Back to Journals » Journal of Inflammation Research » Volume 19
Risk Factors of Postoperative Residual Sinus Inflammation in Patients with Eosinophilic Chronic Rhinosinusitis and Nasal Polyps
Authors Wu PW ![]() , Chang PH
, Chang PH ![]() , Huang CC
, Huang CC ![]() , Yen CI
, Yen CI ![]() , Fan YH, Huang CC
, Fan YH, Huang CC ![]()
Received 30 October 2025
Accepted for publication 6 December 2025
Published 8 January 2026 Volume 2026:19 576040
DOI https://doi.org/10.2147/JIR.S576040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tara Strutt
Pei-Wen Wu,1– 3 Po-Hung Chang,1 Chi-Che Huang,1,2 Cheng-I Yen,4 Yu-Hsi Fan,1 Chien-Chia Huang1– 3
1Division of Rhinology, Department of Otolaryngology, Chang Gung Memorial Hospital and Chang Gung University, Taoyuan, Taiwan; 2School of Medicine, Chang Gung University, Taoyuan, Taiwan; 3Molecular Infectious Disease Research Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan; 4Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital and Chang Gung University, College of Medicine, Taoyuan, Taiwan
Correspondence: Chien-Chia Huang, Division of Rhinology, Department of Otolaryngology, Chang Gung Memorial Hospital and Chang Gung University, No. 5, Fu-Shin Street, Kweishan, Taoyuan, 333, Taiwan, Tel +886-3-3281200 ext. 8466, Fax +886-3-3979361, Email [email protected]
Purpose: The combination of surgery and biologics may be required for patients with severe eosinophilic chronic rhinosinusitis with nasal polyps (CRSwNP) and a high inflammatory burden. This study aimed to identify the risk factors for postoperative residual sinus inflammation in patients with eosinophilic CRSwNP.
Methods: Adult patients with bilateral CRSwNP planning to undergo endoscopic sinus surgery were prospectively recruited. Their clinical information, computed tomography images, and tissue eosinophil count were evaluated. Postoperative residual mucosal inflammation was defined as a modified Lund-Kennedy endoscopy score of ≥ 5 at three months postoperatively.
Results: The study included 143 adult patients with bilateral CRSwNP. Ninety-three patients (65.0%) had eosinophilic CRSwNP based on tissue eosinophil counts of ≥ 10/high power field. Twenty-six patients (28.0%) with eosinophilic CRSwNP experienced postoperative residual sinus inflammation. The prevalence of comorbid asthma, nasal polyp score, Lund-Mackay score, ethmoid/maxillary ratio, olfactory cleft opacification score on computed tomography images, serum eosinophil cationic protein level, and tissue eosinophil count were significantly higher in the patients with than in those without postoperative residual sinus inflammation (all p< 0.05). A nomogram was constructed to predict the probability of experiencing post-op residual sinus inflammation.
Conclusion: Comorbid asthma, nasal polyp score, Lund–Mackay score, ethmoid/maxillary ratio, and olfactory cleft opacification score are significant predictors of postoperative residual sinus inflammation in patients with eosinophilic CRSwNP. Clinicians can use a nomogram based on these factors to predict therapeutic outcomes after sinus surgery and the need for postoperative adjuvant therapy such as biologics.
Plain Language Summary: The combination of surgery and biologics may be required for patients with severe eosinophilic chronic rhinosinusitis with nasal polyps (CRSwNP) and a high inflammatory burden. This study included 143 adult patients with bilateral CRSwNP. Ninety-three patients (65.0%) had eosinophilic CRSwNP. Comorbid asthma, nasal polyp score, Lund–Mackay score, ethmoid/maxillary ratio, and olfactory cleft opacification score are significant predictors of postoperative residual sinus inflammation in patients with eosinophilic CRSwNP. Clinicians can use a nomogram based on these factors to predict therapeutic outcomes after sinus surgery and the need for postoperative adjuvant therapy such as biologics.
Keywords: chronic rhinosinusitis, eosinophil, endoscopic sinus surgery, Lund-Mackay score, modified Lund-Kennedy endoscopy score, nasal polyp
Introduction
Chronic rhinosinusitis (CRS) is characterized by persistent sinonasal inflammation, nasal purulent discharge, and nasal blockage for more than 12 weeks.1,2 CRS is divided into CRS without nasal polyps or with nasal polyps (CRSwNP), according to whether nasal polyps are present or not.3 CRSwNP in Western countries is characterized by type 2 skewed eosinophilic inflammation, which involves the activation of type 2 helper T cell and innate lymphoid cell and increased expressions of interleukin (IL)-4, IL-5, IL-13, and eosinophil cationic protein (ECP).4
Eosinophilic inflammation is significantly less prevalent in patients with CRSwNP in Asia than in the Western countries. Type 2 skewed eosinophilic inflammation occurs in 40–60% of patients with CRSwNP in Japan and East Asia, which is markedly lower than the rate of 80% in Western countries.5–7 However, the prevalence of CRSwNP with eosinophilic infiltration has been increasing in Asia in recent years due to the Westernization of eating habits and environments.8
Endoscopic sinus surgery (ESS) for CRSwNP refractory to medical treatment has been largely reported to be effective and safe.9 However, patients with a high inflammatory burden and severe nasal polyposis have a recurrence rate of 40% in general and up to 60% for those with comorbid asthma after ESS.10,11 Patients with CRSwNP with severe type 2 eosinophilic inflammation usually experience poorer improvement after surgical intervention, have persistent postoperative (post-op) mucosal inflammation, and are more susceptible to recurrence after surgery.12,13
The role of type 2 eosinophilic inflammation in disease severity, recurrence, and comorbidity in CRS has been recognized. Therefore, several biologics targeting IL-4, IL-5, IL-13 and immunoglobulin E (IgE) have been administered, and patients with severe uncontrolled CRSwNP have demonstrated good response in clinical trials and real world clinical practice.14,15 A previous study revealed that patients undergoing ESS achieved a higher reduction of nasal polyp size, while those receiving biologics (Dupilumab, anti-IL-4 α receptor) experienced a higher improvement in the quality of life and smell measurement in CRSwNP.16,17 Sinus surgery can remove sinonasal inflammatory content, open the drainage pathway of sinuses immediately, and relieve patient symptoms early.16 However, biologics targeting type 2 inflammatory mediators can suppress tissue inflammation, restore the epithelial barrier, and resolve post-op residual sinonasal inflammation.17,18 As a result, a combination of surgery and biologics may be required for patients with severe type 2 eosinophilic CRSwNP and a high inflammatory burden to achieve optimal therapeutic outcomes.18–20
Thus, this study aimed to evaluate and identify the risk factors for post-op residual sinus inflammation in patients with eosinophilic CRSwNP after ESS. Patients with type 2 eosinophilic CRSwNP and poor response to ESS would benefit from biologic therapy targeting mediators in type 2 inflammation. This can help clinicians to promptly identify patients with poor surgical response and provide additional treatment to achieve optimal therapeutic outcomes in patients with eosinophilic CRSwNP.
