Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 16
Risk and Survival Outcomes of Secondary Primary Malignancies in Chinese Lymphoma Patients in the Era of Modern Targeted Therapies: A Single-Center Retrospective Cohort Study
Authors Qiu C, Zhang T ![]() , Yang X, Guo Y, Gong Z, Song D
, Yang X, Guo Y, Gong Z, Song D
Received 20 April 2026
Accepted for publication 7 July 2026
Published 14 July 2026 Volume 2026:16 616235
DOI https://doi.org/10.2147/BLCTT.S616235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Wilson Gonsalves
Chen Qiu,1,2,* Tingting Zhang,1,2,* Xuejing Yang,3,* Yafang Guo,4 Zihui Gong,5 Dong Song1,2
1Department of Lymphoma, Shanxi Bethune Hospital (Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University), Taiyuan, Shanxi, People’s Republic of China; 2Sino-German Joint Oncological Research Laboratory, Shanxi Bethune Hospital (Shanxi Academy of Medical Sciences), Taiyuan, Shanxi, People’s Republic of China; 3Department of Thoracic Oncology, Shanxi Bethune Hospital (Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University), Taiyuan, Shanxi, People’s Republic of China; 4Department of Hematology, Shanxi Bethune Hospital (Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University), Taiyuan, Shanxi, People’s Republic of China; 5Pre-Medical Program, School of Arts and Sciences, Massachusetts College of Pharmacy and Health Sciences, Boston, Massachusetts, USA
*These authors contributed equally to this work
Correspondence: Dong Song, Email [email protected]
Introduction: With the advent of modern therapies, including rituximab and novel oral targeted agents such as BTK inhibitors, the survival of lymphoma patients has significantly improved. However, the risk of secondary primary malignancies (SPMs) remains a critical concern. This study aims to evaluate the incidence, risk factors, latency, and survival outcomes of SPMs in lymphoma patients treated in the era of targeted therapies.
Methods: A retrospective cohort study was conducted on 1,715 lymphoma patients diagnosed between October 2011 and October 2024 at Shanxi Bethune Hospital, China. Patients with incomplete records, pediatric cases, or immunodeficiency were excluded. Data on demographics, lymphoma characteristics, treatment modalities, and SPMs were collected. SPMs were classified as synchronous (diagnosed within 6 months of lymphoma) or metachronous (diagnosed after 6 months). Statistical analyses included Cox regression for risk factors and Kaplan-Meier for survival analysis.
Results: Among 1,715 lymphoma patients, 65 (3.8%) developed SPMs, including 10 synchronous (0.6%, descriptive enumeration only), while 55 (3.2%) developed metachronous SPMs that constituted the primary analytic cohort. Aggressive B-cell non-Hodgkin lymphoma (43.6%) was the most common lymphoma subtype among patients who developed SPMs, followed by indolent B-cell non-Hodgkin lymphoma (38.2%). Digestive and respiratory system tumors were the predominant SPMs (34.5% and 23.6%, respectively). Multivariate analysis identified male sex, ECOG performance status ≥ 2, extranodal involvement, bone marrow infiltration, BTK inhibitor use, and radiotherapy as independent risk factors for SPMs. Competing-risk analysis showed a higher cumulative incidence of SPMs in patients exposed to BTK inhibitors than in those not exposed to BTK inhibitors (5-year CIF, 7.92% vs 2.57%; Gray’s test =0.007). Kaplan-Meier analysis showed that patients with SPMs had significantly worse OS than those without SPMs (median OS, 10.3 years; 5-year OS, 69.6% vs 89.6%; log-rank < 0.0001). No significant difference in OS was observed between patients with solid and hematologic SPMs (median OS, 12.8 vs 6.0 years; =0.76).
Discussion: In the transitional era of conventional and targeted therapies, although data are limited.This exploratory analysis confirmed that gastrointestinal and respiratory SPMs predominated in this Asian cohort, and identified male sex, ECOG ≥ 2, extranodal involvement, bone marrow infiltration, radiotherapy, and BTK inhibitor use as independent risk factors. The association with BTK inhibitors (HR=2.56) warrants cautious interpretation and prospective validation. Early detection and tailored surveillance (prioritizing gastrointestinal screening) are essential for improving long-term outcomes.
Keywords: lymphoma, secondary primary malignancies, targeted therapy, risk factors
Introduction
Lymphomas are a heterogeneous group of malignancies affecting the lymphatic system, representing approximately 5% of all hematologic cancers. Traditionally, it is classified into Non-Hodgkin lymphoma (NHL) and Hodgkin lymphoma (HL) based on the morphology of the tumor cells. NHL is the most common type of malignant lymphoma, accounting for approximately 85–90% of all lymphoma cases in Western populations and a similarly predominant proportion in China.1–3 According to the latest global cancer statistics (GLOBOCAN 2022), an estimated 5.8/100,000 new cases of lymphoma were diagnosed worldwide in 2022, with China accounting for approximately 17.1% of global NHL cases.1,2,4,5 The therapeutic landscape for lymphoma has undergone significant changes over the past two decades, notably marked by the integration of the anti-CD20 monoclonal antibody rituximab into standard regimens and the introduction of molecular targeted agents like BTK inhibitors.3,6–8 These advancements have substantially enhanced both progression-free survival (PFS) and overall survival (OS) among lymphoma patients, transforming lymphoma into a condition requiring prolonged surveillance for potential treatment-related complications, such as SPMs. Epidemiological studies have highlighted elevated standardized incidence ratios (SIRs) of both hematologic and solid organ malignancies in lymphoma survivors.6
The pathogenesis of SPMs is particularly associated with the genotoxic effects of treatments including alkylating agents, topoisomerase II inhibitors, and ionizing radiation. These therapies are known to cause dose-dependent damage to clonal hematopoietic cells and impair DNA repair pathways. For rituximab, to date no conclusive evidence has demonstrated a direct increase in SPM risk; its long-term safety profile appears favorable. The hypothetical possibility of very late mutagenic effects, however, cannot be entirely excluded and remains a subject of ongoing surveillance.9–18 The impact of novel agents, especially BTK inhibitors that modulate B-cell receptor signaling chronically, on genomic instability and secondary carcinogenesis is not yet fully understood.6,9
Moreover, most existing SPM data are derived from Western populations (eg, SEER‑based studies), and their applicability to Asian populations remains uncertain. Substantial differences between Asian and Western populations have been documented in lymphoma subtype distribution, genetic susceptibility (eg, TP53 R72P polymorphisms), lifestyle factors (eg, smoking and diet), and healthcare access – all of which influence SPM risk. Therefore, evaluating SPM incidence, risk factors, and survival outcomes specifically in a Chinese cohort is essential for developing region‑appropriate surveillance strategies.
The primary novelty of this study is the evaluation of BTK inhibitor‑associated SPM risk specifically in a Chinese lymphoma cohort, an area for which evidence remains extremely limited. We also aimed to explore the incidence, clinico‑pathological determinants, latency, and survival outcomes of SPMs in the era of modern targeted therapies.
Materials and Methods
Study Design and Patient Population
This retrospective study initially identified 2,106 Chinese patients with pathologically confirmed primary lymphoma (classified according to WHO) who were treated at the Cancer Center of Shanxi Bethune Hospital,China, between October 2011 and October 2024. Patients with pediatric cases (age < 18 years, n=58) were excluded, leaving 2,048 adult patients. Patients with human immunodeficiency virus infection (n=36) or those who had undergone allogeneic hematopoietic stem cell transplantation or solid organ transplantation (n=33) were then excluded due to their inherently higher risk of malignancies related to immunodeficiency. Subsequently, patients with incomplete medical records (n=178), unconfirmed pathological diagnoses (n=67), or postmortem findings (n=19) were excluded. Thus, 1,715 adult patients with complete medical records were retained. All eligible patients were consecutively enrolled from the hospital’s electronic medical record system; no sampling method was applied. From this cohort, patients with lymphoma but without multiple primary malignancies (n=1,621) were excluded. Consequently, 94 adult patients with lymphoma and multiple primary malignancies were identified. Among these, 29 were further excluded: 16 with histological transformation and 13 with second primary lymphoma in survivors of other malignancies. Ultimately, 65 patients with lymphoma as the primary malignancy and subsequent second primary malignancies (SPMs) were included in the final analysis, comprising 55 metachronous SPMs and 10 synchronous SPMs (Figure 1).
