")
Back to Journals » International Journal of General Medicine » Volume 16
Risk of Thrombosis Following the First Dose of ChAdOx1 nCoV-19 Vaccine in Patients Undergoing Maintenance Hemodialysis: A Self-Controlled Case Series Study
Authors Shao SC , Liao TC, Chang KC, Chen HY, Lin SJ, Hsieh CY , Lai ECC
Received 13 May 2023
Accepted for publication 23 August 2023
Published 5 September 2023 Volume 2023:16 Pages 4017—4025
DOI https://doi.org/10.2147/IJGM.S418741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shih-Chieh Shao,1,2 Tzu-Chi Liao,1 Kai-Cheng Chang,1,3 Hui-Yu Chen,3 Swu-Jane Lin,4 Cheng-Yang Hsieh,1,5 Edward Chia-Cheng Lai1
1School of Pharmacy, Institute of Clinical Pharmacy and Pharmaceutical Sciences, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 2Department of Pharmacy, Keelung Chang Gung Memorial Hospital, Keelung, Taiwan; 3Department of Pharmacy, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan; 4Department of Pharmacy Systems, Outcomes and Policy, College of Pharmacy, University of Illinois at Chicago, Chicago, IL, USA; 5Department of Neurology, Tainan Sin Lau Hospital, Tainan, Taiwan
Correspondence: Cheng-Yang Hsieh, Department of Neurology, Tainan Sin Lau Hospital, 57, Section 1, Dongmen Road, East District, Tainan, 70142, Taiwan, Tel +886-6-274-8316, Ext 4180, Fax +886-6-282-4178, Email [email protected]
Background: The ChAdOx1 nCoV-19 vaccine is associated with vaccine-induced thrombosis and thrombocytopenia (VITT). Patients with end-stage renal disease (ESRD) under hemodialysis are at elevated risk of heparin-induced thrombocytopenia, which shares similar mechanisms with VITT. We aimed to examine the risk of VITT after the first dose of ChAdOx1 nCoV-19 vaccine using a self-controlled case series analysis (SCCS) in the hemodialyzed ESRD population.
Methods: Drawing from the largest multi-center electronic medical records database in Taiwan, we identified adult patients, with or without hemodialysis, between 1st December, 2020, and 31st December, 2021, who received a first dose of ChAdOx1 nCoV-19 vaccine and had an outcome of thrombocytopenia, venous thrombosis, or arterial thrombosis. We calculated the incident rate ratios (IRRs) of outcomes in different periods at risk, compared to periods not at risk.
Results: We identified 59 hemodialysis patients and 41 non-dialysis patients with an outcome. The SCCS analyses showed, for the hemodialysis group, a significantly increased risk of outcomes during the period 31 to 60 days post-exposure to ChAdOx1 nCoV-19 vaccine (IRR: 2.823; 95% CI: 1.423– 5.600). However, in non-dialysis patients there was no increase in risks during any of the post-exposure risk periods.
Conclusion: For ESRD patients under hemodialysis, the first dose of ChAdOx1 nCoV-19 vaccine was associated with a 2.8-fold increase in risk of thrombosis.
