Back to Journals » Psychology Research and Behavior Management » Volume 19
Revisiting the Proximal Dominance Assumption: Community Social Inclusion in an Ecological Analysis of Finnish Adolescent Mental Health
Authors Zhou J ![]() , Liu Y
, Liu Y ![]() , Liao C
, Liao C ![]() , Toikko T
, Toikko T ![]()
Received 24 December 2025
Accepted for publication 30 April 2026
Published 15 June 2026 Volume 2026:19 591431
DOI https://doi.org/10.2147/PRBM.S591431
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhenhao Shi
Jing Zhou,1,2 Yongqin Liu,1 Chensi Liao,3 Timo Toikko2
1School of Law, Shanghai Lixin University of Accounting and Finance, Shanghai, 201209, People’s Republic of China; 2Department of Social Sciences, University of Eastern Finland, Kuopio, 70211, Finland; 3School of Social Development and Public Policy, Fudan University, Shanghai, 200433, People’s Republic of China
Correspondence: Yongqin Liu, Email [email protected] Timo Toikko, Email [email protected]
Background and Purpose: Adolescent mental health is shaped by multiple ecological contexts. However, ecological research has often assumed that proximal microsystems show stronger associations with mental health than broader environments. This proximal dominance assumption has rarely been tested within comprehensive models comparing multiple domains across different outcomes. This study assessed whether perceived community social inclusion shows associations with mental health beyond more proximal factors in a large Finnish sample.
Methods: Data from the 2019 Finnish School Health Promotion Study were analyzed. Blockwise OLS regression models estimated incremental associations of five analytic domains (demographic background, individual, family, school and peer, and perceived community social inclusion) with depressive symptoms, anxiety symptoms, loneliness, and life satisfaction. Exploratory moderation analyses tested whether community social inclusion, school belonging, and parent-child relationship buffered associations between cognitive difficulties and outcomes.
Results: Final analytic sample comprised 69,800 adolescents (mean age 15.54 years, 47.0% boys). Final models explained 41.3– 51.9% of variance. Cognitive difficulties showed the strongest associations with depression (β = 0.292) and anxiety (β = 0.375). Perceived community social inclusion showed the largest standardized association with life satisfaction (β = 0.446) and the largest negative association with depression (β = − 0.331), after adjustment for all other domains. Loneliness displayed unique sensitivity to school and peer factors. Moderation results indicated limited cross-level buffering, suggesting predominantly additive patterns.
Conclusion: The findings challenge the proximal dominance assumption. Perceived community social inclusion showed substantial associations with key outcomes after full adjustment. Different mental health outcomes display distinct ecological profiles, consistent with the proposed Asymmetric Ecological Model, in which domain salience varies across outcomes rather than a uniform proximity hierarchy. The predominantly additive pattern suggests promotive pathways rather than buffering pathways. Approaches strengthening social inclusion may complement individual and family interventions, though the cross-sectional design precludes causal inference.
Keywords: depression, anxiety, loneliness, life satisfaction, social inclusion, ecological systems
Introduction
Adolescent mental health has become a major public health priority worldwide, with upward trends in internalizing symptoms documented across multiple countries and cohorts.1–4 A recent community-based study shows 15.5% prevalence of any mental disorder among European youth aged 5–18 years.5 HBSC studies indicate increases in psychological complaints and declines in life satisfaction among adolescents, with persistent gender disparities.6,7 Pandemic-era evidence exhibits further increases in depression and anxiety, especially among girls and socioeconomically disadvantaged youth.8–10 These problems impair social and educational functioning and forecast lower adult wellbeing and economic productivity,11 underscoring the need to identify modifiable determinants.
