")
Back to Journals » Clinical Epidemiology » Volume 15
Risk Profiles of New Users of Oral Anticoagulants Between 2011 and 2019 in Germany
Authors Voss A , Kollhorst B , Platzbecker K , Amann U , Haug U
Received 14 February 2023
Accepted for publication 21 June 2023
Published 18 July 2023 Volume 2023:15 Pages 827—837
DOI https://doi.org/10.2147/CLEP.S405585
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Vera Ehrenstein
Annemarie Voss,1 Bianca Kollhorst,2 Katharina Platzbecker,1 Ute Amann,1 Ulrike Haug1,3
1Department of Clinical Epidemiology, Leibniz Institute for Prevention Research and Epidemiology – BIPS, Bremen, Germany; 2Department of Biometry and Data Management, Leibniz Institute for Prevention Research and Epidemiology – BIPS, Bremen, Germany; 3Faculty of Human and Health Sciences, University of Bremen, Bremen, Germany
Correspondence: Ulrike Haug, Department of Clinical Epidemiology, Leibniz Institute for Prevention Research and Epidemiology – BIPS, Bremen, Germany, Tel +49 421 218 56862, Email [email protected]
Purpose: Over the last decade, the use of direct oral anticoagulants (DOACs) has strongly increased. We aimed to describe and compare risk profiles including potential changes over time among persons with non-valvular atrial fibrillation initiating treatment with different DOACs or phenprocoumon (vitamin K antagonist) between 2011 and 2019 in Germany.
Patients and Methods: Using the German Pharmacoepidemiological Research Database (GePaRD; claims data of ~20% of the German population), we identified persons with a first dispensing of phenprocoumon or a DOAC and a diagnosis of non-valvular atrial fibrillation between August 2011 and December 2019. We described the morbidity of included patients prior to treatment initiation, stratified by year of treatment initiation.
Results: Overall, we included 448,028 new users (phenprocoumon: N = 118,117, rivaroxaban: N = 130,997, apixaban: N = 130,300, edoxaban: N = 38,128, dabigatran: N = 30,486). Comparing new DOAC users in 2019, the proportion with prior ischemic stroke was highest for dabigatran (17%) and lowest for rivaroxaban (8%). The proportion with prior major bleeding was also highest for dabigatran (25%) and lowest for edoxaban (20%). New users of apixaban were oldest and, eg, showed the highest prevalence of congestive heart failure. Changes over time were most pronounced for phenprocoumon. For example, among persons initiating phenprocoumon in 2012 vs 2019, the proportion with prior major bleeding increased from 18% to 35%; the proportion with renal disease increased from 20% to 36% and the proportion with liver disease from 18% to 24%.
Conclusion: This study demonstrated differences in risk profiles between new users of different oral anticoagulants and substantial changes over time among new phenprocoumon users. These differences have to be considered in head-to-head comparisons of these drugs based on observational data, especially regarding potential unmeasured confounding.
Keywords: atrial fibrillation, oral anticoagulants, direct oral anticoagulants, DOACs, risk profiles
Introduction
Atrial fibrillation is one of the major causes of stroke, heart failure, sudden death and cardiovascular morbidity. The global prevalence increased by 33% during the past 20 years and in 2017, over 37 million people worldwide had a diagnosis of atrial fibrillation.1 For many years, vitamin K antagonists (VKAs) had been the most widely used drugs to prevent cerebral embolism in patients with atrial fibrillation. Since 2011, several new oral anticoagulants (OACs) have been approved for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation, known as direct oral anticoagulants (DOACs) or non-vitamin K antagonist oral anticoagulants. The DOAC approved first was dabigatran (2011), a thrombin inhibitor, followed by the three factor Xa inhibitors rivaroxaban (2011), apixaban (2012) and edoxaban (2015). Their safety and effectiveness have been shown to be non-inferior to warfarin, the most commonly used VKA worldwide, in randomized controlled trials (RCTs) and observational studies.2–7 In contrast to VKAs, all DOACs have more predictable pharmacokinetic properties, ie, there is no routine anticoagulation monitoring.8 Their use in clinical practice is increasing rapidly.9
Given that there is no RCT comparing all four DOACs, a direct head-to-head comparison investigating safety and effectiveness based on observational data would be of general interest. Even though there are meta-analyses of existing studies comparing DOACs, the heterogeneity between studies is a limitation of such indirect comparisons and in addition, there were no data on edoxaban.10–12 In preparation of a direct head-to-head comparison of all available DOACs based on observational data, it is important to characterize the users of the different drugs. In case such a study reveals differences in measured confounders between groups, there is also a higher risk of bias due to unmeasured confounding. In fact, there are several reasons why risk profiles between DOAC users may differ. First, the successive approval of DOACs could have resulted in various forms of channelling, possibly also influenced by marketing strategies. Second, antidotes became available over time: for dabigatran, idarucizumab was approved in 2016 and for rivaroxaban and apixaban, andexanet alfa has been available since 2019. For edoxaban, an approved antidote is still missing. Third, differences in dose regimens, ie, once daily (rivaroxaban, edoxaban) or twice daily (dabigatran, apixaban), could have an impact on the treatment decision. Finally, in Germany, discounts for certain drugs and regional recommendations for economical prescribing could also play a role.
Even though there are many observational studies investigating the safety and effectiveness of OACs,13–18 studies systematically comparing the risk profiles of patients using different OACs are lacking. We therefore aimed to describe and compare risk profiles (eg, risk of bleeding, cardiovascular risk) including potential changes over time of patients with non-valvular atrial fibrillation initiating treatment with different DOACs or phenprocoumon, the most commonly used VKA in Germany, between 2011 and 2019.
