Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Saudi Adults’ Understanding and Views of Weight Management Practices and Obesity
Authors Alshehri FS ![]() , Alorfi NM
, Alorfi NM ![]()
Received 3 August 2023
Accepted for publication 27 October 2023
Published 6 November 2023 Volume 2023:16 Pages 3513—3531
DOI https://doi.org/10.2147/DMSO.S433721
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Fahad S Alshehri, Nasser M Alorfi
Department of Pharmacology and Toxicology, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Fahad S Alshehri
Department of Pharmacology and Toxicology, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
, Email [email protected]
Background and Objective: The rising prevalence of overweight and obesity presents a significant global challenge. This study aimed to investigate the understanding and views of weight management practices and obesity among Saudi adults.
Methodology: A cross-sectional online survey was conducted from October 2022 to January 2023 among adults residing in Saudi Arabia. Participants completed a self-administered 41-item questionnaire designed to assess their understanding and views regarding weight management practices and obesity.
Results: A total of 1066 participants completed the survey. Gender distribution showed a majority of males (55.7%). Age-wise, the majority fell below 51 years, with 37.7% (young) between 18– 24, 32.7% (young adult) between 25– 33, and 21.3% (adult) between 34– 51. Employment was reported by one-third (n = 315) of respondents, while 22.0% (n = 234) had a history of chronic diseases. Furthermore, 77.3% (n = 824) engaged in regular physical activity.The study results revealed that participants’ mean score for understanding obesity was 3.28 ± 2.37 (range 0– 6), while the average views score was 28.08 ± 8.79 (range 0– 34). Furthermore, females displayed a higher level of understanding compared to males. Employment status also played a significant role, with employed individuals having a better understanding of obesity than those who were unemployed. Moreover, participants with higher qualifications demonstrated a more comprehensive understanding of obesity compared to those with lower qualifications. Additionally, individuals with higher monthly income levels displayed a greater understanding of obesity compared to those with lower incomes. Lastly, participants who engaged in regular physical activity exhibited a higher level of understanding compared to those who were physically inactive.
Conclusion: The study indicates that factors such as being older, being female, being employed, having higher education and income, and engaging in regular physical activity are associated with increased understanding and favorable views regarding weight management practices and obesity.
Keywords: prevalence, overweight, obesity, weight management, Saudi Arabia
Introduction
People with overweight and obesity is a major health issue faced by many people, and it is linked to various diseases such as diabetes mellitus (DM) and cardiovascular diseases (CVD).1,2 Obesity results from abnormal or excessive increases in person’s weight so that it crosses the body mass index (BMI) threshold of more than 25 (overweight) or 30 (obese).3 The World Health Organization (WHO) reported that 1 billion people worldwide were obese in 2022, including 650 million adults, 340 million teenagers, and 39 million children.4 The prevalence of obesity is rising globally; data show that 60% of people in Europe are overweight, and 40–45% of people in the United States are obese.5 In United States, approximately 35% of adults are diagnosed with obesity, while one-third of children and adolescents in the country are either overweight or obese. In 2017, 39% of adults worldwide were overweight, and 13% were obese.3 In addition, a recent study in Saudi Arabia revealed obesity prevalence rates of 33.7% and overweight prevalence rates of 68.2%, indicating that both are becoming more common.6 Furthermore, the WHO reported that the Gulf regions had the highest rates of obesity and that Saudi Arabia was second in terms of its prevalence in 2022.4
In recent years, the society shift towards urbanization, technology-driven sedentary lifestyles, and changing dietary habits have drove the global rise in obesity and overweight.7 Overweight and obesity are rising everywhere due to several factors, including adopting a Westernized culture and a sedentary lifestyle.6,8 These lifestyle changes, combined with genetic factors, underline the urgency of addressing this complex issue.9 Obesity has a significant economic burden, with rising healthcare costs and decreased productivity.10 It also highlights health disparities among different demographic groups, emphasizing the importance of addressing social determinants of health.11 Moreover, there is evidence that overweight and obesity contribute more to an increase in mortality than being underweight.8 Furthermore, obese people are more likely to develop chronic diseases that significantly and negatively impact the economy due to decreased production, greater disability, increased medical costs and decreased life expectancy.8 As well, it has been shown that developing chronic diseases are also complications of obesity12,13 Monitoring and maintaining a healthy weight is crucial to prevent the risk and incidence of various diseases.14 In recent years, being obese or overweight has been linked to nearly 4.7 million premature deaths worldwide.3 On the other hand, obesity was identified as a risk factor for 6.5 million diseases in 2019 by the Global Burden of Disease research.15,16
Studies have shown that environmental, psychological, and physiological factors were associated with obesity, affecting people of all ages.17–19 As a result, the prevalence of obesity has increased, along with that mortality rates.20 There are a number of psychological factors that contribute to the complexity of the relationship between emotional eating, eating disorders, and obesity.21 Generally, emotional eating refers to the tendency to consume food in response to emotional states rather than physical hunger. Often, it is used as a means of soothing or distracting negative emotions.22 As a consequence, eating disorders such as binge eating disorder or bulimia can result from this pattern of behavior.23 Psychological factors like body dissatisfaction, low self-esteem, perfectionism, and a distorted body image also play a role in the development and maintenance of eating disorders and obesity.24,25 Understanding the interplay of these psychological factors is crucial for effective prevention and treatment approaches that address both the emotional and physical aspects of these conditions.
Obesity and overweight are of particular concern as risk factors for CVD and the development of DM, hypertension (HTN), dyslipidemia, and coronary heart disease.16–19 Several causes of obesity and overweight have been put forward, the most prominent being genetics, a lack of exercise, a sedentary lifestyle, and increased food intake.15 It is generally known that patient counseling and education are essential components of the self-management of many diseases in health care.
Previous studies have assessed the knowledge, attitudes, and practices related to various diseases nationally and internationally.26–32 However, only a few studies have evaluated the knowledge and practices related to obesity internationally.33–35 Although similar studies exist in Saudi Arabia, most were carried out among different populations to this one.35,36 Our study stands out for its original design and sample, complete attention to obesity, and information on disease-related knowledge and management. As a result, it raises public awareness of hidden weight-related diseases.
Furthermore, since overweight and obesity are two of the most under-diagnosed and neglected medical conditions, and individuals’ lack of knowledge about them may give rise to considerable concern, it is important to assess the understanding, views, and practices related to them. Such data are an important element of attempts to curtail their prevalence.6,8,37 Therefore, this study aimed to assess Saudi adults’ understanding and views of weight management practices and obesity. In addition to the global and regional impact, it is crucial to recognize that obesity and overweight are complicated issues that affect individuals.38 The burden of these conditions extends beyond physical health, influencing individuals’ social, psychological, and economic well-being.39 Societal perceptions of body image, self-esteem, and the stigmatization of those with obesity further underscore the complexity of the problem.40,41 Moreover, the consequences are multigenerational, as unhealthy lifestyle habits often continue within families, leading to a cycle of obesity and associated health risks.42 Understanding the wider implications of obesity and overweight is vital for developing valuable strategies that encompass not only medical interventions but also address the psychosocial and environmental factors contributing to these conditions.
Methods
A cross-sectional study was conducted among the Saudi Arabian Saudi public to assess their understanding and views of weight management practices and obesity. The study was conducted over three months, from October 2022 to January 2023, using pre-validated online questionnaires. In addition, a structured, self-administered questionnaire was prepared and distributed online through social media platforms among adults living in Saudi Arabia. This study included individuals over 18 years old, currently residing in Saudi Arabia, willing to provide online consent and complete the questionnaires; others who did not meet the inclusion criteria were excluded from the study.
Study Questionnaires and Procedure
The questionnaire was adopted after a detailed review of the published literature on this topic,2,6,17 and an expert with substantial experience in cross-sectional study design evaluated it. The questionnaire contained five sets of questions. The first set addressed demographic variables, with a total of 11 items (for example, age, gender, nationality, employment, physical activity, disease status, and BMI). The second set consisted of questions about obesity understanding, with a total of 8 items, assessed on “Yes/ No/I do not know” and multiple-choice options. The third set of questions was related to awareness of obesity treatment (5 items), and the fourth set assessed views (10 items) on a five-point Likert scale (agree/disagree/neutral). The last set of questions was designed to assess practices (6 items) related to obesity and weight management.
The questionnaire was translated through forward and backward translation with the help of a native Arabic speaker. In addition, a pilot study was carried out with the prepared Arabic questionnaire with randomly selected individuals (n = 30) to examine the questionnaire’s readability before administering it. The results of the pilot study were not included in the main study. The Cronbach’s alpha scores for understanding, awareness views, and practices were 0.79, 0.70, 0.68, and 0.75, respectively.
The understanding scores were prepared by assigning a score of one for a correct answer and zero for a wrong answer. Next, the mean understanding score was calculated, as were the mean view and practice scores. The understanding and view scores were further divided into “good” and “poor”, following previous studies.31,36 If the participants scored >80% of the total possible score, this was considered to be good, while those who scored <80% were regarded as having poor understanding.
A convenience sampling technique was used to collect the data from the participants. Data was collected using Google forms. Before proceeding to the questionnaire, the participants viewed a statement about the study’s purpose and were asked for online consent; only those who agreed and proceeded to complete the survey were included in the study. An informed consent was obtained from all participants before participating in the study, and this was done through an online consent procedure. Participants were presented with detailed information about the study’s objectives, procedures involved, potential risks and benefits, confidentiality measures, and their right to withdraw from the study at any time. The study involved online consent for all participants, and we followed ethical guidelines and regulations of the Biomedical Research Ethics Committee at Umm Al-Qura University to ensure the validity and integrity of the consent process in accordance with the declaration of Helsinki. The study was approved by the Biomedical Research Ethics Committee at Umm Al-Qura University (HAPO-02-K-012-2023-01-1364). Furthermore, the participants were given adequate time to complete the questionnaire. A researcher was appointed from the College of Pharmacy at Umm Al-Qura University to collect the data. Furthermore, written informed consent was obtained from the participants before starting answering the questionnaire stating the guidelines and the protocol of the study, and they were assured that the data would be used only for research and that their anonymity would be maintained throughout the study.
Statistical Analysis
The data analysis was conducted utilizing IBM SPSS Statistics 22 software (IBM Inc., Chicago, IL, USA). Descriptive statistics, frequencies, and percentages were employed to summarize the data. To examine the correlations between the understanding levels and demographic characteristics of the respondents, the Chi-square or Fisher exact test was utilized. Statistical significance was determined by a p-value of <0.05.
