Back to Journals » Journal of Pain Research » Volume 16
Sarcopenia and Chronic Pain in the Elderly: A Systematic Review and Meta-Analysis
Received 12 September 2023
Accepted for publication 17 October 2023
Published 26 October 2023 Volume 2023:16 Pages 3569—3581
DOI https://doi.org/10.2147/JPR.S435866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kushang V Patel
Jintao Chen,1 Xinyi Wang,1 Zherong Xu2
1The First Affiliated Hospital, Zhejiang University, School of Medicine, Hangzhou, People’s Republic of China; 2Department of Geriatrics, The First Affiliated Hospital, Zhejiang University, School of Medicine, Hangzhou, People’s Republic of China
Correspondence: Zherong Xu, Email [email protected]
Objective: Sarcopenia and chronic pain are prevalent among older adults, and despite numerous studies, the potential epidemiological link between the two conditions remains a topic of controversy. Therefore, we performed a comprehensive systematic review and meta-analysis to assess the relationship between chronic pain and sarcopenia in the elderly.
Methods: EMBASE, Web of Science, PubMed, and the Cochrane Library were searched through 22 March 2023 with additional manual searches of reference lists of included studies and relevant reviews. We used a random effects model to conduct the meta-analysis and evaluated heterogeneity across studies with Cochran’s Q statistic and I2. Subgroup analyses were conducted based on income level, diagnostic criteria for sarcopenia, and pain site.
Results: 17 observational studies (33,600 participants, 49% female) were included, of which 6 articles were retrieved for narrative review. The pooled prevalence of sarcopenia and the pooled odds ratios (OR) between chronic pain and sarcopenia were extracted from the remaining 11 studies. The pooled prevalence of sarcopenia among older adults suffering from chronic pain was 0.11 (95% CI, 0.08– 0.18). Our analysis revealed a statistically significant positive association between chronic pain and an increased risk of sarcopenia, yielding a pooled OR of 1.52 (95% CI, 1.31– 1.76). Furthermore, our subgroup analysis demonstrated that the low-income countries group showed a stronger association (OR, 1.73; 95% CI, 1.54– 1.95) between chronic pain and sarcopenia than the high-income countries group (OR, 1.38; 95% CI, 1.20– 1.60).
Conclusion: Older adults with chronic pain have a significantly higher prevalence of sarcopenia and risk of developing sarcopenia compared to those without pain. These findings highlight the importance of prioritizing the assessment and early detection of chronic pain in older people, as well as implementing proactive intervention measures in clinical practice. In addition, our results suggest that older people with chronic pain should be actively screened for sarcopenia.
Prospero Registration Number: CRD42021239807.
Keywords: the elderly, chronic pain, sarcopenia, meta-analysis
Introduction
Sarcopenia is an age-related syndrome characterized by pathological loss of muscle mass and quality, leading to low muscle strength and/or impaired physical performance.1 It has gradually been found to be associated with a range of negative outcomes such as falls, disability, hospitalization, and death, and is a significant cause of the need for long-term care in older adults.2,3 As the global population ages, sarcopenia is now a global threat. To date, there is still a lack of effective drugs to treat sarcopenia.4 Therefore, it is particularly important to identify the risk factors associated with this disease to reduce its onset in older adults.
Chronic pain is defined as pain that persists beyond the normal healing time.5 Unlike acute pain, chronic pain presents in pathological ways, causing significant distress to the affected individual.6 It is highly prevalent among the elderly population, affecting approximately 30% to 50% of community-dwelling individuals.7 Chronic pain has been linked to reduced mobility, immobility, sedentary behavior, falls, chronic stress, depression, anxiety, sleep disturbances, and frailty.8–10 These chronic pain-related adverse outcomes are considered underlying factors of risk for the advancement of sarcopenia.11 Furthermore, there appear to be shared pathophysiological mechanisms between sarcopenia and chronic pain, such as elevated circulating levels of pro-inflammatory factors and oxidative stress.12,13
The relationship between sarcopenia and chronic pain has not yet been clearly elucidated. Studies have shown that people with sarcopenia tend to report higher rates of pain compared to non-sarcopenic populations.14 However, whether chronic pain increases the risk of sarcopenia, sarcopenia exacerbates pain, or there is an interaction between the two remains controversial. A prospective cohort study of the Health, Aging, and Body Composition found pain to be a predictor of transition towards sarcopenia.15 In contrast, a cross-sectional study from Japan reported that chronic pain in the elderly was not associated with sarcopenia.16 Similarly, a prospective cohort study conducted in England revealed that only severe pain was linked to sarcopenia, while moderate or mild pain did not show any significant correlation. The researchers suggest that this result could be attributed to the use of medication prescribed for severe pain, which likely has a crucial role in the link between sarcopenia and pain.17 Furthermore, although the results of a recent systematic review and meta-analysis of 14 observational studies showed a significant correlation between pain and sarcopenia, the majority of the studies included in this analysis were case-control studies, with some studies having a relatively young average age and all studies being from high-income countries. This may lead to heterogeneity in the results, which could affect the reliability and applicability of the meta-analysis.18 Therefore, we performed a comprehensive systematic review and meta-analysis to assess the relationship between chronic pain and sarcopenia in the elderly. Our primary objective was to determine whether there was significant variation in the occurrence of sarcopenia between older adults with and without chronic pain, and to uncover possible connections between chronic pain and sarcopenia. Our secondary objectives were to evaluate whether the location of pain, the diagnostic criteria for sarcopenia, or the level of income affects the correlation between chronic pain and sarcopenia.
Methods
Protocol Registration
This review had adhered to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines19 for conducting and reporting systematic reviews and meta-analyses and had a registered protocol with the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42023416618 (Supplementary Table 1).