Materials and Methods
Patients
After approval by the Institutional Review Board of Chang Gung Memorial Hospital (IRB numbers: 202002219A3, 202102257A3, and 202202075A3), adult patients (≥18 years) who planned to undergo ESS for bilateral CRSwNP were prospectively enrolled after providing signed informed consent from November 2020 to December 2023 (Figure 1). All procedures were conducted in accordance with the relevant ethical guidelines and regulations, and the Declaration of Helsinki. Previous studies collected preoperative data to evaluated the relationship between clinical markers and tissue type 2 inflammatory severity,7 to characterize the clinical features of patients with comorbid asthma,21 and to investigate the predictive value of the ethmoid-to-maxillary (E/M) ratio based on different CT scoring systems in patients with CRSwNP.22 In the current study, we collected the postoperative data to identify the risk factors for residual sinus inflammation after surgery in patients with eosinophilic CRSwNP.
 |
Figure 1 Algorithm for enrollment of study cohorts. Residual sinus inflammation was defined by modified Lund-Kennedy endoscopic score ≥ 5. Abbreviations: CRSwNP, chronic rhinosinusitis with nasal polyp; FESS, functional endoscopic sinus surgery; TEC, tissue eosinophil count; HPF, high power field; post-op, postoperative; CT, computed tomography. |
CRSwNP was diagnosed according to the EPOS2020 definition.2 The enrolled patients did not respond to three months of conservative medical therapies including intranasal corticosteroids and nasal douches. The presence of nasal polyps was confirmed based on endoscopic findings and histopathological analysis. We excluded patients (a) with sinonasal tumor; (b) having concomitant disorders of immunologic complications, cystic fibrosis, or primary ciliary dyskinesia; and (c) received treatment with oral corticosteroids, monoclonal antibodies, or immunosuppressives before enrolment (e) declined to participate.
Clinical information of the participants, including relevant clinical symptoms, medical history of allergy and comorbid asthma, cigarette smoking, and associated laboratory and image surveys were collected. Allergy was determined using an automated immunoassay (ImmunoCap) to detect serum specific IgE antibodies to the aeroallergens.7 Comorbid asthma was confirmed based on fulfillment of the diagnostic criteria of the Global Initiative for Asthma guidelines and the regular use of inhaled corticosteroids.23 The sinonasal outcome test- 22 (SNOT-22) was used to assess the nasal symptoms and quality of life.24 Each item in the SNOT-22 was scored from 0 to 5 (from no problem to worse), with a total score of up to 110. Laboratory examinations included peripheral blood cell counts, serum total IgE, and ECP concentrations.
All participants underwent bilateral ESS targeting the sinuses, including maxillary, anterior and posterior ethmoid, frontal, and sphenoid sinuses. Sphenoidotomy was performed depending on the presence or absence of sinus opacification on computed tomography (CT) images. After surgery, the participants subsequently received standard post-op care, encompassing antibiotic therapy with Curam 875/125 mg/tab (Amoxicillin + clavulanic acid, SANDOZ GMBH, Aus) for 3 weeks, intranasal corticosteroids, nasal douches, and weekly follow-ups in the first month and monthly for the subsequent two visits. At 3 months after surgery, some patients experienced good response but some exhibited residual sinus inflammation on nasal endoscopic evaluation (Figure 2).
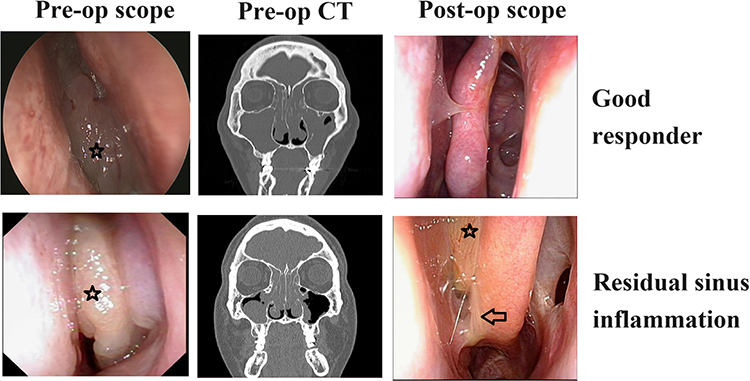 |
Figure 2 Representative computed tomographic images and perioperative endoscopic evaluations in patients with bilateral CRSwNP. Star: nasal polyp; arrow: mucoid discharge. |
Nasal Endoscopic Evaluation
The nasal polyp scoring (NPS) system was used as described previously.25 The polyps were assessed using nasal endoscopy and graded as follows: no polyps (score 0); small polyps in the middle meatus (score 1); polyps reaching below the lower border of the middle turbinate (score 2); polyps medial to the middle turbinate or reaching the lower border of the inferior turbinate (score 3); and large polyps with total obstruction of the inferior meatus (score 4). The modified Lund-Kennedy (MLK) endoscopic scoring system based on the degree of edema, polyps, and discharge was used to evaluate the severity of post-op sinus mucosal inflammation.26 Post-op residual mucosal inflammation was defined as a MLK score of ≥ 5 at three months after surgery according to previous studies (Figure 2).26,27 All patients provided informed consent before participating in the study. All study procedures were performed according to relevant guidelines and regulations.