Results
Descriptive Results
One thousand and sixty-six subjects completed the survey. Table 1 represents the socio-demographic characteristics of the respondents. There were more males (n = 594, 55.7%) than females (n = 472, 44.3%), 37.7% of the participants were aged between 18 and 24 years (n = 402), and almost 98.2% of them were Saudi nationals (n = 1047). Regarding their residences, one-quarter of the respondents (n = 224) resided in the northern region of Saudi Arabia. More than half of the respondents (54.9%, n = 585) were university graduates, and 38.8% (n = 414) had passed higher studies. Almost one-third of the respondents (n = 315) were employed, and only 27% (n = 288) were students. The monthly income of a large proportion of the participants (n = 327; 30.7%) was, on average,>8k SAR. According to the findings, only 22.0% (n = 234) of the respondents had a history of chronic diseases. Moreover, 77.3% (n = 824) were physically active, but 11.1% (n = 118) had undergone surgery to reduce weight (see Table 1).
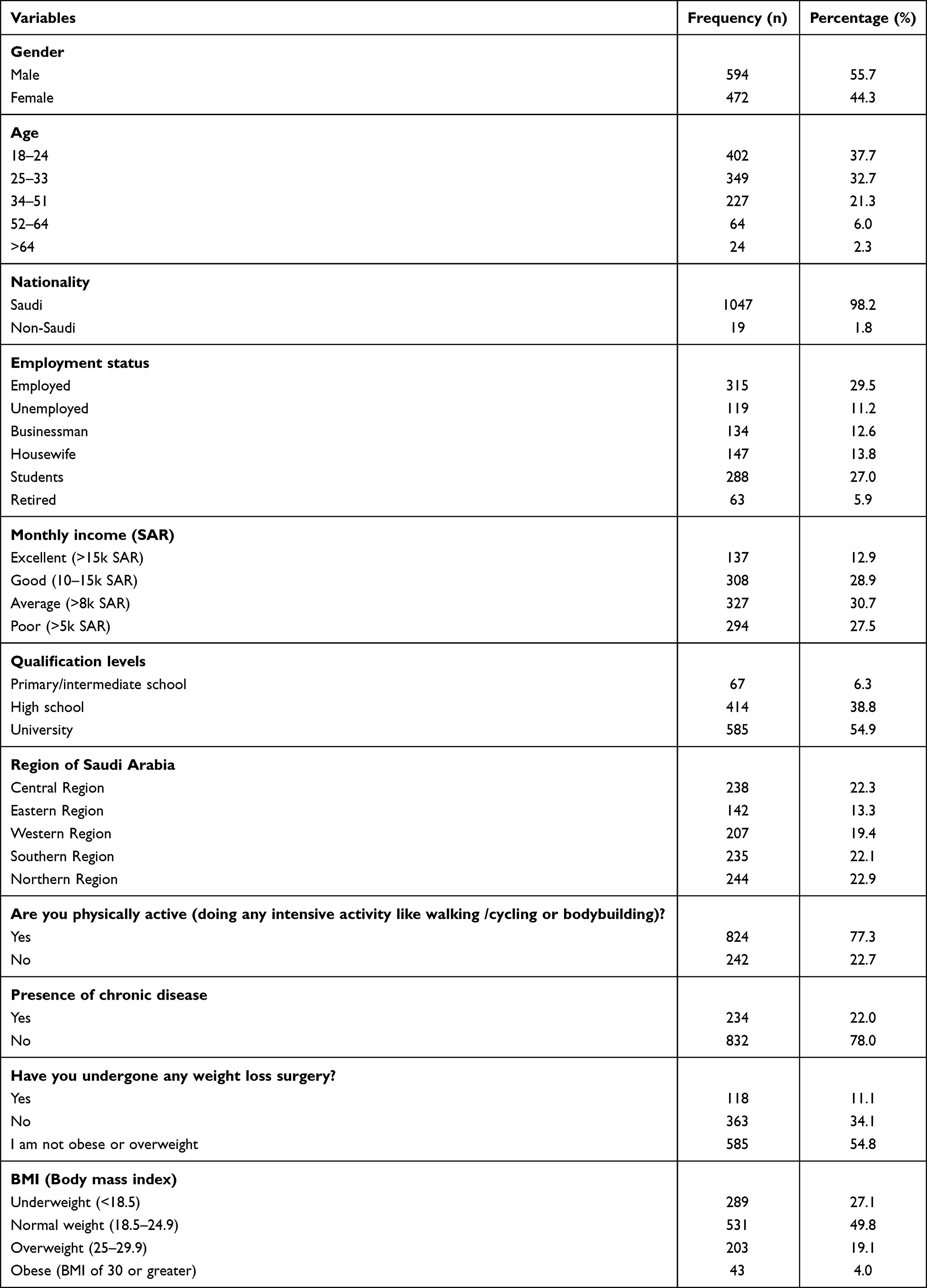 |
Table 1 Socio-Demographic Characteristics of the Participants (N = 1066) |
Table 2 describes the assessment of understanding obesity among Saudi adults. Over half (55.4%, n = 591) were familiar with the term “obesity”, while 58.9% (n = 628) knew that having a diet rich in carbohydrates, fats, and sugars may lead to obesity. Just over half of the respondents knew that consistent stress (n = 568) and smoking (n = 536) were risk factors for obesity. Most of the respondents (n = 625, 58.6%) knew that maintaining good levels of physical activity and a healthy diet would manage obesity. Additionally, 51.3% (n = 549) knew that there were anti-obesity medications approved by the Saudi Food and Drug Authority (SFDA) and the United States Food and Drug Administration (USFDA) that could enhance weight loss along with exercise and a healthy diet.
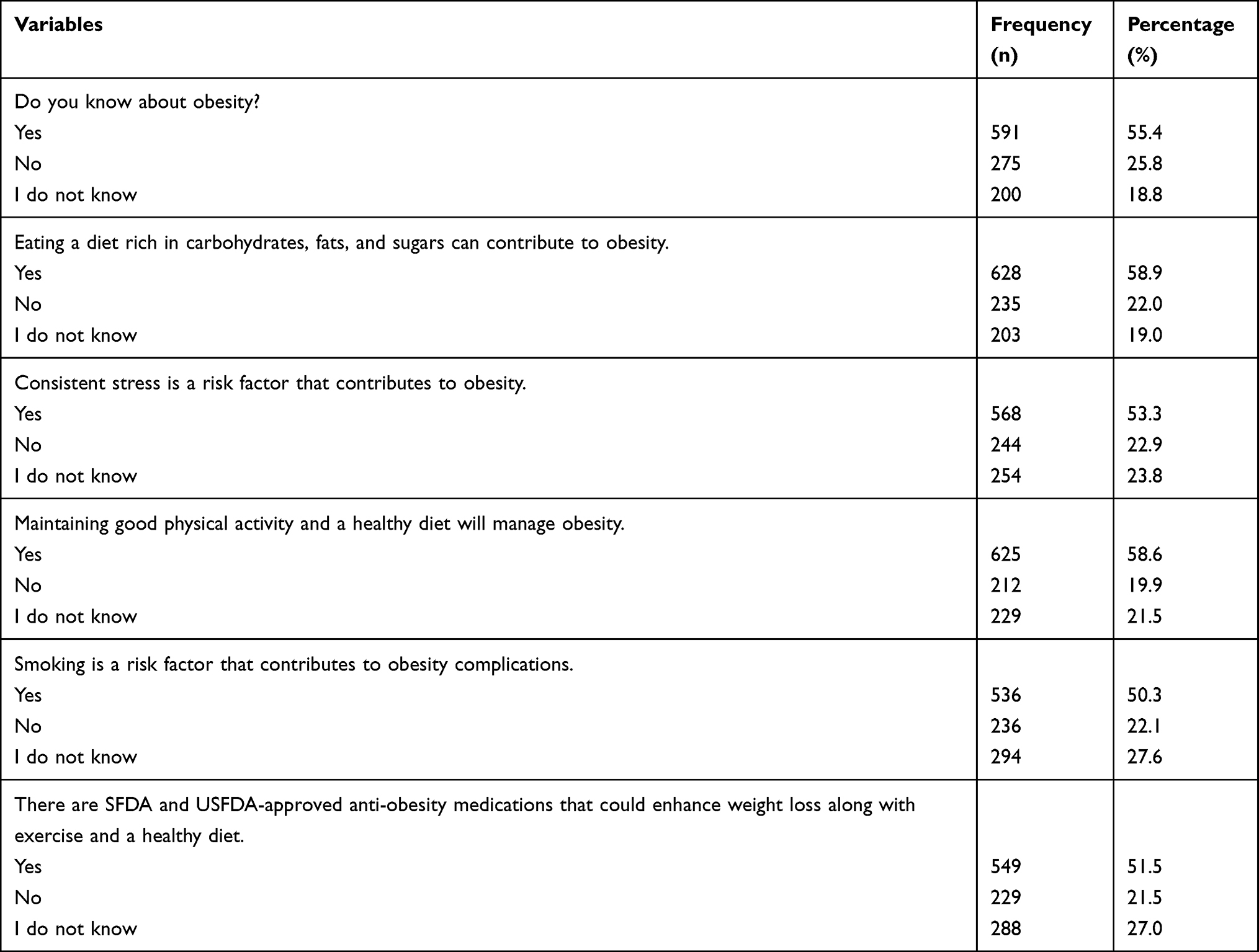 |
Table 2 Understanding Assessment of Obesity Among Saudi Adults |
In this study, 60.8% (n = 648) of the participants identified the heart as the organ the most affected by obesity, followed by joints 43.2% (n = 461), the liver 42.3% (n = 451), lungs 36.6% (n = 390), kidneys 34.8% (n = 371), and pancreas 33.9% (n = 361) Figure 1.
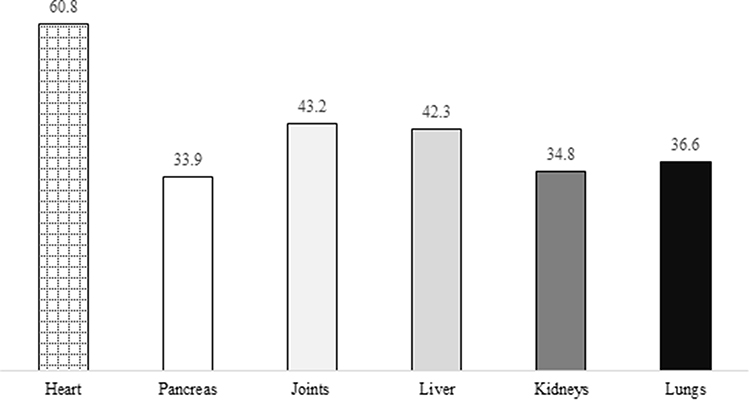 |
Figure 1 Understanding of Vital Organs Affected by Obesity. |
The current study shows that 61.7% (n = 658) of the participants agreed that cardiovascular disease was an obesity-related complication. This was followed by arthritis (49.8%, n = 531), nonalcoholic fatty liver disease (41.7%, n = 444), and hypertension (43.8%, n = 467). The full results of the complications associated with obesity are given in Figure 2. In this study, slightly more than half (54.8%, n = 584) of the respondents were aware of the surgeries available for obesity, and 57.9% (n = 617) were aware that lipid suction and sleeve gastrectomy lowered the amount of fat in the body, which was associated with obesity. Eighty-six percent of the participants (n = 712) thought that products could be used for weight reduction, and a large proportion of the respondents (n = 777, 72.9%) were aware that the usage of weight reduction agents could have side effects. Table 3 describes the respondents’ awareness of obesity treatment and drug products.
