Back to Journals » Journal of Inflammation Research » Volume 18
Safe Use of Corticosteroids in Non-Infectious Uveitis
Authors Belletti M, Izquierdo-Escamez R, Tornero C, Olivas-Vergara O, Peiteado D, Carreño E ![]()
Received 21 August 2025
Accepted for publication 4 October 2025
Published 17 October 2025 Volume 2025:18 Pages 14441—14455
DOI https://doi.org/10.2147/JIR.S540821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shouya Feng
Matteo Belletti,1,2 Rosario Izquierdo-Escamez,3 Carolina Tornero,4 Otto Olivas-Vergara,5 Diana Peiteado,4 Ester Carreño1
1Department of Ophthalmology, Hospital Universitario La Paz, Madrid, Spain; 2Department of Ophthalmology, IRCSS Azienda Ospedaliero-Universitaria Di Bologna, Bologna, Italy; 3Department of Ophthalmology, Hospital Universitario de Torrevieja, Alicante, Spain; 4Department of Rheumatology, Hospital Universitario La Paz, Madrid, Spain; 5Department of Rheumatology, Hospital Universitario Fundación Jiménez Díaz, Madrid, Spain
Correspondence: Ester Carreño, Department of Ophthalmology Hospital Universitario La Paz, P.° de la Castellana 261, Fuencarral-El Pardo, Madrid, 28046, Spain, Email [email protected]
Abstract: Corticosteroids continue to represent the cornerstone of uveitis management, owing to their potent anti-inflammatory effects, which are pivotal for suppressing intraocular inflammation and mitigating the risk of irreversible visual impairment. This review focuses on the safety considerations associated with corticosteroid therapy across multiple administration routes, including topical, periocular, intravitreal, and systemic. Optimal corticosteroid therapy requires a personalized, stepwise approach, commencing with the least invasive modality at the lowest effective dose and escalating based on anatomical involvement, disease severity, and individual risk profiles, to balance efficacy with safety. Special attention is given to strategies for mitigating well-recognized local and systemic adverse effects, such as ocular hypertension, cataracts, osteoporosis, and increased cardiovascular risk. Beyond synthesizing current evidence, this review offers a novel perspective by integrating systemic and local therapy risks and by highlighting safety strategies that can guide individualized regimens. Finally, we identify persisting knowledge gaps, including the lack of long-term comparative safety data, limited evidence on risk stratification, and the need for biomarkers to guide therapy, which represent critical avenues for future research. Adjunctive use of immunosuppressive or biologic agents enables improved long-term control and facilitates corticosteroid tapering.
Keywords: uveitis, non-infectious uveitis, corticosteroids, glucocorticoids, safety
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Xu has been published for this article.
Introduction
Uveitis is a leading cause of vision loss.1 Recurrent inflammatory episodes can result in cumulative ocular damage, progressively increasing the likelihood of visual impairment or blindness, with substantial personal, societal, and economic consequences.2,3 Despite the well-known and potentially severe side effects, corticosteroids are the mainstay for the management of non-infectious uveitis (NIU), but their use requires careful consideration of route, dose, duration, and risk of adverse effects.4 In fact, evidence from the VISUAL-1 and VISUAL-2 trials supports that chronic corticosteroid use in NIU is strongly associated with dose-dependent increases in adverse events, showing significantly higher incidence rates of corticosteroid-related adverse events during prednisone treatment compared to post-taper periods, highlighting the risks of higher dosing in both active and inactive noninfectious uveitis.5
Methods
This work was conducted as a narrative review. Studies were identified and selected based on the authors’ expert knowledge of the field, with prioritization given to publications that have shaped current clinical practice in the management of non-infectious uveitis. No systematic database search or formal inclusion/exclusion criteria were applied. Instead, the selection process relied on expert choice, aiming to provide a balanced synthesis of key concepts and safety considerations across corticosteroid administration routes.
Results
Route and Dose
Topical
For noninfectious anterior uveitis, topical corticosteroids such as prednisolone acetate 1% are first-line, typically started at high frequency (eg, hourly during waking hours) and then tapered based on clinical response.4,6 Other topical steroids such as dexamethasone 0.1% are also frequently used in the treatment of anterior uveitis.7
There is one randomized trial, comparing prednisolone acetate 1% and rimexolone 1%, which demonstrates that both are effective, with no significant difference in reduction of anterior chamber inflammatory cells at 28 days.8 Additionally, a randomized trial found that non-preserved methylprednisolone 1% is non-inferior to preserved prednisolone acetate 1% in efficacy, with lower ocular surface toxicity and less subjective discomfort, but unfortunately this formulation is not commercially available.9
Furthermore, randomized controlled trials have demonstrated that difluprednate 0.05% (not commercially available in the EU) is non-inferior to prednisolone acetate 1% for the treatment of non-infectious anterior uveitis, with similar efficacy in reducing anterior chamber cell grade after 14 days of treatment and subsequent tapering. Notably, difluprednate achieves this effect with less frequent dosing (four times daily) compared to prednisolone acetate (eight times daily), which may improve adherence in some patients.10,11
However, the risk profile of difluprednate requires careful consideration. Both adult and pediatric studies have consistently shown a higher incidence of clinically significant intraocular pressure (IOP) elevation with difluprednate compared to other topical corticosteroids.12 In adults, IOP elevation (ie, ≥21 mmHg or ≥10 mmHg above baseline) occurred in approximately 31% of patients.12 In pediatric populations, up to 50% of eyes experienced significant IOP elevation, and cataract formation or progression was observed in 39% of eyes, necessitating close monitoring.13 Most IOP elevations responded to cessation of difluprednate or addition of topical antihypertensive agents, but some pediatric cases required surgery to lower intraocular pressure.13
However, other topical steroids such as fluorometholone 0.1%, loteprednol 0.5% or hydrocortisone sodium phosphate 0.335% have a low penetrance intraocularly and therefore are not effective in treating anterior NIU.7
According to the SITE (Systemic Immunosuppressive Therapy for Eye Diseases) cohort study, the safe maintenance dose of topical corticosteroids to minimize the risk of adverse events such as cataract and ocular hypertension in the treatment of non-infectious anterior uveitis is ≤2 drops per day of prednisolone acetate 1% (or equivalent).14 Chronic use of higher doses, particularly >3 drops daily, is associated with a significantly increased risk of cataract formation and ocular hypertension, as demonstrated in both adult and pediatric populations.15 In the SITE study, topical corticosteroids were linked to an increased risk of cataract only when anterior chamber inflammation was absent or minimal, suggesting that when used to treat active inflammation (which is itself a risk factor for cataract) they do not result in a net increase in cataract incidence.14
In non-anterior (intermediate, posterior, panuveitis) forms of NIU, topical corticosteroids alone are generally inadequate because they do not reach therapeutic levels in the posterior segment due to limited penetration.7
Periocular or Intravitreal
Local corticosteroid therapies, including periocular injections, intravitreal injections, sustained-release implants, and suprachoroidal injections, are effective for controlling intraocular inflammation and macular edema.4
A recent Cochrane review, including four randomized controlled trials, evaluated the role of intravitreal corticosteroid implants (fluocinolone acetonide and dexamethasone) in non-anterior NIU (intermediate uveitis, posterior uveitis, and panuveitis). Comparing these implants to sham or standard-of-care therapies, it pointed out that corticosteroid implants reduced the risk of uveitis recurrence by 54–60%, though their impact on visual acuity and quality of life was limited or uncertain.16 The implants were consistently associated with increased risks of cataract progression and IOP elevation, often requiring medical or surgical intervention.16 Overall, the evidence supports a modest benefit in controlling inflammation, but highlights the need for careful monitoring and individualized risk–benefit assessment.16
The Multicenter Uveitis Steroid Treatment (MUST) trial was a randomized controlled trial comparing systemic corticosteroid therapy (with immunosuppression as per investigator’s decision) to the surgically placed intravitreal fluocinolone acetonide implant for patients with non-anterior NIU. The MUST trial demonstrated that, over the long term, systemic therapy was associated with slightly better visual acuity outcomes.17 Although no statistically significant difference in mean visual acuity improvement was observed between the groups at 2 and 4.5 years,18,19 by 7 years, systemic therapy was linked to a mean gain of 7.2 letters over the implant group (95% CI, 2.1–12).17 This difference reached clinical significance, although its interpretation is limited by loss to follow-up.
