Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Screening Candidates for Conversion Therapy in Unresectable Hepatocellular Carcinoma Patients After Tyrosine Kinase Inhibitor Plus PD-1/PD-L1 Antibody Therapy: A Multicenter Retrospective Study
Authors Jin Z ![]() , Li X
, Li X ![]() , Lv L, Zhang B, Ma X, Chen S, You J, Wu X
, Lv L, Zhang B, Ma X, Chen S, You J, Wu X ![]() , Wang L, Liu X, Wang F, Chen X, Yu L, Zhang S, Zhang L
, Wang L, Liu X, Wang F, Chen X, Yu L, Zhang S, Zhang L ![]()
Received 27 February 2025
Accepted for publication 2 August 2025
Published 25 August 2025 Volume 2025:12 Pages 1921—1941
DOI https://doi.org/10.2147/JHC.S523476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Prof. Dr. Imam Waked
Zhe Jin,1,* Xueyan Li,2,* Ling Lv,3,* Bin Zhang,1 Xiao Ma,1 Siqin Chen,1 Jingjing You,1 Xuewei Wu,1 Liaoyuan Wang,1 Xin Liu,1 Fei Wang,1 Xiaoming Chen,4 Lijuan Yu,2 Shuixing Zhang,1 Lu Zhang1
1Department of Radiology, The First Affiliated Hospital of Jinan University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Nuclear Medicine, Hainan Cancer Hospital, Haikou, Hainan, People’s Republic of China; 3Department of Radiology, Guangdong Provincial Key Laboratory of Major Obstetric Diseases; Guangdong Provincial Clinical Research Center for Obstetrics and Gynecology; The Third Affiliated Hospital, Guangzhou Medical University, Guangzhou, People’s Republic of China; 4Department of Minimally Invasive Intervention, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuixing Zhang, Department of Radiology, The First Affiliated Hospital of Jinan University, No. 613 Huangpu West Road, Tianhe District, Guangzhou, Guangdong, 510627, People’s Republic of China, Tel +86 13544597585, Email [email protected] Lu Zhang, Department of Radiology, The First Affiliated Hospital of Jinan University, No. 613 Huangpu West Road, Tianhe District, Guangzhou, Guangdong, 510627, People’s Republic of China, Tel +86 020 18009032439, Email [email protected]
Background: Conversion therapies after immune checkpoint inhibitors (ICIs) plus tyrosine-kinase inhibitors (TKIs) provide curative surgery chance and prolong survival for unresectable hepatocellular carcinoma (uHCC). However, only some patients have the opportunity to receive conversion therapies. To this end, we aimed to develop and validate a machine-learning model to identify patients who may have the chance to undergo conversion therapy.
Methods: This retrospective cohort study included 443 patients with uHCC who received ICIs and TKIs from four centers. Variables were analyzed using univariate and multivariate logistic regression to identify independent indicators of conversion therapy. The Gradient Boosting Machine (GBM) algorithm was used to develop and validate model, and the Shapley additive explanation algorithm was used to mechanically explain the prediction of the model.
Results: Overall, 84 (19%) patients underwent conversion therapy, and their prognosis were significantly longer than those did not (P < 0.05). CA125 level, pre-TKI therapy, pre-antiviral therapy, lymph node metastasis status, and number of intrahepatic lesions were identified as indicators of conversion therapy. The GBM-based combined model outperformed the BCLC classification (P < 0.05), yielding an AUC of 0.76 and 0.74 in the training and external validation cohorts, respectively. Survival analyses indicated that patients who underwent surgery as conversion therapy had a better prognosis than those who underwent ablation therapy (P < 0.05).
Conclusion: The GBM-based combined model could identify patients who may benefit from conversion therapy for uHCC treated with ICIs and TKIs. Surgical resection as curative conversion therapy may provide better survival benefits than ablation therapy.
Plain Language Summary: Combining tyrosine kinase inhibitors (TKIs) with anti-programmed cell death protein 1/programmed cell death ligand 1 (anti-PD-1/PD-L1) antibodies has significantly improved treatment outcomes for patients with unresectable hepatocellular carcinoma (uHCC). Consequently, some patients may become eligible for curative conversion. However, identifying patients suitable for curative conversion therapy remains a critical challenge. This study identifies validated clinical predictors and develops an interpretable machine learning model for the potential of conversion therapy following TKI and anti-PD-1/PD-L1 combination therapy. Additionally, it provides a comparative analysis of the survival benefits associated with different conversion therapy regimens. These findings may offer preliminary insights that could inform clinical consideration for uHCC patients.
Keywords: hepatocellular carcinoma, immune checkpoint inhibitor, tyrosine kinase inhibitor, curative conversion therapy, machine learning
Introduction
Liver cancer is the third leading cause of cancer-related deaths globally, with hepatocellular carcinoma (HCC) accounting for over 90% of cases.1,2 HCC often presents with subtle symptoms and approximately 80% of patients are diagnosed at an unresectable stage (uHCC).3–5 This is due to insufficient functional liver reserve, anatomical limitations for primary tumor resection, distant metastasis, or vascular invasion, rendering them ineligible for curative conversion treatments such as surgery, ablation, and transplantation.6
Systemic therapy has become the primary treatment modality for uHCC and has advanced rapidly in recent years.7 In particular, the combination of tyrosine kinase inhibitors (TKIs) and anti-programmed cell death protein 1/programmed cell death ligand 1 (anti-PD-1/PD-L1) antibodies has shown encouraging objective response rates (ORR). The latest Phase III clinical trials have demonstrated promising results: the IMbrave150 trial8 showed an ORR of 44% for intermediate-stage HCC and 27% for advanced-stage HCC with the combination of Atezolizumab and Bevacizumab; the SHR-1210-III-310 trial9,10 reported an ORR of 25% with the combination of Camrelizumab and Rivoceranib; and the LEAP-002 trial11 achieved an ORR of 26.10% with the combination of Lenvatinib and Pembrolizumab. Furthermore, real-world clinical practice has shown an ORR of 33.30% for uHCC patients treated with Lenvatinib in combination with various anti-PD-1/PD-L1 antibodies, highlighting the potential synergistic effects of these combination therapies.12
In traditional systemic therapy, if the drug regimen can achieve disease stabilization or better, treatment should be continued, especially when a partial response (PR) is achieved.13,14 The newly proposed conversion therapy, which applies intervention measures such as local regional or systemic therapy, has enabled patients with unresectable malignant tumors to be downstaged and receive a curative conversion therapy regimen, achieving a cancer-free and drug-free state.15 The combination of TKIs and anti-PD-1/PD-L1 antibodies has shown good efficacy in treating uHCC, and further curative conversion therapy has improved the overall survival (OS) of patients. A recently proposed strategy is curative conversion therapy using atezolizumab and bevacizumab, where after achieving significant tumor shrinkage with the combination of atezolizumab and bevacizumab, curative treatments such as resection, radiofrequency ablation, or super-selective TACE are performed.14,16,17 These studies showed 35–66.70% complete response (CR) rate with the curative conversion approach. Therefore, even if sufficient drug efficacy is achieved, the possibility of curative conversion after combination therapy should not be overlooked.
In the past, conversion therapies mainly relied on local treatments such as transarterial chemoembolization, hepatic arterial infusion chemotherapy, and stereotactic radiotherapy, resulting in conversion resection rates of only 9% to 20%.18–20 With the advancements in systemic therapies, conversion resection rates have increased from 15.9% to 51%.18 Importantly, the combination of local and systemic therapies is a promising strategy. This combined approach, which utilizes different antitumor mechanisms, can achieve better tumor responses and higher conversion rates. However, not all uHCC patients receiving combined TKI and anti-PD-1/PD-L1 antibody therapy qualify for conversion therapy, as excessive treatment may compromise liver function and adversely affect prognosis. Consequently, a thorough evaluation of tumor characteristics and hepatic functional reserve is essential to identify optimal candidates for conversion therapy in a timely manner. Previous studies have identified several predictive factors associated with successful conversion therapy, including Eastern Cooperative Oncology Group Performance Status (ECOG PS), intrahepatic tumor burden, radiographic response to systemic therapy, modified ALBI grade (mALBI), and Barcelona Clinic Liver Cancer (BCLC) stage.21,22 Nevertheless, these previous studies have not yet established a validated tool to screen suitable candidates effectively for conversion therapy—the target that our study aims to address. By developing such a tool, we can maximize conversion rates and improve patient outcomes.
This study aimed to identify the predictive factors associated with curative conversion therapy after TKIs plus anti-PD-1/PD-L1 antibody therapy in patients with uHCC. Based on these factors, further study was designed to develop and validate a pre-treatment predictive model to estimate the likelihood of patients achieving curative resection. This model could serve as a screening tool for identifying patients with uHCC who are suitable candidates for curative conversion therapy, providing valuable guidance for clinical decision-making and optimizing treatment strategies.