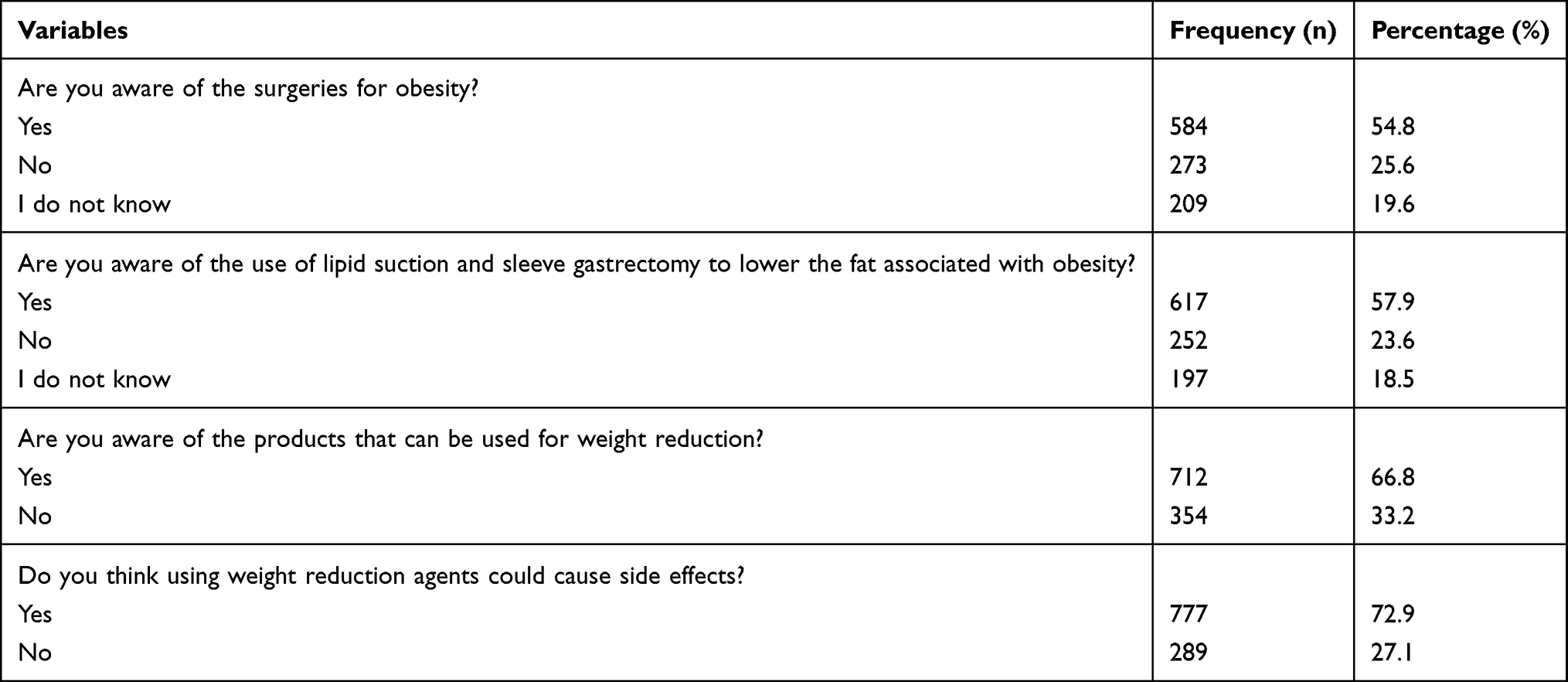 |
Table 3 Participants’ Awareness of Obesity Treatments and Drug Products |
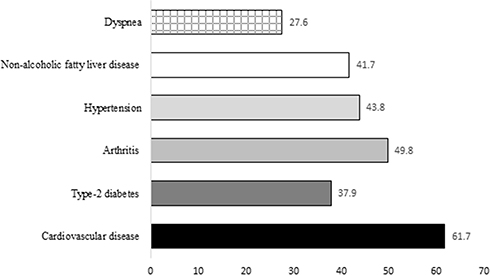 |
Figure 2 Understanding of Complications Associated With Obesity. |
With regard to the most commonly used weight reduction products, 54% (n = 576) identified this as green tea, followed by green coffee bean extract (40.5%, n = 432), ginseng (37.1%, n = 396), and metformin (36.1%, n = 385). The details are given in Figure 3. Over half of the respondents agreed that healthy individuals could consume healthy and unhealthy diets. Almost half of the respondents agreed that once a normal BMI is reached, one can stop maintaining good physical health. Out of 10 items, respondents disagreed with items nos. 3, 6, 7, and 9, which illustrated their view toward obesity. More than two-thirds of the respondents (68.7%) agreed that anti-obesity medications are not safe or as effective for obesity management as exercising and following a healthy diet. When the respondents were asked about stopping the consumption of a healthy diet once a normal weight is reached, 54.6% agreed with this item. Just over two-thirds of the respondents (68.8%) accepted item 8, indicating that they agreed that exercise training was effective for maintaining good physical health. Furthermore, the majority (70.2%) agreed that counseling by dieticians was effective for obesity management. Table 4 presents the results of the views of the respondents toward obesity and its management.
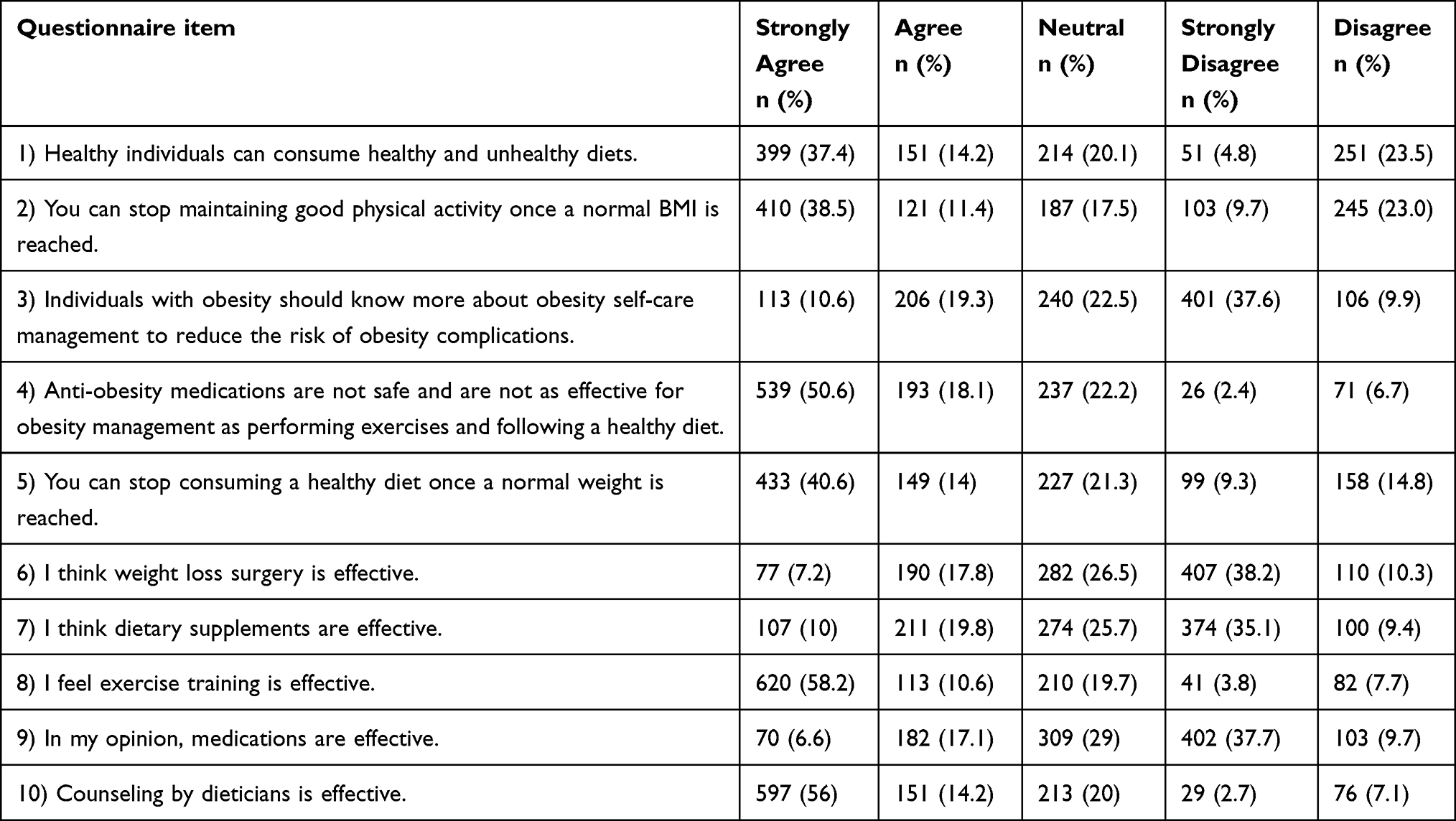 |
Table 4 Views Assessment of the Participants Toward Obesity |
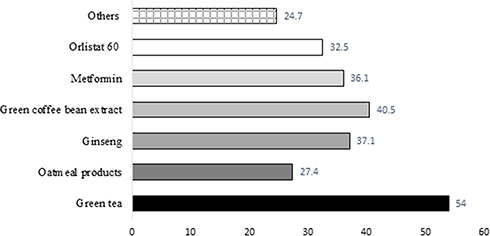 |
Figure 3 Commonly Used Weight Reduction Products. |
Regarding the practice of weight management, we asked six questions. First, the majority of the respondents (44.2%) indicated that they did not drink too many caffeinated drinks (>4 cups), such as tea and coffee. The second and fifth scenarios were related to adopting and maintaining a healthy lifestyle and following a physical exercise regimen to manage obesity; approximately one-third of the respondents agreed with the statements. Third, when asked about smoking or using tobacco products, more than half of the respondents did not smoke or use E-cigarettes. Less than half of the respondents (42.6%) did not consume unhealthy fast food. Lastly, a major proportion of the respondents (56.9%) were not taking any FDA-approved anti-obesity medications for obesity management. Detailed information is presented in Table 5. The overall mean understanding score was 3.28 ± 2.37 (range 0–96), while the view score was 28.08 ± 8.79 (range = 0–34). The mean understanding score was significantly associated with gender, age, employment status, qualifications, and monthly income; p < 0.001. Similarly, the region of the participants was found to be significantly correlated with the mean understanding score (p < 0.001). The participant’s physical activity was also significantly associated with the mean understanding score (p < 0.001), as shown in Table 6.