Control of intraocular inflammation was superior with the implant at all time points, but most patients on systemic therapy also achieved substantial improvement in inflammatory status.18,19 Furthermore, there was a rapid early improvement in macular edema in the implant group, but by 36 months, the rates of macular edema resolution were similar between groups.20 On the contrary, the implant group had higher rates of ocular complications, including cataract surgery, elevated intraocular pressure, and glaucoma, while systemic therapy was associated with more systemic infections requiring antibiotics, but otherwise, serious systemic adverse events were uncommon and similar between groups.18 As a summary, cost-effectiveness and side-effect profiles suggest systemic therapy is generally preferred for bilateral disease, while implant therapy may be considered for unilateral disease or when systemic therapy is contraindicated or unsuccessful.18–22
Nevertheless, the MUST trial used the surgically implanted 0.59 mg fluocinolone acetonide implant (not commercially available in the EU) as the comparator to systemic therapy. Since then, another 0.18/0.19 mg fluocinolone acetonide implant has been presented. The 0.59 mg fluocinolone acetonide implant is associated with the highest rates of adverse events.23 Nearly all phakic eyes develop cataracts requiring surgery within 3 years, and approximately 77% require IOP-lowering medications and 37% require filtering surgery for IOP control.23,24 However, the security profile is more favorable in the case of the 0.18/0.19 mg implants. In pivotal trials, 80% of phakic eyes required cataract surgery over 3 years, and <5% required incisional IOP-lowering surgery; most IOP elevations were managed medically.25
Randomized controlled trials of 0.18/0.19 mg implants, have also demonstrated a significant reduction in uveitis recurrence rates compared to sham (eg, 28% vs 86% recurrence at 12 months; p < 0.01), prolonged time to first recurrence, and improved visual outcomes, with approximately one-third of patients gaining ≥15 letters in BCVA at 36 months.26 Although no head-to-head trials directly compare the 0.18/0.19 mg implants to the 0.59 mg implant, available data and systematic reviews indicate comparable efficacy in controlling inflammation and preserving vision.16,27
In parallel, other trials have compared different corticosteroid delivery methods for uveitic macular edema. The Periocular and Intravitreal Corticosteroids for Uveitic Macular Edema (POINT) Trial was a multicenter randomized clinical trial comparing periocular triamcinolone acetonide, intravitreal triamcinolone acetonide, and the intravitreal dexamethasone implant for the treatment of uveitic macular edema in non-infectious uveitis. At 8 weeks, all three treatments led to significant reductions in central subfield thickness on optical coherence tomography (OCT), but intravitreal therapies were superior to periocular injection.28 Specifically, the mean central subfield thickness reduction from baseline was 23% for periocular triamcinolone acetonide, 39% for intravitreal triamcinolone acetonide, and 46% for intravitreal dexamethasone implant. Both intravitreal triamcinolone acetonide and intravitreal dexamethasone implant were statistically superior to periocular triamcinolone acetonide in reducing central subfield thickness (p < 0.0001). Both intravitreal groups also achieved greater improvements in best-corrected visual acuity, with a mean gain of 5 letters more than the periocular triamcinolone acetonide group at 8 weeks (p < 0.004).28 On the other hand, the risk of IOP elevation (≥24 mmHg) was higher in the intravitreal groups (hazard ratio [HR] 1.83 for intravitreal triamcinolone acetonide and 2.52 for intravitreal dexamethasone implant vs periocular triamcinolone acetonide), although no significant difference in IOP risk between the two intravitreal groups.28
Even though intraocular steroids clearly reduce vitritis and macular edema, their effect on choroidal inflammation remains uncertain. Some studies suggest intraocular steroids may decrease choroidal inflammation and thickness in inflammatory eye disorders, while others, such as those on birdshot chorioretinopathy, indicate systemic therapy provides better control over choroidal inflammation.29
Overall, the risk of glaucoma is dose- and duration-dependent, and is highest with the surgically implanted, higher-dose 0.59 mg fluocinolone acetonide implant. In long-term follow-up of the Multicenter Uveitis Steroid Treatment (MUST) trial, eyes treated with the fluocinolone acetonide implant had a significantly higher cumulative incidence of glaucoma compared to systemic therapy (40% vs 8% at median 6.9 years; HR 5.9), and this risk persisted even after adjusting for IOP elevation during follow-up.21,24,30,31 Of particular concern is that, although most cases of steroid-induced glaucoma following intravitreal corticosteroid implants are indeed preceded by IOP elevation, which is the primary modifiable risk factor for glaucomatous optic neuropathy in this context, long-term prospective studies in uveitis has shown that some patients develop progressive glaucomatous optic nerve damage despite adequate IOP control, suggesting that corticosteroid exposure itself may contribute directly to optic nerve vulnerability or damage, independent of measured IOP.24,30,32 Importantly, while aggressive IOP management prevented progression in most cases, a subset of patients experienced worsening visual field or optic nerve cupping despite controlled IOP, underscoring the need for vigilant, indefinite monitoring for both IOP and structural/functional glaucomatous changes in patients receiving repeated or sustained intravitreal corticosteroid therapy for non-infectious uveitis.24,30,32,33
In summary, repeated or sustained use of intravitreal corticosteroid implants for non-infectious uveitis is associated with a significantly increased risk of glaucoma, and this risk is highest with higher-dose, longer-acting implants and with repeated exposure. Close and indefinite monitoring for IOP elevation and structural glaucomatous damage is required in these patients.24,30,32,33
Conversely, a novel delivery route for triamcinolone acetonide, the suprachoroidal administration, appears to carry a lower risk of developing glaucoma, similar to sham or control treatment.34 In a randomized trial, the incidence of IOP elevation with suprachoroidal triamcinolone was 11.5%, not significantly different from the sham group (15.6%), and the rate of cataract formation was also similar (7.3% vs 6.3%).34 In an open-label safety study, 15.8% of subjects experienced an IOP rise >10 mmHg, and only 5.3% had IOP >30 mmHg; no serious ocular adverse events or cases of glaucoma requiring surgery were reported over 24 weeks.35 These findings suggest a low risk of clinically significant IOP elevation or glaucoma with suprachoroidal triamcinolone acetonide; however, further studies with longer follow-up are warranted to determine whether or not this route of administration is safer than others.
Systemic Steroids
Systemic corticosteroids (eg, oral prednisone) are effective for posterior segment or vision-threatening inflammation, although long-term use, especially at doses >7.5 mg/day, is associated with significant systemic risks, such as hyperglycemia and osteoporosis.1 The addition of immunosuppressive agents is often necessary for steroid-sparing and to achieve long-term disease control.1
The recommended initial dose of oral corticosteroids for the treatment of non-anterior NIU (based on clinical experience) is 1 mg/kg/day of oral prednisone (or equivalent), up to a maximum of 60–80 mg daily.4,36 The dose is then tapered over several weeks based on clinical response and the goal of minimizing long-term corticosteroid exposure.1,4,36 Doses much lower than 1 mg/kg/day are not recommended for induction of remission, as they are generally insufficient to control active intraocular inflammation.