Search Strategy and Selection Criteria
We conducted a comprehensive literature search across multiple databases including EMBASE, PubMed, the Cochrane Library, and the Web of Science. Our search utilized Medical Subject Headings (MeSH) terms in combination with relevant free-text terms (“muscle atrophy”, “sarcopenia”, “chronic pain”, “pain”, “low back pain”, “musculoskeletal pain”, “neuralgia”, “arthralgia”, and “fibromyalgia”) to ensure a thorough search from the inception of the databases to March 22, 2023 (Supplementary Table 2). We limited our search to human studies and also manually reviewed the reference lists of included studies and relevant reviews to identify additional articles. To ensure consistency, two independent authors (J.T. Chen and X.Y. Wang) performed the title/abstract eligibility screening using a pre-planned list of inclusion/exclusion criteria. Any discrepancies were resolved through discussion with the corresponding author (Z.R. Xu). In cases where there were overlapping cohorts, we prioritized studies with larger sample sizes or more data available for subgroup analysis.
We included studies meeting these criteria: (1) no language restrictions; (2) cross-sectional, case-control, and cohort studies examining the association between sarcopenia and chronic pain in older adults; (3) application of a validated and approved consensus or scale (eg European Working Group on Sarcopenia in Older People and the Asian Working Group for Sarcopenia, etc.), to distinguish between participants with and without sarcopenia; and (4) reporting of chronic primary pain syndromes, chronic postsurgical or posttraumatic pain, chronic neuropathic pain, chronic secondary headache or orofacial pain, chronic secondary visceral pain, or chronic secondary musculoskeletal pain, based on the latest World Health Organization criteria for chronic pain classification.
We excluded studies that met the following criteria: (1) abstracts of meetings, case reports, letters, comments, or editorials; (2) cancer-related pain and rheumatoid arthritis pain, the pain-causing diseases themselves increase the risk of myasthenia; and (3) average age was less than 60 years old.
Data Extraction and Study Quality Assessment
Two independent authors (J.T. Chen and X.Y. Wang) utilized a standardized data extraction table to extract data from each included study. The extracted data included various parameters such as the first author’s name, publication year, country of study, study design, sample size, mean age, proportion of females, diagnostic criteria for sarcopenia, measurement tool for muscle mass, pain assessment method, number of sarcopenic individuals with chronic pain, number of individuals with chronic pain, number of non-chronic pain sarcopenic individuals, number of individuals with non-chronic pain, pain location, and confounding variables. The primary objective of the study was to determine the prevalence of sarcopenia in older adults with chronic pain, and investigate the relationship between chronic pain and sarcopenia, along with its influencing factors. The results were expressed using odds ratios (OR) and 95% confidence intervals (CI).
The quality of included studies was also assessed by two authors (J.T. Chen and X.Y. Wang) using a scale in accordance with the Newcastle-Ottawa scale (NOS). Assessments were conducted independently, and any disagreements were resolved through discussions with the corresponding author (Z.R. Xu).
Statistical Analysis
In this study, the eligible study data was subjected to a meta-analysis using the Cochrane Collaboration Review Manager (RevMan 5.4) software. To avoid overestimation of effect sizes, all analyses were performed using a random effects model and heterogeneity across studies was assessed via Cochran’s Q statistic and I2. Significant heterogeneity was defined as I2>50% or P value of Q statistic<0.1. Pre-planned subgroup analyses were performed based on income level (According to the country of residence of the study population, the included studies were categorized into a group of lower- and middle-income countries and a group of high-income countries.), diagnostic criteria for sarcopenia, and pain site (Based on whether the studies differentiate specific pain sites, the included studies were categorized into a group that does not differentiate pain locations and a group that focuses on pain in the lower back or limbs.). Sensitivity analyses were carried out by systematically excluding one study at a time and pooling the remaining studies. Additionally, publication bias was evaluated using funnel plots. The significance level for all analyses was set at p<0.05 (two-tailed).
Results
Study Selection and Characteristics of Included Studies
Out of 16,006 articles identified through electronic database searches, 2254 duplicates and 13,696 ineligible titles/abstracts were excluded. In addition, 2 relevant studies were obtained by manually reviewing the reference lists of the included studies and related reviews. Following a full-text review of the remaining 56 articles, 39 were excluded according to the pre-defined criteria. Ultimately, 17 studies were deemed eligible for qualitative review, with 11 articles included in the subsequent meta-analysis (Figure 1).
