Back to Journals » Journal of Inflammation Research » Volume 18
Tocilizumab for Non-Infectious Uveitis: A Systematic Review
Authors Cao H ![]() , Bian K
, Bian K ![]() , Ma C, Zhang N
, Ma C, Zhang N ![]() , Ma X
, Ma X ![]()
Received 20 May 2025
Accepted for publication 9 September 2025
Published 20 September 2025 Volume 2025:18 Pages 13117—13138
DOI https://doi.org/10.2147/JIR.S533011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Justin Jacob
Haixing Cao,* Kaiyu Bian,* Cong Ma, Naiwen Zhang, Xiang Ma
Department of Ophthalmology, The First Affiliated Hospital of Dalian Medical University, Dalian, Liaoning Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiang Ma, Department of Ophthalmology, the First Affiliated Hospital of Dalian Medical University, 222 Zhongshan Road, Dalian City, Liaoning Province, 116011, People’s Republic of China, Tel +8618098876399, Email [email protected]
Abstract: Non-infectious uveitis (NIU) comprises a heterogeneous group of diseases causing severe ocular inflammation that threatens vision. In addition to visual impairment, patients frequently endure chronic pain, functional disorders, and psychosocial stress, all of which substantially reduce quality of life. Treating NIU remains challenging because many patients respond inadequately to high-dose corticosteroids and various immunosuppressants. This systematic review evaluated the efficacy and safety of tocilizumab (TCZ) in NIU treatment by analyzing case reports and small-scale studies. A systematic search of PubMed, Web of Science, and Embase up to May 1, 2025, identified all published cases reporting baseline and follow-up visual acuity alongside intervention details. The Newcastle-Ottawa Scale (NOS) assessed methodological quality, while the Joanna Briggs Institute (JBI) tool evaluated risk of bias. The systematic review included 96 patients (36 males, 60 females) with an average age of 35 years (range 4– 72). Behçet’s disease (BD) represented the most common underlying condition (33 cases), and panuveitis was the primary anatomical subtype (35 cases). Prior to TCZ initiation, patients had received an average of 2.8 conventional immunosuppressants and 1.6 biologics, yet persistent disease activity remained. The median interval from diagnosis to TCZ treatment was 11.8 months (range 4– 24). Following TCZ administration, vision improved in 62.5% of patients, intraocular inflammation was controlled in 83.3%, and macular edema resolved in 90.9%. Overall, 83.3% (80/96) responded favorably to TCZ. These findings indicate that TCZ may serve as an effective alternative for managing refractory NIU when other treatments fail.
Keywords: non-infectious uveitis, uveitis, tocilizumab, TCZ, interleukin-6, IL-6
Introduction
Non-infectious uveitis (NIU) is an immune-mediated disorder characterized by persistent visual impairment, including visual field defects, blurred vision, and ocular pain, and stands as a leading cause of preventable blindness worldwide.1–3 NIU is classified into idiopathic cases without clear systemic associations and those related to systemic diseases. Juvenile idiopathic arthritis (JIA) represents the most common systemic cause of uveitis in children, with its associated uveitis (JIA-U) accounting for 20–30% of pediatric NIU cases, making it the second most prevalent subtype after idiopathic uveitis. Additional causes include sarcoidosis, Behçet’s disease (BD), and Vogt-Koyanagi-Harada disease (VKH), among others.4–6
Current expert consensus recommends initiating NIU treatment with systemic or local corticosteroids.4,7,8 However, prolonged corticosteroid use carries significant risks such as cataracts, glaucoma, and osteoporosis, restricting long-term application.9–11 When inflammation remains uncontrolled by steroids, immunosuppressive agents like methotrexate and cyclosporine serve as second-line therapies.12,13 Despite these options, many patients exhibit inadequate responses or intolerance to conventional immunomodulatory treatments, resulting in persistent refractory disease. In such cases, biologics targeting tumor necrosis factor-alpha (TNF-α), including adalimumab (ADA) and infliximab (IFX), become therapeutic choices for refractory NIU.14–16
Nevertheless, the efficacy of TNF-α inhibitors remains suboptimal, with adverse events occurring relatively frequently.17,18 IFX demonstrates lower tolerability due to a higher incidence of infusion-related reactions.8,18 Both ADA and IFX achieve efficacy rates between 60% and 70% in NIU.19–21 ADA’s most commonly reported adverse effects include infections and injection-site reactions, affecting approximately 10–20% of patients, while IFX-related adverse events, such as infusion reactions and infections, occur at similar rates of 10–20%.14,22–26 These limitations highlight the need to explore alternative therapies when conventional biologics fail.
Tocilizumab (TCZ), a recombinant humanized monoclonal antibody targeting the interleukin-6 receptor (IL-6R), exerts anti-inflammatory effects by inhibiting IL-6 binding.27–29 Approved by the FDA for moderate-to-severe rheumatoid arthritis (RA), systemic JIA (s-JIA), and polyarticular JIA, TCZ also treats other inflammatory disorders such as giant cell arteritis (GCA), systemic sclerosis-associated interstitial lung disease (SSc-ILD), cytokine release syndrome (CRS), and severe COVID-19.30–33
Emerging evidence suggests that TCZ may offer a promising alternative for patients with NIU unresponsive to traditional immunosuppressants or biologics.34–40 However, a comprehensive systematic review assessing its efficacy and safety remains lacking. This systematic review follows PRISMA 2020 guidelines to quantitatively synthesize published data, evaluate TCZ’s therapeutic profile in NIU, and clarify its role and future prospects within existing treatment paradigms.
Methods
Search Strategy
The systematic review rigorously follows PRISMA 2020 guidelines and has been registered with PROSPERO under registration number CRD420251106755, ensuring transparency and methodological rigor. A comprehensive search of PubMed, Web of Science, and Embase was performed to identify case reports and case series on TCZ use in NIU published up to May 1, 2025, without language restrictions. The search strategy combined subject headings and free-text terms using Boolean operators. For example, the PubMed query included: ((“Uveitis”[Mesh] OR Uveitis OR “non-infectious uveitis”) AND ((“Interleukin-6” OR “Interleukin 6” OR IL-6 OR “B Cell Stimulatory Factor-2” OR BSF-2 OR “Hepatocyte-Stimulating Factor” OR “Interferon beta-2” OR IL6) OR (TCZ OR tocilizumab OR “monoclonal antibody, MRA” OR atlizumab OR Actemra OR Roactemra OR RHPM-1 OR RG-1569 OR RO-4877533 OR R-1569 OR MSB11456 OR MSB-11456 OR BAT-1806 OR BAT1806))) AND (“1900/01/01”[Date - Entry]: “2025/05/01”[Date - Entry])). Additionally, reference lists from pertinent articles underwent manual screening to identify further eligible studies. Initial literature screening and data extraction were conducted by H.C. and K.B, with subsequent review and verification by X.M. to ensure accuracy and methodological integrity. The study selection process is detailed in Figure 1.
 |
Figure 1 PRISMA flowchart for the systematic review. |
Inclusion Criteria
Inclusion criteria were as follows: (1) patients with a confirmed NIU diagnosis according to the Standardization of Uveitis Nomenclature (SUN) criteria, encompassing anterior, intermediate, posterior, or panuveitis;41 (2) treatment with TCZ via any administration route (intravenous or subcutaneous) at any dose; (3) case reports or series providing comprehensive patient-level data, including baseline demographics, etiology, anatomical classification, best-corrected visual acuity (BCVA) before and after treatment, inflammatory activity, central foveal thickness (CFT) changes, and prior immunosuppressive or biologic therapy; (4) Newcastle-Ottawa Scale (NOS) scores ≥4, reflecting moderate to high methodological quality. H.C. and K.B. performed the initial assessment, followed by X.M.’s review and validation to ensure completeness and accuracy.
