Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Risk Factors Associated with Epilepsy Related to Cerebrovascular Disease: A Systematic Review and Meta-Analysis
Authors Mafla-Mendoza AP, Paredes-Urbano ED, Gea-Izquierdo E ![]()
Received 14 September 2023
Accepted for publication 28 November 2023
Published 27 December 2023 Volume 2023:19 Pages 2841—2856
DOI https://doi.org/10.2147/NDT.S439995
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Roger Pinder
Ana Paula Mafla-Mendoza,1,* Esteban David Paredes-Urbano,1,* Enrique Gea-Izquierdo1– 3
1Pontifical Catholic University of Ecuador, Faculty of Medicine, Quito, Ecuador; 2Department of Medical Specialties and Public Health, Rey Juan Carlos University, Madrid, Spain; 3María Zambrano Program, European Union, Rey Juan Carlos University, Madrid, Spain
*These authors contributed equally to this work
Correspondence: Enrique Gea-Izquierdo, Pontifical Catholic University of Ecuador, Faculty of Medicine, Quito, Ecuador, Email [email protected]
Background and Objective: Stroke is one of the most frequent neurological syndromes in the adult population and the cause of 10% of all diagnosed epilepsies. It is attributed to the origin of up to 50% of them in adults > 60 years of age. Although a few risk factors have been described and considered when modeling predictive tools, this aspect is still clinically complex. The objective of this study is to describe and compare predictor scales of post stroke epilepsy (PSE) in adult patients with better performance.
Methods: A systematic review and meta-analysis were performed of studies published between 2010 and 2020 and found in PubMed, Scopus, EMBASE, LILACS, BVS, Google Scholar, and CENTRAL databases. Sixteen studies were included with a total of 298,694 patients with a diagnosis of stroke, 5590 presented late seizures (LS).
Results: Hemorrhage, cortical involvement, and early seizure were the elements most associated with the risk of presenting late seizures. The SeLECT score demonstrated a low risk of bias with a high predictive ability in patients with ischemic stroke (AUC: 0.77 [95% CI: 0.71– 0.82]). In patients with hemorrhagic stroke, the CAVE score demonstrated adequate predictive ability (AUC: 0.81 [95% CI: 0.76– 0.86]), but an uncertain risk of bias. Research has established risk factors for post ictal epilepsy; however, the numerous ways of assessing data in studies and the difference in their designs make the task of producing a predictive scale that covers the most important risk factors and is reliable for application in the clinical setting, regardless of stroke etiology, very arduous.
Conclusion: Hemorrhage, cortical involvement, and early seizure are associated with an increased risk of post ictal epilepsy. Also, elements such as age, traditional vascular risk factors, and functional assessment failed to reflect statistical significance. Finally, further research is required to refine the available predictive tools.
Keywords: cerebrovascular event, seizures, post stroke epilepsy, predictive model, systematic review
Introduction
Stroke is the most frequent neurological syndrome of adulthood;1 it is understood as the abrupt onset of a focal neurological deficit caused by a localized lesion in the central nervous system generated by vascular damage that disrupts the normal blood supply of the brain, retina, or spinal cord,2 resulting in ischemia or an accumulation of blood within the brain tissue or ventricular system. It is noted that ischemic stroke accounts for 80–87% of all strokes and has a complex etiopathogenesis that varies according to the specific cause, such as atrial fibrillation cardioembolism, large vessel atherosclerosis, lacunar infarcts, and undetermined causes.3
Thanks to advances in the management of stroke, mortality and incidence have been reduced since 1950, but there has been an increase in hospitalizations of adults between 18 and 44 years of age and, therefore, the number of survivors living with complications has increased.1–4 According to data from the Global Burden of Diseases (GBD), in 2019, the United States estimated a mortality rate of 37.72 deaths per 100,000 habitants, and that year the prevalence of stroke was 1.03%, which means there are about 6.4 million stroke survivors in this country.5,6
The average overall lifetime risk has increased to 25%,5 and stroke survivors have an increased mortality risk, in some cases even triple it, especially in infarcts involving the middle cerebral artery territory. In survivors, inherent neurological deficits are observed such as fatigability, spasticity, or flaccidity of limbs and face; as well as a plethora of complications including epilepsy and seizures. The latter occur in 3–10%,1,7,8 making them the most common cause of new-onset epilepsy in adults.
The International League Against Epilepsy (ILAE) defines epilepsy as the occurrence of two or more unprovoked seizures (UPSs) in a span of more than 24 hours, or a UPS with a substantial risk of recurrence (60%) within the next 10 years. After contrasting clinical observations, the ILAE concludes that seizures resulting from brain injury, such as stroke, are dichotomized in terms of time into acute symptomatic seizures (ASS) and UPSs: the former occur in the first seven days after stroke; the latter, one week after the cerebrovascular event.8,9 A patient with a persistent proclivity for future seizures has epilepsy if at least one UPS occurs and the likelihood of additional seizures is comparable to the chance of recurrence after two UPSs (at least 60%);9 hence, late seizures (LS) are termed epilepsy.
This differentiation becomes relevant when observing that LS have a higher risk of recurrence. Classically, it is known that the annual rate of seizures in the first year after stroke is 4.2% and at 5 years is 9.7%, and values increase dramatically in the case of hemorrhagic stroke where values of 20% in the first year and 26% at 5 years are found.2,10 According to Hesdorffer et al the risk of subsequent UPS is 33% (95% CI: 20.7–49.9%) in those patients who had an early seizure, and 71.5% (95% CI: 59.7–81.9%) in patients where UPSs were evident one week after the stroke.1,4
UPSs occur due to excessive excitatory activity of a neuronal network in the context of an imbalance of excitatory and inhibitory factors in normal synaptic activity. This results in a disruption of neuronal communication networks and causes excessive discharge within a local or generalized neural network which, in turn, causes a disruption of physiological neuronal metabolism and triggers an epileptiform rhythm within normal cortical activity.11 Causes of epileptic seizures in adult patients without a history of epilepsy include stroke (40%), metabolic disorders (15%), brain neoplasm (10%), and neurodegenerative diseases such as Alzheimer’s disease (5%).12
In 2017 Wang et al presented a meta-analysis on the incidence of seizures after ischemic stroke, acknowledging that in this type of stroke a lower prevalence of post stroke epilepsy (PSE) is observed. They report that in 20 of 35 articles exploring the epidemiology of PSE, a cumulative incidence of eighteen cases per one-thousand-person years is observed (95% CI: 15–22).3,13
In the case of PSE it is distinguished as a seizure that occurs after seven days following the stroke and is related to brain tissue damage as a sequel to the ischemic insult resulting from the lack of vascular supply, from which a hyperexcitable tissue is created. During the first days after the injury, a biochemical imbalance occurs with elevated glutamate levels which results in an increase in the excitatory level of this neurotransmitter resulting in ASS. As a result of structural and physiological damage to the cerebral cortex, structural affectations such as glial scars can emerge during the process of lesion resolution, becoming potential epileptogenic foci.14 The etiopathogenic explanations may variate in the case of a hemorrhagic stroke where the accumulation of hemosiderin, an insoluble protein that stores iron, can cause local irritation in the brain tissue, therefore causing the seizures,15 increasing cellular dysfunction and subsequent neurodegeneration.16–18
In this sense, a variety of risk factors associated with PSE have been described. Tanaka and Ihara mention that there are numerous studies describing risk factors, and most of them describe that cortical involvement, hemorrhage, severity of stroke, comorbidities, and family history of seizures increase the likelihood of PSE.1,4 For Toro Perez there is a segmentation of these risk factors where ischemic stroke will represent a higher probability of risk of PSE in the context of severe neurological impairment, a large extent of the infarct verified with neuroimaging, the location of the lesion, and the origin of ischemia (such as cardioembolism or atherosclerosis); on the other hand, in the case of hemorrhagic stroke the frequency of PSE increases in lobar and subcortical hemorrhages.8 It is estimated that the hemorrhage, the cortical involvement, the early seizures, age, and the cardiovascular risk factors are associated with PSE, hence the scores related to these variables will select individuals with this condition more accurately.