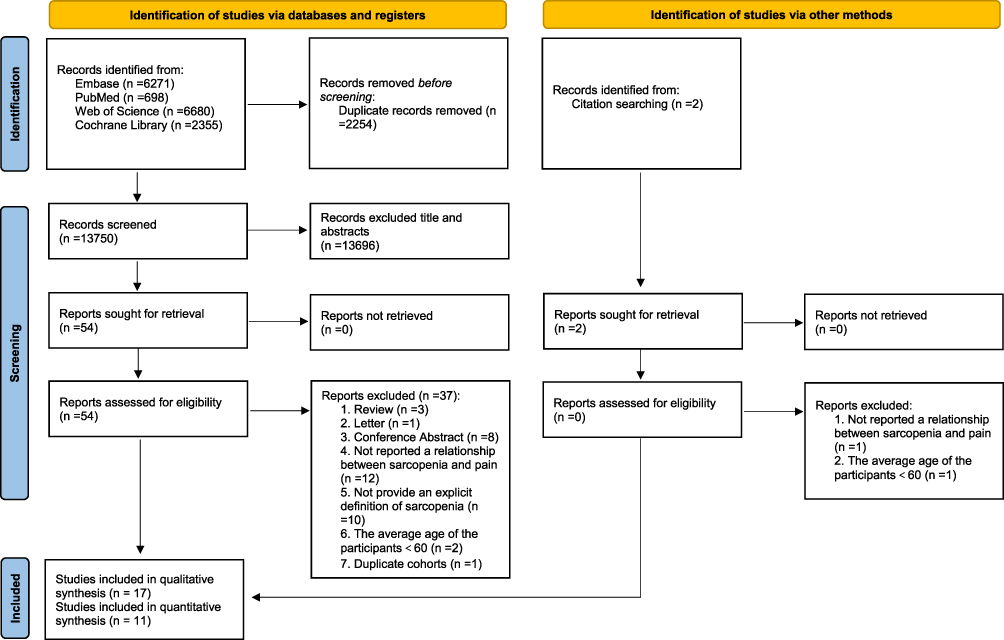 |
Figure 1 The PRISMA flow chart for the study selection process. |
Table 1 presents a summary of the characteristics of all included studies. Of the 17 studies, 14 were conducted in high-income countries and 3 in low- and middle-income countries. Cross-sectional studies accounted for 11 of the 17 studies, while 6 were prospective cohort studies. The sample size of the included studies ranged from 72 to 14,585, with a total of 33,600 individuals across all 17 studies. The average age of the participants ranged from 63.5 to 81.5 years. The results of the NOS quality assessment for the studies included in the quantitative analysis were rated as moderate to high quality (Supplementary Table 3).
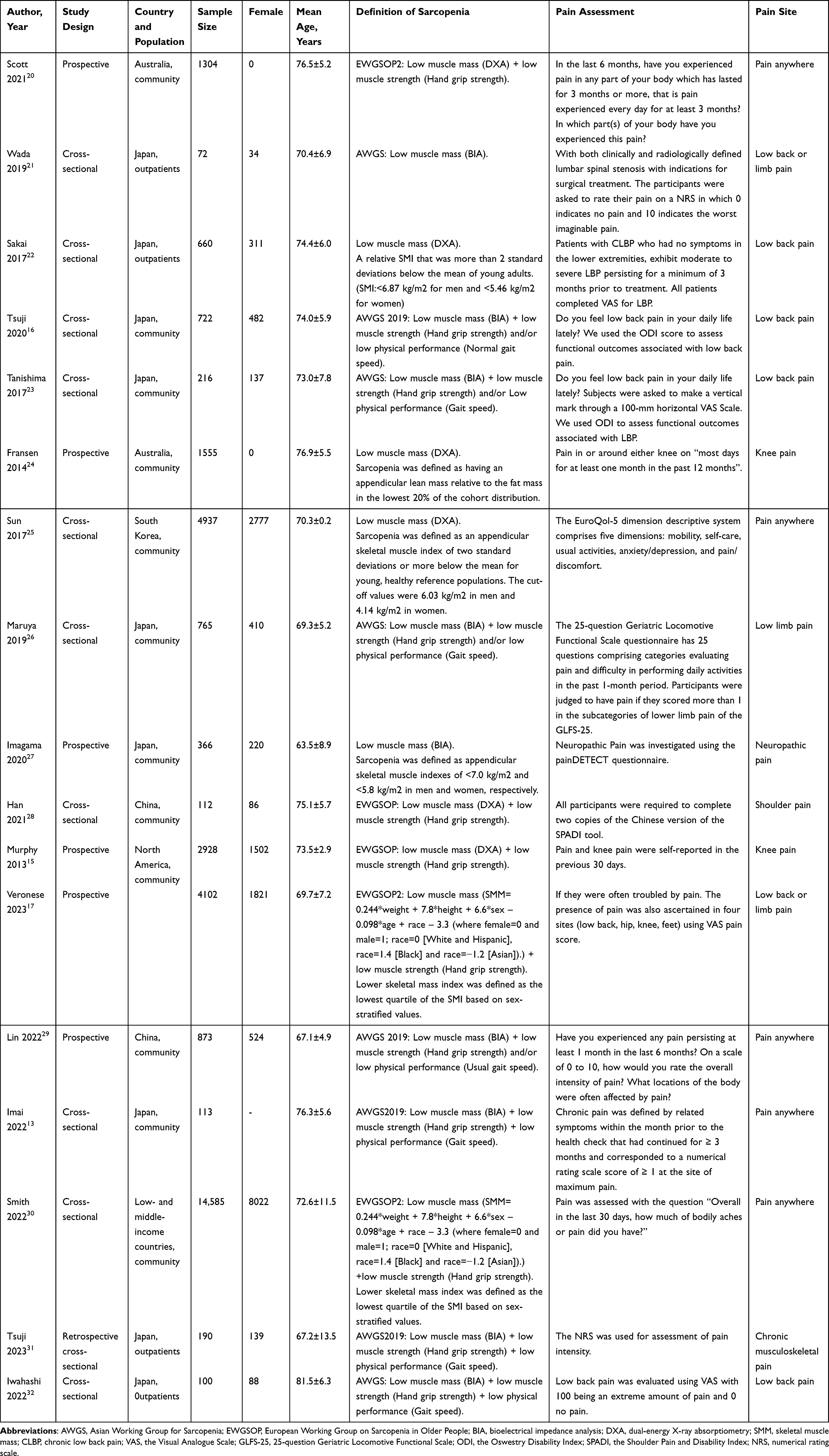 |
Table 1 Summary Characteristics of Included Studies (n=17) |
Among the included studies, 5 studies employed muscle mass alone as the diagnostic criterion for sarcopenia, whereas 12 studies used a combination of muscle mass and grip strength as the diagnostic criterion. Regarding the measurement of muscle mass, dual-energy X-ray absorptiometry (DXA) was used in 7 studies, bioelectrical impedance analysis (BIA) in 8 studies, and a validated equation estimation in 2 studies.
