published for this article.
Introduction
Brucellosis is an infectious zoonotic disease caused by members of the genus Brucella. It is also known commonly as Mediterranean fever, undulant fever, and remitting fever.1 Moreover, annually about 500,000 cases of brucellosis are reported, or about 10/100,000 of the population.2 Human Brucellosis is caused by four spp. namely: B. suis, B. melitensis, B. abortus, and B. canis.3 Brucella species are gram-negative, lacking capsule, or endospores, intracellular coccobacilli and do not produce toxins. Brucella suis which infect pig; B. melitensis infects sheep and goats; B. abortus infects cattle and B. canis infects dogs.4
The major pathways of human infection with Brucella are through direct contact with diseased animals, breathing in airborne agents, or consuming contaminated dairy products.5 Furthermore, organ transplants, blood transfusion, or vertical transfer from mother to developing embryo all are ways for human-to-human transmission.6
Although there is a considerable variation in the manifestation ways of brucellosis, but the vast majority of people who contract the disease report experiencing flu-like symptoms after acquiring infection, including high body temperature, sweating, extreme tiredness, a persistent headache, and muscles and joint pains.7 Variable complications, including involving the heart, nervous system, bones and joints, eyes, and testicles, have been linked to more severe instances.8 Several regions around the world have a persistent problem with brucellosis; such as the Middle Eastern countries including Iraq, Saudi Arabia, Jordan and the Turkish Republic, the central Asia, Mexico, South America, the Asia-Pacific area and North-Africa, including Algeria.9–11
Variable risk factors are associated with human brucellosis due to the wide diversity of animals that serve as reservoirs and the cultural activities that expose people to the disease. In the United States, brucellosis has been connected to pig slaughter,11 in Chad, the handling of cattle umbilical cords12 and in Yemen, to drinking camel milk.13 Disease control in endemic areas relies heavily on identifying the related risk factors and implementing measures to reduce the spread of infection, such as vaccination campaigns, slaughter actions, and enhancing food care, as well as using the precise diagnostic test at the right time, since misdiagnosis and incorrect treatment ensue when tests fail to accurately detect disease.
Countries in which human brucellosis is common face significant difficulties in identifying cases and providing effective treatment. Brucellosis cannot be confirmed by symptoms alone; blood or bone marrow detection of Brucella spp. is the gold standard.14 The RBT is a diagnostic test used to detect antibodies against Brucella, the bacterium that causes brucellosis in cattle and other animals. The RBT is considered a screening tool for brucellosis and is widely used in many countries for the detection of this disease. The test has been shown to have good sensitivity and specificity, which makes it an ideal tool for large-scale surveillance programs. Additionally, the RBT is cost-effective and practical, as it can be performed in the field without the need for expensive laboratory equipments.15,16
Due to the lack of active surveillance, many countries do not have accurate data of human brucellosis. This is especially true in developing countries. Thus, the accurate extent of the disease’s impact is underestimated.17
The purpose of this study was to provide information on the current state of human brucellosis in Duhok city, Iraq and to add epidemiological data, particularly on the risk factors associated with this disease aiming to reduce its prevalence through better practices. In addition, we evaluate RBT as a diagnostic test for human brucellosis in endemic area by using blood culture data and identify the circulating species in this area.
Materials and Methods
Design of Study and Participants
In the period from January to December 2022, a cross-sectional study involving 339 participants, of both gender and different ages (20 to >60 years) were enrolled after taking a verbal consent from each patient for using his/her blood and related data (it was not possible to take a written consent from all patients, since most of the patients were illiterates, from illiterate people a verbal consent was taken, while from literate a written consent was taken. The use of verbal consent from illiterate patients was approved by the Ethics Committee. All specimens involving participants were approved by the Ethics Committee of the University of Zakho (approval no.: BSCUoz/03/01/2023). The methods were carried out in accordance with the Declaration of Helsinki.