Methods
Data Source
We used the German Pharmacoepidemiological Research Database (GePaRD), which consists of claims data from four statutory health insurance providers (SHIs) in Germany. This database currently includes information on >25 million persons who have been insured with one of the participating providers since 2004 or later.19 In addition to demographic data, GePaRD contains information on reimbursable drug dispensations as well as outpatient (ie, from general practitioners and specialists) and inpatient services and diagnoses. Per data year, there is information on approximately 20% of the general population and all geographical regions of Germany are represented.
Study Population and Study Design
To identify new users of OACs, namely phenprocoumon, dabigatran, rivaroxaban, apixaban or edoxaban, we considered all patients with a first-time dispensation (index dispensation) of one of the respective study drugs and a diagnosis of non-valvular atrial fibrillation any time between August 2011 (approval of the first DOAC, dabigatran) and December 2019. Regarding VKAs, we focused on phenprocoumon given that 99% of VKA users in Germany use phenprocoumon, ie, warfarin hardly plays a role and acenocoumarol is not approved in Germany.15 Non-valvular atrial fibrillation was assumed to be present if there were at least one inpatient or two outpatient diagnosis codes (ICD-10 GM I48x) in the year before the index dispensation or an outpatient diagnosis in the same quarter as the index dispensation.20 Patients were excluded if there was any record of mitral stenosis or an artificial heart valve any time before the index dispensation, taking into account the patient’s full database history (ie, also from years before 2011). We also excluded patients with missing or unclear information on sex or age, and those without permanent residency in Germany. Furthermore, we excluded patients who had not been continuously insured for at least one year before the index dispensation and those with a dispensation of any OAC any time before the index dispensation. The date of the index dispensation at which all inclusion and exclusion criteria were met was assigned as the index date. We defined sub-cohorts according to the type of OAC of the index dispensation.
Variables to Characterize the Risk Profiles of New OAC Users
In terms of medication increasing or decreasing the risk of bleeding, we assessed whether there was at least one dispensation of an antiplatelet drug, a non-steroidal anti-inflammatory drug (NSAID), an antiarrhythmic drug, an oral steroid, a selective serotonin reuptake inhibitor (SSRI) or a proton pump inhibitor (PPI) in the year prior to index date. ATC codes are listed in Supplementary Table 1.
Furthermore, we assessed the presence of relevant past cardiovascular events including ischemic stroke, transient ischemic attack (TIA), venous thromboembolisms (including deep vein thrombosis and pulmonary embolism) and major bleedings, as well as chronic diseases such as coronary heart disease, hypertension, heart failure, vascular disease, diabetes mellitus, renal and liver disease recorded any time prior to index date based on algorithms described in Supplementary Table 2. For classification of the stroke and bleeding risk, we calculated the CHA2DS2VASc score21 and the modified HAS-BLED score22 in SAS as described in the Supplementary Tables 3–4.
In sensitivity analyses, we restricted the look-back period for the assessment of comorbidities to “one year prior” to index date (rather than “any time prior”) in order to assess the impact of the length of the look-back period on the prevalence of comorbidities.
Data Analysis
We described the characteristics of the study population using frequency counts and percentages for categorical variables; for continuous variables, we used medians with their interquartile range (IQR) and means with their standard deviation. To assess trends in patient characteristics over time, we stratified the analyses by year of index date. For the sake of clarity, we partly restricted the results presented in the main manuscript to the data year 2019, the most recent data at the time of analysis, but provide the results for all other years in the supplement. The analyses were performed with the statistical software SAS 9.4 (SAS Institute, Cary, NC, USA).
Results
A total of 448,028 new OAC users with non-valvular atrial fibrillation were included in this study (phenprocoumon: N = 118,117, rivaroxaban: N = 130,997, apixaban: N = 130,300, edoxaban: N = 38,128, dabigatran: N = 30,486). In patients with index date in 2019, the proportion of male patients ranged from 49% (apixaban) to 54% (dabigatran and rivaroxaban) in new DOAC users and was 57% in new phenprocoumon users. The median age at index date ranged from 75 years (dabigatran and rivaroxaban) to 77 years (apixaban) and was 75 years among new phenprocoumon users. The proportion of patients aged >75 years was highest in new apixaban users (60.4%), followed by new edoxaban users (57.1%) and new user of dabigatran and rivaroxaban (~51%) (Table 1). Also, in other years, new users of apixaban were oldest and had the lowest proportion of males in comparison to other new OAC users (see Supplementary Table 5a–e).