Exclusion Criteria
Exclusion criteria were as follows: (1) duplicate publications, articles lacking original data, conference abstracts, reviews, animal studies, and studies with NOS scores below 4, indicating low quality; (2) studies reporting only aggregate data without extractable patient-level efficacy or safety outcomes; (3) studies including individuals younger than 2 years or older than 80 years without separate data for pediatric or geriatric subgroups; (4) studies failing to clearly report TCZ dosage, administration intervals, or treatment duration, or mixing multiple dosing regimens without stratified analyses; (5) studies primarily assessing inflammation outside the eyes (eg, joints, skin, intestines) where NIU-specific data could not be isolated; and (6) studies focusing predominantly on pharmacoeconomics, cost-effectiveness, quality of life measures, or patient-reported outcomes (PROs) without objective clinical indicators.
Data Collection
A standardized data extraction form captured patient characteristics and efficacy and safety outcomes. Extracted variables included age, sex, anatomical uveitis classification, laterality (unilateral or bilateral), baseline and follow-up BCVA, ocular complications, prior immunosuppressant and biologic use, and interval from symptom onset to TCZ initiation (in weeks). Details of the TCZ regimen—dosage and frequency—and treatment-emergent adverse events were documented. Imaging data included changes in CFT measured by optical coherence tomography (OCT) before and after TCZ therapy. Macular edema was defined as baseline CFT > 350 μm, with resolution marked by post-treatment CFT < 300 μm. Visual acuity changes were classified as “improved” if follow-up BCVA exceeded baseline or “deteriorated” if worse. This comprehensive dataset enabled thorough assessment of TCZ’s clinical efficacy and safety in NIU.42
Quality Assessment and Risk of Bias
The Joanna Briggs Institute (JBI) critical appraisal tools were applied according to study type—case reports, cohort studies, and case series—to evaluate risk of bias. N.Z. and C.M. independently completed assessments for each article and answered all JBI checklist items. Discrepancies were resolved through consultation, followed by review and verification by X.M. Studies with only one “No” response on the JBI checklist were classified as having low risk of bias. After the evaluation by JBI, we considered all the literature as “low risk of bias”.
Response Criteria
Efficacy was evaluated using a composite endpoint widely adopted in international uveitis research.41,42 TCZ treatment qualified as effective if any of the following criteria were met: (a) a reduction of at least two grades in anterior chamber or vitreous inflammatory cell count from baseline, or reduction to grade 0, based on SUN criteria; (b) a decrease in systemic prednisone dosage to ≤10 mg/day (or equivalent corticosteroid) while maintaining uveitis control; (c) resolution of macular edema, defined as OCT-measured CFT <300 μm, with sustained uveitis control; or (d) overall clinical improvement as assessed by the original study authors. The primary outcome focused on reducing ocular inflammation, while relapse was defined as recurrence of active inflammation after remission.
Statistical Analysis
All extracted data underwent analysis using SPSS version 26.0. Categorical variables were summarized as frequencies and percentages, whereas continuous variables were expressed as mean ± standard deviation or median (range), contingent on data distribution. Chi-square tests examined associations between categorical variables—such as etiology, uveitis type, and TCZ regimen—and treatment response (effective vs ineffective). This test evaluates whether observed frequencies significantly deviate from expected values across categories, applying a significance threshold of p < 0.05.
Logistic regression analysis assessed the influence of categorical predictors on the likelihood of treatment success. Independent variables included etiology, uveitis type, and TCZ regimen, with treatment response as the binary dependent variable. Model fit was evaluated using McFadden’s R2, and odds ratios (OR) with 95% confidence intervals (CI) quantified the strength of associations.
Results
Baseline Characteristics of TCZ-Treated Patients
The literature search identified 5985 potentially relevant articles. Applying inclusion and exclusion criteria narrowed this to 22 studies (case reports or case series) included in the analysis. Due to incomplete individual-level data in some reports, detailed clinical information from 96 patients was extracted for this systematic review, summarized in Table 1. The patients’ mean age was approximately 35 years (range 4–72), with 62.5% (60/96) female. According to the SUN classification, panuveitis represented the most prevalent subtype (35%, 34/96), followed by anterior uveitis (17%, 16/96), intermediate uveitis (7%, 7/96), and posterior uveitis (4%, 4/96). Some studies did not specify anatomical classification. The most common underlying diseases included JIA, BD, and RA, as detailed in Table 2.
 |
Table 1 Baseline Characteristics and Prior Therapies of Patients with NIU |
 |
Table 2 The Clinical Course of NIU Patients Receiving TCZ Treatment |
Prior Treatments Before TCZ Initiation
Before TCZ initiation, patients had undergone multiple treatments. Intravitreal corticosteroid injections were administered to 72.9% (70/96) of patients (Table 1). Systemic conventional immunosuppressants were widely used: methotrexate in 65.6% (63/96) and cyclosporine A in 50% (48/96). Biologic therapies were also frequent, with ADA used in 76% (73/96). TCZ was introduced after high-dose corticosteroids, conventional immunosuppressants, or other biologics failed to control progressive intraocular inflammation adequately.
Statistical Analysis Results
Chi-square tests revealed no significant associations between etiology, uveitis type, or TCZ regimen and treatment response (p > 0.05), as summarized in Table 3.
 |
Table 3 Chi-Square Test Results |
Logistic regression analysis (Table 4) confirmed that none of these variables significantly influenced the likelihood of a favorable response to TCZ (all p > 0.05). The McFadden R2 of 0.134 indicates that these factors explain only a modest proportion of variability in treatment outcomes.