Materials and Methods
Patients
This retrospective study included patients with uHCC who received TKIs combined with anti-PD-1/PD-L1 antibody therapy at four hospitals between March 2017 and April 2023. The diagnosis of HCC was based on biopsy or dynamic imaging (computed tomography [CT] or magnetic resonance imaging [MRI]) of the tumor tissue.23,24 The inclusion criteria were as follows: 1) age > 18 years; 2) BCLC stage B or C; 3) the presence of at least one measurable diameter and arterially enhancing target lesion according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST). Patients were excluded if they had 1) Child-Pugh C liver function or evidence of liver decompensation, including refractory ascites, esophageal/gastric variceal bleeding, or hepatic encephalopathy; 2) ECOG PS > 1; 3) Incomplete follow-up data; or 4) Synchronous malignancies detected via imaging (CT/MRI) or biopsy within ± 6 months of the initial primary cancer diagnosis. In accordance with the Declaration of Helsinki, this study was approved by the Institutional Ethics Committee of each participating institution, and informed consent was waived by the Institutional Review Board due to the retrospective of our study.
Before initiating treatment administration, all patients underwent medical history recording, physical examination, and blood profiling. These included blood tests, liver and kidney function, coagulation function, hepatitis B virus (HBV), hepatitis C virus (HCV), HBV DNA, tumor markers, and radiological examinations (e.g., contrast-enhanced abdominal CT/MRI). In addition, imaging features based on CT/MRI were analyzed, including the intratumoral artery, intratumoral bleeding, tumoral capsule, peritumoral enhancement, and irregular edges. Missing data were handled using multiple imputation method, which generate multiple plausible values for each missing datum to account for the inherent uncertainty.
TKI Plus Anti-PD-1/PD-L1 Antibodies Therapy Regimens
This study utilized various oral TKIs, including Lenvatinib (8 mg/day regardless of body weight), Apatinib (250 mg/day), Sorafenib (800 mg/day) and Bevacizumab (15 mg/kg q3w). The anti-PD-1/PD-L1 antibodies include Sintilimab (200 mg q3w), Nivolumab (3 mg/kg q2w), Tislelizumab (200 mg q3w), Pembrolizumab (200 mg q3w), Camrelizumab (200 mg q2w), Toripalimab (240 mg q3w) and Atezolizumab (1200 mg q3w). Due to the favorable initial efficacy and safety outcomes observed in prior research on combination therapy involving Lenvatinib, it emerged as the preferred TKI option. The selection of the suitable drug combination for each patient was determined through consultations between the clinicians and patients, considering recent efficacy and safety data, treatment cycles, and financial considerations. The dosages of different medications varied.
To manage adverse events, dose adjustments or discontinuation were permitted. Oral antiviral drugs (such as entecavir or tenofovir) were administered to untreated HBV infected individuals and maintained throughout the entirety of their anticancer regimen. Systemic therapy was interrupted upon tumor progression, unacceptable toxicity, or curative-intent liver resection.
Follow Up
Tumor assessment was performed every 4–8 weeks, with contrast-enhanced abdominal CT /MRI to evaluate hepatic lesions and chest CT to assess pulmonary metastases. Tumor response was evaluated according to the mRECIST. The patient’s liver function, treatment-related adverse events, and potential for resection were evaluated based on clinical and laboratory data. Additionally, the ORR (CR and PR) and DCR (CR, PR, and stable disease [SD]) were calculated.
Curative Conversion Therapy
Conversion therapy was defined as systemic treatment that resulted in tumor shrinkage, and all remaining lesions could be treated with additional local curative treatments such as surgical resection or ablation therapy.25 Physicians independently decided to implement conversion therapy when they determined that curative treatment was feasible using additional local curative therapies. All conversion therapies were performed within 1–3 months after the optimal treatment effect was determined. Conversion eligibility was determined by multidisciplinary team consensus based on: (1) radiologic response (mRECIST), (2) liver function reserve (Child-Pugh A), and (3) anatomic resectability criteria (future liver remnant ≥30%).
A cancer-free state was defined as the absence of HCC on imaging examinations for at least 6 months during the observation period after conversion therapy. Patients who underwent curative resection or received curative local-regional treatment were eligible to discontinue treatment if they met the following criteria: (1) achieved CR according to mRECIST through curative-intent surgery or ablation, (2) maintained normalized levels of the three tumor markers for ≥6 months, and (3) contrast-enhanced CT or MRI showed no viable tumor lesions.
Identifying Independent Predictors of Conversion Therapy
Univariate and multivariate logistic regression analyses were performed to identify the independent predictors associated with downstaging following TKI plus anti-PD-1/PD-L1 antibody combination therapy in patients with uHCC. Before the multivariate logistic regression analyses, a correlation analysis was conducted to identify and remove highly correlated variables and mitigate multicollinearity. Factors achieving significance at the 0.05 level in the multivariable model were considered independent predictors for curative conversion therapy and used to build a predictive model.
To examine the relationships between the identified predictors and pathological characteristics of patients with HCC, we performed a correlation analysis and visualized the results using a correlation heatmap. Since all variables included in the correlation analysis were categorical, Kendall’s tau correlation coefficients were calculated to assess the pairwise relationships between these variables. The correlation coefficients were then displayed in a heatmap format, where the color intensity and size of the circles represent the strength of the correlation. Positive correlations are shown in blue, while negative correlations are shown in red. A heatmap was generated using the “corrplot” package (version 0.8.4) in R.
Development of Predictive Model
Based on the remaining factors and BCLC stage, models were constructed to predict the likelihood of uHCC patients receiving curative conversion therapy following combination therapy by using the Gradient Boosting Machine (GBM) algorithm with a five-fold cross-validation grid search method. The models were tested using an independent validation cohort. The predictive performance of the models was evaluated using receiver operating characteristic (ROC) curves, the area under the curve (AUC), accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). The 95% confidence intervals (CIs) were calculated using bootstrapping to estimate variability. Pairwise comparisons of the AUCs were conducted using the DeLong test for each model pair. Net Reclassification Improvement (NRI) and Integrated Discrimination Improvement (IDI) were used to compare model performance, with NRI evaluating threshold-dependent reclassification accuracy and IDI assessing global probability discrimination improvement. Calibration curve was plotted to assess the calibration of the model. Decision curve analysis was conducted to evaluate the clinical utility of the models in an independent validation cohort. This analysis quantifies the net benefit of using models at various threshold probabilities. The model was generated and evaluated using the R package “regplot” (version 1.1), “pROC” (version 1.18.5), “rms” (version 6.7.1), and “Resource Selection” (version 0.3.6).
To address the “black-box” nature of our model, we use the SHapley Additive exPlanations (SHAP) algorithm for interpretability. We used the tree-based SHAP algorithm from the Python “shap” package developed by Lundberg. SHAP features were ranked according to their average absolute Shapley values. A summary plot visualizes the feature importance and effects, with each point representing a feature’s SHAP value for a specific individual. To further illustrate the model outputs, we generated SHAP force plots for representative cases from the external validation dataset. These plots depict the impact of each feature on the predicted probability of curative conversion therapy, with red arrows indicating increases and blue arrows indicating decreases relative to baseline.
Survival Subgroup Analysis
Before delving into a comparison of prognostic variations among different curative conversion therapy regimens, propensity score matching (PSM) was conducted to mitigate potential biases in patient selection. For the propensity score-matched cohorts, the propensity score matching criteria were adjusted based on lymph node metastasis (LNM), alpha-fetoprotein (AFP), TKI therapy before combination therapy (pre-TKI therapy), receiving perfusion therapy before combination therapy (pre-perfusion therapy), Child-Pugh stage, and HBV. PSM was performed using the R package “MatchIt” (version 4.5.5), with caliper=0.03.
Statistical Analysis
Quantitative variables were reported as mean ± standard deviation or median and interquartile range (IQR) and were compared using Student’s t-test or the nonparametric Mann–Whitney U-test, as appropriate. Categorical variables were described as counts with percentages and compared using the chi-square test or Fisher’s exact test, as appropriate. The effects of different TKIs and anti-PD-1/PD-L1 antibodies on patient downstaging outcomes were analyzed using logistic regression. The endpoints were OS and 3-year progression-free survival (PFS). OS was defined as the time interval between the initial combination therapy and all-cause death. Patients who survived until the last follow-up date or were lost to follow-up were censored. The 3-year PFS was defined as the time from the initial combination therapy to disease progression or death from any cause, or the end of 36 months, whichever occurred earlier. Survival analysis was performed using the Kaplan-Meier method and compared using the Log rank test. Survival analysis and survival curves were accomplished using the R package “survminer” (version 0.4.9) and “survival” (version 3.8.3). The statistical significance of the correlations was determined using two-tailed t-tests, and p-values less than 0.05 were considered statistically significant. All statistical analyses were performed using R version 4.3.3.