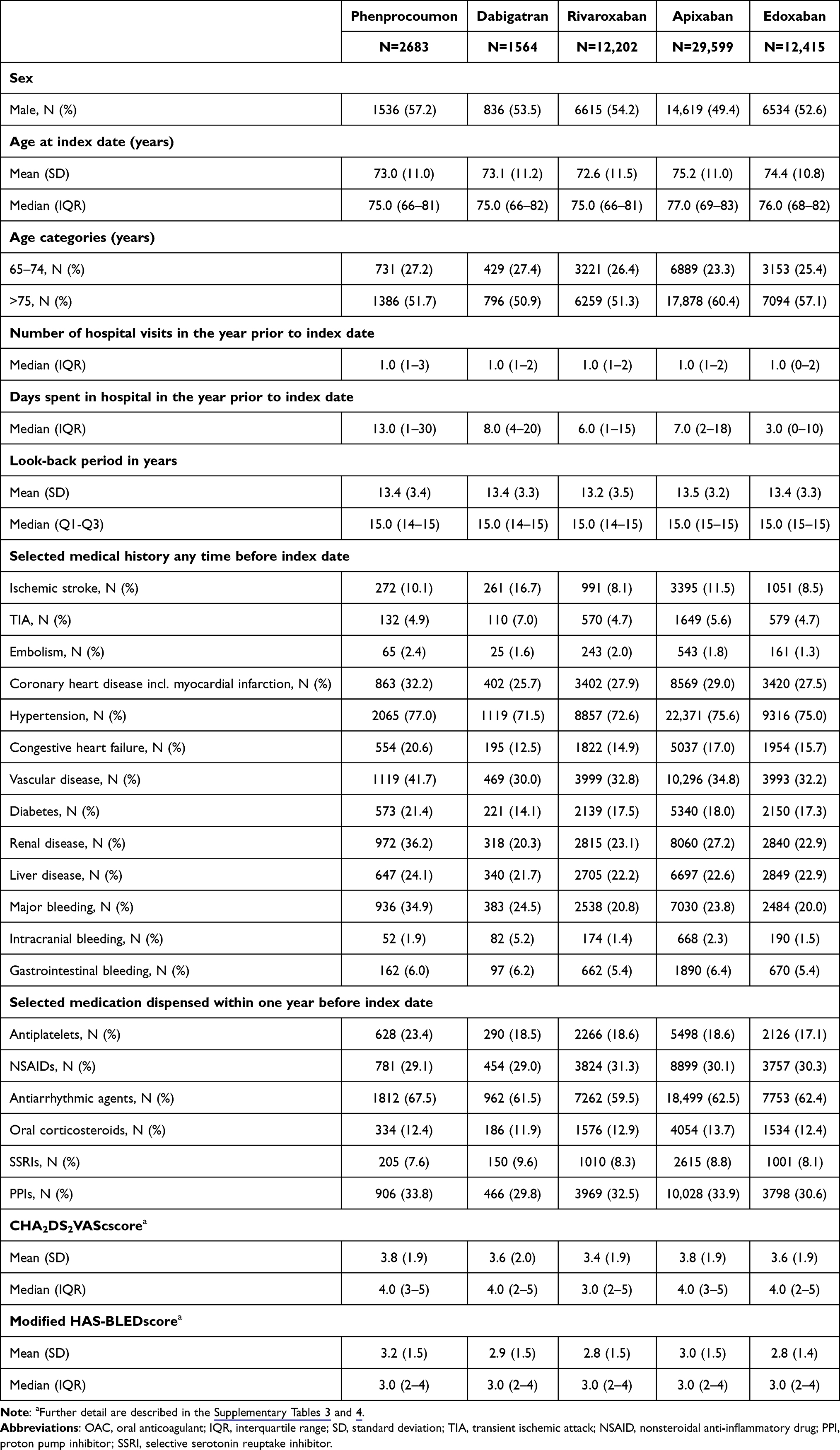 |
Table 1 Baseline Characteristics of New OAC Users with Index Date in 2019, Stratified by Type of OAC Dispensed at the Index Date |
Table 1 shows the prevalences of selected medical conditions for new OAC users with index date in 2019 (results for new OAC users with index date in other years are shown in Supplementary Table 5a–e). Among new DOAC users, the proportion of patients with a history of ischemic stroke ranged from 8.1% (rivaroxaban) to 16.7% (dabigatran) and the proportion of patients with a history of TIA ranged from 4.7% (rivaroxaban and edoxaban) to 7.0% (dabigatran); for phenprocoumon, the proportions were 10.1% and 4.9%, respectively. Among new DOAC users, the prevalences of coronary heart disease, hypertension, congestive heart failure, vascular disease, diabetes mellitus and renal disease were all highest among new users of apixaban and lowest among new users of dabigatran (differences ranged between 3 and 7 percentage points). For phenprocoumon, the prevalences of these conditions exceeded those of new DOAC users (largest difference for renal disease). The prevalence of a history of major bleeding ranged between 20.0% (edoxaban) and 24.5% (dabigatran) among new DOAC users, while it was 34.9% among new phenprocoumon users. Regarding the use of drugs influencing the bleeding risk, the prevalences among new DOAC users varied by three percentage points or less, except for the prevalence of PPI use, which was lowest among new dabigatran users (29.8%) and highest among new apixaban users (33.9%). For most of the drugs, the prevalences among new phenprocoumon users were similar to those of new DOAC users, except for higher prevalences of antiplatelets and antiarrhythmic agents use. The median CHA2DS2VASc score was 4.0 points for all new OAC users except for rivaroxaban (3.0 points). The median HASBLED score was 3.0 points across all groups.
Stratification by year of index date showed that the number of new users (Figure 1) as well as the distribution of their risk profiles (Figures 2a and b) changed over time and the pattern partly differed between OACs. The number of new phenprocoumon users peaked in 2012 and decreased afterwards. The number of new apixaban and edoxaban users steadily increased after their market approvals for non-valvular atrial fibrillation (2012 and 2015, respectively). The number of new rivaroxaban users peaked between 2012 and 2014. The number of new dabigatran users was highest between 2012 and 2013 and decreased afterwards. The share of new phenprocoumon users among all new users decreased from 64% in 2012 to 5% in 2019. For rivaroxaban, the share was highest in 2013/14 (41%) and decreased to 21% in 2019. For dabigatran, the share was highest in 2011/12 (14%) and decreased to 3% in 2019. For apixaban, the share increased from 5% in 2013 to 51% in 2019, and for edoxaban, the share increased from 1% in 2015 to 21% in 2019.