The significant psychosocial burden of epilepsy has an impact on the quality of life of the patient and their family and, indirectly, of the community.19 In this regard, it is considered that it is useful to establish the risk of PSE for the comprehensive management of stroke survivors and proposed to systematically compare the tools described in the literature of the last decade to establish their efficacy and practicality.
Methods
A systematic review and meta-analysis were reported according to the recommendations of the Cochrane Group and the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analysis). Due to the nature of this study, informed consent was not required from the patients.
The investigators performed the review using all the titles and abstracts obtained from the initial search. The investigators independently selected articles for assessment. During the synthesis phase, studies were categorized into groups based on their effect measure.
Eligibility Criteria
Inclusion Criteria
Studies meeting the following criteria were included: (1) published randomized controlled trials (RCTs) and observational studies between 2010 and 2020; (2) original research evaluating risk factors for post stroke epilepsy; (3) incidence and prevalence of seizures in adult patients; (4) time-dependent definition of the clinical presentation of the event (early or late seizures); (5) diagnosis of stroke of any type; and (6) assessment of at least one of the following predetermined study variables (age, modified Rankin Scale or mRs, hemorrhage, cortical involvement, early seizure, lesion size, and vascular risk factors).
Exclusion Criteria
Expert opinions, commentaries, editorials, and case reports were excluded; as well as studies covering etiologies such as trauma, bleeding related to neoplasms, recent brain surgery, central nervous system infections, and iatrogenic causes. Studies whose population included patients with a history of epilepsy, and pediatric and obstetric patients were also excluded.
Sources of Information
A search for scientific publication in the health sciences was initiated in November 2021 in the electronic databases PubMed, Scopus, EMBASE, LILACS, BVS, Cochrane, CENTRAL, and Google Scholar, which included original studies published in English or Spanish for the period between 2010 and 2020. Furthermore, some references20–22 were examined to feed our own database.
Search Strategy
The key search terms were: “ischemic stroke”, “hemorrhagic stroke”, “seizures”, “epilepsy”, and “prognostic model”. Terms derived from Medical Subject Heading (MeSH) were used to improve the search strategy, and results were filtered by date to examine studies published between 2010 and 2020. The strategies used in each search engine are listed in Annex 1.
Selection Process
The authors of the present study independently evaluated the results of the searches in the databases listed in the previous section, initially screening them according to the title and abstract of the articles. Subsequently, the full texts of the articles approved in the initial search were obtained and stratified according to the inclusion criteria stated above. Finally, research articles proposing risk estimation of late seizure risk in adult stroke survivors published between 2010 and 2020 were included in the final analysis.
Data Collection Process
The following numbers were obtained from the search of articles by databases: in PubMed, 658 results; in Scopus, 7; in LILACS, 96; in BVS, 80; in Cochrane, 1; in CENTRAL, 47; and in Google Scholar, 344. A total of 48 duplicate articles were excluded from these, and another 8 that did not meet the criteria. The articles were reported in the PRISMA flowchart format for systematic reviews (Figure 1).
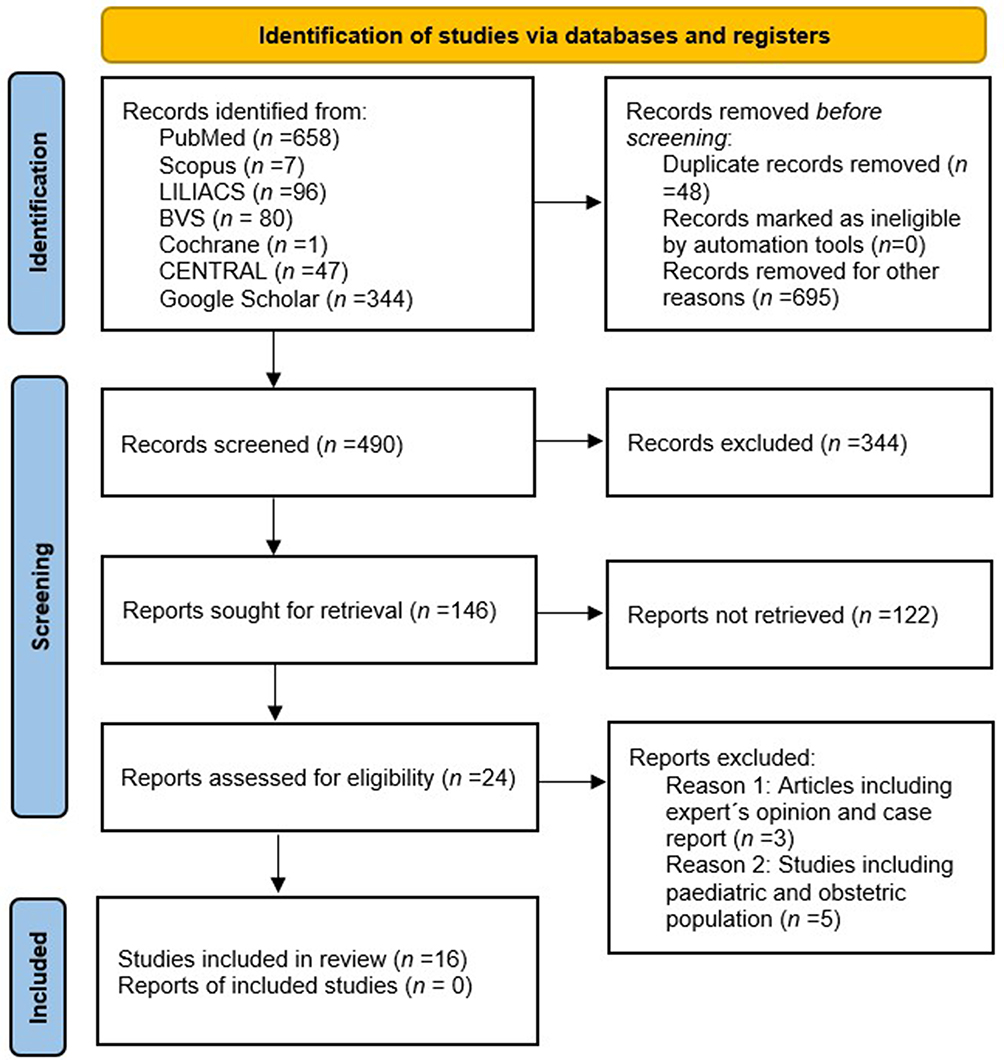 |
Figure 1 PRISMA flowchart. |
Data Extraction
Data extraction was performed independently by the authors using a standardized form taken from the Critical Appraisal and Data Extraction for Systematic Reviews of Prediction Modelling Studies (CHARMS).