Results
A total of 443 consecutive uHCC patients who received TKIs plus anti-PD-1/PD-L1 antibody therapy at four hospitals in China were included (Table 1 and Supplementary Figure 1), of which 84 (19.00%) patients underwent curative resection after the combination therapy. The mean age of all patient was 53.89 ± 12.07 years (range, 24–86 years). Most patients were male (88.94%), had HBV infection (92.55%), but the majority had HBV-DNA < 2000 copies/mL (69.98%), had cirrhosis (71.56%), and were classified as Child-Pugh A (74.94%). In this study, 28.89% and 71.11% of patients were diagnosed with BCLC stage B and C HCC, respectively. For the imaging features, most patients had intratumoral artery (77.88%) and irregular margin (60.05%). Most patients received lenvatinib treatment (85.1%), of which 29% received Camrelizumab, 28.70% received sorafenib, and 28.70% received Tislelizumab. However, there were no statistically significant differences in PFS and OS among the various drug and drug combination subgroups, except for lenvatinib plus toripalimab group (n=10, P = 0.01; Figure 1). Additionally, 181 patients received TKIs plus anti-PD-1/PD-L1 antibody, concurrent local therapies (including TACE, perfusion therapy, or radiotherapy) were administered, with 51 patients undergoing curative conversion therapy following the combination therapy (Table 1). Survival analysis revealed no statistically significant differences in progression-free survival (PFS) or overall survival (OS) between the combined local therapy group and the non-combined therapy group (P > 0.05).
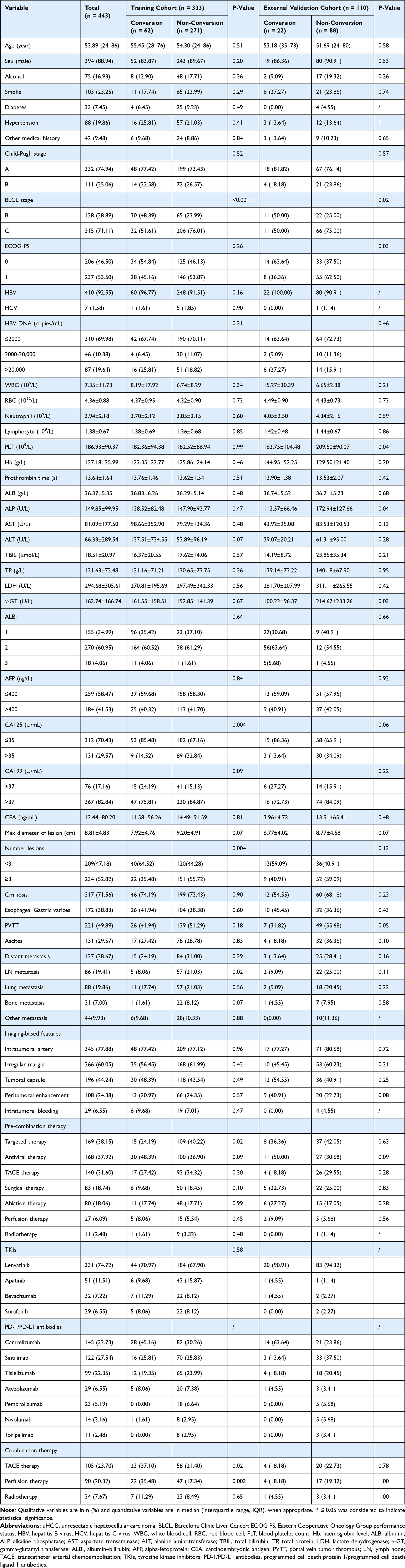 |
Table 1 Baseline Characteristics of uHCC Patients in the Training and External Validation Cohorts |
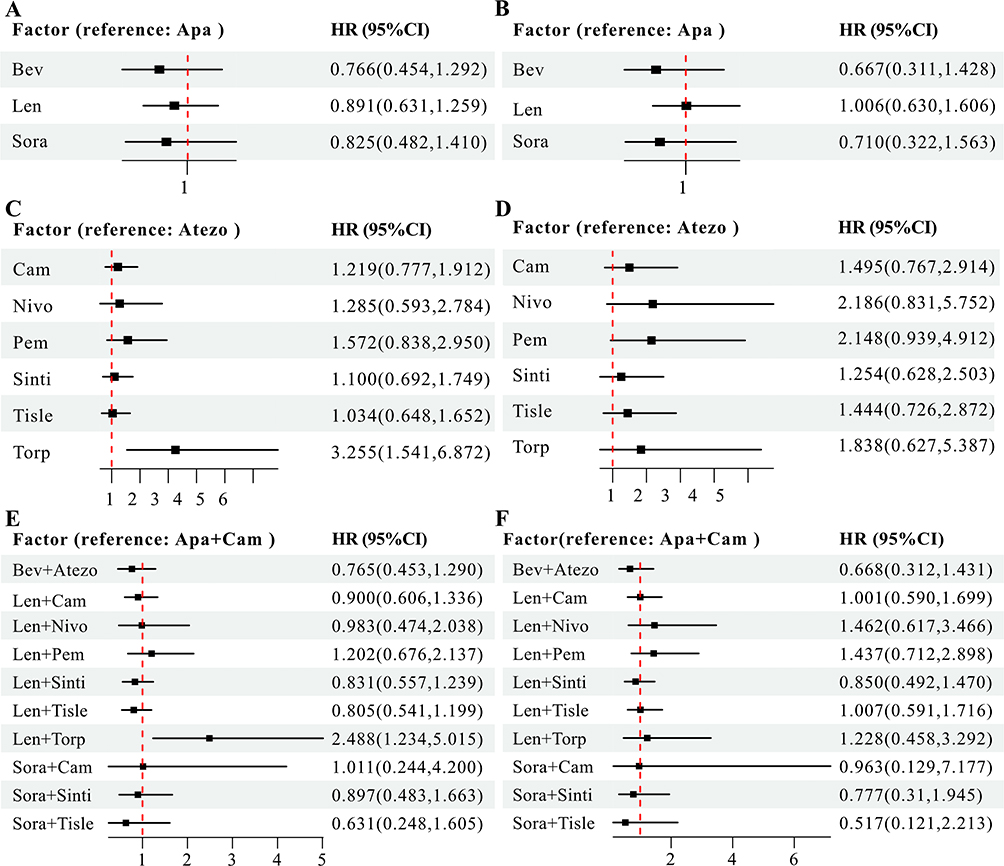 |
Figure 1 Subgroup analysis in Progression-free survival (PFS) and overall survival (OS) subgroups among the various drug or drug combination subgroups. (A and B) Forest plot of PFS and OS among the various tyrosine kinase inhibitors (TKIs). (C and D) Forest plot of PFS and OS among the various anti-PD-1/PD-L1 antibodies. (E and F) Forest plot of PFS and OS among the various TKIs plus anti-PD-1/PD-L1 antibodies. Abbreviations: Apa, Apatinib; Bev, Bevacizumab; Len, Lenvatinib; Sora, Sorafenib; Cam, Camrelizumab; Nivo, Nivolumab; Pem, Pembrolizumab; Sinti, Sintilimab; Tisle, Tislelizumab; Torp, Toripalimab; Atezo, Atezolizumab. |
Tumor Response and Outcome
In the first treatment assessment, 29 patients (6.55%) who received TKIs plus anti-PD-1/PD-L1 antibody therapy achieved a CR, and 120 patients (27.09%) achieved a PR, resulting in an ORR of 33.63% (149/443). Additionally, 174 patients (39.28%) achieved stable disease (SD), resulting in a DCR of 72.91% (323/443). The detailed tumor response data is presented in Table 2. Notably, among the 84 patients who underwent curative conversion therapy, the initial tumor response after combination therapy was as follows: 8 patients (9.52%) achieved a CR, 36 patients (42.86%) achieved a PR, 21 patients (25%) had SD, 19 patients (22.62%) had progressive disease (PD).