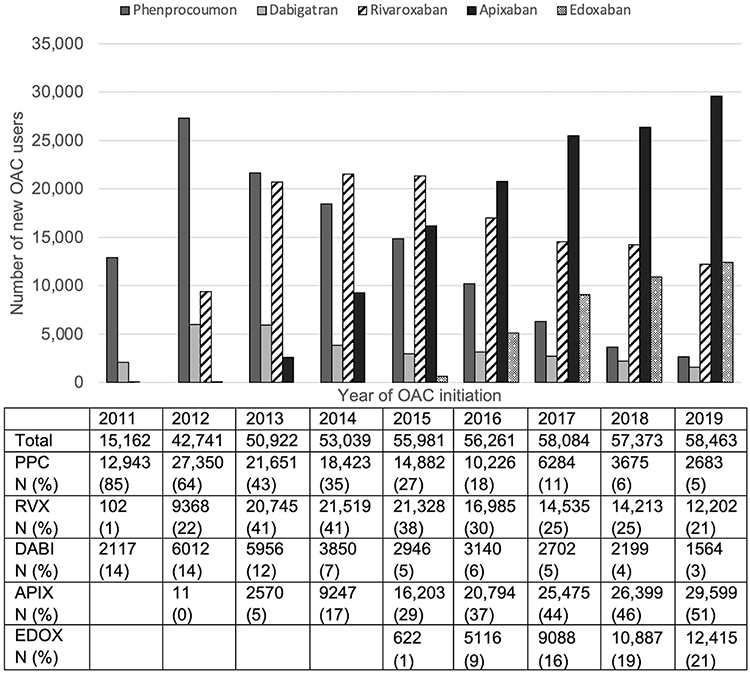 |
Figure 1 Number of new OAC users per year of treatment initiation. Year 2011 only includes data from August 2011 onwards (start of the study period). Abbreviations: PPC, phenprocoumon; RVX, rivaroxaban; DABI, dabigatran; APIX, apixaban, EDOX, edoxaban. |
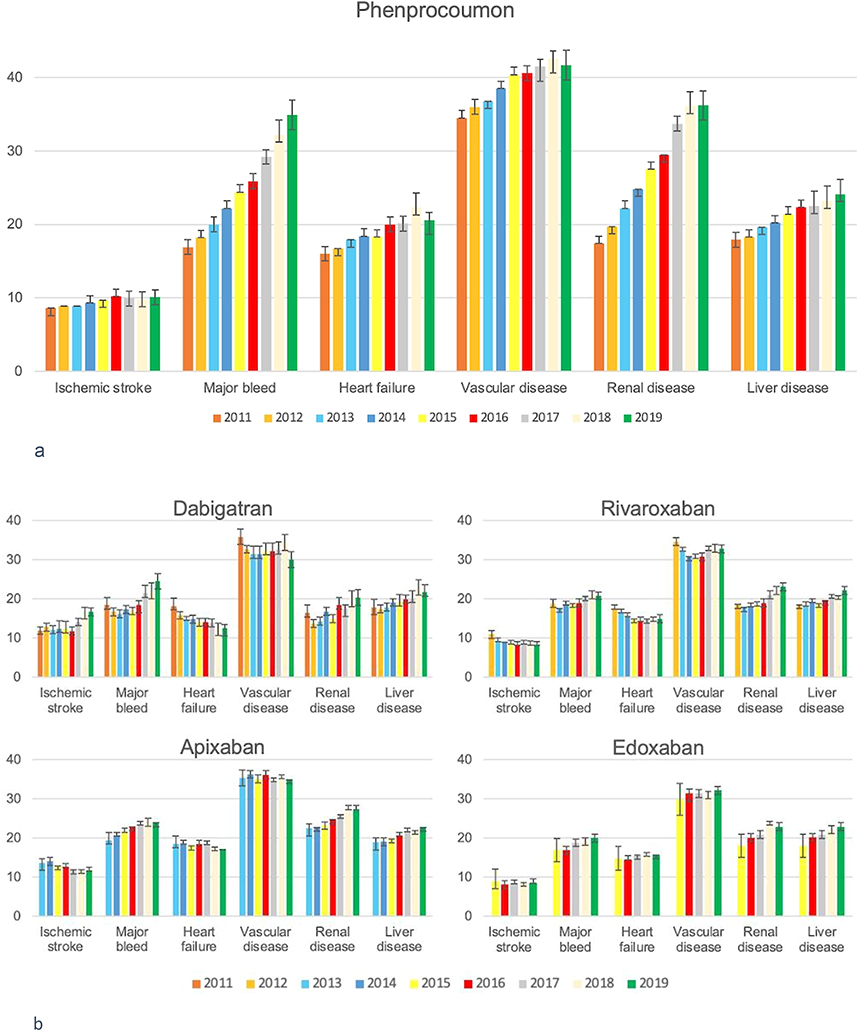 |
Figure 2 (a) Prevalence of selected medical conditions among new users of phenprocoumon stratified by year of index date. Year 2011 only includes data from August 2011 onwards (start of the study period). (b) Prevalence of selected medical conditions among new user of dabigatran, rivaroxaban, apixaban and edoxaban stratified by year of index date. Due to small sample size, the prevalences are partly shown for two years combined. This applies to rivaroxaban regarding the years 2011 and 2012 and to apixaban regarding the years 2012 and 2013. Year 2011 only includes data from August 2011 onwards (start of the study period). |
As shown in Figure 2a, among new phenprocoumon users, the prevalences of a history of ischemic stroke, a history of major bleeding, congestive heart failure, vascular disease, renal disease and liver disease increased between 2012 and 2019. This increase was most pronounced for the prevalence of a history of major bleeding (relative increase by 92%) and of renal disease (relative increase by 84%). We also observed changes in risk profiles among new DOAC users (Figure 2b). Between 2011 and 2019, the proportion with a history of ischemic stroke decreased for new users of rivaroxaban (from 10.9% to 8.1%) and apixaban (from 13.6% to 11.5%), it remained relatively stable for edoxaban (~9%), whereas it increased for dabigatran (from 11.9% to 16.7%). The proportion with a history of major bleeding increased among all new DOAC users (relative increases: dabigatran 33%, apixaban 23%, edoxaban 18%, rivaroxaban 11%). The proportion of new users with congestive heart failure decreased for dabigatran (from 18.2% to 12.5%) and rivaroxaban (from 17.4% to 14.9%), whereas it remained relatively stable for apixaban and edoxaban. The prevalence of vascular disease tended to decrease or remained stable, while the prevalences of liver disease and renal disease increased among new DOAC users between 2011 and 2019. Further details regarding changes in risk profiles of new OAC user can be found in the Supplementary Table 5a–e. In the sensitivity analyses restricting the look-back period for the assessment of comorbidities to “one year prior” to index date (rather than any time prior), the prevalences of comorbidities were lower as expected (Table 2) but the time trends concerning comorbidities were similar to the main analyses (Supplementary Table 6a–e).