Data Elements
For each eligible study, the following data were extracted: name of the first author, name of the predictor tool, year of publication, country, study design, sample size, demographic characteristics (age and sex), clinical characteristics (NIHSS scale, seizure presentation over time, use of neuroimaging techniques, follow-up time, and discrimination ability). These variables and description are summarized in Tables 1–2.
 |
Table 1 Characteristics of the Studies |
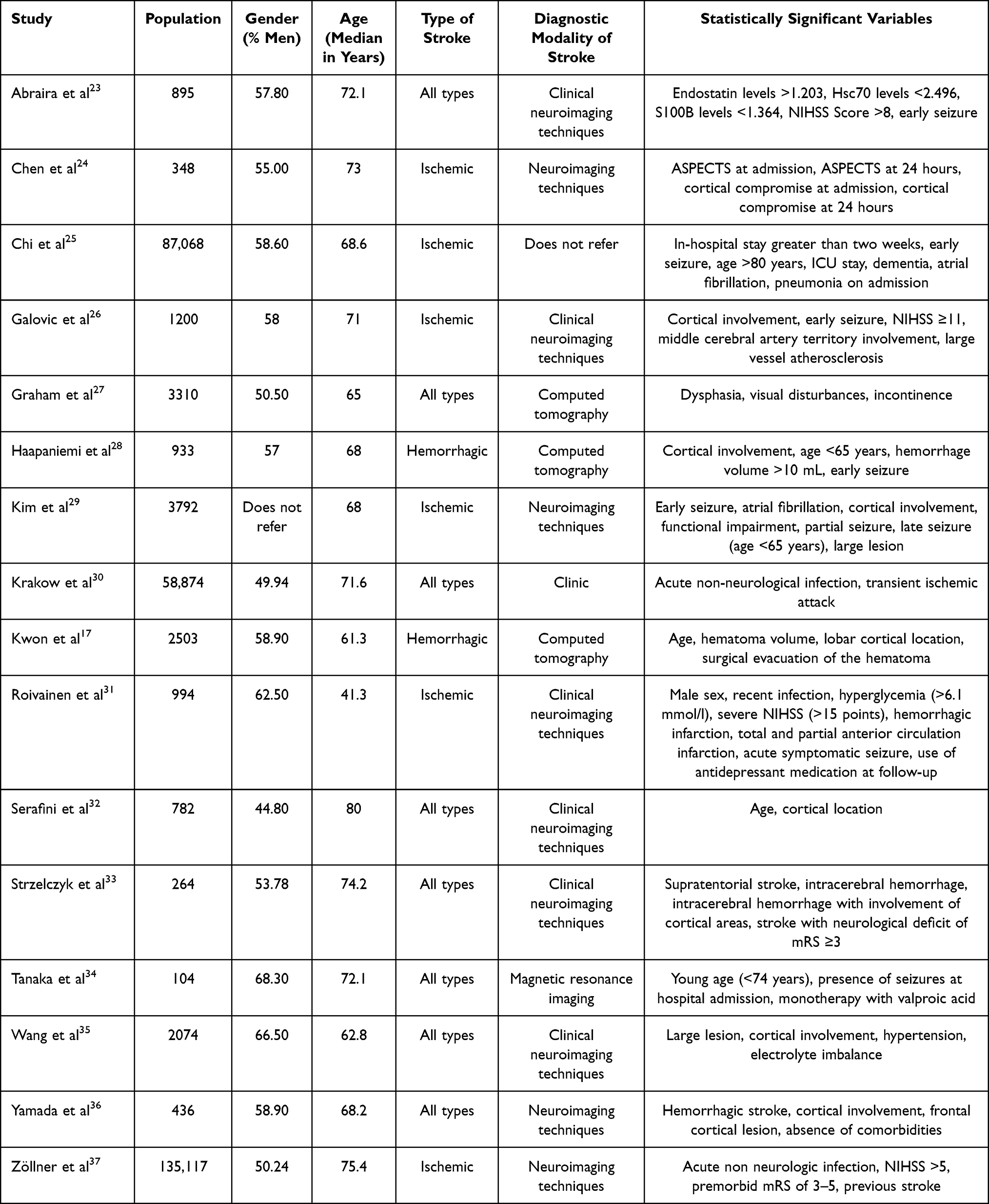 |
Table 2 Characteristics of Participants |
Results
The primary outcomes were the odds ratio (OR) and hazard ratio (HR) measures with their corresponding confidence intervals derived from the risk factors reported in the studies that evaluated the probability of PSE.
Risk of Bias Assessment
To estimate the quality of the selected articles, we applied specific scales. For observational cohort studies the Newcastle–Ottawa Scale allows the assessment of the selection characteristics of the participants, the comparability of the populations and the general results of the research. This tool assigns one star to each category; there is a higher risk of bias when the score is less than six stars; a moderate risk when the score is between six and seven stars; and a low risk of bias when the score is greater than seven stars.38,39
For studies that offer a predictive tool the PROBAST tool was applied since it is a specific score for estimating the quality of predictive models with multiple variables. To do this, each article is evaluated, indicating whether it is under development or in the process of validation by peers, and an in-depth investigation is conducted to assess whether there is a risk of bias in the selection of participants, predictors, and results with a general analysis. In this way, a low, high, and undetermined risk is estimated when there is at least one item classified as high or uncertain; and the concern about the applicability of said predictive tool to be evaluated is considered as low, high, and uncertain.40
Measures of Effects
The main effect measures in this dissertation are the OR and HR, expressed as binary data. The logarithm of OR and HR were calculated for subsequent use in the RevMan program. Means and standard deviations were used for continuous variables. Finally, the randomized effects method was applied according to the heterogeneity of the study conditions.
Synthesis Methods
A database was prepared with the previously stated items. Each study’s statistically significant variables were documented, and the coincidences of these variables between studies were then included in the meta-analysis for its comparison. The chosen studies were classified according to the reported measure of effect, between the OR and the HR. Two separate meta-analyses were performed to group the studies according to the data reported. To identify significant associations between the different PSE risk factors, OR data with 95% confidence intervals were used for comparison of cumulative proportions of LS incidents between the exposed and unexposed groups.
Consequently, we evaluated the studies that reported HR measures with 95% confidence intervals for the comparison of conditional probabilities over time; and we analyzed these data in the Review Manager 5.4.1 developed by Cochrane Reviews, where we entered the data to perform an inverse variance analysis of the OR and HR values of each of the variables identified as coincidences among the studies, thus performing subanalysis for each proposed risk factor.
The level of statistical significance was set at p<0.05 and the heterogeneity of the studies was evaluated visually by means of forest plots, and quantitatively by means of the I², so that the points of 25%, 50%, and 75% were used to consider low, medium, and high heterogeneity, respectively. In this regard, the statistical tables show the categorical data with percentages.
Results
Selection of Studies
After data extraction from the articles, a systematic review and meta-analysis were performed, including sixteen studies: seven were retrospective and nine were prospective. Mean follow-up time was 2.3 years, and a total of 298,694 patients with a diagnosis of stroke were evaluated, where 5590 had seizures. Likewise, nine studies used seven days as the cutoff point to define LS, while seven studies used fourteen days to define LS. These characteristics are summarized in Table 1.
Predictors Associated with PSE
Studies Reporting Odds Ratio
Regarding the analysis of age, five studies were included, with a total population of 201,068, where no significant effect was seen (OR 1.55 [95% CI: 0.38–6.27], Z=0.61, p=0.54) (Figure 2). Regarding mRs, four studies were observed, with a total population of 198,047, where no heterogeneity was seen among them, but an (OR 2.63 [95% CI: 1.28–5.41], Z = 2.64, p=0.008) was evidenced. For the analysis respecting to hemorrhage, there were seven studies included, with a total population of 203,754, where a high heterogeneity of (I²=81%) and a Z value of 3.43 was obtained (OR 2.06 [95% CI: 1.36–3.11], p=0.0006).