In the included studies, pain assessment methods have shown considerable diversity. For example, the 25-question Geriatric Locomotive Functional Scale questionnaire, the EuroQol-5 dimension, the painDETECT questionnaire, and the Shoulder Pain and Disability Index (SPADI) tool were used to determine the presence or absence of pain. However, about 8 studies used a similar question, such as “Do you feel pain in your daily life or last for a month or more?” Most of the studies did not provide information about the specific location of pain, while 7 studies explored the specific location of pain, such as low back, hip, or knee pain. In addition, most studies used a visual analog scale or a numerical rating scale as a tool to measure pain severity.
Sarcopenia and Chronic Pain
In the absence of a dichotomous classification for chronic pain and sarcopenia, we conducted a narrative synthesis of six studies. Among them, three demonstrated that individuals with sarcopenia in chronic pain populations were more prone to experiencing higher levels of pain than those without sarcopenia.21,31,32 Notably, one study identified pain as a predictive factor for the transition from a normal state to sarcopenia.15 Furthermore, one study found individuals with sarcopenia are more likely to develop shoulder pain than those without the condition.28 Similarly, another study revealed an association between sarcopenia and the onset of new neuropathic pain.27 All the six studies supported a potential link between chronic pain and sarcopenia.
Prevalence of Sarcopenia Among Older Adults with Chronic Pain
Prevalence data for sarcopenia were extracted from 11 remaining studies (n=29,832),13,16,17,20,22–26,29,30 yielding a cumulative prevalence of 0.11 (95% CI, 0.08–0.14) (Figure 2). Subgroup analysis revealed a slightly higher prevalence of sarcopenia in low- and middle-income countries (0.12, 95% CI, 0.09–0.16) than in high-income countries (0.11, 95% CI, 0.07–0.15). Moreover, the prevalence of sarcopenia was higher in the group using only muscle mass as the diagnostic criterion (0.14, 95% CI, 0.06–0.22) than in the group using grip strength and/or physical performance as part of the diagnostic criteria (0.10, 95% CI, 0.07–0.14). Additionally, the incidence of sarcopenia was observed to be greater in individuals who reported experiencing low back or limb pain (0.12, 95% CI, 0.06–0.17) as opposed to those who did not distinguish between pain locations (0.10, 95% CI, 0.06–0.15) (Table 2).