Adults who visited this outpatient’s clinic complaining of fever in addition to one or more of the following signs: sweating, anorexia, headaches, myalgia, were enrolled in the study. While the subject which do not met any of the following criteria were excluded from the study: 1) they had another health issue, 2) they were treated for brucellosis last year or 3) they were younger than 20 years. A questionnaire was designed for data collection including socio-demographics, food habits, and contact modalities with livestock.
Collection of Samples
Brucellosis was diagnosed using blood culture and the RBT, which detect antibody in the serum. From each participant about 8 mL of venous blood was withdrawn, 6 mL was inoculated into blood culture bottle and 2 mL was transferred into a gel tube for the Rose Bengal Test.
Brucella Spp. Isolation
The BACTEC 9050 was used for blood culture (Becton Dickinson, Franklin Lakes, USA). Followed by subculturing on Brucella base blood agar. Brucella culture performed in a Biosafety Level 3 (BSL-3) laboratory. Identification was based on colony morphology, and biochemical assays like oxidase, urease, catalase, no sugar fermentation, nitrate reduction and requirement of aerobic conditions, added 5–10% CO2 and incubated at 37°C after incubating all of the bottles for up to 4 weeks when the device gave a positive indicator. The culture was confirmed negative of Brucella species at the end of four weeks when there was no positive sign of bacterial growth.
Identification of Brucella Species
All Brucella spp. isolates were categorized based on H2S production, susceptibility to thionine, and CO2 required.
Rose Bengal Test
For detecting Brucella antibodies, the method of Torax Bioscience (United Kingdom) was used by placing 0.02 mL of serum on enamel plate, then equal amount of antigen was added, mixed and spread over an area of 2 cm in diameter. After four minutes of continuous mixing at room temperature, if any agglutination was observed, the result was considered positive blood culture.
A positive RBT with clinical suspicion of brucellosis together constitute a diagnosis of suspected brucellosis, while isolation of Brucella spp. from blood is considered as a confirmed brucellosis.
Data Management and Analysis
All of the obtained data were loaded into an Excel spreadsheet, and then they were imported to SPSS version 25 for data management, which included the calculation of running frequencies for each variable. The prevalence of Brucella spp. was analyzed using a Chi-square (X2) test to see if there is a significant difference. Regarding the association between brucellosis and the studied parameters, the potential risk factor was regarded statistically significant at the P < 0.05 level.
Institutional Review Board Statement
Patient informed consent and an ethical approval was obtained from Faculty of Sciences, University of Zakho (ethical clearance, no. BSCUoz/03/01/2023) for the use of these data and samples in the study.
Results
Features of Participants
Out of the 339 participants enrolled, 43.1% were at ages of 41 to 60, 53.7% were males, and 46.3% were from urban areas. The mean age was 49 years with a range between 20 and 85 years. From the enrolled participants, 39.6% stated that they drink unpasteurized milk and 37.1% of them had contact with cattle. Table 1 summarizes participant characteristics based on the probability of brucellosis.