In general, long-term maintenance with corticosteroids is not recommended due to the risk of adverse effects; instead, the goal is to taper prednisone to ≤7.5 mg/day within 3 months, at which point steroid-sparing immunosuppressive agents should be introduced if inflammation cannot be controlled at these lower doses.36,37 Furthermore, chronic use of low-dose corticosteroids (<7.5 mg/day) as monotherapy is considered ineffective for disease control and is discouraged in favor of immunosuppressive therapy.36,37
Intravenous corticosteroids should be used in ocular inflammatory conditions that are severe, vision-threatening, or associated with rapid progression, where an immediate and robust anti-inflammatory effect is required. In such cases, promptly concomitant immunosuppressive therapy can also be started, either concurrently or shortly after corticosteroid pulse therapy. The most well-established indications include:
Evidence from retrospective studies demonstrates that intravenous methylprednisolone induces rapid improvement in intraocular inflammation, including anterior chamber cells, vitritis, macular edema, and retinal vasculitis, with a favorable safety profile in the short term.38,40 In a retrospective multicenter cohort, 57% of patients achieved complete remission within 1 month after intravenous methylprednisolone, followed by oral prednisone taper.40
Compared to oral corticosteroids at 1 mg/kg/day, intravenous corticosteroids provide more rapid suppression of inflammation but are not superior for long-term disease control. Oral prednisone at 1 mg/kg/day remains the standard initial therapy for most cases of severe non-infectious uveitis, with intravenous corticosteroids reserved for fulminant or refractory cases, or when immediate vision preservation is critical. Both approaches require transition to steroid-sparing immunosuppressive therapy for long-term management to minimize corticosteroid-related adverse effects.1,4,36
The common side effects of systemic corticosteroids when used for the treatment of non-infectious uveitis include hyperglycemia, osteoporosis, hypertension, weight gain, cushingoid features, mood and psychiatric disturbances, increased risk of infection, adrenal suppression, myopathy, and gastrointestinal complications such as peptic ulcer disease.41 Ocular complications such as cataract and ocular hypertension/glaucoma can also occur, though the risk is more pronounced with local steroid administration; systemic steroids may contribute, especially with prolonged use, as explained above.42
Risk factors for developing these side effects include higher corticosteroid dose, longer duration of therapy, older age, and pre-existing comorbidities (such as diabetes, hypertension, or osteoporosis). The risk of adverse events increases systematically with corticosteroid dose: each 10 mg increase in prednisone is associated with a 1.5- to 2.6-fold increase in overall adverse event rates.5 Chronic use of doses exceeding 7.5 mg/day of prednisone is particularly associated with metabolic and bone complications.43,44
Regular monitoring for side effects and modification of risk factors (eg, bone protection, glucose monitoring) are essential components of care.43,44
Before starting systemic corticosteroid therapy in a patient with non-infectious uveitis, it is recommended to perform baseline evaluations to identify comorbidities and risk factors for corticosteroid-related adverse effects (correcting them when possible), and to monitor for complications during therapy.45 The following tests and analyses are commonly recommended (Table 1):
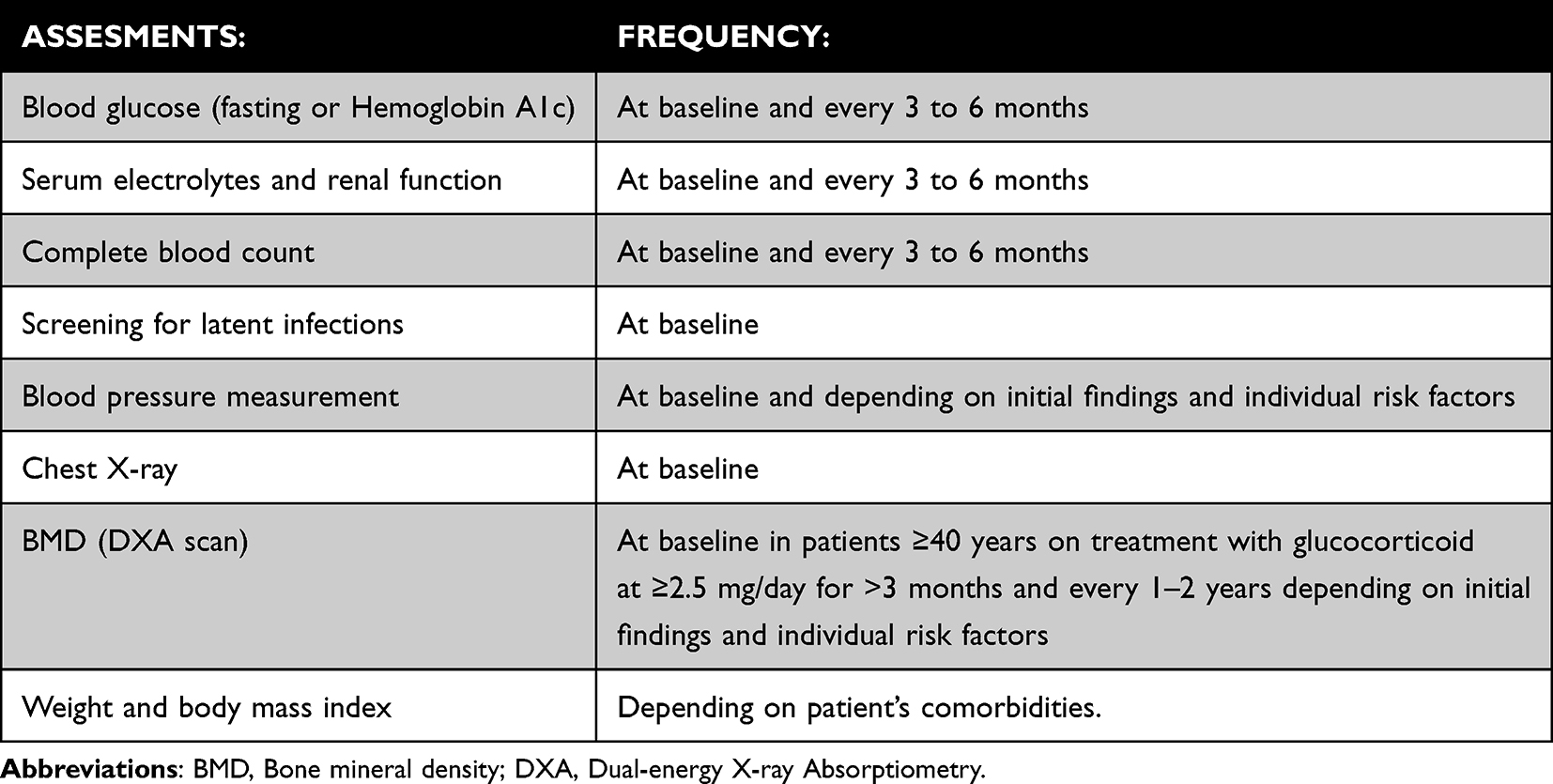 |
Table 1 Recommended Baseline and Follow-up Assessments for Patients with Non-Infectious Uveitis Receiving Systemic Corticosteroid Therapy |
Additional assessments may be indicated based on patient-specific risk factors, such as psychiatric history (for mood disorders), gastrointestinal history (for peptic ulcer risk), and cardiovascular risk profile. Patient education regarding infection risk, adrenal suppression, and the need for regular follow-up is also essential.41
However, recommended baseline assessments and tests should not delay the initiation of systemic corticosteroid therapy when urgent treatment is needed to prevent vision loss in a patient with NIU at risk of vision-threatening disease. In cases where there is imminent risk to vision, immediate initiation of high-dose systemic corticosteroids is recommended to rapidly control inflammation and prevent irreversible ocular damage, even if all baseline investigations have not yet been completed.4,41,44 Baseline assessments are important for identifying risk factors and guiding ongoing management, but they should be performed concurrently with, rather than prior to, urgent corticosteroid initiation in vision-threatening situations. This approach is consistent with expert opinion and clinical practice, which prioritize preservation of vision over the potential risks of corticosteroid therapy in the acute setting.4,36,41,44
Bone Protection
Corticosteroids decrease bone formation and increase bone resorption, leading to bone loss and increased fracture risk. The primary mechanisms include direct inhibition of osteoblastogenesis, promotion of osteoblast and osteocyte apoptosis, and stimulation of osteoclast activity via increased Receptor Activator of Nuclear Factor Kappa-ß Ligand (RANKL) expression.46–52 These effects result in rapid bone loss, particularly in the first 3 to 6 months of therapy, and a marked increase in vertebral and hip fracture risk, even at low to moderate doses (eg, 2.5–7.5 mg prednisolone daily).46–53
Corticosteroids also have indirect effects on bone, such as reducing muscle mass (increasing fall risk), decreasing sex hormone levels, and altering calcium metabolism. The risk of bone loss and fracture is dose- and duration-dependent, but it can occur even with inhaled or intermittent high-dose regimens. Discontinuation of corticosteroids leads to partial recovery of bone mineral density and reduction in fracture risk.46,54
Patients at high risk for corticosteroid-induced bone loss are those who are older (especially age >55 years), postmenopausal women, individuals receiving a daily dose of prednisone higher than 7.5 mg/day (or equivalent), those with prolonged or recent glucocorticoid exposure (≥3 months), an cumulative dose of prednisone > 5 g/year and patients with underlying conditions such as rheumatoid arthritis, inflammatory bowel disease (IBD), or other chronic inflammatory diseases. Additional risk factors include prior fragility fracture, low bone mineral density (T-score <−1.5), white race, low BMI (<18.5), hypogonadism, menopause, smoking, excessive alcohol use, and increased fall risk. The risk of rapid bone loss and fragility fractures is particularly pronounced in the first 3 to 6 months of therapy and increases with both dose and duration of corticosteroid use. Even low doses (as low as 2.5 mg/day) can contribute to bone loss, but fracture risk rises substantially at doses ≥5–7.5 mg/day and with cumulative exposure.46,55–57
Notably, the American College of Rheumatology recommend that all adults receiving ≥2.5 mg of prednisone daily for more than 3 months should be considered at risk of glucocorticoid induced osteoporosis, with higher risk thresholds for those on ≥7.5 mg/day or with additional risk factors. Although the risk of bone loss and fracture decreases after discontinuation of corticosteroids, it may not fully normalize, particularly after prolonged or high-dose exposure.46,53,54,56
The most effective screening strategies for early detection of bone loss in high-risk groups for corticosteroid-induced bone loss are:
1. Early and systematic clinical risk assessment: This includes a detailed history of prior fractures (symptomatic and asymptomatic), glucocorticoid dose and duration, fall risk, low body weight, smoking, alcohol use, hypogonadism, and comorbidities such as rheumatoid arthritis or inflammatory bowel disease. The American College of Rheumatology recommends this assessment for all adults (≥18 years) initiating or continuing glucocorticoid therapy at ≥2.5 mg/day for >3 months, ideally within 6 months of starting therapy.58
2. BMD assessment by DXA: DXA of the lumbar spine and hip is the gold standard for detecting bone loss and should be performed at baseline in patients ≥40 years on treatment with glucocorticoid at ≥2.5 mg/day for >3 months. Repeat DXA is typically advised every 1–2 years depending on initial findings and individual risk factors.58
3. Vertebral fracture assessment (VFA) or lateral spine X-ray: The American College of Rheumatology strongly recommends VFA or spine X-ray at baseline to detect asymptomatic vertebral fractures, which are common and may influence management decisions. Reassessment is advised every 1–2 years if patients continue chronic glucocorticoid therapy at doses ≥2.5 mg/day.56,58
4. Fracture risk estimation using FRAX: For adults ≥40 years, the FRAX tool (with BMD if available) should be used to estimate 10-year fracture risk, with dose adjustment for prednisone >7.5 mg/day (as this is associated with an increase on major osteoporotic fracture risk by 15% and hip fracture risk by 20%). FRAX is not validated for individuals under 40 years or for reassessment during ongoing therapy.58
The most effective alternative medications for the prevention of bone loss in patients at high risk for corticosteroid-induced osteoporosis are oral bisphosphonates, intravenous bisphosphonates, denosumab, and anabolic agents, such as teriparatide or abaloparatide.