 |
Table 4 Logistic Regression Analysis Results |
TCZ Efficacy and Macular Edema Response
TCZ demonstrated a high overall efficacy rate of 83.3% (80/96), as shown in Table 2. Subgroup analysis by etiology revealed the following response rates: Birdshot chorioretinopathy (BSCR), 19 cases (19.8%, 19/96), with all patients achieving clinical efficacy (100%, 19/19); JIA-associated uveitis, 14 cases (14.6%, 14/96), with 10 patients responding to treatment (71.4%, 10/14); BD-associated uveitis, 33 cases (34.3%, 33/96), with 26 effective responses (78.8%, 26/33); RA-associated uveitis, 4 cases (4.2%, 4/96), with 3 patients responding (75%, 3/4); idiopathic panuveitis (IPU), 12 cases (12.5%, 12/96), with 10 effective responses (83.3%, 10/12); refractory idiopathic uveitis (RIU), 7 cases (7.3%, 7/96), with 5 patients responding (71.4%, 5/7); multicentric Castleman disease (MCD), 1 case (1%, 1/96), with efficacy observed in the single case (100%, 1/1); Cogan syndrome with aortitis, 1 case (1%, 1/96), with complete response (100%, 1/1); multiple sclerosis (MS), 1 case (1%, 1/96), with full efficacy (100%, 1/1); psoriatic arthritis (PA), 2 cases (2%, 2/96), both achieving response (100%, 2/2); autoimmune uveitis (AU), 1 case (1%, 1/96), effective (100%, 1/1); and ankylosing spondylitis (AS), 1 case (1%, 1/96), also effective (100%, 1/1). Among all patients, 83.3% (80/96) met clinical efficacy criteria, characterized by significant reduction in intraocular inflammation along with either stabilized or improved visual acuity. Specifically, visual acuity improved in 60 patients (62.5%), remained stable in 6 (6.3%), and declined in 20 (20.8%) following treatment. In the subset of 22 patients with quantifiable macular edema evaluated by OCT, TCZ achieved a resolution rate of 90.9% (20/22), evidenced by normalization of CFT. Only 2 patients (9.1%) exhibited persistent refractory macular edema, indicating high efficacy of TCZ in macular edema management within this cohort.
TCZ Failures, Adverse Events, and Etiology-Specific Outcomes
Although most patients responded favorably to TCZ, 16 cases (16.7%, 16/96) were classified as treatment failures (Table 5). A systematic literature review identified common characteristics among these non-responders: (a) initiation of TCZ during late-stage disease with irreversible ocular damage—such as retinal detachment or refractory macular fibrosis—where inflammation control failed to restore function; (b) treatment discontinuation due to severe adverse events, including infusion-related reactions, serious infections, or laboratory abnormalities like marked neutropenia, which compromised sustained inflammation control; (c) development of severe ocular complications during TCZ therapy, such as cataract progression or retinal detachment, negatively impacting efficacy evaluation; and (d) suboptimal treatment regimens involving inadequate dosing or premature discontinuation, indicating insufficient treatment intensity or exposure contributed to failure.
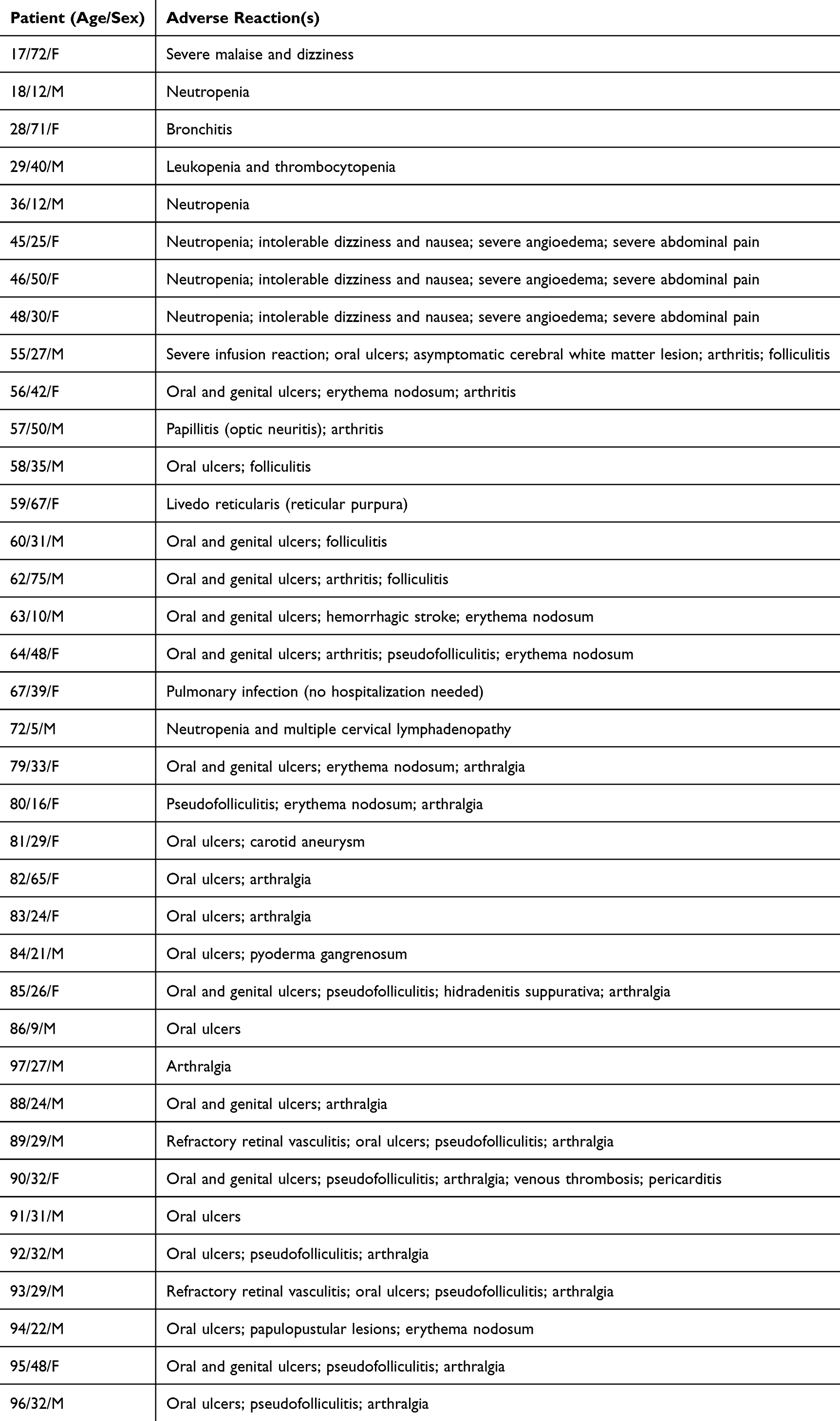 |
Table 5 Adverse Reactions During TCZ Therapy |
Most patients exhibited improvement in inflammatory markers alongside successful corticosteroid tapering. Mean visual acuity also improved post-treatment. Adverse events of varying severity occurred in approximately 34 patients (35%) (Table 5), with the most common being infusion reactions, elevated liver enzymes, and increased infection risk. The majority of adverse events proved manageable through monitoring and appropriate interventions. Nevertheless, a few patients discontinued TCZ due to serious adverse events, including one case of a severe anaphylactic infusion reaction.