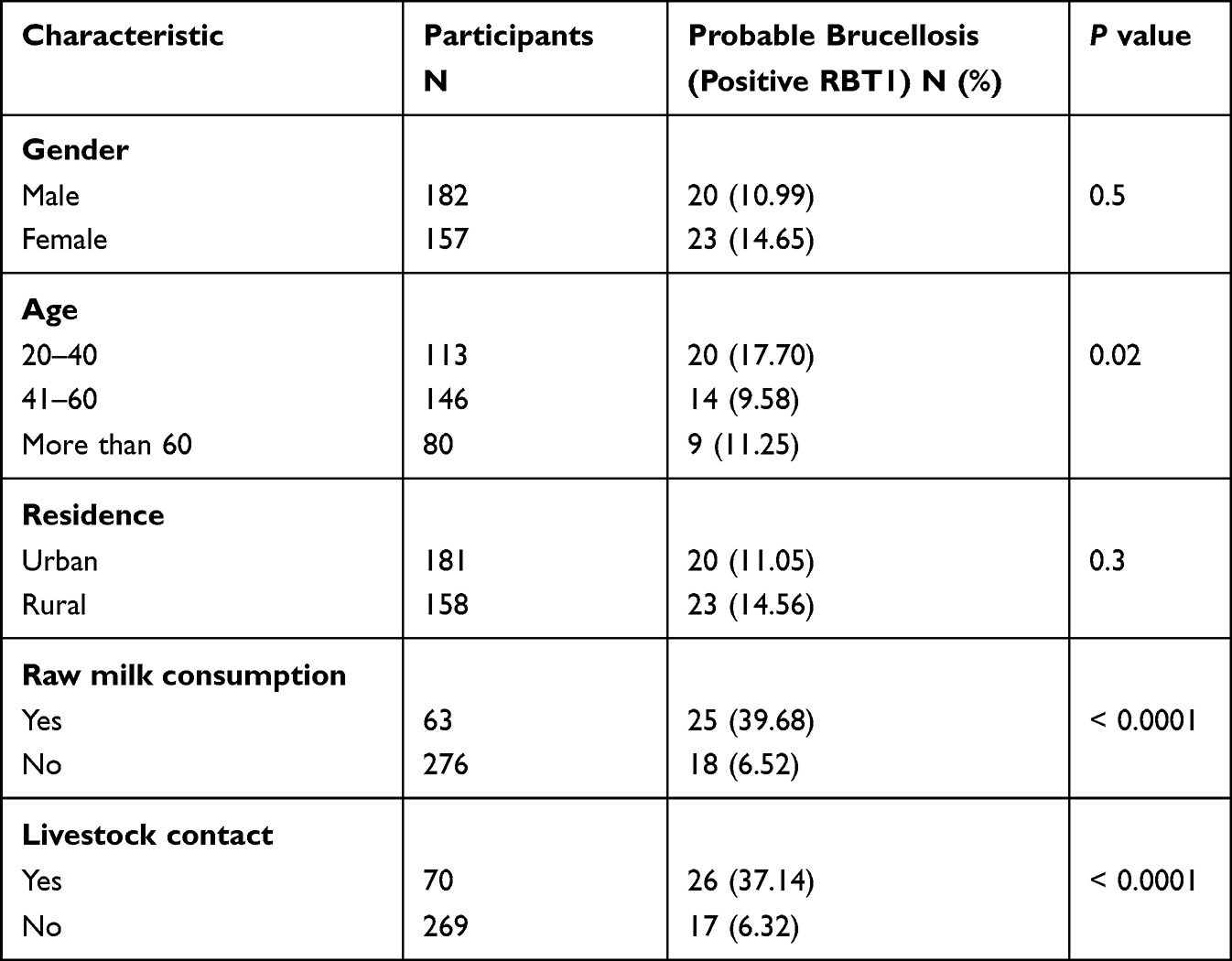 |
Table 1 The Relationships Between Probable Brucellosis and Participant Characteristics (N = 339) |
Human Brucellosis Incidence and Risk Features
Table 1 shows that 12.68% (43/339) of the participants were tested positive for Brucella spp. using the RBT, and 10.32% (35/339) had positive blood cultures for Brucella spp. All cases with positive bottle blood cultures were also positive for RBT, while only 18.6% (8/43) of positive RBT were negative for blood cultures. Regarding the studied parameters, females showed a slightly higher rate than males (14.6% vs 10 0.9%). The ages from 20 to 40 years showed the highest rate (17.6%) of infection with significant difference (P=0.02) from other ages. Moreover, the two main risk factors associated with brucellosis were the consumption of raw milk and animal contact. Both factors had a highly significant (P < 0.0001) effect in increasing the positive rate of infection.