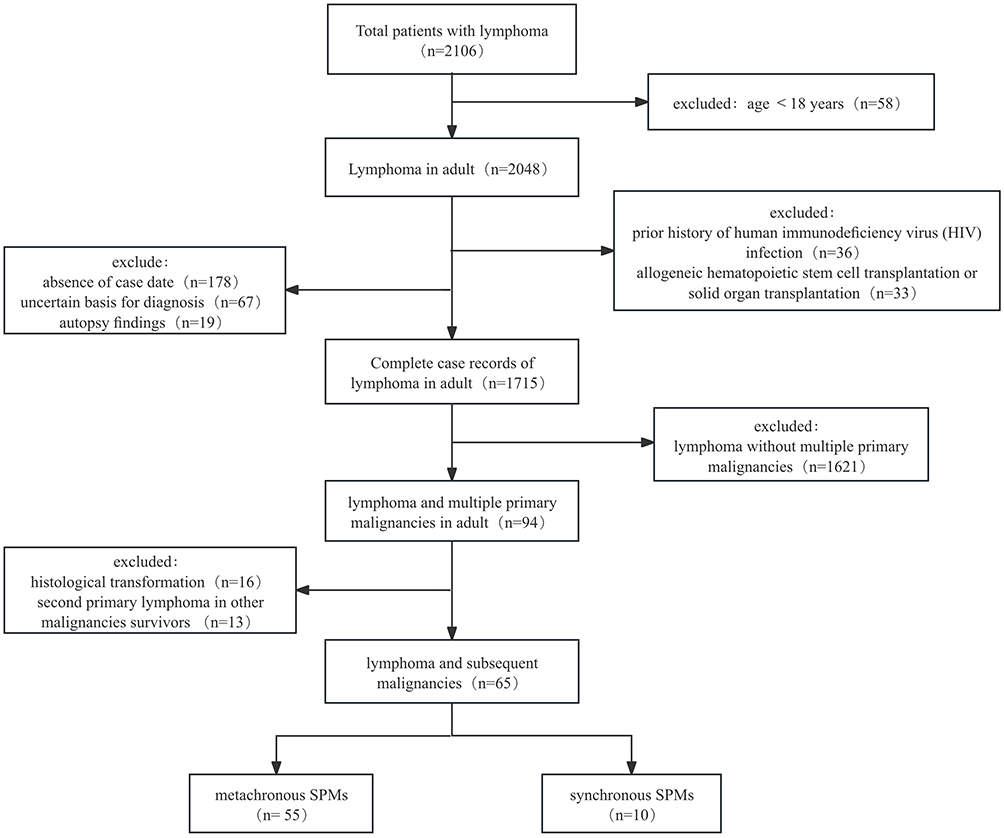 |
Figure 1 Inclusion and exclusion flow charts. |
Data Collection
Data collection was structured into four key domains to ensure a comprehensive analysis. The first domain encompassed demographic characteristics, including age, sex, date of birth, marital status, comorbidities, and family history of cancer. The second domain, oncological characteristics, detailed the date of lymphoma diagnosis, histological subtype, staging (utilizing Binet staging for chronic lymphoid leukemia and Ann Arbor staging for other forms), the International Prognostic Index (IPI) score, primary site of the lymphoma, extranodal involvement (both number and specific sites), Detailed information on chemotherapy cycles (total number from all phases), radiotherapy sites and cumulative doses, and BTK inhibitor treatment line and duration was extracted from electronic medical records, presence of bulky disease, B symptoms, levels of lactate dehydrogenase (LDH), and β2-microglobulin (β2-MG), along with the lymphoma’s status at the time SPM diagnosis. Treatment modalities composed the third domain, comprising surgical interventions, chemotherapy, radiotherapy, targeted therapy, and immunotherapy. The final domain focused on survival data, presenting OS and the latency period between the diagnosis of lymphoma and SPM.
SPMs were defined according to the Warren and Gates criteria, which require that each malignancy be histologically confirmed, distinct from the primary lymphoma, and not represent a metastasis. SPMs were methodologically classified as synchronous if they were diagnosed within six months of the initial lymphoma diagnosis, and as metachronous if diagnosed after this period. Synchronous SPMs were enumerated for descriptive completeness but were excluded from risk-factor and latency analyses, as their pathogenesis likely differs from therapy-related metachronous neoplasms.
Follow-Up Protocol
Patients were followed up through a combination of outpatient visits and telephone interviews. The follow-up period began at the date of lymphoma diagnosis and ended at the date of SPM diagnosis, death, or the study cutoff date (October 31, 2024), whichever occurred first. OS was defined as the time from lymphoma diagnosis to death from any cause or the last follow-up date. OS1 (latency time) was defined as the time from lymphoma diagnosis to SPM diagnosis. OS2 was defined as the time from SPM diagnosis to death or the last follow-up date.
Statistical Analysis
Data were extracted from the hospital’s electronic medical record system. No a priori sample size calculation was performed because the sample size was determined by the number of eligible patients with complete data over the study period (retrospective design). To ensure accuracy, trained personnel independently entered all data using a double-entry method, followed by cross-validation by senior researchers. Missing values were observed for LDH, β2-microglobulin, and ECOG performance status in 0.6%, 1.0%, and 1.3% of patients, respectively. Because the proportion of missing data was low, multiple imputation by chained equations was performed to minimize potential bias and preserve statistical power. All subsequent analyses were conducted using the imputed datasets. Continuous variables with normal distributions were presented as mean±standard deviation, while non-normally distributed variables were reported as median (interquartile range, IQR).
Univariate and multivariate Cox proportional hazards regression models were employed to identify risk factors associated with SPMs. Variables with a significance level of (p<0.05) in univariate analysis were included in the multivariate model. Kaplan-Meier curves were generated to estimate cumulative survival rates, and between-group differences were compared using the Log rank test. For multiple subgroup survival comparisons, P values were adjusted using the Benjamini–Hochberg false discovery rate (FDR) method to control for multiplicity. To account for the competing risk of death before the development of secondary primary malignancies (SPMs), a competing-risk analysis was performed. SPM occurrence was defined as the event of interest, and death before SPM diagnosis was treated as a competing event. The cumulative incidence function (CIF) was estimated according to BTK inhibitor exposure, and between-group differences were compared using Gray’s test. Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated based on the follow-up duration (defined as the interval from lymphoma diagnosis to the study endpoint). Statistical analyses were performed using SPSS 26.0 (IBM Corp., Armonk, NY, USA) and R software version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Clinical Characteristics of Lymphoma
Among 1,715 lymphoma patients, 10 (0.6%) presented with synchronous SPMs (Table 1), while 55 (3.2%) developed metachronous SPMs during a median follow-up of 8.26years (IQR, 5.86–11.06 years) (Table 2). Among patients with metachronous SPMs, aggressive B-cell NHL was the most common lymphoma subtype (43.6%, n=24/55), including 22 diffuse large B-cell lymphoma (DLBCL) and 2 mantle cell lymphoma (MCL), followed by indolent B-cell NHL (38.2%, n=21/55), HL (12.7%, n=7/55), and T-NHL (5.5%, n=3/55). (P<0.001). The cohort exhibited a striking male predominance (male-to-female ratio: 2.9:1), with a median age of 65 years at SPM diagnosis (range: 38–82 years). Hypertension emerged as the most prevalent comorbidity (40.0%, n=22/55). Treatment modalities for the index lymphoma included chemotherapy-based regimens (85.5%, n=47/55), radiotherapy (14.5%, n=8/55), anti-CD20 monoclonal antibodies (49.1%, n=27/55), and novel oral targeted agents (16.4%, n=9/55), including BTK inhibitors (n=9) and lenalidomide (n=2) (Table 2). Notably, 47.3% (n=26/55) of patients had received 4–8 cycles of prior chemotherapy before SPM diagnosis (Table 3).
