")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Self-Care Management for Hypertension in Southeast Asia: A Scoping Review
Authors Irwan AM , Potempa K, Abikusno N, Syahrul S
Received 23 March 2022
Accepted for publication 23 August 2022
Published 9 September 2022 Volume 2022:15 Pages 2015—2032
DOI https://doi.org/10.2147/JMDH.S367638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Andi Masyitha Irwan,1,2 Kathleen Potempa,2 Nugroho Abikusno,3 Syahrul Syahrul1
1Faculty of Nursing, Hasanuddin University, Makassar, Indonesia; 2School of Nursing, University of Michigan, Ann Arbor, MI, USA; 3Faculty of Medicine, Universitas Trisakti, Jakarta, Indonesia
Correspondence: Andi Masyitha Irwan, Faculty of Nursing, Hasanuddin University, Jl. Perintis Kemerdekaan KM.10, Makassar, South Sulawesi, 90245, Indonesia, Tel +6285342600183, Email [email protected]
Background: Self-care practices such as lifestyle modifications in diet, exercise, and stress management are effective in reducing the incidence of and enhancing better management of hypertension. However, little is known about the self-care management practices of people with hypertension in Southeast Asia (SEA) countries where the prevalence of hypertension is sharply increasing.
Methods: A scoping review of research and grey literature (2006– 2021) was performed using Scoping Review Frameworks by Arkey and O’Malley. For the research literature, ten databases were searched followed by a manual search of the reference lists of relevant topical papers. Criteria for inclusion included both qualitative and quantitative primary data studies, focused on adult (18 years and over) hypertensive patients, self-care management methods, conducted in SEA. The study protocol has been registered at Open Science Framework (https://osf.io/s4nvk/).
Results: Out of 1667 studies examined, there were 57 studies that met criteria and were included in this review. Results indicate a paucity of relevant literature. Moreover, most studies reviewed showed an incident rate of 50% or more incidence of behavioural risk factors in people diagnosed with hypertension, including overweight/obesity, poor physical exercise, poor/low-quality dietary intake, and not adhering to medication. Few studies indicated adequate traditional self-care practice among SEA hypertension populations. Use of a non-prescription herbal as the medication is identified in some studies. Several reviewed articles indicated that there is individual variation in the facilitators and barriers to implementing self-care practices and we put it into a working framework. The facilitators and barriers are relevant to personal choice (internal factors) or to the environment or context (external factors).
Conclusion: Enhancing self-care management of hypertension in SEA may require a multi-focused approach including targeting personal choice as well as external factors such as cultural relevance, environment, and resources.
Keywords: self-care hypertension, facilitating and inhibiting factors, Southeast Asia countries
Plain Language Summary
In SEA countries where the prevalence of hypertension is sharply increasing, there are few relevant studies on how patients perform their self-care management practices. The studies that have been completed indicate that many hypertensive people have significant behavioral risk factors for heart disease and stroke despite the common medical advice to address these risk factors through self-care management practices, Irwan et al in their review, found a prevalence rate of 50% or more of hypertension people being overweight/obese, having poor physical exercise and low-quality dietary intake, and not adhering to medication. They also found variation in the facilitators and barriers to implementing self-care practices, including personal choices and cultural influence. This information is useful for nurses suggesting that nurses working in the community in SEA countries should consider a multi-focused approach and cultural aspect in helping hypertensive patients manage their self-care and risk reduction practices.
Introduction
Hypertension is a major chronic disease among adults affecting 1 in 4 men and 1 in 5 women representing over one billion people worldwide.1 The American Heart Association defines hypertension as the systolic blood pressure readings of ≥130 mmHg and/the diastolic blood pressure readings of ≥80 mmHg.2 It is considered a primary risk factor for stroke, heart disease, and kidney failure.3
To reduce the incidence of and to provide better management of hypertension, several self-care activities are recommended by the 8th Joint National Commission including medication adherence, bodyweight management, dietary intake, alcohol consumption, tobacco cessation, and physical exercise.4,5 Modification of lifestyle risk factors addressed through healthy self-care management activities is now a fundamental part of treatment recommendations, as people who implement such self-care strategies have shown a decrease in blood pressure, increase adherence to antihypertensive medications, reductions in complications and in overall mortality rate associated with hypertension.6
Numerous reviews of self-care management for hypertension have been done regarding the experimental approach to lifestyle intervention provided through the research protocol.7–9 While important to understand the efficacy of the intervention, these studies do not address the self-care management initiated and sustained by people in their naturalistic settings. Few studies address potential facilitating and inhibiting factors in practicing self-care management for hypertension. In addition, the majority of studies reviewed were conducted in Western countries.7–9 Different cultures, lifestyles, and food preferences in SEA countries will affect the use and success of self-care management of hypertension.
In SEA countries, the prevalence of hypertension has been sharply increasing for the past two decades.10 In a recent study, there was a reported increase of one-third of the adult population with hypertension in SEA annually.11 SEA countries are currently experiencing rapid modernization and fast-changing lifestyle, conditions contributing to the high prevalence of hypertension.10 However, little is known about the self-care management practices of these populations. The previous review by Nawi et al focused on the prevalence and risk factors of hypertension in the urban area without emphasizing current self-care management for hypertension.11 Understanding the self-care management of people with hypertension is crucial to determine gaps and potential points of intervention to strengthen their use and effectiveness. Therefore, we conducted a scoping review to explore and map the current state of self-care and lifestyle management activities among people with hypertension in SEA countries. Secondarily, we reviewed the retrieved articles for facilitating and inhibiting factors to the reported self-care management practices. The anticipated outcome of such a scoping review is to better understand the current state of self-care practices for hypertension management in SEA. This information will be useful in designing future studies.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews (PRISMA-SCR) was utilized to optimize reporting and increase fidelity (Supplementary File 1). The review was conducted using the guidelines of Scoping Review Frameworks.12 In addition, The Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews (PRISMA-SCR) was utilized to optimize reporting and increase fidelity.13 The study protocol has been registered at Open Science Framework (https://osf.io/s4nvk/). We utilized the five stages of Scoping Review Frameworks as indicated below.
Stage 1: Research Question
The research question raised by this scoping review was:
What type of self-care management strategies do hypertensive people in SEA countries use to control their blood pressure where SEA countries include Brunei, Malaysia, Indonesia, Thailand, Singapore, the Philippines, Vietnam, Laos, Cambodia, Myanmar, and East Timor?
Stage 2: Relevant Studies and Search Terms
The review explored the current state of self-care management practices used by hypertension populations based on evidence from the existing scientific literature for SEA. Because “lifestyle change” and “self-care management” are often used interchangeably in reported studies, we used both terms to identify relevant studies.14–16 Furthermore, specific emphasis was focused on the application of general self-care management techniques practiced across cultures and their geo-socio-political nuances with emphasis on the SEA context.
We used ten data bases used in this scoping review. An initial search was conducted to retrieve titles, abstracts, and content to identify terms and key words including alternative aliases across languages and cultures. Table 1 displays the key words and phrases used in the search. In addition, references in the Google Scholar search engine were sought for additional articles that may have been missed in the previous database searches.
 |
Table 1 Keywords for Databases |
The inclusion and exclusion criteria for the scoping review was based on Population Concept Context (PCC) model17 and are listed in Table 2. The definition of hypertension is as defined by the author(s) of the studies. The review included both qualitative and quantitative primary data studies. Review, intervention, study protocol papers, and pregnancy-induced hypertension populations were not included. The search was limited to full-text articles published in English and Bahasa from 2006 to 2021. Fifteen years was chosen as the time window of the search as that coincides with the recent rise in prevalence of hypertension in SEA countries.
 |
Table 2 Eligibility Criteria for Articles |
Stage 3: Study Selection
Study Extraction from Databases
Figure 1 illustrates the process, screening results, and criteria for manuscript extraction once the initial search was completed based on the study inclusion and exclusion criteria. To summarize, from the 10 databases, 1667 relevant abstracts were collected and 41 additional manuscripts were identified through Google Scholar. After the removal of duplication of articles, 1668 articles remained. Furthermore, titles were screened for their relevance resulting in 167 articles for further screening. Of these, 125 articles were categorized as directly related to the research question, followed by full article reading and study abstraction. Third-stage searching was also conducted by screening reference list from the articles selected by reading full text resulting in an additional 20 articles. Articles were then excluded that were not relevant to the hypertension, not self-care management, not in SEA, or were an intervention, a study protocol, or were a literature review. This selection process resulted in the final inclusion of 57 primary research studies in the analysis.