Understanding adolescent mental health requires moving beyond individual-level risk factors to consider broader environmental contexts.12 Although ecological frameworks emphasize development within nested, interacting systems,13 systematic reviews indicate that studies typically examine one or two ecological levels, with comprehensive multilevel investigations remaining rare.14 This limits our ability to determine the relative importance of different contexts and whether more distal factors remain influential when proximal influences are controlled. This question may be especially salient in mid-adolescence, when young people become increasingly oriented toward broader social recognition, participation, and belonging beyond the family and classroom.15,16
Ecological Systems Framework and the Proximal Dominance Assumption
Bronfenbrenner’s ecological systems theory proposes that adolescent mental health is shaped by multiple, nested contexts, including individual characteristics, family relationships, peer and school environments, and broader community conditions.12,13,17 Rather than isolating a single setting, this perspective emphasizes that development is embedded in interdependent layers of influence, with each level capable of contributing independently and interactively to adolescent outcomes.18 However, ecological research has often carried an implicit assumption that contexts closer to adolescents’ everyday lives, especially family and school microsystems, are likely to show stronger associations with mental health than broader contextual environments beyond the immediate microsystem.13 Although this assumption is broadly consistent with the emphasis on proximal processes in developmental theory, it has rarely been tested directly within comprehensive models that compare multiple ecological levels simultaneously across different mental health outcomes.14,19,20 We refer to this here as the proximal dominance assumption. It is not a formal proposition in Bronfenbrenner’s original work, but rather a recurrent and largely unexamined tendency in how ecological research has been designed and interpreted.
At the individual level, cognitive difficulties and excessive internet use (EIU) have been identified as risk factors. Recent studies illustrate substantial associations between cognitive challenges and internalizing symptoms,21,22 while meta-analyses link problematic internet use to depression and anxiety,23 though effect sizes are modest and causal directions remain debated.24,25
At the family level, socioeconomic status (SES) is consistently correlated with adolescent internalizing problems and lower well-being. Meta-analytic reviews converge on roughly 1.5 to 2 times higher risk of depression and anxiety among youth from lower-SES families,26,27 with gradients varying cross-nationally and tending to be larger where income inequality is higher,6,28 even in Nordic welfare states.29 A recent systematic review finds that adolescent-rated parent-child communication associates with lower depression and anxiety.30 Danish HBSC analyses further show that adolescents who find it very difficult to talk with parents have markedly higher odds of loneliness,31 and better communication correlates with higher life satisfaction.32
At the school and peer level, school climate and peer relationships are important microsystems. Higher school belonging or connectedness prospectively predicts lower depression and anxiety,33 with cohort evidence indicating these benefits persist into young adulthood.34,35 High-quality close friendships are likewise protective, with systematic evidence associating better friendship quality with fewer internalizing symptoms, lower loneliness and higher well-being.36 Conversely, peer victimization remains a robust risk factor.37 Research also indicates that negative affect during recess often coincides with feelings of social exclusion or victimization,38,39 representing a distinct dimension of school social climate.
Beyond immediate interpersonal settings, broader community environments may also matter for adolescent mental health. In the present study, community social inclusion refers not to objective structural characteristics of neighborhoods or municipalities, but to adolescents’ subjective experiences of being valued, accepted, and able to participate in community life.40,41 This distinction is theoretically important: perceived inclusion captures how wider social environments are encountered and interpreted in everyday experience,40 and may therefore represent a psychologically meaningful pathway through which broader contexts become relevant for mental health, not fully reducible to material circumstances.42,43 Previous studies suggest that such perceptions are associated with fewer psychological complaints44–46 and greater life satisfaction,6 even after accounting for individual and family characteristics.6,47 Yet it remains unclear whether perceived social inclusion retains an independent association with mental health when individual, family, and school factors are all considered within the same ecological model, and whether it moderates individual-level vulnerabilities.
Five considerations motivate the present study. First, few studies systematically quantify the relative contribution of each ecological level within a single comprehensive model.14 Most research examines one or two levels in isolation, preventing assessment of whether distal factors remain important when proximal influences are controlled. Second, research on perceived community social inclusion as a determinant remains limited, particularly in models controlling comprehensively for other ecological levels.12,14 Third, potential cross-level buffering effects remain largely untested in large-scale studies.20,48 Fourth, most research examines single mental health outcomes, yet different indicators may show distinct ecological patterns that inform more targeted intervention. Fifth, most ecological research comes from Anglo-American contexts. Finland represents an analytically informative setting: universal welfare supports and well-resourced school and youth services may reduce some material inequalities,28,29 yet perceived social inclusion may remain a distinctive psychological pathway to mental health not fully accounted for by socioeconomic conditions.