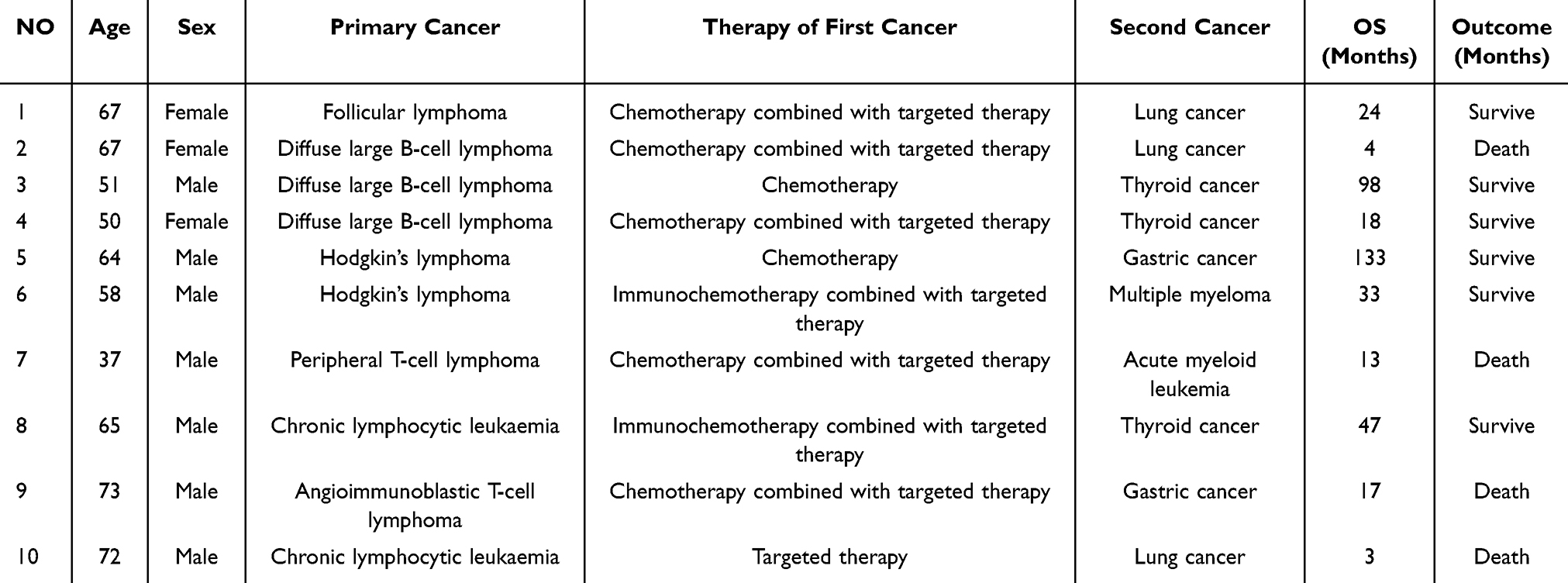 |
Table 1 Characteristics of the Patients with Synchronous Malignancies |
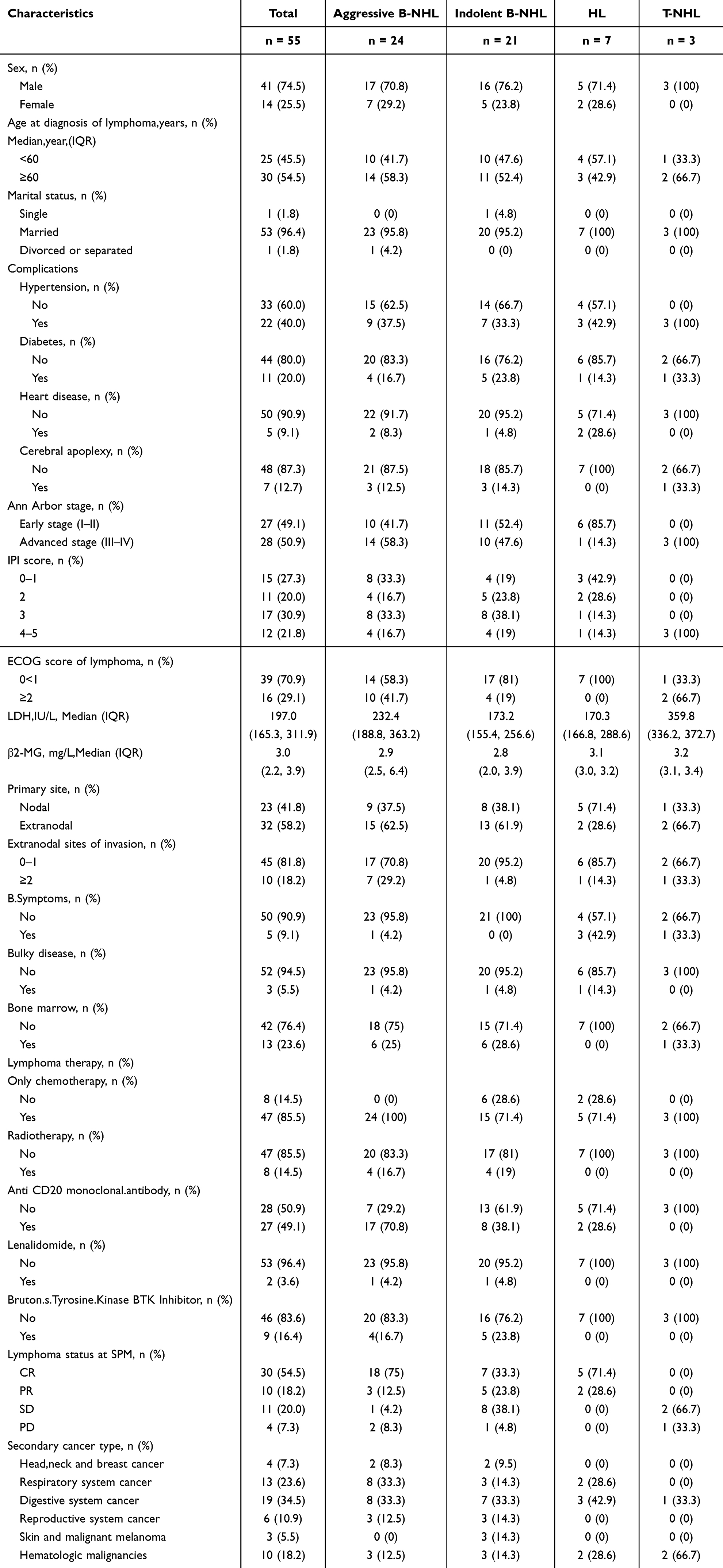 |
Table 2 Basic Clinical Characteristics of Included Populations |
SPM Subtypes and Clinical Management
Among the 55 patients with metachronous SPMs (Figure 2), predominantly gastrointestinal (34.5%, n=19/55; including colorectal [n=9], gastric [n=6], and hepatobiliary [n=4] cancers) and respiratory malignancies (23.6%, n=13/55; lung cancer [n=11], mesothelioma [n=2]). Hematologic SPMs (n=10/55) included acute myeloid leukemia (AML, n=2), acute lymphoblastic leukemia (ALL, n=1), chronic myeloid leukemia (CML, n=1), multiple myeloma (MM, n=1), and secondary NHL (n=5). Two patients developed tertiary malignancies (both solid tumors), and one developed quaternary tumors.
