Back to Journals » Infection and Drug Resistance » Volume 13
Risk Factors for Subsequential Carbapenem-Resistant Klebsiella pneumoniae Clinical Infection Among Rectal Carriers with Carbapenem-Resistant Klebsiella pneumoniae
Authors Chen X, Liu Q, Liu W, Yan Q
Received 23 January 2020
Accepted for publication 16 April 2020
Published 5 May 2020 Volume 2020:13 Pages 1299—1305
DOI https://doi.org/10.2147/IDR.S247101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eric Nulens
Xia Chen, Qingnuan Liu, Wen-en Liu, Qun Yan
Department of Clinical Laboratory, Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China
Correspondence: Qun Yan Tel +86-731-84327440
Fax +86-731-84327332
Email [email protected]
Purpose: Carbapenem-resistant Klebsiella pneumoniae (CRKP) infection has become a critical clinical concern for its high mortality. Rectal carriage of CRKP has been reported playing an important role in CRKP infection; however, the extent to which carrier develops clinical CRKP infection is unclear. This study aimed to identify risk factors for developing subsequential CRKP clinical infection in rectal carriers with CRKP.
Patients and Methods: Patients were screened for rectal carriage of CRKP in a tertiary university hospital; then, rectal CRKP carriers were divided into case group (those who developed subsequential clinical infection) and control group. Demographics, comorbid conditions, invasive procedures, antimicrobial exposure and other clinical parameters of those two groups were compared and analyzed using univariate and multivariate logistic regression analyses. Antimicrobial susceptibility profile and carbapenemase phenotype/genotype of those CRKP isolates were determined. MLST was applied to elucidate the molecular epidemiology of rectal CRKP isolates and clinical infection ones.
Results: Eight hundred and thirty-five patients were screened for rectal CRKP carriage. A total of 62 CRKP rectal carriers were identified; among them, 37.1% (23/62) developed CRKP clinical infection. CRKP isolates were resistant to most of the tested antimicrobial agents. ST11 was the dominant MLST type in rectal CRKP isolates (71.0%), and all the 23 clinical infection isolates were ST11. Multivariate analysis revealed that admission to the intensive care unit (ICU) (OR, 6.753; P=0.006), being in coma condition (OR, 11.085; P=0.015) and receiving central venous catheter (OR, 8.628; P=0.003) were independent risk factors for progressing to subsequential CRKP infection among those rectal carriers.
Conclusion: This study identified independent risk factors for developing subsequential CRKP clinical infection among CRKP rectal carriers, with being in coma condition as a new finding. It would help clinician target those high-risk rectal CRKP-colonized patients for prevention of subsequential clinical infection.
Keywords: carbapenem-resistant Klebsiella pneumoniae, infection, risk factors, rectal carriage
Introduction
Carbapenem-resistant Enterobacteriaceae (CRE) has been reported becoming a serious public health threat worldwide during recent years.1,2 Carbapenem-resistant Klebsiella pneumoniae (CRKP) has been recognized as the most frequently encountered CRE-producing carbapenemases including K. pneumoniae carbapenemases (KPCs), New Delhi metallo-β-lactamases (NDM), Verona integron-encoded metallo-β-lactamases (VIM), imipenem-hydrolyzing metallo-lactamases (IMP) or, the oxacillin-hydrolyzing metallo-β-lactamases (OXA) type carbapenemase,3–5 with KPC being the most common carbapenemase in US, China and other countries.6–9 CRKPs are often extremely drug resistant to most available antimicrobial agents and associated with high morbidity and mortality, as well as high cost.10 Thus, appropriate measures to control their infections are in urgent need.
Previous studies have shown that rectal carriage of CRE played an important role in disseminating those organisms within the hospital settings. Studies have investigated the prevalence of rectal carriage of CRE ranging from 0.3% to 69.5%.11–15 In our previous study, we found 8.5% hospitalized patients colonized with rectal CRE, and KPC-producing K. pneumoniae ST11 were the dominant clone. We further revealed the close clonal relatedness among most of those CRKP isolates.16 A number of studies have explored the risk factors for CRE rectal colonization and revealed several predictors including hospital readmissions, sickbed changes, invasive procedures, malignancy, surgery previous use of antimicrobial, and staying in ICUs were independent risk factors associated with CRE colonization.11,17,18 Though understanding the risk factors for rectal CRE colonization has been well addressed in previous studies, identifying the carrier who is prone to developing subsequential clinical infection is essential for targeting the population to implementing control measures, making the infection control measures efficiently. However, knowledge of risk factors associated with developing CRKP infection among rectal carrier is limited.19–21 In this study, we aimed to identify risk factors for developing CRKP clinical infection among CRKP rectal carrier and investigate the antimicrobial susceptibility profile and genotypes of those CRKP isolates.
