Back to Journals » OncoTargets and Therapy » Volume 15
Selinexor, Bortezomib and Dexamethasone: An Effective Salvage Regimen for Heavily Pretreated Myeloma Patients
Authors Delforge M, Raddoux J, Antonis C, Clement C, Kint N, Vanhellemont A, Bravetti J, Vandenberghe P
Received 16 October 2021
Accepted for publication 24 January 2022
Published 14 March 2022 Volume 2022:15 Pages 243—250
DOI https://doi.org/10.2147/OTT.S341120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Michel Delforge,1 Jolien Raddoux,1 Corine Antonis,1 Céline Clement,1 Nicolas Kint,1 Anneleen Vanhellemont,1 Julie Bravetti,2 Peter Vandenberghe1
1Department of Hematology, University Hospital Leuven, Leuven, Belgium; 2Karyopharm Therapeutics, Newton, MA, USA
Correspondence: Michel Delforge, Department of Hematology, University Hospital Leuven, Herestraat 49, Leuven, 3000, Belgium, Tel +32 16 34 68 80, Email [email protected]
Purpose: Multiple myeloma (MM) patients with triple- and penta-refractory disease have a poor survival and limited treatment options. Selinexor, in combination with bortezomib and dexamethasone, demonstrated clinical activity in the STOMP study as well as in the BOSTON study in previously treated patients with disease refractory to a proteasome inhibitor (PI).
Patients and Methods: Here, we report a real-world case series of 7 heavily pretreated MM patients who had been extensively pretreated with bortezomib and had disease refractory to PIs, including carfilzomib; who were administered a starting dose of 100 mg of selinexor, 20– 40 mg dexamethasone and 1.3 mg/m2 of bortezomib, each once weekly. The majority of these patients (6 patients, 86.0%) had penta-refractory disease, with 5 patients (71.4%) having disease refractory to bortezomib and carfilzomib, and all 7 patients having pomalidomide refractory disease. The median number of prior lines of therapy was 8 (range 4– 12).
Results: The seven patients in this case series received selinexor for a median of 5 cycles (range 1– 10). Four patients (57.1%) had a dose reduction of selinexor. Five patients (71.4%) had a response, of which 2 (29.0%) had a very good partial response (VGPR) and 3 (43.0%) had a partial response (PR). One patient (14.3%) had stable disease (SD) and 1 (14.3%) had progressive disease (PD). There were no new safety signals.
Conclusion: The selinexor, bortezomib, and dexamethasone triplet combination demonstrates activity in PI-resistant MM and patients with heavily pretreated MM with refractory disease and after multiple lines of therapy.
Keywords: multiple myeloma, hematologic malignancies, heavily pretreated disease, real-world experience, case series
Introduction
Multiple myeloma (MM) is characterized by the clonal expansion of malignant plasma cells in the bone marrow. For the diagnosis of MM, 10% or more clonal plasma cells must be present in either bone marrow examination or a biopsy-proven plasmacytoma in addition to ≥1 myeloma defining event. These events are based on the CRAB criteria, which includes hypercalcemia, renal failure, anemia, and bone disease.1,2 The incidence of MM in Europe has been estimated to be 4.5–6.0 people per 100,000 per year.3 Despite numerous advancements of therapeutics increasing patient survival, MM remains an incurable disease with most patients relapsing. Current treatment strategies at both diagnosis and relapse include various combination regimens employing immunomodulatory drugs (IMiDs), proteasome inhibitors (PIs), anti-CD38 monoclonal antibodies, and stem cell therapies.4–6 Doublet and triplet regimens have become the standard in the refractory setting for MM. Combination therapies are particularly attractive in the quest to overcome resistance to certain classes of drugs based on mechanism of action.7
Exportin 1 (XPO1) is a nuclear exporter responsible for the nuclear transport of more than 200 targets including tumor suppressor proteins (TSPs) and oncoprotein mRNAs that associate with the cap-binding protein eIF4E, as well as the glucocorticoid receptor (GR).8,9 Most hematologic and solid tumor malignancies, including MM, overexpress XPO1. Elevation of XPO1 is linked with more aggressive MM, with an increase in osteolytic disease and poor clinical outcomes.10–12 Resistance of MM to PIs, including bortezomib, as well as IMiDs has also been correlated to an increase in XPO1.11,13–16