Tissue Eosinophil Count Quantification
Polyp specimen collected during sinus surgery was fixed in formalin and embedded in paraffin. Standard 5-µm sections underwent haematoxylin and eosin staining. Tissue eosinophils were counted at ×400 magnification (high power field, HPF) microscopic evaluation in three fields with most severe inflammatory cell infiltration and intact mucosal epithelium. Eosinophilic CRSwNP was defined as a tissue eosinophil count of ≥ 10/HPF.2
Sinonasal Computed Tomographic Evaluation
The sinonasal CT images with one section per mm were independently reviewed by two experienced rhinologists. The Lund-Mackay score (LMS) was used to quantify CRS severity radiologically.28 As previously described, the maxillary sinus, anterior and posterior ethmoidal sinuses, frontal sinus, sphenoid sinus, and ostiomeatal complex were assigned scores of 0, 1, or 2 (indicate no abnormality, partial or complete opacification), respectively. The ostiomeatal complex was assigned scores of 0 or 2 (indicating the presence or absence of obstruction). The total score was up to 24 bilaterally.
The E/M ratio was determined by calculating the ratio of the average scores for the anterior and posterior ethmoid sinuses to that of the maxillary sinuses on CT images.29,30 A higher disease involvement in the ethmoid sinus area and central sinonasal compartment was associated with a higher E/M ratio.
The olfactory cleft opacification score was evaluated on a scale of 0–3 indicating clear, less than half, more than half, or total opacification on each side of the olfactory cleft on CT images respectively (Figure 3).7,31
 |
Figure 3 The olfactory cleft opacification on the computed tomography (CT) image (arrow) was graded using a scale of 0–3 indicating clear (score 0), less than half ((a) left nose, score 1), more than half ((b) right nose, score 2), and total ((a) right nose, score 3) opacification at each side of the olfactory cleft (the area between the middle turbinate and the nasal septum on the coronal plane section of the cribriform plate’s CT imaging). |
Statistical Analyses
The data were statistically analysed using GraphPad Prism 5 (GraphPad Prism Software, Inc., San Diego, Calif, USA), SPSS (version 27.0; SPSS Inc., Chicago, IL) and RStudio v2022.02.1 (RStudio, Boston, MA, USA). D’Agostino & Pearson omnibus normality test was used to evaluate the normality of data. Categorical variables were compared using the х2 test or Fisher’s exact test as appropriate. Continuous variables were compared using the Mann–Whitney U-test or t test. Regression analyses were used to assess the association between post-op residual sinus inflammation and clinical variables. R-squared (R2) was used to assess the model fit. To identify the cut-off values for the prediction of residual sinus inflammation in eosinophilic CRSwNP, receiver operating characteristic (ROC) curves were generated and the area under the ROC curve (AUC) was evaluated. Based on the results of the logistic regression analysis, a nomogram model was developed to predict the risk of post-op residual sinus inflammation. In the nomogram, each variable was assigned a score. The total points were derived by calculating the sum of the corresponding scores from the five variables, reflecting the predicted probability of post-op residual sinus inflammation in eosinophilic CRSwNP for an individual. The ROC curve and AUC were used to evaluate the predictive performance of the nomogram model. Statistical significance was set at p < 0.05.
Results
Clinical Characteristics of Patients
A total of 143 adult patients with bilateral CRSwNP were enrolled and evaluated. Ninety-three (65.0%) had eosinophilic CRSwNP (tissue eosinophil count ≥ 10/HPF). Twenty-six of the 93 (28%) patients with eosinophilic CRSwNP experienced post-op residual sinus inflammation defined by a post-op MLK score of ≥ 5 within three months after surgery. The demographic data of the patients with eosinophilic CRSwNP are shown in Table 1. The prevalence of comorbid asthma, NPS, LMS, E/M ratio, olfactory cleft opacification score on CT image, serum ECP level, and tissue eosinophil count were significantly higher for the patients with than for those without post-op residual sinus inflammation (all p < 0.05). The maxillary, anterior and posterior ethmoid, and frontal sinuses of all participants were drained and re-ventilated. The rate of sphenoidotomy was not significantly different between patients with and without post-op residual sinus inflammation (84.6% vs 70.1%, p=0.244).
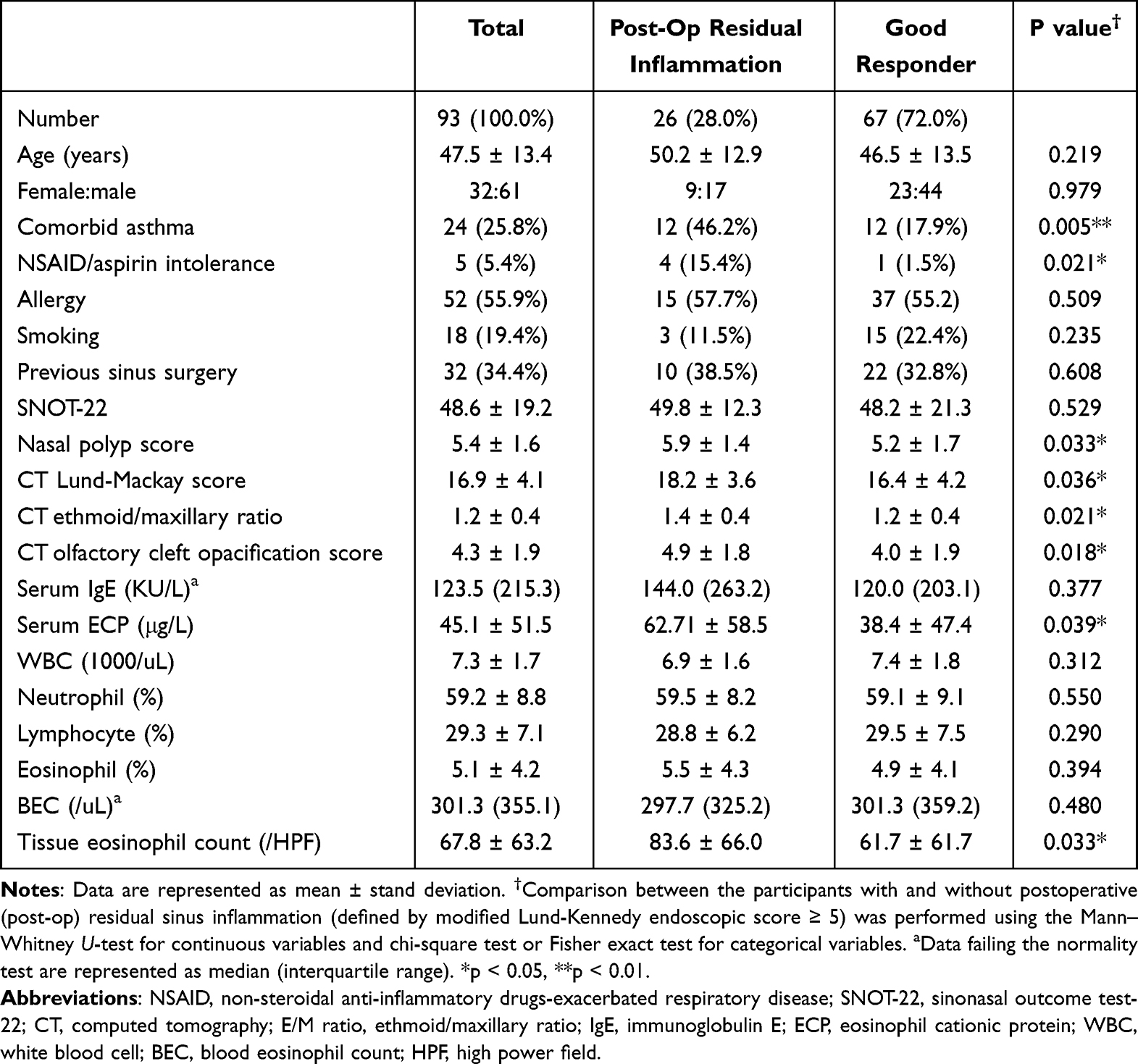 |
Table 1 Clinical Characteristics of Participants with Eosinophilic Chronic Rhinosinusitis with Nasal Polyp |
Regression Analyses
Table 2 shows the associations between the clinical variables and post-op residual sinus inflammation examined using logistic regression analysis. Univariate regression analysis showed that comorbid asthma, NPS, E/M ratio, and olfactory cleft opacification score on CT image were significant predictors of post-op residual sinus inflammation in patients with eosinophilic CRSwNP. Only comorbid asthma maintained a statistically significant association in the multivariate analysis.