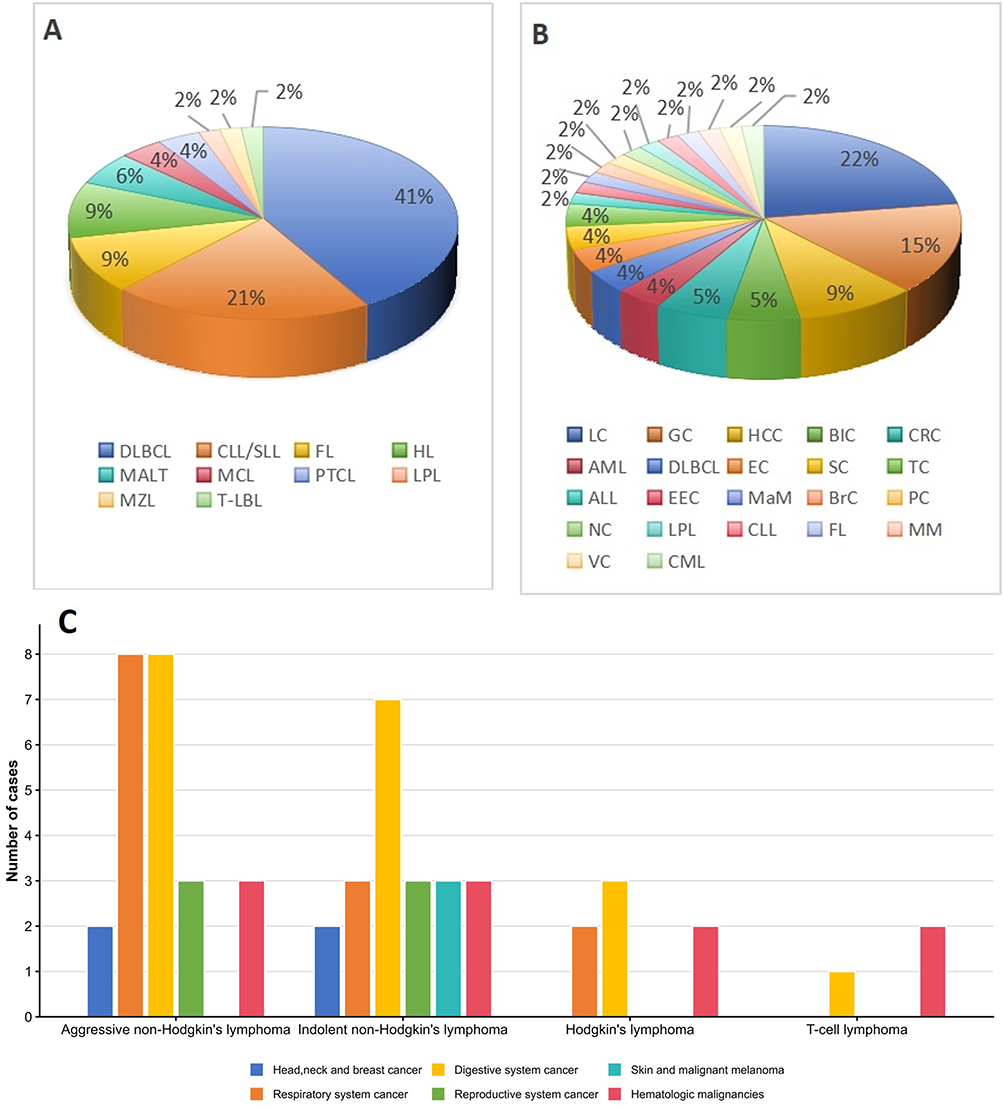 |
Figure 2 The detailed distribution of secondary malignancies among the 55 lymphoma patients. (A) Distribution of lymphoma types. (B). Types and proportions of secondary malignancies. (C). Types and case numbers of secondary malignancies for each lymphoma type. Abbreviations: NHL, non-Hodgkin lymphoma; HL, Hodgkin lymphoma; ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; MM, multiple myeloma; DLBCL, diffuse large B-cell lymphoma; FL, follicular lymphoma; CLL/SLL, chronic lymphocytic leukemia/small lymphocytic leukemia; MALT, extranodal marginal zone B-cell lymphoma of the mucosa associated lymphoid tissue; MZL, marginal zone B cell lymphoma; MCL, mantle cell lymphoma; LPL, plasmacytoma; AITL, angioimmunoblastic T-cell lymphoma; PTCL, peripheral T-cell lymphoma; NPC, nasopharynx cancer; TC, thyroid cancer; BC, Breast cancer; LC, lung cancer; CRC, colorectal cancer; GC, gastric cancer; EC, esophageal cancer; HCC, hepatocellular cancer; EEC, endometrial cancer; CC, cervicalcancer; VC, vaginal cancer; BlC, bladder cancer; PC, prostatic cancer; SC, skin cancer; MaM, malignant melanoma. |
At SPM diagnosis, 54.5% (n=30/55) of patients were in complete remission from their index lymphoma. Solid SPMs (n=45) were managed primarily with surgery (40.0%, n=18/45) or radiotherapy (22.2%, n=10/45), whereas hematologic SPMs (n=10) required systemic therapies, including chemotherapy (100%, n=10/10) and targeted agents (Table 3).
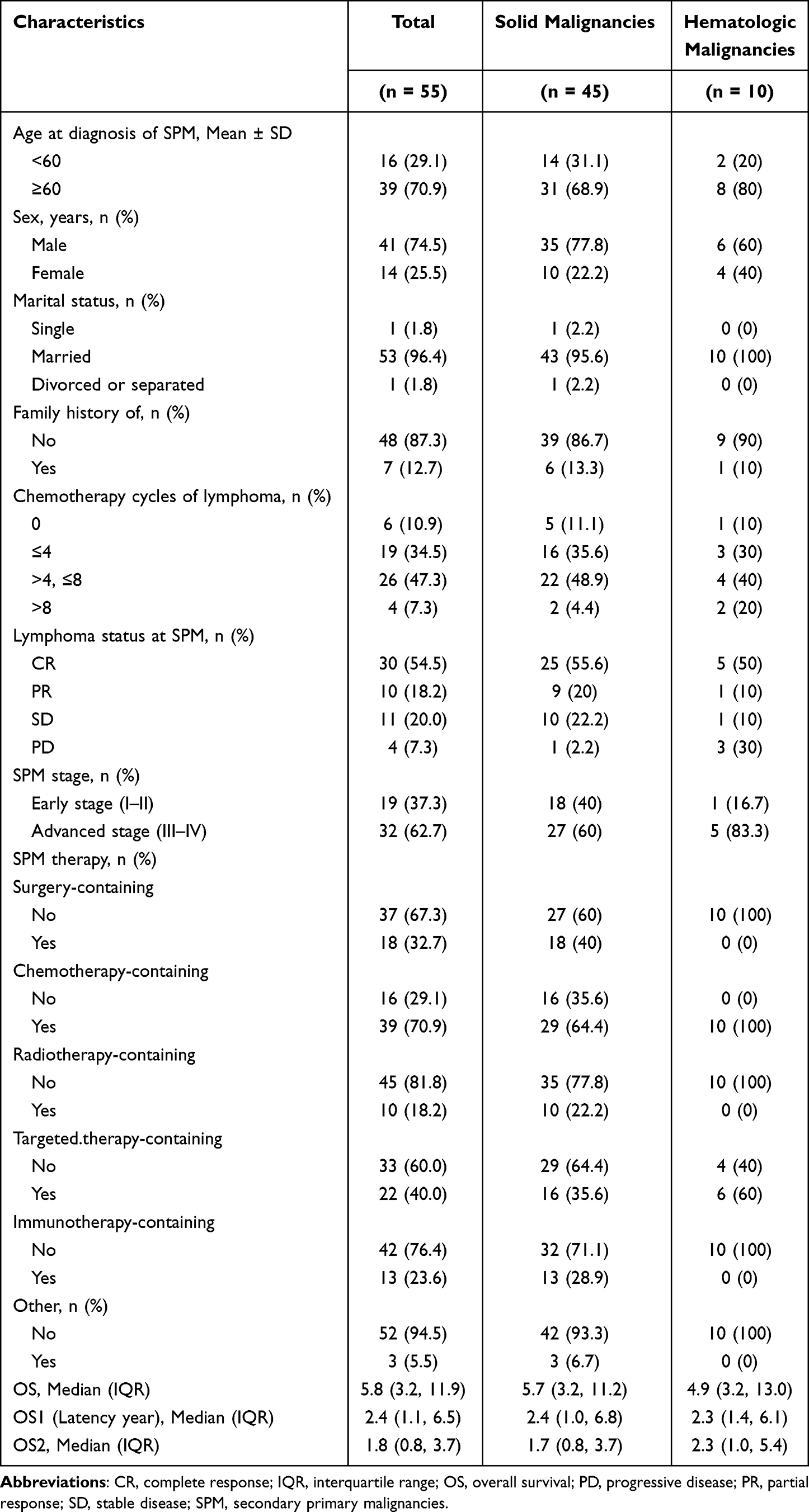 |
Table 3 Basic Clinical Characteristics of Secondary Malignancies |
Risk Factors for SPM Development
Multivariate Cox regression of metachronous SPMs confirmed male sex (HR=2.65, 95% CI: 1.42–4.92), ECOG performance status ≥2 (HR=3.15, 95% CI: 1.62–6.10), extranodal involvement (HR=2.84, 95% CI: 1.60–5.02), bone marrow infiltration (HR=2.66, 95% CI: 1.35–5.26), and exposure to radiotherapy (HR=4.09, 95% CI: 1.79–9.36) or BTK inhibitors (HR=2.56, 95% CI: 1.16–5.63) as independent predictors for SPMs (Table 4 and Figure 3). Among the 101 patients who received BTK inhibitors, 9 (8.9%) developed metachronous SPMs. All nine patients were on continuous BTK inhibitor therapy at the time of SPM diagnosis, with treatment lines distributed as follows: first-line (n=2), second-line (n=5), and third-line (n=2). No SPMs occurred after BTK inhibitor discontinuation.