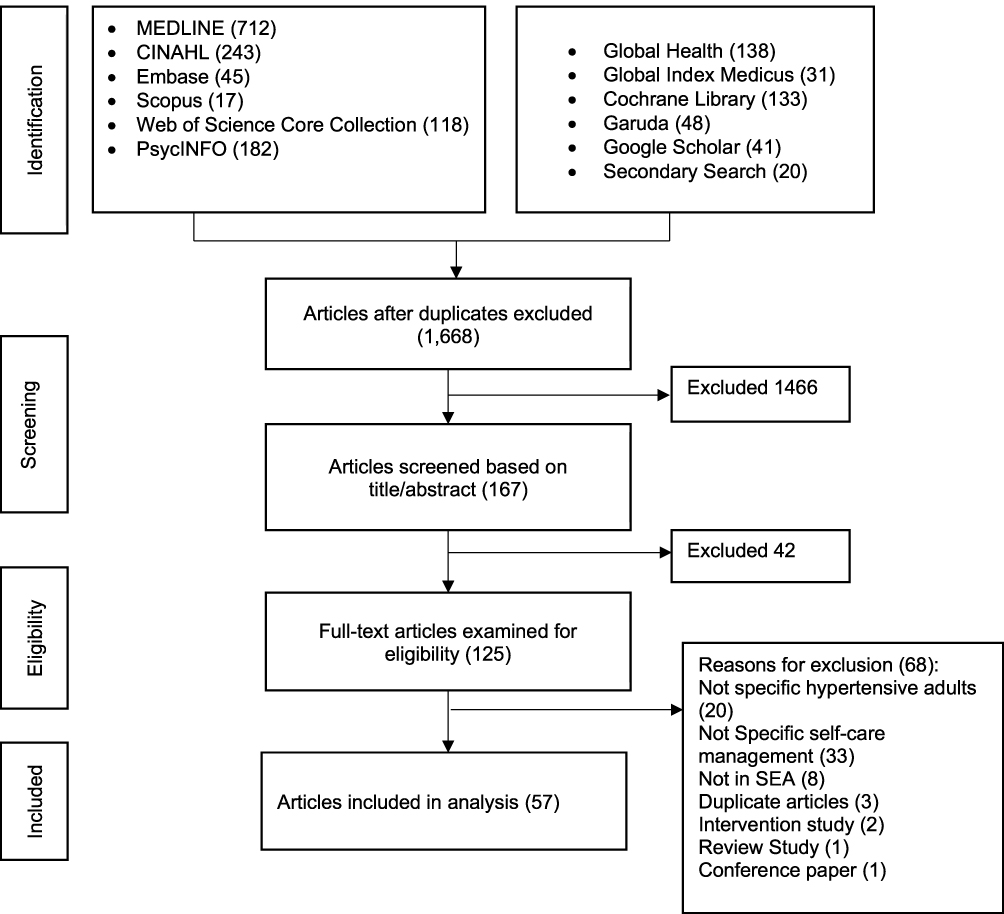 |
Figure 1 PRISMA flowchart. Notes: Adapted from Tricco AC, Lillie E, Zarin W et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med.2018;169(7);467–473.13 |
Reliability of Study Extraction
All abstracts identified from the article search were downloaded to Mendeley software reference manager and exported following de-duplication into the Rayyan software program.18 To ensure inter-rater reliability of articles screened using exclusion and inclusion criteria was established by two reviewer random samples of 25 articles in English language (AMI and KP) for sampling of titles, abstracts, and full