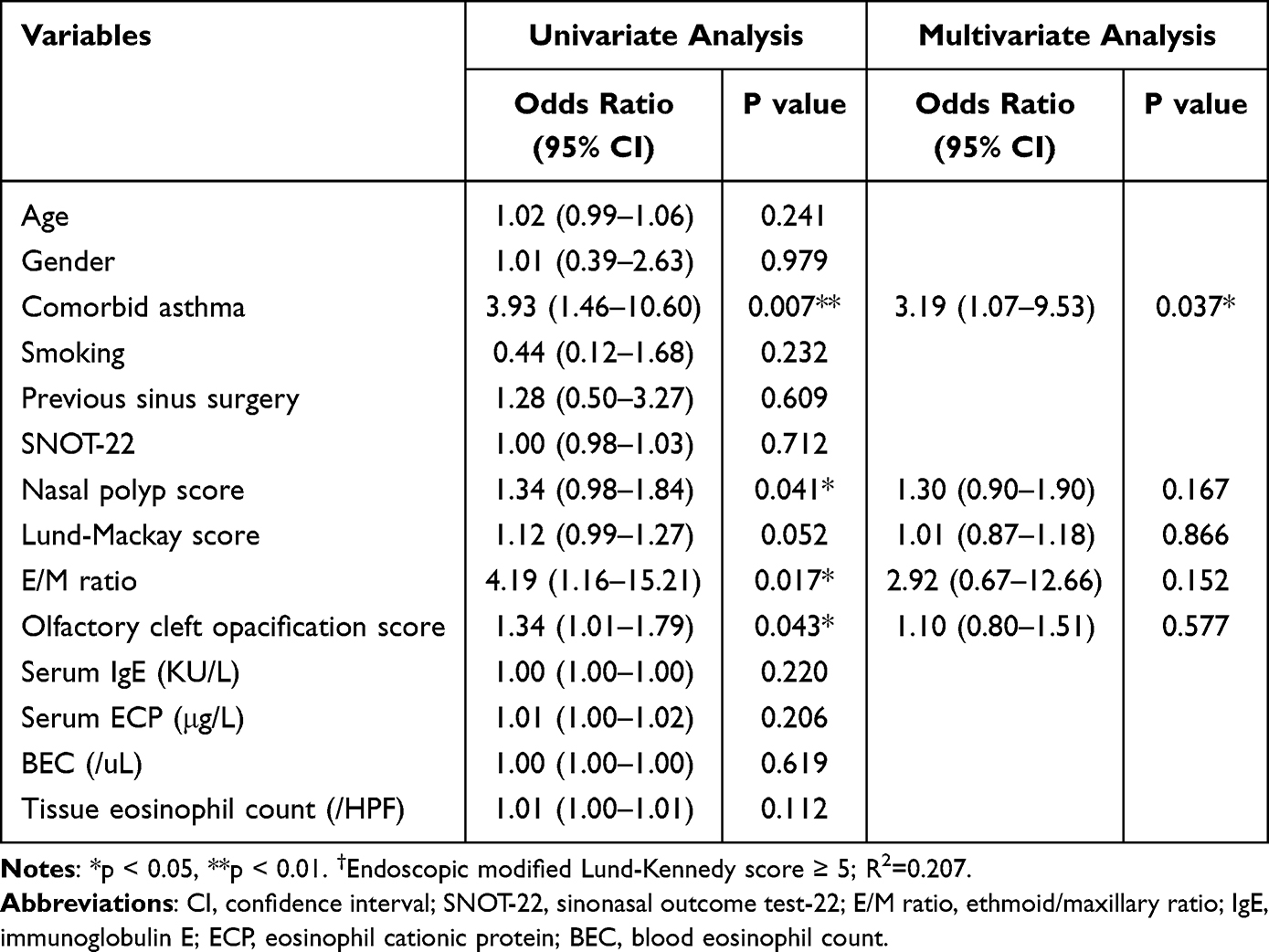 |
Table 2 Logistic Regression Analyses of Clinical Variables for Residual Sinus Inflammation After Surgery† |
ROC Curve Analysis
ROC curves were plotted, and AUC values were calculated to evaluate the sensitivity and specificity of comorbid asthma, NPS, LMS, the E/M ratio, and olfactory cleft opacification score on CT image for predicting post-op residual sinus inflammation in patients with eosinophilic CRSwNP (Figure 4). The AUC was 0.641 for asthma (p = 0.035), 0.606 for NPS (p = 0.114), 0.620 for LMS (p = 0.073), 0.653 for E/M ratio (p = 0.023), and 0.651 for the olfactory cleft opacification score (p = 0.024).