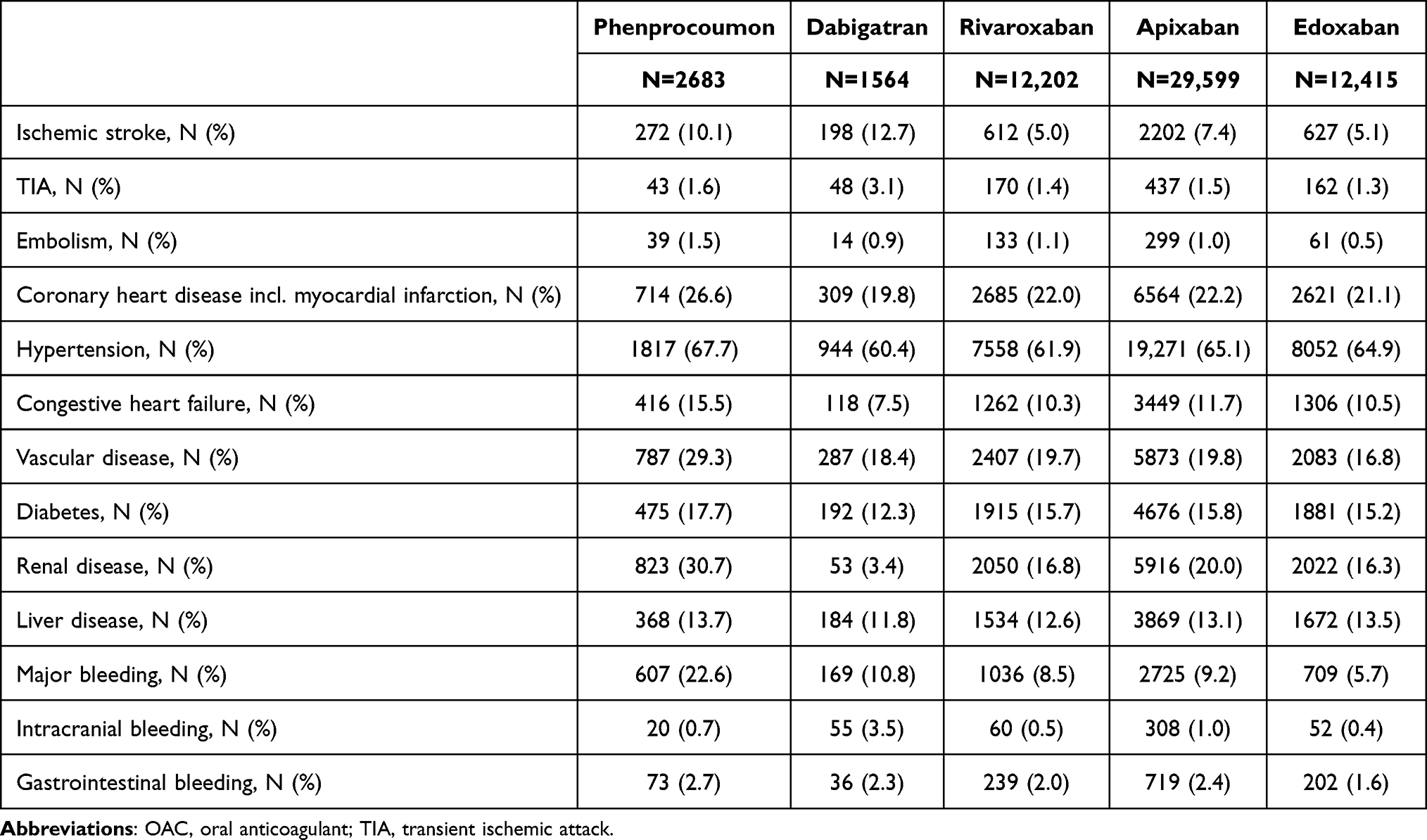 |
Table 2 Baseline Comorbidities of New OAC Users with Index Date in 2019. Here, Comorbidities Were Assessed Solely Based on Information from the Year prior to Index Date |
Discussion
This study including 448,028 patients with non-valvular atrial fibrillation initiating OAC treatment between August 2011 and December 2019 in Germany provides important insights into risk profiles of these patients, in particular regarding differences between new users of individual OACs as well as changes over time. Our findings clearly show that in 2019, new users of phenprocoumon were a highly selected group of patients (eg, highest prevalence of renal disease and a history of major bleeding), while in 2011/12, phenprocoumon was still the most commonly prescribed drug for the initiation of oral anticoagulation. The replacement of phenprocoumon by DOACs as the standard drug for treatment initiation between 2011 and 2019 was a rather dynamic process. Particularly the share of apixaban, but also of edoxaban steadily increased since their approval for the indication non-valvular atrial fibrillation. Even though the differences in risk profiles were most pronounced between new users of phenprocoumon and DOAC, there were also differences between new users of individual DOACs. In 2019, for example, new users of dabigatran showed the highest prevalence of ischemic stroke, TIA and major bleeding, while new users of apixaban showed the highest prevalence of renal disease, were older and more often female than new users of other DOACs.