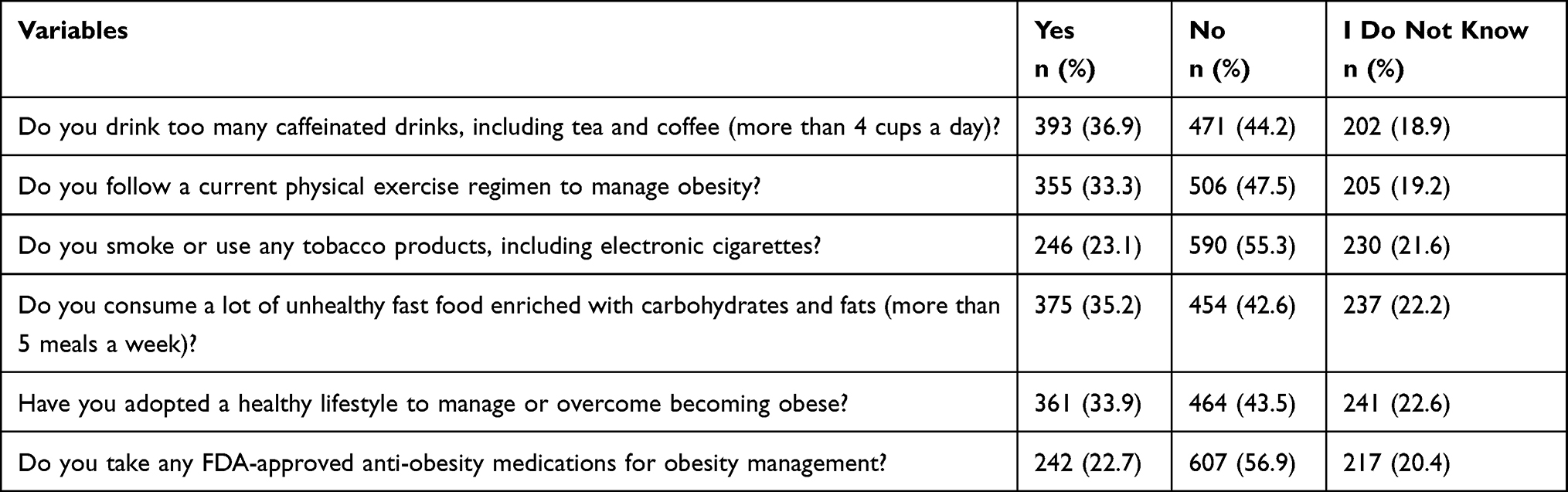 |
Table 5 Respondents’ Weight Management Practices |
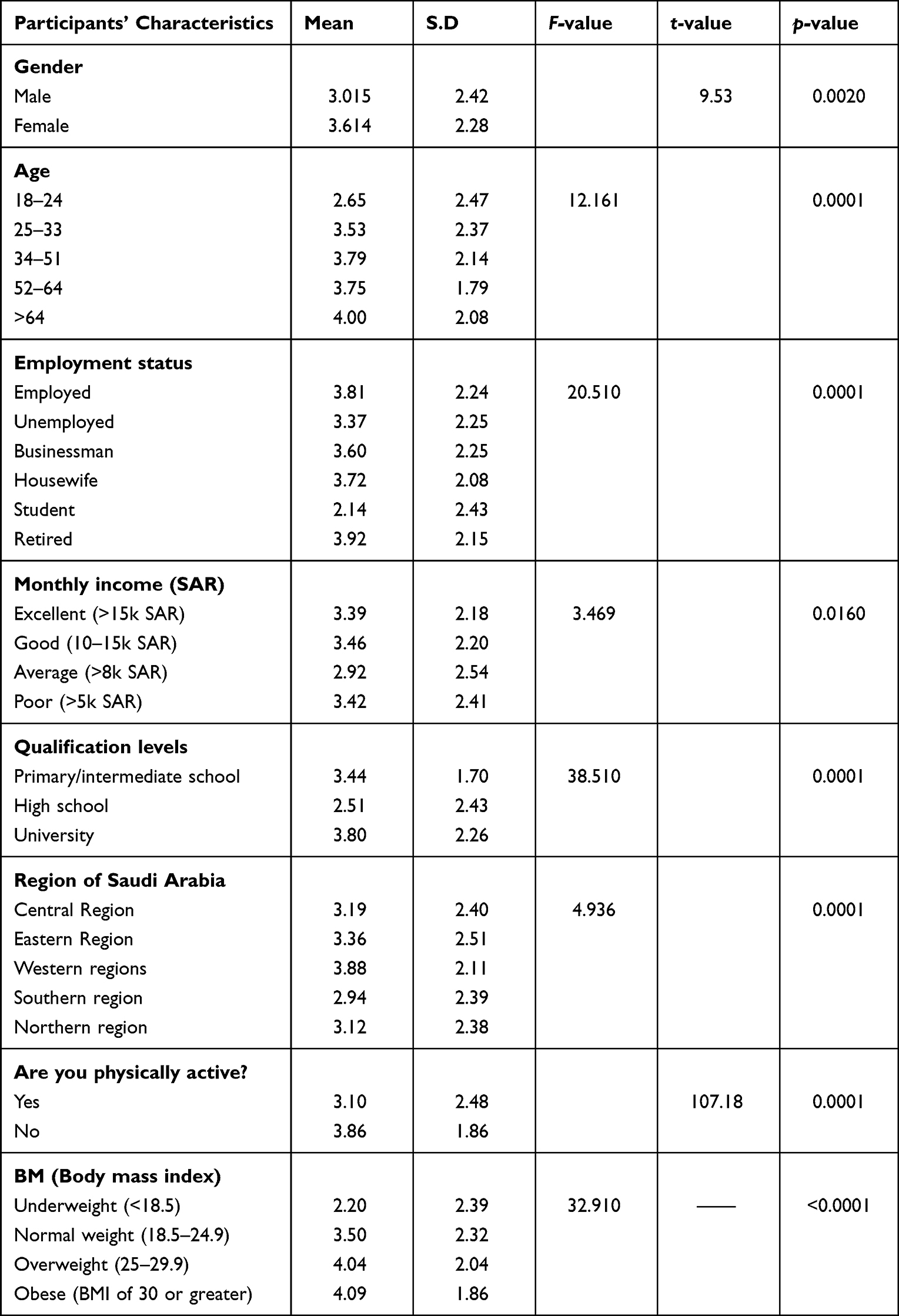 |
Table 6 Association Between Obesity Understanding Score and Characteristics of the Participants |
As previously mentioned, view and understanding scores were compiled, and the mean scores were calculated. A score >80% of the total possible score was considered good, while a score <80% was considered poor. In this study, 73.3% (n = 781) of the participants had a poor understanding of obesity, while 26.7% (n = 285) had good levels of understanding. In addition, only 21.9% (n = 233) of the participants had a good view of obesity; the majority (78.1%, n = 833) had a poor view of obesity and weight management. See Figure 4. The association between the view mean score and characteristics are presented in Table 7. Several characteristics of the participants – age, employment status, monthly income, and region – were significantly associated with the mean view score (p < 0.01), whereas gender and qualification levels, were not (p = 0.612, p = 0.909, respectively).
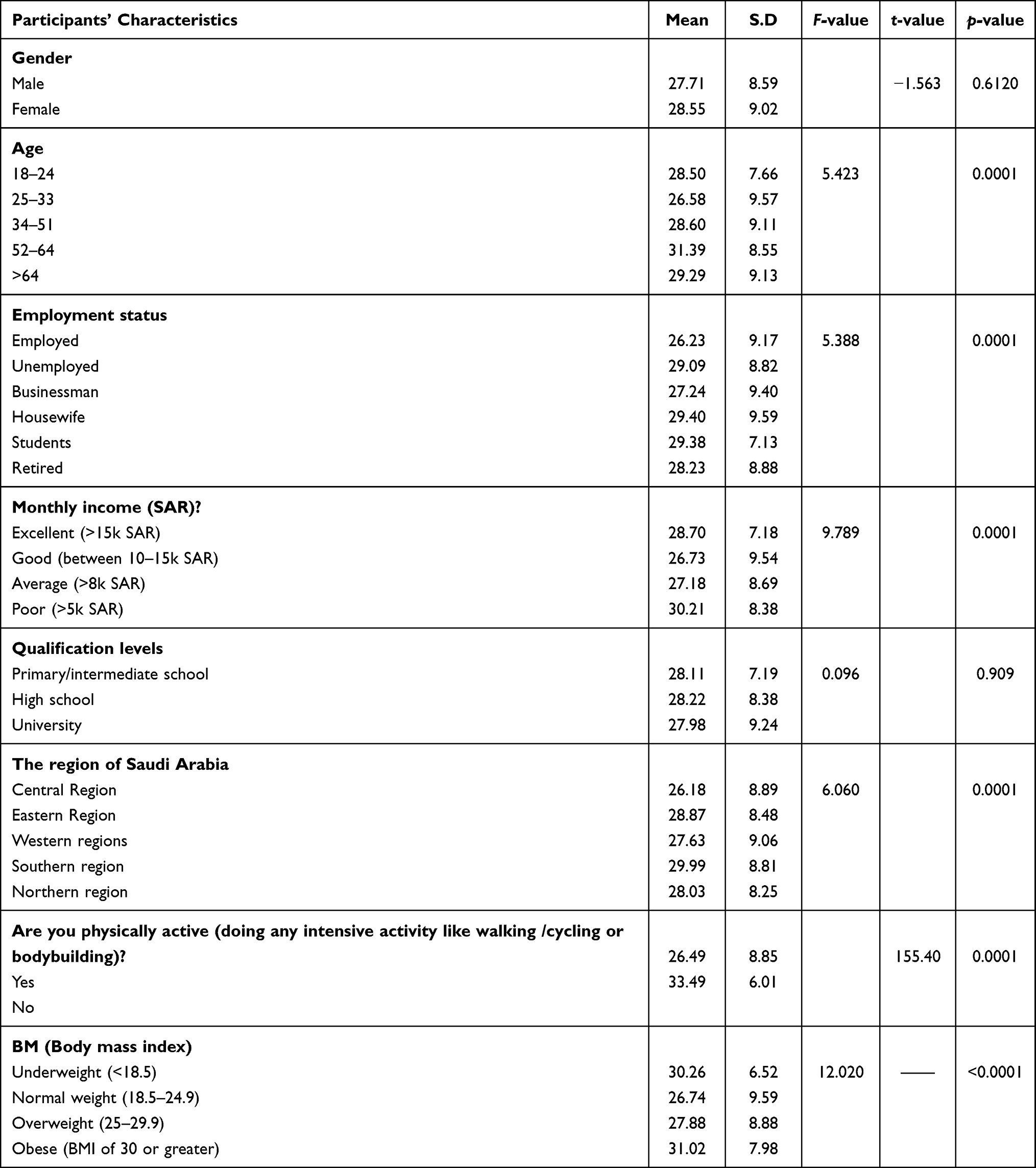 |
Table 7 Association Between View Score and Demographic Characteristics |
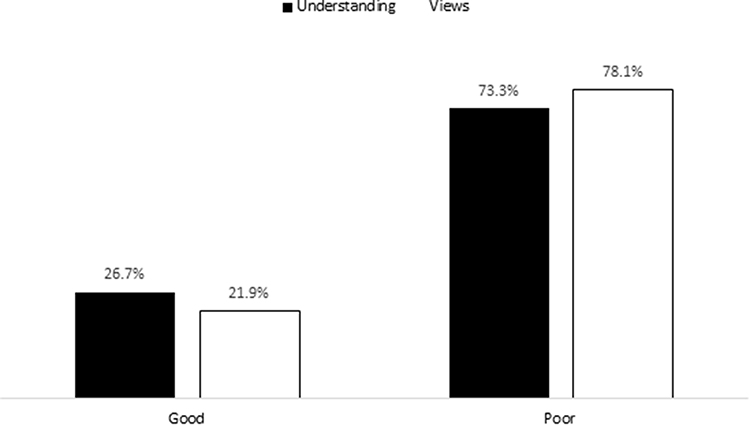 |
Figure 4 Levels of Understanding and Views Toward Overweight and Obesity. |
The current finding revealed that 440 (41.3%) of the males found to have poor understanding of the obesity in comparison to 32% (n=341) of the females. In addition, 14.4% (154) of the males found to have good understanding of obesity comparing to 12.3% (131) of females. However, there was no significant association between the gender and the understanding of the obesity (p=0.503) as shown in the Figure 5. Similarly, the levels of understanding were not significantly associated with the monthly income (p=0.396) Figure 6. In addition, view levels of the obesity were did not found significant. For example, 44.7% (476) of the males found to have poor views towards the obesity in comparison to 33.5% (357) of the females. Although there was no significant association between them. Similarly, the monthly income shows no significant association with respect to the views towards obesity as shown in the Figures 7 and 8.
