Back to Journals » Veterinary Medicine: Research and Reports » Volume 11
Salmonella Mesenteric Lymphadenitis Causing Septic Peritonitis in Two Dogs
Authors Binagia EM, Levy NA ![]()
Received 13 November 2019
Accepted for publication 12 February 2020
Published 27 February 2020 Volume 2020:11 Pages 25—30
DOI https://doi.org/10.2147/VMRR.S238305
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Young Lyoo
Erin M Binagia, Nyssa A Levy
Department of Small Animal Clinical Sciences, College of Veterinary Medicine, Michigan State University, East Lansing, MI, USA
Correspondence: Nyssa A Levy
Department of Small Animal Clinical Sciences, College of Veterinary Medicine, Michigan State University, 736 Wilson Road, East Lansing, MI 48824, USA
Tel +1 517-355-6571
Fax +1 517-432-4091
Email [email protected]
Abstract: This report describes two cases of Salmonella mesenteric lymphadenitis leading to septic peritonitis in two young dogs. The cases were similar in presentation, diagnosis, treatment, and length of hospitalization. Both cases presented with clinical signs of vomiting, abdominal pain, and fever and were treated successfully via surgical debridement, omentalization, and antibiotic therapy. Both cases grew multi-drug resistant Salmonella spp. with resistance to ampicillin sulbactam, which is a common empiric antibiotic choice for cases of canine septic peritonitis. In both cases, the source of Salmonella is proposed to be the raw diet that preceded the septic peritonitis diagnosis. While Salmonella mesenteric lymphadenitis has been reported in humans and pigs, to the authors’ knowledge, this is the first report of Salmonella mesenteric lymphadenitis in dogs.
Keywords: sepsis, abscess, raw, diet
Introduction
Mesenteric lymphadenitis is an inflammatory condition of the lymph nodes and has been documented in humans, pigs, and dogs.1–7 The cause of mesenteric lymphadenitis in dogs can either have an immune-mediated7 or infectious source.5,8 While uncommon, the disease is important to be aware of as early diagnosis and treatment is critical for a favorable outcome. Bacterial agents that have been cultured in mesenteric lymphadenitis in dogs are Escherichia coli, Serratia marcescens, Staphylococcus epidermidis, Staphylococcus aureus, Staphylococcus canis, and Prevotella sp.5 Salmonella has been documented as a cause of mesenteric lymphadenitis in humans3,9 and pigs.1,4 To the authors’ knowledge, no cases of mesenteric lymphadenitis caused by Salmonella have yet been reported in dogs. Salmonella is a zoonotic agent that is often multi-drug resistant and can serve as an important source of nosocomial infection.10–12 This case series describes two cases of canine septic peritonitis caused by Salmonella mesenteric lymphadenitis in which both cases were exposed to a raw diet.
Case Histories
The first case was an 11-month intact male Golden Retriever that presented with a 4-day history of progressive inappetence, lethargy, diarrhea, and vomiting, which began soon after an episode of dietary indiscretion. This dog’s normal daily diet was a commercially available diet with raw ingredients.
Physical exam revealed depressed mentation, tacky mucous membranes, severe abdominal pain, and fever (41.5°C). Cardiopulmonary auscultation was within normal limits. Biochemistry results were within normal limits. Complete blood count (CBC) revealed a neutrophilic (25.3 x 103/uL, RI 4.0–8.1 x 103/uL) leukocytosis (27.2 x 103, RI 6.1–12 x 103/uL). Urinalysis was normal, and urine culture and tick-borne disease testing was negative.