For prevention of glucocorticoid-induced osteoporosis in adults beginning long-term therapy, the American College of Rheumatology strongly recommends oral bisphosphonates (like alendronate or risedronate) as first-line therapy due to their efficacy, safety, and cost-effectiveness. Intravenous bisphosphonates (zoledronic acid, ibandronate) are appropriate for patients who cannot tolerate or adhere to oral therapy. Denosumab is a monoclonal antibody that is an alternative for those with contraindication or intolerance to bisphosphonates and has demonstrated superiority to risedronate in increasing spine bone mineral density in glucocorticoid-treated patients.
Anabolic agents are conditionally recommended as initial therapy over antiresorptive agents for patients at very high fracture risk, such as those with prior fragility fracture, very low BMD, or high dose/prolonged glucocorticoid exposure (>5 g/year), as they increase bone formation and reduce vertebral fracture risk more than bisphosphonates.
Raloxifene (for postmenopausal women intolerant to other agents) and romosozumab (a dual-acting agent that both stimulates bone formation and inhibits bone resorption, in select cases) are additional options but are generally reserved for those who cannot use other therapies due to safety concerns. It is also important to note that abaloparatide and romosozumab are not approved for the treatment of glucocorticoid-induced osteoporosis, and access to these medications for this indication may therefore be limited.58 Furthermore, after discontinuation of anabolic therapy, transition to an antiresorptive agent is recommended to maintain gains in bone density. Similarly, discontinuation of denosumab must be followed by bisphosphonates, beginning at 6 to 7 months after the last dose to prevent rapid bone loss and multiple vertebral fractures.56,58–60
All patients should also receive adequate calcium and vitamin D supplementation and lifestyle optimization. Dietary and supplemented elemental calcium intake of up to 1,000 to 1,200 mg daily is recommended for adults, and serum vitamin D levels should be monitored and vitamin D supplemented to maintain serum vitamin D levels ≥30 to 50 ng/mL (600 to 800 IU daily or more is typically required). Lifestyle modifications should include avoiding smoking, moderating alcohol intake to no more than two drinks per day, following a balanced diet, keeping a healthy body weight in the recommended range and engaging regularly in weight-bearing or resistance exercises.56,58–61
Gastrointestinal Protection
Corticosteroids can affect the gastrointestinal (GI) tract, most notably increasing the risk of gastrointestinal bleeding and peptic ulcer disease. This risk is well established in hospitalized or critically ill patients, especially when used with non-steroidal anti-inflammatory drugs (NSAIDs), but remains controversial in ambulatory patients.62–64
Recent case-control studies have shown that the use of NSAIDs, either alone or in combination with corticosteroids, is associated with a markedly increased risk of peptic ulcer bleeding compared with corticosteroid monotherapy. However, corticosteroids alone were linked to only a moderate increase in risk.65,66 Earlier clinical trials, by contrast, yielded conflicting results, with some suggesting a dose-dependent increase in peptic ulcer risk with corticosteroids,67 while others found no significant difference between corticosteroid and placebo groups.68
The recommended strategies to reduce gastrointestinal complications are currently restricted to high-risk patients on corticosteroids, which include concomitant use of NSAIDs, aspirin, or prior history of peptic ulcer disease or GI bleeding. In these cases, proton pump inhibitors (PPIs) are the preferred gastroprotective option.69 Helicobacter pylori testing and eradication are recommended in patients with a history of peptic ulcers or GI bleeding, as eradication reduces the risk of recurrence. Nevertheless, maintenance PPI therapy remains advisable if concomitant NSAID or antiplatelet treatment is ongoing.70
Altered gastrointestinal motility may also occur, with corticosteroids potentially accelerating gastric emptying and affecting small intestinal transit, though these effects are less clinically significant than bleeding or ulceration.71–73
Adrenal Insufficiency
Glucocorticoid-induced adrenal insufficiency is the most common form of adrenal insufficiency, and the risk is primarily determined by the dose, duration, and route of glucocorticoid administration. According to the 2024 joint clinical guideline from the Endocrine Society and the European Society of Endocrinology, the pooled risk of biochemical adrenal insufficiency after oral glucocorticoid therapy is approximately 48.7% (95% CI, 36.9–60.6), with a higher risk associated with higher doses and longer treatment durations. For example, treatment exceeding one year can result in a risk of 27.4% (95% CI, 17.7–39.8) in asthma patients, and a similar risk is expected in other chronic inflammatory conditions such as NIU.74,75
In the context of NIU, systemic corticosteroids are often used at doses exceeding 7.5 mg/day of prednisone for months, which is well within the range associated with hypothalamic-pituitary-adrenal axis suppression and subsequent adrenal insufficiency. The risk is not negligible even at lower doses or with shorter courses, as suppression can occur with as little as 5 mg/day of prednisone for 3–4 weeks or longer.75
Patients at higher risk for developing adrenal insufficiency during systemic corticosteroid treatment for NIU include those receiving higher daily doses (prednisone ≥7.5 mg/day), those on prolonged courses (≥3–4 weeks), older adults, and individuals with repeated or cumulative exposure to multiple glucocorticoid formulations (oral, inhaled, or injected). The risk is also increased in patients who undergo rapid tapering or abrupt discontinuation of steroids, and in those with comorbidities that increase susceptibility to infections, as intercurrent illness is a common trigger for adrenal crisis in this population.74,76
Early symptoms that may indicate the development of adrenal insufficiency include fatigue, anorexia, weight loss, nausea, vomiting, abdominal pain, muscle or joint pain, and hypotension. These symptoms are often nonspecific and can overlap with the underlying disease or with glucocorticoid withdrawal syndrome, making clinical recognition challenging.76,77
The European Society of Endocrinology emphasizes that hypotension (including postural hypotension), severe fatigue, gastrointestinal symptoms (nausea, vomiting, abdominal pain), and impaired consciousness (lethargy, confusion, somnolence) are key early clinical features, particularly during or after glucocorticoid tapering or abrupt cessation. Laboratory findings may include hyponatremia, hypoglycemia, and, less commonly, hyperkalemia. The risk of adrenal crisis is highest during periods of physiological stress (eg, infection, surgery) or rapid steroid dose reduction.74 Therefore, the EULAR recommends adequate glucocorticoid replacement in acute situations for patients receiving chronic medium- or high-dose corticosteroid therapy, emphasizing that treatment should not be discontinued abruptly but tapered gradually. Currently, there is no evidence to support the superiority of any specific replacement or stress-dose regimen. In practice, clinicians may either increase the oral glucocorticoid dose for approximately three days or, depending on the clinical scenario, switch to intravenous hydrocortisone (eg, twice daily 25 mg for patients on 10 mg prednisone daily, or three times daily 50 mg for those on high-dose glucocorticoid therapy). Although higher stress-dose regimens have not been proven necessary, they may be considered in selected cases.78
