Back to Journals » Journal of Inflammation Research » Volume 18
Histopathological Characteristics of Nasal Tissues From Paediatric Patients with Chronic Rhinosinusitis and Nasal Polyps Requiring Revision Surgery
Authors Hsieh SF ![]() , Wu PW
, Wu PW ![]() , Chiu CH, Huang YL
, Chiu CH, Huang YL ![]() , Huang CC
, Huang CC ![]()
Received 14 May 2025
Accepted for publication 20 September 2025
Published 26 September 2025 Volume 2025:18 Pages 13279—13289
DOI https://doi.org/10.2147/JIR.S540300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Sheng-Feng Hsieh,1,2,* Pei-Wen Wu,2– 4,* Cheng-Hsun Chiu,2,4,5 Yen-Lin Huang,6– 8 Chien-Chia Huang2– 4
1Department of Education, Chang Gung Memorial Hospital, Taoyuan, Taiwan; 2School of Medicine, Chang Gung University, Taoyuan, Taiwan; 3Division of Rhinology, Department of Otolaryngology, Chang Gung Memorial Hospital and Chang Gung University, Taoyuan, Taiwan; 4Molecular Infectious Disease Research Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan; 5Division of Pediatric Infectious Diseases, Department of Pediatrics, Chang Gung Memorial Hospital and Chang Gung University, Taoyuan, Taiwan; 6Department of Anatomic Pathology, Chang Gung Memorial Hospital, Taoyuan, Taiwan; 7School of Medicine, National Tsing-Hua University, Hsinchu, Taiwan; 8Institute of Stem Cell and Translational Cancer Research, Chang Gung Memorial Hospital, Taoyuan, Taiwan
*These authors contributed equally to this work
Correspondence: Chien-Chia Huang, Division of Rhinology, Department of Otolaryngology, Chang Gung Memorial Hospital and Chang Gung University, No. 5, Fu-Shin Street, Kweishan, Taoyuan, 333, Taiwan, Tel +886-3-3281200 ext 8466, Fax +886-3-3979361, Email [email protected]
Purpose: Endoscopic sinus surgery (ESS) is a safe and effective intervention for medically refractory pediatric chronic rhinosinusitis (CRS), particularly in older children and those with nasal polyposis. However, the histopathological characteristics associated with poor surgical outcomes in pediatric chronic rhinosinusitis with nasal polyposis (CRSwNP) have not been fully clarified. This study aimed to to identify histopathological characteristics of CRSwNP prognostic for revision surgery.
Methods: We retrospectively reviewed the medical records of 161 pediatric patients with CRSwNP including 22 patients with recurrent nasal polyps requiring revision surgery. The histopathological characteristics were compared between patients with and without revision surgery.
Results: Histopathological analysis revealed that the degree of inflammation, interstitial-gland percentage, mucosal ulceration, and numbers of eosinophils and goblet cells were significantly higher in participants who underwent revision surgery than in those who did not (all P< 0.05). The degree of inflammation (odds ratio [OR], 2.53; P=0.003), eosinophil count (OR, 1.03; P< 0.001), goblet-cell count (OR, 1.19; P=0.002), interstitial-gland percentage (OR, 1.99; P=0.012), and mucosal ulceration (OR, 3.37; P=0.013) were significantly associated with revision surgery in the univariate regression analysis. Receiver operating characteristic curve analysis identified 2.5 goblet cells per high-power field as the optimal cutoff value for predicting revision surgery, with a sensitivity of 77.3% and a specificity of 67.6%.
Conclusion: Histopathological features, including elevated eosinophil count, goblet-cell hyperplasia, marked mucosal inflammation, interstitial-gland hyperplasia, and mucosal ulceration, were associated with the need for revision in pediatric patients with CRSwNP. These findings could help clinicians stratify disease severity and tailor therapeutic approaches.
Plain Language Summary: This study retrospectively reviewed the medical records of 161 pediatric patients with chronic rhinosinusitis and nasal polyps including 22 patients with recurrent nasal polyps requiring revision surgery. Histopathological features, including elevated eosinophil count, goblet-cell hyperplasia, marked mucosal inflammation, interstitial-gland hyperplasia, and mucosal ulceration, were associated with the need for revision in pediatric patients with chronic rhinosinusitis and nasal polyps. These findings could help clinicians stratify disease severity and tailor therapeutic approaches.
Keywords: endoscopic sinus surgery, goblet cell, histopathology, nasal polyp, pediatric chronic rhinosinusitis
Introduction
Chronic rhinosinusitis (CRS) with nasal polyposis (CRSwNP) is one of the two major phenotypes of CRS and is characterized by persistent inflammation of the sinonasal mucosa for >3 months with the formation of nasal polyps.1,2 The estimated prevalence of CRSwNP in the pediatric population is 0.1%, which is lower than that in adults.3 The symptoms of CRSwNP include nasal congestion, nasal discharge, coughing, and facial pain/pressure. CRSwNP usually has a significant negative impact on sleep, school performance, social interaction, and the overall development and long-term well-being of affected children.4
Endoscopic sinus surgery (ESS) is a safe and effective intervention for medically refractory pediatric CRS, particularly in older children and those with nasal polyposis.5–7 By removing obstructive polyps and inflammatory secretions, ESS facilitates the restoration of normal sinus ventilation and drainage, creates a route for nasal irrigation and topical drug delivery, and leads to improvements in sinonasal symptoms and the quality of life of patients.5 Nevertheless, polyp relapse and the need for revision surgery remain concerns, with previous studies reporting a revision surgery rate of 12.8%.8,9
The histopathological features of nasal polyps,such as such as inflammatory-cell predominance, subepithelial edema, and eosinophil aggregates, are associated with poor outcomes after surgery in adults and are useful for predicting the likelihood of requiring revision surgery.10,11 These findings have helped guide individualized perioperative management, such as preoperative medication, including the use of biologic therapy; extent of surgical intervention; and intensity and extent of postoperative care, to optimize disease control and improve quality of life.12 However, the histopathological characteristics of pediatric CRSwNP associated with poor surgical outcomes have not been fully elucidated, owing to its low prevalence and limited availability of tissue samples.
To the best of our knowledge, no previous study has investigated the differences in the histopathological characteristics of pediatric CRSwNP according to the need for revision surgery. Therefore, this retrospective study aimed to identify useful histopathological characteristics of the nasal tissue removed during ESS for predicting the need for revision surgery in pediatric patients with CRSwNP.
