Back to Journals » Clinical Ophthalmology » Volume 18
Clinical Outcomes of a Bi-Aspheric Trifocal Diffractive Intraocular Lens
Authors Tañá-Sanz S, Tañá-Sanz P, Rodríguez-Carrillo MD, Ruiz-Santos M, Álvarez de Toledo C, Tañá-Rivero P
Received 13 November 2023
Accepted for publication 20 December 2023
Published 4 January 2024 Volume 2024:18 Pages 27—40
DOI https://doi.org/10.2147/OPTH.S445128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Santiago Tañá-Sanz, Pedro Tañá-Sanz, Maria Dolores Rodríguez-Carrillo, María Ruiz-Santos, Clara Álvarez de Toledo, Pedro Tañá-Rivero
Cataract and Surgery Department, Oftalvist Alicante, Alicante, Spain
Correspondence: Pedro Tañá-Rivero, Oftalvist Alicante, C/ Angel Lozano 11, Alicante, 03001, Spain, Tel + 34 965 141 500, Email [email protected]
Purpose: To assess refractive and visual outcomes post-cataract surgery with bilateral implantation of a bi-aspheric diffractive trifocal intraocular lens (IOL).
Methods: A total of 24 patients who underwent bilateral implantation with the Asqelio Trifocal IOL TFLIO130C were evaluated at the 6 months postoperative mark. Key outcome measures included refractive error, photopic monocular and binocular uncorrected and corrected distance visual acuity (UDVA, CDVA), uncorrected and corrected intermediate visual acuity (UIVA, CDIVA) at 60 cm, and uncorrected and corrected near visual acuity (UNVA, CDNVA) at 40 cm. Additionally, monocular and binocular CDNVA were assessed under mesopic conditions. Monocular and binocular defocus curves, and binocular contrast sensitivity under photopic and mesopic conditions, with and without glare, were measured. Catquest-9SF and visual symptoms questionnaires were also administered.
Results: Postoperative average values of binocular logMAR photopic CDVA, photopic CDIVA, photopic CDNVA and mesopic CDNVA were − 0.01± 0.06, 0.03± 0.09, 0.02± 0.05 and 0.19± 0.13, respectively. About 100% of patients showed cumulative CDVA and CDNVA ≥ 20/25, and CDIVA ≥ 20/32. The average absolute depth-of-focus was about 4.50D. The average postoperative spherical equivalent was 0.05± 0.30D and 100% and 93.75% eyes were within ± 1.00D and ± 0.50D, respectively. Contrast sensitivity was either within or above normal levels under both photopic and mesopic conditions, both with and without glare, except for 12 cpd under mesopic conditions with glare where the mean falls just below the normal range. Questionnaires revealed that 87.5% of patients were either satisfied or very satisfied with their vision after the surgery, and higher percentages for no difficulty in performing different activities, ranging from 70.83% to 95.83%, were reported.
Conclusion: This study demonstrates that the bi-aspheric diffractive trifocal IOL yields very good visual performance across distances, fostering high satisfaction levels and minimal difficulties in daily activities.
Keywords: trifocal, diffractive, intraocular lens, phacoemulsification, cataract
Introduction
The advent of trifocal intraocular lenses (IOLs) represents a valuable tool for surgeons addressing cataract patients with a focus on enhancing intermediate visual acuity. These lenses are meticulously designed to not only improve intermediate vision but also uphold satisfactory levels of visual acuity for both distance and near vision. Numerous review articles have underscored the superiority of trifocal IOLs in enabling patients to achieve enhanced intermediate visual acuity compared to bifocal intraocular lenses. Remarkably, this improvement is attained without compromising near and distance visual performance, thereby ensuring spectacle independence or minimal postoperative refraction.1–3 Furthermore, trifocal IOLs have shown better performance and spectacle independence for near than extended depth-of-focus IOLs, but more dysphotopsia.4 The contrast sensitivity and subjective visual quality exhibit comparable outcomes between these design variations. It is important to note that in trifocal designs, the distribution of light between foci can impact the retinal image, potentially leading to a reduction in contrast sensitivity and an increase in photic phenomena. Additionally, it is noteworthy that objective dysphotopsia is not mitigated in extended depth-of-focus intraocular lenses when compared to trifocal intraocular lenses.5
In recent years, various new optical designs have emerged in the market, with trifocal intraocular lenses (IOLs) being among the most commonly implanted. These lenses are frequently utilized to afford pseudophakic patients a comprehensive range of vision, encompassing distances from far to near. One of the newer trifocal IOL designs available in the market is the Asqelio trifocal IOL (AST Products Inc, Billerica, MA, USA). This non-apodized diffractive posterior trifocal lens is based on a bi-aspheric design with two aspheric surfaces in order to increase the optical quality. This bi-aspheric design aimed to provide sharper images by increasing the distance MTF about 30% in relation to mono-aspheric designs. In addition, this also allows the best focus intermediate to be at +2.20D with 24% of light distribution at this focus for a 3-mm pupil aperture. Previous clinical studies done on this lens showed good visual and refractive outcomes on the short follow-up (1–3 months)6,7 and contrast sensitivity and patient reported outcomes.8 However, to the authors’ knowledge, there are no clinical peer-review publications of this lens analyzing specifically its visual and refractive outcomes at longer follow-ups with different visual metrics and questionnaires. Thus, the purpose of the present clinical study was to provide postoperative visual performance at different distances and different lighting conditions, effect of glare, refractive outcomes, and patient-reported outcomes in cataract patients with bilateral implantation at 6 months of follow-up.
Methods
This prospective study was approved by the Ethics Committee of the Hospital Clinico San Carlos (Madrid, Spain) and carried out in accordance with the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients prior to enrolment and after the potential consequences of participation in the study were explained. The study was registered at www.clinicaltrials.gov (registration number: NCT05065749).