Initial resuscitation and treatment included an intravenous (IV) bolus of lactated ringer’s solution of 13 mL/kg followed by a rate of 5 mL/kg/hr, ampicillin sulbactam 30 mg/kg IV q8h, pantoprazole 1 mg/kg IV q12h, and maropitant 1 mg/kg IV q24h. Abdominal radiographs showed mild loss of serosal detail in the mid abdomen (Figure 1).
 |
Figure 1 Abdominal radiographs with left, right, and ventrodorsal views depicting decreased serosal detail in the mid-abdomen. No mass effect was visualized. |
An abdominal ultrasound was performed which revealed all jejunal lymph nodes to be enlarged, hypoechoic, and containing cystic areas, surrounded with hyperechoic perinodal fat (Figure 2A and B). The pancreas was hypoechoic with hyperechoic peripancreatic fat, suggestive of pancreatitis (Figure 2C). Fine needle aspirate samples were taken from a jejunal lymph node, but were of very low cellularity and suggested reactive lymphoid hyperplasia and neutrophilic inflammation. Aerobic, anaerobic, and fungal cultures of the lymph node were submitted. Free peritoneal fluid was found and collected, and cytology was consistent with marked neutrophilic inflammation with bacterial sepsis (various intra- and extracellular rods).
 |
Figure 2 Ultrasound images of enlarged hypoechoic jejunal lymph nodes (A and B) and hypoechoic pancreas, suggesting pancreatitis (C). |
Following the diagnosis of septic peritonitis, abdominal exploration revealed an approximately 12 cm firm fluid-filled ileocolic lymph node. The remaining jejunal lymph nodes appeared diffusely affected, but smaller. All other organs appeared grossly normal. A lymph node biopsy sample was taken for histopathology and tissue culture was collected. The lymph node was lanced and lavaged, then omentalization was performed by placing the greater omentum into the lymph node and secured in place surgically. The abdomen was lavaged and a closed suction drain was placed.
The patient recovered well over the next 3 days. On Day 4, culture results returned multi-drug resistant Salmonella (see Table 1) and antibiotic regimen was switched to cefpodoxime 10 mg/kg PO q24h for 1 week. On Day 5 the drain was pulled and patient was discharged.
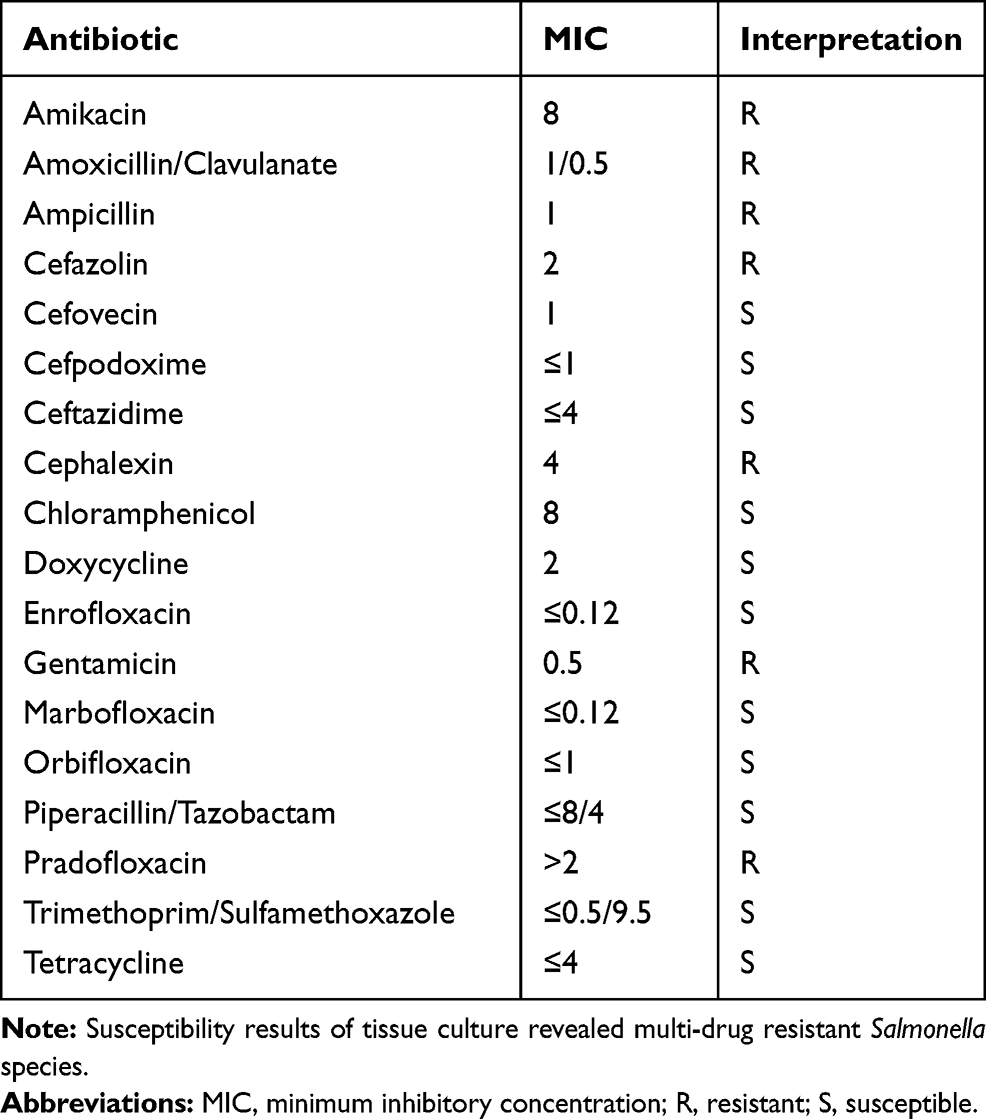 |
Table 1 Case #1 Salmonella Species Susceptibility Results |