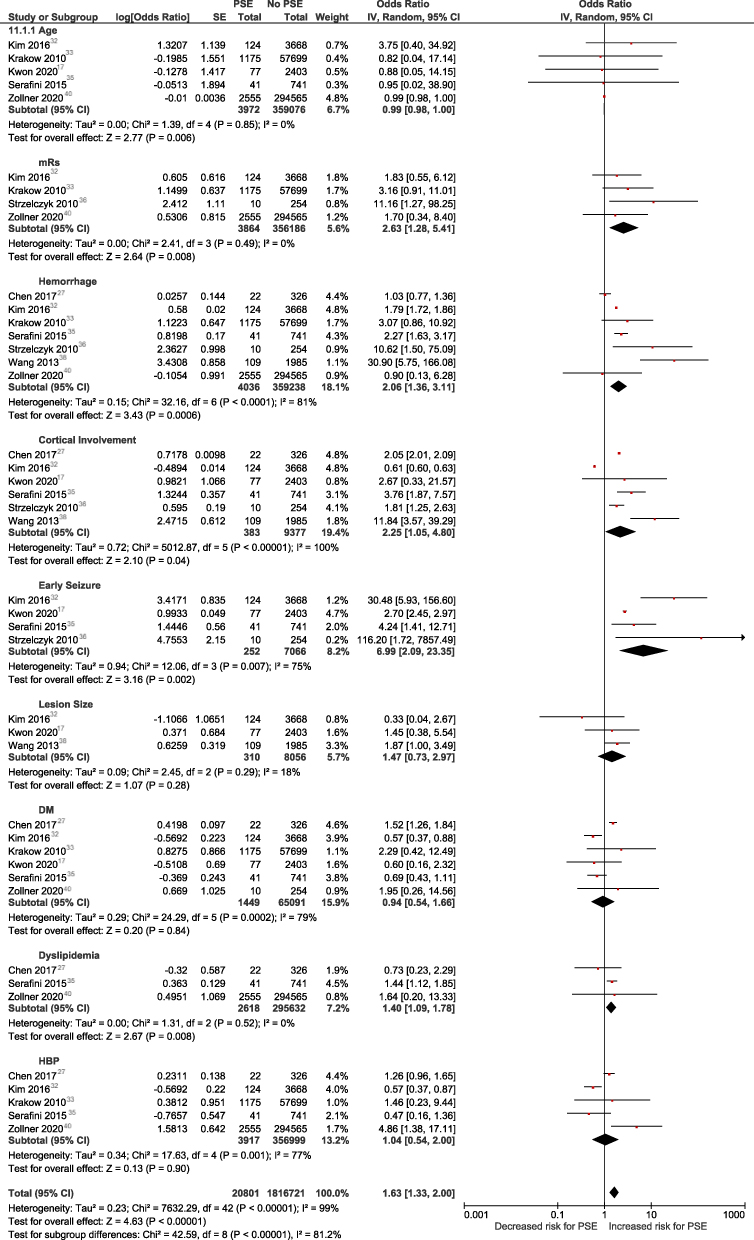 |
Figure 2 Forest plot of OR. |
With cortical involvement, six studies were included in the analysis and showed a high range of heterogeneity (I²=100%), as well as a Z value of 2.1 with a and a pooled (OR 2.25 [95% CI: 1.05–4.8], p=0.04,) which implies that the probability of LS is higher. According to early seizure, there were four studies in this subanalysis where heterogeneity was observed to be high (I²=75%), the estimated effect was 3.16 with an estimated (OR 6.99 [95% CI: 2.09–23.35], p=0.002), thus estimating a significantly higher risk for triggering PSE. Finally, about the lesion size, three studies were included with high heterogeneity (I²=92%), where no significant effect was evidenced as a function of lesion size (OR 0.91 [95% CI: 0.24–3.54], p=0.9).
Additionally, the vascular risk factors such as high blood pressure (HBP), diabetes mellitus (DM), and dyslipidemia were evaluated as independent predictors of PSE. The presence of DM was evaluated in six studies with high heterogeneity (I²=79%) and did not seem to be (OR 0.94 [95% CI: 0.54–1.66], p=0.84); dyslipidemia was evaluated in three studies, where the I² value was 0. There was a significant effect for the occurrence of PSE (OR 1.4 [95% CI: 1.09–1.78], p=0.008); and HBP was assessed in five studies with a population of 198,913, and there was evidence of heterogeneity and no significant effect for the occurrence of PSE (OR 1.04 [95% CI: 0.54–2], p=0.9).
Studies Reporting Hazard Ratio
Regarding age, seven studies were included with a total population of 94,045, where a significant effect was seen (HR 1.91 [95% CI: 1.25–2.90], p=0.003) with a Z value of 3.01 with I²=46% (Figure 3). For mRs, two studies were included with a total population of 99 participants, and no heterogeneity was observed between studies (HR 1.4 [95% CI: 1.14–1.73], Z=3.14, p=0.002). Regarding hemorrhage, six studies were included in this subanalysis with a total population of 6939, and a moderately low heterogeneity (I²=36%) evidenced; furthermore, a Z value of 3.85 was obtained (HR 1.77 [95% CI: 1.32–2.38], p=0.0001).
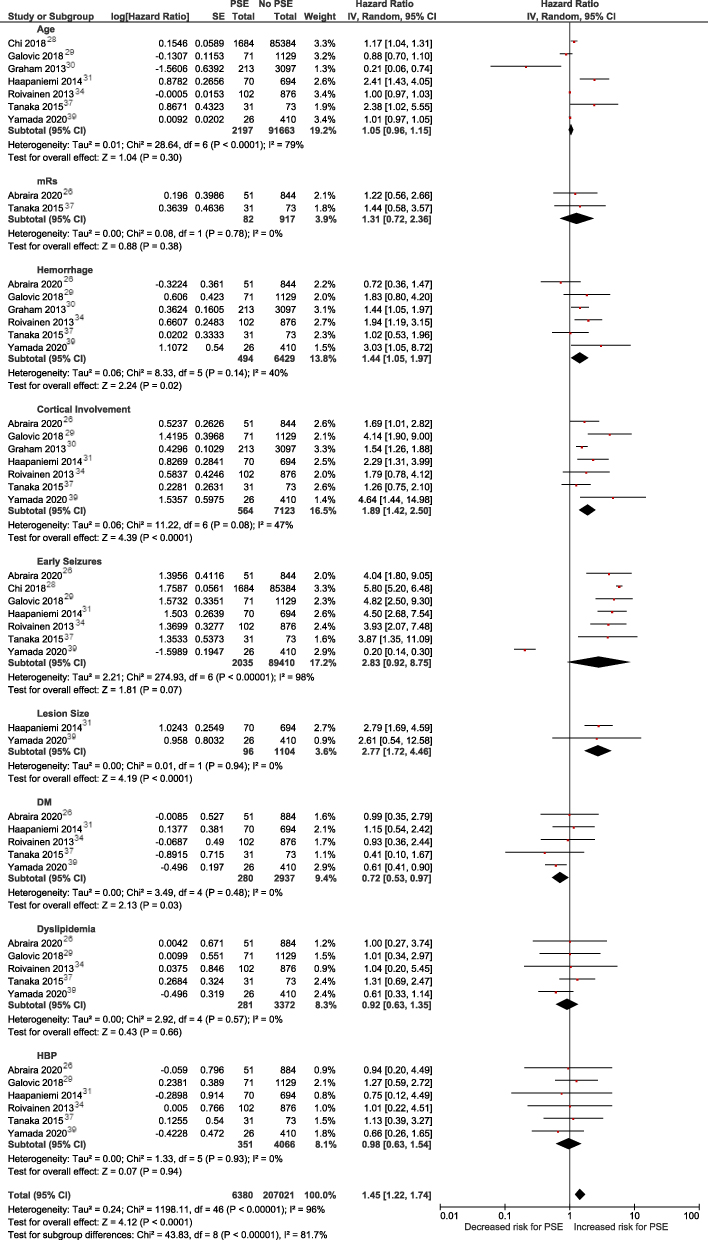 |
Figure 3 Forest plot of HR. |
On the other hand, regarding cortical involvement, seven studies were included in the subanalysis and showed a moderate range of heterogeneity (I²=60%), a Z value of 5.17, and a pool (HR 2.23 [95% CI: 1.65–3.02], p<0.00001), which implied that this variable was independently associated with PSE and can be taken as a predictor factor. For early seizure, seven studies were considered in this subanalysis, and high heterogeneity was proven (I²=98%), and an estimated (HR 2.85 [95% CI: 0.92–8.86], Z = 1.82, p=0.07); due to the very wide confidence intervals a significantly higher risk for triggering PSE was not estimated.