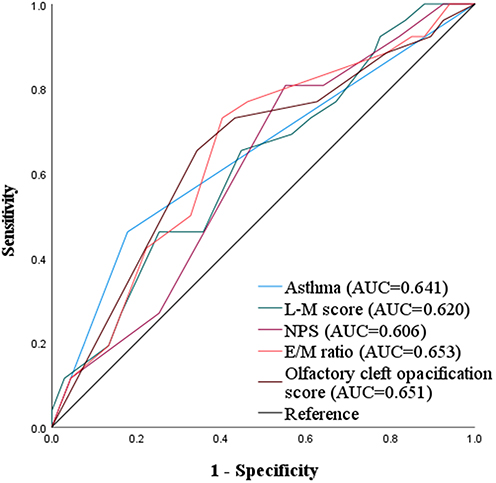 |
Figure 4 Receiver operating characteristic curves of comorbid asthma (p = 0.035), nasal polyp score (NPS; p = 0.114), Lund-Mackay (L-M) score (p = 0.073), ethmoid/maxillary sinus (E/M) ratio (p = 0.023), and olfactory cleft opacification score (p = 0.024) were used to detect the probability of post-op residual sinus inflammation in patients with eosinophilic CRSwNP. Abbreviation: AUC, area under curve. |
Nomogram for Predicting Post-Op Residual Sinus Inflammation
Given that the ROC analysis revealed absence of a single ideal predictor, a nomogram was constructed to predict the probability of post-op residual sinus inflammation in eosinophilic CRSwNP based on the results of the logistic regression analysis (Figure 5). The AUC of the nomogram was 0.747 (95% confidence interval, 0.708–0.804).
 |
Figure 5 A nomogram developed to predict the probability of post-op residual sinus inflammation in patients with eosinophilic CRSwNP according to the results of the logistic regression analysis (a). In the nomogram, each value of a variable represents its score. The total points can be obtained by adding the corresponding scores from the five predictors, and the predicted value of post-op residual sinus inflammation for an individual can be indicated. Receiver operating characteristic (ROC) curve (b) and calibration curve (c) of the nomogram model for predicting the probability of post-op residual sinus inflammation in eosinophilic CRSwNP was plotted. The area under the ROC curve (AUC) was 0.747 (95% confidence interval = 0.708–0.804). The Ideal line represents the ideal model which predicted probabilities perfectly matching the actual probabilities. The Apparent line and the Bias corrected line respectively represent the nomogram model before and after bootstrap re-sampling method. Abbreviation: NPS, nasal polyp score. |
Discussion
ESS has been an effective strategy for treating CRSwNP, but patients with a high inflammatory burden and extensive nasal polyposis have a risk of recurrence of 40% in general and up to 60% when there is comorbid asthma.9–11,32 Patients with CRSwNP with severe type 2 eosinophilic inflammation usually experience poorer improvement after surgical intervention, have persistent post-op mucosal inflammation, and have a greater susceptibility to recurrence after surgery.12 Several biologics targeting mediators in type 2 inflammation have been administered with good response in patients with severe uncontrolled CRSwNP.15 Recent studies have revealed that patients who received adjuvant Dupilumab therapy had significantly better short-term sinonasal endoscopic scores than those who underwent only surgery, although both treatments were effective for symptom reduction.18,20 Sinus surgery removed the sinonasal inflammatory contents and opened the drainage pathway of sinuses immediately, and biologics effectively suppressed the tissue inflammation, restored the epithelial barrier, and suppressed the post-op residual sinonasal inflammation.16 Thus, patients with severe type 2 eosinophilic CRSwNP and a high inflammatory burden may require a combination of surgery and biologics to achieve optimal therapeutic outcomes.18,20
A recent study suggested that nasal endoscopy findings can be used to determine CRS disease control and treatment escalation.33 The current study further evaluated the risk factors for post-op residual sinus inflammation (MLK score ≥ 5 on endoscopy evaluation) after ESS for patients with eosinophilic CRSwNP. The prevalence of comorbid asthma, NPS, LMS, E/M ratio, olfactory cleft opacification score on CT image, serum ECP level, and tissue eosinophil count were significantly higher for the patients with than for those without post-op residual sinus inflammation. Comorbid asthma, NPS, E/M ratio, and olfactory cleft opacification score on CT image were significant predictors of post-op residual sinus inflammation in regression analysis. Given the absence of a single ideal predictor in the ROC analysis, a nomogram was constructed to predict the probability of post-op residual sinus inflammation in eosinophilic CRSwNP based on the results of the regression analysis. This can help clinicians promptly identify patients with poor surgical response and benefits from adjuvant biological therapy and provide additional treatment to achieve optimal therapeutic outcomes in patients with eosinophilic CRSwNP.
Asthma is a common type 2 comorbid airway inflammation in eosinophilic CRSwNP based on the concept of a unified airway.34 Comorbid asthma is a known indicator of more severe inflammation and a higher risk for postoperative recurrence of nasal polyps in patients with CRSwNP.10,35,36 Similar to eosinophilic CRSwNP, comorbid asthma is less prevalent in Asia than in Western countries, which may be up to 60%.6 In our study, comorbid asthma was found in only 25.8% of participants with eosinophilic CRSwNP and was still a strong predictive factor for those with post-op residual sinus inflammation. However, the sensitivity (46.2%) was not high due to the low prevalence. Simultaneous evaluation of other factors is necessary. Also, only five (5.4%) participants with eosinophilic CRSwNP had a history of aspirin or non-steroidal anti-inflammatory drugs (NSAID) intolerance in the present study, and all of them had comorbid asthma. Four of the patients exhibited post-op residual sinus inflammation. NSAID or aspirin-exacerbated respiratory disease in Chinese patients with CRSwNP is not as prevalent as that in Western countries, but it is still considered a predictive factor for severe eosinophilic CRSwNP and post-op residual sinus inflammation.37,38
NPS and LMS reflect the sinus inflammation burden by grading the polyp size and extent of sinus involvement. High NPS and LMS indicate a high inflammatory load and prolonged resolution of sinus inflammation, and it predict susceptibility to post-op residual sinus inflammation. Previous studies also reported that high NPS and LMS were indicators for poor surgical outcomes including polyp recurrence.39–41
Type 2 eosinophilic CRSwNP often involves the central sinonasal area, including ethmoid sinuses, middle turbinates, and the nasal olfactory cleft.26,42 The mechanism underlying the predominant involvement of the central compartment in type 2 eosinophilic CRSwNP remains unclear. The possible explanations include the regional differences in molecular expression patterns within the sinonasal mucosa.43,44 The Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis suggested a greater CT shadow of the ethmoid sinus than that of the maxillary sinus as one of the scoring criteria for eosinophilic CRS.35 Meng et al demonstrated the E/M ratio as a predictor for differentiating adult eosinophilic from non- eosinophilic CRSwNP.29 The current study showed that the E/M ratio and olfactory cleft opacification score on the CT image were associated with post-op residual sinus inflammation. These results indicated that the severity of type 2 eosinophilic inflammation is related to the post-op recovery of sinus mucosal inflammation. Further post-op adjuvant therapy may be required for severe eosinophilic CRSwNP. However, the E/M ratio and olfactory cleft opacification score on the CT image may be limited as type 2 eosinophilic inflammatory markers because the difference may diminish in patients with extensive disease involvement, such as those with total opacification in all sinuses (LMS 24).