Lymph node histopathology revealed neutrophilic necrotizing steatitis, no infectious organisms were seen. Aerobic tissue cultures of the ileocolic lymph node revealed Salmonella species. Anaerobic and fungal cultures were negative.
Patient was rechecked on Day 11 and doing well, and was still alive after follow up 1 year later with no reported chronic diseases.
The second case was a 7-month intact female German Shepherd Dog that was presented on day 1 for progressive lethargy, anorexia, and vomiting over the last 4 days, which began the day after eating a wild bird. This dog’s normal daily diet was a commercially available dry food. Pertinent physical exam findings included depressed mentation, marked ptyalism, fever (41.6°C), mild tachycardia, and a painful abdomen.
Initial diagnostics included a CBC, biochemistry panel, point-of-care ultrasound (POCUS), urinalysis, and abdominal radiographs. Pertinent biochemical abnormalities included mild hypoalbuminemia (2.7, RI 2.8–3.6 g/dL) and mild hyperglobulinemia (4.6, RI 2.3–3.7 g/dL). CBC revealed a neutrophilic (9.7 x 103, RI 4.0–8.1 x 103/uL), monocytic (1.7 x 103, RI 0.1–0.7 x103/uL) leukocytosis with toxic neutrophils on blood smear. Abdominal radiographs revealed generalized loss of serosal detail. The POCUS exam revealed possible mass cranial to urinary bladder and scant free fluid. Initial treatments included IV lactated ringers solution at 3 mL/kg/hr, hydromorphone 0.1 mg/kg IV, and ampicillin sulbactam 30 mg/kg IV q8h. An abdominocentesis and cytology was performed, which revealed neutrophilic and proteinaceous exudate with bacterial sepsis (mixed intracellular rods of different morphologies). The fluid was submitted for aerobic and anaerobic culture.
Following diagnosis of septic peritonitis, abdominal exploratory surgery revealed a large, continuous abscess from the area of the jejunal lymph nodes tracking to the colonic lymph nodes. Gastrointestinal tract appeared normal. Biopsies were taken of multiple abscessed lymph nodes for histopathology. Both the jejunal and colonic lymph node abscesses were thoroughly debrided, lavaged, and omentalized. A final abdominal explore was performed with no other abnormalities found. The abdomen was lavaged and a closed suction drain was placed.
At 8 hrs postoperatively, the patient was stable and eating, but remained febrile. Enrofloxacin 10 mg/kg IV q24h was added and fever resolved 12 hrs later. Patient was discharged on day 5 with oral enrofloxacin 10 mg/kg PO q24h for 14 days.