texts using JBI Manual methods.17 There was disagreement in 5% of articles which was resolved in reviewer discussion to reach 100% agreement at each sampling stage.
Stage 4: The Data
Data were extracted to include important information, encompassing the study site, study design, aim, sample, and main findings. Variable measured are listed in Tables 3 and 4.
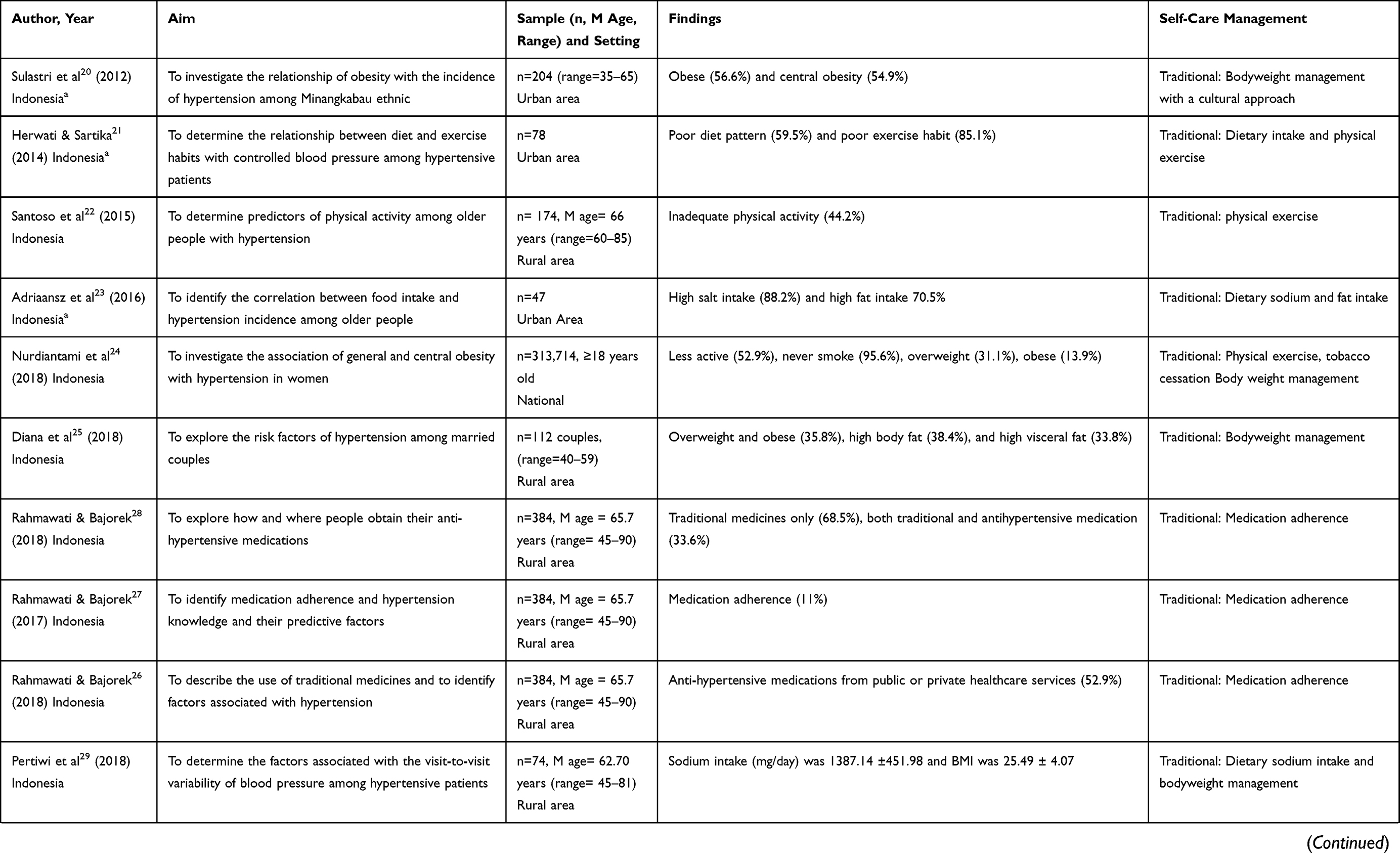 | 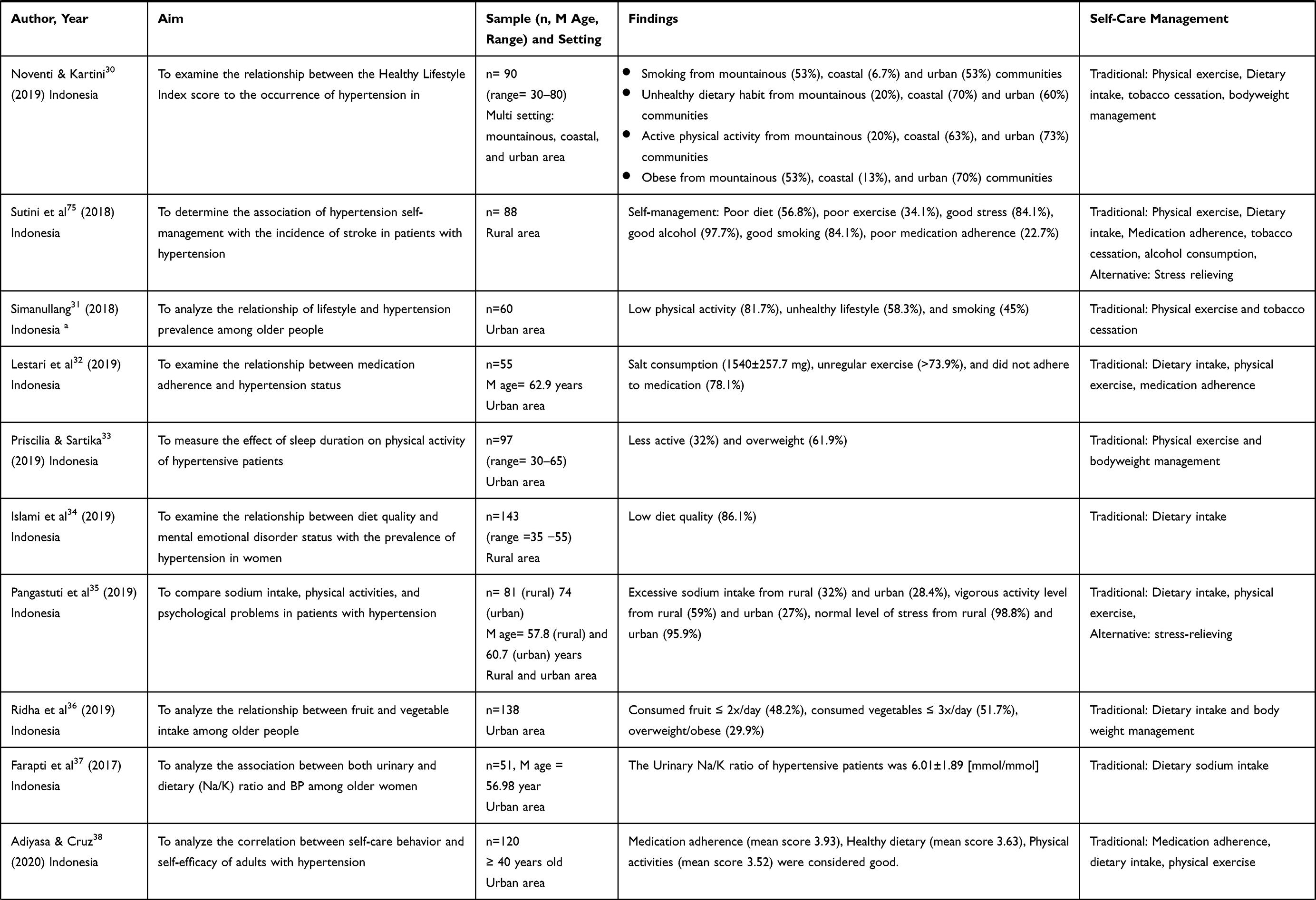 | 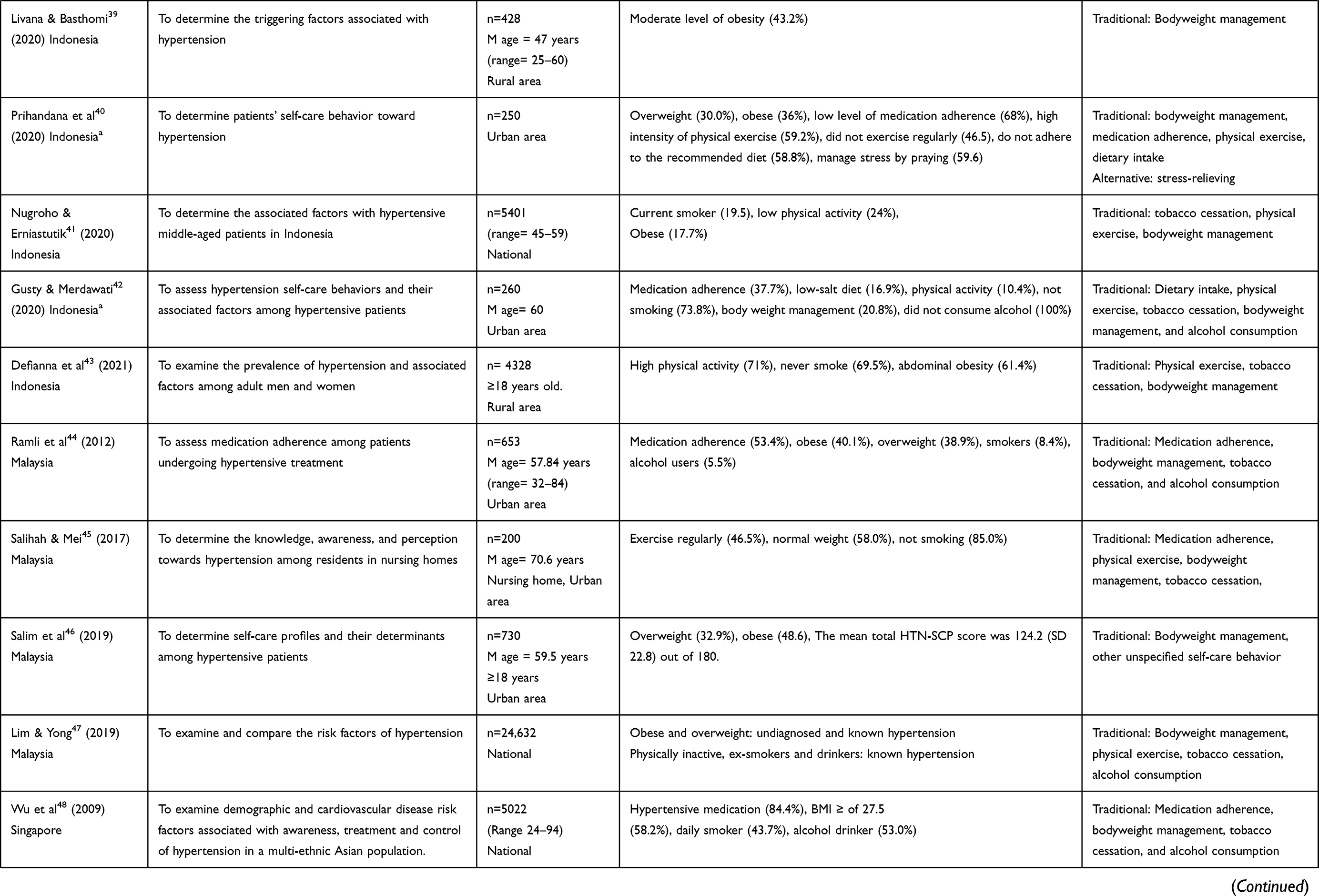 | 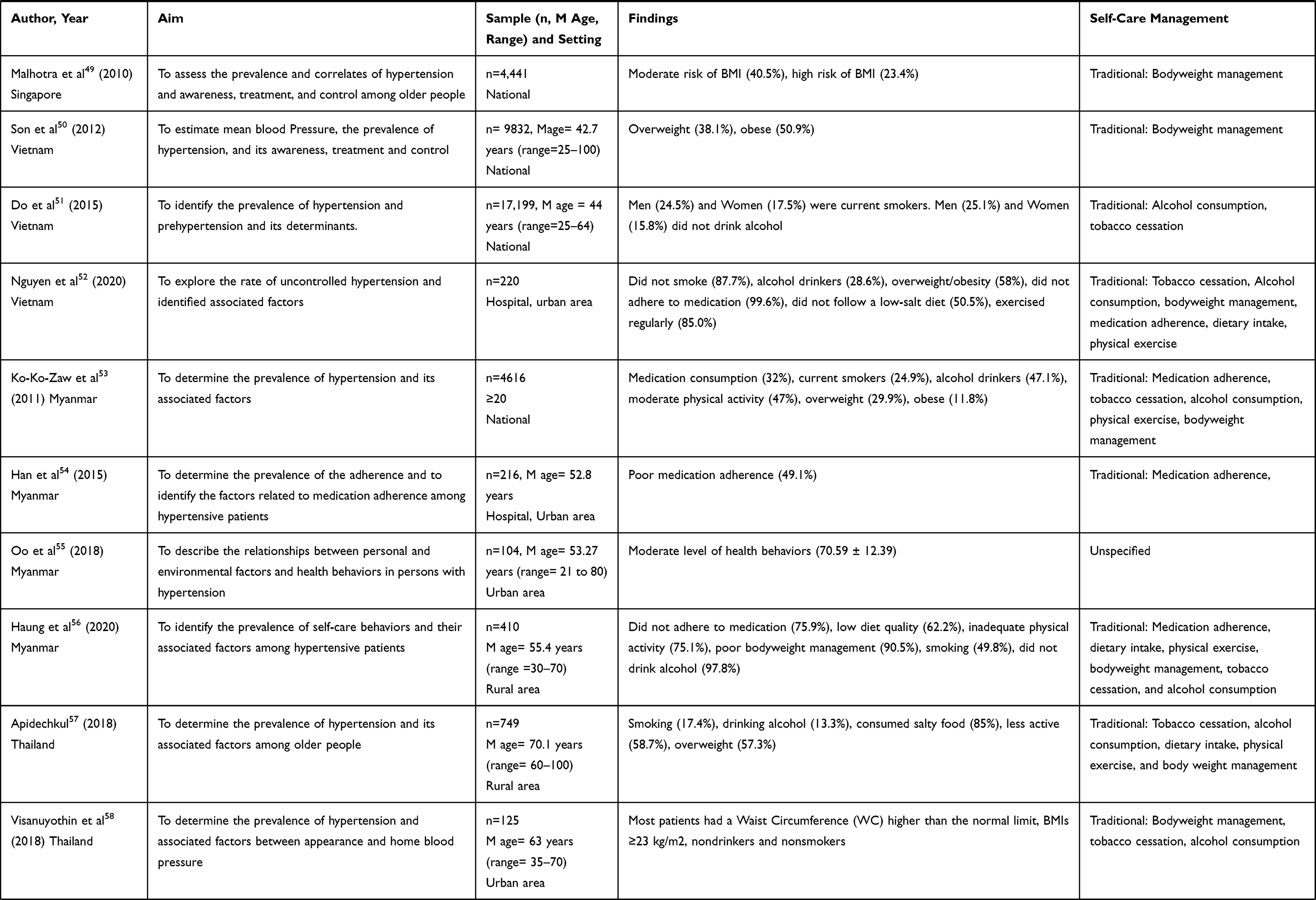 |
Table 3 Articles Exploring Self-Care Management for Hypertension (Quantitative and Mixed Method Studies) |