Keywords: thrombosis, thrombocytopenia, ChAdOx1 nCoV-19 vaccine, hemodialysis, end-stage renal disease
Introduction
Due to their advanced age and multiple medical comorbidities, patients with end-stage renal disease (ESRD) are at a higher risk of death when they contract coronavirus disease 2019 (COVID-19).1 The prevalence of ESRD necessitating dialysis in Taiwan is the highest of any country in the world.2 While hemodialysis is the predominant modality for renal replacement therapy, patients receiving periodic in-hospital hemodialysis are particularly susceptible to infection with severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2).3 Therefore, ESRD patients were given top priority in Taiwan’s nationwide COVID-19 vaccination program.4 As of 1st July 2021, more than 80% of Taiwanese patients with ESRD had received their first dose of ChAdOx1 nCoV-19 (Oxford-AstraZeneca) vaccine, which was largely the only COVID-19 vaccine available to the nationwide vaccination program before 30th June 2021.5,6
The ChAdOx1 nCoV-19 vaccine is a non-replicating adenoviral vector vaccine.7 Its use is correlated with an infrequent yet serious adverse reaction of vaccine-induced thrombosis with thrombocytopenia (VITT).8 The possible mechanism involves the triggering of immune responses to platelet factor-4 (PF4), the production of anti-PF4 autoantibodies and the subsequent activation of platelet-derived coagulation cascades.8,9 VITT shares many of the same characteristics as heparin-induced thrombocytopenia (HIT), which is thought to be brought on by the immune system’s response to heparin and the presence of anti-PF4 antibody.9
The prevalence of positive anti-PF4 antibody in the general population is between 1.0% and 6.6%10,11 During their maintenance hemodialysis sessions, ESRD patients are exposed to heparin on a regular basis. As a result, one in three tests positive for anti-PF4 antibody,10,11 and approximately 12% of dialysis patients may develop HIT resulting from prolonged exposure to heparin.12 Previous investigations have revealed that anti-PF4 antibody is related to arterial stiffness13 and thrombotic occurrences like myocardial infarction or ischemic stroke in the hemodialysis population.14 Given such a high prevalence rate of anti-PF4 antibody, as well as the pre-existing higher risks of venous or arterial thrombosis events,15,16 it was uncertain whether there would be any further increase in thrombosis risk for hemodialyzed ESRD patients after receiving the ChAdOx1 nCoV-19 vaccine. Therefore, we performed this self-controlled case series study using a large hospital-based database to examine the relationship between exposure to the first dose of ChAdOx1 nCoV-19 vaccine and thrombosis events in hemodialyzed ESRD patients in Taiwan.
Methods
Data Sources
The Chang Gung Research Database (CGRD) was used as the data source for this study. A comprehensive description of the CGRD’s data structure can be found in prior literature.17,18 Briefly, the CGRD consists of the collective digital medical records of nine Chang Gung Medical Foundation (CGMF) hospital branches throughout Taiwan, covering an estimated 1.3 million people (or 6% of the total Taiwanese population). The CGRD encompasses information on demographic data, visits to the emergency department, outpatient services, hospitalizations, laboratory tests and medications, making it a valuable source for clinical and pharmacoepidemiologic research.19,20
Study Design
A self-controlled case series approach was used in this study. This method was originally designed to assess the risk of adverse reactions related to vaccinations.21,22 Using this approach, we calculated the risk of outcomes of interest during the post-vaccination exposure period, relative to that during the unexposed baseline period (Figure 1). Statistical inference was made at the level of study subjects, so that factors that stayed the same throughout the study duration (eg, gender, genetics, socioeconomic status, individual frailty, the severity of existing conditions) were held constant. The Institutional Review Board of CGMF approved the protocol of the present study (ID: 202101087B0) and waived the requirement for informed consent.
 |
Figure 1 Schematic illustration of the study design. |
Inclusion and Exclusion Criteria
Adult patients ≥18 years old with ESRD and receiving chronic maintenance hemodialysis, who received a first dose of the ChAdOx1 nCoV-19 vaccine and subsequently suffered a thrombosis event within the study period (from 1st December 2020, to 31st December 2021), were identified from the CGRD. Patients who had received hemodialysis for at least three consecutive months were considered to be under chronic maintenance hemodialysis. The National Health Insurance codes for dialysis procedures in Taiwan are detailed in Supplementary Table 1. We confirmed the vaccination status for COVID-19 using prescription data. We excluded patients receiving the mRNA-1273 (Moderna) or BNT162b2 vaccines, because very few patients with ESRD had received either of these as their first-dose vaccination against COVID-19 during the study period. We excluded prevalent cases with thrombosis events if the same event occurred in the year prior to the beginning of the study period (ie, from 1st December 2019, to 30th November 2020). Patients who had received a second dose of ChAdOx1 nCoV-19 vaccine before the occurrence of a thrombosis event were also excluded, as the focus of the study was on the effects of the first dose. Finally, we excluded patients diagnosed with SARS-CoV-2 infections before the occurrence of a thrombosis event, since SARS-CoV-2 itself could be a cause of thrombosis.23,24 Throughout the study period, the Taiwanese government maintained a strict infection control strategy. Nasal swab polymerase chain reaction (PCR) tests performed by qualified healthcare workers were required to confirm all COVID-19 positive results. It was mandatory for physicians to immediately report the relevant ICD-10 code (i.e., U071) for patients with positive PCR results to the National Health Insurance and Center for Disease Control.