Patients and Methods
Study Design
This study was conducted between December 2014 and January 2016 at Xiangya Hospital, which is a 3500-beds tertiary university hospital (68 wards) with an annual admission of more than 130,000 inpatients in Central-south of China. Hospitalized patients with stool samples submitted for routine analysis were screened for CRKP. Patients with rectal CRKP carriage and without prior positive clinical cultures for CRKP were then divided into case group and control group. Case group included CRKP rectal carriers who developed subsequential CRKP infections in the following 45 days after the first rectal CRKP identified, while control group included asymptomatic carriers.21 Demographics, comorbid conditions, invasive procedures, antimicrobial exposure and other clinical parameters among those two groups were compared.
Data Collection
All data were extracted from the electronic medical records including 1) demographics: gender, age, length of hospital stay, previous hospitalization, history of smoking, history of alcohol, intensive care unit (ICU) admission, hospital transfer and sickbed change; 2) Comorbid conditions: solid tumor, hypertension, heart disease, diabetes mellitus, hematopathy, lung disease, renal disease, liver disease, pancreatitis, enteritis, gastritis, craniocerebral trauma; 3) Invasive procedures: arterial catheter, central venous catheter, endotracheal intubation, tracheotomy, mechanical ventilation, urinary catheter and nasogastric tube; 4) Other clinical parameters: previous surgery in one month and in three months, coma condition (the Glasgow Coma Scale (GCS) score ≤ 8);22 and 5) Antimicrobial exposure within 4 weeks of rectal CRKP detected including penicillin, cephalosporins, carbapenems, aminoglycosides, fluoroquinolones, β-lactam/β-lactamase inhibitors, vancomycin, tigecycline, metronidazole and antifungal agents. CRKP clinical infection included bloodstream infection, pneumonia, peritonitis, wound infection, urinary tract infection, etc., with CRKP isolated in relevant infection sites and having the signs and symptoms meet the criteria of the corresponding infection definition.23
Microbiological Methods
Stool samples were screened for CRKP as previous described,16 clinical samples were cultured and organisms identification was performed using MALDI Biotyper (Bruker, Germany). Antimicrobial susceptibility testing was carried out by Vitek 2 (bioMerieux, France). E. coli strain ATCC 25922 was used for quality control. Results were interpreted using the Clinical and Laboratory Standards Institute (CLSI) breakpoints for all the antimicrobial agents except tigecycline,24 which were interpreted using the European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoints standards from 2014 (http://www.eucast.org/clinical_breakpoints/). Confirmation of carbapenemase phenotype was performed by CarbaNP test.25
Detection of Genotypes
The presence of carbapenemase encoding genes (KPC, NDM, IMP, VIM, and OXA-48) were identified by polymerase chain reaction (PCR) as previously described.16 PCR products were sequenced (Sangon, Shanghai, China) and then confirmed by using BLAST programs (http://blast.ncbi.nlm.nih.gov/Blast.cgi). The clonal relatedness of carbapenem-resistant K. pneumoniae isolates was analyzed by multilocus sequence typing (MLST).16
Statistical Analysis
Continuous variables were analyzed by Student’s t test (normally distributed variables) or the wilcoxon rank-sum test (non normally distributed variables), and categorical variables were compared by Chi-square test or Fisher’s exact test. The odds ratio (OR) and 95% confidence intervals (95% CI) were calculated. A two-tailed P-value≤0.05 in the univariate analysis were entered into the logistic regression model for the multivariate analysis, in which variables with P-value≤0.05 was considered statistically significant. Then, identified independent risk factors were checked for multicollinearity. Data were analyzed by using SPSS version 22.0 software (IBM corporation, USA).
Ethics
This study was reviewed and approved by the Ethics Committee of Xiangya Hospital of Central South University in accordance with the Declaration of Helsinki and its amendments or comparable ethical standards. The written informed consent was waived due to the noninterventional and retrospective nature of the study, all patient data were analyzed in anonymity, this retrospective study did not directly interfere with any patient and there was no adverse effect on the rights of patients.
