Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Risk Factors Associated with a First Exacerbation Among Patients with COPD Classified as GOLD A and B in Routine Clinical Practice in the UK
Authors Rothnie KJ ![]() , Numbere B, Gelwicks S, Lu Y
, Numbere B, Gelwicks S, Lu Y ![]() , Sharma R, Compton C
, Sharma R, Compton C ![]() , Ismaila AS
, Ismaila AS ![]() , Quint JK
, Quint JK ![]()
Received 14 April 2023
Accepted for publication 30 October 2023
Published 21 November 2023 Volume 2023:18 Pages 2673—2685
DOI https://doi.org/10.2147/COPD.S413947
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Kieran J Rothnie,1 Beade Numbere,1 Steven Gelwicks,2 Yifei Lu,1,3 Raj Sharma,4 Chris Compton,4 Afisi S Ismaila,2,5 Jennifer K Quint6
1Value Evidence and Outcomes, R&D Global Medical, GSK, London, UK; 2Value Evidence and Outcomes, R&D Global Medical, GSK, Collegeville, PA, USA; 3Department of Epidemiology, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; 4Global Medical, GSK, London, UK; 5Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, ON, Canada; 6National Heart and Lung Institute, Imperial College London, London, UK
Correspondence: Kieran J Rothnie, Value Evidence and Outcomes, R&D Global Medical, GSK, 980 Great West Road, Brentford, Middlesex, London, TW8 9GS, UK, Tel +44 208 990 3439, Email [email protected]
Purpose: Risk factors for exacerbations of chronic obstructive pulmonary disease (COPD) have been previously characterized for patients with more severe cases of COPD. It is unclear how the risk of first exacerbation may best be identified in patients with less severe disease. This study investigated risk factors for first exacerbation among English patients with COPD classified as Global Initiative for Chronic Obstructive Lung Disease (GOLD) group A or B.
Patients and Methods: A retrospective cohort study using data from the UK Clinical Practice Research Datalink (CPRD) AURUM linked to Hospital Episode Statistics. Patients with COPD aged ≥ 35 years and classified as GOLD group A or B (2020 criteria) from January 2013–December 2019 were eligible. Patients were required to have 24 months history in CPRD (baseline). Two cohorts were defined: cohort 1 included patients with no severe exacerbations during baseline; cohort 2 included patients with no moderate or severe exacerbations during baseline. Risk factors associated with severe, or combined moderate and severe exacerbation were examined for up to 5 years of follow-up.
Results: Overall, 194,948 patients were included in cohort 1 (mean age 66.2 years; 55.2% male), and 148,396 patients in cohort 2 (mean age 66.1 years; 56.6% male). Identified risk factors for exacerbation (and associated 1-year absolute risk of severe, or combined moderate and severe exacerbation, respectively) included: Medical Research Council dyspnea scale score (15.9%/28.4%); COPD Assessment Test score (9.6%/25.3%); GOLD grade of airflow limitation (forced expiratory volume in 1 second % predicted; 13.6%/27.5%); and lung cancer (8.1%/23.6%). After adjustment for risk factors, these factors remained independently associated with severe exacerbation at 1, 3, and 5 years of follow-up.
Conclusion: The identified risk factors may aid physicians in the early recognition of patients with COPD classified as GOLD group A or B at risk of first exacerbation.
Keywords: COPD, CPRD, exacerbation, GOLD A/B, risk factor, UK
Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide, accounting for approximately 3.23 million deaths in 2019.1 In 2015, the global prevalence of COPD was estimated to be 174 million (104.7 million males and 69.7 million females).2 In the UK, the prevalence of diagnosed COPD continues to rise, with an estimated increase of 27% in the last decade.3 Direct costs related to COPD are estimated to be around £1.9 billion each year.4
Exacerbations of COPD are a key driver of the clinical and economic burden of the disease.5 Risk factors for COPD exacerbations have been widely characterized; the history of prior exacerbation is among the most important predictors of frequent exacerbation.6,7 Comorbidity, as well as the presence and severity of airflow limitation (as measured by forced expiratory volume in 1 second [FEV1] % predicted), have been identified as predictors of future exacerbations among patients with prior exacerbations.6 Other potential risk factors such as age, smoking status, and current medication use vary greatly between studies.8 However, among patients without an exacerbation history, it is unclear which factors put patients at higher risk of first exacerbation.
In 2017, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) introduced a revised “ABCD” assessment tool to categorize patients with COPD into one of four groups based upon their symptoms and exacerbation history, for the purpose of selecting an initial maintenance therapy.9 Patients classified as GOLD group B or D have a greater burden of respiratory symptoms; patients classified as GOLD group C or D are considered at higher risk of future events (ie exacerbations, hospital admissions, or death). However, the second highest rates of mortality and severe exacerbation (after group D) have been reported among GOLD group B patients, with levels of breathlessness reported as being a driving factor and associated with poor prognosis.10–13 A 2014 study reported that gastroesophageal reflux disease (GERD), chronic bronchitis, and breathlessness are significantly associated with elevated risk of exacerbation in patients with COPD, even among those without exacerbation history.14 However, many previous studies were conducted in specialist/secondary care and generally included more severe COPD cases. Whether and how such risk factors contribute to first COPD exacerbation in patients with less severe disease not requiring hospitalization is unknown.
Although inhaled corticosteroid (ICS) therapy is not recommended for patients in GOLD groups A or B according to clinical guidelines,15,16 addition of ICS to long-acting bronchodilator therapy is commonly seen in usual care as initial maintenance therapy.17 Identifying characteristics predictive of a first exacerbation among individuals with COPD who are naïve to ICS may help predict patients who would benefit from the earlier introduction of ICS. This study aimed to investigate risk factors for the first exacerbation among patients with COPD who were classified as GOLD group A or B, overall and stratified by ICS use at baseline.