For the diagnosis of adrenal insufficiency in clinically suspected cases, the European Society of Endocrinology and the Endocrine Society recommend initial assessment with an early-morning (typically 8 am) serum cortisol measurement, ideally at least 24 hours after the last glucocorticoid dose to avoid interference from exogenous steroids. A morning cortisol level <5 µg/dl (<138 nmol/l) is highly suggestive of adrenal insufficiency, while a level >10 µg/dl (>276 nmol/l) generally excludes the diagnosis and steroids can be stopped safely. Intermediate values (5–10 µg/dl) require further evaluation with a corticotropin (cosyntropin) stimulation test, measuring serum cortisol before and 30–60 minutes after intravenous administration of 250 µg cosyntropin. Failure to achieve a peak cortisol >18 µg/dL (500 nmol/l) confirms adrenal insufficiency in this context.74
Uncommon Side Effects
Less common side effects of the use of corticosteroids that the clinician needs to be aware of include:
Use in Particular Populations
Pediatric Population
When using systemic corticosteroids to treat NIU in children, several caveats and considerations are critical due to the unique vulnerability of the pediatric population to adverse effects (Table 2). Growth retardation, weight gain, and cushingoid features are among the most common side effects, with growth suppression being particularly concerning due to the impact on final adult height. Osteoporosis and decreased bone density are also significant risks, with decreased bone density observed in over 20% of children on long-term corticosteroids and a smaller but real risk of osteoporosis and fractures.84
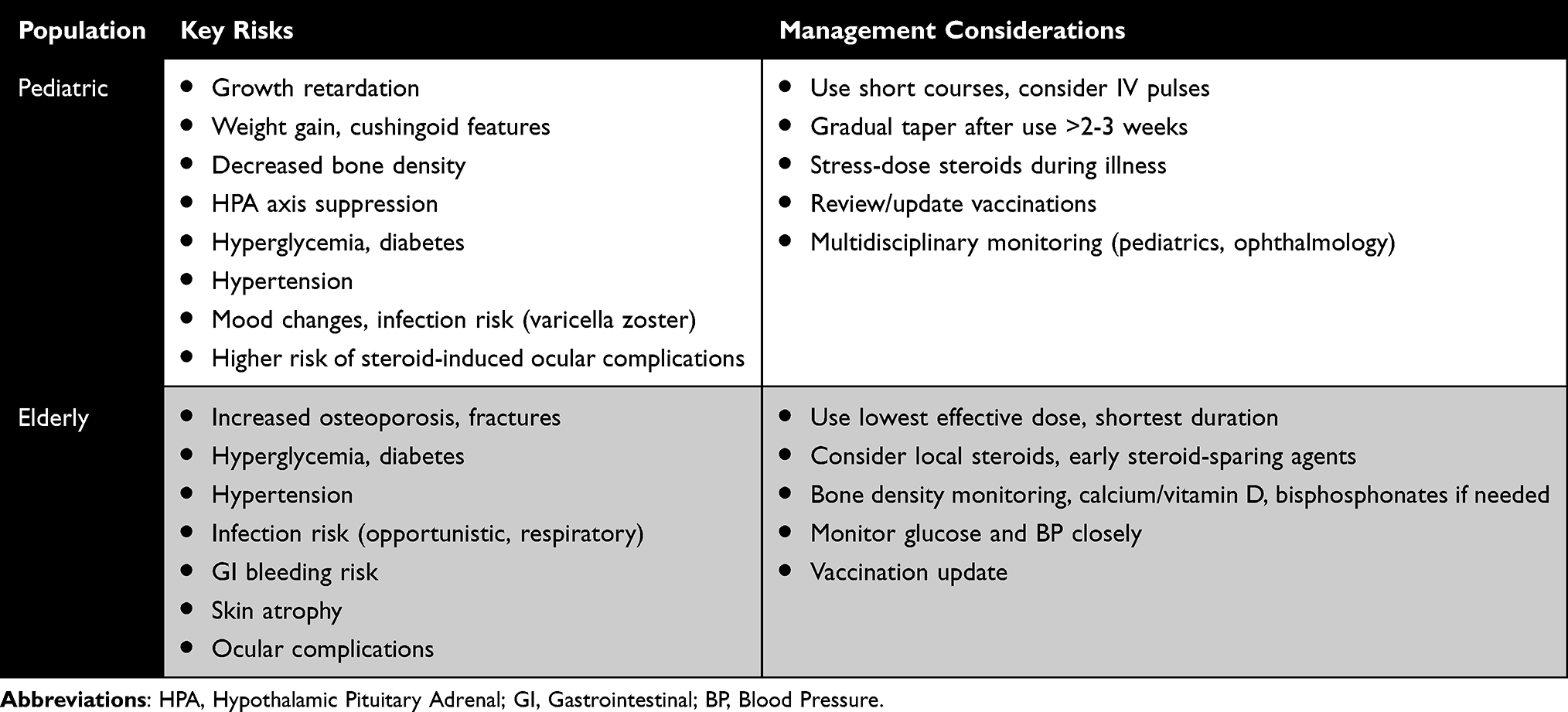 |
Table 2 Key Risks and Management Considerations of Systemic Corticosteroid Use in Special Populations with Non-Infectious Uveitis |
Suppression of the hypothalamic-pituitary-adrenal axis is especially important in children, who are less resilient than adults, may show nonspecific symptoms, and face risks to growth and development. Gradual tapering after prolonged use (>2–3 weeks) and stress-dose steroids during illness or procedures are essential.85
Hyperglycemia and new-onset diabetes mellitus are dose-dependent risks, with high-dose regimens increasing the risk substantially. Hypertension is also a well-documented complication, with a strong dose-response relationship.86 Weight gain and central adiposity are also frequent and can contribute to metabolic syndrome. Skin changes (striae, acne, easy bruising) are common.84 While mood changes (anxiety, agitation, sleep disturbance) are more commonly seen in pediatric steroid users, frank psychosis remains a rare and underreported event.87
Increased susceptibility to infections is the most serious risk, with varicella zoster being particularly dangerous and responsible for mortality in this population; vaccination status should be reviewed and updated before initiating therapy.84,88
Ocular hypertension, glaucoma, and cataract formation are particularly relevant in pediatric uveitis, with children at higher risk for steroid-induced glaucoma and cataracts than adults.88–90
The goal of corticosteroid treatment in children should be a brief, short course of steroids, including intravenous pulses of methylprednisolone (if that means a shorter use of systemic steroids).91,92
Multidisciplinary care, including pediatric rheumatology and ophthalmology, is essential for optimal monitoring and management of these adverse effects.88–90
Elderly
For the safe use of corticosteroids in this population, the clinician should always keep in mind that in the elderly, there is a notable shift away from classic autoimmune causes toward infectious and neoplastic etiologies such as herpetic uveitis and intraocular lymphoma, where the use of steroids may be contraindicated.93,94
When using systemic corticosteroids to treat NIU in elderly patients, special considerations are required due to increased vulnerability to adverse effects and comorbidities (Table 2). The elderly are at increased risk for osteoporosis, fractures, avascular necrosis, hyperglycemia/diabetes, hypertension, infections, gastrointestinal bleeding, skin atrophy, and ocular complications such as glaucoma and cataract. The risk of these complications is dose- and duration-dependent, and even short courses can precipitate significant morbidity in this population.43,44
To minimize these risks, corticosteroids should be used at the lowest effective dose for the shortest possible duration, and early transition to steroid-sparing immunosuppressive agents is recommended. Local corticosteroid delivery may be considered to reduce systemic exposure in selected cases. Elderly patients require vigilant monitoring and proactive management of corticosteroid-related adverse effects.43,44
Conclusions
Corticosteroids remain the foundational therapy in the management of non-infectious uveitis due to their potent and rapid anti-inflammatory effects across all anatomical subtypes. However, their effectiveness must be balanced against the risks of both ocular and systemic adverse effects, which vary depending on the route of administration and duration of use. A strategic, individualized approach to corticosteroid therapy, tailored to the anatomical location, laterality, severity, and chronicity of inflammation, is essential to maximize therapeutic benefit while minimizing toxicity. Topical, periocular, intravitreal, and systemic corticosteroids each play a specific role in the stepwise management of uveitis, and their integration must be guided by clinical judgment and disease.
Given the limitations of prolonged corticosteroid exposure, early consideration of immunomodulatory therapies is warranted in many cases to achieve durable disease control and enable steroid tapering. Recent advances in sustained-release corticosteroid implants and novel drug delivery platforms hold promise for improving patient outcomes with reduced treatment burden. Continued research into personalized treatment algorithms, biomarker-driven approaches, and steroid-sparing strategies will be key to optimizing care for patients with uveitis.
In summary, while corticosteroids remain indispensable in the initial and adjunctive treatment of uveitis, their long-term success depends on thoughtful application within a comprehensive, multidisciplinary management framework.
Data Sharing Statement
No new data were generated or analyzed in support of this article. All data cited in this review are available in the public domain and referenced within the article.
Author Contributions
Conceptualization: Carolina Tornero, Otto M. Olivas-Vergara, Diana Peiteado & Ester Carreño.
Data curation (reference organization, synthesis of findings): All the authors.
Formal analysis (analyze or synthesize study data): All the authors.
Investigation (data/evidence collection): All the authors.
Methodology: All the authors.
Writing – Original Draft: Matteo Belletti, Rosario Izquierdo-Escamez, Ester Carreño
Writing – Review & Editing: Carolina Tornero, Otto M. Olivas-Vergara, Diana Peiteado, Ester Carreño.