Results
Clinical Characteristics
A total of 835 patients from all 68 wards were screened for rectal CRKP colonization in this study, including 105 patients from the central intensive care unit (ICU), 89 from the respiration wards, 68 from the pediatric wards, 59 from the gastroenterology wards, 56 from the infections wards, 53 from the hematology wards, 41 from the traditional Chinese medicine ward. The rest 364 patients were originated from other wards ranging from 1 to 28 patients in one ward. Among the 835 patients, 7.4% (62/835) patients were identified as CRKP rectal carriers. Twenty-three carriers (37.1%, 23/62) developed CRKP clinical infection in the later period, while 39 carriers did not. The majority clinical infections were pneumonia (16, 69.6%), followed by urinary tract infection (2, 8.7%), bloodstream infection (2, 8.7%), wound infection (1, 4.3%), peritonitis (1, 4.3%), and multiple sites infection (1, 4.3%).
Antimicrobial Susceptibility
Antimicrobial-resistant rate of rectal CRKP isolates between case group and control group is shown in Table 1. Although the antimicrobial-resistant rate of rectal CRKP isolates between the case group and control group showed no statistically significant difference, rectal CRKP isolates from case group had higher antimicrobial-resistant rate than those from control group, and they were resistant to most tested antimicrobial agents. In case group, CRKP isolates originated from clinical infection sites presented the exact same antimicrobial susceptibility phenotype as their rectal counterparts.
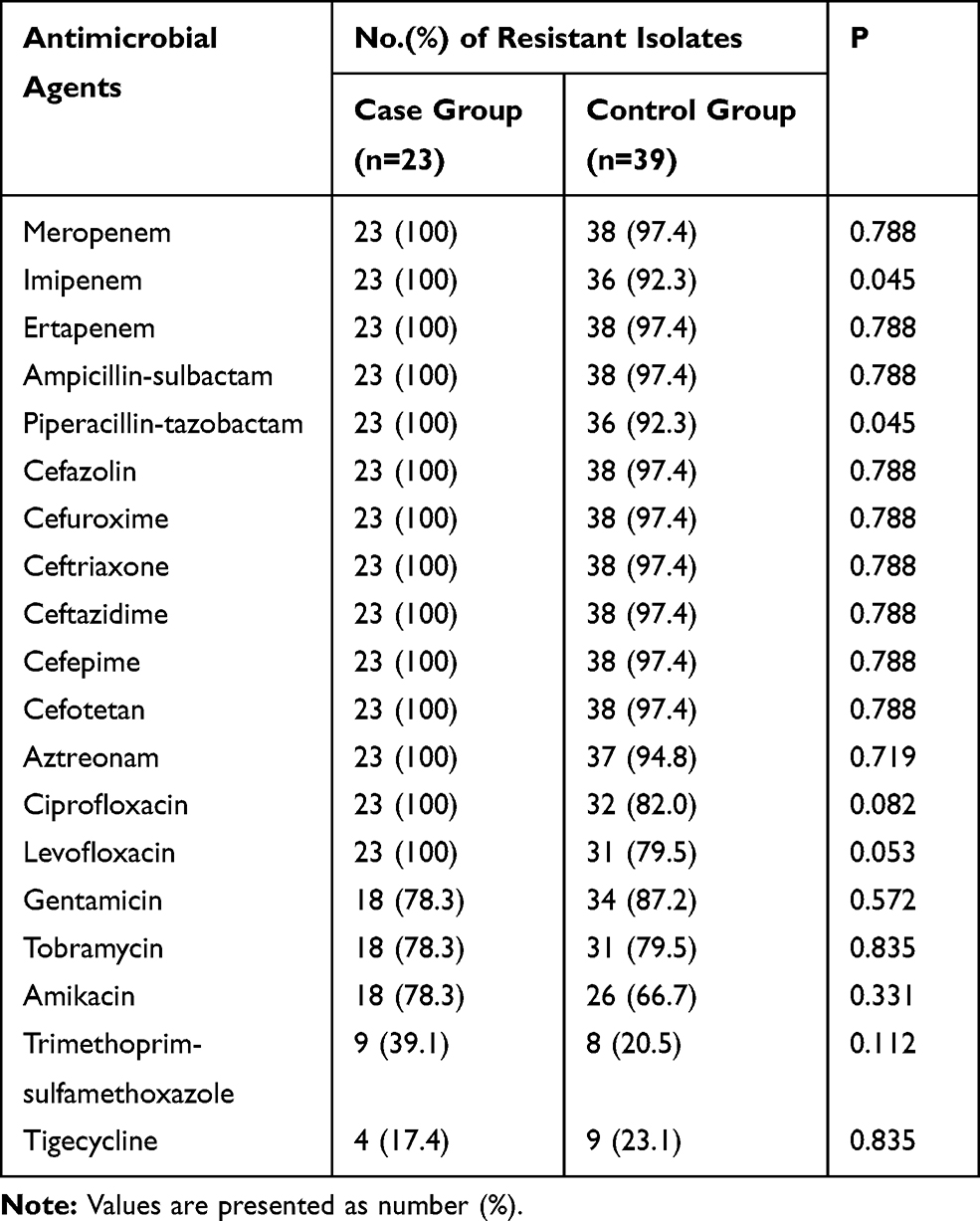 |
Table 1 Antimicrobial Resistance of Rectal Carbapenem-Resistant Klebsiella pneumoniae Isolates |
