Back to Journals » Journal of Pain Research » Volume 12
Sacral (S1) herpes zoster
Authors Chiriac A ![]() , Chiriac AE, Naznean A
, Chiriac AE, Naznean A ![]() , Moldovan C, Podoleanu C
, Moldovan C, Podoleanu C ![]() , Stolnicu S
, Stolnicu S ![]()
Received 21 December 2018
Accepted for publication 10 April 2019
Published 10 May 2019 Volume 2019:12 Pages 1475—1477
DOI https://doi.org/10.2147/JPR.S199124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Anca Chiriac,1–3 Anca E Chiriac,4 Adrian Naznean,5 Cosmin Moldovan,6 Cristian Podoleanu,7 Simona Stolnicu8
1The Department of Dermato-Physiology, Apollonia University, Iaşi, Romania; 2Department of Dermatology, Nicolina Medical Center, Iaşi, Romania; 3“P. Poni’’ Institute of Macromolecular Chemistry, Iaşi, Romania; 4Department of Epidemiology, University of Medicine and Pharmacy " Grigore T Popa", Iaşi, Romania; 5The Department of Foreign Languages, The University of Medicine and Pharmacy of Tîrgu Mureș, Tîrgu Mureș, , Romania; 6The Department of Applied Simulation in Medicine, The University of Medicine and Pharmacy of Tîrgu Mureș, Tîrgu Mureș, Romania; 7The Department of Cardiology, The University of Medicine and Pharmacy of Tîrgu Mureș, Tîrgu Mureș, Romania; 8The Department of Pathology, The University of Medicine and Pharmacy of Tîrgu Mureș, Tîrgu Mureș, Romania
Abstract: Herpes zoster usually affects the thoracic and lumbar vertebra (T3–L3), while sacral herpes zoster has been very rarely reported. We present a very rare case of herpes zoster involving S1 dermatome in a 35-year-old healthy man who presented aching pain and typical herpes zoster eruption on the lateral aspect of the calcaneus, lateral plantar area and dorsal aspect of digits III and IV.
Keywords: herpes zoster, S1, pain, sacral zoster
Introduction
Herpes zoster affects the thoracic and lumbar nerves and dermatomes (T3–L3) in the majority of cases;1 sacral herpes is very rare and it has been reported in only 4–8% of cases.2 When herpes zoster virus affects sacral nerves S2–S3 (motor and sensory nerves of the bladder), urinary dysfunction is reported,2,3 as well as constipation or bowel incontinence.4 Sacral herpes zoster has been described in elderly or in patients with impaired immune system.2
We present a typical case of herpes zoster S1 type with zosteriform eruption within S1 dermatome, intense pain and we review the literature related to S1 herpes zoster.
Case report
A 35-year-old previously healthy man was referred to the Dermatology Clinic for aching pain and clusters of vesicles located on the lateral aspect of the calcaneus, lateral plantar area and dorsal surface of digits III and IV (Figure 1). Pain and skin lesions had started 5 days and 1 day, respectively, before admission to hospital.
 | Figure 1 Clusters of vesicles located on the lateral plantar area (A), dorsal surface of digits III and IV (B), lateral aspect of the calcaneus (C and D). |
Dermatological examination revealed painful erythematous grouped vesicles within S1 dermatome and clinical diagnosis of herpes zoster was made. Laboratory tests, including HIV and hepatitis serology, proved to be within normal limits. Anti-VZV IgM was negative, but anti-VZV IgG was positive. Ballooning multinucleated giant cells were cytological findings of Tzanck smear done from the lesion and confirmed herpes infection.
Systemic administration of acyclovir 3 g/day orally for 10 days and NSAIDs were recommended, with favorable evolution and no complications for short or long term.