Materials and Methods
Patients
Pediatric patients (age <18 years) who underwent ESS for CRSwNP at the Department of Otolaryngology at our institute between 2004 and 2017 were retrospectively identified from the histopathological database and subsequently confirmed via a manual review of medical records. CRSwNP was diagnosed based on the EPOS 2020 criteria.1 The presence of nasal polyps was confirmed by endoscopic examination and histopathological analysis. Patients were excluded if they met any of the following criteria: (1) presence of benign or malignant sinonasal neoplasms; (2) concomitant diagnosis of cystic fibrosis, primary ciliary dyskinesia, or immunologic disorders; and (3) follow-up period <12 months.
The clinical, laboratory, and imaging data of the participants were collected and reviewed. Eosinophilia was defined as a blood eosinophil count of >5% of circulating leukocytes.13 Disease severity was quantified on computed tomography images using the Lund–Mackay score.14 In patients with bilateral lesions, the average of the scores for both sides was used for analysis. The initial ESS was tailored based on the abnormalities observed on preoperative computed tomography, whereas revision procedures involved more extensive surgical intervention. Surgeries were performed by seven experienced rhinologists, and recurrence rates were compared among the surgeons. All patients were followed up postoperatively at our institution. In this study, recurrence was defined solely as the need for revision surgery, which was consistently documented in our institutional medical records. Other follow-up parameters, such as symptom scores or endoscopic findings, were not included as recurrence criteria in the present analysis. All patients who underwent revision surgery had also received their primary surgery at our institution, ensuring consistency in surgical technique and pathological specimen handling. Although surgeries were performed by seven different experienced rhinologists, all followed the same departmental surgical principles and perioperative management protocols.
The study protocol was reviewed and approved by the Institutional Review Board of Chang Gung Memorial Hospital (IRB number: 202201253B0). All procedures were conducted in accordance with the relevant ethical guidelines and regulations, and the Declaration of Helsinki. Considering the retrospective nature of this study and collection of anonymized data, the requirement for informed consent was waived.
Histopathological Evaluation
All specimens were obtained at our institution and processed in the same Department of Pathology using standardized protocols throughout the study period to ensure consistency in specimen preparation and quality. Mucosal specimens obtained during ESS were fixed using formalin and embedded in paraffin. Standard 5-µm sections were stained with hematoxylin and eosin (H&E). Based on previous histopathological studies on CRS, we selected the following nine characteristics for analysis: degree of inflammation, interstitial-gland percentage, epithelial hyperplasia, subepithelial fibrosis, subepithelial edema, mucosal ulceration, basement-membrane thickening, number of eosinophils per high-power field (HPF, 400× magnification), and number of goblet cells per HPF.15
The degree of inflammation was categorized into three levels—mild (lowest one-third), moderate (middle one-third), and severe (highest one-third)—based on the extent of inflammatory cell infiltration (Figure 1a–c), to facilitate a structured analysis of inflammatory severity.15,16 To evaluate interstitial-gland hyperplasia, the areas exhibiting the most severe glandular hyperplasia under low-power magnification (100×) were selected. The severity of hyperplasia was classified into three levels: mild (<35%, score 1), moderate (35%–70%, score 2), and severe (>70%, score 3) (Figure 1d–f).
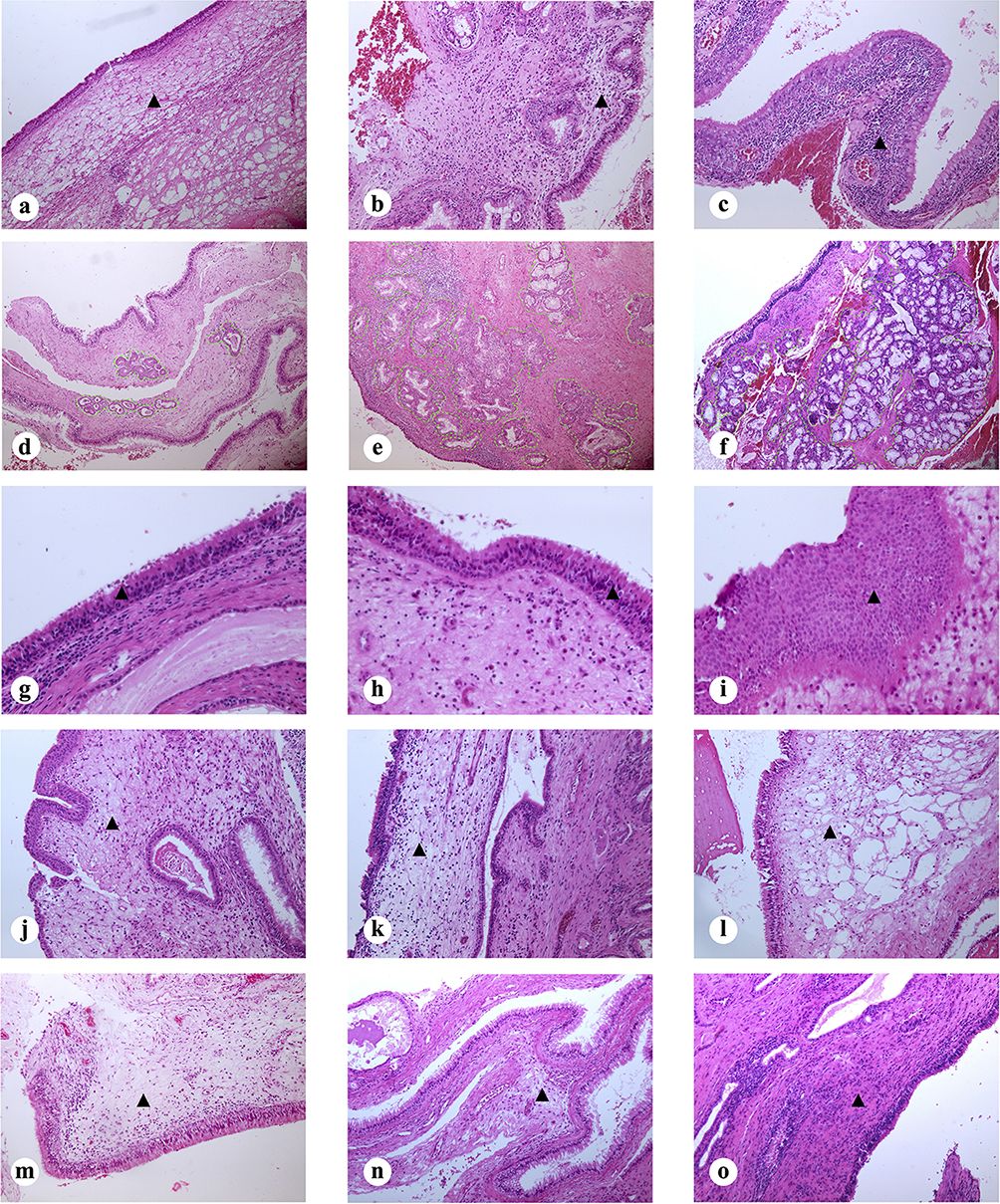 |
Figure 1 Representative histopathological images of degree of inflammation ((a), mild; (b), moderate; (c), severe. Arrowheads indicate inflammatory cell infiltration. Magnification 100X), interstitial gland percentage ((d), mild; (e), moderate; (f), severe. Dashed lines outline interstitial gland areas. Magnification 100X), epithelial hyperplasia ((g), mild; (h), moderate; (i), severe. Arrowheads mark the epithelium. Magnification 200X), subepithelial edema ((j), mild; (k), moderate; (l), severe. Arrowheads indicate areas of edema. Magnification 200X), subepithelial fibrosis ((m), mild; (n), moderate; (o), severe. Arrowheads denote fibrotic regions. Magnification 200X). |
Epithelial hyperplasia was categorized into four levels based on the number of epithelial-cell layers: none (<3 layers, score 0), mild (3–5 layers, score 1), moderate (6–8 layers, score 2), and severe (>8 layers, score 3) (Figure 1g–i). Similarly, the degree of subepithelial edema was stratified into none (absent, score 0), mild (<10% involvement, score 1), moderate (10–50% involvement, score 2), and severe (>50% involvement, score 3) (Figure 1j–l). Subepithelial fibrosis was classified into three levels: mild (<50% involvement, score 1), moderate (50–90% involvement, score 2), and severe (>90% involvement, score 3) (Figure 1m–o).