Aerobic culture of the abscess grew multi-drug resistant Salmonella species (see Table 2). Lymph node biopsy diagnosed reactive lymphoid hyperplasia with draining inflammation and hemorrhage. Biopsy of the mesentery revealed locally extensive pyogranulomatous cellulitis. In both histopathology samples, no infectious etiologies were found.
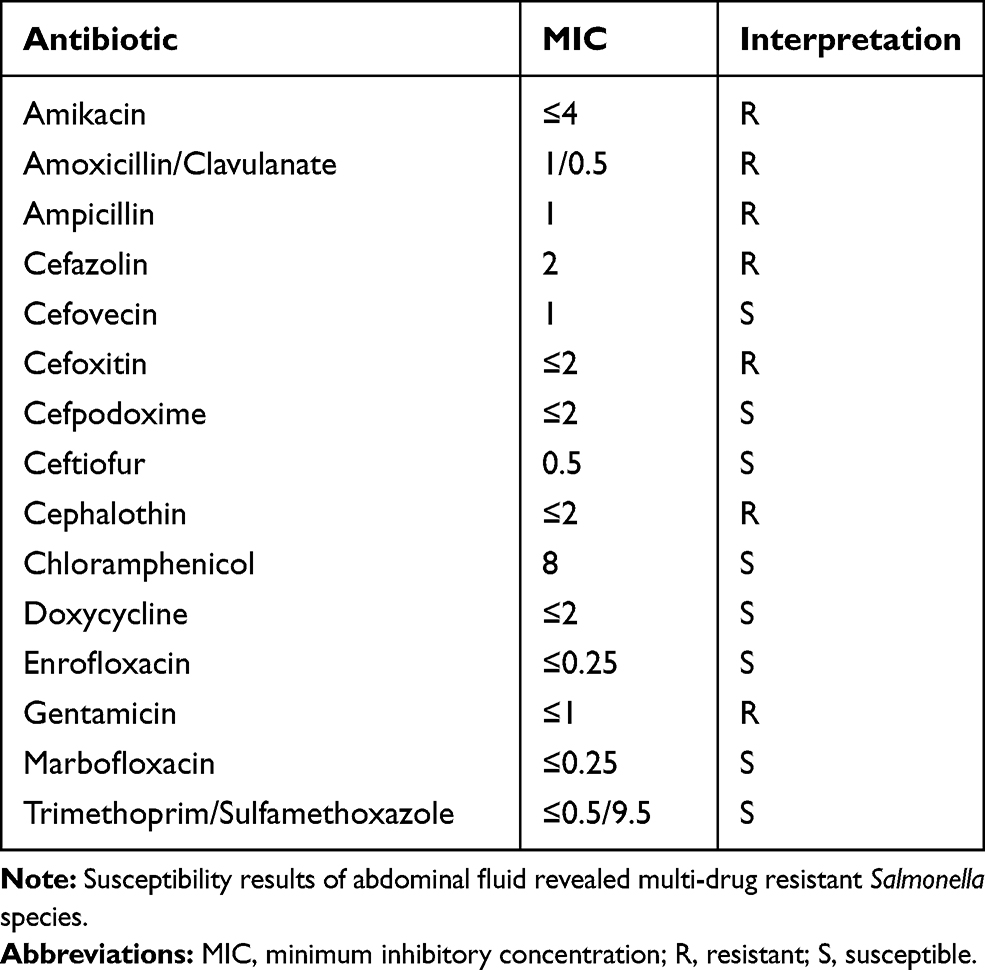 |
Table 2 Case #2 Salmonella Species Susceptibility Results |
Patient presented 1 year later for a wellness exam and was doing well.