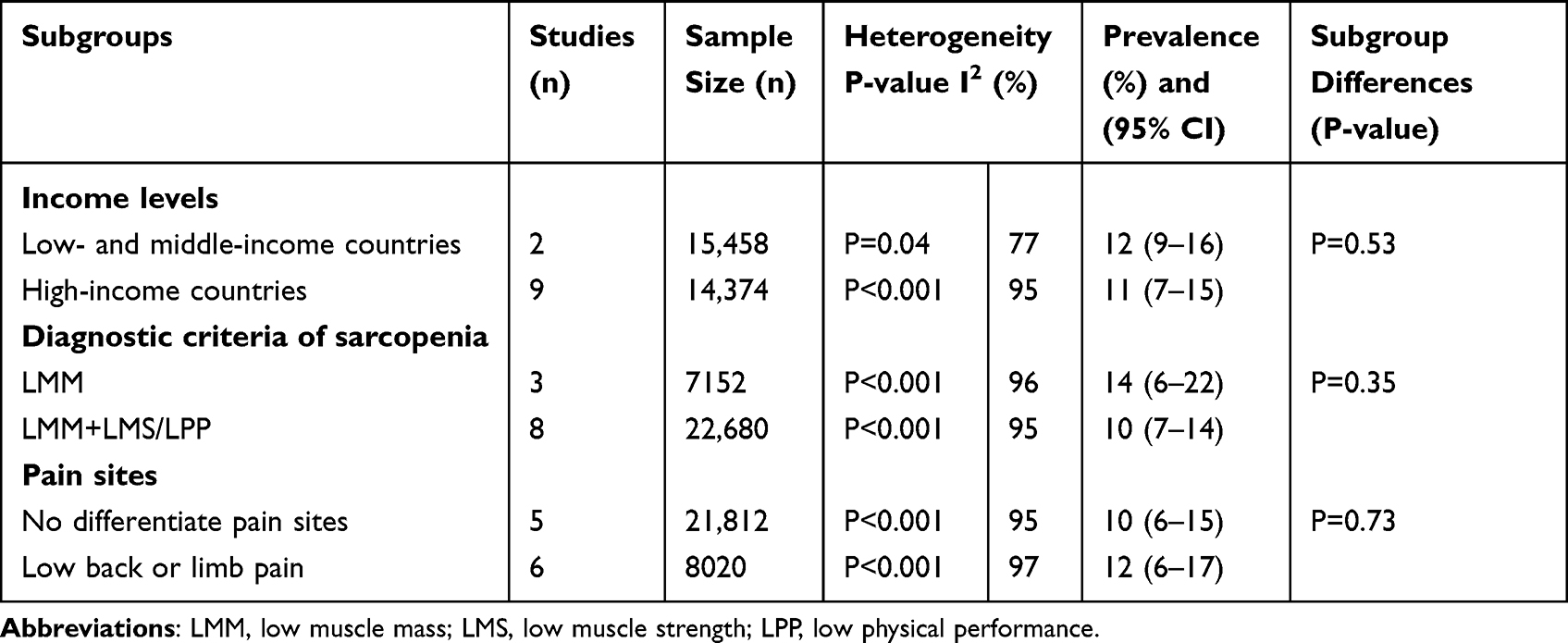 |
Table 2 Subgroup Analyses of the Prevalence of Sarcopenia in People with Chronic |
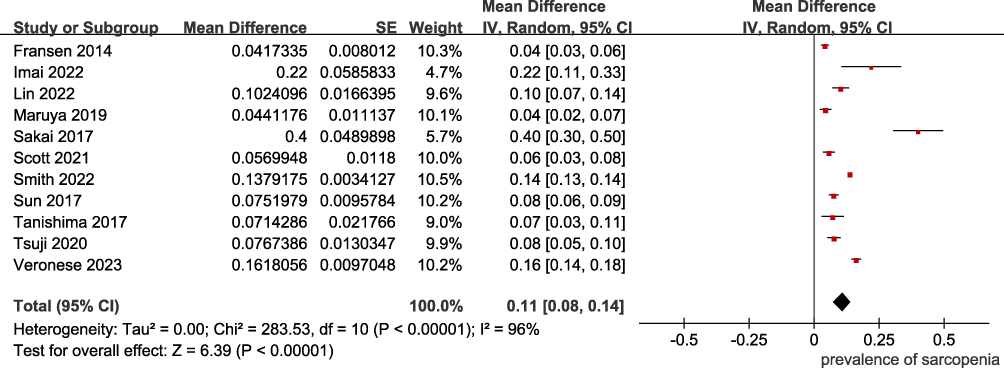 |
Figure 2 Forest plot of the prevalence of sarcopenia among older adults with chronic pain. |
The Link Between Chronic Pain and Sarcopenia
Data regarding the link between chronic pain and sarcopenia were available from 11 studies.13,16,17,20,22–26,29,30 These studies revealed a statistically significant positive correlation between chronic pain and an increased risk of sarcopenia, with a pooled OR of 1.52 (95% CI, 1.31–1.76), and relatively low heterogeneity between studies (I2=36%, p=0.11) (Figure 3). Subgroup analysis based on income level indicated significant differences between subgroups (p=0.02), with the low- and middle-income countries group showing a stronger association (OR, 1.73; 95% CI, 1.54–1.95) than the high-income countries group (OR, 1.38; 95% CI, 1.20–1.60). In terms of the diagnostic criteria for sarcopenia, the group using only muscle mass tended to have a higher correlation (OR, 1.65; 95% CI, 1.08–2.53) than the group using grip strength and/or physical performance as part of the diagnostic criteria (OR, 1.52; 95% CI, 1.30–1.77). Furthermore, the group reporting lower back pain or low limb pain tended to have a higher correlation (OR, 1.55; 95% CI, 1.25–1.93) than the control group that did not differentiate pain sites (OR, 1.47; 95% CI, 1.16–1.86) (Table 3).
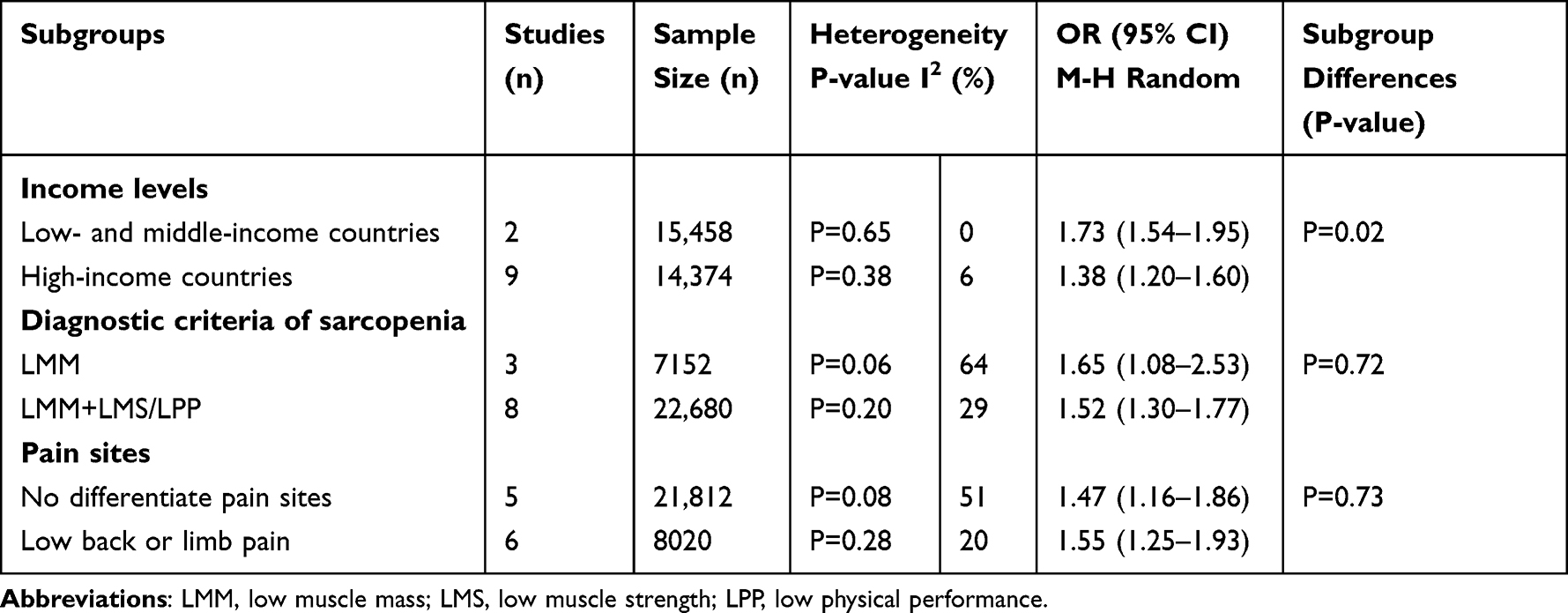 |
Table 3 Subgroup Analysis of the Association Between Chronic Pain and Sarcopenia |
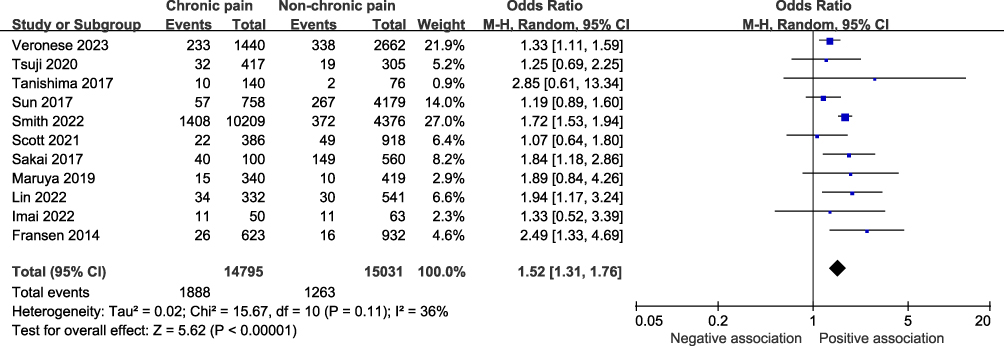 |
Figure 3 Forest plot of the link between chronic pain and sarcopenia. |
Sensitivity Analysis
To assess the robustness and credibility of our results, we conducted a leave-one-out sensitivity analysis. By systematically excluding one study at a time and pooling the remaining studies, we obtained adjusted estimates of sarcopenia prevalence ranging from 9% to 12%, and an adjusted OR between chronic pain and sarcopenia ranging from 1.43 to 1.58. Importantly, these adjusted estimates were akin to those derived from the original analysis, bolstering the reliability and stability of our results.
Publication Bias
In our present systematic review and meta-analysis, we visually inspected the funnel plot and observed a symmetrical distribution of studies, with a roughly even and concentrated distribution on both sides of the pooled effect size (Figure 4). Such a pattern suggests an absence of potential publication bias in our results.