Inclusion criteria were patients 50 years of age or older submitted to cataract surgery and implanted with the Asqelio Trifocal IOL TFLIO130C in accordance with standard clinical practice, patients seeking independence from spectacles following surgery, IOL power between +5.00 and +34.00D, transparent intraocular media, except for the cataract, in both eyes, and post-operatory potential visual acuity of 20/25 or better. Exclusion criteria were preoperatory corneal astigmatism greater than 0.75D, patients not providing informed consent, previous corneal surgery or trauma, irregular cornea (ie keratoconus), choroidal haemorrhage, microphthalmos, severe corneal dystrophy, uncontrolled or medically controlled glaucoma, clinically significant macular changes, severe concomitant ocular disease, not age-related cataract, severe optic nerve atrophy, diabetic retinopathy, amblyopia, extremely shallow anterior chamber, severe chronic uveitis, pregnant or lactating, rubella, mature/Dense cataract making preoperative fundus assessment difficult, previous retinal detachment, concurrent participation in other investigation using drugs or clinical devices and expecting ocular surgery within the study period.
Intraocular Lens
All patients were implanted with the Asqelio Trifocal TFLIO130C model IOL. Powers manufactured range from +5.00 to +34.00D in 0.50 D increments, with a C-Loop platform, 360 degrees square edge and a total IOL diameter of 13.0 mm. It is made of glistening free hydrophobic acrylic material with a refractive index of 1.50, UV absorber, Abbe number of 50, water content <0.5% and a spherical aberration of −0.27 microns.
The lens has a bi-aspheric geometry, with a posterior diffractive optic design that includes 15 rings within the central 4.5 mm of a 6.0 mm in diameter optical zone. The additions provided are +3.30D and +2.20D for near and intermediate distances, respectively. Light distribution among foci is 50% for distance, 24% for intermediate and 26% for near. The A-Constant used was 119.3 and 118.7 for optical and contact ultrasound biometry, respectively, as recommended by the manufacturer.
Surgical Procedure
A 2.2-mm limbal incision was made followed by a standard phacoemulsification using the Centurion® Vision System (Alcon Labs Inc., Fort Worth, TX, USA). After cataract removal and posterior capsule polishing, the capsular bag was filled with sodium hyaluronate 1.0% (Provisc, Alcon, Fort Worth, TX, USA). The spherical IOL power was determined using the ORA system with Verifeye+ (Alcon, Fort Worth, TX, USA) in aphakic condition. Postoperatively, all patients were prescribed with eyedrops of moxifloxacin 5 mg/mL (Vigamox; Alcon), prednisolone 10 mg/mL (Pred-Forte; Allergan, Inc., Irvine, CA, USA), and diclofenac-Lepori 1 mg/mL in a tapering dose for the first 4 weeks postoperatively.
Preoperative and Postoperative Assessment
Preoperatively, patients underwent an extensive ophthalmologic examination, including slit-lamp examination, determination of uncorrected distance visual acuity (UDVA), CDVA, subjective and objective refraction, IOP measurement, funduscopy, corneal topography and biometry with the IOLMaster 700 (Carl Zeiss Meditec AG, Jena, Germany). Barrett, Hoffer Q and SRK/T formulas were used to calculate the IOL power.
Postoperative examinations were carried out 6 months after implantation. A standard ophthalmologic examination, including refraction and slit-lamp biomicroscopy, was performed. Specifically, monocular and binocular UDVA, CDVA, uncorrected distance intermediate visual acuity (UIVA), corrected distance intermediate visual acuity (CDIVA) at 60 cm, uncorrected distance near visual acuity (UNVA) and corrected distance near visual acuity (CDNVA) at 40 cm were measured under photopic conditions using ETDRS charts. Additionally, monocular and binocular CDNVA were also measured under mesopic conditions (3 cd/m2). Monocular and binocular defocus curve were built for each patient with Sloan letter ETDRS chart using the Clinical Trial Suite (M&S Technologies, Inc, IL, USA) under photopic conditions (85cd/m2), from +2.00 to −5.00 D in 0.50 D steps (0.25D steps between 0 and ±0.50D). All data are shown as the mean ± standard deviation (SD) and ranges.
Clinical Trial Suite was also used to determine binocular contrast sensitivity with distance correction, both with and without glare, under photopic conditions (85 cd/m2) for the spatial frequencies of 3, 6, 12, and 18 cycles per degree (cpd), and under mesopic conditions (3 cd/m2) for the spatial frequencies of 1.5, 3, 6, and 12 cpd. The log absolute contrast threshold values were determined for each combination of patient, spatial frequency, and luminance level, and mean values and SD were then calculated. The corresponding contrast sensitivity values were computed from those thresholds as well (log CS), to plot the contrast sensitivity function.
Patients were requested to complete the Catquest-9SF patient outcomes questionnaire. This 9-item questionnaire determines patients’ limitations in daily life for carrying certain activities due to reduced vision, and its value in cataract surgery patients has been well previously reported.9–11 The test consists of 9 items with 4 response options, ranging from 4 for “very great difficulty/very dissatisfied” to 1 for “no difficulty/very satisfied”, and a “cannot decide” additional option, which is treated as missing data. Items A and C1–C7 are related with difficulty, while item B deals with satisfaction. Other questionnaire to assess the visual symptoms was also administered in order to explore the frequency, intensity, and level of bothersome of 10 common visual symptoms: glare, halos, starbursts, foggy vision, blurred vision, distortion, double vision, fluctuation in vision, difficulty focusing, and difficulty judging distances or depth. A simulated image was created and shown to the patient to aid describing each of the symptoms, and they were then asked to respond regarding frequency (from 1 (Never) to 4 (Very often)), intensity (from 1 (None) to 4 (Severe)), and bothersome level (from 1 (None) to 4 (A lot)).
Sample Size and Statistical Analysis
Estimated sample size for the study was calculated using the highest SD of the monocular defocus curve.12 Considering a SD of 0.24 logMAR at +2.00D of defocus, a 95% confidence interval, and a tolerated error of 0.10 logMAR; a minimum of 22 patients was required. SPSS v25.0 (Inc., Chicago, IL, USA) and Microsoft Excel for Mac v16.41 (Microsoft Co, Redmond, WA, USA) were used for data analysis. Significance level was set at p < 0.05. Categorical variables were described as frequencies and percentages, and continuous variables as mean and SD.