Selinexor is a potent, orally available, selective inhibitor of nuclear export (SINE) compound that binds reversibly to Cys528 in the cargo-binding pocket of XPO1 and blocks its function.17 Inhibition of XPO1 leads to apoptosis of tumor cells while generally sparing normal cells through the forced nuclear localization and functional activation of TSPs, suppression of nuclear factor-κB (NF-κB) activity (through enhanced IκB and other proteins), increase in GR function, and reduction in oncoprotein mRNA translation.14,18,19 Preclinically, the administration of selinexor to MM cells results in an elevated localization of p53, IκB and many other tumor suppressor proteins in the nucleus, inducing tumor cell apoptosis.14 A synergistic interaction was observed when selinexor and PIs were administered to PI-resistant MM cells and in a MM xenograft mouse model, as a consequence of the induction of significant tumor-selective cytotoxicity.20
Selinexor demonstrated clinical activity in previously treated MM in the STORM study where patients treated with twice weekly selinexor plus low dose dexamethasone (Xd) had an overall response rate (ORR) of 26% and a median progression-free survival (PFS) of 3.7 months.12 In a less heavily pretreated patient population in the BOSTON study, patients were administered the triplet combination of once weekly selinexor, dexamethasone and bortezomib (XVd) and had an ORR of 76.4%, a median PFS of 13.9 months, and a significantly reduced rate of peripheral neuropathy as compared to the twice weekly dosing of Vd; overall survival trended in favor of XVd.21
Selinexor has been conditionally approved in Europe by the EMA and in the USA by FDA for use with low dose dexamethasone in the treatment of patients with penta-refractory MM. It is recommended by ESMO guidelines for use in patients with triple-class refractory MM, based on the STORM trial.3,12 In the USA, selinexor has also been approved as a triplet combination with bortezomib and low dose dexamethasone for MM patients with at least one prior therapy and is currently awaiting EMA approval for this indication.3,21,22 In addition, single agent selinexor has been approved for the treatment of patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL) in the USA based on the SADAL study.23
The Karyopharm Expanded Access Program (KEAP) provides access to selinexor for patients who have exhausted all available treatment options and are ineligible for currently ongoing selinexor clinical trials. Patients eligible for this program had heavily pretreated MM, and at minimum, were previously treated with 2 IMiDs, 2 PIs, and daratumumab, with progressive disease. Importantly, supportive care was provided to all of the patients based on published recommendations.24,25 Consent was obtained from all patients and approval was obtained from the local institutional ethics committee for KEAP before starting the program. In this report, we describe the treatment and outcomes of 7 patients treated at the University Hospitals Leuven in Belgium, with heavily pretreated MM that were administered XVd through KEAP.
Case Series
A summary of patient characteristics can be seen in Table 1. Seven patients with heavily pretreated myeloma were treated with weekly XVd. At diagnosis, 4 patients (57.1%) had IgA kappa/lambda type MM and 1 patient (14.3%) had light chain disease only. Four patients (57.1%) had cytogenetic abnormalities as determined by fluorescent in situ hybridization (FISH). In 3 patients (43.0%), no cytogenetic information was available. Prior to XVd treatment, all patients had undergone ASCT and had disease that was refractory to pomalidomide. Six patients (86.0%) had disease that was triple class refractory and 5 (71.4%) had penta-refractory MM. Five patients (71.4%) had disease that was refractory to both bortezomib and carfilzomib. Patients had a median of 8 (4–12) prior lines of therapy. A summary of prior treatments is reported in Supplemental Table 1.
 |
Table 1 Demographics and Clinical Parameters (N=7) |
Treatment
All patients started at 100 mg of selinexor, 20–40 mg dexamethasone, and 1.3 mg/m2 bortezomib, all given once weekly. All patients received 2×8 mg/day ondansetron as prophylactic therapy prior to initiating the XVd regimen. In case of severe nausea and/or vomiting, olanzapine 5–10 mg/d was administered.24,25 Four patients (57.1%) had dose reductions. Of these, 2 patients had 3 dose reductions of selinexor to 40 mg per week, one due to Grade 4 thrombocytopenia (without bleeding) after 4 cycles; nevertheless, after 2 cycles this patient had a very good partial response (VGPR). The patient was active on treatment with the selinexor regimen until cycle 10 (06 Apr 2021). The other patient had 2 dose reductions to 40 mg due to nausea and stopped after 8 cycles of treatment (22 May 2021) with best response being PR after 1 cycle.