Discussion
This systematic review of current literature demonstrates that TCZ achieves a high clinical remission rate in NIU, with an efficacy of 83.3% (80/96), significantly improving both inflammation control and visual function.2,60,61 These findings align with recent studies; for example, Uludag et al observed seven cases of refractory uveitis and reported that intravenous TCZ administration led to a substantial reduction in central retinal thickness and improved fluorescein angiography scores, accompanied by minimal severe adverse events, thus supporting TCZ’s efficacy and safety.62 Similarly, a multicenter study involving 11 patients with BD-associated uveitis documented rapid improvement in all ocular inflammation markers following TCZ initiation, with eight patients achieving complete remission.59 These independent studies further validate the high remission rate observed in this systematic review. However, the response to TCZ treatment may vary among different patient populations. In the Phase II APTITUDE trial for JIA-associated uveitis, the primary endpoint response rate was approximately 34%, falling short of expectations.63 Nonetheless, the trial highlighted that some patients unresponsive to conventional immunosuppressants and anti-TNF therapies experienced inflammation control after switching to TCZ.6,25 Currently, no direct comparative studies exist between TNF inhibitors and TCZ in the context of NIU, and a large proportion of patients transition to TCZ after failure of corticosteroids or TNF inhibitors. Therefore, direct comparisons of efficacy between TCZ and corticosteroids or TNF inhibitors are not yet possible. Overall, these findings reinforce TCZ’s role as a valuable rescue therapy in NIU and emphasize the necessity for further research to better define its efficacy within specific patient subgroups.
Mechanistically, IL-6 involvement in uveitis pathogenesis offers a compelling rationale for TCZ’s effectiveness.6 NIU is characterized by an imbalance between pro-inflammatory Th17 cells and anti-inflammatory regulatory T (Treg) cells.64–66 IL-6 serves as a pivotal cytokine driving differentiation of naïve CD4+ T cells into the Th17 lineage, particularly in the presence of transforming growth factor-β.2,67,68 Numerous studies confirm hyperactivation of IL-6-mediated signaling in autoimmune ocular inflammation, closely correlating with disease activity.69–72 Experimental uveitis models demonstrate that IL-6 knockout or anti-IL-6 monoclonal antibody treatment significantly suppresses retinal inflammation.73–77 By blocking IL-6R interaction, TCZ disrupts the inflammatory feedback loop and mitigates immune-mediated ocular damage, forming the basis of its mechanism of action.73 As an IL-6R antagonist, TCZ binds both soluble and membrane-bound IL-6R, inhibiting downstream IL-6/IL-6R/gp130 complex signaling, thereby reducing pro-inflammatory cytokine production and recruitment of inflammatory cells, including neutrophils.78 Some reports suggest that TCZ not only suppresses pathogenic Th17 responses but also helps restore the Th1/Th17 balance, enhancing immune regulation within the retinal microenvironment—an effect critical for controlling refractory ocular inflammation.71,73,79 Collectively, these findings underscore TCZ’s considerable therapeutic potential for managing NIU.
A key finding of this study is that early initiation of TCZ may enhance therapeutic outcomes.80 Patients receiving TCZ early in the disease course generally experienced better recovery, whereas delayed treatment proved less effective at reversing irreversible visual loss. This suggests that for NIU refractory to conventional therapies, introducing biologics with novel mechanisms early—rather than repeatedly using agents within the same class—may better prevent cumulative tissue damage.42 This approach is especially critical for severe, vision-threatening cases, such as refractory Behçet’s uveitis, where early TCZ intervention may reduce the risk of recurrent retinal injury from relapses. However, the precise definition of “early” treatment remains ambiguous; it likely refers to initiation within months of NIU diagnosis and treatment failure, rather than years later when irreversible ocular damage has occurred. Clinical practice should emphasize personalized TCZ strategies, including decisions on combination with conventional immunosuppressants, administration route (intravenous versus subcutaneous), and dosage adjustments.27,81 Comparative studies indicate some refractory cases respond better to intravenous TCZ, highlighting the need to tailor treatment to patient response.82
The safety profile of TCZ in NIU aligns with its established use in rheumatologic conditions.83–90 Common adverse events include infusion reactions, infections—particularly opportunistic infections—neutropenia, elevated liver enzymes, and hyperlipidemia.48,91–93 Approximately 10% of patients in this systematic review discontinued TCZ due to adverse events.46 Although the adverse event rate is relatively high, it highlights the necessity of proactive monitoring and timely intervention to mitigate risks. Regular assessment of inflammatory and immune markers improves treatment safety.94,95 Recommended monitoring includes periodic complete blood counts with emphasis on neutrophil levels; surveillance of C-reactive protein (CRP) to evaluate inflammation and treatment response; and serum IL-6 measurement in patients with systemic involvement for additional insights.78 Upon detecting significant neutropenia or hepatic abnormalities, dose reduction or treatment interruption should be considered alongside infection prophylaxis and management of complications.96–101 Intravenous infusions require medical supervision and slow infusion rates to minimize infusion reaction risks. In summary, comprehensive follow-up protocols and multidisciplinary collaboration—especially between rheumatology and ophthalmology—are essential to minimize TCZ-associated risks.94
This systematic review primarily relies on retrospective case reports and series, which inherently provide a lower level of evidence. The small sample sizes and lack of standardized controls introduce potential selection bias, as successful treatment cases are more likely to be published than failures, potentially leading to an overestimation of efficacy. Additionally, variability in follow-up durations across studies limits the ability to assess long-term efficacy and relapse rates adequately. Therefore, the reported 83.3% remission rate should be interpreted as a synthesis of current data pending confirmation by prospective randomized controlled trials. Logistic regression analysis further revealed that examined variables—etiology, uveitis type, and TCZ regimen—did not significantly influence the likelihood of a favorable TCZ response (p > 0.05). The McFadden R2 value of 0.134 indicates these factors explain only a modest portion of outcome variability, suggesting other unmeasured factors affect TCZ efficacy in NIU. The retrospective design and limited sample size constrain the generalizability of these findings.
Future research should focus on evaluating TCZ efficacy within specific NIU subtypes, such as pediatric versus adult populations and NIU associated with systemic diseases, to better identify optimal candidates. Further studies are warranted to optimize treatment strategies, including combination therapies with other targeted agents, sequential or induction-maintenance regimens, and biomarker-guided personalized dosing. Large-scale, long-term cohort studies are essential to fully characterize TCZ’s safety profile, especially regarding rare but severe adverse events. Beyond TCZ, investigations into novel IL-6/IL-6R inhibitors (eg, sarilumab) and modulators of related pathways (eg, JAK inhibitors) offer promising therapeutic alternatives for uveitis. These avenues will advance biologic treatment strategies for NIU, enhancing precision and efficacy.
Conclusion
The key conclusions of this systematic review are as follows: (1) TCZ, as an IL-6 receptor antagonist, shows promise as a safe and effective treatment option for NIU; (2) early initiation of TCZ after NIU diagnosis, alongside dynamic monitoring of neutrophil counts, CRP, and IL-6 levels, may enhance clinical outcomes, reduce relapse risk, and minimize adverse events; (3) further prospective, multicenter clinical trials are essential to establish optimal timing, dosing, and maintenance strategies for TCZ in NIU, thereby enabling evidence-based personalized therapy.
Acknowledgments
Haixing Cao and Kaiyu Bian are co-first authors for this study. We thank Bullet Edits Limited for the linguistic editing and proofreading of the manuscript.