Results
Forty-eight eyes of 24 consecutive patients were analyzed for the present study. Table 1 shows the demographics for the patients enrolled. The mean age was 67.54±6.82 years (range 56 to 79 years) with 17 being female (87.5%) and 8 male (12.5%).
 |
Table 1 Demographic Characteristics of Participants Shown as Means, SD and Ranges |
Standard graphs for reporting refractive and visual acuity outcomes were built with the outcomes found at 6 months of follow-up.13 Figure 1 was plotted to assess the efficacy of the procedure, providing the cumulative postoperative binocular logMAR UDVA and CDVA (A), UIVA and CDIVA (B), and UNVA and CDNVA (C), respectively. About 100% of patients showed cumulative CDVA and CDNVA of 20/25 or better, and CDIVA of 20/32 or better. Specifically, 83.33% of patients showed an UDVA of 20/25 or better compared to 100% for CDVA, 87.50% of patients showed an UIVA of 20/25 or better compared to 91.76% for CDIVA, and 91.67% of patients showed an UNVA of 20/25 or better compared to 100% for CDNVA. Table 2 shows detailed values for the visual acuity at different distances under photopic and mesopic conditions. The postoperative mean values of binocular logMAR photopic CDVA, photopic CDIVA, photopic CDNVA and mesopic CDNVA were −0.01±0.06, 0.03±0.09, 0.02±0.05 and 0.19±0.13, respectively. Figure 2 depicts the change in lines of visual acuity between the postoperative binocular logMAR UDVA and CDVA. All patients showed an UDVA same or better than CDVA. Figure 3 represents the mean photopic monocular and binocular defocus curves with two main peaks of visual acuity located at 0D and −2.00D.
 |
Figure 1 Cumulative proportion of patients having a given photopic binocular (A) uncorrected distance visual acuity (UDVA) and best-corrected distance visual acuity (CDVA) values, (B) binocular uncorrected distance intermediate visual acuity (UIVA) and corrected distance intermediate visual acuity (CDIVA) values, and (C) uncorrected distance near visual acuity (UNVA) and corrected distance near visual acuity (CDNVA) values, at 6 months after surgery. |
 |
Figure 2 Change in lines of visual acuity between the photopic binocular postoperative uncorrected distance visual acuity (UDVA) and best-corrected distance visual acuity (CDVA) at 6 months after surgery. |
 |
Figure 3 Mean, high-contrast, photopic, monocular and binocular logMAR visual acuity with best correction for distance, as a function of the chart vergence. Error bars represent SD. Right Y-axis shows Snellen feet acuity and superior X-axis shows distance values (cm). |
 |
Table 2 LogMAR Visual Acuity Outcomes of Patients Implanted with the Asqelio Trifocal TFLIO130C Intraocular Lens Shown as Means, SD and Ranges |
To assess predictability, Figure 4 displays the histogram of postoperative spherical equivalent refraction relative to the intended target refraction (A) and preoperative corneal astigmatism and postoperative refractive astigmatism (B). For the spherical equivalent the highest percentage of eyes, 39.58%, was for the range between ±0.13D followed by 31.25% for the +0.14 to +0.50D range. About 100% eyes were within ±1.00D and 93.75% of eyes within ±0.50D. The mean postoperative spherical equivalent was 0.05±0.30 D (ranging from −0.75 to 0.75D). For the astigmatism, 100% of eyes showed a value ≤1.00D and 97.92% a value ≤0.50D, being the mean postoperative refractive cylinder −0.18±0.24D (ranging from 0 to −0.75D).
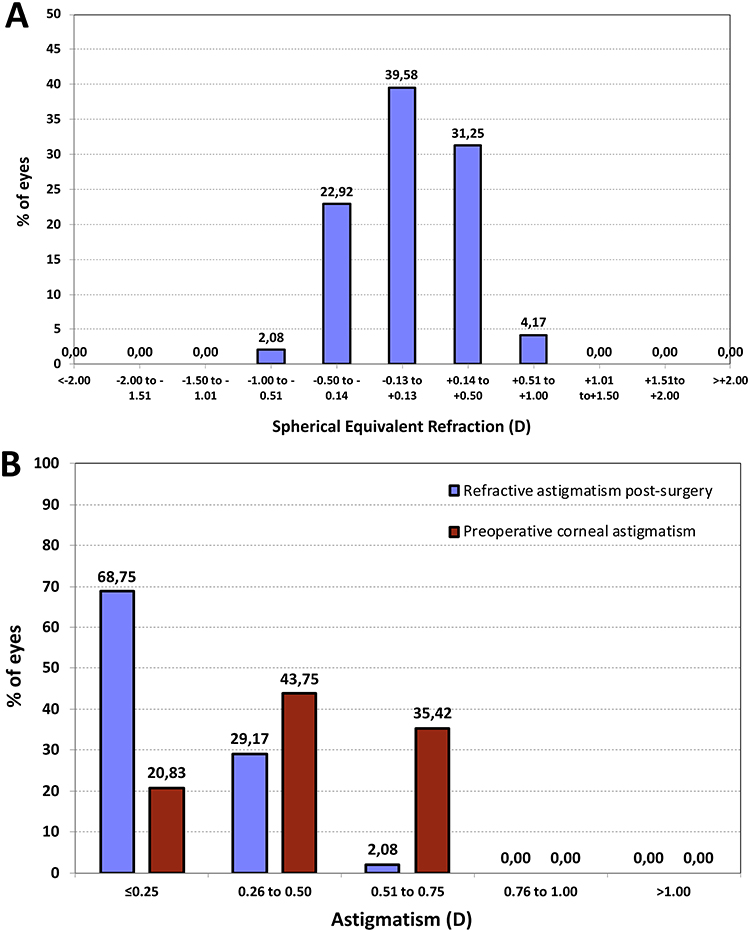 |
Figure 4 Histogram of postoperative spherical equivalent refraction at 6 months after surgery (A), and preoperative corneal astigmatism and postoperative refractive astigmatism at 6 months after surgery (B). |
Figure 5 shows the mean contrast sensitivity function determined under photopic conditions (85 cd/m2) with (A) and without glare (B) and under mesopic conditions (3 cd/m2) with (C) and without glare (D). Since the Clinical Trial Suite system does not include a normality range for healthy subjects under each of the conditions measured photopic and mesopic, with and without glare and similarly to previous reports by the authors,8 the normative ranges for healthy unoperated eyes above 60 years of age used by Escaf et al14 using the Functional Acuity Contrast Test (F.A.C.T.) were used in the present study as a reference to assess CSF outcomes. The results show that contrast sensitivity was either within or above normal levels, both with and without glare, under photopic and mesopic conditions. The only exception to this was mesopic contrast sensitivity for 12 cpd with glare, where the mean falls just underneath the reference range.