Mucosal ulceration (Figure 2a and b), basement-membrane thickening (Figure 2c and d) and goblet cells proliferation (Figure 2e and f) were assessed as either absent or present. Predominant type of inflammatory cell was also determined as eosinophilic inflammation or lymphoplasmacytic inflammation (Figure 2g and h). Tissue eosinophils were counted in the three HPFs with the most severe inflammatory-cell infiltrations in each tissue section, and the average of the three values was used for analysis. Similarly, for goblet-cell quantification, in the average of counts from three distinct HPFs was used for analysis. Type 2 CRSwNP was defined as the presence of ≥10 tissue eosinophils per HPF.
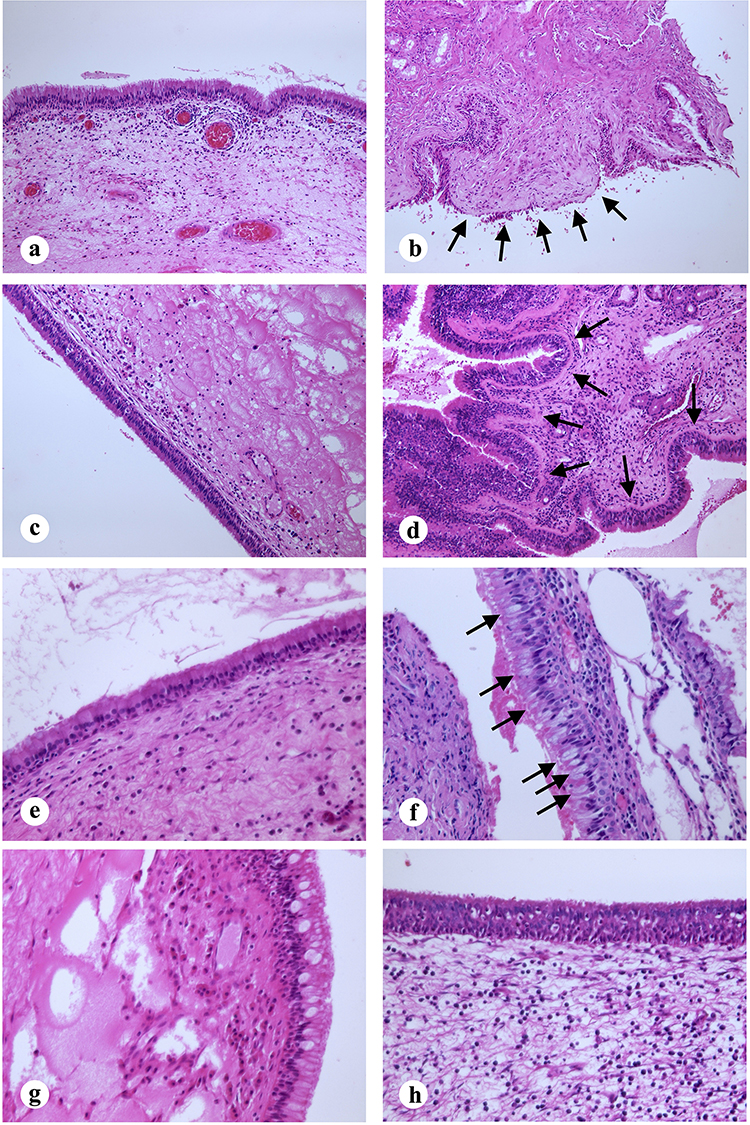 |
Figure 2 Representative histopathological images of mucosal ulceration (a), absence; (b), presence. Arrows indicate areas of mucosal ulceration. Magnification 200X), basement membrane thickening ((c), absence; (d), presence. Arrows highlight the thickened basement membrane. Magnification 200X), goblet cells proliferation ((e), absence; (f), presence. Arrows point to goblet cell hyperplasia. Magnification 400X), predominant type of inflammation (g)), eosinophilic inflammation; (h), lymphoplasmacytic inflammation. Magnification 400X). |
Statistical Analysis
All statistical analyses were performed using SPSS software (version 27.0; IBM Corp., Armonk, NY, USA) and GraphPad Prism 5 (GraphPad Prism Software Inc., San Diego, CA, USA). Continuous variables are expressed as medians ± interquartile ranges. Categorical variables are presented as counts and percentages. Chi square test or Fisher’s exact test was used to compare categorical variables, and the Mann–Whitney U-test was used to compare continuous variables. Logistic regression analyses were used to assess the association between revision surgery and histopathological features by calculating the odds ratios (ORs) with 95% confidence intervals (CIs). To identify the optimal cutoff values for histopathological features to predict the need for revision surgery, receiver operating characteristic (ROC) curves were constructed, and the areas under the curves (AUC) were calculated. Statistical significance was set at P < 0.05. The calculated post-hoc power was 87.3% of the difference between the primary outcomes in the study groups. Prior to conducting multivariate logistic regression, multicollinearity among the independent variables was assessed by calculating variance inflation factors (VIF) through linear regression modeling.