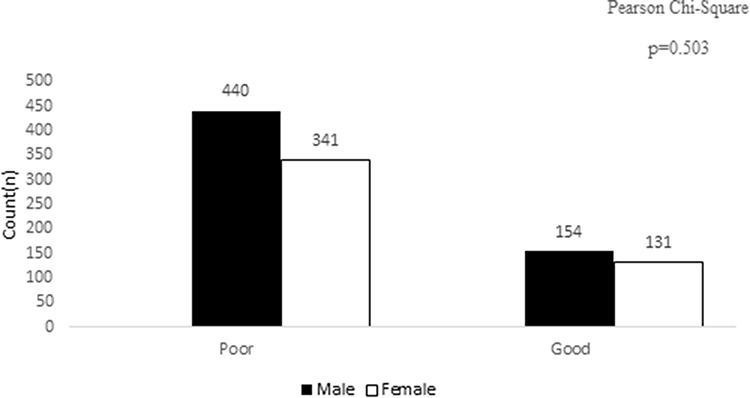 |
Figure 5 Understanding of Obesity According to Gender. |
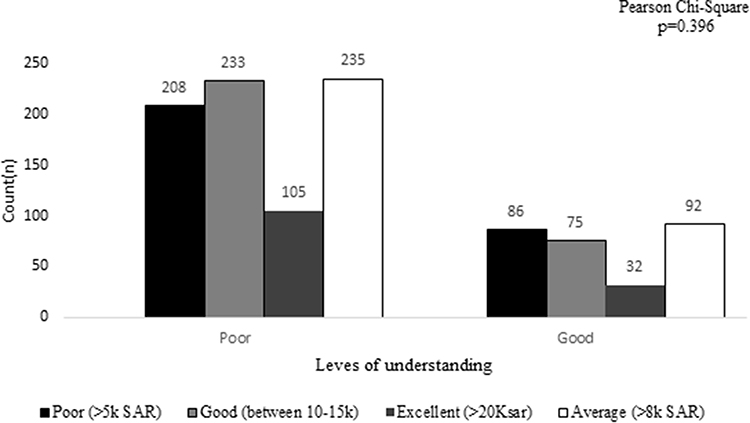 |
Figure 6 Understanding of Obesity According to Income. |
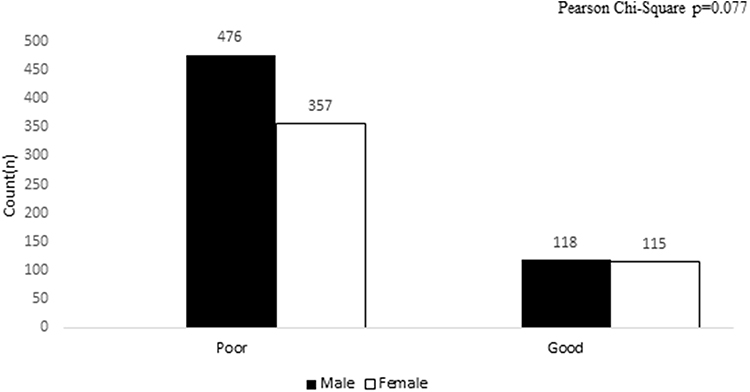 |
Figure 7 Views of Obesity According to Gender. |
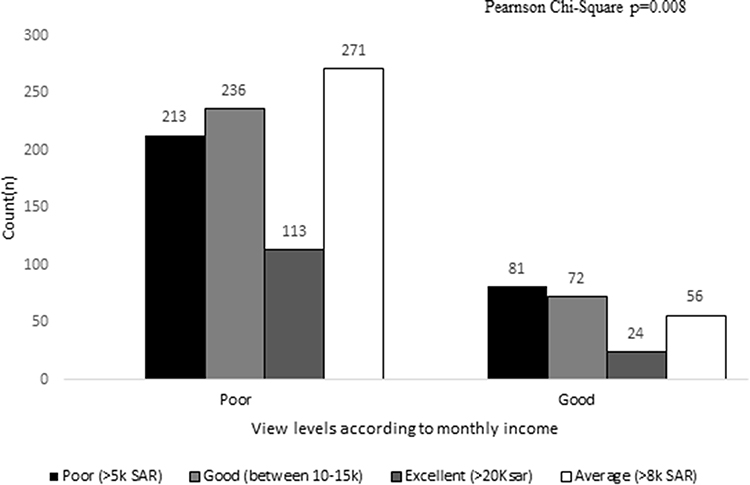 |
Figure 8 Views of Obesity According to Monthly Income. |
However, the results of the multiple linear regression model revealed that there was a significant association between the understanding of obesity, and qualification (SE= 0.015; 95CI= −0.084 to −0.025 p=<.001), physical activity status (SE= 0.033;95Cl = 0.004–0.134; p= 0.038) and presence of chronic diseases (SE= 0.037; 95Cl= −0.221 to −0.074 p=<.001), was the predictor of understanding of obesity as shown in Table 8. Similarly the results of the multiple linear regression revealed that views of the respondents towards obesity was significantly associated with qualification (SE= 0.015; 95Cl= −0.084 to −0.025; p=<.001), Physical activity status (SE= 0.033;95Cl= 0.004–0.134; p = <0.038) and Presence of chronic disease (SE= 0.037; 95 Cl= −0.221- −0.074; p = <0.001) as shown in Table 9. The current findings revealed that understanding and views have a statistically significant linear relationship (r=0.160; p=<.001). Furthermore, the relationship is positive between the understanding and views of the obesity these variables tend to increase together (ie, greater understanding is associated with greater view) as shown in Table 10.
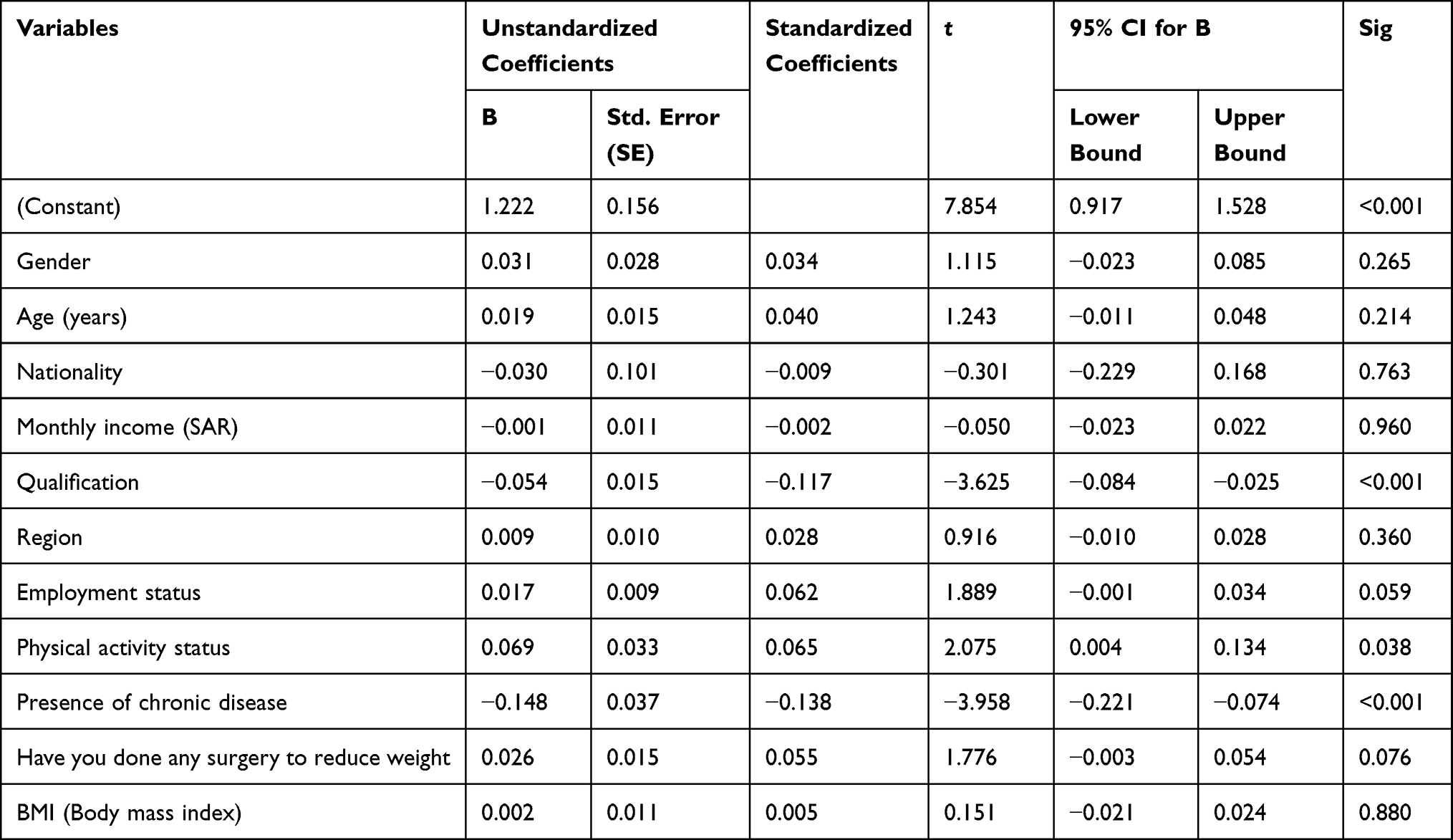 |
Table 8 Multiple Linear Regression Model for Predictors of Understanding of Obesity |
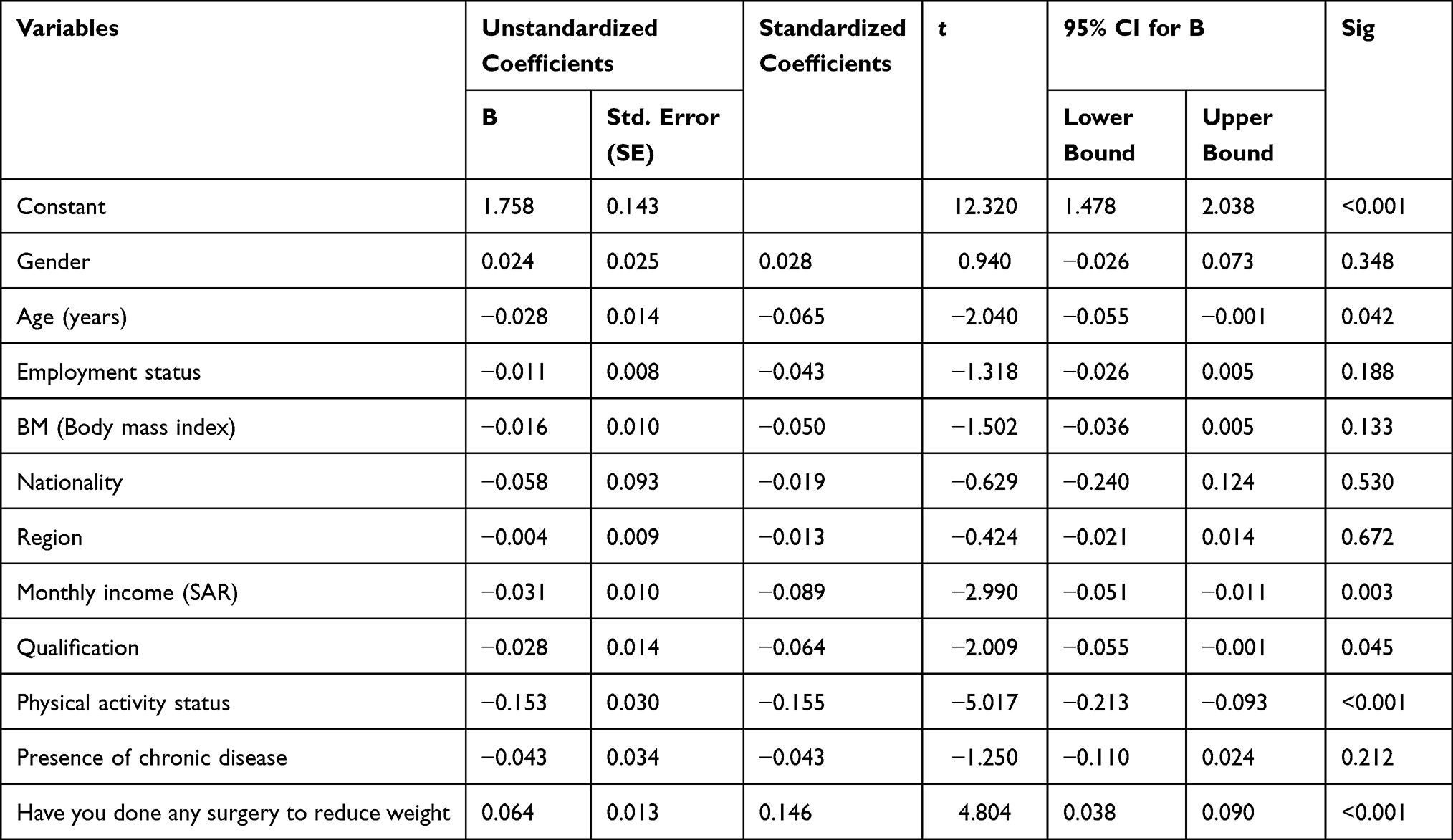 |
Table 9 Multiple Linear Regression Model for Predictors of Views of Obesity |
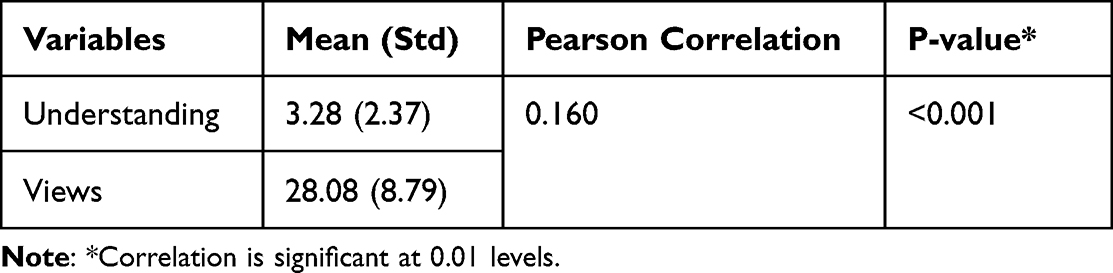 |
Table 10 Correlation Between Understanding and Views |
Discussion
To promote a healthy lifestyle, it is essential to understand and focus on the public’s understanding of and view toward weight management and obesity. This study’s findings revealed that many Saudis possess a poor understanding (73.3%) and views (78.1%) related to obesity and weight management. The understanding and views scores in the current study differed significantly from those of previous studies.34,43–45 For instance, Simkhada et al reported good knowledge but negative attitudes toward obesity in Nepal.34 Similarly, a recent study among adults living in the western region of Saudi Arabia reported mean knowledge and attitudes scores of 20.8 ± 6.8 (range 0–37) and 1.4 ± 1 (range 0–7), respectively.34 Tria et al conducted a similar study in the Philippines and reported adequate knowledge, attitudes, and practices related to weight management;44 however, Alshahrani (2020) reported that the majority of the surveyed participants (85%) had a poor understanding of obesity, and poor attitudes in southern Saudi Arabia.45 It should be pointed out that this study and the above-mentioned previous studies differ in terms of the sample studied, the scoring criteria, and the methodology used.44–46 In this study, 58.9% of the participants were conscious of the relationship between diet and obesity, and 50% knew that smoking and chronic stress are risk factors for obesity. A similar study reported that the participants recognized DM, age, an increased intake of fast food and soft drinks, excessive coffee consumption, and greasy meals as risk factors.46
Most adults in this study (68.7%) agreed that anti-obesity medications are unsafe and are not as effective for obesity management as exercising and following a healthy diet. On the other hand, 25% of the participants showed positive views toward weight loss surgery and agreed it is effective. These results were similar to earlier findings, which reported that most participants would rather lose weight through diet and exercise than through weight loss surgery.6 Although the same study suggested good options for weight loss medication, it acknowledged that these are not necessarily safe.6 Furthermore, medications used to treat obesity should be used over a long period, which may lead to adverse events.47 For example, the USFDA eventually banned the weight management drug lorcaserin from the market since it increased cancer risk. Additionally, behavior-based treatments using one of the prescribed medications under a physician’s supervision can lead to more significant weight loss than that produced by standard care settings. Therefore, medical supervision is recommended to achieve the best outcomes with weight loss medications.47