Two patients had 1 dose reduction to 80 mg per week due to hematological adverse events (AEs) (asymptomatic thrombocytopenia and neutropenia). Best responses from these patients were VGPR after 4 cycles and PR after 3 cycles with a total of 5 cycles of treatment.
Assessments
All patients had weekly assessments which included complete blood count and blood chemistry. On a monthly basis, immunoglobulin and free light chain (FLC) levels were evaluated. The International Myeloma Working Group (IMWG) consensus criteria for response and minimal residual disease assessment in MM was used to evaluate treatment response.26 National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE), version 5.0 were used for AE reporting.27
Response
All treatment characteristics and responses are listed in Table 2. These patients experienced an ORR of 71%. The majority of patients had VGPR (2 patients, 29.0%) or PR (3 patients, 43.0%). Of the remaining patients, 1 (14.3%) had SD and 1 (14.3%) had PD (Figure 1). A total of 4 patients (57.1%) had dose reductions. The median number of cycles was 5 (range, 1–10) and the median time to progression was 172 days (range, 29–342). Two patients (29.0%) did not have extramedullary disease and response on imaging, one (14.3%) had a metabolic response and still had disease present on 08 Aug 2020, another patient had residual pleural lesions on 08 December 2020, one patient had a partial metabolic response on 08 January 2021 and progressive extramedullary disease on 26 May 2021, and another patient had progressive extramedullary disease on 02 November 2020. One patient had progressive extramedullary disease on 24 August 2020 and very progressive extramedullary disease on 20 November 2020.
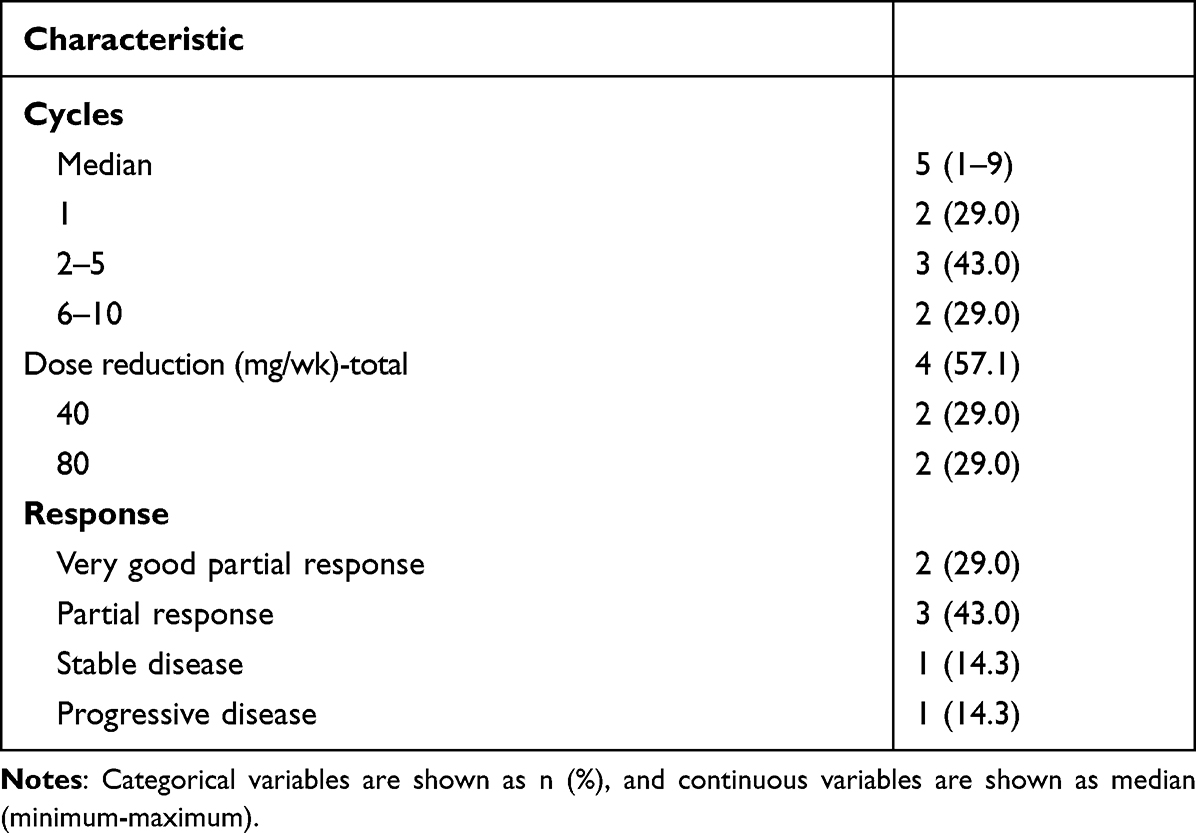 |
Table 2 Treatment Characteristics and Response to Treatment in 7 Subjects |
 |