Results
Clinical Characteristics of Participants
A total of 161 patients diagnosed with CRSwNP, including 64 girls and 97 boys, were included in the study. Twenty-two (13.7%) patients underwent revision surgery. Baseline demographic characteristics of the entire cohort, along with comparisons between patients who underwent revision surgery and those who did not, are summarized in Table 1. The median patient age was 16.0 (1.8) years. The rates of revision surgery did not differ significantly among the surgeons or across different years.
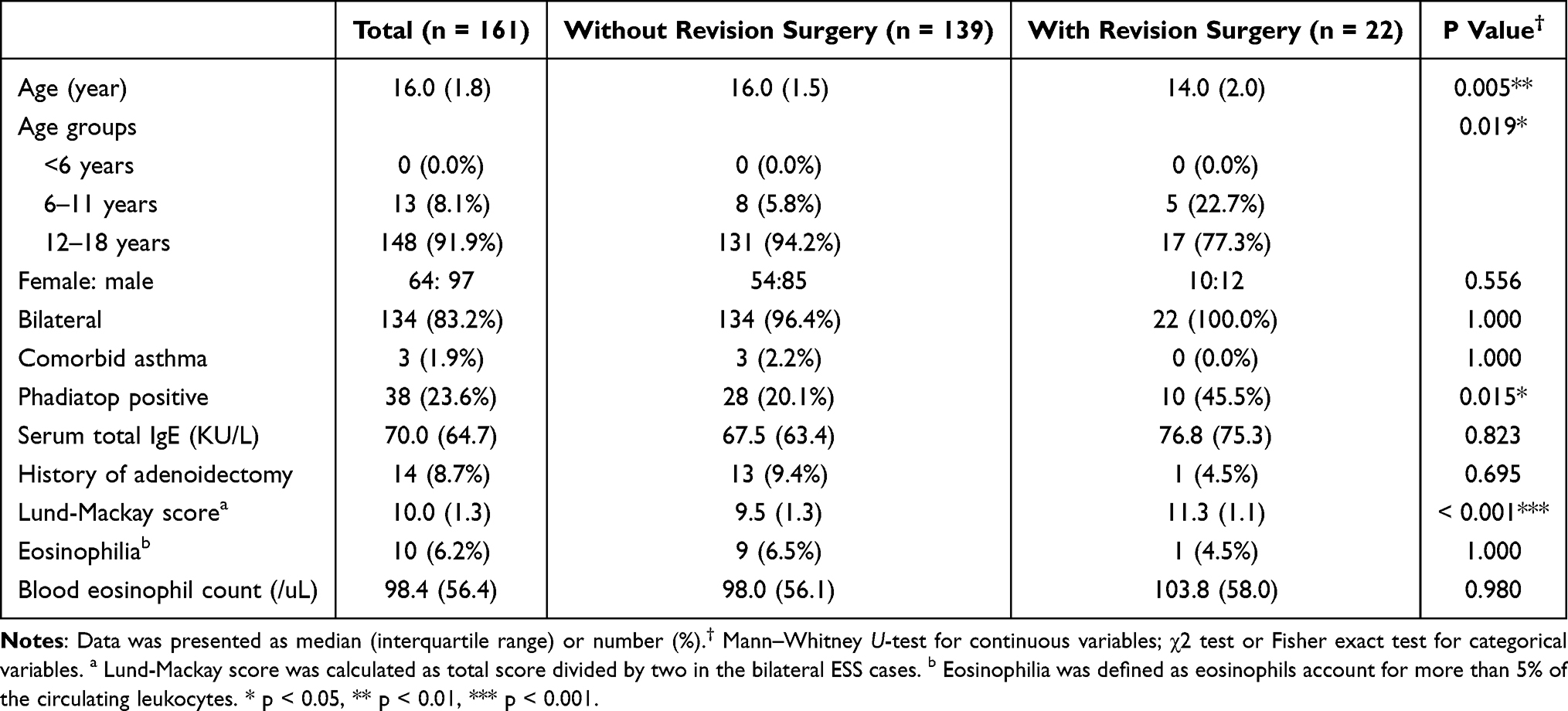 |
Table 1 Clinical Characteristics of the Study Population |
Bilateral nasal polyps and comorbid asthma were observed in 134 (83.2%) and 3 (1.9%) patients, respectively. Inhalant allergy test using ImmunoCAP Phadiatop (ThermoFisher Scientific, Uppsala, Sweden) was positive in 38 patients (23.6%), and the median serum immunoglobulin E (IgE) level was 70.0 (64.7) KU/L, demonstrating variability within the cohort. A history of adenoidectomy was reported in 14 patients (8.7%). The median Lund–Mackay score was 10.0 (1.3), and 10 patients (6.2%) exhibited eosinophilia. The median blood eosinophil count was 98.4 (56.4) /μL (Table 1).
Histopathological Characteristics
Histopathological analysis revealed that the degree of inflammation was significantly higher in participants who underwent revision surgery than in those who did not {2.0 (0.5) vs 1.0 (0.5), P=0.001}. Furthermore, the tissue eosinophil count per HPF was significantly higher in patients requiring revision surgery {33.0 (33.3) vs 12.0 (11.5), P<0.001)}. Similarly, goblet-cell hyperplasia was more pronounced in the revision surgery group than that in the no revision surgery group {median goblet-cell count, 3.7 (2.5) per HPF vs 1.6 (1.0) per HPF, P<0.001} (Figure 3a). Type 2 CRSwNP (defined as a tissue eosinophil count ≥10/HPF) was observed in 94 patients (58.4%) overall, including 18 patients (81.8%) in the revision surgery group and 76 patients (54.7%) in the non-revision group (P = 0.020). Mucosal ulceration was more frequently observed in patients undergoing revision surgery (68.2% vs 38.8%, P=0.012), and the percentage of interstitial-gland involvement was higher in this group {2.0 (1.0) vs 1.0 (0.5), P=0.019}. However, other histopathological parameters, including basement-membrane thickening, epithelial hyperplasia, subepithelial edema, and subepithelial fibrosis were not significantly different between the groups (Table 2).