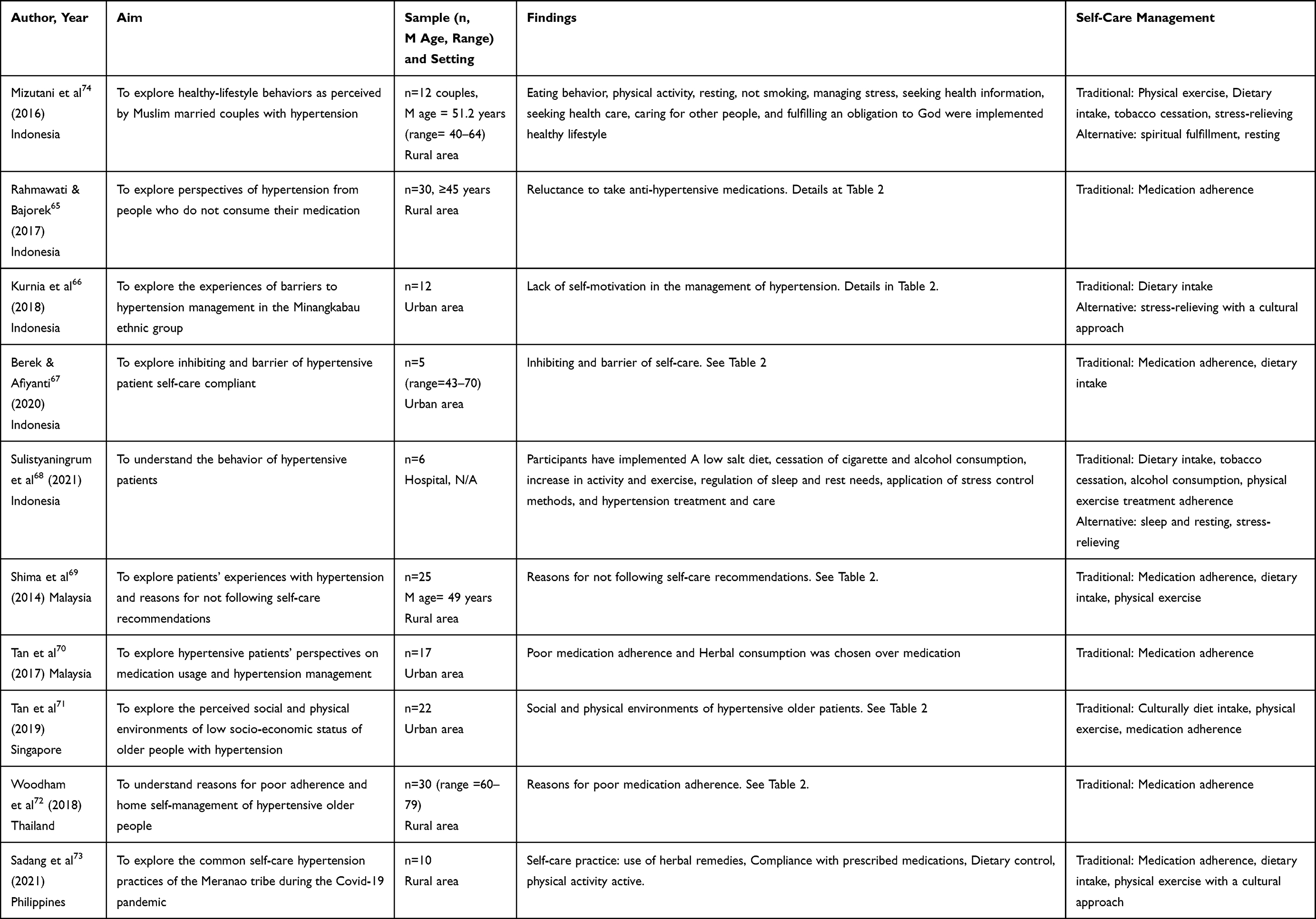 |
Table 4 Articles Exploring Self-Care Management for Hypertension (Qualitative Studies) |
Stage 5: Thematic Summary and Key Findings
Inductive thematic analysis, informed by the work of Braun and Clarke19 across studies, was used to identify emerging key themes. This entails familiarization with each research finding and generating initial codes. These codes were then refined to arrive at the final themes reported in the paper.
Ethical Considerations
This study was exempt from review by the Institutional Review Board for Human Subjects (IRB) because only de-identifiable data is revealed in the articles reviewed.