Figure 1 Best response to study treatment. Swim lane plot showing best response in patients treated with selinexor, bortezomib, and dexamethasone (XVd). Abbreviations: PD, progressive disease; PR, partial response; SD, stable disease; VGPR, very good partial response. |
Safety
Adverse events (AEs) for all patients are in Table 3. All patients experienced thrombocytopenia, with 1 patient (14.3%) having grade 1–2 and 6 patients (86.0%) with grade 3–4. There were no clinically significant bleeding events associated with thrombocytopenia. The majority of patients (6 patients, 86.0%) experienced neutropenia, with 4 (57.1%) having grade 3–4; there were no cases of febrile neutropenia. Of the non-hematological AEs, the most common was grade 1/2 nausea, which was experienced by 6 patients (86.0%). Three patients (43.0%) experienced fatigue, diarrhea, and anorexia and 2 (29.0%) had an upper respiratory infection. One patient had a NYHA grade 4 dyspnea, potentially related to bortezomib-induced pneumonitis. Two patients (29.0%) experienced limited sensible peripheral neuropathy in the fingers or feet and 5 (71.4%) did not have peripheral neuropathy during treatment. During treatment, none of the patients required platelet growth support (romiplostim). All AEs were reversible with proactive supportive care measure and adequate dose modifications.
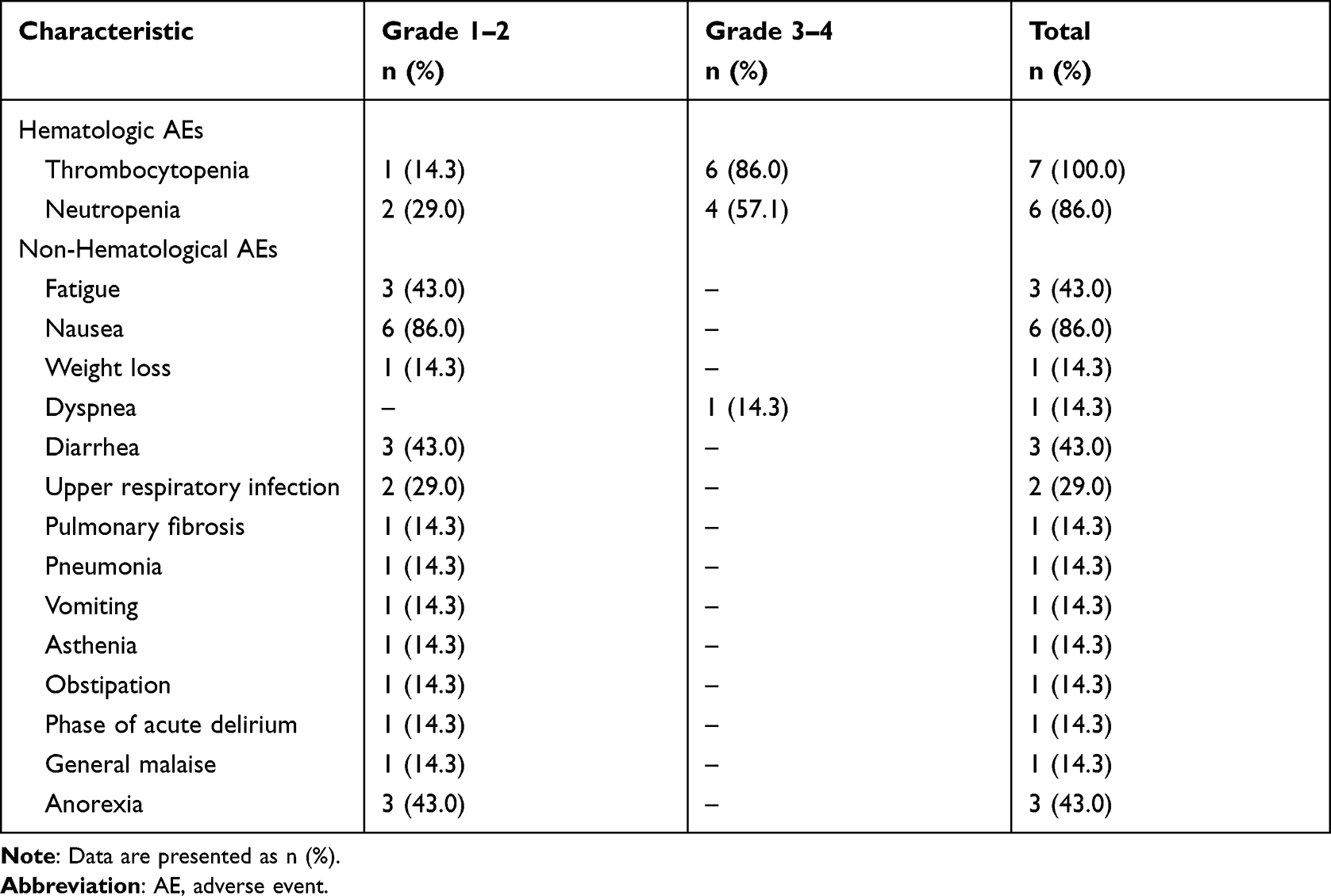 |
Table 3 Adverse Events by Grade in 7 Subjects |
At the time of publication, all patients had discontinued selinexor and one patient was alive and receiving belantamab. Reasons for discontinuation were PD 4 (57.1%), intolerance 1 (14.3%), patient request 1 (14.3%), and 1 (14.3%) was due to end of treatment (bridging for CART therapy). After selinexor treatment, 1 patient (14.3%) was subsequently treated with carfilzomib plus dexamethasone and then treated with belantamab. One patient (14.3%) was treated with CART therapy, then lenalidomide, and lastly with radiotherapy. Three patients (42.8%) were subsequently treated with belantamab. Three patients (42.8%) did not receive another treatment regimen after selinexor.