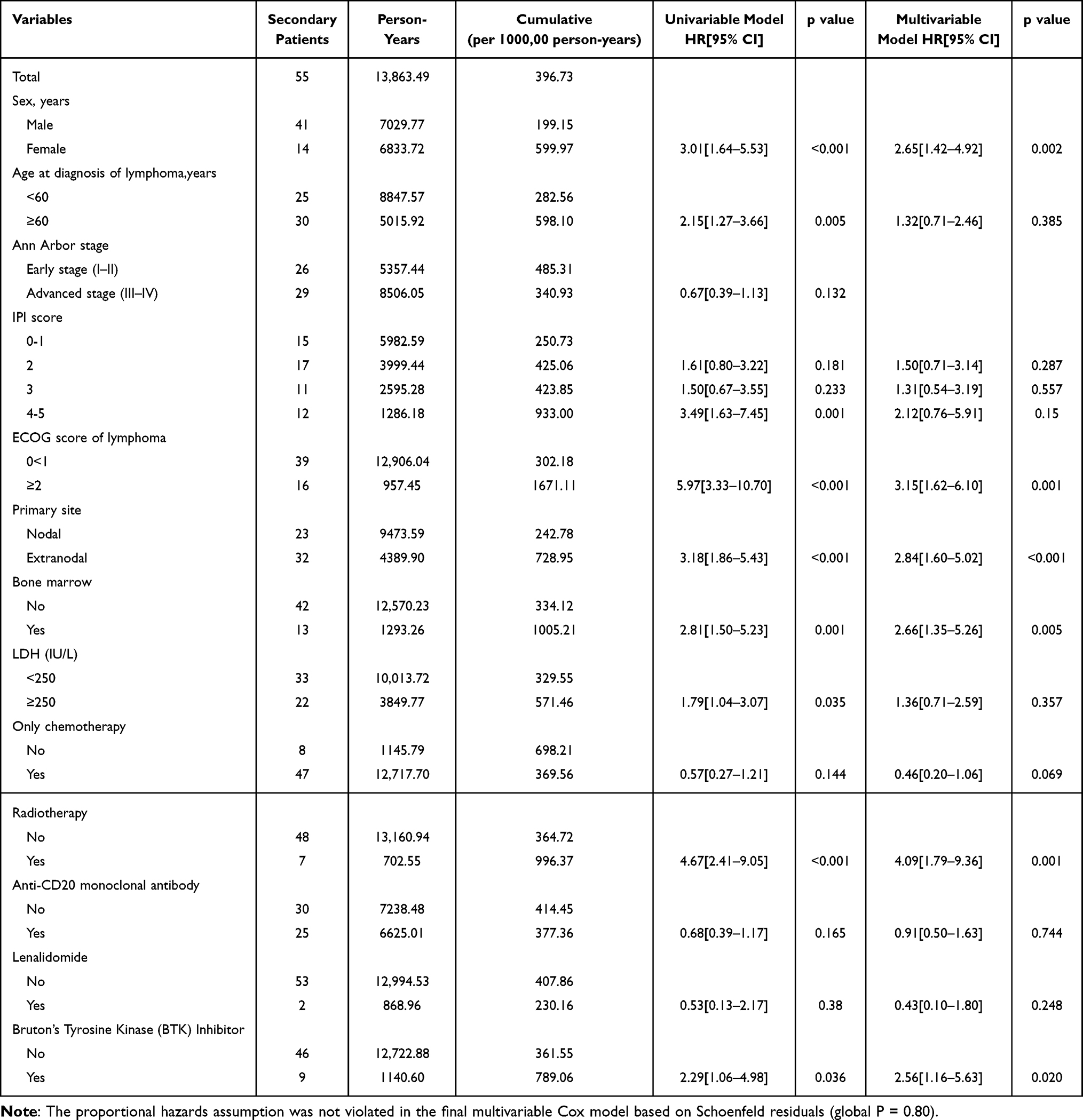 |
Table 4 Univariable and Multivariable Analysis of Risk Factors for second Primary Malignancy |
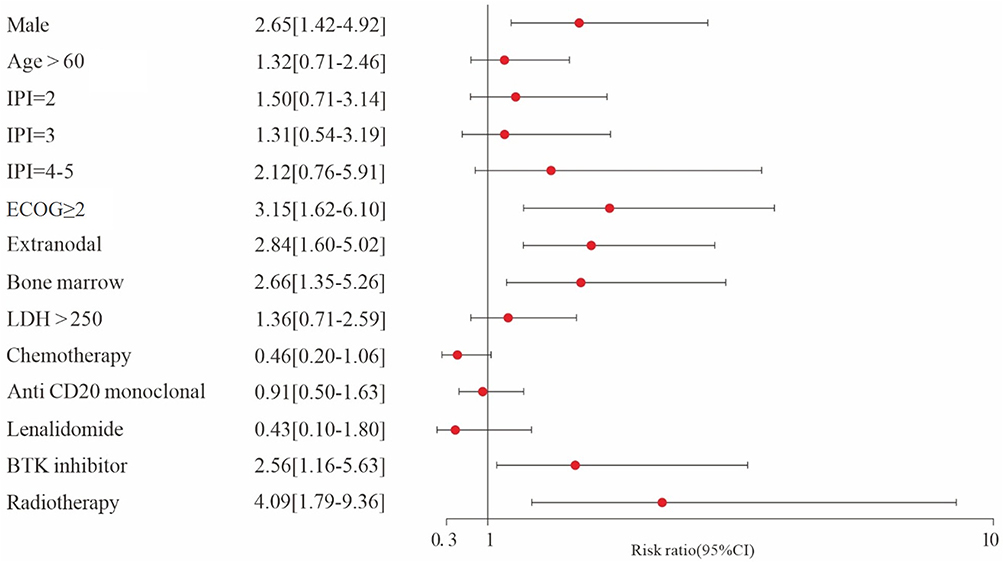 |
Figure 3 Forest plot of hazard ratios for secondary primary malignancies risk factors. |
Latency Period of SPMs (OS1)
The median latency period from lymphoma diagnosis to SPM development was 2.41years (IQR, 1.08–6.54 years). Subgroup analysis revealed shorter latencies in aggressive B-NHL (2.79years IQR, 1.00–7.89) and T-NHL (2.58years IQR, 1.95–2.83) compared to HL (5.75years IQR, 1.25–11.83) (P=0.01) (Figure 4A). However, no significant difference was observed between solid (2.41years IQR, 1.00–6.83) and hematologic SPMs (2.37years IQR, 1.41–6.12) (P=0.92) (Figure 4B).