The serum ECP concentration and tissue eosinophil count were significantly higher in patients with post-op residual sinus inflammation than in those without. However, they were not significant predictors of post-op residual sinus inflammation in the regression analysis. In the current study, we performed analysis only in patients with eosinophilic CRSwNP, and all these patients had high ECP concentrations and tissue eosinophil counts (> 10/HPF). Weak to moderate correlations were also found between the type 2 inflammatory markers such as the serum ECP concentration, blood eosinophil count, and serum total IgE, and tissue eosinophil count (data not shown). Taken together, the determination of residual sinus inflammation may be based on both the severity of type 2 eosinophilic inflammation and extent of the inflammation involved.39 The serum ECP concentration and tissue eosinophil count can only reflect the degree of type 2 eosinophilic inflammation.12 Thus a comprehensive evaluation of the severity and extent of type 2 eosinophilic inflammation in CRSwNP is necessary to predict the therapeutic outcomes after sinus surgery and the need for post-op adjuvant therapy such as biologic therapy.45
Owing to the lack of a single ideal predictor including comorbid asthma, NPS, LMS, E/M ration, and olfactory cleft opacification score in the ROC analysis, we propose a nomogram to predict the probability of post-op residual sinus inflammation in patients with eosinophilic CRSwNP by simultaneously evaluating five clinical variables based on regression analysis results. The total points obtained by calculating the sum of the corresponding scores from these variables provide better precision in predicting the risk of post-op residual sinus inflammation in each patient with eosinophilic CRSwNP. This could help clinicians better evaluate therapeutic outcomes of surgery in patients with eosinophilic CRSwNP and may provide additional adjuvant therapy to facilitate the recovery of post-op sinonasal residual inflammation.
This study had several limitations. First, only patients who underwent sinus surgery in as single centre were enrolled. Patients with milder disease or those who were unwilling to undergo surgery were not recruited and selection bias may have occurred. Nevertheless, all patients diagnosed with bilateral CRSwNP who underwent sinus surgery during the study period were eligible and included to minimise selection bias. Second, this study was conducted in a tertiary referral medical centre and the disease severity of CRSwNP may have been higher than that of the general population. High NPS, LMS, and symptom scores were observed in participants of the current study. However, these patients have the greatest potential to be refractory to surgery and may require adjuvant therapy such as biologics, which warrants further investigation. Third, half of our participants did not undergo the olfaction test because of the COVID-19 pandemic. Instead, we determined the olfactory cleft opacification score using CT images to evaluate the inflammation severity in the olfactory mucosa of patients with eosinophilic CRSwNP. Fourth, we did not determine whether these clinical markers could predict long-term treatment response in the current study. Furthermore, limitations of the use of nomogram by the moderate predictive power and lack of external validation should be acknowledged. All these highlighting the need for future reports with large scale and long-term post-op outcomes. However, our findings emphasise that the detection of post-op residual sinus inflammation may be based on both the severity of type 2 eosinophilic inflammation and the extent of sinonasal inflammation. Thus, a comprehensive evaluation of the severity and extent of type 2 eosinophilic inflammation in patients with CRSwNP is necessary to predict the surgical outcomes and the need for post-op adjuvant therapy.
Conclusion
The determination of post-op residual sinus inflammation may be based on both the severity of type 2 eosinophilic inflammation and the extent of the sinonasal inflammation. Comorbid asthma, NPS, LMS, E/M ratio, and olfactory cleft opacification score were significant predictors of post-op residual sinus inflammation in patients with eosinophilic CRSwNP. This can help clinicians to better evaluate therapeutic outcomes after sinus surgery and predict the need for post-op adjuvant therapy such as biologics.
Abbreviations
CRS, chronic rhinosinusitis; CRSwNP, chronic rhinosinusitis with nasal polyp; IL, interleukin; ECP, eosinophil cationic protein; ESS, Endoscopic sinus surgery; post-op, postoperative; IgE, immunoglobulin E; SNOT-22, sinonasal outcome test- 22; CT, computed tomography; NPS, nasal polyp score; MLK score, modified Lund-Kennedy endoscopic score; HPF, high power field; LMS, Lund-Mackay score; E/M ratio, ethmoid/maxillary ratio; ROC curve, receiver operating characteristic curve; AUC, area under the curve; NSAID, non-steroidal anti-inflammatory drugs - exacerbated respiratory disease; WBC, white blood cell; BEC, blood eosinophil count; TEC, tissue eosinophil count.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, [Chein-Chia H.].
Author Contributions
Chien-Chia H: Conceptualization, Data curation, Formal analysis, Funding acquisition and Writing – review and editing; PWW: Data curation, Formal analysis and Writing – original draft. PHC: Data curation and Supervision; Chi-Che H: Data curation and Supervision; YHF: Formal analysis and Visualization; CIY: Data curation. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received research grants from the Chang Gung Memorial Hospital (CMRPG3P0571) and the Taiwan National Science and Technology Council (114-2314-B-182 −031 -MY2). The funder played no role in the study design, data collection and analysis, decision to publish, or paper preparation.
Disclosure
The authors declare no conflicts of interest.