Materials and Methods
Study Design and Data Source
This was a retrospective, observational cohort study of patients with COPD using primary care data from the UK Clinical Practice Research Datalink (CPRD) AURUM and linked secondary data from the Hospital Episode Statistics (HES) Admitted Patient Care database. CPRD-AURUM is a longitudinal electronic health record database containing the anonymized medical records of all patients registered with a contributing primary care practice across the UK. Data captured in CPRD include demographic information (age, sex, weight); records of clinical events (medical diagnoses); immunization records; diagnostic testing; lifestyle information (eg smoking status and alcohol status); and all other types of care administered as part of routine general practitioner (GP) practice. Linkage of CPRD-AURUM to HES is possible for a subset of approximately 25 million patients registered at GP practices in England that have consented to the linkage scheme. HES datasets contain details of all inpatient episodes of care (including day cases), outpatient appointments, and accident and emergency attendances.
The study design is shown in Figure 1. The study follow-up period spanned from January 2013 to December 2019. The index date was defined as the date 2 years after COPD diagnosis, January 1, 2011, registration at the practice, or of acceptable standard in CPRD, whichever was later. Patients were followed for up to 5 years after the index date, or until December 2019, death, or deregistration from the practice, whichever was earliest. Two separate cohorts were defined: cohort 1 included patients with no prior severe exacerbations in the 24-month pre-index period; cohort 2 included patients with no prior moderate or severe exacerbations in the 24-month pre-index period. Patients were classified as using ICS when there were ≥2 prescriptions within the 24-month pre-index period, at least one of which was within 3 months before, or on, the index date.
 |
Figure 1 Study design. Abbreviations: COPD, chronic obstructive pulmonary disease; GP, general practitioner; ICS, inhaled corticosteroid. |
Study Population
Patients aged ≥35 years with a COPD diagnosis, an FEV1/forced vital capacity <0.7, and who were classified as GOLD group A or B (according to GOLD 2020 criteria) between January 2013 and December 2019 were eligible for inclusion. Patients were required to have 24 months history in CPRD-AURUM prior to the index date and records linked to HES. Patients were excluded from the study if they had a severe exacerbation (cohort 1) or a moderate or severe exacerbation (cohort 2) in the 24 months prior to index, or if they had record of a code for a medical condition incompatible with a COPD diagnosis (including conditions that are related to lung or bronchial developmental anomalies, degenerative processes [cystic fibrosis, pulmonary fibrosis], pulmonary resection, or other significant respiratory disorders other than COPD that can interfere with clinical COPD diagnosis or substantially change the natural history of the disease; those with cancer were not excluded from the study) at any time in their patient history. A 24-month baseline period was used in the study to ensure that patients did not have more than one moderate exacerbation or any severe exacerbations during baseline.
Study Outcomes
The primary objective of the study was to identify factors associated with increased risk of first severe exacerbation in patients with no prior history of severe exacerbations (cohort 1); the secondary objective was to identify factors associated with increased risk of first moderate or severe exacerbation in patients with no prior history of moderate or severe exacerbations (cohort 2); and the exploratory objective was to identify factors associated with increased risk of first moderate exacerbation in patients with no prior history of moderate or severe exacerbations (cohort 2). Outcomes were described for all patients overall and stratified by ICS use at baseline. Measurement and definition of potential risk factors predictive of a first COPD exacerbation are shown in Supplementary Table S1.
COPD exacerbations were identified from CPRD-AURUM and HES (using International Classification of Disease, 10th revision codes) based on a validated algorithm.18,19 Exacerbations resulting in hospitalization (ie recorded in HES and CPRD) were considered severe, while exacerbations managed only in primary care (ie only recorded in CPRD) were considered moderate. Exacerbations on the index date were included. Moderate exacerbations were defined as a record of one of the four following events: prescriptions for antibiotics and oral corticosteroids for a length of 5–14 days each (both prescriptions must have had the same start date but each could last for a different number of days); presence of respiratory symptoms (codes suggesting an increase in two or more of: breathlessness, cough, or sputum volume and/or purulence recorded on the same date) and a prescription for antibiotics or oral corticosteroids (or both) on the same day; lower respiratory tract infection medical code; or a COPD exacerbation-specific medical code.18
The proportion of patients with a severe (primary objective), moderate or severe (secondary objective), or moderate (exploratory objective) exacerbation at 1, 3, and 5 years following the index date was described overall and stratified by: FEV1% predicted (<30%, 30–<50%, 50–<80%, ≥80%); number of moderate exacerbations in the prior year (0 or 1; for primary objective); Medical Research Council (MRC) dyspnea scale score; COPD Assessment Test (CAT) score; comorbidities; and blood eosinophil levels (<150, ≥150–< 300, ≥300 cells/μL). The denominator was determined as included patients who had follow-up at 1, 3, and 5 years after index. Multivariable Cox regression was used to examine the hazard ratio of first exacerbation associated with the above characteristics over up to 5 years of follow-up from index.
Results
Baseline Characteristics
A total of 194,948 patients with COPD were included in cohort 1 (no prior severe exacerbations) and 148,396 patients were included in cohort 2 (no prior moderate or severe exacerbations) (Figure 2). Demographic characteristics of patients included in cohort 1 and cohort 2, overall and stratified by ICS use at baseline, are shown in Table 1; comorbidities at baseline are shown in Supplementary Table S2.