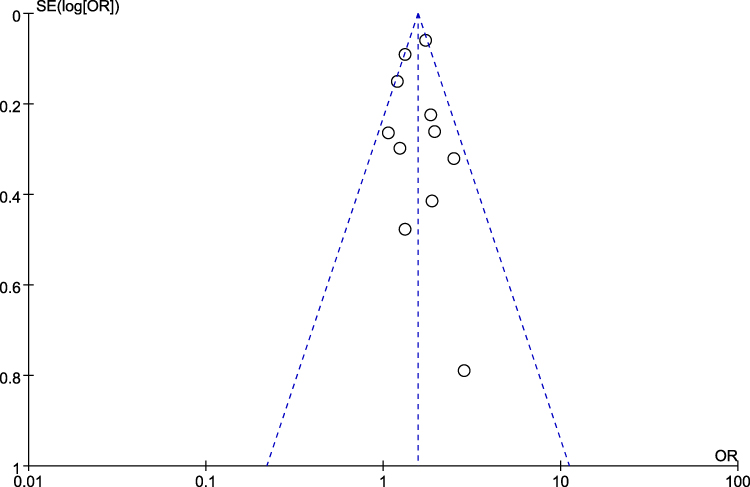 |
Figure 4 Funnel plot in the meta-analysis. |
Discussion
In this systematic review and meta-analysis of 17 studies involving 33,600 older adults with low heterogeneity in the majority of analyses, the analysis revealed that a significant correlation between chronic pain and a higher prevalence of sarcopenia in older adults, with chronic pain being linked to an increased risk of developing sarcopenia. Notably, subgroup analyses showed that these associations were more significant in low- and middle-income countries. Our findings highlight the potential impact of chronic pain on the development of sarcopenia in older adults, particularly in certain global regions.
According to previous epidemiological studies that found significant differences in the prevalence of chronic pain across different socioeconomic conditions,33 we divided the included studies into two subgroups based on their income levels for analysis. Our findings demonstrated that the correlation between chronic pain and sarcopenia was more pronounced in low- and middle-income countries than in high-income countries. There are two possible reasons for this observation. Firstly, low- and middle-income countries often have inadequate healthcare infrastructure and limited medical resources, which may hinder the provision of effective interventions for elderly individuals suffering from chronic pain.34,35 Secondly, low- and middle-income countries tend to have lower levels of education, resulting in a general lack of awareness among the population regarding pain management. This often leads to misconceptions that pain is an inevitable part of aging, which can discourage individuals from taking active measures to manage and alleviate their pain. These factors, combined with the higher prevalence of chronic pain and limited access to appropriate medical care in low-income countries, contribute to an increased incidence of pain-related complications. These findings also indirectly suggest that aggressive treatment of chronic pain may significantly reduce the risk of developing sarcopenia. Therefore, we advocate for greater health education initiatives for the elderly in the community, aimed at dispelling traditional beliefs and promoting awareness and consultation rates, leading to a reduction in the incidence and delay of complications related to chronic pain.