Funding
This research was funded by financial support from the National Natural Science Foundation of China, awarded to Xiang Ma, under grant number 81271022.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zamani R, Tahghighi Sharabian F, Zamani Khorasgani A, Zarei M, Ziaee V. Patterns and outcomes of childhood non-infectious uveitis: a retrospective cohort and review of literature. Ocul Immunol Inflamm. 2025;1–9. doi:10.1080/09273948.2025.2522297
2. Yu X, Duan R, Jiang L, et al. Interleukin-6 in non-infectious uveitis: biology, experimentalevidence and treatment strategies. Biochem Pharmacol. 2024;230(Pt 2):116605. doi:10.1016/j.bcp.2024.116605
3. Rosenbaum JT, Bodaghi B, Couto C, et al. New observations and emerging ideas in diagnosis and management of non-infectious uveitis: a review. Semin Arthritis Rheum. 2019;49(3):438–445. doi:10.1016/j.semarthrit.2019.06.004
4. Touhami S, Diwo E, Sève P, et al. Expert opinion on the use of biological therapy in non-infectious uveitis. Expert Opin Biol Ther. 2019;19(5):477–490. doi:10.1080/14712598.2019.1595578
5. Rosenbaum JT, Dick AD. The eyes have it: a rheumatologist’s view of uveitis. Arthritis Rheumatol. 2018;70(10):1533–1543. doi:10.1002/art.40568
6. Wu X, Tao M, Zhu L, Zhang T, Zhang M. Pathogenesis and current therapies for non-infectious uveitis. Clin Exp Med. 2023;23(4):1089–1106. doi:10.1007/s10238-022-00954-6
7. Younus R, Saeed MA, Arshad M, Farman S, Ahmad NM. Noninfectious uveitis in rheumatology: patterns, treatment, and outcomes. Cureus. 2023;15(6):e39965. doi:10.7759/cureus.39965
8. Espinosa G, Herreras JM, Muñoz-Fernández S, García Ruiz de Morales JM, Cordero-Coma M. Documento de recomendaciones sobre el tratamiento con inmunodepresores de la uveítis no anterior, no infecciosa, no neoplásica [Recommendations statement on the immunosuppressive treatment of non-infectious, non-neoplastic, non-anterior uveitis]. Med Clin. 2020;155(5):220.e1–220.e12. doi:10.1016/j.medcli.2019.10.023
9. Thiele K, Buttgereit F, Huscher D, Zink A. Current use of glucocorticoids in patients with rheumatoid arthritis in Germany. Arthritis Rheum. 2005;53(5):740–747. doi:10.1002/art.21467
10. Goupillou P, Leclercq M, Zourdani L, Muraine M, Fortenfant F, Gueudry J. Correlation Between Optical Coherence Tomography (OCT) and Serum Indirect Immunofluorescence Findings in a Case of Cancer Associated Retinopathy (CAR) Masquerading as White Dot Syndrome. Ocul Immunol Inflamm. 2025;1–5. doi:10.1080/09273948.2025.2542278
11. Muselier A, Bielefeld P, Bidot S, Vinit J, Besancenot JF, Bron A. Efficacy of tocilizumab in two patients with anti-TNF-alpha refractory uveitis. Ocul Immunol Inflamm. 2011;19(5):382–383. doi:10.3109/09273948.2011.606593
12. Kempen JH, Daniel E, Gangaputra S, et al. Methods for identifying long-term adverse effects of treatment in patients with eye diseases: the systemic immunosuppressive therapy for eye diseases (SITE) cohort study. Ophthalmic Epidemiol. 2008;15(1):47–55. doi:10.1080/09286580701585892
13. Valenzuela RA, Flores I, Urrutia B, et al. New pharmacological strategies for the treatment of non-infectious uveitis. A Minireview. Front Pharmacol. 2020;11:655. doi:10.3389/fphar.2020.00655
14. Liu W, Bai D, Kou L. Comparison of infliximab with Adalimumab for the treatment of non-infectious uveitis: a systematic review and meta-analysis. BMC Ophthalmol. 2023;23(1):240. doi:10.1186/s12886-023-02987-1
15. Busto-Iglesias M, Rodríguez-Martínez L, Rodríguez-Fernández CA, et al. Perspectives of therapeutic drug monitoring of biological agents in non-infectious uveitis treatment: a review. Pharmaceutics. 2023;15(3). doi:10.3390/pharmaceutics15030766
16. Sözeri B, Kardeş E, Salı E, Çakır D, Demir F. Drug survival of the infliximab biosimilar (CT-P13) in paediatric patients with non-infectious uveitis. Clin Exp Rheumatol. 2021;39(4):907–912. doi:10.55563/clinexprheumatol/r4gnxm
17. Bernal-Morales C, Ramanan AV, Pavesio C. Use of immunomodulators in non-infectious uveitis: lights and shadows. Eye. 2024;38(17):3231–3242. doi:10.1038/s41433-024-03294-9
18. Borrás-Blasco J, Casterá DE, Cortes X, Abad FJ, Rosique-Robles JD, Mallench LG. Effectiveness of infliximab, Adalimumab and golimumab for non-infectious refractory uveitis in adults. Int J Clin Pharmacol Ther. 2015;53(5):377–390. doi:10.5414/cp202171
19. Çam F, Celiker H. Efficacy, retention rate and safety of Adalimumab treatment in patients with non-infectious uveitis and scleritis: a real-world, retrospective, single-centre study. Eye. 2024;38(5):893–901. doi:10.1038/s41433-023-02800-9
20. Bellur S, McHarg M, Kongwattananon W, Vitale S, Sen HN, Kodati S. Antidrug antibodies to tumor necrosis factor α inhibitors in patients with noninfectious uveitis. JAMA Ophthalmol. 2023;141(2):150–156. doi:10.1001/jamaophthalmol.2022.5584
21. Felfeli T, Balas M, Tai F, et al. Long-term outcomes of noninfectious uveitis treated with systemic immunomodulatory therapy: a retrospective case series. Can J Ophthalmol. 2025;60(1):e133–e143. doi:10.1016/j.jcjo.2024.05.005
22. Authors HD, Mierzwinski-Urban M, Spry C. CADTH Health Technology Review. Adalimumab for the Treatment of Pediatric Populations With Non-Infectious Uveitis: CADTH Health Technology Review. Canadian Agency for Drugs and Technologies in Health.; 2022.