Resources: N/A.
Software: N/A.
Validation: N/A
Visualization: All the authors.
Supervision: Ester Carreño
Project Administration: Ester Carreño.
Funding Acquisition: N/A.
All authors agreed to the final version of the paper accepted for publication; agreed to submit to this journal; and agree to be accountable for the contents of this paper.
Funding
No funding was received.
Disclosure
Ester Carreño reports personal fees from Roche, Active Biotech, Santen outside the submitted work. The other authors have no relevant financial or non-financial competing interests to report.
References
1. Dick AD, Rosenbaum JT, Al-Dhibi HA, et al. Guidance on noncorticosteroid systemic immunomodulatory therapy in noninfectious uveitis: Fundamentals Of Care for UveitiS (FOCUS) Initiative. Ophthalmology. 2018;125(5):757–773. doi:10.1016/j.ophtha.2017.11.017
2. Dick AD, Tundia N, Sorg R, et al. Risk of ocular complications in patients with noninfectious intermediate uveitis, posterior uveitis, or panuveitis. Ophthalmology. 2016;123(3):655–662. doi:10.1016/j.ophtha.2015.10.028
3. Durrani OM, Tehrani NN, Marr JE, Moradi P, Stavrou P, Murray PI. Degree, duration, and causes of visual loss in uveitis. Br J Ophthalmol. 2004;88(9):1159–1162. doi:10.1136/bjo.2003.037226
4. Maghsoudlou P, Epps SJ, Guly CM, Dick AD. Uveitis in adults: a review. JAMA. 2025;334:419. doi:10.1001/jama.2025.4358
5. Suhler EB, Thorne JE, Mittal M, et al. Corticosteroid-related adverse events systematically increase with corticosteroid dose in noninfectious intermediate, posterior, or panuveitis: post hoc analyses from the VISUAL-1 and VISUAL-2 Trials. Ophthalmology. 2017;124(12):1799–1807. doi:10.1016/j.ophtha.2017.06.017
6. Gutteridge IF, Hall AJ. Acute anterior uveitis in primary care. Clin Exp Optom. 2007;90(5):390. doi:10.1111/j.1444-0938.2007.00186.x
7. Balasubramaniam B, Chong YJ, Azzopardi M, Logeswaran A, Denniston AK. Topical anti-inflammatory agents for non-infectious uveitis: current treatment and perspectives. J Inflamm Res. 2022;15:6439–6451. doi:10.2147/JIR.S288294
8. Biswas J, Ganeshbabu TM, Raghavendran SR, Raizada S, Mondkar SV, Madhavan HN. Efficacy and safety of 1% rimexolone versus 1% prednisolone acetate in the treatment of anterior uveitis--a randomized triple masked study. Int Ophthalmol. 2004;25(3):147–153. doi:10.1007/s10792-004-5195-2
9. Hedayatfar A, Hashemi H, Asgari S, Chee SP. Comparison of efficacy and ocular surface toxicity of topical preservative-free methylprednisolone and preserved prednisolone in the treatment of acute anterior uveitis. Cornea. 2014;33(4):366–372. doi:10.1097/ICO.0000000000000039
10. Sheppard JD, Toyos MM, Kempen JH, Kaur P, Foster CS. Difluprednate 0.05% versus prednisolone acetate 1% for endogenous anterior uveitis: a Phase III, multicenter, randomized study. Invest Ophthalmol Vis Sci. 2014;55(5):2993–3002. doi:10.1167/iovs.13-12660
11. Foster CS, Davanzo R, Flynn TE, McLeod K, Vogel R, Crockett RS. Durezol (difluprednate ophthalmic emulsion 0.05%) compared with pred forte 1% ophthalmic suspension in the treatment of endogenous anterior uveitis. J Ocul Pharmacol Ther. 2010;26(5):475–483. doi:10.1089/jop.2010.0059
12. Yakin M, Kumar A, Kodati S, Jones L, Sen HN. Risk of elevated intraocular pressure with difluprednate in patients with non-infectious uveitis. Am J Ophthalmol. 2022;240:232–238. doi:10.1016/j.ajo.2022.03.026
13. Slabaugh MA, Herlihy E, Ongchin S, van Gelder RN. Efficacy and potential complications of difluprednate use for pediatric uveitis. Am J Ophthalmol. 2012;153(5):932–938. doi:10.1016/j.ajo.2011.10.008
14. Papaliodis GN, Rosner BA, Dreger KA, et al. Incidence of and risk factors for cataract in anterior uveitis. Am J Ophthalmol. 2023;254:221–232. doi:10.1016/j.ajo.2023.06.021
15. Thorne JE, Woreta FA, Dunn JP, Jabs DA. Risk of cataract development among children with juvenile idiopathic arthritis-related uveitis treated with topical corticosteroids. Ophthalmology. 2010;117(7):1436–1441. doi:10.1016/j.ophtha.2009.12.003
16. Reddy A, Liu SH, Brady CJ, Sieving PC, Palestine AG. Corticosteroid implants for chronic non-infectious uveitis. Cochrane Database Syst Rev. 2023;8(8):CD010469. doi:10.1002/14651858.CD010469.pub4
17. Tomkins-Netzer O, Lightman SL, Burke AE, et al. Seven-year outcomes of uveitic macular edema: the multicenter uveitis steroid treatment trial and follow-up study results. Ophthalmology. 2021;128(5):719–728. doi:10.1016/j.ophtha.2020.08.035
18. Kempen JH, Altaweel MM, Holbrook JT, et al. Randomized comparison of systemic anti-inflammatory therapy versus fluocinolone acetonide implant for intermediate, posterior, and panuveitis: the multicenter uveitis steroid treatment trial. Ophthalmology. 2011;118(10):1916–1926. doi:10.1016/j.ophtha.2011.07.027
19. Kempen JH, Altaweel MM, Drye LT, et al. Benefits of systemic anti-inflammatory therapy versus fluocinolone acetonide intraocular implant for intermediate uveitis, posterior uveitis, and panuveitis: fifty-four-month results of the Multicenter Uveitis Steroid Treatment (MUST) trial and follow-up study. Ophthalmology. 2015;122(10):1967–1975. doi:10.1016/j.ophtha.2015.06.042
20. Tomkins-Netzer O, Lightman S, Drye L, et al. Outcome of treatment of uveitic macular edema: the multicenter uveitis steroid treatment trial 2-year results. Ophthalmology. 2015;122(11):2351–2359. doi:10.1016/j.ophtha.2015.07.036
21. Kempen JH, Altaweel MM, Holbrook JT, et al. association between long-lasting intravitreous fluocinolone acetonide implant vs systemic anti-inflammatory therapy and visual acuity at 7 years among patients with intermediate, posterior, or panuveitis. JAMA. 2017;317(19):1993–2005. doi:10.1001/jama.2017.5103
22. Sugar EA, Holbrook JT, Kempen JH, et al. Cost-effectiveness of fluocinolone acetonide implant versus systemic therapy for noninfectious intermediate, posterior, and panuveitis. Ophthalmology. 2014;121(10):1855–1862. doi:10.1016/j.ophtha.2014.04.022
23. Jaffe GJ, Martin D, Callanan D, et al. Fluocinolone acetonide implant (Retisert) for noninfectious posterior uveitis: thirty-four-week results of a multicenter randomized clinical study. Ophthalmology. 2006;113(6):1020–1027. doi:10.1016/j.ophtha.2006.02.021
24. Friedman DS, Holbrook JT, Ansari H, et al. Risk of elevated intraocular pressure and glaucoma in patients with uveitis: results of the multicenter uveitis steroid treatment trial. Ophthalmology. 2013;120(8):1571–1579. doi:10.1016/j.ophtha.2013.01.025
25. Singer MA, Sheth V, Mansour SE, Coughlin B, Gonzalez VH. Three-year safety and efficacy of the 0.19-mg fluocinolone acetonide intravitreal implant for diabetic macular edema: the PALADIN study. Ophthalmology. 2022;129(6):605–613. doi:10.1016/j.ophtha.2022.01.015
26. Jaffe GJ, Pavesio CE, Investigators S. Effect of a fluocinolone acetonide insert on recurrence rates in noninfectious intermediate, posterior, or panuveitis: three-year results. Ophthalmology. 2020;127(10):1395–1404. doi:10.1016/j.ophtha.2020.04.001
27. Smith JR, Thorne JE, Flaxel CJ, et al. Treatment of noninfectious uveitic macular edema with periocular and intraocular corticosteroid therapies: a report by the American Academy of Ophthalmology. Ophthalmology. 2024;131(9):1107–1120. doi:10.1016/j.ophtha.2024.02.019