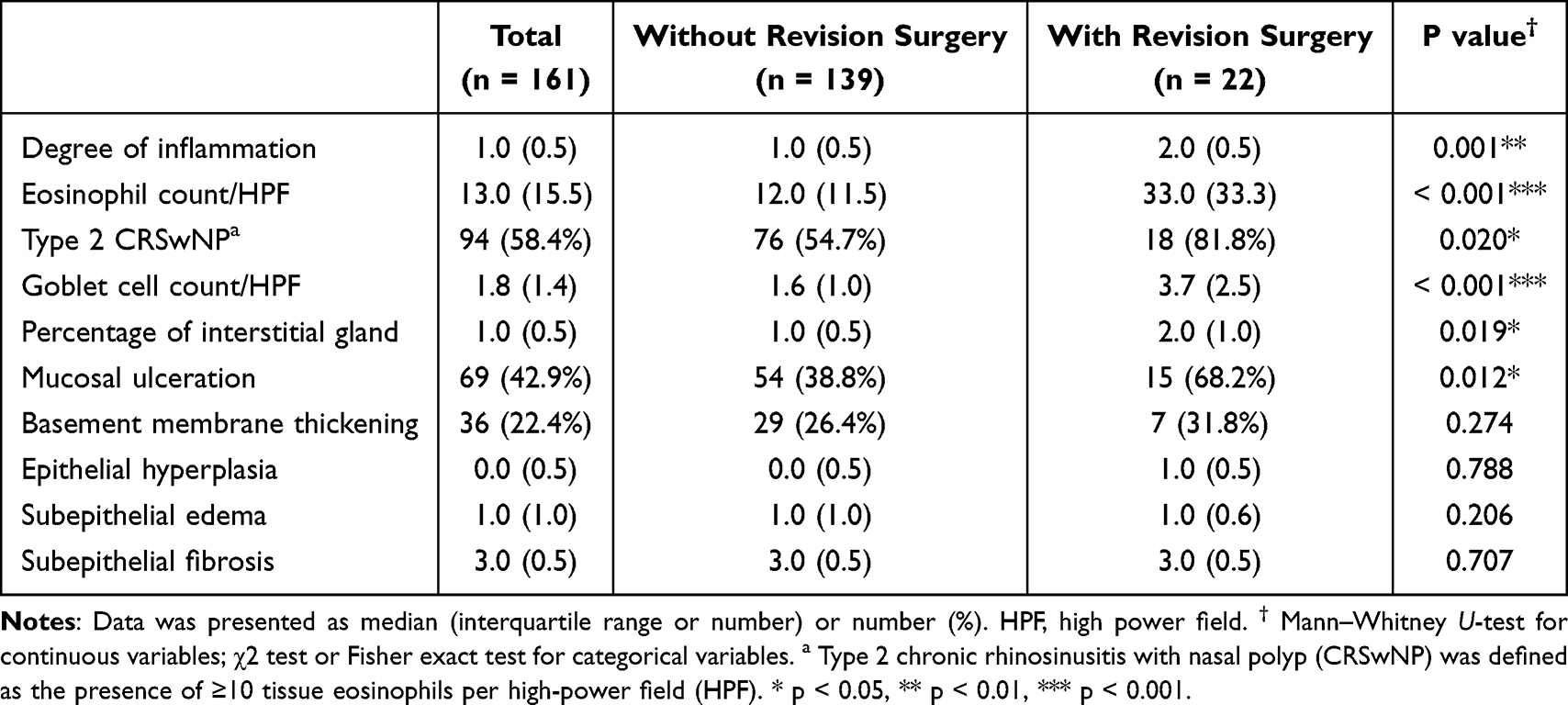 |
Table 2 Histopathologic Characteristics of the Study Population |
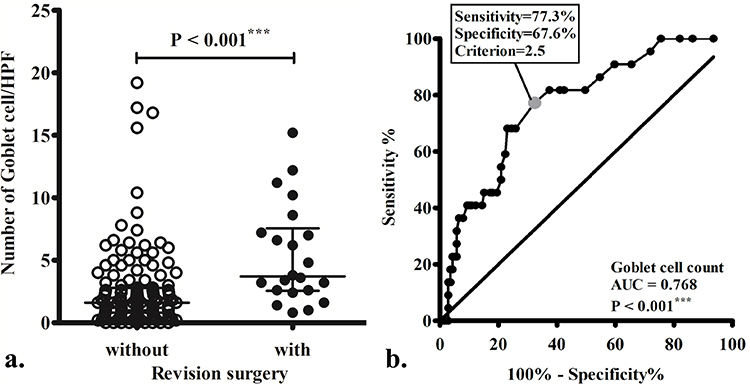 |
Figure 3 Quantitative analysis and diagnostic performance of goblet cell count. (a) Scatter plot comparing goblet cell count between patients with and without revision surgery. A statistically significant difference is observed between the two groups (P < 0.001). (b) Receiver operating characteristic curve assessing the diagnostic value of goblet cells count. The area under the curve (AUC = 0.768, P < 0.001), along with the optimal cutoff value of 2.5 showing the best predictive power for revision surgery after endoscopic sinus surgery (sensitivity = 77.3%; specificity = 67.6%). *** P < 0.001. |
Logistic Regression Analyses of the Histopathological Variables for Revision Surgery
In the univariate regression analysis, several factors were significantly associated with revision surgery, including degree of inflammation (OR, 2.53; P=0.003), eosinophil count per HPF (OR, 1.03; P<0.001), goblet-cell count per HPF (OR, 1.19; P=0.002), interstitial-gland percentage (OR, 1.99; P=0.012), and mucosal ulceration (OR, 3.37; P=0.013) were significantly associated with revision surgery.
No significant multicollinearity was detected among the independent variables included in the multivariate logistic regression model (VIF < 2). In the multivariate regression analysis, the degree of inflammation (OR, 2.30; P=0.028), eosinophil count per HPF (OR, 1.031; P<0.001), and goblet-cell count per HPF (OR, 1.201; P=0.004) were significantly associated with revision surgery (Table 3).