However, with lesion size, two studies were included with no measurable heterogeneity (I²=0%) and showed a significant effect according to lesion size (HR 2.77 [95% CI: 2.17–3.55], p=0.03). Finally, regarding vascular risk factors, HBP, DM, and dyslipidemia were evaluated as independent predictors of PSE. The presence of DM was evaluated in five studies with I²=0% and with an apparent protective effect (HR 0.72 [95% CI: 0.53–0.97], p=0.03). Dyslipidemia as a predictive factor was evaluated in five studies where no heterogeneity was evidenced (I²=0%), with an effect that showed no difference between the exposed and unexposed groups (HR 0.92 [95% CI: 0.63–1.35], p=0.66); and HBP was assessed in six studies with a population of 4562, where high heterogeneity was seen (I²=93%) and no significant effect for the prediction of PSE between the exposed and unexposed groups (HR 0.98 [95% CI: 0.63–1.54], p=0.94).
Risk of Bias in the Studies
Two types of tools already described were used to identify bias in the publications used. For the cohort studies, the Newcastle–Ottawa Scale was used, where eight articles with low risk of publication bias were identified (Table 3), corresponding to the following authors: Abraira et al,23 Chen et al,24 Graham et al,27 Krakow et al,30 Roivainen et al,31 Serafini et al,32 and Tanaka et al.34 On the other hand, there were some with a high risk of bias: Wang et al35 and Zöllner et al.37 The PROBAST tool, specific for these studies, was used in the articles that provided a predictor score. It was found that the work of Galovic et al26 was the only one in which a low risk of bias and a low concern for its applicability were evidenced (Table 4). Meanwhile, Chi et al,25 Haapaniemi et al,28 Kim et al,29 Kwon et al,17 and Strzelczyk et al33 were studies with an uncertain risk of bias and uncertain concern regarding their applicability.
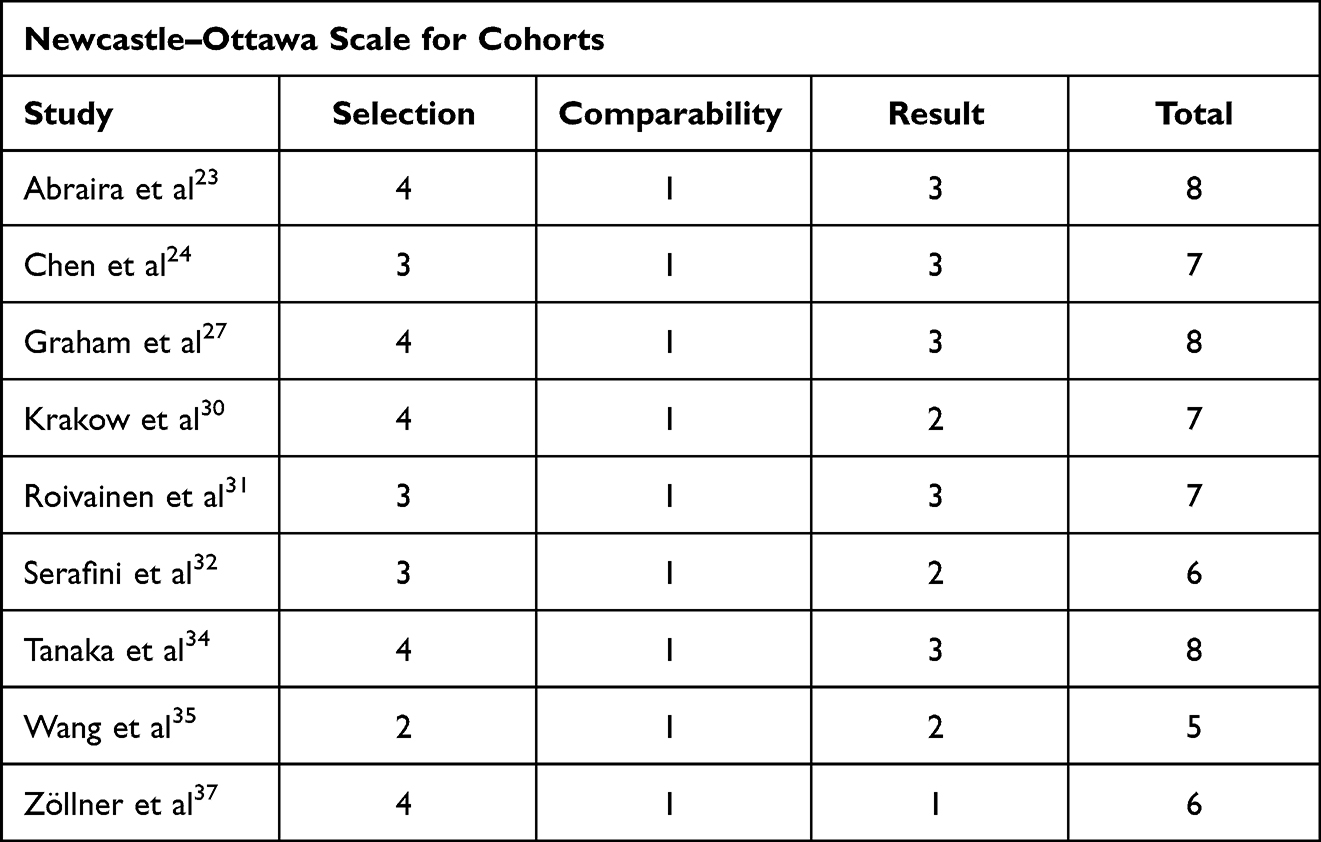 |
Table 3 Studies Evaluated with the Newcastle–Ottawa Scale |
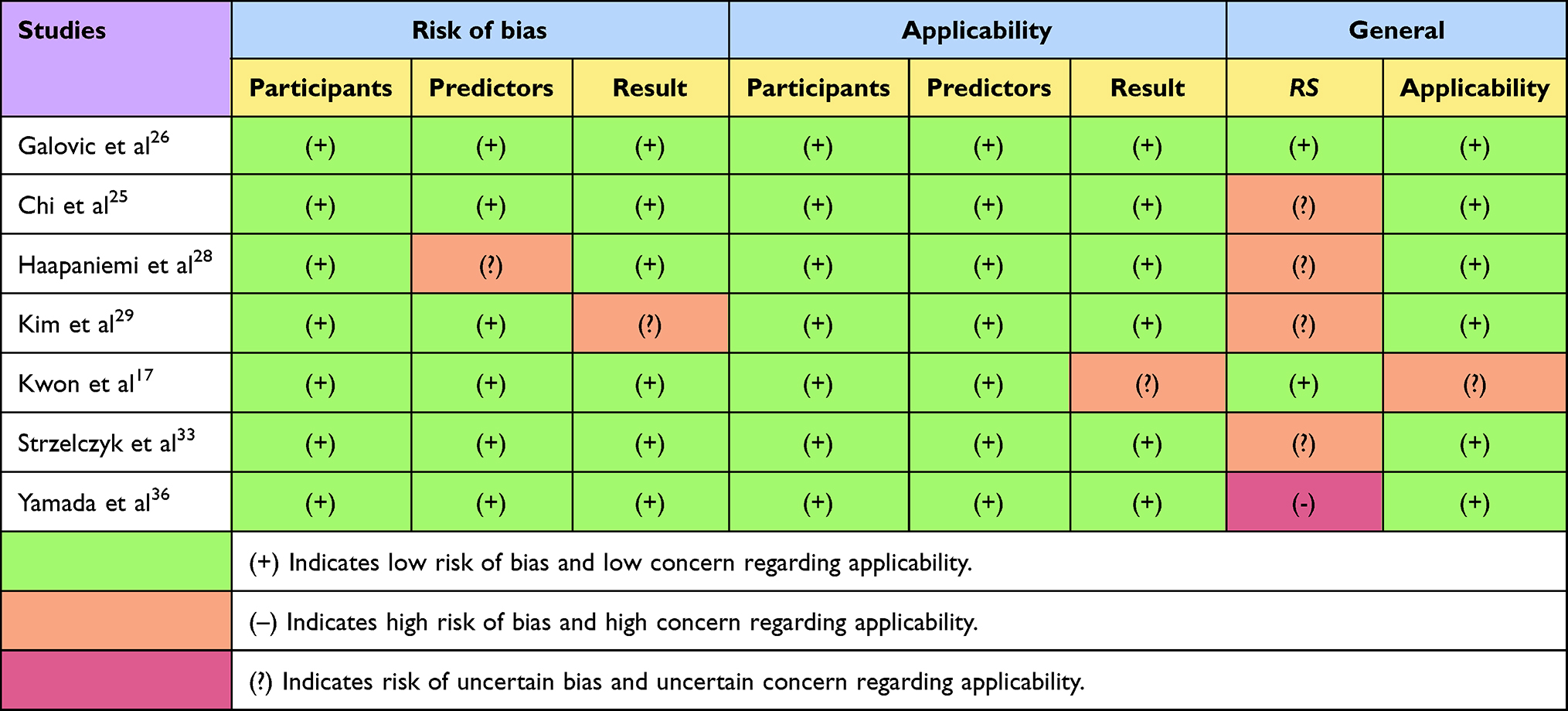 |
Table 4 Studies Evaluated with PROBAST |
Discussion
Despite the constraints imposed by the quality of the included studies (with approximately half of the studies being retrospective) and the high heterogeneity observed (in terms of design and in terms of the included population, the way to define epilepsy and early seizure in time, length and form of follow-up, and the proposed variables), our meta-analysis underscores that the cortical involvement, the hemorrhage, and the early seizures are linked to an elevated likelihood of developing PSE.
The epileptogenic role of cortical involvement and the presence of extravasated blood in the brain parenchyma is supported by clinical and experimental evidence, and this meta-analysis confirms these statements where the risk is doubled; nevertheless the assessment of the lesion size is one the variables most inconsistently reported, in which five different studies have examined this particular aspect and their findings diverge in terms of defining risk thresholds. In this matter the authors have noted that the significant interest in the development of risk models for predicting the likelihood of the onset of late seizures in stroke patients serves various purposes, having implications not only in the clinical practice but in the research and understanding of this peculiar pathophysiology.
The integration of biomarkers represents an innovative approach to addressing this condition; however, only a limited number of studies incorporate biomarkers as predictive tools, preventing their meta-analysis. In the prospective longitudinal study by Abraira et al,23 the authors suggested that reduced levels of S100B and Hsc70, coupled with elevated levels of endostatin, collectively indicate a 17% increased risk of PSE. Based on present literature the significance of inflammatory mediators such as interleukins IL-1, IL-6, and IL-10 is noted in the interplay between seizures and stroke. Additionally, the presence of the CD40/CD40L system, associated with seizure susceptibility, further contributes to inflammatory mechanisms.41,42