 |
Figure 5 Contrast sensitivity function determined under photopic conditions (85 cd/m2) with (A) and without induced glare (B) and under mesopic conditions (3 cd/m2) with (C) and without induced glare (D) Dotted lines delimit the normal range for non-operated eyes above 60 years of age using the Functional Acuity Contrast Test (F.A.C.T.).14 Error bars represent the 95% confidence intervals. |
In relation to the questionnaires, the outcomes found with the Catquest-9SF (Table 3) show that 87.5% of patients are satisfied (5/24) or very satisfied (16/24) with their vision after surgery, and one of the patients reports unsatisfaction with the results. The table displays the average grading and frequency of responses to difficulties in performing the daily activities included in the Catquest-9SF. In all cases, the results indicate higher percentages for no difficulty (R4) in performing any of those activities (ranging from 70.83% to 95.83%). Table 4 summarizes the outcomes of the visual symptoms’ questionnaire following the surgery. It indicates no relevant visual symptoms in either frequency, intensity or bothersome after implantation of the trifocal IOL. As expected for diffractive IOLs, and agreeing with previous reports with this IOL design,8 the frequency was higher for halos than for the other visual symptoms, with 33% of patients reporting quite often (4%) or very often (29%) presence of halos, but 83% of patients report either no bothersome (58%) or a little (25%).
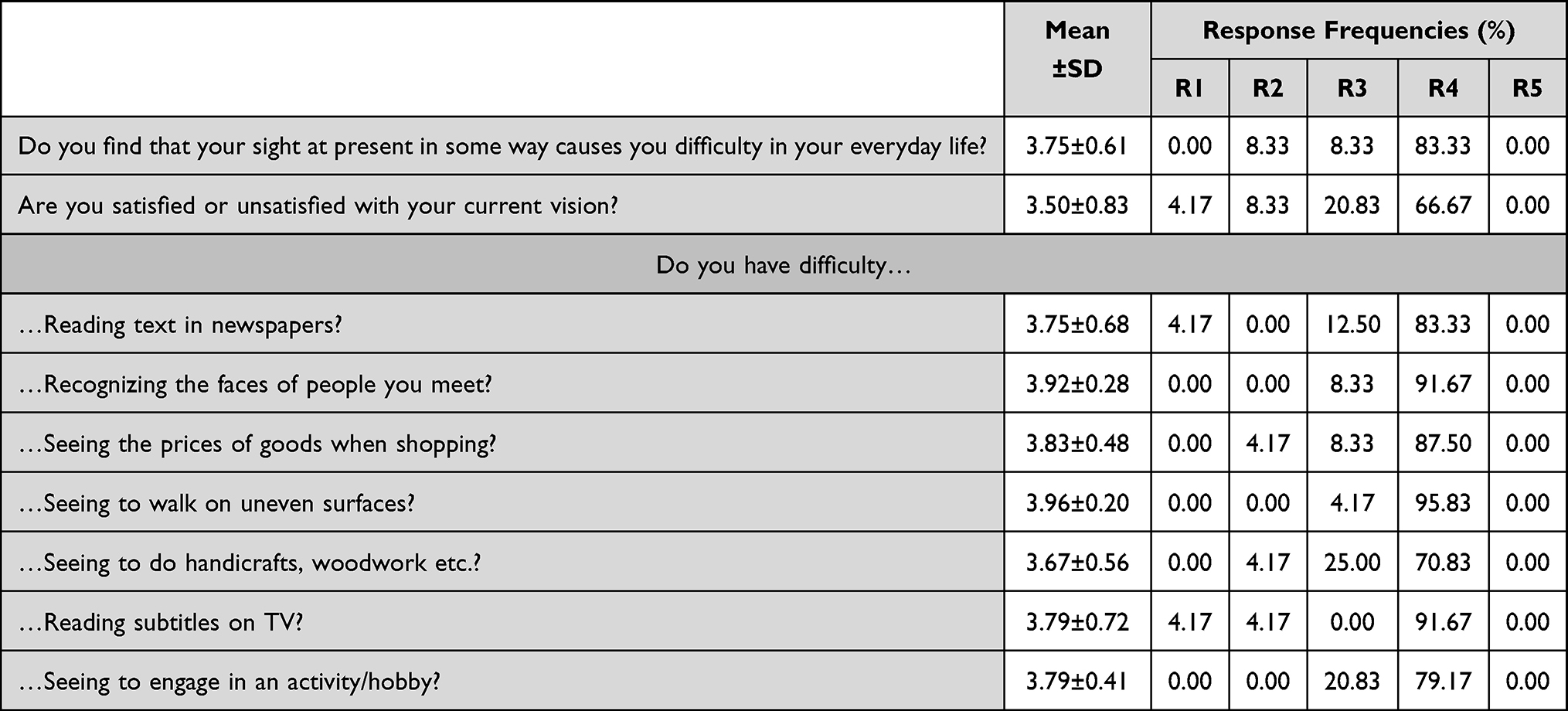 |
Table 3 Summary of Patient-Reported Difficulties and Satisfaction with Their Vision as per Catquest-9SF. Response Coding: R1 (Yes, Extreme Difficulty), R2 (Yes, Great Difficulty), R3 (Yes, Some Difficulty), R4 (No, No Difficulty), R5 (Cannot Decide) for Difficulties and R1 (Very Unsatisfied), R2 (Fairly Unsatisfied), R3 (Fairly Satisfied), R4 (Very Satisfied), R5 (Cannot Decide). SD: Standard Deviation |
 |
Table 4 Summary of Patient Reported Visual Symptoms (Mean Score, Type of Symptom and Frequency of Responses) as per Visual Quality Questionnaire. Response Coding (Frequency/Severity/Bothersome): R1 (Never/None/None), R2 (Occasionally/Mild/A Little), R3 (Quite Often/Moderate/Quite a Bit), R4 (Very Often/Severe/A Lot). SD: Standard Deviation |
Discussion
The main purpose of the present clinical study was to assess the refractive and visual outcomes at different distances following cataract surgery and implantation of the new bi-aspheric diffractive trifocal Asqelio Trifocal IOL. Previous clinical investigations have scrutinized the visual and refractive outcomes of other trifocal IOLs featuring diverse optical designs, affirming the commendable visual performance, especially at intermediate distances, in patients with these lenses,1–4 confirming the good visual performance of patients implanted with these lenses, particularly for intermediate distances. The current study scrutinized a recently introduced trifocal IOL with a bi-aspheric design, distinguishing it in the market for its potential to enhance optical and, consequently, visual quality for patients.