Species of Brucella Identified
In this investigation, two species of Brucella were identified, which were B. melitensis and B. abortus, by using biochemical and agglutination assays of Brucella isolates (Table 2).
 |
Table 2 Distribution of Brucella Spp. According to Participant Characteristics |
Discussion
This study found that 12.6% of patients in Duhok City/Iraq were positive for probable brucellosis, while another study also in Duhok city, in 2017 reported a higher seroprevalence rate of 17.8%.18 On the other hand, a lower seroprevalence rate (10.7%) during 2012 was reported in Erbil city, Iraq.19 In both of these studies, the analyzed data for RBT were from RBT people suspected to have brucellosis.
Human brucellosis has been estimated in studies in various countries worldwide with variable rates, such as: 6.59% in Iran,20 12.7% in Saudi Arabia,21 8.8% in Turkey,22 6.1% in Rwanda,23 16.7% in India.24 In these studies, only patients with nonspecific symptoms were enrolled for serological brucellosis test. Due to the presence of great variations in brucellosis prevalence among livestock, as well as socioeconomic features. This emphasizes the significance of identifying the primary risk factors associated with the disease in all region in order to reduce the rate of this infection or to control it through the application of prevention measures.
In the current research, some of the risk factors that might have a great impact in the disease have been recognized such as: the drinking raw milk and livestock contact. A highly significant correlation was observed between brucellosis and drinking raw milk. This is consistent with previous research that showed an increased risk of infection with drinking raw milk, while drinking boiled milk effectively prevented it.25
Therefore, the consumption of safe milk is a crucial step in reducing the rate of brucellosis, particularly considering the importance of milk and dairy products to human health. The other factor that significantly affects the prevalence of brucellosis is the interaction with livestock. This result is consistent with a study performed in Erbil that indicated the presence of significant correlation between the epidemiology of brucellosis and contact with livestock.19 Protective measures might give benefit in knowing which livestock species act as a reservoir for a particular Brucella spp. close result in this direction were observed in Saudi Arabia26 and Iran.20
Although brucellosis can infect people of any age, young adults are at the highest risk.27 The findings of the current study confirm this fact because young adults are more likely to come into contact with animals mostly due to occupational risks.
Moreover, nonsignificant association was observed between gender and brucellosis cases in this investigation. This observation is debatable, since a study done in Saudi Arabia reported a higher prevalence of brucellosis in men who suffered more frequently from the disease than women.28 Another study in Pakistan stated that most brucellosis patients were women because women had more direct contact with livestock in addition of sharing the field work with men.29 Therefore, the style of the community life must be considered in evaluating the relationship between gender and the rate of infection with brucellosis.
In the current study, a high prevalence of brucellosis was noted among inhabitants of rural areas. This finding is consistent with studies from Iran30 and Uganda.31 That reported higher brucellosis cases in rural residents and attributed them to the living conditions since in rural areas people more likely interact with livestock.
The Brucella species has a significant impact on how human brucellosis spreads: B. melitensis spreads through drinking unpasteurized milk or related dairy products, whereas B. abortus infects people through invasion of the mucosal membrane by ingested microorganisms, or abraded skin.32
Additionally, each species has different hosts; B. melitensis is primarily hosted by sheep, goats, and buffalo, whereas B. abortus is primarily hosted by cattle.33 Since there is no vaccine for human protection, identifying the common species in a given area permits the implementation of preventative measures to break the transmission of the disease to humans.
This study demonstrated that B. melitensis was responsible for 57.1% of human brucellosis cases while B. abortus was responsible for 42.7% of the cases. This finding contradicts with the study done in Erbil city in 2012 that reported a higher prevalence of B. abortus than B. melitensis at rates of 71.71% and 28.22%, respectively.19
The differences in the prevalence of each species in a given area or country might be due to differences in the traditional livestock in that country.29 For example, out of 330 cultures performed in Yemen, 45 were positive for B. abortus and only 7 were positive for B. melitensis.34 While, in Iran, researchers isolated sixty B. melitensis and eight B. abortus cases from a total of 68 human and animal specimens.35 Also, Brucella melitensis have been described as the primary cause of brucellosis in Saudi Arabia,36 and, in Turkey, B. melitensis was found in 98.2% of the specimens.37
The gold standard method for diagnosing brucellosis is the isolation of Brucella spp. from clinical specimens.38 There are a number of reasons why this procedure cannot be performed frequently, because it is time-consuming and complicated and the patient must not receive antibiotics before the test. As a result, providing an alternate test is critical, especially in developing countries with limited laboratory facilities. On the basis of culture results, RBT demonstrated good specificity and sensitivity.