23. Tao T, Yang S, He D, et al. The efficacy of adalimumab in children with chronic non-infectious posterior uveitis and panuveitis: a retrospective cohort study. Ophthalmol Ther. 2024;13(5):1239–1253. doi:10.1007/s40123-024-00884-4
24. Ogata A, Tanimura K, Sugimoto T, et al. Phase III study of the efficacy and safety of subcutaneous versus intravenous tocilizumab monotherapy in patients with rheumatoid arthritis. Arthritis Care Res. 2014;66(3):344–354. doi:10.1002/acr.22110
25. Scheinfeld N. Adalimumab: a review of side effects. Expert Opin Drug Saf. 2005;4(4):637–641. doi:10.1517/14740338.4.4.637
26. Kunimi K, Usui Y, Asakage M, et al. Anti-TNF-α therapy for refractory uveitis associated with behçet’s syndrome and sarcoidosis: a single center study of 131 patients. Ocul Immunol Inflamm. 2022;30(1):223–230. doi:10.1080/09273948.2020.1791346
27. Sheppard M, Laskou F, Stapleton PP, Hadavi S, Dasgupta B. Tocilizumab (Actemra). Hum Vaccin Immunother. 2017;13(9):1972–1988. doi:10.1080/21645515.2017.1316909
28. Trivedi A, Katelaris C. The use of biologic agents in the management of uveitis. Intern Med J. 2019;49(11):1352–1363. doi:10.1111/imj.14215
29. Sadiq MA, Hassan M, Afridi R, et al. Posterior segment inflammatory outcomes assessed using fluorescein angiography in the STOP-UVEITIS study. Int J Retina Vitreous. 2020;6:47. doi:10.1186/s40942-020-00245-w
30. Sato T, Minakuchi S, Mochizuki M, Takeuchi M. Acute anterior uveitis after discontinuation of tocilizumab in a patient with rheumatoid arthritis. Clin Ophthalmol. 2014;8:187–190. doi:10.2147/opth.S54929
31. Leclercq M, Desbois AC, Domont F, et al. Biotherapies in Uveitis. J Clin Med. 2020;9(11). doi:10.3390/jcm9113599
32. Rubbert-Roth A, Furst DE, Nebesky JM, Jin A, Berber E. A review of recent advances using tocilizumab in the treatment of rheumatic diseases. Rheumatol Ther. 2018;5(1):21–42. doi:10.1007/s40744-018-0102-x
33. Salo JLM, Marcelo LJN, Sanchez ACA, et al. Effectiveness of tocilizumab in COVID-19 patients with pneumonia: a systematic review. Acta Med Philipp. 2025;59(2):72–80. doi:10.47895/amp.vi0.8188
34. Hammami R, Nobari H, Hanen W, et al. Exploring of two different equated instability resistance training programs on measure of physical fitness and lower limb asymmetry in pre-pubertal weightlifters. BMC Sports Sci Med Rehabil. 2023;15(1):40. doi:10.1186/s13102-023-00652-0
35. Suzuki K, Akiyama M, Saito K, Shimanuki K, Kaneko Y. Efficacy of tocilizumab monotherapy for autoimmune hemolytic anemia associated with idiopathic multicentric Castleman disease: a case-based review. Rheumatol Int. 2025;45(5):113. doi:10.1007/s00296-025-05880-w
36. Han T, Song P, Wu Z, et al. Inflammatory stimulation of astrocytes affects the expression of miRNA-22-3p within NSCs-EVs regulating remyelination by targeting KDM3A. Stem Cell Res Ther. 2023;14(1):52. doi:10.1186/s13287-023-03284-w
37. Raad M, Suresh KV, Puvanesarajah V, Forsberg J, Morris C, Levin A. The pathologic fracture mortality index: a novel externally validated tool for predicting 30-day postoperative mortality. J Am Acad Orthop Surg. 2021;29(23):e1264–e1273. doi:10.5435/jaaos-d-20-01309
38. Parisi S, Ditto MC, Ghellere F, et al. Update on tocilizumab in rheumatoid arthritis: a narrative review. Front Immunol. 2025;16:1470488. doi:10.3389/fimmu.2025.1470488
39. Zur bonsen LS, Schulze D, Künzel SE, Rübsam A, Pleyer U, Pohlmann D. Long-term effects of tocilizumab on retinal and choroidal inflammation in Birdshot uveitis. J Ophthalmic Inflamm Infect. 2024;14(1):61. doi:10.1186/s12348-024-00443-9
40. Sepah YJ, Sadiq MA, Chu DS, et al. Primary (Month-6) outcomes of the STOP-uveitis study: evaluating the safety, tolerability, and efficacy of tocilizumab in patients with noninfectious uveitis. Am J Ophthalmol. 2017;183:71–80. doi:10.1016/j.ajo.2017.08.019
41. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of uveitis nomenclature for reporting clinical data. Results of the first international workshop. Am J Ophthalmol. 2005;140(3):509–516. doi:10.1016/j.ajo.2005.03.057
42. Mesquida M, Molins B, Llorenç V, Sainz de la Maza M, Adán A. Long-term effects of tocilizumab therapy for refractory uveitis-related macular edema. Ophthalmology. 2014;121(12):2380–2386. doi:10.1016/j.ophtha.2014.06.050
43. Oshitari T, Kajita F, Tobe A, et al. Refractory uveitis in patient with castleman disease successfully treated with tocilizumab. Case Rep Ophthalmol Med. 2012;2012:968180. doi:10.1155/2012/968180
44. Shibuya M, Fujio K, Morita K, Harada H, Kanda H, Yamamoto K. Successful treatment with tocilizumab in a case of Cogan’s syndrome complicated with aortitis. Mod Rheumatol. 2013;23(3):577–581. doi:10.1007/s10165-012-0691-0
45. Tappeiner C, Heinz C, Ganser G, Heiligenhaus A. Is tocilizumab an effective option for treatment of refractory uveitis associated with juvenile idiopathic arthritis? J Rheumatol. 2012;39(6):1294–1295. doi:10.3899/jrheum.120010
46. Adán A, Mesquida M, Llorenç V, Modesto C. Tocilizumab for retinal vasoproliferative tumor secondary to juvenile idiopathic arthritis-associated uveitis: a case report. Graefes Arch Clin Exp Ophthalmol. 2014;252(1):163–164. doi:10.1007/s00417-013-2466-5
47. Adán A, Mesquida M, Llorenç V, et al. Tocilizumab treatment for refractory uveitis-related cystoid macular edema. Graefes Arch Clin Exp Ophthalmol. 2013;251(11):2627–2632. doi:10.1007/s00417-013-2436-y
48. Tsang AC, Roth J, Gottlieb C. Tocilizumab for severe chronic anterior uveitis associated with juvenile idiopathic arthritis in a pediatric patient. Ocul Immunol Inflamm. 2014;22(2):155–157. doi:10.3109/09273948.2013.866254
49. Calvo-Río V, de la Hera D, Beltrán-Catalán E, et al. Tocilizumab in uveitis refractory to other biologic drugs: a study of 3 cases and a literature review. Clin Exp Rheumatol. 2014;32(4 Suppl 84):S54–7.