We stratified our study into two subgroups based on the diagnostic criteria for sarcopenia, and the results were consistent with our expectations. When diagnosing sarcopenia based on low muscle mass (LMM) alone, the cumulative prevalence increased to 14%, whereas it decreased to 10% when combined with poor physical function and/or low muscle strength (LMS). Furthermore, the meta-analysis revealed that the pooled OR of studies that employed a combination of LMM, LMS, and/or poor physical performance as diagnostic criteria for sarcopenia was lower than that of studies that solely utilized LMM as the diagnostic criterion. This is due to the contradictory relationship between sensitivity and specificity of diagnostic criteria. Generally, using LMM alone may increase sensitivity and decrease specificity, whereas using LMM in combination with LMS and/or physical function may increase specificity and decrease sensitivity. Therefore, when developing diagnostic criteria in clinical studies, a balance must be achieved between sensitivity and specificity, and the most appropriate diagnostic criteria must be selected according to the practical application scenarios. The current international consensus recommends defining sarcopenia as a geriatric syndrome characterized by LMM, LMS, and/or poor physical performance, rather than just LMM. We recommend using international consensus diagnostic criteria as much as possible in such studies to obtain more convincing results.
To investigate the hypothesis that chronic pain may increase the risk of sarcopenia by impairing mobility and promoting a sedentary lifestyle,30 we conducted analysis on two subgroups based on pain location. Our findings support the proposed hypothesis, as the group reporting low back pain or low limb pain exhibited a higher prevalence of sarcopenia than the control group that did not differentiate by pain site. Moreover, individuals reporting low back pain or low limb pain displayed an increased risk of developing sarcopenia compared to those who did not differentiate between pain sites. Nevertheless, the intergroup analysis did not reveal significant differences, which we suspect may be attributed to the relatively limited number of participants in the group reporting low back pain or low limb pain. Additional research is necessary to validate the results in the future. Nonetheless, our findings indicate that we must prioritize pain areas that hinder mobility in older adults and implement aggressive pain relief interventions.
The findings of this study are in line with those of a recent systematic review and meta-analysis of 14 observational studies.18 However, this study has three distinct advantages. Firstly, most of the studies included in this meta-analysis are large sample cohort studies, which lend greater reliability and applicability to the results. In contrast, recent meta-analyses have included more case-control studies, which may introduce greater heterogeneity into the findings. Secondly, the population included in this study has an average age of 60 years or older, making the results of the meta-analysis more applicable to the elderly population. By comparison, recent meta-analyses have included younger populations, which may introduce bias and limit the reliability of the results. Thirdly, this study includes research from countries with diverse income levels, increasing the generalizability of the meta-analysis results. Recent meta-analyses have predominantly included research from high-income countries, which may limit the universality of the findings. Of course, our meta-analysis is not immune to limitations. Firstly, most of the included studies were cross-sectional in design, precluding the establishment of causality. Secondly, there were significant variations in the appraisal of chronic pain among the included studies, potentially impacting the accuracy of our outcomes. Lastly, the availability of data in the included studies was constrained, precluding an inquiry into the relationship between pain severity and sarcopenia.
Conclusion
Our systematic review and meta-analysis provided evidence that the prevalence of sarcopenia is significantly higher in older adults with chronic pain compared to those without pain. There was also a significant positive correlation between chronic pain and an increased risk of sarcopenia. Additionally, pain in the low back or lower limbs, which can affect the mobility of older adults, was found to be associated with a higher likelihood of developing sarcopenia. However, the pathogenesis underlying the relationship between chronic pain and sarcopenia in older adults remains unknown. Several possible mechanisms have been proposed, including reduced activity and chronic inflammation, but these require further investigation through large-scale clinical studies in the future.
Data Sharing Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Consent for Publication
Approval was obtained from all authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(4):601. doi:10.1093/ageing/afz046
2. Veronese N, Demurtas J, Soysal P, et al. Sarcopenia and health-related outcomes: an umbrella review of observational studies. Eur Geriatr Med. 2019;10(6):853–862. doi:10.1007/s41999-019-00233-w
3. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636–2646. doi:10.1016/S0140-6736(19)31138-9
4. Liu X, Yue J. Precision intervention for sarcopenia. Precis Clin Med. 2022;5(2):pbac013. doi:10.1093/pcmedi/pbac013
5. Bonica JJ. The management of cancer pain. GP. 1954;10(5):35–43.
6. Kuner R, Flor H. Structural plasticity and reorganisation in chronic pain. Nat Rev Neurosci. 2017;18(2):113. doi:10.1038/nrn.2017.5
7. Dieppe P. Chronic musculoskeletal pain. BMJ. 2013;346(may16 6):f3146. doi:10.1136/bmj.f3146
8. Wernli K, Tan JS, O’Sullivan P, Smith A, Campbell A, Kent P. Does movement change when low back pain changes? A systematic review. J Orthop Sports Phys Ther. 2020;50(12):664–670. doi:10.2519/jospt.2020.9635