Exposure Risk Period
We defined the periods at risk using the following pre-specified time periods: 0–5, 6–30, 31–60 and 61–120 days after the vaccination date (Figure 1). Using these multiple risk intervals, a distinction could be made between acute and non-acute phases, in terms of thrombosis risk after vaccination. The period not at risk was defined as the time between 1st December 2020, and 31 days prior to the ChAdOx1 nCoV-19 vaccination date, and from 121 days after ChAdOx1 nCoV-19 vaccination until 31st December 2021. We also defined the 30-day interval before the date of ChAdOx1 nCoV-19 vaccination as the baseline period. This was to address the potential bias which could arise if the outcome event momentarily changed the probability of ChAdOx1 nCoV-19 vaccination. Supplementary Figure 1 presents the data distribution for the day intervals between vaccination and event occurrence.
Study Outcome
Our primary outcome was a composite of thrombocytopenia, venous thromboembolism or arterial thromboembolism, which we identified using inpatient discharge diagnosis codes. Hospitalizations were identified from the CGRD between 1st December 2020, and 31st December 2021, based on International Classification of Diseases, 10th version, Clinical Modification (ICD-10-CM) codes in the first 5 columns of diagnostics that indicated the primary outcome. We present the details of these ICD-10-CM codes for study outcomes in Supplementary Table 2. We defined the admission date of hospitalization for the primary outcome as the event date. The sensitivity and positive predictive value of ICD-10-CM codes for venous or arterial thromboembolism in Taiwan have been validated previously.25–27
Statistical Analysis
We used descriptive statistics to present the characteristics of the study cohort (ESRD patients under maintenance hemodialysis who received a first dose of ChAdOx1 nCoV-19 vaccine and subsequently recorded the study outcome of interest) in terms of age, sex, comorbidities and laboratory data during the baseline period. A self-controlled case series model was fitted using conditional Poisson regression. We calculated the incident rates, incident rate ratios and 95% confidence intervals of the study outcome for different risk periods, compared to periods not at risk. To confirm the validity of this study, the following additional analyses were conducted. First, we selected bone fracture as a negative control event, and applied the same self-controlled case series model to test the robustness of our study. Since bone fracture should be unrelated to vaccination, there should be no correlation between vaccination and bone fracture outcomes. The ICD-10-CM codes for bone fracture are also listed in Supplementary Table 2. Second, given the critical nature of thrombosis in hemodialysis patients, we performed the same analysis for thrombosis events in the general population not receiving any form of dialysis. We expected the correlation between vaccination and thrombosis outcome to be either non- or barely significant in the general population. All statistics were conducted using SAS 9.4 for Windows (SAS Institute, Inc., Cary, NC). Two-tailed p-values < 0.05 were regarded as statistically significant.
Results
Between 1st December 2020, and 31st December 2021, 242 adult patients received their first dose of vaccine for COVID-19 and subsequently experienced a thrombosis event. Following our inclusion and exclusion criteria, a total of 59 patients were eligible for the main analysis (Figure 2).