It is well known that trifocal IOLs use different technologies and designs to improve intermediate and near visual performance not compromising distance vision than the vision offered by monofocal models. Different designs may, obviously, provide different visual outcomes. The present study shows the outcomes of new design including bi-asphericity to provide good visual acuity over a range of distances usually required in daily tasks. In this regard, results revealed good visual acuities obtained at different distances: 100% of patients showed a cumulative CDVA and CDNVA of 20/25 or better, and CDIVA of 20/32 or better, being the mean values of −0.01±0.06, 0.03±0.09, 0.02±0.05 and 0.19±0.13 logMAR, respectively. A direct comparison with earlier studies on this trifocal IOL at this specific follow-up was unfeasible, as, to the best of the authors’ knowledge, this represents the inaugural investigation evaluating the performance of this IOL at the 6-month mark post-implantation. Palomino-Bautista et al6 analyzed the depth-of-focus and visual performance on 25 consecutive patients implanted with this IOL model at 1- and 3-months after implantation. At 3 months postop, they found mean values of −0.05±0.06, 0.03±0.08 and 0.04 and 0.08 logMAR for CDVA, CDIVA and CDNVA, respectively. Cano-Ortiz et al7 also examined 25 patients at 3 months and obtained the following mean values: −0.06±0.06, 0.02±0.09 and 0.06±0.07 logMAR, respectively. These previous reports with this IOL are in agreement with the outcomes obtained in the present study. In relation to the visual acuity at different vergences, Figure 3 shows the binocular defocus curve. Considering an absolute depth-of-focus as the range of visual acuity values ≤0.3 logMAR,15 considered as an adequate standard of distance vision for driving, it was about 4.50D from +1.00 to −3.50D. Palomino-Bautista et al6 obtained a mean monocular value of 4.82±0.69D when the same 0.3 logMAR cutoff value was considered, and Cano-Ortiz et al7 a binocular value of 3.64±0.70D considering a 0.1 logMAR threshold. The curves obtained in the present study show a peak at 0D of defocus (distance vision) with an average visual acuity around 0 logMAR, followed by a smooth decline up to −1.00D of defocus (equivalent to 1 m) and another peak at about −2.00D (equivalent to 50 cm) with a visual acuity better than 0.10 logMAR. This suggests that the lens not only ensures excellent distance vision but also delivers satisfactory intermediate and near vision.
In relation to refractive accuracy, a mean spherical equivalent of 0.05±0.30D and a mean postoperative refractive cylinder of −0.18±0.24D was obtained, with 100% eyes within ±1.00D and 93.75% of eyes within ±0.50D of spherical equivalent and 100% of eyes with ≤1.00D and 97.92% with ≤0.50D for refractive cylinder (see Figure 4). These results were good (mean values less than a quarter of diopter) and broadly agree with previous literature. In this sense, the mean spherical equivalent obtained by Palomino-Bautista et al6 was 0.05±0.23D and the residual cylinder was 0.01±0.23D, and by Cano-Ortiz et al7 was 0.21±0.27D and −0.20±0.35D, respectively. In addition, Cano-Ortiz et al7 found 84% and 100% of eyes within ±0.50D and ±1.00D of spherical equivalent, respectively, and 98% of eyes with ≤1.00D and 86% with ≤0.50D for refractive cylinder, respectively. These results support the good refractive outcomes of the lens when implanted.
Contrast sensitivity curves, plotted in Figure 5 for photopic and mesopic lighting conditions with and without glare, show average values within normal range or better in all cases. Under photopic conditions without glare, values were above normal range for low spatial frequencies and within normal range for the rest of frequencies explored, as occurs under mesopic conditions without glare. With glare, values were within normal range for all spatial frequencies under photopic conditions, while above normal range for lower spatial frequencies and only 12cpd falling just below normal range under mesopic conditions. All these results align with, and slightly surpass, those documented by the authors in a study conducted on a comparable sample utilizing the same system.8 Contrast sensitivity values are excellent under all conditions tested but, as indicated in that previous paper, it must be pointed out that the reference ranges considered in the analysis correspond to values obtained with a different CS system, due to the lack of an age-matched reference range with the CTS system used.