In the clinical field, the studies included in this meta-analysis have not shown evidence supporting the prophylactic use of antiseizure medications in the post stroke setting. Serafini et al32 suggested that patients with hemorrhagic stroke could benefit from the antiseizure drugs; Tanaka et al34 evaluated different families of antiepileptic drugs and conclude that valproic acid does not improve prognosis; and Yamada et al36 mentioned that prophylactic antiepileptic therapy of short duration could be beneficial in high-risk patients with intracerebral hematomas, or with at least two factors identified in their study. Chi et al25 pointed out that it would pose a risk if antiepileptic therapy was routinely administered to all stroke patients, therefore it is important to identify those patients who are at most risk of experiencing complications like PSE. Despite the PSEiCARe score’s adequate predictability, the study was unable to establish a cutoff point at which antiepileptic therapy should be initiated.
As aforementioned, the early seizures have shown a strong correlation with PSE; however, some authors17,36 argue that early seizure is a difficult factor to evaluate, due to the probability of the introduction of antiepileptic drugs during the acute setting affecting the occurrence of LS and, therefore, of recurrence. Recognizing this factor might have been the reason why Kwon et al17 did not observed statistically significance of early seizure in their sample, so it was disregarded in their remodeling of the CAVE score and replaced by surgical evacuation as a predictor item.28 Furthermore, the authors recognized that the epileptogenic process between early and late seizures differs, also noted in Kim et al29 noticing that the factors related to early seizure did not overlap with the factors for PSE; however, Haapaniemi et al28 mentioned that the relevance of this variable is due to the fact that early epileptiform activity increases metabolic demand, causes secondary alterations, and accelerates gliotic scarring processes, similarly Galovic et al26 stated that patients who suffered an early seizure have a greater predisposition to generate epileptiform activity, which implies that their seizure threshold is lower, so this is a factor that is considered.
Similarly, the variables related to the stroke risk, like DM and dyslipidemia, showed varied associations with PSE. Krakow et al30 identified DM as an important risk factor in young patients with ischemic stroke and noted that dyslipidemia is projected as a probable risk factor, but further studies are required, because these variables are usually only relevant in univariate analyses. Yamada et al36 observed that more than one comorbidity is associated with a lower probability of developing PSE and mentioned that some reports show an anticonvulsant effect of certain drugs used for the treatment of chronic illnesses, such as dipeptidyl-peptidase 4 (DPP 4) inhibitors used in the treatment of DM, or angiotensin II receptor blockers (ARB, Annex 2), used in the treatment of HBP. Our analysis on these variables did not show association with PSE, however, in the subanalysis of studies that examined DM using the HR it appeared to be a protective factor. The identification of high-risk individuals based on their risk factors brings another practical application which lies in optimizing related to antiepileptogenesis following strokes. Once the individual seizure risk is acknowledged based on the evidenced-based risk factors can enhance the study power and potentially lead to more successful trials, thus, the approach that we have implemented in this meta-analysis may aid in the shifting of the research focus, avoiding the random inclusion of individuals with low risk for seizures into the clinical trials, which may also lower the research costs while still assuring study power. For examples, following the evidence we have extracted it is noted that most studies agree that age is inversely proportional to the probability of suffering a PSE. Serafini et al32 mentioned that the older the age of patients with ischemic stroke, the lower the probability of LS (OR=0.96 [95% CI: 0.92–0.99], p=0.020). Tanaka et al34 noted that patients younger than 74 years were more frequently associated with late seizures. Graham et al27 concurred with these observations, as in their cohort 15.6% of patients younger than 65 years were affected with PSE as opposed to those older than 85 years, who were affected by only 4.4%. Roivainen et al31 aligned with the same results, noting that the range of seizures decreases over time during follow-up and becomes stable by the fourth year, but their frequency remains higher than the general population, thus confirming the link between stroke and seizures. In this regard, future clinical trials should consider the heterogeneity in the fluctuating state of this feature, which limits the association between this variable with PSE, bringing the focus to the patients in high-risk ages.