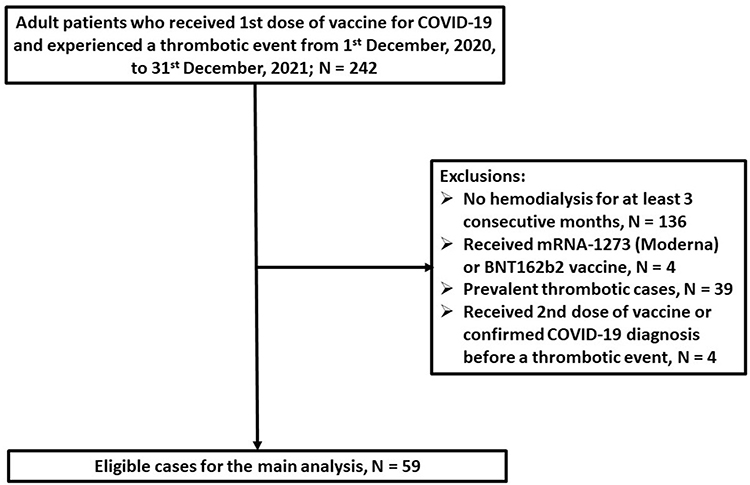 |
Figure 2 Flow chart for selection of cases for the main analysis. |
Table 1 outlines the baseline demographics and characteristics of the 59 patients. The patients’ mean age was 65 years old, 39% were female, 75% were living in northern locations and their mean platelet count was 198 x103/μL during the baseline period. Supplementary Figure 1 illustrates the distribution of day intervals between vaccination and event occurrence in these patients. At around 30 days post-vaccination, there was a surge in thrombosis events. Table 2 shows the results of the self-controlled case series analysis. The incident rate ratio (IRR) significantly increased during the 31- to 60-days post-vaccination risk period, compared to periods not at risk. There were 33 bone fracture events for the negative control analysis; however, as shown in Table 3, the first dose of ChAdOx1 nCoV-19 vaccine was not associated with this outcome during any of the risk intervals. Finally, a first dose of the ChAdOx1 nCoV-19 vaccine was not associated with thrombosis events in any of the risk intervals in the non-dialysis population (Table 4).
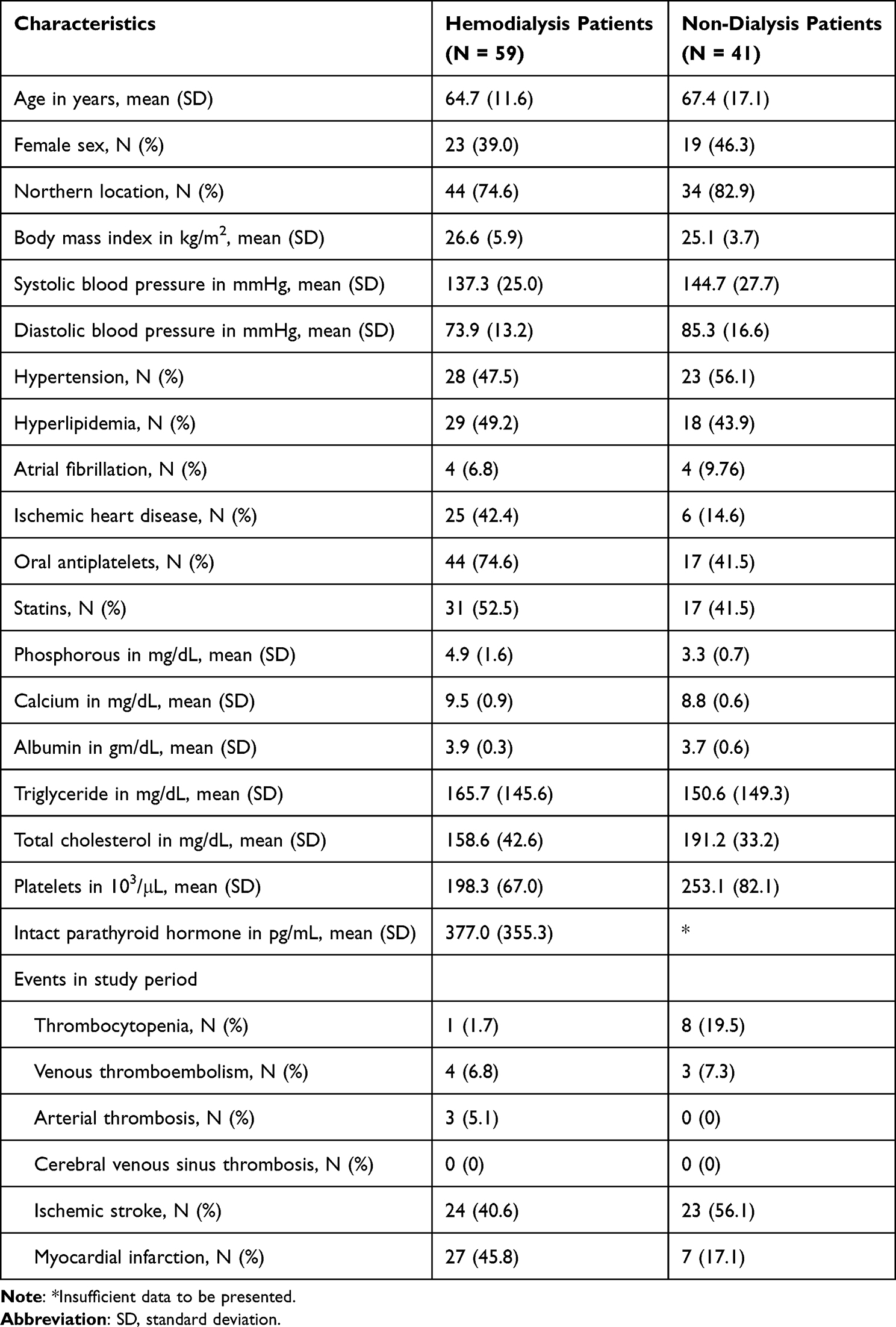 |
Table 1 Baseline Demographics of Cases Selected for the Self-Controlled Case Series Analysis |
 |
Table 2 Incident Rate and IRR of Thrombosis Events in Each Risk Period Compared to Periods Not at Risk for ESRD Patients Receiving Chronic Maintenance Hemodialysis (Total N = 59) |
 |
Table 3 Incident Rate and IRR of Bone Fracture Events in Each Risk Period, Compared to Periods Not at Risk for ESRD Patients Receiving Chronic Maintenance Hemodialysis (Total N = 83) |
 |
Table 4 Incident Rate and IRR of Thrombosis Events in Each Risk Period, Compared to Periods Not at Risk for the Non-Dialysis Population (Total N = 41) |
Discussion
We found that for ESRD patients under chronic maintenance hemodialysis, the first dose of ChAdOx1 nCoV-19 vaccine was significantly associated with a 2.8-fold increase in risk of thrombosis events during the period 31 to 60 days after vaccination, compared to periods not at risk. The ChAdOx1 nCoV-19 vaccine was not associated with an increased risk of bone fracture during any of the post-exposure periods in hemodialysis patients, and it was not associated with thrombosis events in the non-dialysis population either.