Comparing our findings to data from other countries would be interesting, but to the best of our knowledge there has been no similar study so far. Some information—though not on time trends and mostly not on all DOACs investigated in our study—can be drawn from baseline characteristics of observational studies investigating the safety and effectiveness among new OAC users.23,24 For example, Halvorsen et al conducted a study based on a Scandinavian cohort including 219,545 patients with atrial fibrillation. They reported that apixaban and warfarin initiators were older and had higher CHA2DS2-VASc scores compared with dabigatran and rivaroxaban initiators.23 A study by Gupta et al based on US data described that warfarin initiators were older and their mean CHA2DS2-VASc score was significantly higher than among those initiating DOAC therapy.24 We recently conducted a study based on German and Dutch data, but it was restricted to new users of rivaroxaban, to data years until 2016/2017 and the definition of “new use” focused on rivaroxaban, ie, patients using VKAs before rivaroxaban treatment were also included.25 At least with respect to rivaroxaban, this study indicated that trends in risk profiles of users differ between countries, ie, the findings from our study may not be generalizable and applicable to other countries. It is also likely that shares of individual DOACs including their trends over time differ between countries given that they may not only be determined by current clinical guidelines. For example, it may also depend on whether or not there are differences in costs between DOACs. In Germany, there are differences but the system is complex, including potential variation on the regional level. Also, it may vary between countries whether the availability of new anticoagulants has increased the overall prevalence of anticoagulant use. Furthermore, differences in the health-care system may matter, eg, whether there is an obligatory health insurance and reimbursement of DOACs such as in Germany.
Still, there are clinical factors that could partly explain the patterns we observed. A decline in the share of phenprocoumon users among new OAC users was expected due to the increasing evidence on the effectiveness and safety of DOACs and their advantages in clinical practice. Nonetheless, the extent of this decline—in 2019 only 5% of patients initiating OACs were treated with phenprocoumon—is surprising in view of the contraindications of DOACs. The small group of new users treated with phenprocoumon in 2019 was highly selected with respect to contraindications of DOACs (renal disease) or other reasons for which a closer monitoring may be reasonable. The latter could also explain the higher proportion of patients with a history of major bleeding among phenprocoumon users. Physicians may prefer an anticoagulation monitoring in these patients. For dabigatran, an antidote has already been available since 2016. The availability of an antidote allowing to reverse anticoagulation in case of major bleeding or prior to intravenous thrombolysis in acute ischemic stroke26,27 could explain the higher prevalence of high-risk patients (ie, with a history of ischemic stroke, TIA or major bleeding) among new users of dabigatran compared to other DOAC users. Nonetheless, the share of dabigatran users among all new OAC users was low (<10%) from 2014 onwards even though it remained the only DOAC with an antidote through 2019. Thus, the availability of an antidote does not seem to be the key driver of treatment decisions.
The strongly increasing share of apixaban among new users during the study period could partly be explained by the fact that this is the only DOAC for which RCT showed superiority over VKAs (ie, not only non-inferiority).5 Indeed, the Drug Commission of the German Medical Association emphasizes this fact in its recommendation on the choice of drugs for oral anticoagulation treatment.28 However, this recommendation also emphasizes disadvantages of edoxaban (no antidote, decreasing effectiveness with increasing creatinine clearance), which is not reflected in our results. In 2019, one-fifth of new OAC users in our study were treated with edoxaban. Whether the dose regimen of edoxaban (once-daily) could explain this pattern is not clear, given that apixaban (twice-daily) was used even more often. Smits et al found out that adherence and persistence, which are essential for effective treatment, were higher in OAC users with once daily versus twice daily regimens in Germany.29 Also, the reasons for the higher proportion of women, the higher age and the higher prevalences of comorbidities among new users of apixaban in our study are not fully clear. In part, this might be due to specific knowledge on patient subgroups with frailty and a higher risk of falls from clinical trials. Whether the weight-based dosing of apixaban also impacts the prescribing behaviour would be interesting but we could not investigate this in our study.