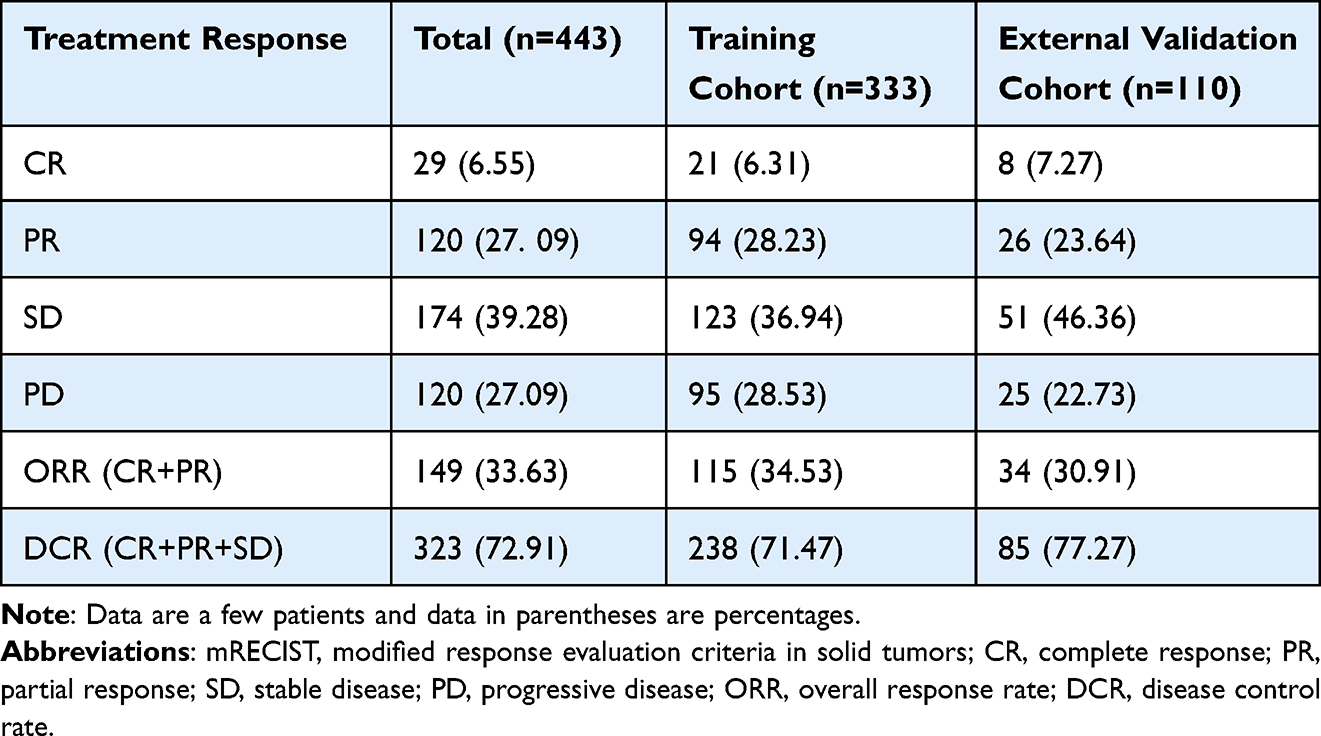 |
Table 2 Radiological Response According to mRECIST Criteria in the Training and External Validation Cohorts |
At the data cut-off, 186 (41.99%) patients died. The median progression-free survival (PFS) and OS for all patients was 6.0 months (range, 0.50–47.20 months) and 14.0 months (range, 1.10–60.00 months), respectively. Patients who underwent curative conversion therapy had longer PFS as well as OS compared to those who did not (median PFS: 13.4 [95% CI: 5.4–21.3] vs 6.13 months [95% CI: 5.3–7.0], P < 0.001, Figure 2A; median OS: 42.2 [95% CI: 29.5–54.9] vs 25.5 months [95% CI: 19.0–31.2], P = 0.001, Figure 2B).
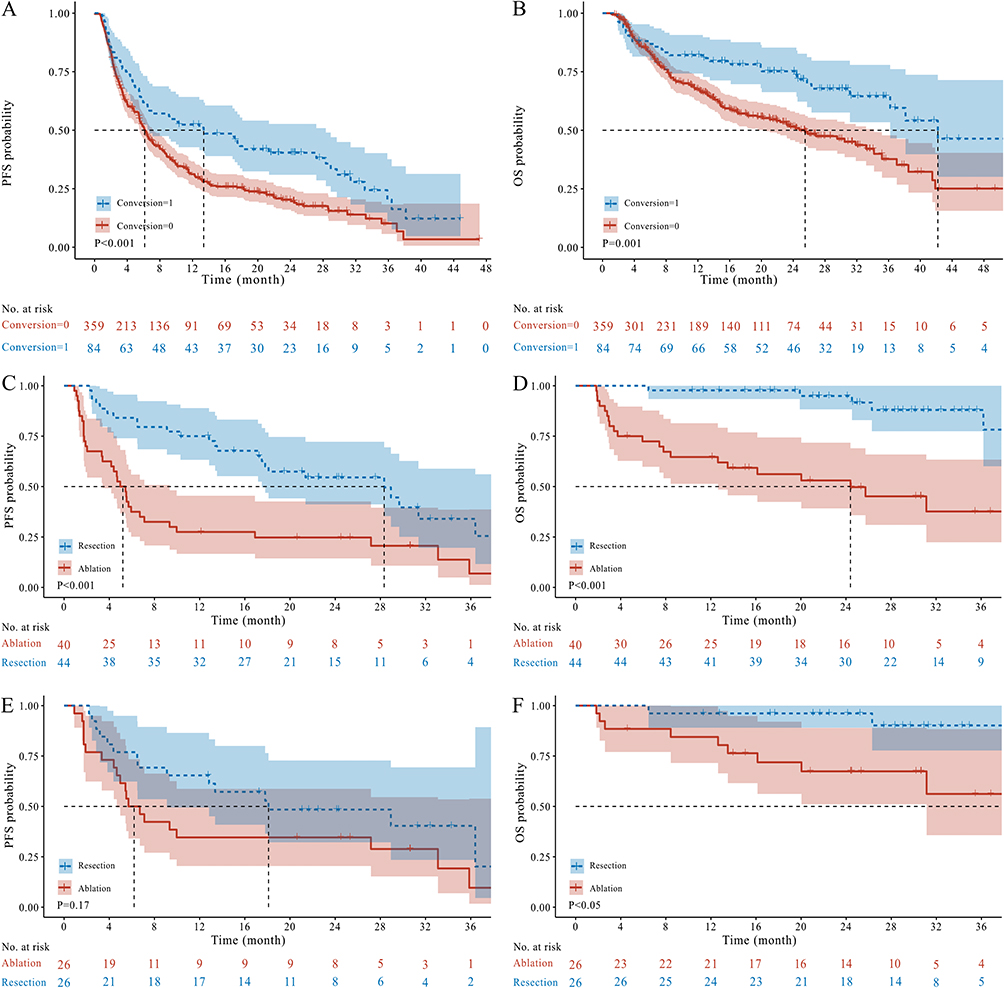 |
Figure 2 Kaplan-Meier estimates of progression-free survival (PFS) and overall survival (OS). (A and B) Survival analysis between with curative conversion therapy and without curative conversion therapy; (C and D) Survival analysis between two curative conversion therapy strategies (resection and ablation therapies); (E and F) After propensity score matching, survival analysis between two curative conversion therapy strategies (resection and ablation therapies). |
Treatment-related adverse events (TRAEs) associated with TKIs plus anti-PD-1/PD-L1 antibody therapy and conversion therapy are detailed in Table 3. Overall, 229 patients (51.7%) experienced TRAEs, with 16 of these patients undergoing conversion therapy. The most common TRAEs observed were liver dysfunction (n=107), decreased lymphocyte count (n=54), and decreased hemoglobin count (n=52). Twenty-five patients (5.6%) experienced grade 3–4 TRAEs, including 1 patient receiving conversion therapy. The most frequent grade 3–4 TRAEs were liver dysfunction (n=8), myelosuppression (n=3), and cardiac function injuries (n=3). All TRAEs were evaluated to be mild and manageable during the follow-up period.
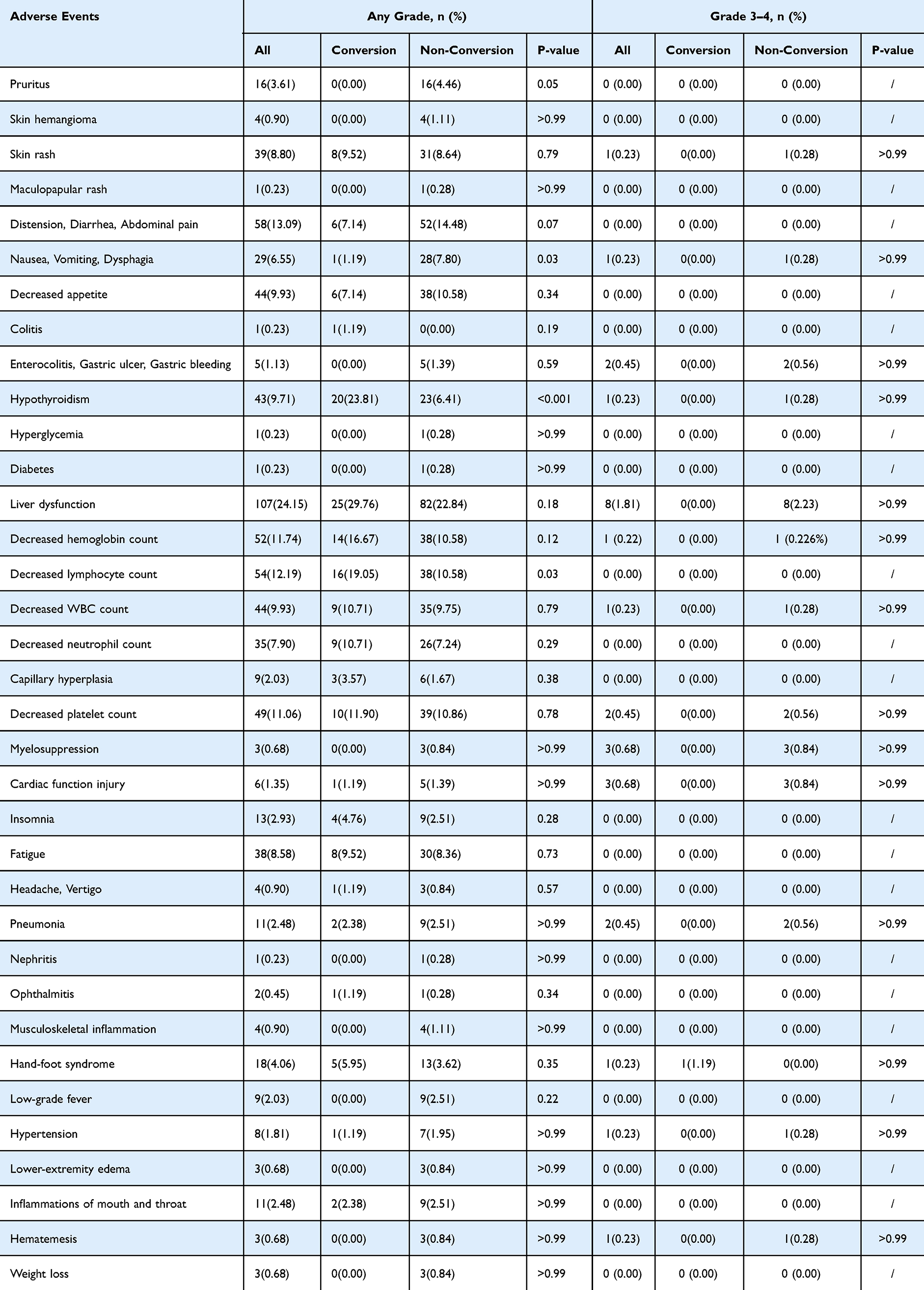 |
Table 3 Adverse Events |
Predictors for Curative Conversion Therapy
According to multivariate logistic regression analysis, CA125, pre-TKI therapy, antiviral therapy before combination therapy (pre-antiviral therapy), LNM, and number of intrahepatic lesions were identified as independent predictors for curative conversion therapy following combination therapy (all P < 0.05), as shown in Table 4. Only the pre-antiviral therapy showed a positive association with curative conversion therapy (OR 1.9 [95% CI: 1.0–3.5]; P < 0.05), whereas the others displayed negative correlations.