Although there is extensive literature addressing the occurrence of VITT after exposure to the ChAdOx1 nCoV-19 vaccine, very little of it specifically focuses on the ESRD population. In a small single-center study,5 the incident rate of vascular access thrombosis was 0.011 per person-month within 30 days after receiving the first dose of ChA-dOx1 nCoV-19 vaccine. This was numerically higher than the rate during the 3 months (0.006 per person-month) before vaccine exposure, though a self-controlled case series analysis failed to show a significant difference, probably due to small event numbers (5 and 3 events before and after the exposure, respectively) leading to insufficient statistical power. By contrast, our multi-center study covered a much larger number of events and detected a higher risk of thrombosis at 31 to 60 days after ChAdOx1 nCoV-19 vaccination, using self-controlled case series analysis.
Typically, a VITT is characterized by thrombocytopenia, thrombosis event, elevated D-dimer level and the presence of high-avidity IgG anti-PF4 antibodies, within 6–30 days following exposure to an adenoviral vector vaccine like ChAdOx1 nCoV-19.8,9 PF4, a positively charged chemokine, is emitted from the α-granules of activated platelets as an immune defense mechanism. It can opsonize the negatively charged surfaces of bacteria, thereby promoting the binding of anti-PF4 antibodies.8 In HIT, heparin, acting as a polyanion, causes a transformation of PF4 tetramers and leads to the induction of anti-PF4/heparin antibody, which, in turn, activates platelets via the FcγRIIa receptor for the Fc domain of IgG antibodies.9 The ensuing release of platelet-derived procoagulant microvesicles leads to severe thrombocytopenia, disseminated intravascular coagulation and thrombosis events at atypical sites.8 It has been hypothesized that, as in the case of HIT, the binding of PF4 and capsid proteins from the adenoviral vectors of the ChAdOx1 nCoV-19 vaccine induces the formation of anti-PF4 antibodies and subsequent thrombocytopenia and thrombosis responses in VITT.8,9
Because of their regular exposure to heparin during each regular hemodialysis session, 33.8% to 35.7% of ESRD patients receiving chronic maintenance hemodialysis have tested positive for anti-PF4 antibodies.13,14 The pre-existing B-cell clones for the production of anti-PF4 antibodies may partly explain the increased risk of thrombosis events observed in the present study, owing to the shared pathophysiological mechanisms between VITT and HIT. However, the increased risk occurred during the period 31 to 60 days post-exposure, not the period 6 to 30 days post-exposure, as seen in a typical VITT.13,14 It would seem more logical to observe a faster response in the ESRD population, since they are already “primed” by having anti-PF4 antibodies. Furthermore, thrombocytopenia is under-represented in our patients as an event of interest. A delayed mechanism other than anti-PF4 antibodies might be responsible for our findings and this warrants further investigation.