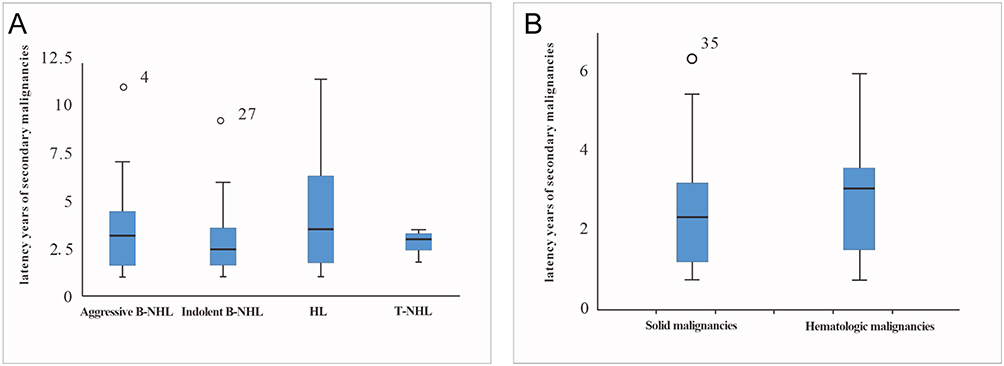 |
Figure 4 Latency periods stratified by (A) lymphoma subtype and (B) secondary primary malignancies type. Abbreviations: HL, Hodgkin lymphoma; NHL, non-Hodgkin lymphoma. |
Survival Analysis
Among the entire cohort, the 5-year OS rate was 89.6% (Figure 5A). Among patients who developed SPMs, the median OS was 11.2 years and the 5-year OS rate was 69.6% (Figure 5B). The 10 patients with synchronous SPMs had a 5-year OS rate of 60.0% (Figure 5C). Patients with SPMs had significantly inferior survival compared with lymphoma patients without SPMs (median OS in the SPM group, 10.3 years; log-rank  <0.0001; Figure 5D). Among SPM patients, solid malignancies showed a numerically longer median OS than hematologic malignancies (12.8 vs 6.0 years), but this difference was not statistically significant (
<0.0001; Figure 5D). Among SPM patients, solid malignancies showed a numerically longer median OS than hematologic malignancies (12.8 vs 6.0 years), but this difference was not statistically significant ( =0.76; Figure 5E). Survival differed significantly across lymphoma subtypes among patients with SPMs (
=0.76; Figure 5E). Survival differed significantly across lymphoma subtypes among patients with SPMs ( =0.037; Figure 5F): the median OS was 12.75 years for aggressive B-cell NHL, 10.17 years for indolent B-cell NHL, 10.75 years for HL, and 3.92 years for T-cell lymphoma. In the competing-risk analysis accounting for death before SPM development as a competing event, 55 metachronous SPMs, 184 competing events (death before SPM), and 1,476 censored observations were observed among the 1,715 lymphoma patients. The cumulative incidence of SPMs was higher in patients exposed to BTK inhibitors than in those without BTK inhibitor exposure. The 5-year CIF was 7.92% in the BTK inhibitor group and 2.57% in the non-BTK inhibitor group. The 10-year CIF was 7.92% and 2.85%, respectively, and the 12-year CIF was 7.92% and 3.42%, respectively. Gray’s test showed a statistically significant difference between the two groups (P = 0.007) (Table S1).
=0.037; Figure 5F): the median OS was 12.75 years for aggressive B-cell NHL, 10.17 years for indolent B-cell NHL, 10.75 years for HL, and 3.92 years for T-cell lymphoma. In the competing-risk analysis accounting for death before SPM development as a competing event, 55 metachronous SPMs, 184 competing events (death before SPM), and 1,476 censored observations were observed among the 1,715 lymphoma patients. The cumulative incidence of SPMs was higher in patients exposed to BTK inhibitors than in those without BTK inhibitor exposure. The 5-year CIF was 7.92% in the BTK inhibitor group and 2.57% in the non-BTK inhibitor group. The 10-year CIF was 7.92% and 2.85%, respectively, and the 12-year CIF was 7.92% and 3.42%, respectively. Gray’s test showed a statistically significant difference between the two groups (P = 0.007) (Table S1).
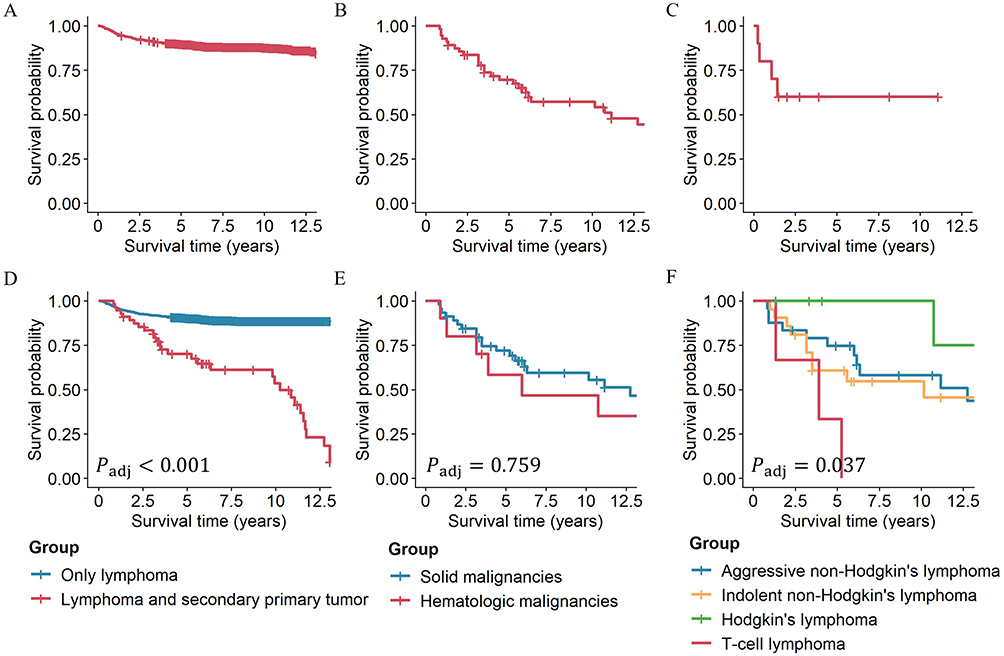 |
Figure 5 Survival analysis for lymphoma patients developing SPMs. (A). Survival analysis for the entire cohort. (B). Survival analysis for metachronous SPMs. (C). Survival analysis for synchronous SPMs. (D). Survival analysis stratified by SPM status (SPM vs non-SPM). (E). Survival analysis stratified by SPM type (solid vs hematologic). (F). Survival analysis by lymphoma subtype in SPM patients. |
Discussion
This study furnishes critical insights into the incidence, risk factors, and survival outcomes of SPMs in Chinese lymphoma patients treated with contemporary therapies, including chemotherapy, radiotherapy and targeted therapy. Our findings both corroborate and expand upon prior reports concerning SPMs epidemiology within Western cohorts, while underscoring unique population-specific patterns necessitating tailored survivorship strategies.19–21 Furthermore, when considered in conjunction with emerging research highlighting the influence of primary nodal site on SPM risk in NHL patients, our data contribute to a more nuanced understanding of the complex landscape of SPM development post-lymphoma.
The cumulative incidence of SPMs in our cohort (3.2%) was lower than the 9.2% reported in the SEER-based study by Rock et al21 This discrepancy likely reflects population-specific differences, evolution of treatment paradigms, and our longer median follow-up (8.26 vs 5.83 years) may paradoxically reflect higher competing mortality from lymphoma or other causes, as formalized in our competing-risk analysis. An elevated SPM risk associated with BTK inhibitors was observed, although the underlying mechanisms remain hypothetical.6,22,23 Similarly, radiotherapy was associated with an increased risk, consistent with established carcinogenic effects of ionizing radiation,24–26 although our cohort exhibited a predominance of gastrointestinal and respiratory malignancies, contrasting with the bladder cancer predominance reported in long-term SEER analyses.21,27 It’s important to note, as highlighted by studies focusing on NHL primary nodal sites, that radiotherapy to specific areas, such as the head and neck region, has been linked to increased risks of thyroid and other cancers, suggesting a localized impact of treatment modalities.24,28,29
The pronounced male predominance (male-to-female ratio: 2.9:1) and association with extranodal disease (HR=2.84) observed in our cohort have not been emphasized in prior studies, and may reflect ethnic variations in genetic susceptibility (eg TP53 R72P polymorphism prevalence in Asians) or lifestyle factors (eg smoking rates)30,31 Conversely, the reduced bladder cancer risk in our cohort compared to Western data potentially stems from differential screening practices or genetic modifiers.32,33 This contrasts with findings in NHL patients categorized by primary nodal site, where site-specific risks are more prominently featured rather than broad demographic factors like sex.
A notable finding was the identification of male sex, ECOG performance status ≥2, extranodal involvement, bone marrow infiltration, radiotherapy, and BTK inhibitor exposure as independent risk factors for SPMs. The association between BTK inhibitor exposure and increased SPM risk remained significant in multivariable Cox regression, with the proportional hazards assumption confirmed. Competing-risk analysis further demonstrated a significantly higher cumulative incidence of SPMs among patients receiving BTK inhibitors, consistent with prior evidence that chronic B-cell receptor inhibition may impair immune surveillance and promote clonal evolution.6,22,23 However, this finding should be interpreted cautiously. In China, BTK inhibitors were introduced later and incorporated into national medical insurance coverage only in 2018, resulting in predominant use in later-line or salvage settings; consequently, patients receiving BTK inhibitors may have had more advanced disease, heavier prior treatment exposure, and closer clinical monitoring, potentially introducing residual confounding. The association between radiotherapy and SPMs aligns with established carcinogenic effects of ionizing radiation.24–29 These readily available variables may serve as practical indicators for preliminary SPM risk stratification.