Genotypic Characteristics
In case group, all rectal CRKP isolates produced KPC carbapenemase, with one isolate co-producing both KPC and NDM, and one isolate co-producing both KPC and IMP. Also shown in control group, most isolates (97.4%, 38/39) produced KPC, 5.1% (2/39) produced NDM, and 2.6% (1/39) produced IMP. VIM and OXA-48 were not detected. There was no significant difference of the carbapenemase genes detected between case group and control group (Table 2). All CRKP isolates originated from clinical infection sites also produced KPC. ST11 were the dominant MLST type (44/62, 71.0%) among rectal K. pneumoniae isolates. Other ST types included ST208, ST307, ST309, ST414, ST722, ST1466 and ST1899. All the clinical CRKP isolates were also ST11 type.
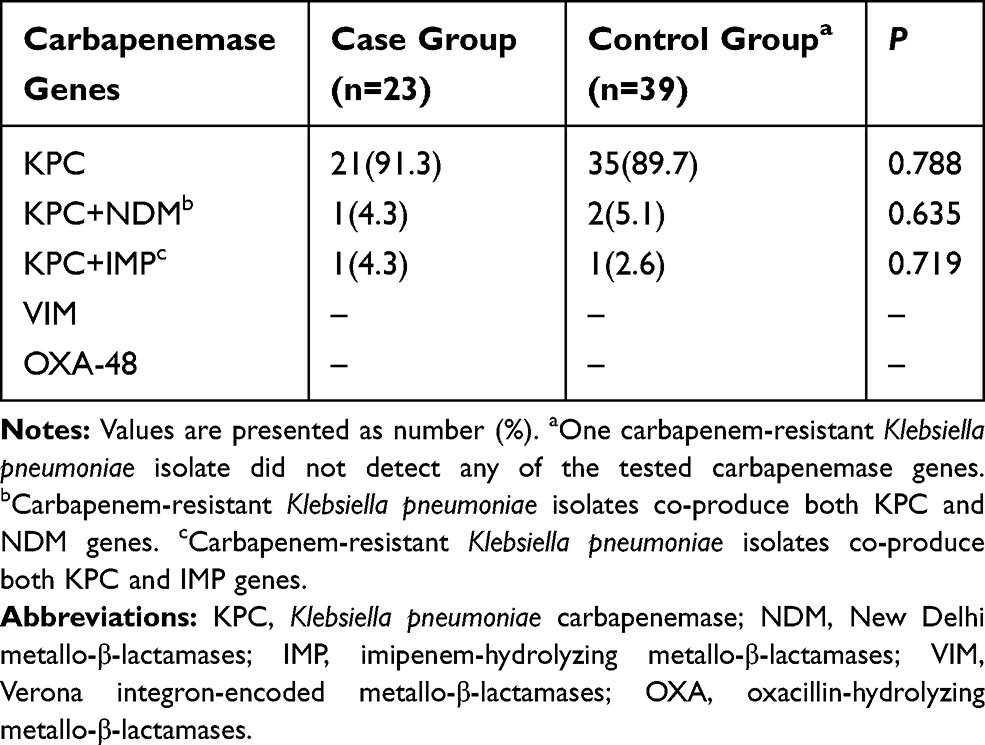 |
Table 2 Carbapenemase Genes Detected in Rectal Carbapenem-Resistant Klebsiella pneumoniae Isolates |
Risk Factors Analysis
The median age of the patients in case group (CRKP infection) was 55 years (range, 22–81) while it was 42 years in control group (range, 0–84) (P=0.039). The length of hospital stay in case group was significantly longer than that in control group (interquartile range, 45 versus 18 days, P=0.026). On univariate analysis, case group patients were more likely to be admitted to ICU (78.3% versus 38.5%, P=0.002), having received central venous catheter (65.2% versus 30.8%, P=0.008), having mechanical ventilated (69.6% versus 41.0%, P=0.030), having gastritis (52.2% versus 17.9%, P=0.005), being in coma condition (30.4% versus 7.7%, P=0.019), or receiving carbapenems (69.6% versus 41.0%, P=0.030), or receiving Tigecycline (26.1% versus2.6%, P=0.005) (Table 3).