We used bone fracture events as a negative control, and as expected, the ChAdOx1 nCoV-19 vaccine was not associated with risks of bone fracture. Finally, we found that, in the non-dialysis population, the ChAdOx1 nCoV-19 vaccine was not associated with thrombosis risks during any of the post-exposure risk periods. Such a non-significant finding may be explained by so-called notoriety bias.28 That is, the launch and implementation of the nationwide vaccination program in Taiwan were delayed as late as May 2021 (coinciding with the second wave of community outbreak of COVID-19). At that time, the risk of thrombosis had been fully publicized in the media. We speculated that patients who were at higher risk of VITT (eg, the younger age group [19 to 39 years]29,30 may have turned down adenoviral vector vaccine and preferred to wait for the mRNA vaccines, which were to become available just a few months later in Taiwan at that time. Notably, our non-dialysis patients with thrombosis events were much older (mean age: 67.4 years) (Table 1), compared to those reported in the literature (mean age: 50.1 years).29
Our study had several limitations. First, we may not have been able to confirm that subsequent exposures were not affected by previous events, which may have influenced the estimation by self-controlled case series. However, such an influence would have applied equally to the analysis of the dialysis and non-dialysis population. Second, although the codes we used to define thrombosis and thrombocytopenia were in accordance with prior literature,28 we did not follow the stricter definition of VITT (eg, as described by Pavord et al).31 We were unable to adopt those definitions because diagnostic items for VITT, such as anti-PF4 antibody or D-dimer, were not routinely checked in our patients. Third, due to small event numbers, we could not perform additional analysis of thrombosis risks among ESRD patients receiving peritoneal dialysis, or the effect of mRNA vaccines on thrombosis risks. Finally, IRRs in different risk periods (Table 2) had wide and overlapping 95% confidence intervals. These could be due to the ethnicity or specific underlying risk factors that are more prevalent in the Taiwanese ESRD population. Our results should be interpreted with caution and verified by future studies targeting a wider geographical range.
Conclusions
For ESRD patients under chronic maintenance hemodialysis, the administration of the first dose of ChAdOx1 nCoV-19 vaccine was associated with a 2.8-fold increase in the risk of thrombosis events during the period 31 to 60 days after exposure. Our results indicate that adequate monitoring and prevention of adverse reactions are especially needed among vulnerable populations like ESRD patients, when administering adenoviral vector type vaccines.
Data Sharing Statement
Access to the analyzed electronic medical records data requires official approval from the CGMF. Due to data privacy and safety concerns, all analyses must be conducted onsite at the CGMF, and no individual-level data are permitted to be taken out. However, the analytical codes of the SAS software used in this study are available from the first (SCS) or corresponding author (CYH) upon reasonable request.
Ethics Approval
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of CGMF (ID: 202101087B0). The requirement for informed consent was waived due to the retrospective design.