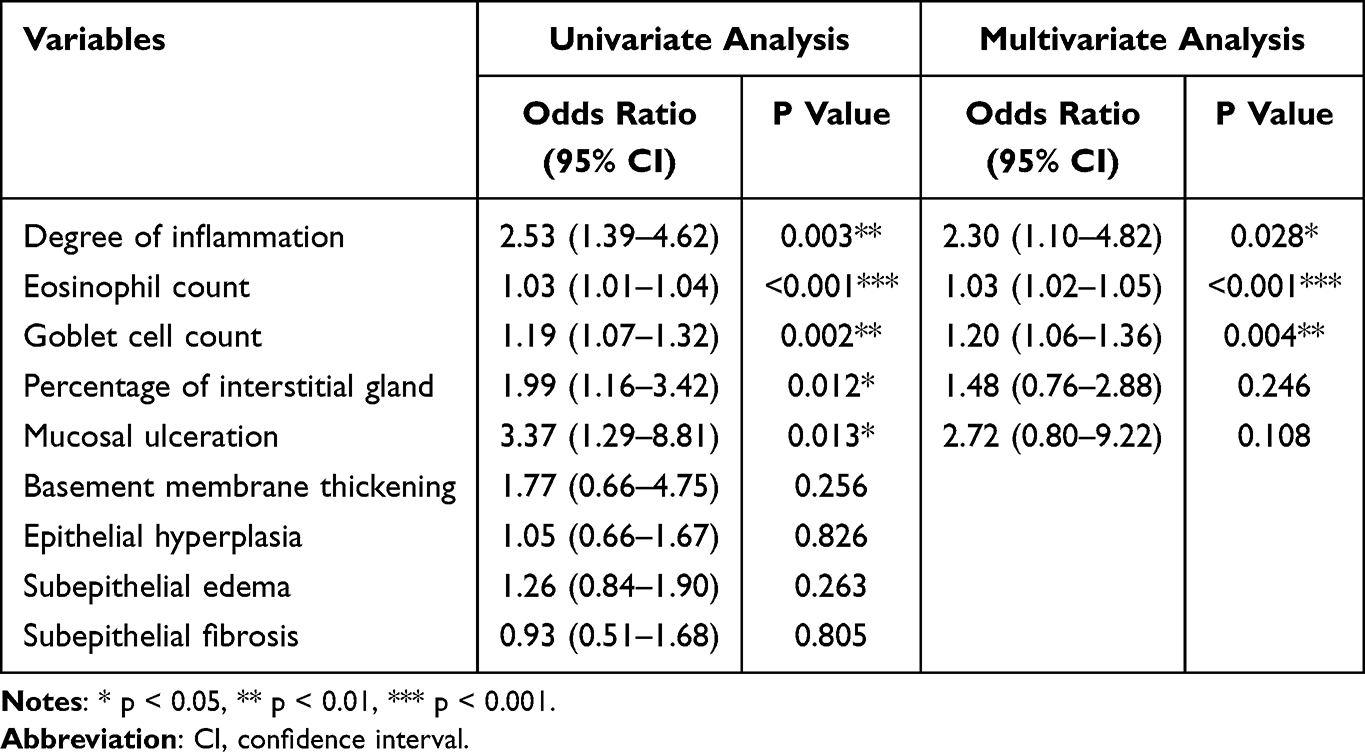 |
Table 3 Logistic Regression Analyses of the Variables for Revision Surgery |
Association of Goblet-Cell Count with the Need for Revision Surgery
The AUC for the goblet-cell count was 0.768 (P<0.001). The optimal cutoff value for predicting revision surgery was 2.5 goblet cells per HPF, with a sensitivity of 77.3% and specificity of 67.6% (Figure 3b). Similarly, the AUC for the tissue eosinophil count was 0.743; the optimal cutoff value was 21.5 eosinophils per HPF, with a sensitivity of 68.2% and a specificity of 69.1%.
Discussion
In this study, a higher degree of inflammation, eosinophilic infiltration, goblet-cell hyperplasia, interstitial-gland hyperplasia, and mucosal ulceration were significantly more prevalent in patients requiring revision surgery. Moreover, both goblet-cell and eosinophil counts emerged as independent indicators for predicting the likelihood of revision surgery.
The sinonasal epithelium and its underlying mucosa function as active organs that defend against external stimuli by dynamically modulating their tissue architecture.16–19 In this study, we identified several variables that were significantly associated with disease recurrence, including the degree of inflammation, mucosal integrity, and number of mucus-secreting cells. Our study revealed that both interstitial-gland percentage and goblet-cell count were significantly higher in patients who underwent revision surgery, suggesting that a higher mucus-secreting-cell count may represent a heavier disease burden in pediatric patients with CRSwNP. According to the EPOS definition, a key difference in clinical diagnosis between adults and children lies in symptom presentation; adults often report a reduction or loss of smell, whereas children more commonly present with cough.1 Our findings offer a plausible explanation for this. An increased number of mucus-secreting cells may alter both the composition and volume of the mucus, contributing to coughing. This symptom burden, in turn, may affect the patient’s or caregiver’s decision regarding revision surgery, although it may also be attributed to children’s limited ability to articulate their symptoms and the generally more conservative treatment approach in pediatric care.20–22 In our study, goblet-cell count was identified as an independent variable for predicting the recurrence of CRSwNP. A cutoff value of 2.5 goblet cells per HPF effectively distinguished recurrent from non-recurrent cases, with an AUC of 0.768, sensitivity of 77.3%, and specificity of 67.6%. Considering that our study cohort consisted of pediatric patients whose epithelial tissues are typically thinner and more intact, precise quantification of goblet-cell counts was feasible.23,24 This quantifiable parameter may serve as a valuable marker in clinical practice, aiding clinicians in identifying pediatric patients at increased risk of recurrence and facilitating individualized postoperative management strategies.25,26
In our cohort, the prevalence of type 2 CRSwNP (defined as a tissue eosinophil count ≥10/HPF) was higher in patients requiring revision surgery compared to those without revision (81.8% vs 54.7%). This suggests that type 2 eosinophilic inflammation may be associated with poorer surgical outcomes, consistent with adult CRSwNP literature, where type 2 inflammation is a well-recognized predictor of recurrence.1 These findings indicate that type 2 endotyping remains relevant in pediatric patients and may aid in postoperative risk stratification. However, although the eosinophil count was an independent predictor of revision surgery in our cohort, previous studies have shown that its prognostic value in children is generally less pronounced than in adults,20,24 reflecting differences in the underlying inflammatory profile.
Snidvongs et al reported that pediatric CRS is predominantly characterized by neutrophilic, macrophagic, and lymphocytic infiltration.20 Similarly, Mahdavinia et al observed a more prominent lymphocytic infiltration in children, whereas adult patients tended to exhibit a stronger eosinophilic response along with marked glandular hyperplasia.27 Furthermore, Berger et al reported that the inflammatory pattern in pediatric CRS was dominated by chronic inflammatory-cell infiltration and fibrosis within the lamina propria, with only sparse eosinophils observed.23 This histological distinction is consistent with the findings of Chan et al, who reported that the density of submucosal eosinophils was significantly lower in children than in adults.24 In our study, the tissue eosinophil count was 13.0 ± 15.5 per HPF, which is markedly lower than the values typically reported in adults. These findings imply that the eosinophilic inflammatory response in children may be lower than that in adults, possibly because of their relatively immature immune system. This may also explain the observed increase in the number of mucus-secreting cells as a compensatory response.28 This emphasizes the importance of identifying alternative histopathological markers in children.
The prevalence of comorbid asthma reported in our study cohort was lower than that in previous reports. The lack of comprehensive pulmonary assessments prior to surgery in the majority of patients, combined with reliance solely on medical chart reviews, may have resulted in undiagnosed or unrecorded cases of asthma among our participants. However, previous studies on adult CRS reported a lower prevalence of comorbid asthma and type 2 inflammation in Asian patients with CRSwNP (10–20%), compared to those in Western countries (40–60%).29 Additionally, the prevalence of CRSwNP and concomitant asthma increases with age.30,31 Furthermore, a previous study also revealed that asthma remained undiagnosed in many patients with CRSwNP.32 Taken together, asthma may be easily undiagnosed due to its relatively low prevalence in pediatric CRSwNP. Future studies with comprehensive pulmonary evaluations for asthma comorbidity in pediatric patients with CRSwNP are necessary.