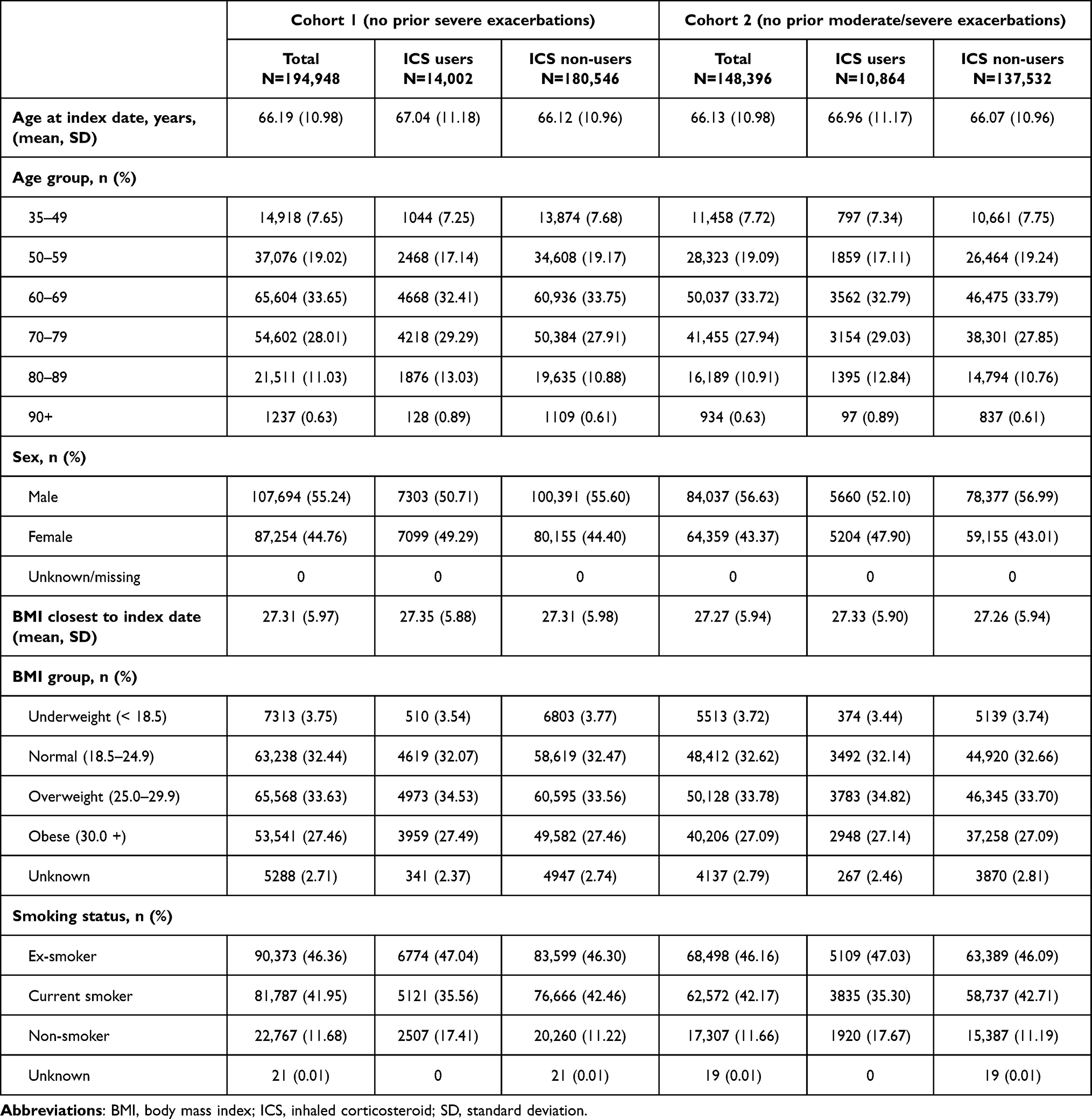 |
Table 1 Demographic characteristics of patients included in cohort 1 and cohort 2, overall and stratified by ICS use at baseline |
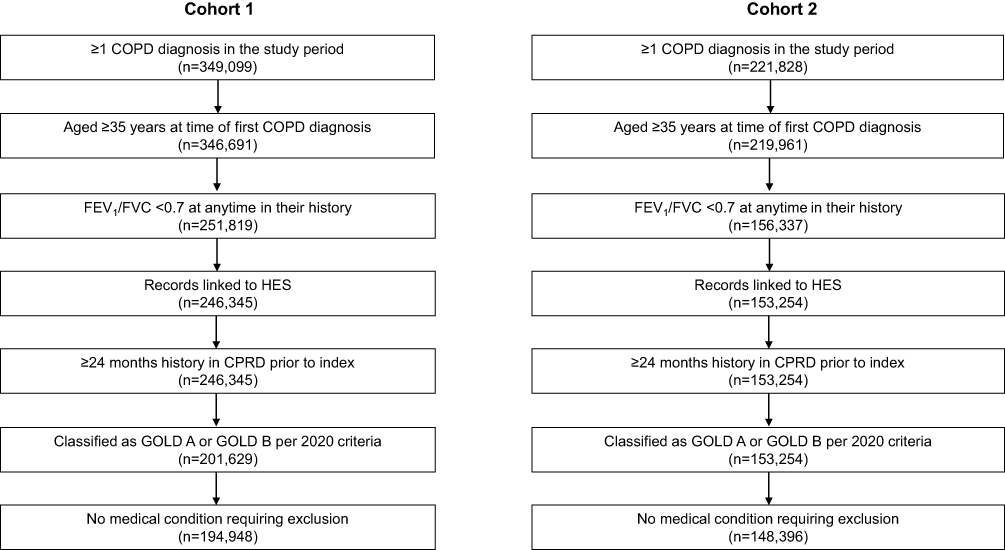 |
Figure 2 Patient attrition. Abbreviations: COPD, chronic obstructive pulmonary disease; CPRD, Clinical Practice Research Datalink; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HES, Hospital Episode Statistics. |
Of the 194,948 patients included in cohort 1, 14,002 (7.2%) had documented ICS use prior to index. The mean (standard deviation [SD]) age at index was 66.2 (11.0) years, and 55.2% were male. The most common comorbidities among patients in cohort 1 were depression (29.8%), rheumatoid/osteo arthritis (28.0%), anxiety (18.0%), and GERD (13.4%). Of the 148,396 patients included in cohort 2, 10,864 (7.3%) had documented ICS use prior to index. The mean (SD) age at index was 66.1 (11.0) years, and 56.6% were male. The most common comorbidities among patients in cohort 2 were depression (29.0%), rheumatoid/osteo arthritis (27.3%), anxiety (17.4%), and GERD (12.9%).