Acknowledgments
This study is based in part on data from the CGRD provided by CGMF. The interpretation and conclusions contained herein do not represent the position of CGMF. The authors also thank Mr Stuart Neff, MSTCM for English language editing.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
This research was funded by Tainan Sin Lau Hospital, under grant number SLH-111-07. The funder had no part in this study, including study design and conduct, data collection, management, analysis and interpretation, manuscript preparation, review and approval, and decision to publish.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Salerno S, Messana JM, Gremel GW, et al. COVID-19 risk factors and mortality outcomes among medicare patients receiving long-term dialysis. JAMA Netw Open. 2021;4:e2135379. doi:10.1001/jamanetworkopen.2021.35379
2. Lai TS, Hsu CC, Lin MH, Wu VC, Chen YM. Trends in the incidence and prevalence of end-stage kidney disease requiring dialysis in Taiwan: 2010–2018. J Formos Med Assoc. 2022;121:S5–S11. doi:10.1016/j.jfma.2021.12.013
3. Lee JJ, Lin CY, Chiu YW, Hwang SJ. Take proactive measures for the pandemic COVID-19 infection in the dialysis facilities. J Formos Med Assoc. 2020;119:895–897. doi:10.1016/j.jfma.2020.03.022
4. Yen CC, Lin SY, Chen SC, Chiu YW, Chang JM, Hwang SJ. COVID-19 vaccines in patients with maintenance hemodialysis. J Pers Med. 2021;11:789. doi:10.3390/jpm11080789
5. Yang IN, Lu CL, Tang HJ, et al. Safety of ChAdOx1 NCoV-19 vaccination in patients with end-stage renal disease on hemodialysis. PLoS One. 2022;17:e0273676. doi:10.1371/journal.pone.0273676
6. Chen CY, Ye JJ, Huang TS, et al. Effective preventive strategies to prevent secondary transmission of COVID-19 in hemodialysis unit: the first month of community outbreak in Taiwan. Healthcare. 2021;9:1173. doi:10.3390/healthcare9091173
7. Voysey M, Clemens SAC, Madhi SA, et al. Safety and efficacy of the ChAdOx1 NCoV-19 Vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised Controlled Trials in Brazil, South Africa, and the UK. Lancet. 2021;397:99–111. doi:10.1016/s0140-6736(20)32661-1
8. Michele MD, Kahan J, Berto I, et al. Cerebrovascular Complications of COVID-19 and COVID-19 Vaccination. Circ Res. 2022;130:1187–1203. doi:10.1161/circresaha.122.319954
9. Buoninfante A, Andeweg A, Baker AT, et al. Understanding Thrombosis with Thrombocytopenia Syndrome after COVID-19 Vaccination. NPJ Vaccines. 2022;7:141. doi:10.1038/s41541-022-00569-8
10. Hursting MJ, Pai PJ, McCracken JE, et al. Platelet Factor 4/heparin antibodies in blood bank donors. Am J Clin Pathol. 2010;134:774–780. doi:10.1309/ajcpg0mnr5ngknfx
11. Arepally GM, Hursting MJ. Platelet Factor 4/Heparin Antibody (IgG/M/A) in healthy subjects: a literature analysis of commercial immunoassay results. J Thromb Thrombolysis. 2008;26:55–61. doi:10.1007/s11239-008-0217-y
12. Lin YL, Lin CY, Liu JH. Vaccine-Induced immune thrombotic thrombocytopenia presenting as a mimic of heparin-induced thrombocytopenia in a hemodialysis patient receiving ChAdOx1 NCoV-19 vaccine. Ren Fail. 2022;44:1131–1134. doi:10.1080/0886022x.2022.2098772
13. Kuo C, Tsai CC, Chen CA, Tsai YF, Chen YH. Anti-platelet factor 4/heparin antibody plays a significant role in progression of arterial stiffness among hemodialysis patients. Acta Cardiol Sin. 2017;33:188–194. doi:10.6515/acs20160818b
14. Liu CC, Chou LP, Chen TS, Chen CA, Tsai YF. Significant association of anti-platelet factor 4/heparin antibody with cardiovascular disease in hemodialysis patients: a longitudinal 7-year study. Int Urol Nephrol. 2018;50:2289–2297. doi:10.1007/s11255-018-2002-y
15. Lu HY, Liao KM. Increased risk of deep vein thrombosis in end-stage renal disease patients. BMC Nephrol. 2018;19:204. doi:10.1186/s12882-018-0989-z