Regardless of the reasons, it is important to note that there are differences in risk profiles between users of OACs. Observational studies play an important role in the comparison of effectiveness and safety between VKAs and DOACs or between different DOACs given the challenges to reach sufficient power in randomized trials for such comparisons. However, a key question is whether in observational studies adjustment for measured confounders can sufficiently balance the groups (ie, whether randomization can be emulated). Our findings suggest that new users of VKAs are very different from new users of DOACs, especially in more recent years, so there may be a high risk of residual confounding if these groups are compared. Even though differences in risk profiles between the users of different DOACs were less pronounced, it is also important to consider the potential impact of unmeasured confounding in studies comparing their effectiveness and safety. Interestingly, the findings of existing studies in this field were often not consistent,15,16 which may partly be due to this problem. When planning an observational study, eg, a direct head-to-head comparison of different DOACs, it would be important to identify further reasons that could explain treatment decisions. If the choice between DOACs was mainly driven by non-clinical factors (eg, discount rates for certain drugs), then unmeasured confounding (eg, by indication or contraindication) is less likely. Considering potential imbalance between groups is particularly relevant for the interpretation of existing meta-analyses comparing VKA and different DOACs, as they synthesize data from different countries and time periods. These questions will also be relevant for observational studies on new oral anticoagulants that may enter the market such as factor XIa inhibitors. As the aim of their development is to prevent thromboembolic events without increasing the risk of bleeding channelling bias could be of high relevance in such studies, but also potentially higher costs of newly developed drugs might influence treatment decisions.
A main strength of our study is the large database covering 20% of the German population. The data reflect routine clinical practice in Germany and they are free of non-responder and recall bias. As the database contains data from 2004 to 2019, there were several years of pre-observation to assess whether new users were actually naive to OAC treatment. Furthermore, we could assess time trends in the use of OACs over several years after the approval of the first DOAC in August 2011. Our study also has limitations. First, even though we used algorithms for the definition of comorbidities with a focus on high specificity, there may still be some misclassification due to the nature of claims data. We also used an algorithm for the indication “atrial fibrillation”. Given the strict data privacy regulations in Germany, a direct validation of this algorithm by linkage of claims data and medical records was not possible. However, we had the possibility to check plausibility by comparison to databases from other countries in the context of an international study by Komen et al.20 This comparison supported the plausibility of our case definition. Second, over-the-counter medication is not captured in claims data. Therefore, the use of low-dose acetylsalicylic acid (captured in antiplatelets) or NSAIDs may have been underestimated. Third, our study was merely descriptive, as such, it did not allow us to identify the reasons for differences in risk profiles. Fourth, it should be noted that the increase in the prevalence of morbidities among new DOAC users over time could partly be due to the study design. Our definition of new DOAC users did not include patients switching from VKAs to DOACs but only patients initiating DOAC who were naive to any oral anticoagulants. If these switchers had a higher morbidity and switching from VKAs to DOACs became less common over the years, then this selection mechanism would have led to a putative increase in the prevalence of morbidities among new DOAC users over the years.
In conclusion, our study demonstrated differences in risk profiles between new users of different OACs. Furthermore, there were substantial changes in risk profiles over time among new users of phenprocoumon. These differences have to be considered in head-to-head comparisons of these drugs based on observational data, especially regarding potential bias due to unmeasured confounding.
Ethics
The utilization of health insurance data for scientific research in Germany is regulated by the Code of Social Law. All involved health insurance providers as well as the German Federal (Social) Insurance Office and the Senator for Science, Health, and Consumer Protection in Bremen as their responsible authorities approved the use of GePaRD data for this study. Informed consent for studies based on claims data is required by law unless obtaining consent appears unacceptable and would bias results, which was the case in this study. According to the Ethics Committee of the University of Bremen studies based on GePaRD are exempt from institutional review board review. We thus complied with relevant data and privacy regulations.
Acknowledgment
The authors would like to thank all statutory health insurance providers which provided data for this study, namely AOK Bremen/Bremerhaven, DAK-Gesundheit, Die Techniker (TK), and hkk Krankenkasse. The authors would also like to thank Anja Gabbert and Philipp Alexander Volkmar for their support.
Disclosure
BK and UH are working at an independent, non-profit research institute, the Leibniz Institute for Prevention Research and Epidemiology – BIPS. AV, KP and UA were employees at BIPS at the time when the study was conducted. Unrelated to this study, BIPS occasionally conducts post-authorization safety studies (PASS) requested by health authorities which are financed by pharmaceutical industry and performed in line with the ENCePP Code of Conduct. The design and conduct of this study as well as the interpretation and publication are not influenced by the pharmaceutical industry. The authors report no other conflicts of interest in this work.
References
1. Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. 2021;16(2):217–221. doi:10.1177/1747493019897870
2. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955–962. doi:10.1016/S0140-6736(13)62343-0
3. Friberg L, Oldgren J. Efficacy and safety of non-vitamin K antagonist oral anticoagulants compared with warfarin in patients with atrial fibrillation. Open Heart. 2017;4(2):e000682. doi:10.1136/openhrt-2017-000682
4. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883–891. doi:10.1056/NEJMoa1009638
5. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981–992. doi:10.1056/NEJMoa1107039
6. Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093–2104. doi:10.1056/NEJMoa1310907
7. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139–1151. doi:10.1056/NEJMoa0905561
8. Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(38):2893–2962. doi:10.1093/eurheartj/ehw210
9. Ludwig W-D, Mühlbauer B, Seifert R. Antithrombotika und Antihämorrhagika [Antithrombotics and antihemorrhagics]. In: Arzneiverordnungs-Report 2021. Springer; 2021:299–326. German.