Brucellosis is diagnosed by serological and bacteriological assays. Bacteriological tests detect Brucella bacteria in body fluids or tissues, while serological testing detects antibodies produced by the body. Brucellosis serological tests include the RBT, standard tube agglutination test (STAT), complement fixation test (CFT), and enzyme-linked immunosorbent assay (ELISA). Culture and isolation of bacteria from blood or other body fluids are bacterial testing.39
We suggest that RBT could be employed to diagnose brucellosis in endemic areas where isolation of Brucella and ELISA is challenging, provided that the clinician considers the compatibility of clinical features when interpreting positive results, as indicated in recent studies.40
There were some limits to this study: the number of human brucellosis risk variables investigated was small, limiting our capacity to completely assess the reasons and apply proper preventative practices, particularly in urban regions; and all data are dependent on participants reporting. Despite its limitations, this study provided an important updated epidemiology data regarding this widespread infection and according to our knowledge, this is the first study in Duhok city to identify the Brucella species by using blood cultures.
Conclusions
Patients suffering from fever in Duhok city, Iraq are often young people, and human brucellosis was a possible cause of their illness. The most common species of Brucella that were responsible for infection were B. melitensis and B. abortus. Factors that increase a person’s likelihood of contracting brucellosis included drinking raw milk and having contact with animals. These results emphasize on the significance of vaccinating cattle and implementing health education measures among the population and emphasizing on drinking pasteurized or boiled milk and other dairy products in order to minimize the occurrence of this infection.
Acknowledgments
The author thanks the Biology Department, Faculty of Science, Zakho University, Zakho city, Duhok province, Kurdistan region/Iraq, for providing some research facilities, and for private clinical center for providing the blood samples.
Disclosure
The author declares no conflict of interest.
References
1. Głowack P, Żakowska D, Naylor K, et al. Brucella – virulence factors, pathogenesis and treatment. Pol J Microbiol. 2018;67:151–161. doi:10.21307/pjm-2018-029
2. Seleem MN, Boyle SM, Sriranganathan N. Brucellosis: a re-emerging zoonosis. Vet Microbiol. 2010;140:392–398. doi:10.1016/j.vetmic.2009.06.021
3. Xavier MN, Costa EA, Paixão TA, et al. The genus Brucella and clinical manifestations of brucellosis. Ciênc Rural. 2009;39:2252–2260. doi:10.1590/S0103-84782009005000167
4. Bukhari EE. Pediatric brucellosis. An update review for the new millennium. Saudi Med J. 2018;9:336–341. doi:10.15537/smj.2018.4.21896
5. Godfroid J, Al Dahouk S, Pappas G, et al. One Health” surveillance and control of brucellosis in developing countries: moving away from improvisation. Comp Immunol Microbiol Infect Dis. 2013;36:241–248. doi:10.1016/j.cimid.2012.09.001
6. Ay N, Kaya S, Anil M, et al. Pulmonary involvement in brucellosis, a rare complication of renal transplant: case report and brief review. Exp Clin Transplant. 2018;16:757–760. doi:10.6002/ect.2015.0324
7. Buzgan T, Karahocagil MK, Irmak H, et al. Clinical manifestations and complications in 1028 cases of brucellosis: a retrospective evaluation and review of the literature. Int J Infect Dis. 2010;14:e469–e478. doi:10.1016/j.ijid.2009.06.031
8. Herrick JA, Lederman RJ, Sullivan B, et al. Brucella arteritis: clinical manifestations, treatment, and prognosis. Lancet Infect Dis. 2014;14:520–526. doi:10.1016/S1473-3099(13)70270-6
9. Dean AS, Crump L, Greter H, et al. Global burden of human brucellosis: a systematic review of disease frequency. PLoS Negl Trop Dis. 2012;6:e1865. doi:10.1371/journal.pntd.0001865
10. Rubach MP, Halliday JE, Cleaveland S, et al. Brucellosis in low-income and middle-income countries. Curr Opin Infect Dis. 2013;26:404–412. doi:10.1097/QCO.0b013e3283638104
11. Adel M. Survey on therapeutic protocols of Human brucellosis prescribed by urban and rural physicians and persistence risk factors in the Governorate of Biskra. Algeria J Pharm Chem Biol Sci. 2018;5(4):437–448.