50. Burlo F, Tumminelli C, Pastore S, et al. Subcutaneous tocilizumab in the management of non-infectious uveitis in children: a brief report. Pediatr Rheumatol Online J. 2023;21(1):99. doi:10.1186/s12969-023-00883-y
51. Silpa-Archa S, Oray M, Preble JM, Foster CS. Outcome of tocilizumab treatment in refractory ocular inflammatory diseases. Acta Ophthalmol. 2016;94(6):e400–6. doi:10.1111/aos.13015
52. Kearsley-Fleet L, Davies R, Baildam E, et al. Factors associated with choice of biologic among children with Juvenile Idiopathic Arthritis: results from two UK paediatric biologic registers. Rheumatology. 2016;55(9):1556–1565. doi:10.1093/rheumatology/kev429
53. Atienza-Mateo B, Calvo-Río V, Beltrán E, et al. Anti-interleukin 6 receptor tocilizumab in refractory uveitis associated with Behçet’s disease: multicentre retrospective study. Rheumatology. 2018;57(5):856–864. doi:10.1093/rheumatology/kex480
54. Leclercq M, Le Besnerais M, Langlois V, et al. Tocilizumab for the treatment of birdshot uveitis that failed interferon alpha and anti-tumor necrosis factor-alpha therapy: two cases report and literature review. Clin Rheumatol. 2018;37(3):849–853. doi:10.1007/s10067-018-4007-4
55. Babu K, Sudheer B, Rao AP. Intravenous tocilizumab in idiopathic pediatric uveitis with refractory cystoid macular edema - A case report. Indian J Ophthalmol. 2019;67(6):975–977. doi:10.4103/ijo.IJO_1938_18
56. Gil W, Lagrib H, Olagne L, et al. Multiple sclerosis-associated uveitis: a case report of refractory bilateral chronic granulomatous panuveitis successfully treated with tocilizumab. Ocul Immunol Inflamm. 2024;32(9):2264–2267. doi:10.1080/09273948.2024.2332783
57. Adán A, Moll-Udina A, Ramirez J, Llorenç V. Subcutaneous tocilizumab for cystoid macular edema secondary to juvenile idiopathic arthritis (JIA)-associated uveitis: a case report. Ocul Immunol Inflamm. 2021;29(1):6–8. doi:10.1080/09273948.2019.1644350
58. Wennink RAW, Ayuso VK, de Vries LA, Vastert SJ, de Boer JH. Tocilizumab as an effective treatment option in children with refractory intermediate and panuveitis. Ocul Immunol Inflamm. 2021;29(1):21–25. doi:10.1080/09273948.2020.1712431
59. Khitri MY, Bartoli A, Maalouf G, et al. Tocilizumab in Behçet disease: a multicenter study of 30 patients. J Rheumatol. 2023;50(7):916–923. doi:10.3899/jrheum.221106
60. Onishi A, Tanaka M, Fujii T, et al. Comparative effectiveness of subcutaneous sarilumab 200 mg biweekly, subcutaneous Tocilizumab 162 mg biweekly, and intravenous Tocilizumab 8 mg/kg every 4 weeks in patients with rheumatoid arthritis: a prospective cohort study. Arthritis Res Ther. 2025;27(1):52. doi:10.1186/s13075-025-03514-x
61. Cao H, Ma X. Rituximab in the treatment of non-infectious uveitis: a review. J Inflamm Res. 2024;17:6765–6780. doi:10.2147/jir.S477708
62. Uludag G, Karaca I, Akhavanrezayat A, et al. Efficacy and safety of tocilizumab in the management of non-infectious uveitis failed with conventional immunomodulatory and Anti-TNFα therapies. Ocul Immunol Inflamm. 2024;32(6):891–897. doi:10.1080/09273948.2022.2126374
63. Ramanan AV, Dick AD, Guly C, et al. Tocilizumab in patients with anti-TNF refractory juvenile idiopathic arthritis-associated uveitis (APTITUDE): a multicentre, single-arm, Phase 2 trial. Lancet Rheumatol. 2020;2(3):e135–e141. doi:10.1016/s2665-9913(20)30008-4
64. Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. 2014;6(10):a016295. doi:10.1101/cshperspect.a016295
65. Yoshida H, Magi M, Tamai H, et al. Effects of interleukin-6 signal inhibition on Treg subpopulations and association of Tregs with clinical outcomes in rheumatoid arthritis. Rheumatology. 2024;63(9):2515–2524. doi:10.1093/rheumatology/keae196
66. Kikuchi J, Hashizume M, Kaneko Y, Yoshimoto K, Nishina N, Takeuchi T. Peripheral blood CD4(+)CD25(+)CD127(low) regulatory T cells are significantly increased by tocilizumab treatment in patients with rheumatoid arthritis: increase in regulatory T cells correlates with clinical response. Arthritis Res Ther. 2015;17(1):10. doi:10.1186/s13075-015-0526-4
67. Karkhur S, Hasanreisoglu M, Vigil E, et al. Interleukin-6 inhibition in the management of non-infectious uveitis and beyond. J Ophthalmic Inflamm Infect. 2019;9(1):17. doi:10.1186/s12348-019-0182-y
68. Lin P. Targeting interleukin-6 for noninfectious uveitis. Clin Ophthalmol. 2015;9:1697–1702. doi:10.2147/opth.S68595
69. Yoshimura T, Sonoda KH, Ohguro N, et al. Involvement of Th17 cells and the effect of anti-IL-6 therapy in autoimmune uveitis. Rheumatology. 2009;48(4):347–354. doi:10.1093/rheumatology/ken489
70. Su CG, Lichtenstein GR. Influence of immunogenicity on the long-term efficacy of infliximab in Crohn’s disease. Gastroenterology. 2003;125(5):1544–1546. doi:10.1016/j.gastro.2003.05.009
71. Targan SR, Hanauer SB, van Deventer SJ, et al. A short-term study of chimeric monoclonal antibody cA2 to tumor necrosis factor alpha for Crohn’s disease. Crohn’s Disease cA2 Study Group. N Engl J Med. 1997;337(15):1029–1035. doi:10.1056/nejm199710093371502
72. Tanaka T, Kishimoto T. Targeting interleukin-6: all the way to treat autoimmune and inflammatory diseases. Int J Biol Sci. 2012;8(9):1227–1236. doi:10.7150/ijbs.4666
73. Papo M, Bielefeld P, Vallet H, et al. Tocilizumab in severe and refractory non-infectious uveitis. Clin Exp Rheumatol. 2014;32(4 Suppl 84):S75–9.