Discussion
This is the first report of real-world experience with XVd of patients in Europe with heavily pretreated refractory MM. Here, we show that after multiple lines of treatments with the most common MM drugs, XVd conferred clinical benefits. In this series, patients had exhausted all MM treatments available in our institution and had a very poor prognosis. The once weekly regimen with bortezomib supports the preclinical observation that there is a synergistic effect in enhancing the functional activity of TSPs by blocking nuclear export and cytoplasmic degradation/inactivation when selinexor is combined with a PI like bortezomib.20,28
The patients reported in this cohort were in worse health, with heavily pretreated disease without other remaining treatment options, and more heavily pretreated compared with patients in the BOSTON study. In the latter study, patients had been previously treated with only 1–3 lines of therapy, including PIs. The median PFS of patients treated with XVd in the BOSTON study was 13.9 months and the median OS was not reached. As compared to the BOSTON study, this cohort of patients had poor baseline characteristics and had received more prior lines of therapy (median 2 [1–3] versus 8 [4–12] lines). All patients in this report had undergone previous ASCT compared to only 35% in the BOSTON study.21 Interestingly, although patients were very heavily pretreated in comparison with patients enrolled in the BOSTON study, similar response rates to XVd were observed in this cohort: VGPR 29% vs 28%, PR 43.0% vs 32%, and SD 14.3% vs 13%, respectively.21 Of the 5 (71.4%) patients that had disease refractory to bortezomib, 3 (43.0%) had PR and of those patients, 2 (29.0%) had penta-refractory disease and 1 (14.3%) had triple-class refractory disease, demonstrating that patients with bortezomib resistance and poly-refractory disease benefitted from the XVd regimen.