12. Chomel BB, Debess EE, Mangiamele DM, et al. Changing trends in the epidemiology of human brucellosis in California from 1973 To 1992: a shift toward foodborne transmission. J Infect Dis. 1994;170:1216–1223. doi:10.1093/infdis/170.5.1216
13. Schelling E, Diguimbaye C, Daoud S, et al. Brucellosis and Q-fever seroprevalences of nomadic pastoralists and their livestock in Chad. Prev Vet Med. 2003;61:279–293. doi:10.1016/j.prevetmed.2003.08.004
14. Almashhadany DA. Prevalence of brucellosis in human and camels in Thamar Province/Yemen. J Saudi Soc Agric Sci. 2014;13:132–137.
15. Di Bonaventura G, Angeletti S, Ianni A, et al. Microbiological laboratory diagnosis of human brucellosis: an overview. Pathogens. 2021:101623. doi:10.3390/pathogens10121623
16. Ruiz-Mesa JD, Sánchez-Gonzalez J, Reguera JM, et al. Rose Bengal test: diagnostic yield and use for the rapid diagnosis of human brucellosis in emergency departments in endemic areas. Clin Microbiol Infect. 2005;11:221–225. doi:10.1111/j.1469-0691.2004.01063.x
17. Mantur BG, Amarnath SK, Shinde RS. Review of clinical and laboratory features of human brucellosis. Indian J Med Microbiol. 2007;25:188–202. doi:10.4103/0255-0857.34758
18. Assafi MS, Allu MA, Abdulrahman IS, et al. The seroprevalence of human brucellosis in different age groups patients and other associated risk factors in Duhok, Iraq. Rev Innovaciencia. 2019;7:1–7. doi:10.15649/2346075X.479
19. Rasul D, Mansoor I, Hussein K. Seroprevalence of human brucellosis in Erbil city. Zanco J Med Sci. 2012;16:220–226. doi:10.15218/zjms.2012.0038
20. Keramat F, Karami M, Alikhani MY, et al. Cohort profile: famenin brucellosis cohort study. J Res Health Sci. 2019;19:e00453.
21. Alkahtani AM, Assiry MM, Chandramoorthy HC, et al. Sero-prevalence and risk factors of brucellosis among suspected febrile patients attending a referral hospital in southern Saudi Arabia (2014–2018). BMC Infect Dis. 2020;20:1–8. doi:10.1186/s12879-020-4763-z
22. Aypak C, Altunsoy A, Çelik AK. Epidemiological and clinical aspects of human brucellosis in eastern Anatolia. J Nippon Med Sch. 2012;79:343–348. doi:10.1272/jnms.79.343
23. Gafirita J, Kiiza G, Murekatete A, et al. Seroprevalence of Brucellosis among patients attending a district hospital in Rwanda. Am J Trop Med Hyg. 2017;97:831–835. doi:10.4269/ajtmh.16-0632
24. Bansal Y, Aggarwal A, Gadepalli R, et al. Seroprevalence of brucellosis in Western Rajasthan: a study from a tertiary care centre. Indian J Med Microbiol. 2019;37:426–429. doi:10.4103/ijmm.IJMM_19_358
25. Kiambi SG, Fèvre EM, Omolo J, et al. Risk factors for acute human brucellosis in Ijara, northeastern Kenya. PLoS Negl Trop Dis. 2020;14:e0008108. doi:10.1371/journal.pntd.0008108