10. Menichelli D, Del Sole F, Di Rocco A, et al. Real-world safety and efficacy of direct oral anticoagulants in atrial fibrillation: a systematic review and meta-analysis of 605 771 patients. Eur Heart J Cardiovasc Pharmacother. 2021;7(FI1):f11–f19. doi:10.1093/ehjcvp/pvab002
11. Zhu W, Ye Z, Chen S, et al. Comparative effectiveness and safety of non–vitamin K antagonist oral anticoagulants in atrial fibrillation patients. Stroke. 2021;52(4):1225–1233. doi:10.1161/STROKEAHA.120.031007
12. Li G, Lip GY, Holbrook A, et al. Direct comparative effectiveness and safety between non-vitamin K antagonist oral anticoagulants for stroke prevention in nonvalvular atrial fibrillation: a systematic review and meta-analysis of observational studies. Eur J Epidemiol. 2019;34:173–190. doi:10.1007/s10654-018-0415-7
13. Laliberte F, Cloutier M, Nelson WW, et al. Real-world comparative effectiveness and safety of rivaroxaban and warfarin in nonvalvular atrial fibrillation patients. Curr Med Res Opin. 2014;30(7):1317–1325. doi:10.1185/03007995.2014.907140
14. Larsen TB, Skjøth F, Nielsen PB, Kjældgaard JN, Lip GYH. Comparative effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: propensity weighted nationwide cohort study. BMJ. 2016;353:i3189. doi:10.1136/bmj.i3189
15. Paschke LM, Klimke K, Altiner A, von Stillfried D, Schulz M. Comparing stroke prevention therapy of direct oral anticoagulants and vitamin K antagonists in patients with atrial fibrillation: a nationwide retrospective observational study. BMC Med. 2020;18(1):1–13. doi:10.1186/s12916-020-01695-7
16. Hohnloser SH, Basic E, Hohmann C, Nabauer M. Effectiveness and safety of non–vitamin K oral anticoagulants in comparison to phenprocoumon: data from 61,000 patients with atrial fibrillation. Thromb Haemost. 2018;118(03):526–538. doi:10.1160/TH17-10-0733
17. Hohnloser SH, Basic E, Nabauer M. Comparative risk of major bleeding with new oral anticoagulants (NOACs) and phenprocoumon in patients with atrial fibrillation: a post-marketing surveillance study. Clin Res Cardiol. 2017;106(8):618–628. doi:10.1007/s00392-017-1098-x
18. Jaksa A, Gibbs L, Kent S, et al. Using primary care data to assess comparative effectiveness and safety of apixaban and rivaroxaban in patients with nonvalvular atrial fibrillation in the UK: an observational cohort study. BMJ Open. 2022;12(10):e064662. doi:10.1136/bmjopen-2022-064662
19. Haug U, Schink T. German pharmacoepidemiological research database (GePaRD). In: Databases for Pharmacoepidemiological Research. Springer; 2021:119–124.
20. Komen JJ, Pottegård A, Mantel-Teeuwisse AK, et al. Persistence and adherence to non-vitamin K antagonist oral anticoagulant treatment in patients with atrial fibrillation across five Western European countries. EP Europace. 2021;23(11):1722–1730. doi:10.1093/europace/euab091
21. Lip GY, Frison L, Halperin JL, Lane DA. Identifying patients at high risk for stroke despite anticoagulation: a comparison of contemporary stroke risk stratification schemes in an anticoagulated atrial fibrillation cohort. Stroke. 2010;41(12):2731–2738. doi:10.1161/STROKEAHA.110.590257
22. Lip GY, Frison L, Halperin JL, Lane DA. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile INR, elderly, drugs/alcohol concomitantly) score. J Am Coll Cardiol. 2011;57(2):173–180. doi:10.1016/j.jacc.2010.09.024
23. Halvorsen S, Johnsen SP, Madsen M, et al. Effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in atrial fibrillation: a Scandinavian population-based cohort study. Eur Heart J Qual Care Clin Outcomes. 2022;8(5):577–587. doi:10.1093/ehjqcco/qcab048
24. Gupta K, Trocio J, Keshishian A, et al. Effectiveness and safety of direct oral anticoagulants compared to warfarin in treatment naïve non-valvular atrial fibrillation patients in the US Department of defense population. BMC Cardiovasc Disord. 2019;19(1):1–10. doi:10.1186/s12872-019-1116-1
25. Voss A, Smits E, Swart KM, et al. Time trends in patient characteristics of new rivaroxaban users with atrial fibrillation in Germany and the Netherlands. Drugs Real World Outcomes. 2023. doi:10.1007/s40801-022-00350-2
26. Berge E, Whiteley W, Audebert H, et al. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur Stroke J. 2021;6(1):I–LXII. doi:10.1177/2396987321989865
27. Schell M, Thomalla G. Intravenöse Lyse-Therapie beim ischämischen Schlaganfall–Schritt für Schritt. [Intravenous lysis therapy in ischemic stroke - step by step]. Neurologie up2date. 2020;3(4):329–336. German. doi:10.1055/a-1163-4712
28. Leitfaden der Arzneimittelkommission der deutschen Ärzteschaft (AkdÄ). “Orale Antikoagulation bei nicht valvulärem Vorhofflimmern”[Guidelines of the Drug Commission of the German Medical Association “Oral anticoagulation in non-valvular atrial fibrillation”]. Empfehlungen zum Einsatz der direkten oralen Antikoagulanzien Dabigatran (Pradaxa®), Apixaban (Eliquis®), Edoxaban (Lixiana®) und Rivaroxaban (Xarelto®). [Recommendations for the use of the direct oral anticoagulants dabigatran (Pradaxa®), apixaban (Eliquis®), edoxaban (Lixiana®) and Rivaroxaban (Xarelto®)]; 2019. German.
29. Smits E, Andreotti F, Houben E, et al. Adherence and persistence with once-daily vs twice-daily direct oral anticoagulants among patients with atrial fibrillation: real-world analyses from the Netherlands, Italy and Germany. Drugs Real World Outcomes. 2022; 2022:1–11. doi:10.1007/s40801-021-00289-w
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.