Patients in this cohort did have a higher incidence of thrombocytopenia compared to the BOSTON study, but this is mostly likely due to the extensive prior treatment, including ASCT, affecting residual bone marrow reserve and the fact that all patients started at a high dose of selinexor. One patient had a NYHA grade 4 dyspnea that could have resulted from an interstitial pneumonitis caused by bortezomib, which was subsequently discontinued. Otherwise, no new safety signals were observed. Although the patients in this cohort had heavily pretreated disease and multiple lines of prior treatment, they were able to respond and tolerate the once weekly selinexor treatment.
Other case series evaluating heavily pretreated RRMM patients treated with XVd from Magen et al and Mouhieddine et al had similar response rates to this cohort of patients.29,30 In contrast to the data presented here, patients in the Magen et al case series had a higher incidence of PD, which could be due to the fact that most patients were started at 60 mg of selinexor with rapidly progressing MM.29 The patient cohort in the Mouhieddine et al case series was also heavily pretreated and benefited from XVd treatment with prolonged survival. Of those patients, one had been previously treated with selinexor in the STORM study, having achieved a good response but eventually requiring dose reductions, which resulted in a loss of treatment response.30 These two case series further support the use of XVd in patients with heavily pretreated disease that have exhausted all other options. The results are also consistent with the use of higher (eg, 80–100 mg) initial doses of selinexor in order to arrest disease progression, and then the dose may be reduced. Along these lines, it is worth noting that there was only a single instance of PD in the BOSTON study amongst the 195 patients treated with once weekly XVd,21 as compared with 10 cases of PD amongst the 200 patients with twice weekly Vd, further supporting the potency of the higher dose regimen.
Selinexor in combination with dexamethasone (Xd) has been given conditional marketing authorization by the EMA (EMA number: EMEA/H/C/005127/0000) for adult patients with MM with a minimum of 4 prior lines of treatment with progression of disease from last line of therapy and who have refractory disease that includes at least 2 PIs, 2 IMiDs, and an anti-CD38 monoclonal antibody.31 This represents a major milestone towards the treatment of MM and currently the use of XVd is under review with the EMA based on the BOSTON study.3,21 In alignment with this goal, there is also an ongoing trial in Israel to evaluate XVd in heavily pretreated patients with relapsed/refractory (RR) MM. Taken together, these results are promising and could support future studies with a larger patient cohort for patients with heavily pretreated MM that have exhausted all other options.
Conclusion
This is the first real-world report of once weekly oral selinexor in combination with weekly bortezomib and dexamethasone to treat RRMM in Europe. Seven patients with heavily pretreated MM after exhaustion of all treatment options, including PIs such as bortezomib and carfilzomib and whose disease was refractory to either or both, benefited from XVd treatment. The ORR of 71%, acceptable safety profile, and management of AEs with supportive care and dose reduction indicates a benefit of XVd in heavily pretreated RRMM patients. Supportive care involved the prophylactic administration of ondansetron, and olanzapine in case of severe nausea and/or vomiting.24,25 Despite the small number of patients, XVd in this population demonstrated clinical activity in a real-world setting, and these results may guide future studies with increased patient numbers. The use of once weekly oral selinexor treatment in combination with PIs (as well as IMiDs32,33 and CD38 mAbs34) could be a promising treatment option, filling an unmet need for patients with advanced and refractory MM.
Ethics Approval and Informed Consent
Consent was obtained from all patients and approval was obtained from Ethical Committee UZ Leuven for the Karyopharm Expanded Access Program before starting the program and performed in accordance with the International Conference on Harmonization Good Clinical Practice Guidelines and the Declaration of Helsinki.
Consent for Publication
Written informed consent for publication of their clinical details was obtained from the patients. A copy of the consent form is available for review by the Editor of this journal.
Acknowledgments
Selinexor for compassionate use was provided by Karyopharm Therapeutics. JetPub Scientific Communications LLC assisted the authors in the preparation of this manuscript, in accordance with Good Publication Practice (GPP3) guidelines.
Disclosure
MD has received honoraria from Amgen, BMS, Celgene, Janssen, Sanofi, Takeda and Karyopharm Therapeutics. JB is an employee of Karyopharm Therapeutics. PV reports honoraria from BMS, Gilead, Janssen, Miltenyi biotech, Novartis, Pfizer. NK reports conference travel supports from Janssen, Takeda, Celgene, and Amgen, outside the submitted work. All other authors report no conflicts of interest in this work.