Many studies have reported that physical activity is the key to better health, preventing various metabolic-related diseases and helping with weight loss. According to the WHO, at least 150–300 minutes of moderate physical activity a week is recommended for healthy adults.48 Therefore, it is important to encourage and promote healthy habits, including physical activity and diet, to prevent the possible incidence of obesity and overweight. On the other hand, it is widely documented that sedentary behavior is associated with people with overweight and obesity, hypertension, diabetes, and cardiovascular diseases.49 Therefore, it is crucial to promote physical activity, given the links in the literature between sedentary lifestyles and poor health outcomes.50–52 Furthermore, public health campaigns are an effective way of raising awareness of the value of physical activity in battling and preventing various weight-related diseases and discouraging sedentary behavior.
In this study, most participants were aware of the treatment for overweight and obesity; for instance, 54.8% were aware of the surgeries for obesity. Similarly, 57.9% were aware of lipid suction and sleeve gastrectomy as ways to lower the fat associated with obesity. On the other hand, a large proportion of the respondents (72.9%) knew that using weight reduction agents could cause side effects. It has been reported that patients believed medications were a safe and effective way of managing obesity, indicating poor knowledge and awareness of obesity.6,53 This indicates that better understanding and views toward obesity medication are required for the public. Creating awareness in society and resolving misconceptions about weight reduction medications could help ensure that individuals maintain good health.
Moreover, it is important to recognize the potential role of dietary supplements and drugs that are not registered for the treatment of obesity in the context of weight management.54,55 Dietary supplements, such as herbal products or over-the-counter weight loss aids, are prevalent among individuals seeking to lose weight.56 However, these supplements often lack robust scientific evidence as many of these products are not regulated by the FDA.57 Future research should focus on clinical trials to determine the effectiveness and safety of these interventions in the context of obesity treatment. Additionally, research should focus on understanding the impact of such interventions on the overall quality of life of patients, including their ability to maintain weight loss in the long term.
In this study, there was a statistically significant association between the participants’ mean understanding and view scores and various demographic features. The mean understanding score was significantly associated with gender, age, employment status, qualifications, monthly income, BMI, and physical activity (p < 0.001). Similarly, the mean view score was significantly associated with age, employment status, monthly income, and BMI. However, gender and qualification levels were not significantly associated with the mean view score (p = 0.612). Our research involved a diverse sample of 1066 respondents, with a substantial proportion being Saudi nationals, reflecting the sociodemographic diversity of the population. We observed gender disparities within our sample, with 55.7% being male and 44.3% female, indicating the potential influence of gender on perceptions of obesity. Additionally, socioeconomic factors emerged as notable determinants, with 54.9% of respondents holding university degrees and 30.7% reporting monthly incomes exceeding 8000 SAR. Our findings further revealed that 22.0% of participants had a history of chronic diseases, while 77.3% were physically active. These disparities highlight the relevance of considering social determinants of health, such as income and education, in understanding obesity awareness. Furthermore, the variations in understanding and views of obesity between different gender groups emphasize the importance of accounting for gender variables in modifying obesity awareness and management strategies. Other national and international studies have reported similar results, for instance, Alhawiti (2019) among the Saudi population residing in Madina;43 Laar et al among Pakistanis;58 and Saleh et al among the Bangladeshi population.59 They all reported that understanding and attitudes toward weight management and obesity were positively associated with the participants’ BMI. Furthermore, researchers have also reported that the higher the participants’ education, the higher their level of knowledge and the better their attitudes toward diseases.30,43,58–62 Some of these factors were modifiable.