The present outcomes revealed that 87.5% of patients are either satisfied or very satisfied with their vision after bilateral implantation of Asqelio Trifocal IOLs, as per the Catquest9SF. Palomino-Bautista et al6 asked their patients to grade their satisfaction on a scale from 0 to 10, with being 10 completely satisfied, and reported a mean response of 8.32/10 for overall satisfaction, 8.24/10 for satisfaction at distance, 8.04/10 for satisfaction at intermediate distances, and 7.88/10 for near. Cano-Ortiz et al7 used the Catquest-9SF questionnaire, the patient-reported spectacle independence questionnaire (PRSIQ) and the patient-reported visual symptoms questionnaire (PRVSQ) to determine the patient-reported outcomes after bilateral implantation of Asqelio Trifocal IOLs. They found that all patients achieved spectacle independence for distance vision, while 96% did for intermediate and 88% for near, and 92% reported having achieved independence for vision at all distances. They also reported that >80% of patients were either very satisfied or completely satisfied with their vision without additional compensation for distance, intermediate, or overall. This percentage decreased to 56% for near vision.
With regards to visual symptoms, halos were by far the most frequent among the patients in the present study, with 33% of patients reporting halos as a quite often (4%) or very often (29%) event, followed by starburst (21%), while 83% of patients reported to be either not bothered at all (58%) or just a little (25%) by halos. These results agree with previous patient-reported outcomes after bilateral implantation of this IOL design.6,7 Palomino-Bautista et al6 asked their patients to score the perception and bothersome levels of halo after surgery on a scale from 0 (not perceiving/bothered by halos) to 10 (very concerned about halos). They reported an average response for bothersome of 4.36. Cano-Ortiz et al7 found that more than 50% of the patients were aware of halos most of the time, but only 16% reported a severe bothersome. For starbursts, they found 28% experienced them most of the time, but only 8% reported a severe bothersome. In the case of glare, 20% reported experiencing most of the time, and 12% reported severe impairment.
The outcomes of the present study analyzed against those reported for other trifocal IOL designs available in the market show comparable results. Martínez de Carnero-Llorente et al16 compared PanOptix, AT Lisa tri 839MP and FineVision IOLs in 40 patients per IOL group. At 6 months post-surgery they did not find statistically significant differences between-groups for spherical equivalent, UDVA, CDVA, DCNVA, reading performance or contrast sensitivity under photopic and mesopic conditions. Sezgin17 conducted a comparison between the PanOptix and the AT Lisa tri 839 MP IOLs in a sizable sample (238 eyes, 119 patients). The study found that the mean corrected distance intermediate visual acuity (CDIVA) at 60 cm was superior in the PanOptix group compared to the AT Lisa IOL group (0.07±0.07 vs 0.22±0.10 logMAR, respectively; P<0.001). In the present study, Asqelio Trifocal exhibited a mean value of 0.09±0.11 logMAR under monocular conditions. The mean CDIVA at 80 cm favoured the AT Lisa IOL group over PanOptix (0.07±0.08 vs 0.17±0.09 logMAR, respectively; P<0.001). However, at vergence distances ranging from 1.00D to −2.50D, PanOptix demonstrated significantly better outcomes (P=0.011 to <0.001). The study concluded that both lenses provided similar and favourable visual and refractive outcomes, with the PanOptix lens being more suitable for patients requiring optimal closer intermediate viewing. In a study by Ribeiro and Ferreira,18 the outcomes of the FineVision, RayOne trifocal, and PanOptix IOLs were compared in 30 eyes of 15 patients per group at 3 months post-surgery. The results indicated no statistically significant differences between groups for distance, intermediate, and near visual acuity (p≥0.112), as well as for postoperative refraction (p≥0.059). Binocular uncorrected intermediate visual acuity (UIVA) of ≥0.10 logMAR was observed in 93.33% (14 patients) in the three groups, while it was 87.50% in the present study (see Figure 1B). Binocular uncorrected near visual acuity (UNVA) of ≥0.10 logMAR was found in 86.67% (13), 93.33% (14), and 86.67% (13) patients in the FineVision, RayOne, and PanOptix IOLs groups, respectively, compared to 91.67% in the present study (see Figure 1C). The study reported no statistically significant differences between groups for scotopic contrast sensitivity with and without glare and quality of vision questionnaire scores (p≥0.057), except for the difference between the FineVision and RayOne IOLs groups in depth perception severity, which was lower for the RayOne IOL group (p=0.019). Lapid-Gortzak et al19 in a multicenter study evaluated the visual outcomes of the AcrySof IQ PanOptix and the AT Lisa tri 839MP in 182 patients. They found that the PanOptix IOL demonstrated superior visual outcomes compared to the AT Lisa lens in binocular uncorrected intermediate visual acuity (UIVA) and uncorrected near visual acuity (UNVA) and noninferior outcomes in uncorrected distance visual acuity (UDVA). The mean defocus curve from 0 to −3D ranged from 0.1 to 0.0 logMAR for both lens designs, with better mean logMAR visual acuity observed for the PanOptix IOL between −1.50 and −2.50 D vergence distances compared to the AT Lisa IOL group. The defocus curve obtained in the present study (Figure 3) exhibits a similar performance. Contrast sensitivity values reported in this study were comparable between lenses in all conditions. They concluded that improved visual performance at near and intermediate distances with PanOptix IOL compared with that of AT Lisa tri IOL. Carreño et al20 compared PanOptix and FineVision IOLs in a sample of 500 eyes (250 patients) and found that 96% of all eyes were within ±0.50D of the intended spherical equivalent correction and the mean defocus was ≥0.1 logMAR from 0.00 to −3.00 D. Also found, with a cutoff of 0.2 logMAR, that 96% of patients had a range of vision ≥2.5 D. The accuracy in the present study was similar, a 93.75%. Hienert et al21 compared the RayOne Trifocal and the AT Lisa tri 839 MP IOLs and concluded that both IOLs delivered good and comparable visual function with low degrees of disturbing dysphotopsia, with the RayOne behaving slightly better as plotted in the defocus curve, whereas the AT Lisa performed better with regards to contrast sensitivity and positive dysphotopsia. Ferreira et al22 compared the PanOptix and the FineVision POD F trifocal IOLs in 60 patients (30 per group) at 3 months post-surgery and found no statistically significant differences between them in monocular CDIVA (0.05±0.09 and 0.08±0.01 logMAR, respectively), similar to the 0.09±0.11 logMAR found in the present study. Also, recently, a large sample study was carried out by Brenner et al23 with 17,603 consecutive patients submitted to bilateral presbyopia refractive lens exchange with the FineVision trifocal IOL. The authors of this study found that 85% of the patients presented binocular UDVA ≥0.0 LogMAR and Jaeger 3, whereas 85.6% of the eyes were within ±0.50D from emmetropia (in the present study were 93.75%). Safety and efficacy indices reported were 0.98±0.11 and 0.85±0.18, respectively. About 0.38% of the eyes lost ≥2 lines of CDVA, with cystoid macular oedema (40.8%) and posterior capsular opacification (26.9%) being regarded as the main causes. Authors indicated that after proper care, the final incidence of ≥2 lines of vision loss was 0.08%.