Study Characteristics
Across the 57 included studies, more than half (thirty studies) were conducted in Indonesia, seven in Thailand, six in Malaysia, four in Myanmar, three for each in Vietnam and in Singapore, one in the Philippines, one in Laos, and two combined across SEA countries. There are three countries of SEA which have no included articles: Brunei, Cambodia, and East Timor. The design of the studies was varied. Forty-five were cross-sectional studies,20–64 ten were qualitative,65–74 one case control,75 and one mixed-method design.76 The findings of quantitative and mixed-method studies are displayed in Table 3 and qualitative studies in Table 4. The sample sizes of quantitative and mixed-method studies ranged from 47 to 313,714 participants. A study with the largest sample (313,714) was conducted by Nurdiantami et al.24 Sample sizes ranged from 5 to 30 participants in the qualitative studies reviewed. For study settings, in quantitative and mixed-method studies, 10 studies took place nationally,24,41,47–51,53,63,64 19 in the urban areas,20,21,23,31–33,36–38,40,42,44–46,52,54,55,58,76 16 in rural areas,22,25–29,34,39,43,56,57,59–62,75 and two studies in multiple settings.30,35 For quantitative studies, four of them were conducted in urban settings,66,67,70,71 five were in the rural area65,69,72–74 and one study could not be specified.68 Overall, thirteen22,26–29,32,42,45,57–60,64 studies have the mean age of older people as the participants (60 years old and above), whereas the rest of the studies were adults 18 years and older.
Self-Care and Lifestyle Management
In the quantitative and mixed-method studies, body weight management (29 studies20,24,25,29,30,33,36,39–50,52,53,56–62,64) and physical exercise (22 studies21,22,24,30–33,35,38,40–43,45,47,52,53,56,57,60,61,75) were the most reported, whereas in the qualitative studies, medication adherence and diet intake was the most reported self-care practice. In addition, a few studies described alternative self-care management methods such as stress-relieving methods (6 studies35,40,60,66,68,75), sleep and rest (2 studies68,74), and spiritual fulfilment was described in one study.
In the quantitative and mixed-method studies, studies indicated that traditional self-care management, such as body weight management, physical exercise, dietary intake, and medication adherence were poorly practiced. Respectively, studies showed unaddressed risk factors for heart disease and stroke with a 50% incidence or more being reported for overweight/obese (8 studies20,30,33,50,52,56,57,61), low level physical exercise (8 studies21,24,31,32,45,56,57,61), poor/low-quality dietary intake (9 studies21,23,30,34,40,56,57,60,75), and poor adherence to medication (4 studies27,32,52,56).
In the qualitative studies, the majority explored reasons for not adhering to self-care management mainly on medication adherence which we will explain in detail in the next section. Overall, a few studies28,70,73 identified the usage of herbal as medication for hypertension.
Facilitating and Inhibiting Factors
In the review of the retrieved articles, we identified facilitating and inhibiting factors of self-care management for hypertension. These factors are described in the article texts as examples from the statements of participants found in the studies and are described in Table 5. We further divided these examples into internal and external associated factors. Internal sources are those that are under individual’s control or influence and external sources or associated factors are those that are influenced by others in the household or by the community or environment in which the participant lives. Statements described in the articles text such as “Put reminder not to forget” and “motivation to avoid progression” are considered as internal facilitating factors to practice self-care management. Having “discussion with partners related to medication problems and organized activities by the health center” to improve health, are examples of external facilitating associated factors. Whereas statements in the text such as “Perceived self-care practice not as a priority”, ‘side effects’, “feeling tired of medication”, “having no signs and symptoms” of hypertension, as well as “time and financial barrier” were classified as internal inhibitory sources which inhibit self-care practice among hypertensive subjects in SEA. Whereas hypertension diet “not adjusted to the culture”, “distance barrier” to the health center, “lack of family support”, and “lack of knowledge” related to hypertension and its management were considered as external sources.
 |
Table 5 The Facilitating and Inhibiting Factors of Self-Care Management for Hypertension |
Discussion
The primary aim of this review was to examine and map the state of the science of self-care management of hypertensive people living in SEA countries. The evidence presented indicates that there is a high rate of overweight/obese, poor physical exercise, poor/low-quality dietary intake, and not adhering to medication in hypertensive people in the SEA region. As a consequence of economic development, significant changes in diet, mainly the increased consumption of high fat and sugar, combined with physical exercise reduction occurred in many Asian countries.77,78 Other economically developed or developing countries show similar trends. In the USA, diet adherence and body weight management are only 18% and 39%, respectively, among hypertensive patients.80 Poor body weight management (53.2%) and poor physical exercise (69%) were reported among hypertensive patients in Ethiopia.79 In Iran, among hypertensive patients, only 24.5% adhered to performing physical exercise and 39.2% managed their body weight.80 Lifestyle has been a critical factor contributing to the rise in incidence of hypertension globally, and lifestyle risk factors remain poorly managed by many populations including SEA. A focus on lifestyle risk reduction in hypertensive people is a clear implication of our findings.
Another finding of our review is the use of herbal as hypertension medication. Similarly, previous studies have shown that using a herbal as self-medication is not only found with older age, but also among young people in SEA. Fear of adverse reactions in prescribed medicine, the effectiveness of herbal medicine, and easier access were reasons for choosing herbal.83–85 However, consuming herbals as self-medication poses a health risk as dosing is unreliable, efficacy for short- and long-term use is understudied, and harmful interaction effects with polypharmacy may occur.84–86 Therefore, it is important to assess the knowledge of patients in using herbal and to what extent herbal medicine is used to manage hypertension.
We report various internal and external factors described across studies influencing poor self-care management. Because this is a secondary finding of our review, further research into the scope and complexity of factors influencing self-care management is warranted.
Hypertensive study participants described unique challenges across studies we examined. However, some patterns emerged. We found that motivation to avoid the progress of hypertension, having discussion partners, and various health activities conducted by health centers were facilitating factors in the practice of self-care management. Others have reported that the motivation to avoid the progress of hypertension increases when patients have sufficient knowledge of the disease process. Knowledge of hypertension was positively related to self-care management of hypertension.81,82 By sharing with others, patients have a chance to exchange information, share their problems and increase their willingness to manage their hypertension.81,83,84 Therefore, assessing knowledge of hypertension, ensuring the availability of partner to support hypertension management, and creative program offered by community health centers are important to consider in future research.
Another consideration of self-care management for hypertensive patients in SEA countries is family structure, where most are extended families.85,86 People living under the same roof will affect self-care management as indicated in our findings. Lack of family support is one of the inhibiting factors in implementing high-quality dietary intake. In one study, low family support also correlated with the low score of hypertension self-care among hypertensive patients.87 Therefore, involving family while working with hypertensive patients to strengthen their self-care management need to be considered in future research.