It has been demonstrated that psychotherapy, such as cognitive-behavioral therapy (CBT), interpersonal therapy (IPT), or dialectical behavior therapy (DBT), can promote sustainable behavior change and enhance psychological well-being among obese individuals.63,64 The complex nature of obesity makes it essential to integrate psychotherapy into comprehensive treatment plans in order to address the underlying emotional and psychological issues contributing to overeating and weight gain.65 Future studies should aim to explore the effectiveness of different psychotherapeutic interventions and their specific applications within obesity treatment. By incorporating psychotherapy into future research, we can enhance our understanding of the comprehensive treatment approaches necessary to address both obesity physiological and psychological aspects effectively. This is important because psychological issues, such as emotional eating, or lack of motivation to exercise, can be a factor in obesity.66,67 Understanding how to address these psychological aspects can help us to develop more effective treatments for obesity.
In this study, most participants were young, employed, and educated, all of which were highly correlated. Additionally, a lack of exposure to the disease or awareness of disease management may have contributed to this result. Unfortunately, studies examining the general public’s understanding of and views toward obesity and weight management and their association with social factors, particularly in Saudi Arabia, are limited. However, the literature search identified that there had been some studies evaluating the knowledge and attitudes related to obesity and weight management among prospective community pharmacists and other populations.33,45 Hence, the current study’s findings will serve as a reference for upcoming national and international studies.
This study has certain limitations. First, the findings were based on a self-administered questionnaire, which could have increased the risk of biases such as social desirability or recall bias. Second, the findings were based on a specific population, focusing only on Saudis living in Saudi Arabia, making them non-representative of others at national and international levels and, therefore, ungeneralizable. Despite these drawbacks, our research suggests that greater emphasis should be given to educating people about the harmful impacts of people with overweight and obesity to improve the health of everyone in the community. It is imperative to recognize the significance of psychotherapy as a valuable treatment modality for addressing psychological factors that cause obesity. While this study focused on a specific intervention or aspect related to obesity, it did not include psychotherapy as part of the treatment protocol. Psychotherapy, with its focus on exploring emotions, behaviors, and thought patterns, has shown promise in addressing underlying issues such as emotional eating, body image concerns, and self-esteem issues. Its inclusion in future research would provide a more comprehensive understanding of obesity’s multifaceted nature and allow for a more holistic approach to treatment. Given these limitations, the current findings point to the need for further research with a larger sample size, different nationalities living in Saudi Arabia, and a focus on the understanding, views, and practices related to obesity as well as its challenges.
This study demonstrates that people in Saudi Arabia generally lack an understanding of obesity and have poor views toward obesity and weight management. It is well known that obesity is a significant risk factor for coronary heart disease. Those with a body mass index (BMI) higher than the average have an increased risk of heart disease, similar to those with dyslipidemia, hypertension, or are smokers. Therefore, it is essential for those who are considered obese to take steps to reduce their risk of heart disease by making lifestyle changes such as increasing physical activity and eating a healthier diet. Community programs should provide tailored nutrition, physical activity guidance, and social support, which has been demonstrated to lead to weight loss in people with overweight and obesity persons. In addition, these programs should include follow-up assessments to ensure long-term adherence to healthy lifestyle changes. Long-term adherence is essential for successful weight management, as habits adopted for a short duration are unlikely to be maintained. Furthermore, physical activity can help to reduce stress, improve mood, and increase energy levels, all of which can help to reinforce the positive changes that have been made.
The study’s results provide valuable insights into the influence of sociodemographic factors, particularly gender, on individuals’ understanding and views of obesity. The findings revealed a subtle difference in the understanding of obesity, with a slightly higher percentage of males exhibiting a poor understanding compared to female. A similar pattern was observed regarding their views on obesity. However, despite these distinctions, the study did not establish a significant association between gender and the level of understanding or views on obesity. This suggests that gender alone may not be the factor determinant of one’s comprehension of obesity or their perspectives on it. In addition, the study’s exploration of monthly income revealed a lack of a significant relationship with participants’ understanding or views. This suggests that while income may play a role in other aspects of health and well-being, its influence on understanding and views of obesity is limited.
A crucial aspect of the study was its identification of important determinants that shape individuals’ understanding and views of obesity. The multiple linear regression models showed that qualification, physical activity status, and the presence of chronic diseases as significant predictors for both understanding and views of obesity. These findings underscore the essential role of education, physical activity, and health status affecting public perspectives on obesity. The association between higher qualifications and better understanding of obesity suggests that educational interventions and programs could be effective in improving public knowledge on the subject. Similarly, the link between physical activity and positive views on obesity underscores the importance of promoting an active lifestyle as a means to support a more satisfactory outlook on the issue.
Conclusion
The findings of this study shed light on the factors linked to an enhanced understanding and positive perceptions of weight management practices among the participants under evaluation. The results reveal that certain factors, namely age, gender, employment status, higher education and income levels, and regular physical activity engagement, contribute significantly to a greater understanding and more favorable views concerning weight management practices and obesity. Also, over half of the respondents were familiar with the term “obesity”, and a majority recognized that a diet high in carbohydrates, fats, and sugars can lead to obesity. Additionally, the study found that participants had a higher level of knowledge and understanding regarding obesity prevention when they had higher levels of education, income, and physical activity. Furthermore, the majority of participants believed that weight reduction products could be utilized, although they were also aware of the potential side effects associated with their usage. Also, participants felt that dietary changes and increased physical activity were the most appropriate methods for sustained obesity prevention, thus indicating a shift in the perception of weight loss products. The study indicates that factors such as age, gender, employment status, higher education, and income levels, and regular physical activity are associated with increased understanding and favorable views regarding weight management practices and obesity. Moreover, these factors could be used to target those who are not adequately informed and aim to reduce the societal stigma related to obesity. In light of the positive linear relationship between understanding and views of obesity, public health initiatives can strategically prioritize enhancing knowledge to promote more supportive and empathetic societal attitudes towards individuals dealing with obesity, ultimately contributing to a healthier and more inclusive society. These findings provide valuable insights for healthcare professionals and policymakers seeking to develop effective strategies and interventions to enhance awareness and practices related to weight management among various population groups in Saudi Arabia.
Ethical Statement
The study protocol and questionnaire were reviewed and approved by the Biomedical Research Ethics Committee at Umm Al-Qura University (HAPO-02-K-012-2023-01-1364).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any external funds.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Engin A. The definition and prevalence of obesity and metabolic syndrome. Adv Exp Med Biol. 2017;960:1–17.
2. Alluhidan M, Alsukait RF, Alghaith T, et al. Overview: challenges and opportunities for obesity prevention in Saudi Arabia; 2022.
3. Ritchie H, Roser M. Micronutrient Deficiency. Our World in data; 2017.
4. World Health Organization. World Obesity Day 2022-Accelerating Action to Stop Obesity. World Health Organization; 2022.
5. Boutari C, Mantzoros CS. A 2022 Update on the Epidemiology of Obesity and a Call to Action: As Its Twin COVID-19 Pandemic Appears to Be Receding, the Obesity and Dysmetabolism Pandemic Continues to Rage on. Elsevier; 2022:155217.
6. Almubark RA, Alqahtani S, Isnani AC, et al. Gender differences in the attitudes and management of people with obesity in Saudi Arabia: data from the ACTION-IO Study. Risk Manag Healthc Policy. 2022;15:1179–1188. doi:10.2147/RMHP.S346206
7. Chunzhi L. How globalization has impacted on the global trend of obesity epidemic from the perspective of macro factors. In:
8. Alluhidan M. Overweight and Obesity in Saudi Arabia. Washington, DC: World Bank; 2022.
9. Loos RJF, Yeo GSH. The genetics of obesity: from discovery to biology. Nat Rev Genet. 2022;23(2):120–133. doi:10.1038/s41576-021-00414-z
10. Okunogbe A, Nugent R, Spencer G, et al. Economic impacts of overweight and obesity: current and future estimates for eight countries. BMJ Glob Health. 2021;6(10):e006351. doi:10.1136/bmjgh-2021-006351
11. Anekwe CV, Jarrell AR, Townsend MJ, et al. Socioeconomics of Obesity. Curr Obes Rep. 2020;9(3):272–279. doi:10.1007/s13679-020-00398-7
12. Telford RD. Low physical activity and obesity: causes of chronic disease or simply predictors? Med Sci Sports Exerc. 2007;39(8):1233–1240. doi:10.1249/mss.0b013e31806215b7
13. Lavie CJ, Schutter AD, Archer E, et al. Obesity and prognosis in chronic diseases--impact of cardiorespiratory fitness in the obesity paradox. Curr Sports Med Rep. 2014;13(4):240–245. doi:10.1249/JSR.0000000000000067
14. NIH. National institute on aging. Maintaining a Healthy Weight. Available from: https://www.nia.nih.gov/health/maintaining-healthy-weight.Last.
15. NIH. Causes-obesity. Available from: https://www.nhs.uk/conditions/obesity/causes/.
16. Roth CL, Elfers C, Kratz M, et al. Vitamin d deficiency in obese children and its relationship to insulin resistance and adipokines. J Obes. 2011;2011:495101. doi:10.1155/2011/495101
17. Somannavar MS, Appajigol JS. Knowledge, attitudes, and practices of public sector primary health care physicians of rural north Karnataka towards obesity management. J Family Med Prim Care. 2014;3(4):400–403. doi:10.4103/2249-4863.148126
18. Astrup A, Raben A, Geiker N. The role of higher protein diets in weight control and obesity-related comorbidities. Int J Obes. 2015;39(5):721–726. doi:10.1038/ijo.2014.216
19. Bluher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019;15(5):288–298. doi:10.1038/s41574-019-0176-8
20. Haththotuwa RN, Wijeyaratne CN, Senarath U. Worldwide Epidemic of Obesity, in Obesity and Obstetrics. Elsevier; 2020:3–8.