In relation to the questionnaire outcomes, Rementería-Capelo et al24 used the Catquest-9SF questionnaire in 125 patients implanted bilaterally with the PanOptix trifocal IOLs at 3 months post-surgery. They found that patients implanted with these lenses, using both toric and non-toric models, said that they had little difficulty carrying out everyday life activities, and being satisfied overall with their postoperative vision. In a different study,25 the same questionnaire was used in patients implanted with the FineVision (n=32) and the PanOptix (n=36) lenses. The authors found that the percentage of patients reporting satisfaction with their vision were 83.9% and 88.9% for the FineVision and PanOptix groups of patients, respectively. The present study revealed that 87.5% of patients are either satisfied or very satisfied with their vision after implantation of Asqelio Trifocal IOL.
It is important to acknowledge that methodological differences between the clinical protocols of various studies may contribute to the observed discrepancies. For instance, the present study employed the CTS system to control all visual parameters, while many studies in the literature utilize standard LogMAR charts, and illuminance control is not consistently ensured. Despite these variations, the overall comparison suggests comparable outcomes with the studied IOL design and those reported in existing literature. It would be beneficial to compare the outcomes of the present study with research conducted by different investigators using the same IOL, and with longer follow-up periods. Future investigations should also explore the toric version of this model, emphasizing rotational stability at different post-surgery intervals.
Conclusion
To conclude, the present study supports that the Asqelio Trifocal TFLIO130C lens is efficient trifocal IOL design providing good clinical outcomes at all distances. The reported high level of patient satisfaction post-implantation positions it as a valuable choice for individuals seeking independence from spectacles, with minimal impact on visual disturbance and very good visual outcomes visual outcomes.
Data Sharing Statement
The data are not available for sharing.
Funding
This study has been funded by AST Products, Inc. (Billerica, MA, USA).
Disclosure
Dr Pedro Tañá-Rivero reports grants from AST Products Inc, during the conduct of the study; grants from Alcon Labs, grants from Carl Zeiss Meditec, grants from Heidelberg Engineering, grants from Hoya Surgical, grants from Humanoptics Holding, grants from Johnson&Johnson, grants from BVI, grants from Staar Surgical, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Shen Z, Lin Y, Zhu Y, Liu X, Yan J, Yao K. Clinical comparison of patient outcomes following implantation of trifocal or bifocal intraocular lenses: a systematic review and meta-analysis. Sci Rep. 2017;7(1):45337. doi:10.1038/srep45337
2. Yang JJ, Liu QP, Li JM, Qin L. Comparison of visual outcomes with implantation of trifocal versus bifocal intraocular lens after phacoemulsification: a meta-analysis. Int J Ophthalmol. 2018;11(3):484–492. doi:10.18240/ijo.2018.03.20
3. Jin S, Friedman DS, Cao K, et al. Comparison of postoperative visual performance between bifocal and trifocal intraocular Lens based on randomized controlled trails: a meta-analysis. BMC Ophthalmol. 2019;19(1):78. doi:10.1186/s12886-019-1078-1
4. Zhong Y, Wang K, Yu X, Liu X, Yao K. Comparison of trifocal or hybrid multifocal-extended depth of focus intraocular lenses: a systematic review and meta-analysis. Sci Rep. 2021;11(1):6699. doi:10.1038/s41598-021-86222-1
5. Escandón-García S, Ribeiro FJ, McAlinden C, Queirós A, González-Méijome JM. Through-focus vision performance and light disturbances of 3 new intraocular lenses for presbyopia correction. J Ophthalmol. 2018;2018:6165493. doi:10.1155/2018/6165493
6. Palomino-Bautista C, Cerviño A, Cuiña-Sardiña R, Carmona-Gonzalez D, Castillo-Gomez A, Sanchez-Jean R. Depth of field and visual performance after implantation of a new hydrophobic trifocal intraocular lens. BMC Ophthalmol. 2022;22(1):240. doi:10.1186/s12886-022-02462-3
7. Cano-Ortiz A, Á S-V, González-Cruces T, et al. Visual performance, satisfaction, and spectacle independence after implantation of a new hydrophobic trifocal intraocular lens. J Clin Med. 2022;11(19):5931. doi:10.3390/jcm11195931
8. Tañá-Rivero P, Orts-Vila P, Aguilar-Córcoles S, Tañá-Sanz P, Tañá-Sanz S. Contrast sensitivity and patient reported outcomes after bilateral implantation of a bi-aspheric hydrophobic trifocal diffractive intraocular lens. Clin Ophthalmol. 2023;17:247–258. doi:10.2147/OPTH.S400136
9. McAlinden C, Gothwal VK, Khadka J, Wright TA, Lamoureux EL, Pesudovs K. A head-to-head comparison of 16 cataract surgery outcome questionnaires. Ophthalmology. 2011;118(12):2374–2381. doi:10.1016/j.ophtha.2011.06.008
10. Khadka J, McAlinden C, Pesudovs K. Quality assessment of ophthalmic questionnaires: review and recommendations. Optom Vis Sci. 2013;90:8):720–744. doi:10.1097/OPX.0000000000000001
11. Kabanovski A, Hatch W, Chaudhary V, et al. Validation and application of catquest-9SF in various populations: a systematic review. Surv Ophthalmol. 2020;65(3):348–360. doi:10.1016/j.survophthal.2019.12.002
12. Sullivan L Power and Sample Size determination. Boston University School of public health. Available from: https://sphweb.bumc.bu.edu/otlt/MPHzodules/BS/BS704_Power/BS704_Power_print.html.