28. Thorne JE, Sugar EA, Holbrook JT, et al. Periocular triamcinolone vs. intravitreal triamcinolone vs. intravitreal dexamethasone implant for the treatment of uveitic macular edema: the periocular vs. intravitreal corticosteroids for uveitic macular edema (POINT) trial. Ophthalmology. 2019;126(2):283–295. doi:10.1016/j.ophtha.2018.08.021
29. Cheng SK, Thompson I, Okeagu C, Nida Sen H. Choroidal lesions unresponsive to fluocinolone acetonide intravitreal implant in birdshot chorioretinopathy. Retin Cases Brief Rep. 2022;16(1):56–58. doi:10.1097/ICB.0000000000000909
30. Kempen JH, Van Natta ML, Friedman DS, et al. Incidence and outcome of uveitic glaucoma in eyes with intermediate, posterior, or panuveitis followed up to 10 years after randomization to fluocinolone acetonide implant or systemic therapy. Am J Ophthalmol. 2020;219:303–316. doi:10.1016/j.ajo.2020.06.038
31. Group MUSTMTF-uSR. Quality of life and risks associated with systemic anti-inflammatory therapy versus fluocinolone acetonide intraocular implant for intermediate uveitis, posterior uveitis, or panuveitis: fifty-four-month results of the multicenter uveitis steroid treatment trial and follow-up study. Ophthalmology. 2015;122(10):1976–1986. doi:10.1016/j.ophtha.2015.06.043
32. Parekh A, Srivastava S, Bena J, Albini T, Nguyen QD, Goldstein DA. Risk factors associated with intraocular pressure increase in patients with uveitis treated with the fluocinolone acetonide implant. JAMA Ophthalmol. 2015;133(5):568–573. doi:10.1001/jamaophthalmol.2015.51
33. Roberti G, Oddone F, Agnifili L, et al. Steroid-induced glaucoma: epidemiology, pathophysiology, and clinical management. Surv Ophthalmol. 2020;65(4):458–472. doi:10.1016/j.survophthal.2020.01.002
34. Henry CR, Shah M, Barakat MR, et al. Suprachoroidal CLS-TA for non-infectious uveitis: an open-label, safety trial (AZALEA). Br J Ophthalmol. 2022;106(6):802–806. doi:10.1136/bjophthalmol-2020-318019
35. Fung S, Syed YY. Suprachoroidal space triamcinolone acetonide: a review in uveitic macular edema. Drugs. 2022;82(13):1403–1410. doi:10.1007/s40265-022-01777-1
36. Jabs DA. Immunosuppression for the Uveitides. Ophthalmology. 2018;125(2):193–202. doi:10.1016/j.ophtha.2017.08.007
37. Nguyen QD, Hatef E, Kayen B, et al. A cross-sectional study of the current treatment patterns in noninfectious uveitis among specialists in the United States. Ophthalmology. 2011;118(1):184–190. doi:10.1016/j.ophtha.2010.03.029
38. Vegas-Revenga N, Martín-Varillas JL, Calvo-Río V, et al. Intravenous methylprednisolone induces rapid improvement in non-infectious uveitis: a multicentre study of 112 patients. Clin Exp Rheumatol. 2022;40(1):142–149. doi:10.55563/clinexprheumatol/imrgo2
39. Jabs DA, Rosenbaum JT, Foster CS, et al. Guidelines for the use of immunosuppressive drugs in patients with ocular inflammatory disorders: recommendations of an expert panel. Am J Ophthalmol. 2000;130(4):492–513. doi:10.1016/S0002-9394(00)00659-0
40. Charkoudian LD, Ying GS, Pujari SS, et al. High-dose intravenous corticosteroids for ocular inflammatory diseases. Ocul Immunol Inflamm. 2012;20(2):91–99. doi:10.3109/09273948.2011.646382
41. Stanbury RM, Graham EM. Systemic corticosteroid therapy--side effects and their management. Br J Ophthalmol. 1998;82(6):704–708. doi:10.1136/bjo.82.6.704
42. Posarelli C, Talarico R, Vella G, Passani A, Mosca M, Figus M. Do systemic steroids increase the risk of ocular complication in uveitis patients? Focus on a Italian referral center. Clin Rheumatol. 2019;38(10):2917–2923. doi:10.1007/s10067-019-04585-3
43. Ormaechea MS, Hassan M, Onghanseng N, et al. Safety of systemic therapy for noninfectious uveitis. Expert Opin Drug Saf. 2019;18(12):1219–1235. doi:10.1080/14740338.2019.1692810
44. Valdes LM, Sobrin L. Uveitis therapy: the corticosteroid options. Drugs. 2020;80(8):765–773. doi:10.1007/s40265-020-01314-y
45. Hoes JN, Jacobs JW, Boers M, et al. EULAR evidence-based recommendations on the management of systemic glucocorticoid therapy in rheumatic diseases. Ann Rheum Dis. 2007;66(12):1560–1567. doi:10.1136/ard.2007.072157
46. Buckley L, Humphrey MB. Glucocorticoid-Induced Osteoporosis. N Engl J Med. 2018;379(26):2547–2556. doi:10.1056/NEJMcp1800214
47. Gado M, Baschant U, Hofbauer LC, Henneicke H. Bad to the bone: the effects of therapeutic glucocorticoids on osteoblasts and osteocytes. Front Endocrinol. 2022;13:835720. doi:10.3389/fendo.2022.835720
48. Komori T. Glucocorticoid signaling and bone biology. Horm Metab Res. 2016;48(11):755–763. doi:10.1055/s-0042-110571
49. Hardy RS, Zhou H, Seibel MJ, Cooper MS. Glucocorticoids and bone: consequences of endogenous and exogenous excess and replacement therapy. Endocr Rev. 2018;39(5):519–548. doi:10.1210/er.2018-00097
50. Hartmann K, Koenen M, Schauer S, et al. Molecular actions of glucocorticoids in cartilage and bone during health, disease, and steroid therapy. Physiol Rev. 2016;96(2):409–447. doi:10.1152/physrev.00011.2015
51. Canalis E, Delany AM. Mechanisms of glucocorticoid action in bone. Ann N Y Acad Sci. 2002;966:73–81. doi:10.1111/j.1749-6632.2002.tb04204.x
52. Weinstein RS, Jilka RL, Parfitt AM, Manolagas SC. Inhibition of osteoblastogenesis and promotion of apoptosis of osteoblasts and osteocytes by glucocorticoids. Potential mechanisms of their deleterious effects on bone. J Clin Invest. 1998;102(2):274–282. doi:10.1172/JCI2799
53. Adami G, Fassio A, Rossini M, et al. Bone loss in inflammatory rheumatic musculoskeletal disease patients treated with low-dose glucocorticoids and prevention by anti-osteoporosis medications. Arthritis Rheumatol. 2023;75(10):1762–1769. doi:10.1002/art.42529
54. Urquiaga M, Saag KG. Risk for osteoporosis and fracture with glucocorticoids. Best Pract Res Clin Rheumatol. 2022;36(3):101793. doi:10.1016/j.berh.2022.101793
55. Chotiyarnwong P, McCloskey EV. Pathogenesis of glucocorticoid-induced osteoporosis and options for treatment. Nat Rev Endocrinol. 2020;16(8):437–447. doi:10.1038/s41574-020-0341-0
56. Compston JE. Extensive expertise in endocrinology: advances in the management of glucocorticoid-induced osteoporosis. Eur J Endocrinol. 2023;188(3):R46–R55. doi:10.1093/ejendo/lvad029
57. Adami G, Saag KG. Glucocorticoid-induced osteoporosis: 2019 concise clinical review. Osteoporos Int. 2019;30(6):1145–1156. doi:10.1007/s00198-019-04906-x
58. Humphrey MB, Russell L, Danila MI, et al. American college of rheumatology guideline for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Rheumatol. 2023;75(12):2088–2102. doi:10.1002/art.42646
59. Agarwal A, Adachi JD. Therapies for preventing bone loss with glucocorticoid treatment. Curr Osteoporos Rep. 2021;19(1):34–39. doi:10.1007/s11914-020-00653-9
60. Raterman HG, Bultink IEM, Lems WF. Current treatments and new developments in the management of glucocorticoid-induced osteoporosis. Drugs. 2019;79(10):1065–1087. doi:10.1007/s40265-019-01145-6
61. Paccou J, Yavropoulou MP, Naciu AM, et al. Prevention and treatment of glucocorticoid-induced osteoporosis in adults: recommendations from the European Calcified Tissue Society. Eur J Endocrinol. 2024;191(6):G1–G17. doi:10.1093/ejendo/lvae146
62. Narum S, Westergren T, Klemp M. Corticosteroids and risk of gastrointestinal bleeding: a systematic review and meta-analysis. BMJ Open. 2014;4(5):e004587. doi:10.1136/bmjopen-2013-004587