21. Hill A, Williams G, Fruhbeck G. Social and psychological factors in obesity. Obesity. 2009;2009:347–366.
22. Robinson E, Roberts C, Vainik U, et al. The psychology of obesity: an umbrella review and evidence-based map of the psychological correlates of heavier body weight. Neurosci Biobehav Rev. 2020;119:468–480. doi:10.1016/j.neubiorev.2020.10.009
23. Freshwater M, Christensen S, Oshman L, et al. Behavior, motivational interviewing, eating disorders, and obesity management technologies: an obesity medicine association (OMA) clinical practice statement (CPS) 2022. Obesity Pillars. 2022;2:100014. doi:10.1016/j.obpill.2022.100014
24. Moradi M, Mozaffari H, Askari M, et al. Association between overweight/obesity with depression, anxiety, low self-esteem, and body dissatisfaction in children and adolescents: a systematic review and meta-analysis of observational studies. Crit Rev Food Sci Nutr. 2021;62(2):555–570. doi:10.1080/10408398.2020.1823813
25. KavehFarsani Z, Kelishadi R, Beshlideh K. Study of the effect of family communication and function, and satisfaction with body image, on psychological well-being of obese girls: the mediating role of self-esteem and depression. Child Adolesc Psychiatry Ment Health. 2020;14:39. doi:10.1186/s13034-020-00345-3
26. Alsanea S, Alrabiah Z, Samreen S, et al. Prevalence, knowledge and attitude toward electronic cigarette use among male health colleges students in Saudi Arabia—A cross-sectional study. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.827089
27. Samreen S, Siddiqui NA, Mothana RA. Prevalence of anxiety and associated factors among pharmacy students in Saudi Arabia: a Cross-Sectional Study. Biomed Res Int. 2020;2020:1–6. doi:10.1155/2020/2436538
28. Sales IA, Syed W, Almutairi MF, et al. Public knowledge, attitudes, and practices toward seasonal influenza vaccine in Saudi Arabia: a cross-sectional study. Int J Environ Res Public Health. 2021;18(2):479. doi:10.3390/ijerph18020479
29. Samreen S, Sales I, Bawazeer G, et al. Assessment of beliefs, behaviors, and opinions about blood donation in Telangana, India—a cross sectional community-based study. Front Public Health. 2021;9:785568. doi:10.3389/fpubh.2021.785568
30. Syed W, Alharbi MK, Samarkandi OA, et al. Evaluation of knowledge, awareness, and factors associated with diabetes: a cross-sectional community-based study. Int J Endocrinol. 2022;2022:1921010. doi:10.1155/2022/1921010
31. Syed W, Samarkandi OA, Alsadoun A, et al. Evaluation of clinical knowledge and perceptions about the development of thyroid cancer—an observational study of healthcare undergraduates in Saudi Arabia. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.912424
32. Wajid S, Samreen S, Sales I, et al. What has changed in the behaviors of the public after the COVID-19 pandemic? A cross-sectional study from the Saudi community perspective. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.723229
33. Njelekela MA, Muhihi A, Mpembeni RM, et al. Knowledge and attitudes towards obesity among primary school children in Dar es Salaam, Tanzania. Niger Med J. 2015;56(2):103. doi:10.4103/0300-1652.150692
34. Simkhada P, Poobalan A, Simkhada PP, et al. Knowledge, attitude, and prevalence of overweight and obesity among civil servants in Nepal. Asia Pacific J Public Health. 2011;23(4):507–517. doi:10.1177/1010539509348662
35. Al-Khaldi YM, Al-Shehri F, Aljoudi A, et al. Towards an integrated national obesity control program in Saudi Arabia. Saudi J Obesity. 2014;2(2):49. doi:10.4103/2347-2618.147342
36. Tashkandi MA, Almalki MA, Alhazmi AA, et al. Assessment of prevalence and factors associated with obesity among secondary school students at Makkah in Saudi Arabia 2021. Anna Roman Soc Cell Biol. 2021;25(7):2284–2294.
37. Association AD. Position of the American Dietetic Association: weight management. J Am Diet Assoc. 2009;109(2):330–346.
38. De Lorenzo A, Romano L, Di Renzo L, et al. Obesity: a preventable, treatable, but relapsing disease. Nutrition. 2020;71:110615. doi:10.1016/j.nut.2019.110615
39. Ng ACT, Delgado V, Borlaug BA, et al. Diabesity: the combined burden of obesity and diabetes on heart disease and the role of imaging. Nat Rev Cardiol. 2021;18(4):291–304. doi:10.1038/s41569-020-00465-5
40. Weinberger NA, Luck-Sikorski C. Body appreciation and appearance evaluation in individuals with obesity compared to individuals with normal-weight: findings from a representative German population sample. Eat Weight Disord. 2021;26(7):2241–2249. doi:10.1007/s40519-020-01071-7
41. Sarigiani PA, Olsavsky AL, Camarena PM, et al. Obesity and depressive symptoms in college women: analysis of body image experiences and comparison to non-obese women. Int J Adolesc Youth. 2020;25(1):765–779. doi:10.1080/02673843.2020.1740751
42. Haire-Joshu D, Tabak R. Preventing obesity across generations: evidence for early life intervention. Annu Rev Public Health. 2016;37:253–271. doi:10.1146/annurev-publhealth-032315-021859
43. Alhawiti RM. Knowledge, attitude, and practice about obesity among adults (18-45 years) in primary health care in Medina, KSA 2019. Age. 2021;18(28):101.
44. Tria DMM, Africa LS, Barrion AS, et al. Knowledge, attitude and practices of adults on cholesterol management in CALABARZON region. Acta Med Philipp. 2021;55:4.
45. Alshahrani SM. Assessment of knowledge, attitudes, and practice of community pharmacists regarding weight reduction agents and supplements in aseer region, Saudi Arabia. Risk Manag Healthc Policy. 2020;13:347. doi:10.2147/RMHP.S234818
46. Oyewande AA, Ademola A, Okuneye T, et al. Knowledge, attitude and Perception regarding risk factors of overweight and obesity among secondary school students in Ikeja Local Government Area, Nigeria. J Fam Med Primary Care. 2019;8(4):1391. doi:10.4103/jfmpc.jfmpc_160_19
47. Tak YJ, Lee SY. Anti-obesity drugs: long-term efficacy and safety: an updated review. World J Mens Health. 2021;39(2):208–221. doi:10.5534/wjmh.200010
48. World health organization. Physical activity. Available from: https://www.who.int/health-topics/physical-activity#tab=tab_1.
49. Samarkandi OA. Prevalence of physical activity among healthcare students in King Saud University, Riyadh, Saudi Arabia. An observational study. INQUIRY. 2022;59:00469580221100157.
50. Biswas A, Oh PI, Faulkner GE, et al. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Ann Intern Med. 2015;162(2):123–132. doi:10.7326/M14-1651
51. Patterson R, McNamara E, Tainio M, et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Eur J Epidemiol. 2018;33(9):811–829. doi:10.1007/s10654-018-0380-1
52. Guo C, Zhou Q, Zhang D, et al. Association of total sedentary behaviour and television viewing with risk of overweight/obesity, type 2 diabetes and hypertension: a dose-response meta-analysis. Diabetes Obes Metab. 2020;22(1):79–90. doi:10.1111/dom.13867
53. Sharaf S, Al-shalabi BT, Althani GF, et al. Obesity self-management: knowledge, attitude, practice, and pharmaceutical use among healthy obese individuals in Saudi Arabia. Int J Fam Community Med. 2021;5(4):110–121. doi:10.15406/ijfcm.2021.05.00232
54. Ríos-Hoyo A, Gutiérrez-Salmeán G. New dietary supplements for obesity: what we currently know. Curr Obes Rep. 2016;5:262–270. doi:10.1007/s13679-016-0214-y
55. Barrea L, Altieri B, Polese B, et al. Nutritionist and obesity: brief overview on efficacy, safety, and drug interactions of the main weight-loss dietary supplements. Int J Obes Suppl. 2019;9(1):32–49. doi:10.1038/s41367-019-0007-3
56. Bonetti G, Herbst KL, Donato K, et al. Dietary supplements for obesity. J Prev Med Hyg. 2022;63(2):E160–E168. doi:10.15167/2421-4248/jpmh2022.63.2S3.2757
57. Kidambi S, Batsis JA, Donahoo WT, et al. Dietary supplements and alternative therapies for obesity: a Perspective from The Obesity Society’s Clinical Committee. Obesity. 2021;29(7):1095–1098. doi:10.1002/oby.23189
58. Laar RA, Shi S, Ashraf MA, et al. Impact of physical activity on challenging obesity in Pakistan: a knowledge, attitude, and practice (KAP) study. Int J Environ Res Public Health. 2020;17(21):7802. doi:10.3390/ijerph17217802
59. Saleh F, Mumu SJ, Ara F, et al. Knowledge, attitude and practice of type 2 diabetic patients regarding obesity: study in a tertiary care hospital in Bangladesh. J Public Health Africa. 2012;3(1). doi:10.4081/jphia.2012.e8
60. Wajid S, N. Al-Arifi M, Babelghaith SD, et al. Pharmacy students’ knowledge and attitudes towards diabetes: a cross-sectional study. Bio Res. 2018;29(19):3638–3642. doi:10.4066/biomedicalresearch.29-18-1074
61. Syed W, Menaka M, Parimalakrishnan S, Yamasani VV. A study on diabetes-related self-care plan and its determinants among diabetes patients in a Warangal region, Telangana, India. Brazil J Pharm Sci. 2023;2023:58.
62. Syed W, Menaka M, Parimalakrishnan S, et al. Evaluation of the association between social determinants and health-related quality of life among diabetic patients attending an outpatient clinic in the Warangal region, Telangana, India. J Diabetol. 2022;13(3):285. doi:10.4103/jod.jod_51_22
63. Becker S, Rapps N, Zipfel S. Psychotherapie bei Adipositas - Ein systematischer Überlick [Psychotherapy in obesity--a systematic review]. Psychother Psychosom Med Psychol. 2007;57(11):420–427. German. doi:10.1055/s-2007-986202
64. Teufel M, Becker S, Rieber N, et al. Psychotherapie und Adipositas [Psychotherapy and obesity: strategies, challenges and possibilities]. Nervenarzt. 2011;82(9):1133–1139. German. doi:10.1007/s00115-010-3230-2
65. Plourde G, Prud’homme D. Managing obesity in adults in primary care. CMAJ. 2012;184(9):1039–1044. doi:10.1503/cmaj.111640
66. Andrade AM, Coutinho SR, Silva MN, et al. The effect of physical activity on weight loss is mediated by eating self-regulation. Patient Educ Couns. 2010;79(3):320–326. doi:10.1016/j.pec.2010.01.006
67. Geiker NRW, Astrup A, Hjorth MF, et al. Does stress influence sleep patterns, food intake, weight gain, abdominal obesity and weight loss interventions and vice versa? Obes Rev. 2018;19(1):81–97. doi:10.1111/obr.12603
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Is Intermittent Fasting Better Than Continuous Energy Restriction for Adults with Overweight and Obesity?
Ye YF, Zhang MX, Lin Z, Tang L
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2813-2826
Published Date: 15 September 2022
Correlation of Obesity and Overweight with Cervical Vascular Function Among Healthy Populations
Pan X, Chen X, Ren L, Li Z, Chen S
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2927-2938
Published Date: 25 September 2022
Association Between Nutritional Knowledge, Dietary Regimen, and Excess Body Weight in Primary School Teachers
Saintila J, Calizaya-Milla YE, Calizaya-Milla SE, Elejabo-Pacheco AA, Sandoval-Valentin GA, Rodriguez-Panta SG
Journal of Multidisciplinary Healthcare 2022, 15:2331-2339
Published Date: 14 October 2022
Patient and Healthcare Professional Preferences for Prescription Weight Loss Medications in Australia: Two Discrete Choice Experiments
Fifer S, Keen B, Porter A
Patient Preference and Adherence 2024, 18:435-454
Published Date: 19 February 2024
The Economic Impact of Obesity in Turkey: A Micro-Costing Analysis
Gogas Yavuz D, Akhtar O, Low K, Gras A, Gurser B, Yilmaz ES, Basse A
ClinicoEconomics and Outcomes Research 2024, 16:123-132
Published Date: 5 March 2024