13. Reinstein DZ, Archer TJ, Srinivasan S, et al. Standard for reporting refractive outcomes of intraocular lens-based refractive surgery. J Refract Surg. 2017;33(4):218–222. doi:10.3928/1081597X-20170302-01
14. Escaf LJ, Escaf LC, Polo S, Rodríguez-Vallejo M, Fernández J. Standard results and contrast sensitivity reestablishment after implantation of a trifocal intraocular lens. Curr Eye Res. 2021;46(5):672–677. doi:10.1080/02713683.2020.1828486
15. Plakitsi A, Charman N. Comparison of the depths of focus with the naked eye and with three types of presbyopic contact lens correction. J Br Contact Lens Assoc. 1995;18(4):119–125. doi:10.1016/S0141-7037(95)80023-9
16. Martínez de Carneros-Llorente A, Martínez de Carneros A, Martínez de Carneros-Llorente P, Jiménez-Alfaro I. Comparison of visual quality and subjective outcomes among 3 trifocal intraocular lenses and 1 bifocal intraocular lens. J Cataract Refract Surg. 2019;45(5):587–594. doi:10.1016/j.jcrs.2018.12.005
17. Sezgin Asena B. Visual and refractive outcomes, spectacle independence, and visual disturbances after cataract or refractive lens exchange surgery: comparison of 2 trifocal intraocular lenses. J Cataract Refract Surg. 2019;45(11):1539–1546. doi:10.1016/j.jcrs.2019.06.005
18. Ribeiro F, Ferreira TB. Comparison of clinical outcomes of 3 trifocal IOLs. J Cataract Refract Surg. 2020;46(9):1247–1252. doi:10.1097/j.jcrs.0000000000000212
19. Lapid-Gortzak R, Bhatt U, Sanchez JG, et al. Multicenter visual outcomes comparison of 2 trifocal presbyopia-correcting IOLs: 6-month postoperative results. J Cataract Refract Surg. 2020;46(11):1534–1542. doi:10.1097/j.jcrs.0000000000000274
20. Carreño E, Carreño EA, Carreño R, Carreño M, López V, Potvin R. Refractive and visual outcomes after bilateral implantation of a trifocal intraocular lens in a large population. Clin Ophthalmol. 2020;14:369–376. doi:10.2147/OPTH.S238841
21. Hienert J, Stjepanek K, Hirnschall N, Ruiss M, Zwickl H, Findl O. Visual performance of two diffractive trifocal intraocular lenses: a randomized trial. J Refract Surg. 2021;37(7):460–465. doi:10.3928/1081597X-20210420-01
22. Ferreira TB, Ribeiro FJ, Silva D, Matos AC, Gaspar S, Almeida S. Comparison of refractive and visual outcomes of 3 presbyopia-correcting intraocular lenses. J Cataract Refract Surg. 2022;48(3):280–287. doi:10.1097/j.jcrs.0000000000000743
23. Brenner LF, Nistad K, Schonbeck U. Rethinking presbyopia: results of bilateral refractive lens exchange with trifocal intraocular lenses in 17 603 patients. Br J Ophthalmol. 2023;107(7):912–919. doi:10.1136/bjophthalmol-2021-319732
24. Rementería-Capelo LA, Contreras I, García-Pérez JL, Blázquez V, Ruiz-Alcocer J. Visual quality and patient satisfaction with a trifocal intraocular lens and its new toric version. J Cataract Refract Surg. 2019;45(11):1584–1590. doi:10.1016/j.jcrs.2019.06.014
25. Rementería-Capelo LA, García-Pérez JL, Gros-Otero J, Carrillo V, Pérez-Lanzac J, Contreras I. Real-world evaluation of visual results and patient satisfaction for extended range of focus intraocular lenses compared to trifocal lenses. Int Ophthalmol. 2021;41(1):163–172. doi:10.1007/s10792-020-01563-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Refractive and Visual Outcomes of a Monofocal Non-Constant Aberration Aspheric Intraocular Lens
Hernández-Martínez A, Díaz-del-Rio MA, Ruiz-Santos M, Ruiz-Mesa R, Tañá-Rivero P
Clinical Ophthalmology 2022, 16:2521-2530
Published Date: 10 August 2022
Long Term Clinical Outcomes of Hydrophilic and Hydrophobic Versions of a Trifocal IOL with the Same Optical Design
Ang RET
Clinical Ophthalmology 2023, 17:623-632
Published Date: 21 February 2023
Clinical Outcomes of a Monofocal, Optimized, Aspheric, Hydrophobic Acrylic Intraocular Lens Implant
García-Tomás B, Marín-Sánchez JM, García-Elskamp C, Alcon-Ruiz E, Montesinos-López L, García Martínez-Lozano B
Clinical Ophthalmology 2023, 17:3215-3224
Published Date: 27 October 2023
Clinical Performance of a New Trifocal IOL with a 7.0 mm Optical Zone
Pastor-Pascual F, Orts-Vila P, Tañá-Sanz P, Tañá-Sanz S, Tañá-Rivero P
Clinical Ophthalmology 2023, 17:3397-3407
Published Date: 7 November 2023
Six-Month Visual and Patient-Reported Outcomes of a Biaspheric Trifocal IOL in Asian and European Cataract Patients: A Comparative Study
Hwang YS, Tañá-Rivero P, Tañá-Sanz S, Lee JS, Tañá-Sanz P, Cerviño A
Clinical Ophthalmology 2025, 19:4481-4491
Published Date: 8 December 2025