Discussion
Mesenteric lymphadenitis is theorized to result from diffuse gastrointestinal inflammatory diseases such as pancreatitis, gastroenteritis, or inflammatory bowel disease.2,5,13,14 The responsible bacterial agents are theorized to either come from the skin or intestinal tract, and once in the gastrointestinal tract, small amounts migrate to the lymph nodes naturally to contribute to innate immunity.15 In the presence of inflammatory intestinal disease, however, a large amount of bacteria can migrate into the lymph nodes or translocate into the bloodstream, leading to severe mesenteric lymphadenitis and sepsis.5,6,16-18 Bacterial agents previously cultured in dogs with mesenteric lymphadenitis include Escherichia coli, Bacteroides, Serratia marcescens, Staphylococcus epidermidis, Staphylococcus aureus, Staphylococcus canis, Staphylococcus pseudintermedius, and Prevotella sp.5,8
While the condition is well described in humans, mesenteric lymphadenitis is rarely reported in dogs. In both humans and dogs, the most common clinical signs include fever and abdominal pain, and ultrasonography is the main method of diagnosis.2,3,5,7 In humans, the condition is often treated medically, while surgery is recommended in the presence of an abscess or septic peritonitis.2 In a retrospective study of 14 dogs, the majority of mesenteric lymphadenitis cases were treated surgically, with only a few treated medically. Of those treated medically, 75% experienced a relapse within 4 months of discharge and required continued antibiotic therapy, compared to no relapses in the surgical cases.5 This observation suggests that conservative therapy is possible in animals, but surgery should be recommended in the presence of an abscess or septic peritonitis.
Salmonella enterica has been documented as a cause of mesenteric lymphadenitis in humans and pigs.1,3,4 It is a gram-negative bacteria transmitted fecal-orally, with multiple serotypes that infect a wide variety of mammals, birds, and reptiles. These characteristics make Salmonella an important source of zoonotic and nosocomial infections. Additionally, multiple surveillance studies have found Salmonella is often resistant to commonly used antibiotics (ampicillin, cephalosporins, tetracyclines), with a high prevalence of multi-drug resistance, which may complicate empiric antibiotic treatment.19,20
Infections with Salmonella enterica are uncommon in dogs, with an overall prevalence of 1% to 36% reported in dogs, many of which are subclinical carriers.16,21-25 While animals infected may not show clinical signs, they do serve as an infectious source, shedding the bacteria in their feces for up to 6 weeks, contributing to environmental contamination.16 Puppies (less than 1 year of age) are more susceptible to infection and clinical illness compared to adults.16,26 Important sources of salmonellosis in companion animals include raw diets,22,27-30 pet reptiles in the household,23 and ingestion of wild birds.31 Raw pet foods have been surveyed worldwide for salmonellosis, with reported positive samples ranging from 7.1% to 21%.27,28,32 This prevalence of Salmonella in raw food diets is significantly higher than commercial dry dog food products,22,33 indicating raw food diets pose higher risk of Salmonella exposure to pet dogs. In a study evaluating the prevalence of Salmonella in 2422 dogs, it was found that Salmonella-positive dogs were significantly more likely to have consumed raw food.21 Fecal shedding rates after ingesting a single raw meal diet have been reported significantly higher (30–44%) than those not fed raw diets.22,34 Pet owners should understand the high risk of Salmonella contamination in commercial raw food diets with the consequential high fecal shedding rate of Salmonella.
In conclusion, while uncommon in dogs, mesenteric lymphadenitis should be on the differential list in dogs with acute vomiting, abdominal pain, and fever. Diagnosis can be made via ultrasonography or abdominal exploratory surgery if septic peritonitis is diagnosed via fluid analysis. Salmonellosis should be a differential for cases of mesenteric lymphadenitis, especially if the patient is young (less than 1 year of age) with a history of ingestion of raw diet or wild birds. As Salmonella is often resistant to commonly used antibiotics, appropriate broad-spectrum antibiotic therapy and surgical debridement should be initiated as soon as possible.
Ethics Statement
Treatment of the animals described in this case series followed best practice veterinary care guidelines, with written informed consent provided by their owners.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Garrido V, Sánchez S, San Román B, et al. Simultaneous infections by different Salmonella strains in mesenteric lymph nodes of finishing pigs. BMC Vet Res. 2014;10:59. doi:10.1186/1746-6148-10-59
2. Helbling R, Conficconi E, Wyttenbach M, et al. Acute nonspecific mesenteric lymphadenitis: more than “no need for surgery”. Biomed Res Int. 2017;2017:9784565. doi:10.1155/2017/9784565
3. Nakachi S, Nakamura T, Agha N, et al. Clinical features and early diagnosis of typhoid fever emphasizing usefulness of detecting mesenteric lymphadenopathy with ultrasound as diagnostic method. Southeast Asian J Trop Med Public Health. 2003;34 Suppl 2(Suppl 2):153–157.