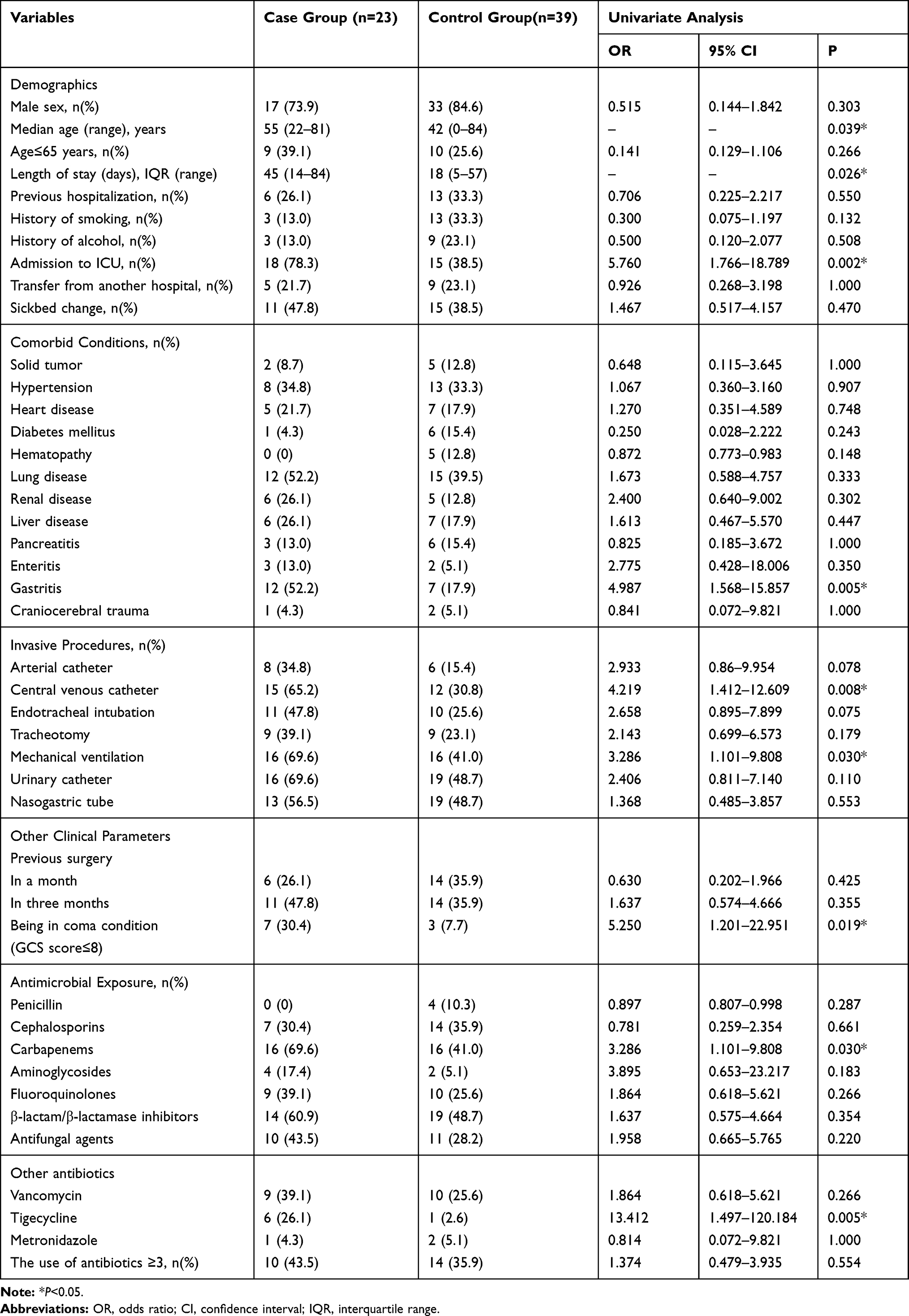 |
Table 3 Univariate Analysis of Risk Factors Associated with Subsequential CRKP Clinical Infection Among CRKP Rectal Carriers |
Multivariate analysis revealed that the variables that remained independent risk factors for CRKP clinical infection among CRKP rectal carriers were admission to ICU (OR, 6.753; 95% CI, 1.732–26.327; P=0.006), being in coma condition (OR, 11.085; 95% CI, 1.588–77.386; P=0.015) and receiving central venous catheter (OR, 8.628; 95% CI, 2.033–36.624; P=0.003) (Table 4). The multicollinearity parameters of eigenvalue, condition index and variance proportion showed that those identified independent risk factors were not collinear (Supplementary Table S1).