References
1. Rajkumar SV. Multiple myeloma: 2020 update on diagnosis, risk-stratification and management. Am J Hematol. 2020;95(5):548–567. doi:10.1002/ajh.25791
2. Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538–e548. doi:10.1016/S1470-2045(14)70442-5
3. Dimopoulos MA, Moreau P, Terpos E, et al. Multiple myeloma: EHA-ESMO clinical practice guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2021;32(3):309–322. doi:10.1016/j.annonc.2020.11.014
4. Kumar S, Callander N, Adekola K, et al. Multiple Myeloma, version 3.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2020;28(12):1685–1717. doi:10.6004/jnccn.2020.0057
5. Nijhof IS, van de Donk NWCJ, Zweegman S, Lokhorst HM. Current and new therapeutic strategies for relapsed and refractory multiple myeloma: an update. Drugs. 2018;78(1):19–37. doi:10.1007/s40265-017-0841-y
6. Anderson KC. Progress and paradigms in multiple myeloma. Clin Cancer Res. 2016;22(22):5419–5427. doi:10.1158/1078-0432.CCR-16-0625
7. Sonneveld P. Management of multiple myeloma in the relapsed/refractory patient. Hematol Am Soc Hematol Educ Progr. 2017;2017(1):508. doi:10.1182/ASHEDUCATION-2017.1.508
8. Xu D, Grishin NV, Chook YM. NESdb: a database of NES-containing CRM1 cargoes. Mol Biol Cell. 2012;23(18):3673–3676. doi:10.1091/mbc.E12-01-0045
9. Camus V, Miloudi H, Taly A, Sola B, Jardin F. XPO1 in B cell hematological malignancies: from recurrent somatic mutations to targeted therapy. J Hematol Oncol. 2017;10(1). doi:10.1186/s13045-017-0412-4
10. Gandhi UH, Senapedis W, Baloglu E, et al. Clinical implications of targeting XPO1-mediated nuclear export in multiple myeloma. Clin Lymphoma Myeloma Leuk. 2018;18(5):335–345. doi:10.1016/j.clml.2018.03.003
11. Azizian NG, Li Y. XPO1-dependent nuclear export as a target for cancer therapy. J Hematol Oncol. 2020;13(1):1–9. doi:10.1186/s13045-020-00903-4
12. Chari A, Vogl DT, Gavriatopoulou M, et al. Oral selinexor-dexamethasone for triple-class refractory multiple myeloma. N Engl J Med. 2019;381(8):727–738. doi:10.1056/NEJMoa1903455
13. Gravina GL, Senapedis W, McCauley D, Baloglu E, Shacham S, Festuccia C. Nucleo-cytoplasmic transport as a therapeutic target of cancer. J Hematol Oncol. 2014;7(1). doi:10.1186/s13045-014-0085-1
14. Tai YT, Landesman Y, Acharya C, et al. CRM1 inhibition induces tumor cell cytotoxicity and impairs osteoclastogenesis in multiple myeloma: molecular mechanisms and therapeutic implications. Leukemia. 2014;28(1):155–165. doi:10.1038/leu.2013.115
15. Chanukuppa V, Paul D, Taunk K, et al. XPO1 is a critical player for bortezomib resistance in multiple myeloma: a quantitative proteomic approach. J Proteomics. 2019;209:103504. doi:10.1016/j.jprot.2019.103504
16. Bhutani M, Zhang Q, Friend R, et al. Investigation of a gene signature to predict response to immunomodulatory derivatives for patients with multiple myeloma: an exploratory, retrospective study using microarray datasets from prospective clinical trials. Lancet Haematol. 2017;4(9):e443–e451. doi:10.1016/S2352-3026(17)30143-6
17. Jardin F, Pujals A, Pelletier L, et al. Recurrent mutations of the exportin 1 gene (XPO1) and their impact on selective inhibitor of nuclear export compounds sensitivity in primary mediastinal B-cell lymphoma. Am J Hematol. 2016;91(9):923–930. doi:10.1002/ajh.24451
18. Golomb L, Bublik DR, Wilder S, et al. Importin 7 and exportin 1 link c-Myc and p53 to regulation of ribosomal biogenesis. Mol Cell. 2012;45(2):222–232. doi:10.1016/j.molcel.2011.11.022
19. Schmidt J, Braggio E, Kortuem KM, et al. Genome-wide studies in multiple myeloma identify XPO1/CRM1 as a critical target validated using the selective nuclear export inhibitor KPT-276. Leukemia. 2013;27(12):2357–2365. doi:10.1038/leu.2013.172
20. Turner JG, Kashyap T, Dawson JL, et al. XPO1 inhibitor combination therapy with bortezomib or carfilzomib induces nuclear localization of IκBα and overcomes acquired proteasome inhibitor resistance in human multiple myeloma. Oncotarget. 2016;7(48):78896–78909. doi:10.18632/oncotarget.12969
21. Grosicki S, Simonova M, Spicka I, et al. Once-per-week selinexor, bortezomib, and dexamethasone versus twice-per-week bortezomib and dexamethasone in patients with multiple myeloma (BOSTON): a randomised, open-label, Phase 3 trial. Lancet. 2020;396(10262):1563–1573. doi:10.1016/S0140-6736(20)32292-3
22. XPOVIO (Karyopharm Therapeutics Inc.): FDA package insert. Available from: https://medlibrary.org/lib/rx/meds/xpovio-1/.