References
1. Orlandi RR, Kingdom TT, Smith TL, et al. International consensus statement on allergy and rhinology: rhinosinusitis 2021. Int Forum Allergy Rhinol. 2021;11(3):213–12. doi:10.1002/alr.22741
2. Fokkens WJ, Lund VJ, Hopkins C, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology. 2020;58(Suppl S29):1–464. doi:10.4193/Rhin20.401
3. Cho SH, Hamilos DL, Han DH, Laidlaw TM. Phenotypes of chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2020;8(5):1505–1511. doi:10.1016/j.jaip.2019.12.021
4. Kato A, Peters AT, Stevens WW, Schleimer RP, Tan BK, Kern RC. Endotypes of chronic rhinosinusitis: relationships to disease phenotypes, pathogenesis, clinical findings, and treatment approaches. Allergy. 2022;77(3):812–826. doi:10.1111/all.15074
5. Nakayama T, Lee IT, Le W, et al. Inflammatory molecular endotypes of nasal polyps derived from White and Japanese populations. J Allergy Clin Immunol. 2022;149(4):1296–1308.e6. doi:10.1016/j.jaci.2021.11.017
6. Yao Y, Zeng M, Liu Z. Revisiting Asian chronic rhinosinusitis in the era of type 2 biologics. Clin Exp Allergy. 2022;52(2):231–243. doi:10.1111/cea.14065
7. Wu PW, Huang CC, Chang PH, Lee TJ, Fan YH, Huang CC. Blood eosinophil count is the dominant clinical marker for type 2 inflammatory severity in CRSwNP. Laryngoscope. 2025;135(4):1326–1334. doi:10.1002/lary.31899
8. Wang W, Gao Y, Zhu Z, et al. Changes in the clinical and histological characteristics of Chinese chronic rhinosinusitis with nasal polyps over 11 years. Int Forum Allergy Rhinol. 2019;9(2):
9. Ryan MT, Patel K, Fischer JL, et al. Gender differences in outcomes following endoscopic sinus surgery: a systematic review and meta-analysis. Rhinology. 2024;62(5):514–525. doi:10.4193/Rhin24.009
10. Loftus CA, Soler ZM, Koochakzadeh S, et al. Revision surgery rates in chronic rhinosinusitis with nasal polyps: meta-analysis of risk factors. Int Forum Allergy Rhinol. 2020;10(2):199–207. doi:10.1002/alr.22487
11. Rodriguez-Van Strahlen C, Arancibia C, Calvo-Henriquez C, Mullol J, Alobid I. Systematic review of long term sinonasal outcomes in CRSwNP after endoscopic sinus surgery: a call for unified and standardized criteria and terms. Curr Allergy Asthma Rep. 2024;24(8):443–456. doi:10.1007/s11882-024-01154-w
12. Van Zele T, Holtappels G, Gevaert P, Bachert C. Differences in initial immunoprofiles between recurrent and nonrecurrent chronic rhinosinusitis with nasal polyps. Am J Rhinol Allergy. 2014;28(3):192–198. doi:10.2500/ajra.2014.28.4033
13. Rosati D, Rosato C, Pagliuca G, et al. Predictive markers of long-term recurrence in chronic rhinosinusitis with nasal polyps. Am J Otolaryngol. 2020;41(1):102286. doi:10.1016/j.amjoto.2019.102286
14. Huber P, Förster-Ruhrmann U, Olze H, et al. Real-world data show sustained therapeutic effects of dupilumab in chronic rhinosinusitis with nasal polyps (CRSwNP) over 3 years. Allergy. 2024;79(11):3108–3117. doi:10.1111/all.16263
15. Bachert C, Zhang N, Cavaliere C, Weiping W, Gevaert E, Krysko O. Biologics for chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol. 2020;145(3):725–739. doi:10.1016/j.jaci.2020.01.020
16. Dharmarajan H, Falade O, Lee SE, Wang EW. Outcomes of dupilumab treatment versus endoscopic sinus surgery for chronic rhinosinusitis with nasal polyps. Int Forum Allergy Rhinol. 2022;12(8):986–995. doi:10.1002/alr.22951
17. De Corso E, Porru DP, Corbò M, et al. Comparative real-world outcomes of dupilumab versus endoscopic sinus surgery in the treatment of severe CRSwNP patients. Clin Otolaryngol. 2024;49(4):481–489. doi:10.1111/coa.14172
18. Wu PW, Huang CC, Chang PH, Lee TJ, Huang CC. The benefit of dupilumab as a postoperative short-term adjuvant therapy for chronic rhinosinusitis with nasal polyps: a preliminary study. Laryngoscope Investig Otolaryngol. 2024;9(4):e1296. doi:10.1002/lio2.1296
19. Guo CL, Liu FF, Wang DY, Liu Z. Type 2 biomarkers for the indication and response to biologics in CRSwNP. Curr Allergy Asthma Rep. 2023;23(12):703–713. doi:10.1007/s11882-023-01114-w
20. Liu CN, Yeh TH, Lin CF, Lin YT. The efficacy of dupilumab as an adjuvant treatment after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyps: a retrospective cohort analysis. Clin Exp Otorhinolaryngol. 2025;18(3):271–279. doi:10.21053/ceo.2024.00310
21. Wu PW, Chang PH, Huang CC, Lee TJ, Fan YH, Huang CC. Impact of comorbid asthma on life quality of patients with chronic rhinosinusitis and nasal polyps. J Asthma Allergy. 2025;18:567–578. doi:10.2147/JAA.S517258
22. Wu PW, Wei ZH, Huang CC, Chang PH, Lee TJ, Huang CC. Predictive value of computed tomographic ethmoid-to-maxillary ratio in patients with chronic rhinosinusitis and nasal polyp. J Asthma Allergy. 2025;18:1167–1177. doi:10.2147/JAA.S536368