Risk Factor Characteristics
The distribution of potential risk factors for COPD exacerbation among included patients is shown in Supplementary Table S3.
Among patients in cohort 1, 67.2% were classified as GOLD A and 32.8% were classified as GOLD B. In total, 11.8% of patients in cohort 1 had a moderate exacerbation in the baseline period. Most patients had an MRC dyspnea grade 2 (38.5%), followed by grade 3 (22.0%) and grade 1 (20.7%), and the majority of patients with available data had a CAT score indicative of less severe respiratory symptoms (around 8% for both 0–9 and 10–19 groups; 78% of patients had unknown CAT score). The FEV1% predicted values followed the same pattern, with most patients having either moderate or mild airflow limitation. The most commonly used respiratory medication at baseline was short-acting β2-agonist (SABA; 72.7%). The most recently used respiratory medications prior to the index date were SABA (27.3%), ICS/long-acting β2-agonist (ICS/LABA; 20.8%), and ICS/long-acting muscarinic antagonist/LABA (ICS/LAMA/LABA; 15.5%). Similar risk factor distribution patterns were observed for patients in cohort 2 (Supplementary Table S3).
Absolute Risk of Severe COPD Exacerbation
At MRC dyspnea grade 1, there was a 2.1% absolute risk of severe exacerbation at 1 year, which increased across the scale to a 15.9% absolute risk at MRC grade 5 (Figure 3). CAT score 0–9 was associated with a 2.6% absolute risk of severe exacerbation at 1 year, which increased across scores to a 9.6% absolute risk at CAT score 30–40. For FEV1% predicted values, at the highest level (≥80%) there was a 2.4% absolute risk of severe exacerbation at 1 year; the absolute risk increased as FEV1% predicted values decreased (13.6% absolute risk at FEV1% predicted <30%). The presence of comorbidities including acute myocardial infarction, congestive heart failure, stroke, bronchiectasis, and lung cancer were associated with an elevated risk of exacerbation versus patients without these comorbidities (7.1% vs 4.5%, 8.5% vs 4.5%, 7.1% vs 4.5%, 7.1% vs 4.6%, and 8.1% vs 4.6%, respectively) at 1 year; conversely, the presence of depression, anxiety, or GERD was not associated with an elevated risk of exacerbation a 1 year (Supplementary Figure S1). At each risk factor level, the 1-year absolute risk of severe COPD exacerbation was slightly greater among ICS non-users compared with ICS users. The absolute risk patterns of severe exacerbation across risk factor levels remained largely similar at 3 years and 5 years of follow-up; however, the magnitude was greater when more years of observation were included (Figure 3).
 |
Figure 3 Absolute risk of severe exacerbation across different levels of risk factors among patients in cohort 1. Abbreviations: CAT, Chronic Obstructive Pulmonary Disease Assessment Test; GOLD, Global Initiative for Chronic Obstructive Lung Disease; MRC, Medical Research Council. |
Hazard Ratio of Severe COPD Exacerbation
After adjustment for risk factors, the Cox proportional hazards modeling showed that most potential risk factors were associated with an increased rate of severe exacerbation at 1 year of follow-up (Figure 4A).
 |
Figure 4 Hazard ratio of severe exacerbation at (A) 1 year, (B) 3 years, and (C) 5 years post-index by risk factors. Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; MRC, Medical Research Council. |
A higher rate of severe COPD exacerbation was observed among those with a moderate COPD exacerbation at baseline (hazard ratio [HR]: 1.14, 95% confidence interval [CI]: 1.06–1.23) compared with those without a moderate exacerbation (reference group). Of note, when stratified by ICS use, moderate exacerbation (1 vs 0) during baseline was found to be predictive of severe exacerbation at 1 year of follow-up among ICS non-users (HR: 1.16, 95% CI: 1.07–1.25) but not among ICS users (HR: 1.00, 95% CI: 0.77–1.36). FEV1% predicted values ≥30–<50% and <30% were associated with a 30.0%, and 82.2% increased rate of severe COPD exacerbation, respectively; FEV1% predicted ≥50–<80% showed a non-significant increase in severe exacerbation compared with the reference group (FEV1% predicted ≥80%). Patients with an MRC dyspnea grade 2 showed a non-significant increase in the rate of severe exacerbation compared with MRC grade 1 (reference group); however, patients with an MRC grade 3, 4, and 5 showed an increased rate of severe COPD exacerbation of 29.4%, 61.8%, and 117.6%, respectively, compared with the reference group. In the model restricted to patients with available CAT score, higher CAT scores were associated with a higher rate of severe COPD exacerbation when compared with the lowest CAT score level of 0–9 (reference group), with HRs of 1.44 for CAT score 10–19, 1.55 for CAT score 20–29, and 1.47 for CAT score 30–40. The presence of lung cancer was also associated with a higher risk of severe exacerbation (HR: 1.42, 95% CI: 1.26–1.59), as was anxiety (HR: 1.11, 95% CI: 1.02–1.20), myocardial infarction (HR: 1.16, 95% CI: 1.06–1.26), and congestive heart failure (HR: 1.16, 95% CI: 1.07–1.27). Other examined comorbidities (including bronchiectasis and GERD) were not associated with an increased risk of severe exacerbation.