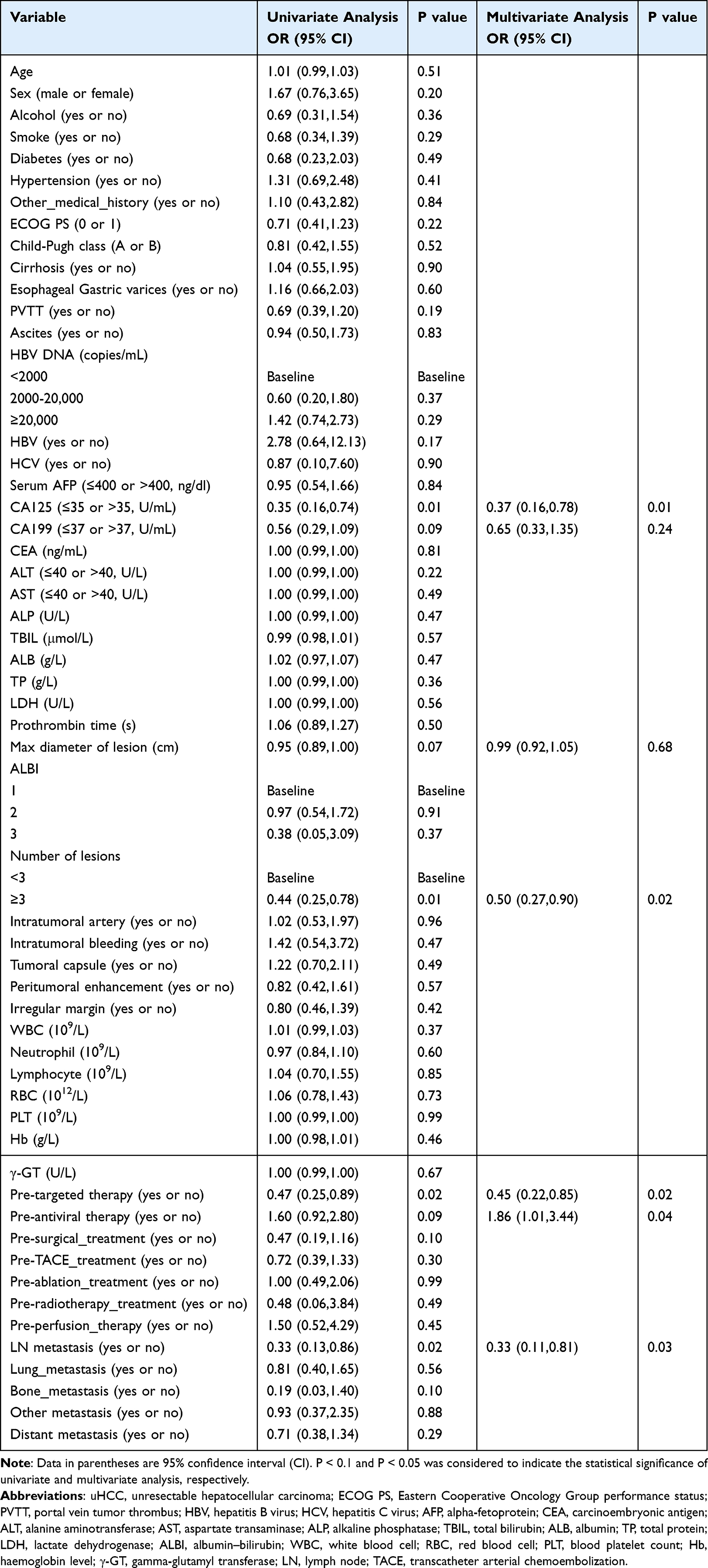 |
Table 4 Risk Factors Associated with the Conversion Therapy in Patients with uHCC |
The correlation heatmap (Figure 3) illustrates the pairwise relationships between the identified predictors and pathological characteristics of patients with uHCC. Pre-TKI therapy showed a strong negative correlation with hepatocyte (r = −0.29, P < 0.001), CD34 (r = −0.40, P < 0.001), AFP (r = −0.24, P < 0.01), and Arginase (r = −0.41, P < 0.001). Pre-antiviral therapy showed a strong negative correlation with the adjacent to the liver capsule (r = −0.0.32, P < 0.001), break through the liver capsule (r = −0.48, P < 0.001), chronic inflammatory changes in non-tumor liver tissue (r = −0.53, P < 0.001), and satellite nodules (r = −0.50, P < 0.001). Additionally, MVI was negatively correlated with pre-antiviral therapy (r = −0.22, P < 0.05) and positively correlated with LNM (r = 0.19, P < 0.05).
 |
Figure 3 Heatmap illustrating the correlation between identified predictors and pathological characteristics of HCC patients. Statistical significance is indicated by stars: *** (P < 0.001), ** (P < 0.01), * (P < 0.05). Blue hues represent positive correlations, while red hues indicate negative correlations. The intensity of the color (from light to dark) reflects the strength of the correlation, with darker shades signifying stronger positive or negative relationships between the variables. Abbreviations: LNM, lymph node metastasis; pre-TKI therapy, TKI therapy before combination therapy; pre-antiviral therapy, antiviral therapy before combination therapy. |
After PSM analysis, 52 matched patients were included to compare survival outcomes between two curative conversion therapy strategies: surgical resection and ablation therapies. The baseline characteristics of these cohorts are presented in Supplementary Table 1. Details regarding the balance of the PSM data are provided in Supplementary Table 2. The results indicated that regardless of whether PSM was applied, resection therapy resulted in significantly better PFS and OS than ablation therapy (P < 0.05, Figure 2C, D, and F). However, the difference in PFS was not statistically significant after PSM (P = 0.17, Figure 2E).