9. Abdulla A, Bone M, Adams N, et al. Guidance on the management of pain in older people. Age Ageing. 2013;42(Suppl 1):i1–i57. doi:10.1093/ageing/afs199
10. Rodríguez-Sánchez I, García-Esquinas E, Mesas AE, et al. Frequency, intensity and localization of pain as risk factors for frailty in older adults. Age Ageing. 2019;48(1):74–80. doi:10.1093/ageing/afy163
11. Pang BWJ, Wee S-L, Lau LK, et al. Prevalence and associated factors of sarcopenia in Singaporean Adults-the Yishun Study. J Am Med Dir Assoc. 2021;22(4):885.e1–885.e10. doi:10.1016/j.jamda.2020.05.029
12. Livshits G, Kalinkovich A. A cross-talk between sestrins, chronic inflammation and cellular senescence governs the development of age-associated sarcopenia and obesity. Ageing Res Rev. 2023;86:101852. doi:10.1016/j.arr.2023.101852
13. Imai R, Imaoka M, Nakao H, et al. Association between chronic pain with presarcopenia and central sensitization in Japanese community-dwelling older adults: a cross-sectional study. Medicine. 2022;101(32):e29998. doi:10.1097/MD.0000000000029998
14. Sit RWS, Zhang D, Wang B, et al. Sarcopenia and chronic musculoskeletal pain in 729 community-dwelling Chinese older adults with multimorbidity. J Am Med Dir Assoc. 2019;20(10):1349–1350. doi:10.1016/j.jamda.2019.04.009
15. Murphy RA, Ip EH, Zhang Q, et al. Transition to sarcopenia and determinants of transitions in older adults: a population-based study. J Gerontol a Biol Sci Med Sci. 2014;69(6):751–758. doi:10.1093/gerona/glt131
16. Tsuji S, Shinmura K, Nagai K, et al. Low back pain is closely associated with frailty but not with sarcopenia: cross-sectional study of rural Japanese community-dwelling older adults. Geriatr Gerontol Int. 2021;21(1):54–59. doi:10.1111/ggi.14100
17. Veronese N, Koyanagi A, Barbagallo M, et al. Pain Increases the risk for sarcopenia in community-dwelling adults: results from the English Longitudinal Study of Ageing. J Gerontol a Biol Sci Med Sci. 2023:glad062. doi:10.1093/gerona/glad062
18. Lin T, Dai M, Xu P, et al. Prevalence of sarcopenia in pain patients and correlation between the two conditions: a systematic review and meta-analysis. J Am Med Dir Assoc. 2022;23(5):902.e1–902.e20. doi:10.1016/j.jamda.2022.02.005
19. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. doi:10.1371/journal.pmed.1000100
20. Scott D, Blyth F, Naganathan V, et al. Prospective associations of chronic and intrusive pain with sarcopenia and physical disability amongst older Australian men: the Concord Health and Ageing in Men Project. Exp Gerontol. 2021;153:111501. doi:10.1016/j.exger.2021.111501
21. Wada T, Tanishima S, Osaki M, Nagashima H, Hagino H. Relationship between sarcopenia and pain catastrophizing in patients with lumbar spinal stenosis: a cross-sectional study. Osteoporos Sarcopenia. 2019;5(4):132–136. doi:10.1016/j.afos.2019.12.001
22. Sakai Y, Matsui H, Ito S, et al. Sarcopenia in elderly patients with chronic low back pain. Osteoporos Sarcopenia. 2017;3(4):195–200. doi:10.1016/j.afos.2017.09.001
23. Tanishima S, Hagino H, Matsumoto H, Tanimura C, Nagashima H. Association between sarcopenia and low back pain in local residents prospective cohort study from the GAINA study. BMC Musculoskelet Disord. 2017;18(1):452. doi:10.1186/s12891-017-1807-7
24. Fransen M, Su S, Harmer A, et al. A longitudinal study of knee pain in older men: concord Health and Ageing in Men Project. Age Ageing. 2014;43(2):206–212. doi:10.1093/ageing/aft188
25. Sun DS, Lee H, Yim HW, Won HS, Ko YH. The impact of sarcopenia on health-related quality of life in elderly people: Korean National Health and Nutrition Examination Survey. Korean J Intern Med. 2019;34(4):877–884. doi:10.3904/kjim.2017.182
26. Maruya K, Fujita H, Arai T, et al. Sarcopenia and lower limb pain are additively related to motor function and a history of falls and fracture in community-dwelling elderly people. Osteoporos Sarcopenia. 2019;5(1):23–26. doi:10.1016/j.afos.2019.03.002
27. Imagama S, Ando K, Kobayashi K, et al. Risk factors for neuropathic pain in middle-aged and elderly people: a five-year longitudinal cohort in the Yakumo study. Pain Med. 2020;21(8):1604–1610. doi:10.1093/pm/pnaa036
28. Han D-S, Wu W-T, Hsu P-C, et al. Sarcopenia is associated with increased risks of rotator cuff tendon diseases among community-dwelling elders: a Cross-Sectional Quantitative Ultrasound Study. Front Med. 2021;8:630009. doi:10.3389/fmed.2021.630009
29. Lin T, Huang X, Guo D, et al. Pain as a risk factor for incident sarcopenia in community-dwelling older adults: a 1-year prospective cohort study. J Am Geriatr Soc. 2023;71(2):546–552. doi:10.1111/jgs.18118
30. Smith L, López Sánchez GF, Veronese N, et al. Association between pain and sarcopenia among adults aged ≥65 years from low- and middle-income countries. J Gerontol a Biol Sci Med Sci. 2023:glad002. doi:10.1093/gerona/glad002
31. Tsuji H, Tetsunaga T, Misawa H, Nishida K, Ozaki T. Association of phase angle with sarcopenia in chronic musculoskeletal pain patients: a retrospective study. J Orthop Surg Res. 2023;18(1):87. doi:10.1186/s13018-023-03567-1
32. Iwahashi S, Hashida R, Matsuse H, et al. The impact of sarcopenia on low back pain and quality of life in patients with osteoporosis. BMC Musculoskelet Disord. 2022;23(1):142. doi:10.1186/s12891-022-05086-2
33. Todd A, McNamara CL, Balaj M, et al. The European epidemic: pain prevalence and socioeconomic inequalities in pain across 19 European countries. Eur J Pain. 2019;23(8):1425–1436. doi:10.1002/ejp.1409
34. Morriss WW, Roques CJ. Pain management in low- and middle-income countries. BJA Educ. 2018;18(9):265–270. doi:10.1016/j.bjae.2018.05.006
35. Jackson T, Thomas S, Stabile V, et al. Prevalence of chronic pain in low-income and middle-income countries: a systematic review and meta-analysis. Lancet. 2015;385(Suppl 2):S10. doi:10.1016/S0140-6736(15)60805-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.