63. Nielsen GL, Sørensen HT, Mellemkjoer L, et al. Risk of hospitalization resulting from upper gastrointestinal bleeding among patients taking corticosteroids: a register-based cohort study. Am J Med. 2001;111(7):541–545. doi:10.1016/S0002-9343(01)00941-X
64. Butler E, Møller MH, Cook O, et al. The effect of systemic corticosteroids on the incidence of gastrointestinal bleeding in critically ill adults: a systematic review with meta-analysis. Intensive Care Med. 2019;45(11):1540–1549. doi:10.1007/s00134-019-05754-3
65. Reinau D, Schwenkglenks M, Früh M, Signorell A, Blozik E, Meier CR. Glucocorticoids and the risk of peptic ulcer bleeding: case-control analysis based on Swiss claims data. Drug Saf. 2018;41(7):725–730. doi:10.1007/s40264-018-0645-3
66. Tseng CL, Chen YT, Huang CJ, et al. Short-term use of glucocorticoids and risk of peptic ulcer bleeding: a nationwide population-based case-crossover study. Aliment Pharmacol Ther. 2015;42(5):599–606. doi:10.1111/apt.13298
67. Messer J, Reitman D, Sacks HS, Smith H, Chalmers TC. Association of adrenocorticosteroid therapy and peptic-ulcer disease. N Engl J Med. 1983;309(1):21–24. doi:10.1056/NEJM198307073090105
68. Conn HO, Poynard T. Corticosteroids and peptic ulcer: meta-analysis of adverse events during steroid therapy. J Intern Med. 1994;236(6):619–632. doi:10.1111/j.1365-2796.1994.tb00855.x
69. Lanza FL, Chan FK, Quigley EM. Gastroenterology PPCotACo. Guidelines for prevention of NSAID-related ulcer complications. Am J Gastroenterol. 2009;104(3):728–738. doi:10.1038/ajg.2009.115
70. Nagata N, Niikura R, Sekine K, et al. Risk of peptic ulcer bleeding associated with Helicobacter pylori infection, nonsteroidal anti-inflammatory drugs, low-dose aspirin, and antihypertensive drugs: a case-control study. J Gastroenterol Hepatol. 2015;30(2):292–298. doi:10.1111/jgh.12805
71. Caplan A, Fett N, Rosenbach M, Werth VP, Micheletti RG. Prevention and management of glucocorticoid-induced side effects: a comprehensive review: gastrointestinal and endocrinologic side effects. J Am Acad Dermatol. 2017;76(1):11–16. doi:10.1016/j.jaad.2016.02.1239
72. Tena-Garitaonaindia M, Arredondo-Amador M, Mascaraque C, et al. Modulation of intestinal barrier function by glucocorticoids: lessons from preclinical models. Pharmacol Res. 2022;177:106056. doi:10.1016/j.phrs.2022.106056
73. Filaretova L, Podvigina T, Yarushkina N. Physiological and pharmacological effects of glucocorticoids on the gastrointestinal tract. Curr Pharm Des. 2020;26(25):2962–2970. doi:10.2174/1381612826666200521142746
74. Beuschlein F, Else T, Bancos I, et al. European society of endocrinology and endocrine society joint clinical guideline: diagnosis and therapy of glucocorticoid-induced adrenal insufficiency. Eur J Endocrinol. 2024;190(5):G25–G51. doi:10.1093/ejendo/lvae029
75. Broersen LH, Pereira AM, Jørgensen JO, Dekkers OM. Adrenal Insufficiency in corticosteroids use: systematic review and meta-analysis. J Clin Endocrinol Metab. 2015;100(6):2171–2180. doi:10.1210/jc.2015-1218
76. Vaidya A, Findling J, Bancos I. Adrenal insufficiency in adults: a review. JAMA. 2025;334:714. doi:10.1001/jama.2025.5485
77. Laugesen K, Petersen I, Sørensen HT, Jørgensen JOL. Clinical indicators of adrenal insufficiency following discontinuation of oral glucocorticoid therapy: a Danish population-based self-controlled case series analysis. PLoS One. 2019;14(2):e0212259. doi:10.1371/journal.pone.0212259
78. Duru N, van der Goes MC, Jacobs JW, et al. EULAR evidence-based and consensus-based recommendations on the management of medium to high-dose glucocorticoid therapy in rheumatic diseases. Ann Rheum Dis. 2013;72(12):1905–1913.
79. Pereira RM, Freire de Carvalho J. Glucocorticoid-induced myopathy. Joint Bone Spine. 2011;78(1):41–44. doi:10.1016/j.jbspin.2010.02.025
80. Haran M, Schattner A, Kozak N, Mate A, Berrebi A, Shvidel L. Acute steroid myopathy: a highly overlooked entity. QJM. 2018;111(5):307–311. doi:10.1093/qjmed/hcy031
81. Mont MA, Pivec R, Banerjee S, Issa K, Elmallah RK, Jones LC. High-dose corticosteroid use and risk of hip osteonecrosis: meta-analysis and systematic literature review. J Arthroplasty. 2015;30(9):1506–1512e1505. doi:10.1016/j.arth.2015.03.036
82. Aaron RK, Voisinet A, Racine J, Ali Y, Feller ER. Corticosteroid-associated avascular necrosis: dose relationships and early diagnosis. Ann N Y Acad Sci. 2011;1240:38–46. doi:10.1111/j.1749-6632.2011.06218.x
83. Lagerberg T, Gustafsson TT, Molero Y, et al. Oral glucocorticoids and risk of psychiatric and suicidal behaviour outcomes: population-based cohort study. Br J Psychiatry;2025. 1–8. doi:10.1192/bjp.2025.128
84. Aljebab F, Choonara I, Conroy S. Systematic review of the toxicity of long-course oral corticosteroids in children. PLoS One. 2017;12(1):e0170259. doi:10.1371/journal.pone.0170259
85. Improda N, Chioma L, Capalbo D, Bizzarri C, Salerno M. Glucocorticoid treatment and adrenal suppression in children: current view and open issues. J Endocrinol Invest. 2025;48(1):37–52. doi:10.1007/s40618-024-02461-9
86. Horton DB, Xie F, Chen L, et al. Oral glucocorticoids and incident treatment of diabetes mellitus, hypertension, and venous thromboembolism in children. Am J Epidemiol. 2021;190(3):403–412. doi:10.1093/aje/kwaa197
87. Fani-Molky P, Bradley J, Cooper MS. Glucocorticoid-Induced psychosis in children and adolescents: a systematic review. J Child Adolesc Psychopharmacol. 2023;33(3):78–90. doi:10.1089/cap.2022.0077
88. Leal I, Steeples LR, Wong SW, et al. Update on the systemic management of noninfectious uveitis in children and adolescents. Surv Ophthalmol. 2024;69(1):103–121. doi:10.1016/j.survophthal.2023.01.002
89. Nguyen AT, Kone-Paut I, Dusser P. Diagnosis and management of non-infectious uveitis in pediatric patients. Paediatr Drugs. 2024;26(1):31–47. doi:10.1007/s40272-023-00596-5
90. Pilly B, Heath G, Tschuor P, Lightman S, Gale RP. Overview and recent developments in the medical management of paediatric uveitis. Expert Opin Pharmacother. 2013;14(13):1787–1795. doi:10.1517/14656566.2013.816677
91. Ghoraba HH, Matsumiya W, Khojasteh H, et al. Safety of intravenous methylprednisolone in refractory and severe pediatric uveitis. Clin Ophthalmol. 2022;16:1697–1706. doi:10.2147/OPTH.S366370
92. Schnabel A, Unger E, Bruck N, et al. High-dose intravenous methylprednisolone in juvenile non-infectious uveitis: a retrospective analysis. Clin Immunol. 2020;211:108327. doi:10.1016/j.clim.2019.108327
93. Thorne JE, Suhler E, Skup M, et al. Prevalence of noninfectious uveitis in the united states: a claims-based analysis. JAMA Ophthalmol. 2016;134(11):1237–1245. doi:10.1001/jamaophthalmol.2016.3229
94. Samalia P, Sims J, Niederer R. The role of ageing in the clinical presentation of uveitis. Am J Ophthalmol. 2025;272:58–66. doi:10.1016/j.ajo.2025.01.007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Efficacy and Low Adverse Events of Methylprednisolone Pulses Combined to Low-Dose Glucocorticoids for Systemic Sclerosis: A Retrospective Clinical Study of 10 Years’ Follow-Up
Cheng H, Yu Z, Yan CL, Yang HD, Gao C, Wen HY
Journal of Inflammation Research 2022, 15:4421-4433
Published Date: 4 August 2022
Tocilizumab for Non-Infectious Uveitis: A Systematic Review
Cao H, Bian K, Ma C, Zhang N, Ma X
Journal of Inflammation Research 2025, 18:13117-13138
Published Date: 20 September 2025