Conversely, a current asthma diagnosis (HR: 0.92, 95% CI: 0.86–0.99) or historical asthma diagnosis (HR: 0.86, 95% CI: 0.81–0.93) was found to be associated with a lower risk of severe COPD exacerbation at 1 year of follow-up. When stratified by ICS use, asthma diagnosis remained protective in association with severe exacerbation for both ICS users and non-ICS users; the magnitude of the association was stronger in ICS users versus non-ICS users (current asthma diagnosis: ICS users HR 0.70 vs non-ICS users HR 0.94; historical asthma diagnosis: ICS users HR 0.52 vs non-ICS users HR 0.90). Eosinophil levels of ≥150–<300 cells/µL were also associated with a significantly lower risk of severe COPD exacerbation compared with eosinophils <150 cells/µL (reference group) (HR: 0.92, 95% CI: 0.86–0.98), as was female sex (7.3% lower rate of severe COPD exacerbation compared with male sex). When stratified by ICS use, eosinophil levels ≥150–300 cells/µL remained protective in association with severe exacerbation among non-ICS users but not ICS users (non-ICS users HR 0.91 [95% CI 0.85–0.97]; ICS users HR 1.09 [95% CI 0.84–1.04]). Largely consistent patterns were observed between risk factors and severe COPD exacerbations at 3 years and 5 years of follow-up, with a few exceptions (Figure 4B and C).
Absolute Risk of Moderate/Severe COPD Exacerbation
At MRC dyspnea grade 1, there was a 12.9% absolute risk of moderate to severe exacerbation at 1 year, which increased across the grades to a 28.4% absolute risk at MRC grade 5 (Figure 5). CAT score 0–9 was associated with a 13.5% absolute risk of moderate to severe exacerbation at 1 year, which increased across scores to a 25.3% absolute risk of moderate to severe exacerbation at CAT score 30–40. For FEV1% predicted values, at the highest level (≥80%) there was a 13.5% absolute risk of moderate to severe exacerbation at 1 year; the absolute risk increased as FEV1% predicted values decreased (27.5% absolute risk at FEV1% predicted <30%). The presence of all examined comorbidities was associated with an increased risk of exacerbation at 1 year (Supplementary Figure S2). At each risk factor level, the 1-year absolute risk of moderate to severe COPD exacerbation was largely comparable between ICS non-users and ICS users. The absolute risk patterns of severe exacerbation across risk factor levels remained largely similar at 3 years and 5 years of follow-up (Figure 5).
 |
Figure 5 Absolute risk of moderate or severe exacerbation across different levels of risk factors among patients in cohort. Abbreviations: CAT, Chronic Obstructive Pulmonary Disease Assessment Test; GOLD, Global Initiative for Chronic Obstructive Lung Disease; MRC, Medical Research Council. |
Hazard Ratio of Moderate/Severe COPD Exacerbation
After adjustment for risk factors, the Cox proportional hazards modeling showed that most potential risk factors were associated with an increased rate of moderate to severe exacerbation at 1 year of follow-up (Figure 6A).
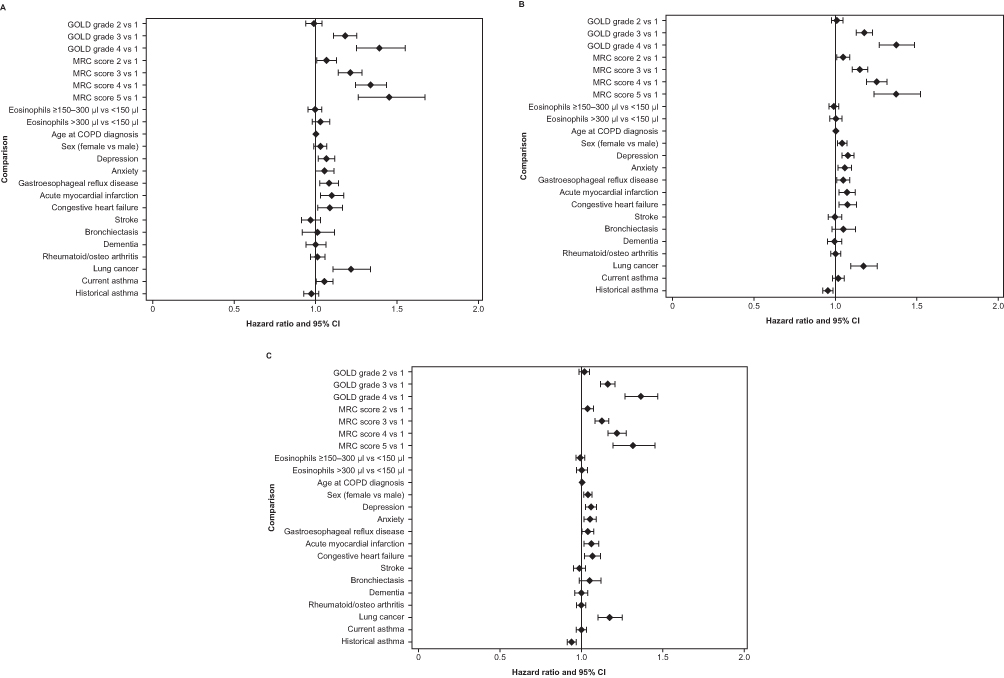 |
Figure 6 Hazard ratio of moderate or severe exacerbation at (A) 1 year, (B) 3 years, and (C) 5 years post-index by risk factors. Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; MRC, Medical Research Council. |
FEV1% predicted values ≥30–<50% and <30% were associated with a 18.0%, and 39.3% increased rate of moderate to severe COPD exacerbation, respectively; FEV1% predicted ≥50–<80% showed a non-significant increase in moderate to severe exacerbations compared with the reference group (FEV1% predicted ≥80%). Patients with MRC dyspnea grade 2, 3, 4, and 5 showed an increased rate of moderate to severe COPD exacerbation of 6.6%, 21.1%, 33.8%, and 45.3%, respectively, compared with patients with MRC grade 1 (reference group). In the model restricted to patients with available CAT score, CAT score 10–19, 20–29, and 30–40 was associated with a 10.3%, 15.8%, and 36.3% higher rate of moderate to severe COPD exacerbation, respectively, when compared with the lowest CAT score level of 0–9 (reference group). The presence of lung cancer was also associated with a higher risk of moderate or severe exacerbation (HR: 1.22, 95% CI: 1.11–1.34), as was depression (HR: 1.07, 95% CI: 1.02–1.12), GERD (HR: 1.08, 95% CI: 1.03–1.14), myocardial infarction (HR: 1.10, 95% CI: 1.03–1.17), congestive heart failure (HR: 1.09, 95% CI: 1.01–1.16), and current asthma diagnosis (HR: 1.06, 95% CI: 1.01–1.11). Largely consistent association patterns were observed between each risk factor and moderate to severe COPD exacerbation at 3 years and 5 years of follow-up with only a few exceptions (Figure 6B and C).