Predictive Model Construction and Validation
Correlation analysis revealed a correlation coefficient greater than 0.3 between the BCLC stage and both LNM and maximum lesion diameter (Supplementary Figure 2), and then the BCLC stage was removed prior to the multivariate analysis. However, because the GBM algorithm employed can handle both linear and nonlinear relationships, the presence of collinearity among these features did not impede model construction. Furthermore, previous studies have demonstrated a significant association between BCLC stage and the likelihood of achieving curative conversion therapy. As a result, a logistic regression model based on the BCLC stage, a GBM model on the five remaining variables, a GBM-based combined model integrating the BCLC stage, and five independent predictors were constructed in the training cohort. The GBM model yielded an AUC, accuracy, sensitivity, and specificity of 0.75 (95% CI: 0.69–0.82), 69.7% (95% CI: 64.6–74.8), 66.1% (95% CI: 54.8–77.4), 70.5% (95% CI: 64.9–76) in the training cohort, and 0.71 (95% CI: 0.60–0.83), 68.2% (95% CI: 60–76.4), 54.5% (95% CI: 36.4–77.3), and 71.6% (95% CI: 61.4–80.7) in the external validation cohort, respectively. Then, the GBM-based combined model yielded an AUC, accuracy, sensitivity, and specificity of 0.76 (95% CI: 0.70–0.83), 71.8% (95% CI: 67.30–76.6), 62.9% (95% CI: 50.0–74.2), and 73.8% (95% CI: 68.6–79.0) in the training cohort, respectively. In the external validation cohort, the GBM-based combined model yielded an AUC, accuracy, sensitivity, and specificity of 0.74 [95% CI: 0.64–0.85], 72.7% (95% CI: 64.5–80.9), 59.1% (95% CI: 36.4–81.8), and 76.1% (95% CI: 67.0–85.2), respectively. The detailed results are presented in Table 5, Supplementary Figure 3, and Supplementary Figure 4. The GBM-based combined model outperformed BCLC stage in both the training (P < 0.05; Figure 4A and Table 5) and validation cohorts (P < 0.05; Figure 4B and Table 5). The combined model demonstrated significant improvements over the BCLC stage in both discrimination and reclassification accuracy. The IDI was 8.8% (95% CI: 5.9–11.8; P < 0.001), indicating an 8.8% average increase in predicted probabilities for events (Supplementary Table 3). The NRI reached 13% (95% CI: 1.2–22.1; P < 0.05), with 13% more high-likelihood cases correctly reclassified (Supplementary Table 4). The combined model achieves superior calibration to BCLC stage predictions, with close agreement between predicted and observed conversion therapy incidence (Figure 4C). The decision curve analysis results further demonstrated that our combined model provides greater clinical utility than the BCLC stage (Figure 4D).
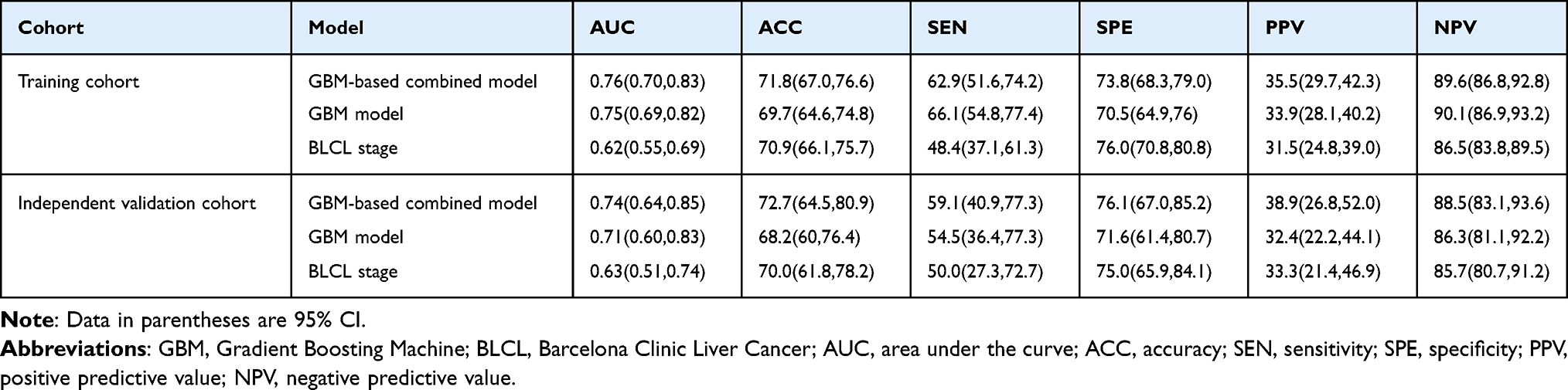 |
Table 5 Predictive Performance of GBM-Based Combined, GBM, and BLCL Models on the Training and External Validation Cohort |
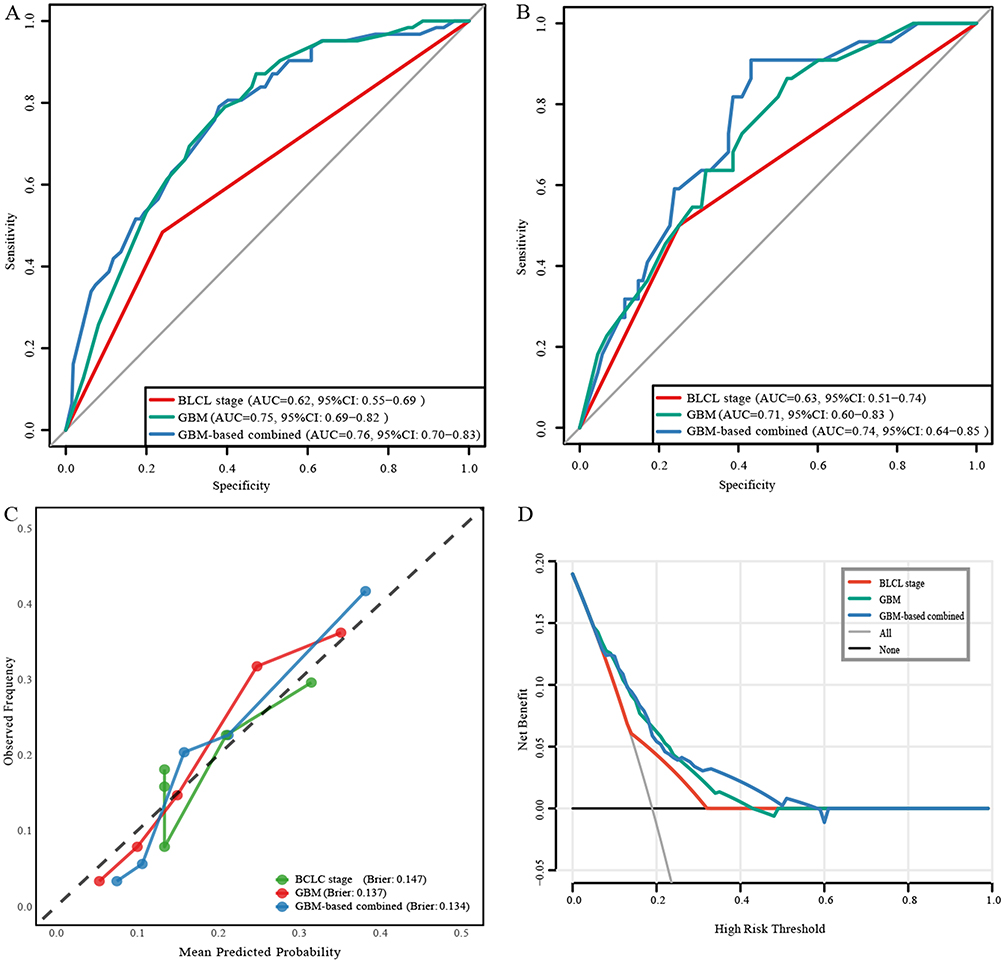 |
Figure 4 Receiver operating characteristic (ROC) analysis, Calibration curve, and Decision curve analysis (DCA). (A and B) ROC analysis in training and independent validation cohort. (C) Calibration curves of the GBM-based combined, GBM, and BCLC stage models. (D) DCA of the GBM-based combined, GBM, and BCLC stage models. |
The SHAP feature importance plots ranked the following selected features: BCLC stage, CA125 level, number of intrahepatic lesions, pre-antiviral therapy, pre-TKI therapy, and LNM (Figure 5A). The summary plot indicated that only pre-antiviral therapy had a positive association with curative conversion therapy, whereas the others showed a negative correlation (Figure 5B). Figures 5C and D displays the SHAP explanation force plots for two representative cases from the external validation cohort, which demonstrates how the features push the output of the GBM model from the baseline.
 |
Figure 5 Histogram illustrating the importance of the variables with curative conversion therapy. (A) The importance of features plots (left panel) shows that the features were ranked by descending importance measured as the mean absolute Shapley values. The larger the average absolute SHapley Additive exPlanation (SHAP) value of the feature, the more important the feature to the model. (B) The SHAP summary plots (right panel) show the distribution of the effect of each feature on the model output. Each dot is created for each feature attribution value of each patient, and multiple dots of the same feature attribution value converge into violin plots, using width to represent patient density. The color gradient (red for high, blue for low, purple for intermediate) represents the feature’s encoding value. The horizontal axis represents the Shapley value, with higher values indicating a greater probability of being classified as a suitable candidate for curative conversion therapy. To illustrate the model’s interpretability, we present SHAP force plots for two representative cases: (C) classified as a suitable candidate for receiving curative conversion therapy, and (D) classified as not a suitable candidate. These plots reveal that the most influential features contributing to the model’s predictions can vary significantly between individuals, highlighting the model’s ability to capture nuanced decision-making processes. |
Discussion
The current study found that 19.00% of the uHCC patients were converted to resectable disease and achieved clinical or pathological CR after combination therapy with a TKI and anti-PD-1/ PD-L1 antibodies. Patients who underwent curative conversion therapy had a significantly better prognosis than those who did not, with a median overall survival time of 40 months. After univariate and multivariate analyses, five factors were identified as significantly associated with curative conversion therapy: CA125, pre-TKI therapy, pre-antiviral therapy, LNM, and number of intrahepatic lesions. To facilitate the timely monitoring and screening of suitable candidates for conversion therapy, we constructed a model using these five predictors. The model classified patients into low- and high-likelihood groups for conversion therapy and demonstrated a significant difference in prognosis between the groups. Additionally, regardless of whether PSM was added, patients who received surgical resection as curative conversion therapy had a better prognosis than those who received ablation therapy.