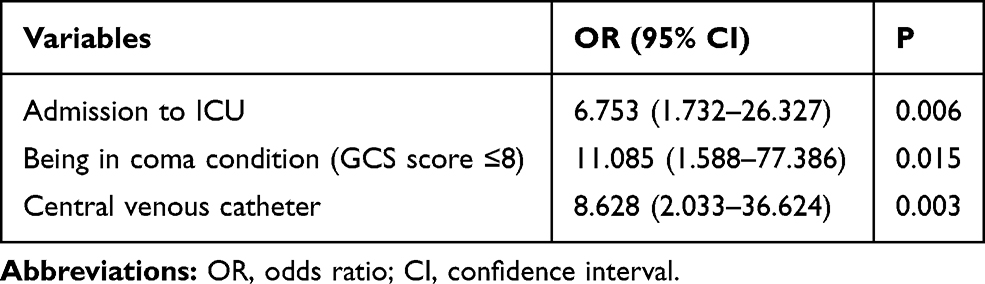 |
Table 4 Multivariate Analysis of Risk Factors Associated with Subsequential CRKP Clinical Infection Among CRKP Rectal Carriers |
Discussion
In this study, we screened 835 patients for rectal CRKP and found 37.1% CRKP those rectal carriers developed CRKP clinical infection. A subsequent retrospective case–control study identified that admission to ICU, being in coma condition and receiving central venous catheter are the independent risk factors for the subsequential infection.
Compared with limited studies undertaking to identify risk factors for progressing to clinical infection among rectal CRKP carriers, which are limited to particular wards,15,26,27 and mainly focused on certain type of infection,20,21 this study not only included patients originated from various wards in a large teaching university hospital but also included various clinical infections such as bloodstream infection, pneumonia, urinary tract infection, wound infection and peritonitis. In this study, we used 45 days as the time period watching for subsequential infection according to the observation that all the rectal CRKP carriers either developed subsequential infection or not and got discharged from hospital within 45 days after the first rectal CRKP identified. A previous study of subsequential bloodstream infection among rectal CRKP carries also used the same observation time period.21 This study showed 37.1% CRKP rectal carrier developed subsequential CRKP clinical infection and the infection rate is lower than that in a previous study which conducted in a medical-surgical ICU in Isreal. That study showed that of 49 CRKP rectal-colonized ICU patients, 23 (47%) subsequently developed clinical microbiological cultures.26 Their higher infection rate might be attributed to the studied population were ICU patients. While, according to another study in Isreal, only 9% CRKP-colonized patients developed clinical CRKP infection in an acute tertiary care university teaching hospital.19 Two studies focused on bloodstream infection showed that the rate of developing subsequential bloodstream infection among rectal CRKP carriers was7.8%, 20%, respectively.20,21 It may due to geographic differences in studied population.
In this study, we identified admission to ICU, receiving central venous catheter and being in coma condition were the independent risk factors for progression to clinical infection among CRKP carriers. Previous studies showed that admission to ICU, central venous catheter, previous invasive procedures, tracheostomy, urinary catheter insertion, invasive abdominal procedures, diabetes mellitus, solid tumor, antipseudomonal penicillin, chemotherapy/radiation therapy and colonization at site besides stool were independent predictors for infection development patients with CRKP colonization.19,20 Both shown in our study and others, patients admitted to ICU, or receiving invasive procedures are more likely to get infected with CRKP. However, the identification of being in coma condition as a risk factor has never been reported before, but a coma patient might be associated with receiving invasive procedures such as urinary catheter insertion or tracheal intubation, which are in accordance with those findings above.
In this study, we found KPC is the dominant carbapenemase both in the rectal and clinical infected CRKP isolates. This finding is similar to previous reports in China.6 Among 62 rectal CRKP isolates, only one K. pneumoniae was not found any of the five carbapenemase genes tested, possibly due to producing another carbapenemase gene or having other carbapenemase-resistant mechanism. There is no significant difference of the type of carbapenemase genes in CRKP isolates between the case group and control group.