Risk of Moderate COPD Exacerbation
Results of the exploratory analysis are presented in the Supplementary Appendix (Supplementary Results R1 and R2, Figures S3 and S4).
Discussion
This study identified factors associated with an increased risk of first severe, first moderate or severe, or first moderate exacerbation among patients with COPD classified as GOLD group A or B, overall, and stratified by ICS use at baseline.
Among patients with no prior severe or moderate/severe exacerbations during baseline (cohorts 1 and 2), GOLD grade of airflow limitation (FEV1% predicted), CAT score, and MRC dyspnea score were associated with the largest increased risk of exacerbation at 1 year. Notably, lower FEV1% predicted values and higher symptom scores were bigger predictors (ie, larger HRs) of severe exacerbation events. This is suggestive that as well as predicting the frequency of future events, risk factors can also predict the severity of future events. Clinicians should keep this in mind when assessing the risk of future events for their patients with COPD.
Among patients with no severe exacerbations during baseline (cohort 1), previous moderate exacerbation, depression, anxiety, myocardial infarction, congestive heart failure, and lung cancer were significantly associated with severe exacerbation at 1 year. These risk factors remained significantly associated with severe exacerbation at 3 years and 5 years. Although cardiovascular comorbidities were not major predictors of exacerbation (ie, HRs were not as high as for other predictors eg, FEV1% predicted and MRC dyspnea scale score), this study focused on first exacerbation; this result may not be the same among patients with more severe disease (ie, GOLD grade C/D). Of note, comorbid GERD was not associated with an increased risk of exacerbation in this cohort of patients. Eosinophil count ≥150–300 µL, the presence of rheumatoid/osteo arthritis and current or historical asthma were found to be protective for severe exacerbation at 1, 3, and 5 years of follow-up among this cohort. Among ICS users, there was no evidence of GOLD grade of airflow limitation, CAT score, or lung cancer being associated with increased risk of severe exacerbation; MRC dyspnea score (grade 4 and 5) and stroke were shown to be risk factors of severe exacerbation among this population. This may suggest that the use of ICS had ameliorated the risk associated with these factors; however, the low percentage of ICS users (7%) likely had limited power to show association between other risk factors and severe exacerbation.
Among patients with no prior moderate or severe exacerbations during baseline (cohort 2), depression, GERD, acute myocardial infarction, congestive heart failure, and lung cancer were significantly associated with moderate/severe exacerbation at 1 year. Many of these risk factors (except GERD) remained significantly associated with severe exacerbation at 3 years and 5 years. Among ICS users, there was no evidence that COPD GOLD grade of airflow limitation, CAT score, and MRC dyspnea scale grade 2, 3, or 5 were associated with moderate/severe exacerbation. However, MRC dyspnea scale grade 4 and lung cancer were shown to be risk factors for moderate/severe exacerbation at 1 year. When moderate exacerbations were examined as the outcome of interest, many potential risk factors were associated with an increased risk of exacerbation at 1, 3, and 5 years of follow-up.
To the authors’ knowledge, this is the first study to examine risk factors for exacerbation in patients with COPD classified as GOLD A or B as a combined group, and the only study to include a 5-year follow-up period. Of note, even when adjusted for lung function, symptoms scores (MRC and CAT) were identified as predictive factors for exacerbation in the current study; conversely, comorbid asthma and blood eosinophil count were not predictive of exacerbation risk. This is consistent with a recent study from SPIROMICS, in which neither baseline blood nor sputum eosinophils were found to be associated with exacerbation risk20 and a post-hoc analysis of real-world study data, which reported that whilst exacerbation history was a reliable predictor of future exacerbations, blood eosinophil was not;21 previous mixed findings may be due to an enrichment of studies including patients with a history of exacerbations. Risk factors for exacerbation in patients classified as GOLD group B in Denmark have previously been examined;22 similar factors to the current study were identified (FEV1% predicted and MRC score). However, female sex was also identified as a risk factor, which differs from the current study.
This analysis was conducted among all patients and among patients stratified by ICS use at baseline. The majority of patients in the current study were ICS non-users; the potential risk factors for exacerbation that were identified may be useful in guiding earlier use of ICS where appropriate. Other future research should focus on better understanding potential risk factors for exacerbations among patients with COPD and implementing these findings in the clinical management of patients, for example, via individual patient prognostic modeling.23,24
To note, although the study period pre-dated the GOLD 2020 strategy, the criteria for classification of patients into GOLD A or GOLD B groups (via MRC score, CAT score, and prior exacerbation history) in the GOLD 2020 strategy is the same as the previous GOLD strategy,9 and similar to the prior 2011 strategy.25 The classification criteria for GOLD A and GOLD B also remains unchanged in the current GOLD 2023 strategy.15
The results of this study should be considered in the context of a few potential limitations. To make sure that the first exacerbation in the observation period was identified for each patient, it was specified that participants had to survive for 2 years with no exacerbations before entry. This may have introduced some element of survivor bias and is likely to have biased towards a less severe population. Therefore, the current estimates of absolute risk should be seen as conservative. There is the possibility of asthma being mis-diagnosed as COPD and vice versa, particularly in patients aged ≥40 years. The sensitivity of the algorithm for moderate exacerbations was around 70% (meaning approximately 30% of moderate exacerbations were not picked up by the algorithm);18 reported absolute risk estimates are therefore conservative. Also, CAT scores were missing for some patients; although using a 24-month baseline period for assessment of CAT score decreased missingness, it should be noted that the analysis population for MRC and CAT were different. Finally, although lung cancer was included as an exposure of interest, it may be complicated to differentiate COPD exacerbations in patients with acute episodes of deterioration associated with lung cancer itself, meaning any “signal” of a higher risk of exacerbation associated with lung cancer should be interpreted with caution.