In this aspect, the authors believe that taking into account the risk factors assessed in this meta-analysis helps supporting the pathophysiological conclusions and therefore expands our understanding of this entity, for example, for the details involving the stroke severity, the evidence is not noticeably clear. Wang et al35 pointed out that there is no increased risk depending on the severity measured by the NIHSS. Zöllner et al37 showed that there is an increase in risk of 9.2% for each point increase in the score during admission. Abraira et al23 considered the NIHSS score important, since they observed that epilepsy occurs more frequently in patients with high scores and pointed out a correlation that is verified with cortical involvement. Finally, Krakow et al30 evaluated the severity of symptoms using mRs and recognized that severe neurological deficit is associated with an increased risk of seizures, but this is only true for patients with ischemic stroke and not for patients with hemorrhagic stroke. The authors explained that this is probably because generally patients with intracranial hemorrhage tend to have greater deficits, but cortical injury may be less; and this aligns with what was found in the present study, where the estimated effect of cortical involvement is always greater than the estimated effect of hemorrhage, regardless of whether the study reports its results with odds ratio or hazard ratio. In this same matter, the notions regarding a specific location of the lesions and the development of PSE do not have a strong correlation, only Tanaka et al34 mentioned that occipital lesions are associated with seizure recurrence, and Yamada et al36 identified frontal lobe involvement as a risk factor. Overall, retrospective studies were unable to investigate this type of variables because their datasets lacked the necessary details to establish size parameters or location. We believe that it is vital to standardize the examination of these data during the hospitalization to clarify the association between the extent of the lesion and the risk of PSE.
The significance of factors like cortical involvement, the connection between hemorrhagic stroke and early seizures, and the extent of the ischemic area for seizure development has been corroborated by other researchers.43 In the assessment of hemorrhagic stroke, an unexplored predictive tool called the LANE score, formulated within the Chinese population, incorporates four elements: lobar hemorrhage, age over 65 years, an NIHSS score exceeding 15, and the existence of early seizures (ES). The LANE score produces comparable statistics to the CAVE score.44
When looking at the model performances (discrimination and calibration) provided by the included studies they exhibit a moderate to acceptable punctuation, implying there is room for improvement. A variable that displays potential is the non-neurological infection. For Krakow et al30 this is a powerful predictor, but it involves many confounding variables in its analysis since the use of antibiotics or metabolic alterations related to the infection should also be evaluated.
Chi et al25 showed that non-neurological infections such as pneumonia increase the risk of PSE, but there is a correlation between prolonged hospital stay and infection. Therefore, they considered that on many occasions patient conditions require airway protection, dysphagia screening, and antibiotic measures to prevent conditions such as aspiration pneumonia, which reduces the seizure threshold and increases the likelihood of observing PSE. Consequently, a separate analysis was performed where variables were excluded and observed for difference in the predictive power of the model.
Considering the addition of EEG to the clinical variables that constitute the predictive tools yields no benefit in terms of PPV and low sensitivity, according to Strzelczyk et al33 so including it in the analyses or proposing it as an element that amplifies the predictive power is not very encouraging. Abraira et al23 made a brief mention to acknowledge that very few of the patients in their sample underwent EEG, so they considered it likely that seizures without motor symptoms had been overlooked. Galovic et al26 also mentioned that they did not use EEG as a predictive method; instead, they clarified that it refines follow-up conditions. In this context, an unexamined study by Bentes et al45 presented a contrary stance. After conducting a prospective investigation involving video EEG within the initial 72 hours of the patient’s admission the study revealed a 3.2-fold higher risk of PSE in patients with background activity asymmetry, even after adjusting for age, admission NIHSS score, and ASPECT. The risk was also increased 3.8 times when interictal epileptiform activity was present. The study identified periodic discharges as an independent predictor of epileptiform activity during hospitalization. The authors acknowledged that continuous EEG, while valuable, has limitations due to its time-consuming nature, need for specialized human resources, and limited accessibility in all centers, posing a constraint as an additional element in the described predictive tools.
Overall, risk models for the prediction of entities like PSE offer versatile applications, enhancing patient care of those who are at high risk, refining the research strategies for future clinical trials, and aiding our understanding of the disease mechanisms. While uncertainties and challenges remain, refining models and validating their performance will positively impact the patient’s outcomes while properly routing healthcare costs. Altogether, the well-recognized limitations associated with observational studies, if not appropriately addressed in a meta-analysis, can pose a risk to the conclusion drawn. Furthermore, the anticipated substantial diversity across populations, settings, and methodologies adds an additional layer of complexity to the synthesis of their results, but the utilization of the data obtained in these studies may offer a certain advantage over the RCTs due the inclusion of a richer pool of information, broader applicability of the findings, and the ability to assess infrequent and extended-term outcomes.
Limitations
Several limitations were identified, the primary limitation of this study was the significant heterogeneity observed in the included studies which restricted the generation of pooled estimates. Despite employing a comprehensive search strategy, it is possible that we may have missed some relevant studies. Furthermore, since all the included studies were observational the quality of evidence presented represents another limitation. Few studies that presented a predictive score presented the sensitivity and specificity values for these tools, thus, the data concerning that aspect could not be analyzed by this study.
Conclusion
Hemorrhage is one of the major risk factors; however, as far as hematoma size is concerned, there is no clear consensus on the correct way to measure its dimensions. Factors like acute non-neurological infection are reported as relevant but have not been evaluated in this review due to lack of data; furthermore, there are many elements related to this condition that could serve as confounding factors. This research identified biomarkers that amplified the predictive power of clinical variables, but they were not evaluated in other studies.
Few studies have attempted to create a predictive scale applicable to hemorrhagic stroke and ischemic stroke, but it is considered that, given the heterogeneity observed, the scales should be used accordingly to the etiology. The components included in the SeLECT and CAVE scores have demonstrated good predictive ability with low risk of bias and are therefore suggested for the stratification of patients at high risk, although it is recognized that these require further validation in other types of populations for wide clinical implementation.
Institutional Review Board Statement
The protocol was approved by the Human Research Ethics Committee of the Pontifical Catholic University of Ecuador, campus Quito-Ecuador, under the protocol number EO-166-2022, V1.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ropper AH, Klein JP, Samuels MA, et al., editors. Principios de neurología [Principles of Neurology].
2. Aminoff MJ, Josephson SA, Eds.. Aminoff’s Neurology and General Medicine.
3. Sacco RL, Kasner SE, Broderick JP, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064–2089. doi:10.1161/STR.0b013e318296aeca
4. Tanaka T, Ihara M. Post-stroke epilepsy. Neurochem Int. 2017;107:219–228. doi:10.1016/j.neuint.2017.02.002
5. Elkind MSV, Wing EJ, Schiffman FJ. Cecil Essentials of Medicine.
6. Institute for Health Metrics and Evaluation GBD Compare; 2019. Available from: http://vizhub.healthdata.org/gbd-compare.