23. Kalakonda N, Maerevoet M, Cavallo F, et al. Selinexor in patients with relapsed or refractory diffuse large B-cell lymphoma (SADAL): a single-arm, multinational, multicentre, open-label, Phase 2 trial. Lancet Haematol. 2020;7(7):e511–e522. doi:10.1016/S2352-3026(20)30120-4
24. Mikhael J, Noonan KR, Faiman B, et al. Consensus recommendations for the clinical management of patients with multiple myeloma treated with selinexor. Clin Lymphoma Myeloma Leuk. 2020;20(6):351–357. doi:10.1016/j.clml.2019.12.026
25. Gavriatopoulou M, Chari A, Chen C, et al. Integrated safety profile of selinexor in multiple myeloma: experience from 437 patients enrolled in clinical trials. Leukemia. 2020;34(9):2430–2440. doi:10.1038/s41375-020-0756-6
26. Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328–e346. doi:10.1016/S1470-2045(16)30206-6
27. Cancer Institute N. Common Terminology Criteria for Adverse Events (CTCAE) Common Terminology Criteria for Adverse Events (CTCAE) V5.0; 2017.
28. Kashyap T, Argueta C, Unger T, et al. Selinexor reduces the expression of DNA damage repair proteins and sensitizes cancer cells to DNA damaging agents. Oncotarget. 2018;9(56):30773–30786. doi:10.18632/oncotarget.25637
29. Magen H, Geva M, Volchik Y, Avigdor A, Nagler A. Selinexor, bortezomib, and dexamethasone for heavily pretreated multiple myeloma: a case Series. Clin Lymphoma Myeloma Leuk. 2020;20(12):e947–e955. doi:10.1016/j.clml.2020.07.016
30. Mouhieddine TH, Parekh S, Cho HJ, et al. Selinexor, bortezomib, and dexamethasone (SVD) in heavily treated relapsed refractory multiple myeloma. Ann Hematol. 2021;100(12):3057–3060. doi:10.1007/s00277-020-04293-y
31. Nexpovio-Union Register of medicinal products - Public health - European Commission. Available from: https://ec.europa.eu/health/documents/community-register/html/h1537.htm.
32. White DJ, Lentzsch S, Gasparetto C, et al. Safety and efficacy of the combination of selinexor, lenalidomide and dexamethasone (SRd) in Patients with newly diagnosed multiple myeloma. Blood. 2019;134(Supplement_1):3165. doi:10.1182/blood-2019-124370
33. Chen CI, Bahlis N, Gasparetto C, et al. Selinexor, pomalidomide, and dexamethasone (SPd) in patients with relapsed or refractory multiple myeloma. Blood. 2019;134(Supplement_1):141. doi:10.1182/BLOOD-2019-122907
34. Gasparetto C, Lentzsch S, Schiller GJ, et al. Selinexor, daratumumab, and dexamethasone in patients with relapsed/refractory multiple myeloma (MM). J Clin Oncol. 2020;38(15_suppl):8510. doi:10.1200/jco.2020.38.15_suppl.8510
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.