74. Ghasemi H. Roles of IL-6 in ocular inflammation: a review. Ocul Immunol Inflamm. 2018;26(1):37–50. doi:10.1080/09273948.2016.1277247
75. Toppila M, Ranta-Aho S, Kaarniranta K, Hytti M, Kauppinen A. Metformin alleviates inflammation and induces mitophagy in human retinal pigment epithelium cells suffering from mitochondrial damage. Cells. 2024;13(17). doi:10.3390/cells13171433
76. Chen TE, Lo J, Huang SP, et al. Glaucine inhibits hypoxia-induced angiogenesis and attenuates LPS-induced inflammation in human retinal pigment epithelial ARPE-19 cells. Eur J Pharmacol. 2024;981:176883. doi:10.1016/j.ejphar.2024.176883
77. Carriello MA, Costa DFB, Alvim PHP, et al. Retinal layers and symptoms and inflammation in schizophrenia. Eur Arch Psychiatry Clin Neurosci. 2024;274(5):1115–1124. doi:10.1007/s00406-023-01583-0
78. Schmitt C, Brockwell L, Giraudon M, et al. Intravenous tocilizumab for the treatment of giant cell arteritis: a phase Ib dose-ranging pharmacokinetic bridging study. Arthritis Res Ther. 2022;24(1):133. doi:10.1186/s13075-022-02815-9
79. Haruta H, Ohguro N, Fujimoto M, et al. Blockade of interleukin-6 signaling suppresses not only th17 but also interphotoreceptor retinoid binding protein-specific Th1 by promoting regulatory T cells in experimental autoimmune uveoretinitis. Invest Ophthalmol Vis Sci. 2011;52(6):3264–3271. doi:10.1167/iovs.10-6272
80. Saiki O, Uda H. Efficacy and safety of extending intravenous tocilizumab intervals from 4 to 6 weeks in rheumatoid arthritis patients with good response to 4-week intervals. Rheumatol Int. 2018;38(12):2307–2313. doi:10.1007/s00296-018-4149-3
81. Leclercq M, Goupillou P, Gomez H, et al. Efficacious switching from subcutaneous to intravenous tocilizumab in patients with non-infectious non-anterior uveitis. J Ophthalmic Inflamm Infect. 2023;13(1):32. doi:10.1186/s12348-023-00336-3
82. Saki A, Rajaei E, Rahim F. Safety and efficacy of tocilizumab for rheumatoid arthritis: a systematic review and meta-analysis of clinical trial studies. Reumatologia. 2021;59(3):169–179. doi:10.5114/reum.2021.107026
83. Jones G, Ding C. Tocilizumab: a review of its safety and efficacy in rheumatoid arthritis. Clin Med Insights Arthritis Musculoskelet Disord. 2010;3:81–89. doi:10.4137/cmamd.S4864
84. Alsuweiti MO, Alma’aitah HQ, Alnsour HM, et al. Biological agents’ adverse events in jordanian childhood rheumatic diseases: a single-center experience. Cureus. 2025;17(1):e78122. doi:10.7759/cureus.78122
85. Song SN, Yoshizaki K. Tocilizumab for treating rheumatoid arthritis: an evaluation of pharmacokinetics/pharmacodynamics and clinical efficacy. Expert Opin Drug Metab Toxicol. 2015;11(2):307–316. doi:10.1517/17425255.2015.992779
86. Ogata A, Morita T, Yoshida Y, Tanaka T. Subcutaneous formulation of tocilizumab for treatment of rheumatoid arthritis. Ther Deliv. 2015;6(3):283–295. doi:10.4155/tde.14.118
87. Ogata A, Kato Y, Higa S, Maeda K. Subcutaneous tocilizumab: recent advances for the treatment of rheumatoid arthritis. Expert Opin Drug Deliv. 2019;16(6):639–648. doi:10.1080/17425247.2019.1618828
88. Ogata A, Amano K, Dobashi H, et al. Longterm safety and efficacy of subcutaneous tocilizumab monotherapy: results from the 2-year open-label extension of the MUSASHI study. J Rheumatol. 2015;42(5):799–809. doi:10.3899/jrheum.140665
89. Mena-Vázquez N, Manrique-Arija S, Rojas-Giménez M, Ureña-Garnica I, Jiménez-Núñez FG, Fernández-Nebro A. Análisis de la efectividad, seguridad y optimización de tocilizumab en una cohorte de pacientes con artritis reumatoide en práctica clínica [Analysis of effectiveness, safety and optimization of tocilizumab in a cohort of patients with rheumatoid arthritis in clinical practice]. Reumatol Clin. 2019;15(1):21–26. doi:10.1016/j.reuma.2017.05.012
90. Isaacs JD, Salih A, Sheeran T, et al. Efficacy and safety of subcutaneous tocilizumab in rheumatoid arthritis over 1 year: a UK real-world, open-label study. Rheumatol Adv Pract. 2019;3(1):rkz010. doi:10.1093/rap/rkz010
91. Curtis JR, Perez-Gutthann S, Suissa S, et al. Tocilizumab in rheumatoid arthritis: a case study of safety evaluations of a large postmarketing data set from multiple data sources. Semin Arthritis Rheum. 2015;44(4):381–388. doi:10.1016/j.semarthrit.2014.07.006
92. Kessler EA, Vora SS, Verbsky JW. Risk of significant cytopenias after treatment with tocilizumab in systemic juvenile arthritis patients with a history of macrophage activation syndrome. Pediatr Rheumatol Online J. 2012;10(1):30. doi:10.1186/1546-0096-10-30
93. Nagase FN, Fukui S, Takizawa N, et al. Tocilizumab (TCZ) for giant cell arteritis: clinical outcomes following relapses and TCZ discontinuation due to adverse events. J Rheumatol. 2025;52(3):270–279. doi:10.3899/jrheum.2024-0612
94. Campbell L, Chen C, Bhagat SS, Parker RA, Östör AJ. Risk of adverse events including serious infections in rheumatoid arthritis patients treated with tocilizumab: a systematic literature review and meta-analysis of randomized controlled trials. Rheumatology. 2011;50(3):552–562. doi:10.1093/rheumatology/keq343
95. Yoo JR, Kim M, Kang MJ, Kim S, Lee KH, Heo ST. Tocilizumab for patients with severe fever with thrombocytopenia syndrome: tocilizumab observational SFTS study-1. Yonsei Med J. 2025;66(5):321–327. doi:10.3349/ymj.2024.0209
96. Sun X, Fang C, Jin S, et al. Serum IL-6 level trajectory for predicting the effectiveness and safety of tocilizumab in the treatment of refractory Takayasu arteritis. Eur J Intern Med. 2024;126:77–82. doi:10.1016/j.ejim.2024.04.004
97. Shimamoto K, Ito T, Ozaki Y, et al. Serum interleukin 6 before and after therapy with tocilizumab is a principal biomarker in patients with rheumatoid arthritis. J Rheumatol. 2013;40(7):1074–1081. doi:10.3899/jrheum.121389
98. Park MC, Chung SJ, Park YB, Lee SK. Relationship of serum TWEAK level to cytokine level, disease activity, and response to anti-TNF treatment in patients with rheumatoid arthritis. Scand J Rheumatol. 2008;37(3):173–178. doi:10.1080/03009740801898608
99. Aizu M, Mizushima I, Nakazaki S, et al. Changes in serum interleukin-6 levels as possible predictor of efficacy of tocilizumab treatment in rheumatoid arthritis. Mod Rheumatol. 2018;28(4):592–598. doi:10.1080/14397595.2017.1370766
100. Wang J, Devenport J, Low JM, Yu D, Hitraya E. Relationship between baseline and early changes in C-reactive protein and interleukin-6 levels and clinical response to tocilizumab in rheumatoid arthritis. Arthritis Care Res. 2016;68(6):882–885. doi:10.1002/acr.22765
101. Kojima T, Yabe Y, Kaneko A, et al. Monitoring C-reactive protein levels to predict favourable clinical outcomes from tocilizumab treatment in patients with rheumatoid arthritis. Mod Rheumatol. 2013;23(5):977–985. doi:10.1007/s10165-012-0782-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Safe Use of Corticosteroids in Non-Infectious Uveitis
Belletti M, Izquierdo-Escamez R, Tornero C, Olivas-Vergara O, Peiteado D, Carreño E
Journal of Inflammation Research 2025, 18:14441-14455
Published Date: 17 October 2025