4. Nollet N, Maes D, Duchateau L, et al. Discrepancies between the isolation of Salmonella from mesenteric lymph nodes and the results of serological screening in slaughter pigs. Vet Res. 2005;36(4):545–555. doi:10.1051/vetres:2005014
5. Salavati Schmitz S. Retrospective characterisation and outcome of canine idiopathic mesenteric purulent lymphadenitis and lymph node abscesses at a teaching hospital from 2005 to 2015. J Small Anim Pract. 2016;57(12):690–697. doi:10.1111/jsap.2016.57.issue-12
6. Zińczuk J, Wojskowicz P, Kiśluk J, Fil D, Kemona A, Dadan J. Mesenteric lymphadenitis caused by Yersinia enterocolitica. Prz Gastroenterol. 2015;10(2):118–121. doi:10.5114/pg.2014.47504
7. Ribas Latre A, McPartland A, Cain D, et al. Canine sterile steroid-responsive lymphadenitis in 49 dogs. J Small Anim Pract. 2019;60(5):280–290. doi:10.1111/jsap.2019.60.issue-5
8. Beaumont PR, Glauberg AF. Necrotizing lymphadenitis as a cause of acute abdominal distress in a dog. Mod Vet Pract. 1979;60(11):890–892.
9. Gremillon DH, Geckler R, Ellenbogen C. Salmonella abscess. A potential nosocomial hazard. Arch Surg. 1977;112(7):843–845. doi:10.1001/archsurg.1977.01370070057007
10. Uhaa IJ, Hird DW, Hirsh DC, Jang SS. Case-control study of risk factors associated with nosocomial Salmonella krefeld infection in dogs. Am J Vet Res. 1988;49(9):1501–1505.
11. Walther B, Tedin K, Lübke-Becker A. Multidrug-resistant opportunistic pathogens challenging veterinary infection control. Vet Microbiol. 2017;200:71–78. doi:10.1016/j.vetmic.2016.05.017
12. Wright JG, Tengelsen LA, Smith KE, et al. Multidrug-resistant Salmonella Typhimurium in four animal facilities. Emerg Infect Dis. 2005;11(8):1235–1241. doi:10.3201/eid1108.050111
13. Qin HL, Su ZD, Gao Q, Lin QT. Early intrajejunal nutrition: bacterial translocation and gut barrier function of severe acute pancreatitis in dogs. Hepatobiliary Pancreat Dis Int. 2002;1(1):150–154.
14. Unterer S, Lechner E, Mueller RS, et al. Prospective study of bacteraemia in acute haemorrhagic diarrhoea syndrome in dogs. Vet Rec. 2015;176(12):309. doi:10.1136/vr.102521
15. Macpherson AJ, Smith K. Mesenteric lymph nodes at the center of immune anatomy. J Exp Med. 2006;203(3):497–500. doi:10.1084/jem.20060227