Previous retrospective and prospective studies have reported conversion therapy rates ranging from 4.90% to 46.80% with the combination of TKIs and PD-1/PD-L1 inhibitors.4,15,16,22 This multicenter retrospective study achieved a conversion therapy rate of 19.00%, consistent with these previously reported rates. The variability in conversion rates across studies may be attributed to the differences in the clinical criteria used to determine surgical resectability. Multidisciplinary evaluation, considering factors such as tumor size, location, vascular invasion, and hepatic function, is often involved in assessing operability. Additionally, patient selection, specific TKI and PD-1/PD-L1 inhibitor regimens, and the timing of surgical intervention can influence the success of conversion therapy. The 19.00% CR rate reported in the current retrospective analysis suggests that TKIs plus PD-1/PD-L1 combination therapy can be an effective approach for downstaging and converting previously unresectable liver tumors to a surgically operable state in a meaningful proportion of patients. However, the lack of standardized criteria for assessing resectability may limit the ability to make direct comparisons between studies.
Previous studies have identified key factors associated with successful conversion therapy in patients with uHCC. Zhu et al21 found that patients with an ECOG PS of 0, fewer intrahepatic tumors, or radiographic response to systemic therapy were more likely to undergo curative resection. Additionally, Tomonari et al22 reported that patients with a mALBI grade of 1 or 2a and BCLC stage B had significantly higher rates of transitioning to conversion therapy. Kikuchi et al17 work further emphasized the association between BCLC stage and likelihood of successful conversion therapy. Building upon these findings, the current study incorporated additional parameters reflecting tumor burden, liver function, and tumor markers. The results indicated that patients with normal CA-125 levels, ≤ two lesions, no LNM, pre-antiviral treatment, and no pre-TKI treatment were more likely to achieve curative conversion after receiving TKIs plus immunotherapy.
Interestingly, our findings revealed a significant positive association between antiviral treatment and successful conversion therapy. This observation may be explained by the fact that reducing the viral load through antiviral therapy may contribute to a more favorable immune environment by mitigating chronic inflammation and fibrosis.26 Kim et al27 have emphasized the cost-effectiveness of initiating antiviral therapy early in the immune-tolerant phase of chronic hepatitis B. Recent studies have also reported that antiviral therapy was associated with improved prognosis in patients with HBV-related HCC undergoing curative resection.28 Our pathological correlation analysis further supports the potential of antiviral therapy to suppress tumor progression and metastasis as well as alleviate chronic liver inflammation. However, further research is needed to fully elucidate the specific mechanisms and effects of antiviral therapy.
These results also indicated that pre-TKI therapy was unfavorable for conversion therapy. This observation was further supported by our pathological correlation analysis, which suggested that pre-TKI therapy may exacerbate liver function impairment or induce metabolic changes, potentially hindering the effectiveness of the subsequent combined therapy. This observation aligns with previous studies reporting TKI-induced biological resistance (eg, through RIOK1-mediated stress granule formation) and systemic response delays (such as tumor vascular abnormality), both of which may contribute to diminished therapeutic efficacy in subsequent treatments.29,30 Additionally, we found that MVI had a significant positive correlation with LNM, while LNM had a negative correlation with conversion therapy. Therefore, we can infer that MVI may be one of the pathological reasons patients cannot undergo further conversion therapy. Early identification of MVI can enable clinicians to make informed treatment decisions, including whether a patient is a suitable candidate for conversion therapy.
Given that the BCLC staging system has previously been proposed as a predictor for conversion therapy response, this study developed a composite model integrating BCLC stage with additional prognostic factors.17 Our analysis suggests that this integrated model may offer improved predictive capability compared to BCLC staging alone in our cohort. This model could potentially help identify patients likely to be suitable candidates for conversion therapy before treatment initiation. Notably, candidates selected by this model demonstrated more favorable prognosis in this retrospective analysis compared to patients who did not undergo conversion therapy. While these results appear promising, further validation is needed to establish clinical utility. It should be noted that Lin et al developed a distinct tool focusing on preoperative and postoperative recurrence risk (preoperative risk score model included the NLR ≥ 1.39, multiple tumors, absence of radiographic response, and no AFP response), reporting 1-year/2-year tdROCs for the preoperative risk score were 0.760/0.682 (validation). In contrast, our model aims to provide clinicians with a complementary assessment tool focused specifically on predicting pre-treatment conversion therapy benefits.31 Considering the model’s development from retrospective data and its current performance characteristics, we recommend cautious interpretation. These findings represent a preliminary step toward developing more personalized treatment selection approaches, not a definitive clinical decision tool at this stage.
In addition, this study proposed different conclusions regarding the selection of different conversion therapy strategies. After survival analysis, we found that patients undergoing surgical resection had significantly better outcomes in terms of both PFS and OS than those undergoing ablation therapy. However, Tomonari et al22 showed that the choice between ablation and surgical resection did not show significant differences in these patients. This controversial result may be related to various factors such as sample size and treatment protocols. The studies had a limited sample size (only 15 and 52 patients), which may have influenced the results. Further prospective studies with larger sample sizes and standardized treatment protocols are needed to confirm this finding and to determine the optimal conversion therapy strategy. The therapy regimens used in this study were generally well tolerated, with manageable adverse events and no new or unexpected toxicities. However, liver dysfunction was the most common grade ≥ 3 TRAEs. Therefore, during the treatment process, clinicians should pay close attention to the protection of liver function and monitor liver function in real-time.
This study has important limitations inherent to its retrospective multicenter design, including potential selection bias and lack of centralized imaging review. While subgroup analyses addressed treatment heterogeneity among various TKI/anti-PD-1 combinations, the small sample size of specific subgroups (particularly lenvatinib-toripalimab, n=10) limits definitive efficacy comparisons. Our study revealed no significant prognostic differen ces between targeted-immunotherapy (TKI plus anti-PD-1/PD-L1) with or without additional local therapies (eg, TACE, perfusion therapy, radiotherapy). In contrast, Yang DL et al32 reported that TACE combined with TKIs and anti-PD-1/PD-L1 antibodies significantly improved survival and conversion rates versus TACE alone in uHCC patients. The pooled analysis of diverse local modalities (TACE, perfusion, radiotherapy) in our study may obscure modality-specific synergies, whereas Yang DL et al evaluated a standardized TACE-centric protocol. Non-randomized design and heterogeneous local therapies limit causal inferences. Future trials should standardize protocols. Although our GBM model outperformed BCLC staging using five clinically relevant predictors (CA125, pre-TKI therapy, etc), its accuracy could be enhanced by incorporating radiomic features, genomic markers, and tumor microenvironment characteristics. The retrospective nature also precluded uniform conversion decision protocols across institutions. These findings require prospective validation in randomized trials with larger cohorts and biological markers to establish clinical utility and generalizability.
Conclusion
This study provides a reference regarding the efficacy of combination therapy using TKIs and anti-PD-1/PD-L1 antibodies in converting uHCC to resectable disease, which in turn results in enhanced survival outcomes. The development of a model based on predictors offers a potential tool for clinicians to identify patients likely to benefit from conversion therapy. This enables timely intervention and may enhance outcomes by preventing the loss of opportunities for curative treatment.
Abbreviations
uHCC, unresectable hepatocellular carcinoma; TKIs, tyrosine kinase inhibitors; PD-1/PD-L1 antibodies, programmed cell death protein 1/programmed cell death ligand 1 antibodies; BCLC, Barcelona Clinic Liver Cancer; GBM, Gradient Boosting Machine; SHAP, SHapley Additive exPlanations; OS, overall survival; PFS, progression-free survival.