In this study, all key histopathological markers were identified using routine H&E staining, and they exhibited consistent visibility and quantifiability under standard evaluation protocols. These findings have immediate clinical applicability, as they can be readily incorporated into histopathological reports to assist in postoperative risk stratification and guide the intensity of follow-up care. Their measurable and reproducible natures make them ideal input variables for artificial intelligence-based image-recognition models aimed at predicting surgical recurrence.33 Together, these dual strengths underscore the broader significance of our results, suggesting that they may not only inform current clinical practice, but also contribute to the development of artificial intelligence-assisted diagnostic tools in the future.34,35 In addition, our study provides a detailed characterization of the inflammatory patterns in pediatric CRSwNP, offering valuable histological insights into this relatively underexplored population.
Several limitations of our study must be acknowledged. First, the retrospective design of our study has several inherent limitations, including missing data, non-standardized clinical information, and insufficient long-term follow-up. Second, the homogeneity and comparability across surgical teams cannot be assured due to the retrospective nature of the review. However, surgical principles and perioperative management protocols were similar among the surgeons, and the rates of revision surgery did not differ significantly between surgeons or across different years within the current study cohort. Although surgical principles and perioperative management protocols remained consistent among surgeons during the study period, diagnostic and therapeutic approaches for pediatric CRSwNP may have gradually evolved over the 13 years. These changes were not specifically evaluated in the analysis. Third, our cohort was recruited from a single tertiary referral medical center, introducing a potential selection bias and limiting the generalizability of our findings owing to variations in patient characteristics and treatment approaches across different hospitals and regions, especially considering the significant heterogeneity observed in CRSwNP. However, patients with severe disease burden are also prone to resistance to therapy and require comprehensive evaluations. Finally, our study evaluated treatment success solely based on the need for revision surgery without considering other crucial clinical outcomes such as symptom improvement or quality-of-life measures. Future studies should incorporate comprehensive clinical assessment tools to facilitate better clinical management and holistic prognostic evaluations.36,37
Conclusion
Histopathological features, including elevated eosinophil count, goblet-cell hyperplasia, marked mucosal inflammation, interstitial-gland hyperplasia, and mucosal ulceration, were associated with the need for revision in pediatric patients with CRSwNP. Incorporating these histopathological characteristics into routine evaluations may aid clinicians in stratifying disease severity and tailoring the intensity of postoperative adjunctive therapies and follow-up care.
Abbreviations
ESS, Endoscopic sinus surgery; CRS, chronic rhinosinusitis; CRSwNP, chronic rhinosinusitis with nasal polyp; OR, odds ratio; H&E, hematoxylin and eosin; HPF, high-power field; CI, confidence interval; ROC, Receiver operating characteristic; AUC, area under the curve; IgE, immunoglobulin E; VIF, variance inflation factors.
Funding
The authors received research grants from the Chang Gung Memorial Hospital (CMRPG3P0351 and CMRPG3P0571) and the Taiwan National Science and Technology Council (114-2314-B-182-031-MY2). The funder played no role in the study design, data collection and analysis, decision to publish, or manuscript preparation.
Disclosure
The authors declare no conflicts of interest.
References
1. Fokkens WJ, Lund VJ, Hopkins C. et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology. 2020;58(Suppl S29):1–464. doi:10.4193/Rhin20.401
2. Min HK, Lee S, Kim S, et al. Global Incidence and Prevalence of Chronic Rhinosinusitis: a Systematic Review. Clin Exp Allergy. 2025;55(1):52–66. doi:10.1111/cea.14592
3. Settipane GA. Epidemiology of nasal polyps. Allergy Asthma Proc. 1996;17(5):231–236. doi:10.2500/108854196778662246
4. Hamilos DL. Pediatric chronic rhinosinusitis. Am J Rhinol Allergy. 2015;29(6):414–420. doi:10.2500/ajra.2015.29.4238
5. Vlastarakos PV, Fetta M, Segas JV, Maragoudakis P, Nikolopoulos TP. Functional endoscopic sinus surgery improves sinus-related symptoms and quality of life in children with chronic rhinosinusitis: a systematic analysis and meta-analysis of published interventional studies. Clin Pediatr. 2013;52(12):1091–1097. doi:10.1177/0009922813506489
6. Heath J, Hartzell L, Putt C, Kennedy JL. Chronic Rhinosinusitis in Children: pathophysiology, Evaluation, and Medical Management. Curr Allergy Asthma Rep. 2018;18(7):37. doi:10.1007/s11882-018-0792-8
7. Torretta S, Guastella C, Ibba T, Gaffuri M, Pignataro L. Surgical Treatment of Paediatric Chronic Rhinosinusitis. J Clin Med. 2019;8(5):684. doi:10.3390/jcm8050684
8. Wu PW, Huang CC, Yang SW, et al. Endoscopic sinus surgery for pediatric patients: prognostic factors related to revision surgery. Laryngoscope. 2020;130(4):1051–1055. doi:10.1002/lary.28106
9. Wu PW, Chiu CH, Huang YL, et al. Tissue eosinophilia and computed tomography features in paediatric chronic rhinosinusitis with nasal polyps requiring revision surgery. Rhinology. 2023;61(3):348–357. doi:10.4193/Rhin22.435
10. Bai J, Huang JH, Price CPE, et al. Prognostic factors for polyp recurrence in chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol. 2022;150(2):352–61.e7. doi:10.1016/j.jaci.2022.02.029