We identified some cultural aspects as inhibiting factors to implement self-care practice as in Figure 2. Food intake in SEA countries is still closely affected by the culture in terms of salty, oily, and cooked with coconut milk.81 Things that should be reduced in self-care management. Approach that aptly adopts culture could increase the successfulness of intervention.14
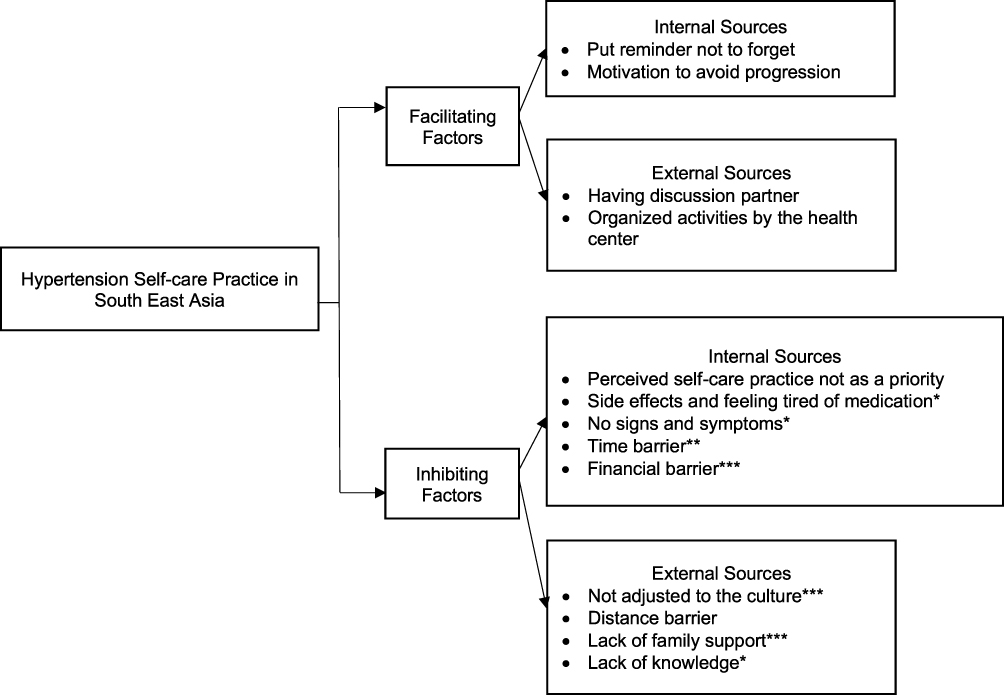 |
Figure 2 The framework of hypertension self-care practices inhibiting and facilitating factors in South East Asia. *Factors of not adhering to medication. **Factors of poor physical exercise. ***Factors of overweight/obese and poor/low-quality dietary intake. |
Another inhibiting factor is the financial status of the individual and family. Insufficient response of health-care systems in low-income/middle-income countries in many SEA nations left the burden of medical cost to the patients,88 including the patient with chronic diseases such as hypertension who need lifelong treatment. The cost of medication was a major reason for non-compliance in self-care management.89,90
Better understanding of the particular issues confronting hypertensive individuals will allow for a better-adjusted response to address the need of particular patients and for particular environments and contexts.95 Personalized approaches that consider both personal attributes and external circumstances in self-management of hypertensive populations were found to be important in this scoping review and should be rigorously studied in future research. Nurses working in the community have an important role to help manage the self-care practice and should consider individual and cultural aspect in helping hypertensive patients to manage their self-care. In addition, health service agencies must consider issues of access and cost of hypertension treatment which is prevalent among the adult populations of SEA and requires lifetime treatment.
The limitations of the review are only English and Bahasa material were included in the analysis.
Conclusions
Our review is the first to explore hypertension self-care management in SEA countries in naturalistic setting. Our findings indicate a high prevalence of obesity, low physical exercise, poor quality dietary intake and poor adherence to prescribed medications in many of the studies reviewed. Use of herbals as the anti-hypertensive medication is also identified in some of the reviewed studies. Our review indicates a range of challenges for individuals in practicing hypertensive self-care. Further prospective research on the challenges to self-care management of hypertension needs to be done to better understand individual and contextual influences. Personalized approaches to manage these challenges will require rigorous study.
Acknowledgments
The authors would like to express appreciation for UMCN librarians: Gurpreet Rana, MLIS and Kate Saylor, MSI to introduce Rayyan software and data searching.
Funding
This work was supported by the HHS, NIH/Fogarty International Center, 2D43 TW009883 D43 Post-Doctoral Program, School of Nursing, University of Michigan, USA.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Hypertension; 2021. Available from: https://www.who.int/health-topics/hypertension#tab=tab_1.
2. American College of Cardiology. New ACC/AHA high blood pressure guidelines lower definition of hypertension. ACC News Story; 2017.
3. Olsen MH, Angell SY, Asma S, et al. A call to action and a lifecourse strategy to address the global burden of raised blood pressure on current and future generations: the Lancet Commission on hypertension. Lancet. 2016;388:10060. doi:10.1016/S0140-6736(16)31134-5
4. Irwan AM, Kato M, Kitaoka K, Ueno E, Tsujiguchi H, Shogenji M. Development of the salt-reduction and efficacy-maintenance program in Indonesia. Nurs Health Sci. 2016;18(4):519–532. doi:10.1111/nhs.12305
5. James PA, Oparil S, Carter BL, et al. 2014 Evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). J Am Med Assoc. 2014;311(5):507–520. doi:10.1001/jama.2013.284427
6. Weber MA, Schiffrin EL, White WB, et al. Clinical Practice Guidelines for the Management of Hypertension in the Community: a Statement by the American Society of Hypertension and the International Society of Hypertension Clinical Practice Guidelines for the Management of Hypertension in the Community: a Statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens. 2014;16(1). doi:10.1111/jch.12237
7. Li R, Liang N, Bu F, Hesketh T. The effectiveness of self-management of hypertension in adults using mobile health: systematic review and meta-analysis. JMIR Mhealth Uhealth. 2020;8(3):e17776. doi:10.2196/17776
8. Ma Y, Cheng HY, Cheng L, Sit JWH. The effectiveness of electronic health interventions on blood pressure control, self-care behavioural outcomes and psychosocial well-being in patients with hypertension: a systematic review and meta-analysis. Int J Nurs Stud. 2019;92. doi:10.1016/j.ijnurstu.2018.11.007
9. Kitt J, Fox R, Tucker KL, McManus RJ. New approaches in hypertension management: a review of current and developing technologies and their potential impact on hypertension care. Curr Hypertens Rep. 2019;21(6). doi:10.1007/s11906-019-0949-4
10. Noncommunicable diseases country profiles 2018. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO.
11. Nawi AM, Mohammad Z, Jetly K, et al. The prevalence and risk factors of hypertension among the urban population in southeast Asian countries: a systematic review and meta-analysis. Int J Hypertens. 2021;2021. doi:10.1155/2021/6657003
12. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
13. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
14. NIH. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; 2003.
15. Niriayo YL, Ibrahim S, Kassa TD, et al. Practice and predictors of self-care behaviors among ambulatory patients with hypertension in Ethiopia. PLoS One. 2018;14(6). doi:10.1371/journal.pone.0218947
16. Motlagh SFZ, Chaman R, Sadeghi E, Ali Eslami A. Self-care behaviors and related factors in hypertensive patients. Iran Red Crescent Med J. 2016;18(6). doi:10.5812/ircmj.35805
17. Joanna Briggs Institute. JBI Manual for Evidence Synthesis. JBI; 2020.
18. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1). doi:10.1186/s13643-016-0384-4
19. Braun V, Clarke V. Thematic analysis. In: APA Handbook of Research Methods in Psychology, Vol 2: Research Designs: Quantitative, Qualitative, Neuropsychological, and Biological. 2012. doi:10.1037/13620-004
20. Sulastri D, Elmatris, Ramadhani R. Hubungan obesitas dengan kejadian hipertensi pada masyarakat etnik Minangkabau di kota Padang [The relationship between obesity and hypertension incidence among Minangkabau Ethnic in Padang city]. Majalah Kedokteran Andalas. 2012;36(2):188–201. doi:10.22338/mka.v36.i2.p188-201.2012
21. Herwati SW. Terkontrolnya tekanan darah penderita hipertensi berdasarkan pola diet dan kebiasaan olahraga di Padang tahun 2011 [Controlled blood pressure among hypertensive patients based on diet pattern and physical exercise habit in Padang 2011]. J Kesehatan Masyarakat. 2013;8(1):45.
22. Santoso NK, Thongpat S, Wattanakul B. Predictors of physical activity in older people with hypertension, Bantul, Indonesia. J Health Res. 2015;29. DOI:10.14456/jhr.2015.43.
23. Adriaansz PN, Rottie J, Lolong J, Studi P, Keperawatan I, Kedokteran F. Hubungan konsumsi makanan dengan kejadian hipertensi pada lansia di puskesmas ranomuut Kota Manado [The relationship between meal consumption and hypertension incidence among older people at ranomuut public health centre Manado city]. J Keperawat. 2016;4(1).