26. Al-Sekait MA. Epidemiology of brucellosis in al Medina region, Saudi Arabia. J Family Community Med. 2000;7:47.
27. Niaz S, Raqeeb A, Khan A, et al. Status of human brucellosis in district Malakand, Khyber Pakhtunkhwa, Pakistan. J Infect Public Health. 2021;14:423–427. doi:10.1016/j.jiph.2019.12.013
28. Aloufi AD, Memish ZA, Assiri AM, et al. Trends of reported human cases of brucellosis, Kingdom of Saudi Arabia, 2004–2012. J Epidemiol Glob Health. 2016;6:11–18. doi:10.1016/j.jegh.2015.09.001
29. Malik S, Sarwar I, Rauf A, et al. Seroprevalence of brucellosis among patients presenting with non-specific symptoms at Ayub Teaching Hospital Abbottabad. J Ayub Med Coll Abbottabad. 2018;30:566–570.
30. Ebrahimpour S, Youssefi MR, Karimi N, et al. The prevalence of human Brucellosis in Mazandaran province, Iran. African J Microbiol Res. 2012;6:4090–4094. doi:10.5897/AJMR11.1076
31. Dieckhaus KD, Kyebambe PS. Human brucellosis in rural Uganda: clinical manifestations, diagnosis, and comorbidities at Kabale Regional Referral Hospital, Kabale, Uganda. Open Forum Infect Dis. 2017;4:1–6. doi:10.1093/ofid/ofx237
32. Perez A, Berhe M. Brucella, a bacterium with multiple ways of causing infection. Baylor Univ Med Cent Proc. 2020;34:99–101. doi:10.1080/08998280.2020.1805674
33. González-Espinoza G, Arce-Gorvel V, Mémet S, et al. Brucella: reservoirs and niches in animals and humans. Pathogens. 2021;10:186. doi:10.3390/pathogens10020186
34. Refai M. Incidence and control of brucellosis in the Near East region. Vet Microbiol. 2002;90:81–110. doi:10.1016/s0378-1135(02)00248-1
35. Hashemifar I, Yadegar A, Jazi FM, Amirmozafari N. Molecular prevalence of putative virulence-associated genes in Brucella melitensis and Brucella abortus isolates from human and livestock specimens in Iran. Microb Pathog. 2017;105:334–339. doi:10.1016/j.micpath.2017.03.007
36. Elfaki MG, Uz-Zaman T, Al-Hokail AA, et al. Detection of Brucella DNA in sera from patients with brucellosis by polymerase chain reaction. Diagn Microbiol Infect Dis. 2005;53:1–7. doi:10.1016/j.diagmicrobio.2005.03.011
37. Dal T, Kara SS, Cikman A. Comparison of multiplex real-time polymerase chain reaction with serological tests and culture for diagnosing human brucellosis. J Infect Public Health. 2019;12:337–342. doi:10.1016/j.jiph.2018.11.008
38. Khurana SK, Sehrawat A, Tiwari R, et al. Bovine brucellosis – a comprehensive review. Vet Q. 2021;41:61–88. doi:10.1080/01652176.2020.1868616
39. Raies Ul Islam M, Pratap GM, Kaur SP, et al. Comparative evaluation of indirect enzyme linked immunosorbent assay, Rose Bengal plate test, microagglutination test, and polymerase chain reaction for diagnosis of brucellosis in buffaloes. Turk J Vet Anim Sci. 2013;37:306–310. doi:10.3906/vet-1201-39
40. Ekiri AB, Kilonzo C, Bird BH, et al. Utility of the Rose Bengal Test as a point-of-care test for human brucellosis in endemic African settings: a systematic review. J Trop Med. 2020:6586182. doi:10.1155/2020/6586182
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.