Differed from other previous studies, we also investigated the clonal relatedness between the rectal CRKP and subsequential infection CRKP isolates by using MLST. The result showed that KPC-producing ST11 K. pneumoniae was the most common MLST type (71.0%) in rectal CRKP isolates. It is worth noting that all the subsequential infection CRKP isolates were also ST11 type, which is accordance with that ST11 is the most frequently reported ST type in China, contributing to the spread of antimicrobial resistance.6,28
The limitation of this study is that it is a single-center study and the limitation of patient populations may result in the conclusion lacking of generalization. However, our hospital is a 3,500-beds hospital, one of the largest hospitals in Southern China with more than 130,000 annual admission from all over the region. Despite the limitation, the investigation of the risk factors of progressing to clinical infection among CRKP carriers in a large scope of a teaching hospital in China is noteworthy.
Conclusion
In conclusion, this study identified independent risk factors for developing subsequential CRKP clinical infection among CRKP rectal carrier. Especially, being in coma condition as an independent risk factor is an important new finding. These findings would be useful to help clinician target those high-risk rectal CRKP-colonized patients for prevention of subsequential infection.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 81672066).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Meng X, Liu S, Duan J, et al. Risk factors and medical costs for healthcare-associated carbapenem-resistant Escherichia coli infection among hospitalized patients in a Chinese teaching hospital. BMC Infect Dis. 2017;17(1):82. doi:10.1186/s12879-016-2176-9
2. David S, Reuter S, Harris SR, et al. Epidemic of carbapenem-resistant Klebsiella pneumoniae in Europe is driven by nosocomial spread. Nat Microbiol. 2019;4(11):1919–1929. doi:10.1038/s41564-019-0492-8
3. Wang C, Yuan Z, Huang W, Yan L, Tang J, Liu CW. Epidemiologic analysis and control strategy of Klebsiella pneumoniae infection in intensive care units in a teaching hospital of People’s Republic of China. Infect Drug Resist. 2019;12:391–398. doi:10.2147/IDR.S189154
4. Zhang Y, Zeng J, Liu W, et al. Emergence of a hypervirulent carbapenem-resistant Klebsiella pneumoniae isolate from clinical infections in China. J Infect. 2015;71(5):553–560. doi:10.1016/j.jinf.2015.07.010
5. Grundmann H, Glasner C, Albiger B, et al. Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European survey of carbapenemase-producing Enterobacteriaceae (EuSCAPE): a prospective, multinational study. Lancet Infect Dis. 2017;17(2):153–163. doi:10.1016/S1473-3099(16)30257-2
6. Meng X, Yang J, Duan J, et al. Assessing molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae (CR-KP) with MLST and MALDI-TOF in Central China. Sci Rep. 2019;9(1):2271. doi:10.1038/s41598-018-38295-8
7. Li P, Wang M, Li X, et al. ST37 Klebsiella pneumoniae: development of carbapenem resistance in vivo during antimicrobial therapy in neonates. Future Microbiol. 2017;12:891–904. doi:10.2217/fmb-2016-0165
8. Hauck C, Cober E, Richter SS, et al. Spectrum of excess mortality due to carbapenem-resistant Klebsiella pneumoniae infections. Clin Microbiol Infect. 2016;22(6):513–519. doi:10.1016/j.cmi.2016.01.023
9. Hawkey PM. Multidrug-resistant Gram-negative bacteria: a product of globalization. J Hosp Infect. 2015;89(4):241–247. doi:10.1016/j.jhin.2015.01.008
10. Chotiprasitsakul D, Srichatrapimuk S, Kirdlarp S, Pyden AD, Santanirand P. Epidemiology of carbapenem-resistant Enterobacteriaceae: a 5-year experience at a tertiary care hospital. Infect Drug Resist. 2019;12:461–468. doi:10.2147/IDR.S192540
11. Zhao ZC, Xu XH, Liu MB, Wu J, Lin J, Li B. Fecal carriage of carbapenem-resistant enterobacteriaceae in a Chinese university hospital. Am J Infect Control. 2014;42(5):e61–64. doi:10.1016/j.ajic.2014.01.024
12. Mittal G, Gaind R, Kumar D, et al. Risk factors for fecal carriage of carbapenemase producing Enterobacteriaceae among intensive care unit patients from a tertiary care center in India. BMC Microbiol. 2016;16(1):138. doi:10.1186/s12866-016-0763-y