24. Nurdiantami Y, Watanabe K, Tanaka E, Pradono J, Anme T. Association of general and central obesity with hypertension. Clin Nutr. 2018;37(4):1259–1263. doi:10.1016/j.clnu.2017.05.012
25. Diana R, Nurdin NM, Anwar F, Riyadi H, Khomsan A. risk factors of hypertension among adult in rural indonesia. J Gizi Dan Pangan. 2018;13(3):111–116. doi:10.25182/jgp.2018.13.3.111-116
26. Rahmawati R, Bajorek B. The use of traditional medicines to lower blood pressure. Australas Med J. 2018;11(3). doi:10.21767/amj.2018.3269
27. Rahmawati R, Bajorek B. Factors affecting self-reported medication adherence and hypertension knowledge: a cross-sectional study in rural villages, Yogyakarta Province, Indonesia. Chronic Illn. 2018;14(3):212–227. doi:10.1177/1742395317739092
28. Rahmawati R, Bajorek BV. Access to medicines for hypertension: a survey in rural Yogyakarta province, Indonesia. Rural Remote Health. 2018;18(3). doi:10.22605/RRH4393
29. Pertiwi GAR, Aryawangsa AAN, Prabawa IPY, et al. Factors associated with visit-to-visit variability of blood pressure in hypertensive patients at a Primary Health Care Service, Tabanan, Bali, Indonesia. Fam Med Commun Health. 2018;6(4):191–199. doi:10.15212/FMCH.2018.0124
30. Noventi I, Kartini Y. The relationship of healthy lifestyle index (HLI) to the occurrence of hypertension in mountains, coastal and urban communities. J Keperawat. 2019;8(2):140–152. doi:10.36720/nhjk.v8i2.119
31. Simanullang P. Hubungan Gaya hidup dengan kejadian hipertensi pada lansia di Puskesmas Darussalam Medan [The relationship between lifestyle and hypertension incidence among older people at Darussalam Public Health Centre Medan]. J Darma Agung. 2018;XXVI(1):522–532.
32. Lestari P, Suastika L, Widyadharma I. Relationship between medication adherence and hypertension status in public health center. Int J Med Rev Case Rep. 2019;1. DOI:10.5455/ijmrcr.medicationadherenceandhypertension-status-public-health-center.
33. Priscilia I, Sartika RAD. Effect of sleep duration on physical activity among hypertensive patients in Bogor, Indonesia. Indian J Public Health Res Dev. 2019;10(12):1740–1744. doi:10.37506/v10/i12/2019/ijphrd/192115
34. Islami DR, Tanziha I, Martianto D, Rachman PH. DASH diet quality and status of mental emotional disorder among hypertensive women in rural area. J Gizi Dan Pangan. 2019;14(3):127–134. doi:10.25182/jgp.2019.14.3.127-134
35. Pangastuti HS, Perdana M, Wati DA, Ihsanda H, Melati T, Latifah R. The difference of sodium intake, physical activities and psychological problems of patients suffering from hypertension in rural and urban area. J INJEC. 2018;3(1):71–78. doi:10.24990/injec.v3i1.196
36. Ridha A, Hanim D, Suminah S. Relationship between intake of fruits and vegetables toward hypertension among elderly in Yogyakarta. Bali Med J. 2019;8(3). doi:10.15562/bmj.v8i3.1483
37. Farapti F, Nadhiroh SR, Sayogo S, Mardiana N. Urinary and dietary sodium to potassium ratio as a useful marker for estimating blood pressure among older women in Indonesian Urban coastal areas. Med J Nutr Metab. 2017;10(2):113–122. doi:10.3233/MNM-17138
38. Adiyasa RP, Cruz BGM. The correlation between self-care behavior and the self-efficacy of hypertensive adults. J INJEC. 2020;5(1):44–50. doi:10.24990/injec.v5i1.273
39. Livana PH, Basthomi Y. Triggering factors related to hypertension in the City of Kendal, Indonesia. Arter Hypertens. 2020;24(4):181–191. doi:10.5603/AH.A2020.0024
40. Prihandana S, Laksananno GS, Mulyadi A, Self-care behavior of outpatients in controlling hypertension in Tegal City. J Appl Health Manag Technol. 2020;2(3):97–103. doi:10.31983/jahmt.v2i3.5870
41. Nugroho A. Erniastutik. determinants of hypertension incidence among middle-aged in Indonesia-A study of Indonesian family life survey 5 data. Pak J Med Health Sci. 2020;14(2):1512–1516.
42. Gusty RP, Merdawati L. Self-care behaviour practices and associated factors among adult hypertensive patient in Padang. J Keperawat. 2020;11(1):64. doi:10.22219/jk.v11i1.10281
43. Defianna SR, Santosa A, Probandari A, et al. Gender differences in prevalence and risk factors for hypertension among adult populations: a cross-sectional study in Indonesia. Int J Environ Res Public Health. 2021;18(12):6259. doi:10.3390/ijerph18126259
44. Ramli A, Ahmad NS, Paraidathathu T. Medication adherence among hypertensive patients of primary health clinics in Malaysia. Patient Prefer Adherence. 2012;6:613–622. doi:10.2147/PPA.S34704
45. Wei TM, Salihah OM. Self-management approaches among hypertensive residents in nursing homes in Malaysia. Malays Fam Physician. 2017;12(3):8–17.
46. Salim H, Lee PY, Sazlina SG, et al. The self-care profiles and its determinants among adults with hypertension in primary health care clinics in Selangor, Malaysia. PLoS One. 2019;14(11):11. doi:10.1371/journal.pone.0224649
47. Lim OW, Yong CC. The risk factors for undiagnosed and known hypertension among Malaysians. Malays J Med Sci. 2019;26(5):98–112. doi:10.21315/mjms2019.26.5.9
48. Wu Y, Tai ES, Heng D, Tan CE, Low LP, Lee J. Risk factors associated with hypertension awareness, treatment, and control in a multi-ethnic Asian population. J Hypertens. 2009;27(1):190–197. doi:10.1097/HJH.0b013e328317c8c3
49. Malhotra R, Chan A, Malhotra C, Østbye T. Prevalence, awareness, treatment and control of hypertension in the elderly population of Singapore. Hypertens Res. 2010;33(12):1223–1231. doi:10.1038/hr.2010.177
50. Son PT, Quang NN, Viet NL, et al. Prevalence, awareness, treatment and control of hypertension in Vietnamresults from a national survey. J Hum Hypertens. 2012;26(4):268–280. doi:10.1038/jhh.2011.18
51. Do HTP, Geleijnse JM, Le MB, Kok FJ, Feskens EJM. National prevalence and associated risk factors of hypertension and prehypertension among Vietnamese adults. Am J Hypertens. 2015;28(1):89–97. doi:10.1093/ajh/hpu092
52. Nguyen HT, Hoang Thi Phuong N, Tran Nguyen N, Nguyen Anh T, Nguyen Dang V. Characterizing patients with uncontrolled blood pressure at an urban hospital in Hanoi, Vietnam. Int J Hypertens. 2020;2020:1–7. doi:10.1155/2020/5710281
53. Zaw -K-K, Latt T-S, Aung -P-P, Thwin T-G, Myint T-K. Prevalence of hypertension and its associated factors in the adult population in YangonDivision, Myanmar. Asia Pac J Public Health. 2011;23(4):496–506. doi:10.1177/1010539509349147
54. Han WP, Hong SA, Tiraphat S. Factors related to medication adherence among essential hypertensive patients in tertiary hospitals in Yangon, Myanmar. J Public Health Develop. 2015;13(2).
55. Oo H, Sakunhongsophon S, Terathongkum S. Factors related to health behaviors in persons with hypertension, Myanmar. Makara J Health Res. 2018;22(3). doi:10.7454/msk.v22i3.10018
56. Haung Z, Hong SA, Tejativaddhana P, Puckpinyo A, Myint MNHA. Multiple self-care behaviors and associated factors in community-dwelling patients with hypertension in Myanmar. Nagoya J Med Sci. 2020;82(2):363–376. doi:10.18999/nagjms.82.2.363
57. Apidechkul T. Prevalence and factors associated with type 2 diabetes mellitus and hypertension among the hill tribe elderly populations in northern Thailand. BMC Public Health. 2018;18(1). doi:10.1186/s12889-018-5607-2
58. Visanuyothin S, Plianbangchang S, Somrongthong R. Appearance and potential predictors of poorly controlled hypertension at the primary care level in an urban community. J Multidiscip Healthc. 2018;11:131–138. doi:10.2147/JMDH.S156518
59. Meelab S, Bunupuradah I, Suttiruang J, et al. Prevalence and associated factors of uncontrolled blood pressure among hypertensive patients in the rural communities in the central areas in Thailand: a cross-sectional study. PLoS One. 2019;14(2):e0212572. doi:10.1371/journal.pone.0212572
60. Chotisiri L, Yamarat K, Taneepanichskul S. Exploring knowledge, attitudes, and practices toward older adults with hypertension in primary care. J Multidiscip Healthc. 2016;9:559–564. doi:10.2147/JMDH.S112368
61. Somprasong K, Apidechkul T, Kullawong N, et al. Prevalence of and factors associated with hypertension among the hill tribe population aged 35 years and over in Northern Thailand: a cross-sectional study. Am J Cardiovasc Dis. 2020;10(1):6.