Patients with high-risk features—particularly those with prior radiotherapy exposure or receiving continuous BTK inhibitor therapy—may benefit from intensified long-term monitoring, including symptom-guided assessment, age-appropriate gastrointestinal cancer screening, and low-dose chest CT in selected high-risk individuals.16,30,34 In the future, integrating molecular biomarkers such as clonal hematopoiesis of indeterminate potential (CHIP) into predictive models may further refine risk stratification and optimize survivorship management.35–37
We found in this study that: survival analysis of SPMs across lymphoma subtypes revealed a paradoxical prognostic pattern: patients with aggressive B-cell lymphomas (eg, DLBCL) who developed SPMs exhibited superior OS compared to those with indolent B-cell lymphomas (eg, follicular lymphoma), contrasting with the established prognosis of de novo lymphomas (where aggressive subtypes typically confer poorer survival).38,39 This counterintuitive observation may be attributed to two interrelated mechanisms: 1. Divergent disease trajectories: Aggressive B-cell lymphoma patients demonstrated significantly prolonged latency periods before SPM development,40,41 with 75% achieving sustained complete remission of their primary lymphoma at SPM diagnosis. Consequently, their OS was predominantly influenced by SPM progression rather than lymphoma activity. 2. Dual disease burden: In contrast, 61.9% indolent B-cell lymphoma patients maintained stable disease or partial remission of their primary lymphoma at SPM onset, resulting in compounded mortality risks from both persistent lymphoma and secondary malignancy. These findings underscore the critical interplay between lymphoma biology, treatment-induced remission status, and SPM-related survival outcomes, challenging conventional prognostic paradigms based solely on primary tumor aggressiveness. In addition, among SPM patients, those with solid malignancies had a numerically longer median survival than those with hematologic malignancies (12.8 vs 6.0 years), although the difference did not reach statistical significance (log-rank P=0.76), This apparently paradoxical finding primarily reflects imbalance in group sizes, which substantially limited statistical power. Nevertheless, the 6.8 year absolute survival gap carries clear clinical relevance, suggesting that hematologic SPMs may represent a prognostically inferior subtype—consistent with the recognized aggressive biology and short survival of therapy-related myeloid neoplasms. Accordingly, this descriptive observation is awaiting validation in larger, adequately powered cohorts.
This study has several limitations. First, its retrospective, single-center design may introduce selection bias and limit generalizability. Although proportional hazards assumptions were assessed and competing-risk analysis was performed to improve methodological robustness, the total number of SPM events remained limited, particularly among BTK inhibitor–exposed patients (n = 9), potentially reducing statistical power and increasing uncertainty in effect estimation. Second, several important confounders—including smoking status, alcohol consumption, environmental exposure, genetic susceptibility, and molecular markers such as CHIP—were not fully captured.35–37 Third, as patients with more advanced lymphoma or those receiving targeted therapies may undergo more frequent follow‑up imaging, potentially leading to earlier detection of SPMs. This surveillance bias may have artificially inflated the observed cumulative incidence in the BTK inhibitor group. Finally, although the median follow-up duration of 8.26 years allowed evaluation of early and intermediate SPM events, it may still underestimate the incidence of late-onset solid tumors with longer latency periods. Therefore, larger multicenter prospective studies involving more diverse populations, longer follow-up, and more detailed treatment and molecular data are warranted to validate the present findings.
In conclusion, this exploratory study systematically evaluated the incidence, risk factors, and survival impact of SPMs among Chinese lymphoma patients in the era of modern targeted therapy. SPMs were associated with inferior survival, with gastrointestinal and respiratory malignancies representing the predominant secondary tumor types. Radiotherapy and BTK inhibitor exposure, together with several baseline clinicopathological features, may help identify patients requiring intensified surveillance. These findings support a transition toward precision, risk-adapted survivorship care in lymphoma patients.
Data Confidentiality
All patient data were de-identified prior to analysis to ensure confidentiality. Access to raw data was restricted to authorized researchers, and all analyses were performed on encrypted servers compliant with the General Data Protection Regulation (GDPR) and Chinese Data Security Law.
Abbreviations
BTK, Bruton’s Tyrosine Kinase; SPMs, Secondary primary malignancies; ECOG, Eastern Cooperative Oncology Group; NHL, Non-Hodgkin lymphoma; HL, Hodgkin lymphoma; PFS, Progression-free survival; OS, Overall survival; SIRs, Standardized incidence ratios; IPI, International Prognostic Index; LDH, lactate dehydrogenase; β2-MG, β2-microglobulin; DLBCL, Diffuse large B-cell lymphoma; MCL, Mantle cell lymphoma; AML, Acute myeloid leukemia; ALL, Acute lymphoblastic leukemia; CML, Chronic myeloid leukemia; MM, Multiple myeloma; B-NHL, B-cell non-Hodgkin lymphoma; T-NHL, T-cell non-Hodgkin lymphoma; SEER, Surveillance, Epidemiology, and End Results; CHIP, Clonal hematopoiesis of indeterminate potential.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding authors upon request.
Ethical Approval
The need for individual informed consent was waived by the IRB due to the retrospective nature of the study and the use of anonymized patient data extracted from electronic medical records.
Informed Consent
For prospective follow-up components (e.g., telephone interviews), verbal consent was obtained from participants, documented in the hospital’s electronic record system, and approved by the IRB. Patients retained the right to withdraw from follow-up at any time without affecting their clinical care.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the National Natural Science Foundation of China (No. 82300227 to Dr. Tingting Zhang) and Fundamental Research Program of Shanxi Province (No.202203021221246 to Dr. Dong Song, No. 202203021212089 to Dr. Xuejing Yang, and No. 202303021222318 to Dr. Tingting Zhang), Research and Innovation Team Project for Scientific Breakthroughs at Shanxi Bethune Hospital (2024AOXIANG04 to Dr. Tingting Zhang) and Talents Induction Program of Shanxi Bethune Hospital (No. 2023RC08 to Dr. Tingting Zhang).
Disclosure
All authors declare no competing interests in this work.