Data Sharing Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the First Affiliated Hospital of Jinan University (No. KY-2024-237). Written informed consent was waived because of the retrospective nature of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We acknowledge financial support from the National Key Research and Development Program of China (2023YFF1204600), National Natural Science Foundation of China (82227802, 82302306), Clinical Frontier Technology Program of the First Affiliated Hospital of Jinan University, China (No. JNU1AF-CFTP-2022-a01201), Science and Technology Projects in Guangzhou (202201020022, 2023A03J1036, 2023A03J1038, 2025A04J3482), Science and Technology Youth Talent Nurturing Program of Jinan University (21623209), Postdoctoral Science Foundation of China (2022M721349), and Hainan Natural Science Foundation Youth Fund (822QN482). The authors declare no competing financial interests.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7:6. doi:10.1038/s41572-020-00240-3
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2024;74:229–263. doi:10.3322/caac.21834
3. Villanueva A. Hepatocellular Carcinoma. N Engl J Med. 2019;380:1450–1462. doi:10.1056/NEJMra1713263
4. Wu J-Y, Yin Z-Y, Bai Y-N, et al. Lenvatinib combined with Anti-PD-1 antibodies plus transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma: a multicenter retrospective study. J Hepatocell Carcinoma. 2021;8:1233–1240. doi:10.2147/JHC.S332420
5. Ho WJ, Zhu Q, Durham J, et al. Neoadjuvant cabozantinib and nivolumab convert locally advanced hepatocellular carcinoma into resectable disease with enhanced antitumor immunity. Nat Cancer. 2021;2:891–903. doi:10.1038/s43018-021-00234-4
6. Zhang L, Ding J, Li HY, Wang ZH, Wu J. Immunotherapy for advanced hepatocellular carcinoma, where are we? Biochim Biophys Acta Rev Cancer. 2020;1874:188441. doi:10.1016/j.bbcan.2020.188441
7. Pinter M, Scheiner B, Pinato DJ. Immune checkpoint inhibitors in hepatocellular carcinoma: emerging challenges in clinical practice. Lancet Gastroenterol Hepatol. 2023;8:760–770. doi:10.1016/S2468-1253(23)00147-4
8. Cheng A-L, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76:862–873. doi:10.1016/j.jhep.2021.11.030
9. Qin S, Chan LS, Gu S, et al. LBA35 Camrelizumab (C) plus rivoceranib (R) vs. sorafenib (S) as first-line therapy for unresectable hepatocellular carcinoma (uHCC): a randomized, phase III trial. Ann Oncol. 2022;33:S1401–S1402. doi:10.1016/j.annonc.2022.08.032
10. Qin S, Chan SL, Gu S, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international Phase 3 study. Lancet. 2023;402:1133–1146. doi:10.1016/S0140-6736(23)00961-3
11. Llovet JM, Kudo M, Merle P, et al. Lenvatinib plus pembrolizumab versus lenvatinib plus placebo for advanced hepatocellular carcinoma (LEAP-002): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2023;24:1399–1410. doi:10.1016/S1470-2045(23)00469-2
12. Huang C, Zhu X-D, Shen Y-H, et al. Organ specific responses to first-line lenvatinib plus anti-PD-1 antibodies in patients with unresectable hepatocellular carcinoma: a retrospective analysis. Biomarker Res. 2021;9:9. doi:10.1186/s40364-021-00262-3
13. Kudo M. A novel treatment strategy for patients with intermediate-stage HCC who are not suitable for TACE: upfront systemic therapy followed by curative conversion. Liver Cancer. 2021;10:539–544. doi:10.1159/000519749
14. Zhu AX, Abbas AR, de Galarreta MR, et al. Molecular correlates of clinical response and resistance to atezolizumab in combination with bevacizumab in advanced hepatocellular carcinoma. Nature Med. 2022;28:1599–1611. doi:10.1038/s41591-022-01868-2
15. Zhang W, Tong S, Hu B, et al. Lenvatinib plus anti-PD-1 antibodies as conversion therapy for patients with unresectable intermediate-advanced hepatocellular carcinoma: a single-arm, Phase II trial. J ImmunoTher Cancer. 2023;2023:11.
16. Kudo M, Aoki T, Ueshima K, et al. Achievement of complete response and drug-free status by atezolizumab plus bevacizumab combined with or without curative conversion in patients with transarterial chemoembolization-unsuitable, intermediate-stage hepatocellular carcinoma: a multicenter proof-of-concept study. Liver Cancer. 2023;12:321–338. doi:10.1159/000529574
17. Kikuchi T, Takeuchi Y, Nouso K, et al. Predictive factors for transition to conversion therapy in hepatocellular carcinoma using atezolizumab plus bevacizumab. Liver Int. 2024;44:1456–1463. doi:10.1111/liv.15907
18. Tang H, Cao Y, Jian Y, et al. Conversion therapy with an immune checkpoint inhibitor and an antiangiogenic drug for advanced hepatocellular carcinoma: a review. Biosci Trends. 2022;16:130–141. doi:10.5582/bst.2022.01019
19. Sun H-C, Zhou J, Wang Z, et al. Chinese expert consensus on conversion therapy for hepatocellular carcinoma (2021 edition). Hepatobiliary Surg Nutr. 2022;11:227–252. doi:10.21037/hbsn-21-328
20. Zhu D, Tulahong A, Abuduhelili A, et al. Machine learning prognostic model for post-radical resection hepatocellular carcinoma in hepatitis B patients. J Hepatocell Carcinoma. 2025;12:353–365. doi:10.2147/JHC.S495059
21. Zhu X-D, Huang C, Shen Y-H, et al. Hepatectomy after conversion therapy using tyrosine kinase inhibitors plus Anti-PD-1 antibody therapy for patients with unresectable hepatocellular carcinoma. Ann Surg Oncol. 2022;30:2782–2790. doi:10.1245/s10434-022-12530-z
22. Tomonari T, Tani J, Sato Y, et al. Clinical features and outcomes of conversion therapy in patients with unresectable hepatocellular carcinoma. Cancers. 2023;16:15. doi:10.3390/cancers16010015
23. European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236. doi:10.1016/j.jhep.2018.03.019
24. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67:358–380. doi:10.1002/hep.29086
25. Vitale A, Cabibbo G, Rimassa L, et al. The concept of “Converse Therapeutic Hierarchy” for patients with hepatocellular carcinoma. Liver Cancer;2025. 1–15. doi:10.1159/000546360
26. Hwang JP, Feld JJ, Hammond SP, et al. Hepatitis B virus screening and management for patients with cancer prior to therapy: ASCO provisional clinical opinion update. J Clin Oncol. 2020;38:3698–3715. doi:10.1200/JCO.20.01757
27. Kim H-L, Kim G-A, Park J-A, Kang H-R, Lee E-K, Lim Y-S. Cost-effectiveness of antiviral treatment in adult patients with immune-tolerant phase chronic hepatitis B. Gut. 2021;70:2172–2182. doi:10.1136/gutjnl-2020-321309
28. Huang DQ, Hoang JK, Kamal R, et al. Antiviral therapy utilization and 10-year outcomes in resected hepatitis B virus– and hepatitis C virus–related hepatocellular carcinoma. J Clin Oncol. 2024;42:790–799. doi:10.1200/JCO.23.00757
29. Meng F, Li H, Huang Y, et al. RIOK1 phase separation restricts PTEN translation via stress granules activating tumor growth in hepatocellular carcinoma. Nat Cancer. 2025;2025:1.
30. Loh JJ, Ng KY, Huang IB, et al. DGKH-mediated phosphatidic acid oncometabolism as a driver of self-renewal and therapy resistance in HCC. Hepatology. 2024. doi:10.1097/HEP.0000000000001158
31. Lin KY, Liu HZ, Liu JW, et al. Online risk scores for pre- and postoperative prediction of early recurrence in hepatocellular carcinoma patients undergoing conversion liver resection after tyrosine kinase inhibitors and immune checkpoint inhibitors therapy. Eur J Surg Oncol. 2025;51:110220. doi:10.1016/j.ejso.2025.110220
32. Yang D-L, Ye L, Zeng F-J, et al. Multicenter, retrospective GUIDANCE001 study comparing transarterial chemoembolization with or without tyrosine kinase and immune checkpoint inhibitors as conversion therapy to treat unresectable hepatocellular carcinoma: survival benefit in intermediate or advanced, but not early, stages. Hepatology. 2025;2025:1.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Machine Learning Model Based on Health Records for Predicting Recurrence After Microwave Ablation of Hepatocellular Carcinoma
An C, Yang H, Yu X, Han Z, Cheng Z, Liu F, Dou J, Li B, Li Y, Li Y, Yu J, Liang P
Journal of Hepatocellular Carcinoma 2022, 9:671-684
Published Date: 28 July 2022
Prognosis and Personalized Treatment Prediction in Different Mutation-Signature Hepatocellular Carcinoma
Zhang Y, Liu Z, Li J, Li X, Duo M, Weng S, Lv P, Jiang G, Wang C, Li Y, Liu S, Li Z
Journal of Hepatocellular Carcinoma 2023, 10:241-255
Published Date: 15 February 2023
Breaking the Barriers of Therapy Resistance: Harnessing Ferroptosis for Effective Hepatocellular Carcinoma Therapy

Lv X, Lan G, Zhu L, Guo Q
Journal of Hepatocellular Carcinoma 2024, 11:1265-1278
Published Date: 2 July 2024
Safety and Efficacy of TACE-HAIC Combined with Lenvatinib and PD-1 Inhibitors in Large Intermediate-Stage Hepatocellular Carcinoma: A Multi-Center Retrospective Study
Ni J, Li C, Sun H, Liu Y, Guo G, Zhou X, Zhou Z, Fan R, Hu H, Xu L
Journal of Hepatocellular Carcinoma 2026, 13:586001
Published Date: 24 April 2026
Development and Validation of a Machine Learning-Based Individualized Model to Predict TKI Benefit in Postoperative Recurrent HCC
Li M, Jiang Y, Gong L, Sun R, Hao A, Liu K, Luan K, Jia Z, Zhang S, Liu K, Tan B, Hu W, Qu C, Cao J
Journal of Hepatocellular Carcinoma 2026, 13:599142
Published Date: 16 June 2026