62. Rusmevichientong P, Morales C, Castorena G, Sapbamrer R, Seesen M, Siviroj P. Dietary salt-related determinants of hypertension in rural Northern Thailand. Int J Environ Res Public Health. 2021;18(2):1–16. doi:10.3390/ijerph18020377
63. Pengpid S, Vonglokham M, Kounnavong S, Sychareun V, Peltzer K. The prevalence, awareness, treatment, and control of hypertension among adults: the first crosssectional national population-based survey in laos. Vasc Health Risk Manag. 2019;15:27–33. doi:10.2147/VHRM.S199178
64. Wee SYM, Salim H, Mawardi M, et al. Comparing and determining factors associated with hypertension self-care profiles of patients in two multi-ethnic Asian countries: cross-sectional studies between two study populations. BMJ Open. 2021;11(6):e044192. doi:10.1136/bmjopen-2020-044192
65. Rahmawati R, Bajorek B. Understanding untreated hypertension from patients’ point of view: a qualitative study in rural Yogyakarta province, Indonesia. Chronic Illn. 2018;14(3):228–240. doi:10.1177/1742395317718034
66. Kurnia V, Suza D, Ariani Y, Experience of barriers to hypertension management in Minangkabau ethnic group in Payakumbuh Indonesia: a phenomenological study. Belitung Nurs J. 2018;4(2):154–160. doi:10.33546/bnj.313
67. Berek PAL, Afiyanti Y. Compliance of hypertension patients in doing self-care: a grounded theory study. J Sahabat Keperawat. 2020;2(01):21–35. doi:10.32938/jsk.v2i01.448
68. Sulistyaningrum YI, Artana IW, Kio AL. Perilaku penderita hipertensi di rumah sakit X [Hypertensive patients behavior at Hospital X]. Nurs News. 2021;5:45–55.
69. Shima R, Farizah MH, Majid HA. A qualitative study on hypertensive care behavior in primary health care settings in Malaysia. Patient Prefer Adherence. 2014;8:1597–1609. doi:10.2147/PPA.S69680
70. Tan CS, Hassali MA, Neoh CF, Saleem F. A qualitative exploration of hypertensive patients’ perception towards quality use of medication and hypertension management at the community level. Pharm Pract (Granada). 2017;15(4):1074. doi:10.18549/PharmPract.2017.04.1074
71. Tan ST, Quek RYC, Haldane V, et al. The social determinants of chronic disease management: perspectives of elderly patients with hypertension from low socio-economic background in Singapore. Int J Equity Health. 2019;18(1). doi:10.1186/s12939-018-0897-7
72. Woodham NS, Taneepanichskul S, Samrongthong R, Auamkul N. Self-care management among elderly patients with hypertension and poor adherence to treatment, living in rural Thailand: a qualitative study. Pak J Public Health. 2018;8(2):84–89. doi:10.32413/pjph.v8i2.131
73. Sadang JM, Macaronsing SIP, Alawi NM, Taib NM, HK Pangandaman. Hypertension self-care management during covid-19 pandemic crisis in the meranao tribe: a phenomenological inquiry. J Keperawat Indonesia. 2021;24(2):74–81. doi:10.7454/jki.v24i2.1308
74. Mizutani M, Tashiro J, Maftuhah SH, Yulaikhah L, Carbun R. Model development of healthy-lifestyle behaviors for rural Muslim Indonesians with hypertension: a qualitative study. Nurs Health Sci. 2016;18(1):15–22. doi:10.1111/nhs.12212
75. Sutini NK, Septarini NW, Wirawan IMA, Sawitri AAS. The association between hypertension self-management and stroke event in male patients at the Badung District Hospital, Bali. Public Health Prev Med Arch. 2018;6(2):82. doi:10.15562/phpma.v6i2.14
76. Rahman ARA, Wang JG, Kwong GMY, Morales DD, Sritara P, Sukmawan R. Perception of hypertension management by patients and doctors in Asia: potential to improve blood pressure control. Asia Pac Fam Med. 2015;14(1). doi:10.1186/s12930-015-0018-3
77. Kaufman ND, Chasombat S, Tanomsingh S, Rajataramya B, Potempa K. Public health in Thailand: emerging focus on non-communicable diseases. Int J Health Plan Manag. 2011;26(3):e197–212. doi:10.1002/hpm.1078
78. Hardianto Y, Rabia R, Rijal R, Syahrul S. The physical activity level of adolescents and its correlation with the nutritional and socioeconomic status in Indonesia. Enferm Clin. 2020;30. DOI:10.1016/j.enfcli.2020.06.071.
79. Hussen FM, Adem HA, Roba HS, Mengistie B, Assefa N. Self-care practice and associated factors among hypertensive patients in public health facilities in Harar Town, Eastern Ethiopia: a cross-sectional study. SAGE Open Med. 2020;8:205031212097414. doi:10.1177/2050312120974145
80. Zinat Motlagh SF, Chaman R, Sadeghi E, Ali Eslami A. Self-care behaviors and related factors in hypertensive patients. Iran Red Crescent Med J. 2016;18(6). doi:10.5812/ircmj.35805
81. Giena VP, Thongpat S, Nitirat P. Predictors of health-promoting behaviour among older adults with hypertension in Indonesia. Int J Nurs Sci. 2018;5(2):201–205. doi:10.1016/J.IJNSS.2018.04.002
82. Zuraida E, Irwan AM, Sjattar EL. Self-management education programs for patients with heart failure: a literature review. Cent Eur J Nurs Midwifery. 2021;12(1):279–294. doi:10.15452/CEJNM.2020.11.0025
83. Yatim MH, Wong YY, Neoh CF, Lim SH, Hassali MA, Hong YH. Factors influencing patients’ hypertension self-management and sustainable self-care practices: a qualitative study. Public Health. 2019;173:5–8. doi:10.1016/J.PUHE.2019.04.020
84. Saleem F, Hassali MA, Shafie AA, Bashir S, Atif M. Perceptions of disease state management among Pakistani hypertensive patients: findings from a focus group discussion. Trop J Pharmaceut Res. 2011;10(6):833–840. doi:10.4314/tjpr.v10i6.18
85. Dommaraju P, Tan JE. Households in contemporary Southeast Asia. J Comp Fam Stud. 2014;45(4):559–580. doi:10.3138/jcfs.45.4.559
86. Yeung WJJ, Desai S, Jones GW. Families in Southeast and South Asia. Annu Rev Sociol. 2018;44(1):469–495. doi:10.1146/annurev-soc-073117-041124
87. Lee EJ, Park E. Self-care behavior and related factors in older patients with uncontrolled hypertension. Contemp Nurse. 2017;53(6):607–621. doi:10.1080/10376178.2017.1368401
88. Mannava P, Abdullah A, James C, Dodd R, Annear PL. Health systems and noncommunicable diseases in the Asia-Pacific Region: a review of the published literature. Asia Pac J Public Health. 2015;27(2):NP1–NP19. doi:10.1177/1010539513500336
89. Rahmawati R, Bajorek BV. Self-medication among people living with hypertension: a review. Fam Pract. 2017;34(2):147–153. doi:10.1093/fampra/cmw137
90. van der Laan DM, Elders PJM, Boons CCLM, Beckeringh JJ, Nijpels G, Hugtenburg JG. Factors associated with antihypertensive medication non-adherence: a systematic review. J Hum Hypertens. 2017;31(11):687–694. doi:10.1038/jhh.2017.48
91. Center for Southeast Asian Studies [homepage on the Internet]. Southeast Asian Countries - NIU - Center for Southeast Asian Studies. Available from: https://www.niu.edu/clas/cseas/resources/countries.shtml.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.