Conclusions
This study identified risk factors associated with an increased risk of first severe or first moderate/severe exacerbation in patients with COPD classified as GOLD group A or B at 1, 3, and 5 years of follow-up. Among patients with no prior severe exacerbations (cohort 1), MRC dyspnea score, CAT score, GOLD grade of airflow limitation (FEV1% predicted), lung cancer, previous moderate exacerbation, age, depression, anxiety, acute myocardial infarction, and congestive heart failure were significantly associated with severe exacerbation at 1 year. Among patients with no prior moderate or severe exacerbations (cohort 2), MRC dyspnea score, CAT score, FEV1% predicted, lung cancer, age, depression, GERD, acute myocardial infarction, congestive heart failure, and current asthma were significantly associated with moderate/severe exacerbation at 1 year. Blood eosinophil count was not predictive of exacerbation risk. The identified risk factors can aid physicians in the early identification of patients with COPD classified as GOLD A or B at risk of first exacerbation, and who may benefit from earlier optimization of therapy to prevent exacerbations.
Abbreviations
CAT, COPD Assessment Test; CI, confidence interval; COPD, chronic obstructive pulmonary disease; CPRD, Clinical Practice Research Datalink; FEV1, forced expiratory volume in 1 second; GERD, gastroesophageal reflux disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; GP, general practitioner; HES, Hospital Episode Statistics; HR, hazard ratio; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; MRC, Medical Research Council; SABA, short-acting β2-agonist; SD, standard deviation.
Data Sharing Statement
The data analyzed in this publication are derived from the Clinical Practice Research Datalink (www.cprd.com) and Hospital Episode Statistics database (https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/hospital-episode-statistics). The data are provided by patients and collected by the NHS as part of their care and support. Authors had access to the study data for the purposes of this work only. The interpretation and conclusions contained in this study are those of the authors alone. Data were accessed through an existing GSK license to address the prespecified research questions only. Therefore, the data cannot be broadly disclosed or made publicly available at this time. Access to each database can be requested via the respective websites. Contains information from NHS Digital, licensed under the current version of the Open Government License. Copyright © (2022), re-used with the permission of The Health & Social Care Information Centre. All rights reserved.
Ethics Approval and Informed Consent
This study complied with all applicable laws regarding patient privacy. No direct patient contact or primary collection of individual patient data occurred; therefore, informed patient consent was not required. This study was approved by CPRD (study number 21_000600). Generic ethical approval for observational research approved by CPRD has been granted by a Health Research Authority Research Ethics Committee (East Midlands-Derby, UK; REC reference number 5/MRE04/87).
Acknowledgments
Editorial support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing, and referencing) was provided by Rebecca Cunningham of Apollo, OPEN Health Communications, and was funded by GSK. Data from this study have previously been presented in abstract/poster presentation form at the 2022 European Respiratory Society – 32nd Annual Congress. The abstract was published in. European Respiratory Journal Sep 2022, 60 (suppl 66) 647; DOI: 10.1183/13993003.congress-2022.647. Available from https://erj.ersjournals.com/content/60/suppl_66/647.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the manuscript; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by GSK (study number 217450). GSK-affiliated authors were involved in study conception and design, data analysis, data interpretation, and the decision to submit the article for publication. GSK funded the article processing charges and open access fee.
Disclosure
Kieran J Rothnie, Steven Gelwicks, Raj Sharma, Chris Compton, and Afisi S Ismaila are employees of GSK and/or hold stocks/shares in GSK. Afisi S Ismaila is also an unpaid part-time member of the McMaster University faculty. Beade Numbere is an employee of CY Partners Recruitment Ltd and on assignment at GSK as a Complementary Worker. Yifei Lu is a university worker of GSK and a graduate researcher at University of North Carolina at Chapel Hill. Jennifer K Quint has received research grants from The Health Foundation, MRC, HDR UK, GSK, Bayer, Boehringer Ingelheim, asthma+lung, Chiesi, and AstraZeneca; and personal fees for advisory board participation or speaking fees from GSK, Boehringer Ingelheim, AstraZeneca, Chiesi, Insmed, and Bayer. The authors report no other conflicts of interest in this work.
References
1. WHO Chronic obstructive pulmonary disease (COPD); 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
2. NICE Chronic obstructive pulmonary disease: how common is it?; 2023. Available from: https://cks.nice.org.uk/topics/chronic-obstructive-pulmonary-disease/background-information/prevalence-incidence/.
3. British Lung Foundation Chronic obstructive pulmonary disease (COPD) statistics; 2022. Available from: https://statistics.blf.org.uk/copd.
4. British lung foundation the battle for breath - the impact of lung disease in the UK; 2016. Available from: https://statistics.blf.org.uk/.
5. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic burden of chronic obstructive pulmonary disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/COPD.S234942
6. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
7. Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
8. Adibi A, Sin DD, Safari A, et al. The Acute COPD Exacerbation Prediction Tool (ACCEPT): a modelling study. Lancet Respir Med. 2020;8(10):1013–1021. doi:10.1016/S2213-2600(19)30397-2
9. GOLD Global Initiative for Chronic Obstructive Lung Disease - global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2017 report; 2017. Available from: https://goldcopd.org/wp-content/uploads/2017/02/wms-GOLD-2017-FINAL.pdf.