16. Greene C. Enteric bacterial infections — Salmonellosis. In: Greene, CE (Ed), Infectious Diseases of the Dog and Cat.
17. Alexander JW, Boyce ST, Babcock GF, et al. The process of microbial translocation. Ann Surg. 1990;212(4):
18. Dahlinger J, Marks SL, Hirsh DC. Prevalence and identity of translocating bacteria in healthy dogs. J Vet Intern Med. 1997;11(6):319–322. doi:10.1111/jvim.1997.11.issue-6
19. Srisanga S, Angkititrakul S, Sringam P, Le Ho PT, Vo AT, Chuanchuen R. Phenotypic and genotypic antimicrobial resistance and virulence genes of Salmonella enterica isolated from pet dogs and cats. J Vet Sci. 2017;18(3):273–281. doi:10.4142/jvs.2017.18.3.273
20. Philbey AW, Mather HA, Gibbons JF, Thompson H, Taylor DJ, Coia JE. Serovars, bacteriophage types and antimicrobial sensitivities associated with salmonellosis in dogs in the UK (1954–2012). Vet Rec. 2014;174(4):94. doi:10.1136/vr.101864
21. Reimschuessel R, Grabenstein M, Guag J, et al. Multilaboratory survey to evaluate Salmonella prevalence in diarrheic and nondiarrheic dogs and cats in the United States between 2012 and 2014. J Clin Microbiol. 2017;55(5):1350–1368. doi:10.1128/JCM.02137-16
22. Finley R, Ribble C, Aramini J, et al. The risk of salmonellae shedding by dogs fed Salmonella-contaminated commercial raw food diets. Can Vet J. 2007;48(1):69–75.
23. Arsevska E, Singleton D, Sánchez-Vizcaíno F, et al. Small animal disease surveillance: GI disease and salmonellosis. Vet Rec. 2017;181(9):228–232. doi:10.1136/vr.j3642
24. Fukata T, Naito F, Yoshida N, Yamaguchi T, Mizumura Y, Hirai K. Incidence of Salmonella infection in healthy dogs in Gifu Prefecture, Japan. J Vet Med Sci. 2002;64(11):1079–1080. doi:10.1292/jvms.64.1079
25. Fukushima H, Nakamura R, Iitsuka S, Ito Y, Saito K. Presence of zoonotic pathogens (Yersinia spp., Campylobacter jejuni, Salmonella spp., and Leptospira spp.) simultaneously in dogs and cats. Zentralbl Bakteriol Mikrobiol Hyg B. 1985;181(3–5):430–440.
26. Bagcigil AF, Ikiz S, Dokuzeylu B, Basaran B, Or E, Ozgur NY. Fecal shedding of Salmonella spp. in dogs. J Vet Med Sci. 2007;69(7):775–777. doi:10.1292/jvms.69.775
27. Davies RH, Lawes JR, Wales AD. Raw diets for dogs and cats: a review, with particular reference to microbiological hazards. J Small Anim Pract. 2019;60(6):329–339. doi:10.1111/jsap.2019.60.issue-6
28. Hellgren J, Hästö LS, Wikström C, Fernström LL, Hansson I. Occurrence of Salmonella, Campylobacter, Clostridium and Enterobacteriaceae in raw meat-based diets for dogs. Vet Rec. 2019;184(14):442. doi:10.1136/vr.105199
29. Lefebvre SL, Reid-Smith R, Boerlin P, Weese JS. Evaluation of the risks of shedding Salmonellae and other potential pathogens by therapy dogs fed raw diets in Ontario and Alberta. Zoonoses Public Health. 2008;55(8–10):470–480. doi:10.1111/j.1863-2378.2008.01145.x
30. Lenz J, Joffe D, Kauffman M, Zhang Y, LeJeune J. Perceptions, practices, and consequences associated with foodborne pathogens and the feeding of raw meat to dogs. Can Vet J. 2009;50(6):637–643.
31. Giovannini S, Pewsner M, Hüssy D, et al. Epidemic of salmonellosis in passerine birds in Switzerland with spillover to domestic cats. Vet Pathol. 2013;50(4):597–606. doi:10.1177/0300985812465328
32. van Bree FPJ, Bokken GCAM, Mineur R, et al. Zoonotic bacteria and parasites found in raw meat-based diets for cats and dogs. Vet Rec. 2018;182:50. doi:10.1136/vr.104535
33. Nemser SM, Doran T, Grabenstein M, et al. Investigation of Listeria, Salmonella, and toxigenic Escherichia coli in various pet foods. Foodborne Pathog Dis. 2014;11(9):706–709. doi:10.1089/fpd.2014.1748
34. Joffe DJ, Schlesinger DP. Preliminary assessment of the risk of Salmonella infection in dogs fed raw chicken diets. Can Vet J. 2002;43(6):441–442.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.