23. Global initiative for asthma (GINA). 2024. Available from: https://ginasthma.org/.
24. Li Z, Lu T, Sun L, et al. Factors for predicting the outcome of surgery for non-eosinophilic chronic rhinosinusitis with nasal polyps. Ann Allergy Asthma Immunol. 2024;133(5). doi:10.1016/j.anai.2024.05.023
25. Gevaert P, De Craemer J, Bachert C, et al. European academy of allergy and clinical immunology position paper on endoscopic scoring of nasal polyposis. Allergy. 2023;78(4):912–922. doi:10.1111/all.15650
26. Psaltis AJ, Li G, Vaezeafshar R, Cho KS, Hwang PH. Modification of the Lund-Kennedy endoscopic scoring system improves its reliability and correlation with patient-reported outcome measures. Laryngoscope. 2014;124(10):2216–2223. doi:10.1002/lary.24654
27. Png LH, Kalish L, Campbell RG, et al. Predictors of persistent disease in biologic treated type 2 diffuse/eosinophilic chronic rhinosinusitis undergoing surgery. Int Forum Allergy Rhinol. 2024;14(5):909–918. doi:10.1002/alr.23282
28. Hopkins C, Browne JP, Slack R, Lund V, Brown P. The Lund-Mackay staging system for chronic rhinosinusitis: how is it used and what does it predict? Otolaryngol Head Neck Surg. 2007;137(4):555–561. doi:10.1016/j.otohns.2007.02.004
29. Meng Y, Lou H, Wang C, Zhang L. Predictive significance of computed tomography in eosinophilic chronic rhinosinusitis with nasal polyps. Int Forum Allergy Rhinol. 2016;6(8):812–819. doi:10.1002/alr.21749
30. Lin YT, Lin CF, Liao CK, Yeh TH. Comprehensive evaluation of type 2 endotype and clinical features in patients with chronic rhinosinusitis with nasal polyps in Taiwan: a cross-sectional study. Eur Arch Otorhinolaryngol. 2023;280(12):5379–5389. doi:10.1007/s00405-023-08118-2
31. Wu PW, Chiu CH, Huang YL, et al. Tissue eosinophilia and computed tomography features in paediatric chronic rhinosinusitis with nasal polyps requiring revision surgery. Rhinology. 2023;61(3):348–357. doi:10.4193/Rhin22.435
32. Wu CL, Lee TJ, Huang CC, Chang PH, Fu CH. Clinical predictors of revision surgery for chronic rhinosinusitis with nasal polyposis within 5-year follow-up. Am J Otolaryngol. 2020;41(6):102654. doi:10.1016/j.amjoto.2020.102654
33. Sedaghat AR, Cotter RA, Alobid I, et al. Nasal endoscopy score thresholds to trigger consideration of chronic rhinosinusitis treatment escalation and implications for disease control. Rhinology. 2025;63(1):54–62. doi:10.4193/Rhin24.291
34. Peters AT, Tan BK, Stevens WW. Consultation for chronic rhinosinusitis with nasal polyps and asthma: clinical presentation, diagnostic work-up, and treatment options. J Allergy Clin Immunol Pract. 2024;12:
35. Tokunaga T, Sakashita M, Haruna T, et al. Novel scoring system and algorithm for classifying chronic rhinosinusitis: the JESREC Study. Allergy. 2015;70(8):995–1003. doi:10.1111/all.12644
36. Tomassen P, Vandeplas G, Van Zele T, et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J Allergy Clin Immunol. 2016;137(5):1449–1456.e4. doi:10.1016/j.jaci.2015.12.1324
37. Meng J, Ye J, Zhang L, et al. Expert consensus on the diagnosis and treatment of respiratory diseases exacerbated by nonsteroidal anti-inflammatory drugs (2024, Chengdu). Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2024;38(6):453–462. doi:10.13201/j.issn.2096-7993.2024.06.001
38. Elahi S, Peters AT, Kato A, Stevens WW. Clinical and mechanistic advancements in aspirin exacerbated respiratory disease. J Allergy Clin Immunol. 2025;155(5):1411–1419. doi:10.1016/j.jaci.2025.03.006
39. DeConde AS, Mace JC, Levy JM, Rudmik L, Alt JA, Smith TL. Prevalence of polyp recurrence after endoscopic sinus surgery for chronic rhinosinusitis with nasal polyposis. Laryngoscope. 2017;127(3):550–555. doi:10.1002/lary.26391
40. Fageeh YA, Basurrah MA, Hakami KT, Almalki ZA, Alnemari FS, Altalhi WA. Risk factors for recurrence of chronic rhinosinusitis with nasal polyps after endoscopic sinus surgery: a retrospective study. Saudi Med J. 2023;44(12):1254–1259. doi:10.15537/smj.2023.44.12.20230396
41. Kim DH, Han JS, Kim GJ, Basurrah MA, Hwang SH. Clinical predictors of polyps recurring in patients with chronic rhinosinusitis and nasal polyps: a systematic review and meta-analysis. Rhinology. 2023;61(6):482–497. doi:10.4193/Rhin23.136
42. Stevens WW, Peters AT, Tan BK, et al. Associations between inflammatory endotypes and clinical presentations in chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2019;7(8):2812–2820. doi:10.1016/j.jaip.2019.05.009
43. Yao Y, Zhu HY, Zeng M, Liu Z. Immunological mechanisms and treatable traits of chronic rhinosinusitis in Asia: a narrative review. Clin Otolaryngol. 2023;48(2):363–370. doi:10.1111/coa.14001
44. Szucs E, Ravandi S, Goossens A, Beel M, Clement PA. Eosinophilia in the ethmoid mucosa and its relationship to the severity of inflammation in chronic rhinosinusitis. Am J Rhinol. 2002;16(3):131–134. doi:10.1177/194589240201600301
45. Saito T, Okazaki K, Fushimi K, Tsuzuki K. Usefulness of post-operative endoscopic score for optimal treatment selection in recurrent eosinophilic chronic rhinosinusitis. J Laryngol Otol. 2024;138(2):162–168. doi:10.1017/S0022215123000798
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics of Eosinophilic Chronic Rhinosinusitis with Nasal Polyps in Adolescents
Huang CC, Chang PH, Huang YL, Lee TJ, Huang CC, Wu PW
Journal of Asthma and Allergy 2023, 16:1197-1206
Published Date: 30 October 2023
Histopathological Characteristics of Nasal Tissues From Paediatric Patients with Chronic Rhinosinusitis and Nasal Polyps Requiring Revision Surgery
Hsieh SF, Wu PW, Chiu CH, Huang YL, Huang CC
Journal of Inflammation Research 2025, 18:13279-13289
Published Date: 26 September 2025
Minimal Clinically Important Difference of the Taiwan Smell Test in Patients with Bilateral Chronic Rhinosinusitis and Nasal Polyps Post-Sinus Surgery
Wu PW, Shen PH, Lee YS, Chang PH, Huang CC, Huang CC
Journal of Asthma and Allergy 2025, 18:1347-1353
Published Date: 1 October 2025