10. Gedebjerg A, Szépligeti SK, Wackerhausen LH, et al. Prediction of mortality in patients with chronic obstructive pulmonary disease with the new Global Initiative for Chronic Obstructive Lung Disease 2017 classification: a cohort study. Lancet Respir Med. 2018;6(3):204–212. doi:10.1016/S2213-2600(18)30002-X
11. Agusti A, Edwards LD, Celli B, et al. Characteristics, stability and outcomes of the 2011 GOLD COPD groups in the ECLIPSE cohort. Eur Respir J. 2013;42(3):636–646. doi:10.1183/09031936.00195212
12. Punekar YS, Mullerova H, Small M, et al. Prevalence and burden of dyspnoea among patients with chronic obstructive pulmonary disease in five European countries. Pulm Ther. 2016;2(1):59–72. doi:10.1007/s41030-016-0011-5
13. Sansbury LB, Rothnie KJ, Bains C, Compton C, Anley G, Ismaila AS. Healthcare, medication utilization and outcomes of patients with COPD by GOLD classification in England. Int J Chron Obstruct Pulmon Dis. 2021;16:2591–2604. doi:10.2147/COPD.S318969
14. Martinez CH, Okajima Y, Murray S, et al. Impact of self-reported gastroesophageal reflux disease in subjects from COPDGene cohort. Respir Res. 2014;15(1):62. doi:10.1186/1465-9921-15-62
15. GOLD Global Initiative for Chronic Obstructive Lung Disease - global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2023 report; 2022. Available from: https://goldcopd.org/2023-gold-report-2/.
16. NICE Chronic obstructive pulmonary disease in over 16s: diagnosis and management; 2018. Available from: https://www.nice.org.uk/guidance/ng115/resources/chronic-obstructive-pulmonary-disease-in-over-16s-diagnosis-and-management-pdf-66141600098245.
17. Price D, Miravitlles M, Pavord I, et al. First maintenance therapy for COPD in the UK between 2009 and 2012: a retrospective database analysis. NPJ Prim Care Respir Med. 2016;26:16061. doi:10.1038/npjpcrm.2016.61
18. Rothnie KJ, Müllerová H, Hurst JR, et al. Validation of the recording of acute exacerbations of COPD in UK primary care electronic healthcare records. PLoS One. 2016;11(3):e0151357. doi:10.1371/journal.pone.0151357
19. Rothnie KJ, Müllerová H, Thomas SL, et al. Recording of hospitalizations for acute exacerbations of COPD in UK electronic health care records. Clin Epidemiol. 2016;8:771–782. doi:10.2147/CLEP.S117867
20. Hastie A, Quibrera PM, Couper D, et al. Neither baseline blood nor sputum eosinophils predict future exacerbations in the SPIROMICS cohort. Eur Respir J. 2022;60(suppl 66):959. doi:10.1183/13993003.congress-2022.959
21. Worth H, Buhl R, Criee CP, Kardos P, Guckel E, Vogelmeier CF. In ‘real world’ patients with COPD, exacerbation history, and not blood eosinophils, is the most reliable predictor of future exacerbations. Respir Res. 2023;24(1):2. doi:10.1186/s12931-023-02311-x
22. Løkke A, Hilberg O, Lange P, et al. Disease trajectories and impact of one moderate exacerbation in GOLD B COPD patients. Int J Chron Obstruct Pulmon Dis. 2022;17:569–578. doi:10.2147/COPD.S344669
23. Roche N, Devillier P, Berger P, et al. Individual trajectory-based care for COPD: getting closer, but not there yet. ERJ Open Res. 2021;7(4):00451–02021. doi:10.1183/23120541.00451-2021
24. Steyerberg EW, Eijkemans MJ, Van Houwelingen JC, Lee KL, Habbema JD. Prognostic models based on literature and individual patient data in logistic regression analysis. Stat Med. 2000;19(2):141–160. doi:10.1002/(SICI)1097-0258(20000130)19:2<141::AID-SIM334>3.0.CO;2-O
25. Vestbo J, Hurd SS, Rodriguez-Roisin R. The 2011 revision of the global strategy for the diagnosis, management and prevention of COPD (GOLD)–why and what? Clin Respir J. 2012;6(4):208–214. doi:10.1111/crj.12002
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pulmonologists’ Opinion on the Use of Inhaled Corticosteroids in Chronic Obstructive Pulmonary Disease Patients in Spain: A Cross-Sectional Survey
Miravitlles M, González-Torralba F, Represas-Represas C, Pomares X, Márquez-Martín E, González C, Amado C, Forné C, Alonso S, Alcázar B, Barrecheguren M, Jurado Mirete JM, Naval E
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1577-1587
Published Date: 12 July 2022
Lack of COPD-Related Follow-Up Visits and Pharmacological Treatment in Swedish Primary and Secondary Care
Sandelowsky H, Janson C, Wiklund F, Telg G, de Fine Licht S, Ställberg B
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1769-1780
Published Date: 9 August 2022
The Effect of Maintenance Treatment with Erdosteine on Exacerbation Treatment and Health Status in Patients with COPD: A Post-Hoc Analysis of the RESTORE Dataset

Calverley PMA, Papi A, Page C, Rogliani P, Dal Negro RW, Cazzola M, Cicero AF, Wedzicha JA
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1909-1920
Published Date: 22 August 2022
Burden of Disease in Patients with Mild or Mild-to-Moderate Chronic Obstructive Pulmonary Disease (Global Initiative for Chronic Obstructive Lung Disease Group A or B): A Systematic Literature Review
Czira A, Purushotham S, Iheanacho I, Rothnie KJ, Compton C, Ismaila AS
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:719-731
Published Date: 29 April 2023
Prevalence of Chronic Obstructive Pulmonary Disease in England from 2000 to 2019
Stone PW, Osen M, Ellis A, Coaker R, Quint JK
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1565-1574
Published Date: 21 July 2023