16. Ocak G, Vossen C, Rotmans J, et al. Venous and arterial thrombosis in dialysis patients. Thromb Haemost. 2011;106:1046–1052. doi:10.1160/th11-06-0422
17. Tsai MS, Lin MH, Lee CP, et al. Chang gung research database: a multi-institutional database consisting of original medical records. Biomed J. 2017;40:263–269. doi:10.1016/j.bj.2017.08.002
18. Shao S, Lai EC, Huang T, et al. The chang gung research database: multi‐institutional real‐world data source for traditional Chinese medicine in Taiwan. Pharmacoepidem Drug Safe. 2021;30:652–660. doi:10.1002/pds.5208
19. Shao SC, Su YC, Lai ECC, et al. Association between sodium glucose co-transporter 2 inhibitors and incident glaucoma in patients with type 2 diabetes: a multi-institutional cohort study in Taiwan. Diabetes Metab. 2022;48:101318. doi:10.1016/j.diabet.2022.101318
20. Su YC, Hung JH, Chang KC, et al. Comparison of sodium-glucose cotransporter 2 inhibitors vs glucagonlike peptide-1 receptor agonists and incidence of dry eye disease in patients with type 2 diabetes in Taiwan. JAMA Netw Open. 2022;5:e2232584. doi:10.1001/jamanetworkopen.2022.32584
21. Petersen I, Douglas I, Whitaker H. Self controlled case series methods: an alternative to standard epidemiological study designs. BMJ. 2016;354:i4515. doi:10.1136/bmj.i4515
22. Yen CC, Wei KC, Wang WH, Huang YT, Chang YC. Risk of guillain-barré syndrome among older adults receiving influenza vaccine in Taiwan. JAMA Netw Open. 2022;5:e2232571. doi:10.1001/jamanetworkopen.2022.32571
23. Snell J. SARS-CoV-2 infection and its association with thrombosis and ischemic stroke: a review. Am J Emerg Medicine. 2021;40:188–192. doi:10.1016/j.ajem.2020.09.072
24. Gorog DA, Storey RF, Gurbel PA, et al. Current and novel biomarkers of thrombotic risk in COVID-19: a consensus statement from the international COVID-19 thrombosis biomarkers colloquium. Nat Rev Cardiol. 2022;19:475–495. doi:10.1038/s41569-021-00665-7
25. Hsieh MT, Hsieh CY, Tsai TT, Wang YC, Sung SF. Performance of ICD-10-CM diagnosis codes for identifying acute ischemic stroke in a national health insurance claims database. Clin Epidemiol. 2020;12:1007–1013. doi:10.2147/clep.s273853
26. Hsieh MT, Hsieh CY, Tsai TT, Sung SF. Validation of stroke risk factors in patients with acute ischemic stroke, transient ischemic attack, or intracerebral hemorrhage on Taiwan’s national health insurance claims data. Clin Epidemiol. 2022;14:327–335. doi:10.2147/clep.s353435
27. Liao SC, Shao SC, Lai ECC, Lin SJ, Huang WI, Hsieh CY. Positive predictive value of ICD-10 codes for cerebral venous sinus thrombosis in Taiwan’s national health insurance claims database. Clin Epidemiol. 2022;14:1–7. doi:10.2147/clep.s335517
28. Hippisley-Cox J, Patone M, Mei XW, et al. Risk of thrombocytopenia and thromboembolism after covid-19 Vaccination and SARS-CoV-2 positive testing: self-controlled case series study. BMJ. 2021;374(1931). doi:10.1136/bmj.n1931
29. Higgins H, Andrews N, Stowe J, et al. Risk of thrombosis with thrombocytopenia syndrome after COVID‐19 vaccination prior to the recognition of vaccine‐induced thrombocytopenia and thrombosis: a self‐controlled case series study in England. Res Pract Thromb Haemost. 2022;6:e12698. doi:10.1002/rth2.12698
30. Krzywicka K, Munckhof A, Kammen MS, et al. Age-stratified risk of cerebral venous sinus thrombosis after SARS-CoV-2 vaccination. Neurology. 2022;98:e759–e768. doi:10.1212/wnl.0000000000013148
31. Pavord S, Scully M, Hunt BJ, et al. Clinical features of vaccine-induced immune thrombocytopenia and thrombosis. New Engl J Med. 2021;385:1680–1689. doi:10.1056/nejmoa2109908
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.