Discussion
Similar to other previous studies, a recent study confirms segmental involvement in herpes zoster related to epidemiology of herpes zoster: thoracic zoster 65.4%, cervical zoster 11.5%, lumbar zoster 8.3%, and sacral type only 3.5%.5
The person’s immune status is a key factor in determining the risk of developing herpes zoster; this can be induced by contact with a person with varicella or by reactivation of the virus in latently infected individuals. The reactivation rate of herpes zoster virus correlates with the decrease of immunity and with age.6
Subclinical reactivation of the virus has been described in some patients in response to stress,7 although, during lifetime, the immune system of the host contributes to the maintenance of immunity against herpes zoster virus .8
Sacral herpes zoster is rare and is usually located in S2–4 dermatome affecting the lower urinary tract,2-4 penis and scrotum,9 and rectum associated with constipation.10
A case of restless legs syndrome was reported in association with herpes zoster affecting S1 and S2 dermatomes, with zosteriform lesions located on the left buttock and the posterior aspect of left lower limb in the presence of high titer of varicella zoster virus-specific IgM in the blood, but no strict correlation was accomplished.10,11
S1 dermatome is anatomically delineated by the lateral aspect of the foot, the heel, and most of the sole (Figure 2).
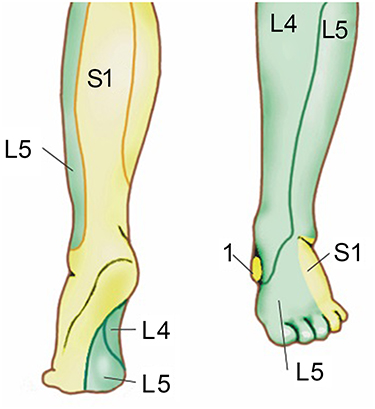 | Figure 2 S1 dermatome area, anatomically delineated by the lateral aspect of the foot, the heel, and most of the sole; L4–5: lumbar dermatoma. |
Conclusion
The present case is a rare type of S1 herpes zoster.
Ethical Approval
Ethical Approval was obtained from the Ethics Committee of Nicolina Medical Center, Iaşi.
Written informed consent has been provided by the patient to have the case details and any accompanying images published.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Whitley RJ. Varicella-Zoster virus infection. In: Longo DL, Fauci AS, Kasper DL, editors. Harrison‘S Principles of Internal Medicine,
2. Hur J. Sacral herpes zoster associated with voiding dysfunction in a young patient with scrub typhus. Infect Chemother. 2015;47(2):133–136.
3. Broseta E, Osca JM, Morera J, Martinez-Agullo E, Jimenez-Cruz JF. Urological manifestations of herpes zoster. Eur Urol. 1993;24(2):244–247.
4. Richmond W. The genito-urinary manifestations of herpes zoster. Three case reports and a review of the literature. Br J Urol. 1974;46(2):193–200.
5. Aggarwal SK, Radhakrishnan S. A clinico-epidemiological study of herpes zoster. Med J Armed Forces India. 2016;72(2):175–177. doi:10.1016/j.mjafi.2015.05.003
6. Cohrs RJ, Mehta SK, Schmid DS, Gilden DH, Pierson DL. Asymptomatic reactivation and shed of infectious varicella zoster virus in astronauts. J Med Virol. 2008;80(6):1116–1122. doi:10.1002/(ISSN)1096-9071
7. Ogunjimi B, Smits E, Heynderickx S, et al. Influence of frequent infectious exposures on general and varicella-zoster virus-specific immune responses in pediatricians. Clin Vaccine Immunol. 2014;21(3):417–426. doi:10.1128/CVI.00818-13
8. Marinelli I, van Lier A, de Melker H, Pugliese A, van Boven M. Estimation of age-specific rates of reactivation and immune boosting of the varicella zoster virus. Epidemics. 2017;19:1–12.
9. Arshad AR, Alvi KY, Chaudhary AA. Herpes zoster involving penis and scrotum: an unusual occurrence. J Coll Physicians Surg Pak. 2015;25(3):218–219. doi:08.2014/JCPSP.218219
10. Matsumoto H, Shimizu T, Tokushige S, Mizuno H, Igeta Y, Hashida H. Rectal ulcer in a patient with VZV sacral meningoradiculitis (Elsberg syndrome). Intern Med. 2012;51(6):651–654.
11. IpekdalI H, Karadas O, Oz O, Ulas UH. Restless legs syndrome secondary to sacral zona zoster. J Pain Symptom Manage. 2011;41(4):e8–e11. doi:10.1016/j.jpainsymman.2010.11.007
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.