References
1. Huang J, Chan SC, Lok V, et al. Global burden, risk factors, and trends of non-Hodgkin lymphoma: a worldwide analysis of cancer registries. Cancer Med. 2024;13(5):e7056. doi:10.1002/cam4.7056
2. Liu W, Liu J, Song Y, et al. Burden of lymphoma in China, 2006-2016: an analysis of the global burden of disease study 2016. J Hematol Oncol. 2019;12(1):115. doi:10.1186/s13045-019-0785-7
3. Zhan Z, Guo W, Wan X, Bai O. Second primary malignancies in non-Hodgkin lymphoma: epidemiology and risk factors. Ann Hematol. 2023;102(2):249–16. doi:10.1007/s00277-023-05095-8
4. Miller KD, Nogueira L, Devasia T, et al. Cancer treatment and survivorship statistics, 2022. CA Cancer J Clin. 2022;72(5):409–436. doi:10.3322/caac.21731
5. Luo J, Craver A, Bahl K, et al. Etiology of non-Hodgkin lymphoma: a review from epidemiologic studies. J Natl Cancer Cent. 2022;2(4):226–234. doi:10.1016/j.jncc.2022.08.003
6. Bond DA, Huang Y, Fisher JL, et al. Second cancer incidence in CLL patients receiving BTK inhibitors. Leukemia. 2020;34(12):3197–3205. doi:10.1038/s41375-020-0987-6
7. Pichler AS, Amador C, Fujimoto A, et al. Advances in peripheral T cell lymphomas: pathogenesis, genetic landscapes and emerging therapeutic targets. Histopathology. 2025;86(1):119–133. doi:10.1111/his.15376
8. Duell J, Westin J. The future of immunotherapy for diffuse large B-cell lymphoma. Int, J, Cancer. 2025;156(2):251–261. doi:10.1002/ijc.35156
9. Dostálová H, Kryštof V. Strategies for overcoming resistance to Bruton’s tyrosine kinase inhibitor zanubrutinib. Hematol Oncol. 2024;42(4):e3294. doi:10.1002/hon.3294
10. Davoodi-Moghaddam Z, Jafari-Raddani F, Noori M, Bashash D. A systematic review and meta-analysis of immune checkpoint therapy in relapsed or refractory non-Hodgkin lymphoma; a friend or foe. Transl Oncol. 2023;30:101636. doi:10.1016/j.tranon.2023.101636
11. Tward JD, Wendland MM, Shrieve DC, et al. The risk of secondary malignancies over 30 years after the treatment of non-Hodgkin lymphoma. Cancer. 2006;107(1):108–115. doi:10.1002/cncr.21971
12. Donin N, Filson C, Drakaki A, et al. Risk of second primary malignancies among cancer survivors in the United States, 1992 through 2008. Cancer. 2016;122(19):3075–3086. doi:10.1002/cncr.30164
13. Major A, Smith DE, Ghosh D, et al. Risk and subtypes of secondary primary malignancies in diffuse large B-cell lymphoma survivors change over time based on stage at diagnosis. Cancer. 2020;126(1):189–201. doi:10.1002/cncr.32513
14. Sung H, Siegel RL, Hyun N, et al. Subsequent primary cancer risk among 5-year survivors of adolescent and young adult cancers. J Natl Cancer Inst. 2022;114(7):1095–1108. doi:10.1093/jnci/djab013
15. Joelsson J, Wästerlid T, Rosenquist R, et al. Incidence and time trends of second primary malignancies after non-Hodgkin lymphoma: a Swedish population-based study. Blood Adv. 2022;6(9):2657–2666. doi:10.1182/bloodadvances.2021005936
16. Moser O, Zimmermann M, Meyer U, et al. Second malignancies after treatment of childhood non-Hodgkin lymphoma: a report of the Berlin-Frankfurt-Muenster study group. Haematologica. 2021;106(5):1390–1400. doi:10.3324/haematol.2020.266023
17. Jégu J, Colonna M, Daubisse-Marliac L, et al. The effect of patient characteristics on second primary cancer risk in France. BMC Cancer. 2014;14:94. doi:10.1186/1471-2407-14-94
18. Lorenzo Bermejo J, Pukkala E, Johannesen TB, et al. Age-time risk patterns of solid cancers in 60 901 non- H odgkin lymphoma survivors from F inland, N orway and S weden. Br J Haematol. 2014;164(5):675–683. doi:10.1111/bjh.12693
19. Wood ME, Vogel V, Ng A, et al. Second malignant neoplasms: assessment and strategies for risk reduction. J Clin Oncol. 2012;30(30):3734–3745. doi:10.1200/JCO.2012.41.8681
20. Haque W, Dabaja B, Tann A, et al. Changes in treatment patterns and impact of radiotherapy for early stage diffuse large B cell lymphoma after rituximab: a population-based analysis. Radiother Oncol. 2016;120(1):150–155. doi:10.1016/j.radonc.2016.05.027
21. Rock CB, Chipman JJ, Parsons MW, et al. Second primary malignancies in diffuse large b-cell lymphoma survivors with 40 years of follow up: influence of chemotherapy and radiation therapy. Adv Radiat Oncol. 2022;7(6):101035. doi:10.1016/j.adro.2022.101035
22. Morton LM, Curtis RE, Linet MS, et al. Second malignancy risks after non-Hodgkin’s lymphoma and chronic lymphocytic leukemia: differences by lymphoma subtype. J Clin Oncol. 2010;28(31):4935–4944. doi:10.1200/JCO.2010.29.1112
23. Wu J, Liu Y, Qin Y, et al. Secondary primary malignancies in chinese chronic lymphocytic leukemia patients treated with btk inhibitors. Front Oncol. 2022;12:876543. doi:10.3389/fonc.2022.876543
24. Dracham CB, Shankar A, Madan R. Radiation induced secondary malignancies: a review article. Radiat Oncol J. 2018;36(2):85–94. doi:10.3857/roj.2018.00153
25. Tao L, Clarke CA, Rosenberg AS, et al. Subsequent primary malignancies after diffuse large B-cell lymphoma in the modern treatment era. Br J Haematol. 2017;178(1):72–80. doi:10.1111/bjh.14638
26. Lowry L, Smith P, Qian W, et al. Reduced dose radiotherapy for local control in non-Hodgkin lymphoma: a randomised Phase III trial. Radiother Oncol. 2011;100:86–92. doi:10.1016/j.radonc.2011.05.013
27. Jiang S, Zhen H, Jiang H. Second primary malignancy in diffuse large B-cell lymphoma patients: a SEER database analysis. Curr Probl Cancer. 2020;44:100502. doi:10.1016/j.currproblcancer.2019.100502
28. Cho SF, Wu WH, Yang YH, Chang CS. Risk of second primary cancer in patients with B-cell non-Hodgkin lymphoma receiving rituximab-containing chemotherapy: a nationwide population-based study. Anticancer Res. 2015;35:1809–1814.
29. Pirani M, Marcheselli R, Marcheselli L, Bari A, Federico M, Sacchi S. Risk for second malignancies in non-Hodgkin’s lymphoma survivors: a meta-analysis. Ann Oncol. 2011;22:1845–1858. doi:10.1093/annonc/mdq697
30. Chattopadhyay S, Zheng G, Sud A, et al. Second primary cancers in non-Hodgkin lymphoma: family history and survival. Int, J, Cancer. 2020;146:970–976. doi:10.1002/ijc.32391
31. Lu C, Xie M, Wendl MC, et al. Patterns and functional implications of rare germline variants across 12 cancer types. Nat Commun. 2015;6:10086. doi:10.1038/ncomms10086
32. Travis LB, Curtis RE, Glimelius B, et al. Bladder and kidney cancer following cyclophosphamide therapy for non-Hodgkin’s lymphoma. J Natl Cancer Inst. 1995;87:524–530. doi:10.1093/jnci/87.7.524
33. Chou WH, McGregor B, Schmidt A, et al. Cyclophosphamide-associated bladder cancers and considerations for survivorship care: a systematic review. Urol Oncol. 2021;39:678–685. doi:10.1016/j.urolonc.2021.05.017
34. Smith A, Howell D, Patmore R, et al. Incidence of haematological malignancy by sub-type: a report from the Haematological Malignancy Research Network. Br J Cancer. 2011;105:1684–1692. doi:10.1038/bjc.2011.450
35. Klener P. Advances in molecular biology and targeted therapy of mantle cell lymphoma. Int J Mol Sci. 2019;20:4417. doi:10.3390/ijms20184417
36. Higgins A, Shah MV. Genetic and genomic landscape of secondary and therapy-related acute myeloid leukemia. Genes. 2020;11:749. doi:10.3390/genes11070749
37. Gibson CJ, Lindsley RC, Tchekmedyian V, et al. Clonal hematopoiesis associated with adverse outcomes after autologous stem-cell transplantation for lymphoma. J Clin Oncol. 2017;35:1598–1605. doi:10.1200/JCO.2016.71.6712
38. Liu W, Ji X, Song Y. Song Y et al Improving survival of 3760 patients with lymphoma: experience of an academic center over two decades. Cancer Med. 2020;9:3765–3774. doi:10.1002/cam4.3037
39. Sacchi S, Marcheselli L, Bari A, et al. Secondary malignancies after treatment for indolent non-Hodgkin’s lymphoma: a 16-year follow-up study. Haematologica. 2008;93:398–404. doi:10.3324/haematol.12120
40. Li M, Dave N, Salem AH, Freise KJ. Model-based meta-analysis of progression-free survival in non-Hodgkin lymphoma patients. Medicine. 2017;96:e7988. doi:10.1097/MD.0000000000007988
41. Milrod CJ, Kim KW, Raker C, Ollila TA, Olszewski AJ, Pelcovits A. Progression-free survival is a weakly predictive surrogate end-point for overall survival in follicular lymphoma: a systematic review. Br J Haematol. 2024;204:2237–2241. doi:10.1111/bjh.19449
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of Causes and Risk Factors for Deaths Among Pediatric Oncology Patients: A 20-Year Observation
Mitura-Lesiuk M, Dubaj M, Drabko K, Zawitkowska J
Cancer Management and Research 2026, 18:604728
Published Date: 5 May 2026