13. Schechner V, Kotlovsky T, Kazma M, et al. Asymptomatic rectal carriage of blaKPC producing carbapenem-resistant enterobacteriaceae: who is prone to become clinically infected? Clin Microbiol Infect. 2013;19(5):451–456. doi:10.1111/j.1469-0691.2012.03888.x
14. Tischendorf J, de Avila RA, Safdar N. Risk of infection following colonization with carbapenem-resistant Enterobacteriaceae: a systematic review. Am J Infect Control. 2016;44(5):539–543. doi:10.1016/j.ajic.2015.12.005
15. Zhang L, Zhai W, Lin Q, et al. Carbapenem-resistant enterobacteriaceae in hematological patients: outcome of patients with carbapenem-resistant enterobacteriaceae infection and risk factors for progression to infection after rectal colonization. Int J Antimicrob Agents. 2019;54:527–529. doi:10.1016/j.ijantimicag.2019.06.023
16. Liu Q, Liu L, Li Y, Chen X, Yan Q, Liu WE. Fecal carriage and epidemiology of carbapenem-resistant enterobacteriaceae among hospitalized patients in a University Hospital. Infect Drug Resist. 2019;12:3935–3942. doi:10.2147/IDR.S233795
17. Giannella M, Pascale R, Gutierrez-Gutierrez B, Cano A, Viale P. The use of predictive scores in the management of patients with carbapenem-resistant Klebsiella pneumoniae infection. Expert Rev Anti Infect Ther. 2019;17(4):265–273. doi:10.1080/14787210.2019.1595590
18. Ulu-Kilic A, Alp E, Percin D, et al. Risk factors for carbapenem resistant Klebsiella pneumoniae rectal colonization in pediatric units. J Infect Dev Ctries. 2014;8(10):1361–1364. doi:10.3855/jidc.4593
19. Borer A, Saidel-Odes L, Eskira S, et al. Risk factors for developing clinical infection with carbapenem-resistant Klebsiella pneumoniae in hospital patients initially only colonized with carbapenem-resistant K pneumoniae. Am J Infect Control. 2012;40(5):421–425. doi:10.1016/j.ajic.2011.05.022
20. Giannella M, Trecarichi EM, De Rosa FG, et al. Risk factors for carbapenem-resistant Klebsiella pneumoniae bloodstream infection among rectal carriers: a prospective observational multicentre study. Clin Microbiol Infect. 2014;20(12):1357–1362. doi:10.1111/1469-0691.12747
21. Amit S, Mishali H, Kotlovsky T, Schwaber MJ, Carmeli Y. Bloodstream infections among carriers of carbapenem-resistant Klebsiella pneumoniae: etiology, incidence and predictors. Clin Microbiol Infect. 2015;21(1):30–34. doi:10.1016/j.cmi.2014.08.001
22. Teasdale G, Maas A, Lecky F, Manley G, Stocchetti N, Murray G. The glasgow coma scale at 40 years: standing the test of time. Lancet Neurol. 2014;13(8):844–854. doi:10.1016/S1474-4422(14)70120-6
23. Tian X, Sun S, Jia X, Zou H, Li S, Zhang L. Epidemiology of and risk factors for infection with extended-spectrum beta-lactamase-producing carbapenem-resistant enterobacteriaceae: results of a double case-control study. Infect Drug Resist. 2018;11:1339–1346. doi:10.2147/IDR.S173456
24. Cockerill FR. Performance Standards for Antimicrobial Susceptibility Testing. 24th Informational Supplement. Wayne: Clinical and Laboratory Standards Institute; 2014.
25. Yan Q, Liu Q, Li Y, et al. Detection of carbapenemase-producing gram-negative bacteria using a simplified Carba NP test. J Microbiol Methods. 2016;123:1–3. doi:10.1016/j.mimet.2016.02.008
26. Debby BD, Ganor O, Yasmin M, et al. Epidemiology of carbapenem resistant Klebsiella pneumoniae colonization in an intensive care unit. Eur J Clin Microbiol Infect Dis. 2012;31(8):1811–1817. doi:10.1007/s10096-011-1506-5
27. Papadimitriou-Olivgeris M, Marangos M, Fligou F, et al. KPC-producing Klebsiella pneumoniae enteric colonization acquired during intensive care unit stay: the significance of risk factors for its development and its impact on mortality. Diagn Microbiol Infect Dis. 2013;77(2):169–173. doi:10.1016/j.diagmicrobio.2013.06.007
28. Li J, Zou MX, Wang HC, et al. An outbreak of infections caused by a Klebsiella pneumoniae st11 clone coproducing klebsiella pneumoniae carbapenemase-2 and RmtB in a Chinese Teaching Hospital. Chin Med J. 2016;129(17):2033–2039. doi:10.4103/0366-6999.189049
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.