11. Calvanese L, Fabbris C, Brescia G, et al. Polyps’ Extension and Recurrence in Different Endotypes of Chronic Rhinosinusitis: a Series of 449 Consecutive Patients. J Clin Med. 2024;13(4):1125. doi:10.3390/jcm13041125
12. Wu PW, Huang CC, Chang PH, Lee TJ, Huang CC. The benefit of dupilumab as a postoperative short-term adjuvant therapy for chronic rhinosinusitis with nasal polyps: a preliminary study. Laryngoscope Investig Otolaryngol. 2024;9(4):e1296. doi:10.1002/lio2.1296
13. Tokunaga T, Sakashita M, Haruna T, et al. Novel scoring system and algorithm for classifying chronic rhinosinusitis: the JESREC Study. Allergy. 2015;70(8):995–1003. doi:10.1111/all.12644
14. Lund VJ, Kennedy DW. Staging for rhinosinusitis. Otolaryngol Head Neck Surg. 1997;117(3):S35–S40. doi:10.1016/S0194-5998(97)70005-6
15. Alobid I, Armengot-Carceller M, Pinilla Urraca M, et al. When the Nose Meets the Lab: histopathological Analysis in Chronic Rhinosinusitis with Nasal Polyps for Routine Clinical Practice. Curr Allergy Asthma Rep. 2024;24(12):657–665. doi:10.1007/s11882-024-01180-8
16. Carroll WW, O’Connell BP, Schlosser RJ, et al. Fibroblast levels are increased in chronic rhinosinusitis with nasal polyps and are associated with worse subjective disease severity. Int Forum Allergy Rhinol. 2016;6(2):162–168. doi:10.1002/alr.21636
17. Bae JS, Ryu G, Kim JH, et al. Effects of Wnt signaling on epithelial to mesenchymal transition in chronic rhinosinusitis with nasal polyp. Thorax. 2020;75(11):982–993. doi:10.1136/thoraxjnl-2019-213916
18. He Y, Fu Y, Wu Y, Zhu T, Li H. Pathogenesis and treatment of chronic rhinosinusitis from the perspective of sinonasal epithelial dysfunction. Front Med Lausanne. 2023;10:1139240. doi:10.3389/fmed.2023.1139240
19. Lamouille S, Xu J, Derynck R. Molecular mechanisms of epithelial-mesenchymal transition. Nat Rev Mol Cell Biol. 2014;15(3):178–196. doi:10.1038/nrm3758
20. Snidvongs K, Sangubol M, Poachanukoon O. Pediatric Versus Adult Chronic Rhinosinusitis. Curr Allergy Asthma Rep. 2020;20(8):29. doi:10.1007/s11882-020-00924-6
21. Ni JS, Kompelli AR, Nguyen SA, Schlosser RJ, Clemmens C, Soler ZM. The Sinus and Nasal Quality of Life Survey (SN-5) in the Management of Pediatric Chronic Rhinosinusitis: a systematic review and meta-analysis. Int J Pediatr Otorhinolaryngol. 2018;111:162–169. doi:10.1016/j.ijporl.2018.06.010
22. Ramadan HH. Pediatric chronic rhinosinusitis. Eur Arch Otorhinolaryngol. 2024;281(3):1131–1137. doi:10.1007/s00405-023-08307-z
23. Berger G, Kogan T, Paker M, Berger-Achituv S, Ebner Y. Pediatric chronic rhinosinusitis histopathology: differences and similarities with the adult form. Otolaryngol Head Neck Surg. 2011;144(1):85–90. doi:10.1177/0194599810390443
24. Chan KH, Abzug MJ, Coffinet L, Simoes EA, Cool C, Liu AH. Chronic rhinosinusitis in young children differs from adults: a histopathology study. J Pediatr. 2004;144(2):206–212. doi:10.1016/j.jpeds.2003.11.009
25. Xu X, Seet JE, Yap QV, et al. Latent class analysis of structured histopathology in prognosticating surgical outcomes of chronic rhinosinusitis with nasal polyps in Singapore. Rhinology. 2023;61(4):358–367. doi:10.4193/Rhin22.455
26. Cui Y, Wang K, Shi J, Sun Y. Endotyping Difficult-to-Treat Chronic Rhinosinusitis with Nasal Polyps by Structured Histopathology. Int Arch Allergy Immunol. 2023;184(10):1036–1046. doi:10.1159/000530864
27. Mahdavinia M, Grammer III LC. Chronic rhinosinusitis and age: is the pathogenesis different? Expert Rev Anti Infect Ther. 2013;11(10):1029–1040. doi:10.1586/14787210.2013.839380
28. Kao SS, Bassiouni A, Ramezanpour M, et al. Proteomic analysis of nasal mucus samples of healthy patients and patients with chronic rhinosinusitis. J Allergy Clin Immunol. 2021;147(1):168–178. doi:10.1016/j.jaci.2020.06.037
29. Yao Y, Zeng M, Liu Z. Revisiting Asian chronic rhinosinusitis in the era of type 2 biologics. Clin Exp Allergy. 2022;52(2):231–243. doi:10.1111/cea.14065
30. Wu PW, Chang PH, Huang CC, Lee TJ, Fan YH, Huang CC. Impact of Comorbid Asthma on Life Quality of Patients with Chronic Rhinosinusitis and Nasal Polyps. J Asthma Allergy. 2025;18:567–578. doi:10.2147/JAA.S517258
31. Huang CC, Chang PH, Huang YL, Lee TJ, Huang CC, Wu PW. Clinical Characteristics of Eosinophilic Chronic Rhinosinusitis with Nasal Polyps in Adolescents. J Asthma Allergy. 2023;16:1197–1206. doi:10.2147/JAA.S437876
32. Laidlaw TM, Mullol J, Woessner KM, Amin N, Mannent LP. Chronic Rhinosinusitis with Nasal Polyps and Asthma. J Allergy Clin Immunol Pract. 2021;9(3):1133–1141. doi:10.1016/j.jaip.2020.09.063
33. Hsu YC, Lin KT, Lee MS, Shen LS, Yeh TH, Lin YT. Multiple instance learning for eosinophil quantification of sinonasal histopathology images: a hierarchical determination on whole slide images. Int Forum Allergy Rhinol. 2024;14(9):1513–1516. doi:10.1002/alr.23365
34. Wu Q, Chen J, Deng H, et al. Expert-level diagnosis of nasal polyps using deep learning on whole-slide imaging. J Allergy Clin Immunol. 2020;145(2):698–701.e6. doi:10.1016/j.jaci.2019.12.002
35. Wang K, Ren Y, Ma L, et al. Deep learning-based prediction of treatment prognosis from nasal polyp histology slides. Int Forum Allergy Rhinol. 2023;13(5):886–898. doi:10.1002/alr.23083
36. Kay DJ, Rosenfeld RM. Quality of life for children with persistent sinonasal symptoms. Otolaryngol Head Neck Surg. 2003;128(1):17–26. doi:10.1067/mhn.2003.41
37. Rudnick EF, Mitchell RB. Improvements in quality of life in children after surgical therapy for sinonasal disease. Otolaryngol Head Neck Surg. 2006;134(5):737–740. doi:10.1016/j.otohns.2005.12.033
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors of Postoperative Residual Sinus Inflammation in Patients with Eosinophilic Chronic Rhinosinusitis and Nasal Polyps
Wu PW, Chang PH, Huang CC, Yen CI, Fan YH, Huang CC
Journal of Inflammation Research 2026, 19:576040
Published Date: 8 January 2026