7. Toro-Pérez JE, Villafuerte MV, Burneo JG. Epilepsia post ictus. Rev Neuropsiquiatr. 2013;75(2):58–65. doi:10.20453/rnp.v75i2.1310
8. Benninger F. HMBE, Beghi E, Benninger F, et al. European stroke organisation guidelines for the management of post-stroke seizures and epilepsy. Eur Stroke J. 2017;2(2):103–115. doi:10.1177/2396987317705536
9. Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55(4):475–482. doi:10.1111/epi.12550
10. Burn J, Dennis M, Bamford J, et al. Epileptic seizures after a first stroke: the Oxfordshire community stroke project. BMJ. 1997;315(7122):1582–1587. doi:10.1136/bmj.315.7122.1582
11. Pitkänen A, Engel J. Past and present definitions of epileptogenesis and its biomarkers. Neurotherapeutics. 2014;11(2):231–241. doi:10.1007/s13311-014-0257-2
12. Goldman L, Schafer AI. Goldman-Cecil Medicine.
13. Wang JZ, Vyas MV, Saposnik G, et al. Incidence and management of seizures after ischemic stroke: systematic review and meta-analysis. Neurology. 2017;89(12):1220–1228. doi:10.1212/WNL.0000000000004407
14. Castro-Apolo R, Huang JF, Vinan Vega M, et al. Outcome and predictive factors in post-stroke seizures: a retrospective case-control study. Seizure. 2018;62:11–16. doi:10.1016/j.seizure.2018.09.007
15. Kumar V, Aster J, Abbas AK, et al. Patología Humana.
16. Xie WJ, Dong M, Liu Q, et al. Early predictors and prevention for post-stroke epilepsy: changes in neurotransmitter levels. Transl Neurosci. 2016;7(1):1–5. doi:10.1515/tnsci-2016-0001
17. Kwon SY, Obeidat AZ, Sekar P, et al. Risk factors for seizures after intracerebral hemorrhage: ethnic/racial variations of intracerebral hemorrhage (ERICH) study. Clin Neurol Neurosurg. 2020;192:105731. doi:10.1016/j.clineuro.2020.105731
18. Tröscher AR, Gruber J, Wagner JN, et al. Inflammation mediated epileptogenesis as possible mechanism underlying ischemic post-stroke epilepsy. Front Aging Neurosci. 2021;13:781174. doi:10.3389/fnagi.2021.781174
19. Mula M, Sander JW. Psychosocial aspects of epilepsy: a wider approach. BJPsych Open. 2016;2(4):270–274. doi:10.1192/bjpo.bp.115.002345
20. Ferlazzo E, Gasparini S, Beghi E, et al. Epilepsy in cerebrovascular diseases: review of experimental and clinical data with meta-analysis of risk factors. Epilepsia. 2016;57(8):1205–1214. doi:10.1111/epi.13448
21. Lekoubou A, Debroy K, Kwegyir-Aggrey A, et al. Risk models to predict late-onset seizures after stroke: a systematic review. Epilepsy Behav. 2021;121:108003. doi:10.1016/j.yebeh.2021.108003
22. Wiśniewski A, Jatužis D. Multifactorial predictors of late epileptic seizures related to stroke: evaluation of the current possibilities of stratification based on existing prognostic models - A comprehensive review. Int J Environ Res Public Health. 2021;18(3):1079. doi:10.3390/ijerph18031079
23. Abraira L, Santamarina E, Cazorla S, et al. Blood biomarkers predictive of epilepsy after an acute stroke event. Epilepsia. 2020;61(10):2244–2253. doi:10.1111/epi.16648
24. Chen Z, Churilov L, Koome M, et al. Post-stroke seizures is associated with low Alberta stroke program early CT score. Cerebrovascular Dis. 2017;43(5–6):259–265. doi:10.1159/000458449
25. Chi NF, Kuan YC, Huang YH, et al. Development and validation of risk score to estimate 1-year late poststroke epilepsy risk in ischemic stroke patients. Clin Epidemiol. 2018;10:1001–1011. doi:10.2147/CLEP.S168169
26. Galovic M, Döhler N, Erdélyi Canavese B, et al. Prediction of late seizures after ischaemic stroke with a novel prognostic model (the select score): a multivariable prediction model development and validation study. Lancet Neurol. 2018;17(2):143–152. doi:10.1016/S1474-4422(17)30404-0
27. Graham NSN, Crichton S, Koutroumanidis M, et al. Incidence and associations of poststroke epilepsy: the prospective South London stroke register. Stroke. 2013;44(3):605–611. doi:10.1161/STROKEAHA.111.000220
28. Haapaniemi E, Strbian D, Rossi C, et al. The CAVE score for predicting late seizures after intracerebral hemorrhage. Stroke. 2014;45(7):1971–1976. doi:10.1161/STROKEAHA.114.004686
29. Kim HJ, Park KD, Choi KG, et al. Clinical predictors of seizure recurrence after the first post-ischemic stroke seizure. BMC Neurol. 2016;16(1):212. doi:10.1186/s12883-016-0729-6
30. Krakow K, Sitzer M, Rosenow F, et al. Predictors of acute poststroke seizures. Cerebrovascular Dis. 2010;30(6):584–589. doi:10.1159/000319777
31. Roivainen R, Haapaniemi E, Putaala J, et al. Young adult ischaemic stroke related acute symptomatic and late seizures: risk factors. Eur J Neurol. 2013;20(9):1247–1255. doi:10.1111/ene.12157
32. Serafini A, Gigli GL, Gregoraci G, et al. Are early seizures predictive of epilepsy after a stroke? Results of a population-based study. Neuroepidemiology. 2015;45(1):50–58. doi:10.1159/000382078
33. Strzelczyk A, Haag A, Raupach H, et al. Prospective evaluation of a post-stroke epilepsy risk scale. J Neurol. 2010;257(8):1322–1326. doi:10.1007/s00415-010-5520-9
34. Tanaka T, Yamagami H, Ihara M, et al. Seizure outcomes and predictors of recurrent post-stroke seizure: a retrospective observational cohort study. PLoS One. 2015;10(8):e0136200. doi:10.1371/journal.pone.0136200
35. Wang G, Jia H, Chen C, et al. Analysis of risk factors for first seizure after stroke in Chinese patients. Biomed Res Int. 2013;2013:1–9. doi:10.1155/2013/702871
36. Yamada S, Nakagawa I, Tamura K, et al. Investigation of poststroke epilepsy (INPOSE) study: a multicenter prospective study for prediction of poststroke epilepsy. J Neurol. 2020;267(11):3274–3281. doi:10.1007/s00415-020-09982-2
37. Zöllner JP, Misselwitz B, Kaps M, et al. National Institutes of Health Stroke Scale (NIHSS) on admission predicts acute symptomatic seizure risk in ischemic stroke: a population-based study involving 135,117 cases. Sci Rep. 2020;10(1):3779. doi:10.1038/s41598-020-60628-9
38. Wells G, Shea B, Peterson J, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa hospital research institute; 2000. Available from: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
39. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605. doi:10.1007/s10654-010-9491-z
40. Wolff RF, Moons KGM, Riley RD, et al. PROBAST: a tool to assess the risk of bias and applicability of prediction model studies. Ann Intern Med. 2019;170(1):51. doi:10.7326/M18-1376
41. Naydenov C, Prakova G, Tsokeva J, et al. Epilepsy in stroke as de novo independent nosology unit – physiology, pathogenesis, histology, clinical picture, diagnosis, and treatment – a systematic review. Open Access Maced J Med Sci. 2023;11(F):11–19. doi:10.3889/oamjms.2023.10976
42. Liang M, Zhang L, Geng Z, Flannery JG, MacLaren RE, Cehajic-Kapetanovic J. Advances in the development of biomarkers for poststroke epilepsy. Biomed Res Int. 2021;2021:1–8. doi:10.1155/2021/5567046
43. Dziadkowiak E, Guziński M, Chojdak-łukasiewicz J, et al. Predictive factors in post-stroke epilepsy: retrospective analysis. Adv Clin Exp Med. 2021;30(1):29–34. doi:10.17219/acem/128745
44. Wang Y, Li Z, Zhang X, et al. Development and validation of a clinical score to predict late seizures after intracerebral hemorrhage in Chinese. Epilepsy Res. 2021;172:106600. doi:10.1016/j.eplepsyres.2021.106600
45. Bentes C, Martins H, Peralta AR, et al. Early EEG predicts poststroke epilepsy. Epilepsia Open. 2018;3(2):203–212. doi:10.1002/epi4.12103
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.