Clarifying these issues matters for at least four reasons. Theoretically, if more distal experiences such as perceived community inclusion remain substantially associated with adolescent mental health after proximal contexts are considered, this would suggest that ecological influence cannot be inferred from contextual proximity alone and would motivate refinement of how ecological hierarchy is conceptualized. Methodologically, it would underscore the limitations of studies that examine only one or two settings in isolation. Developmentally, mid-adolescence may be a period in which broader social recognition becomes especially salient as young people expand their social worlds beyond family and classroom routines, making community belonging a potentially powerful correlate of psychological functioning.49 Contextually, Finland provides an analytically informative case because of its extensive welfare-state supports and school-based service infrastructure,50 which may alter the relative salience of different ecological contexts.
Present Study
Using a large, nationally representative sample of Finnish adolescents, the present study examines how factors across five analytic domains, including demographic background, individual attributes, family environment, school and peer context, and perceived community inclusion, are associated with four mental health outcomes: depressive symptoms, anxiety symptoms, loneliness, and life satisfaction. We pursue three aims. First, we compare the relative contribution of each analytic domain within the same framework to assess whether more distal factors remain associated with mental health after more proximal factors are considered. Second, we test whether perceived community social inclusion shows an independent association with mental health outcomes beyond individual, family, and school factors and, on an exploratory basis, whether it moderates the associations involving cognitive vulnerabilities. Third, we compare patterns across outcomes in order to identify whether different indicators of adolescent mental health show distinct ecological signatures. (See Supplementary Figure 1 for the conceptual framework).
Methods
Participants and Procedure
Data came from the 2019 wave of the Finnish School Health Promotion Study (SHPS), a biennial national survey conducted by the Finnish Institute for Health and Welfare (THL).51 Prior to data collection, the research protocol received ethical review from THL, which serves as the national authority responsible for the design, administration, and ethical governance of the SHPS. Participation was voluntary and responses were anonymous.52 For participants under 15 years of age, parental consent was obtained in accordance with Finnish national regulations governing school-based health surveys. Participants provided responses during school hours through a standardized electronic questionnaire under teacher supervision. The dataset analyzed in this study was obtained through the Finnish Social Science Data Archive (FSD), which administers data access in coordination with THL. Access to this pre-existing anonymized dataset was granted through a formal application procedure. Ethical approval and data protection considerations are described in the Declarations section.
The initial dataset comprised 87,215 students. The analytic sample was restricted to students in grades 8 and 9 with complete data on all study variables, yielding a final sample of 69,800 participants. No participants were excluded on the basis of pre-existing mental health conditions. The SHPS is a universal population-based survey, and the present study examines variation in mental health outcomes across the full community sample rather than a clinically screened population. This design choice is consistent with the study’s aim of identifying ecological correlates at the population level. Students were excluded solely due to missing data on one or more study variables (see Analytic strategy for details).
Measures
We used four mental health outcomes as continuous indicators.
Depressive symptoms were measured with the six-item Beck Depression Inventory (BDI-6), a brief index yielding a summed score from 0–18, with higher scores indicating more severe depressive symptoms.53,54 The Cronbach’s α is 0.887.
Anxiety symptoms were assessed with the seven-item Generalized Anxiety Disorder scale (GAD-7), a validated self-report screener with scores from 0 to 21 and higher scores indicating greater anxiety symptoms.55,56 Prior validation demonstrated strong internal consistency and construct validity in adolescent populations.57,58 The Cronbach’s α is 0.917.
Loneliness was a single item measure asking, “Do you ever feel lonely?” Responses were scaled from 0 (never) to 4 (all the time), with higher scores reflecting greater perceived loneliness.
Life satisfaction was evaluated with a standard single item (“How satisfied are you with your life at the moment?”) rated on a 5-point scale. Higher scores indicated greater satisfaction.
Single-item measures of loneliness and life satisfaction have been widely used in large-scale research and are considered to have strong content validity,59,60 though they provide more limited construct coverage than multi-item instruments.
Predictors were organized into five analytic domains. Control variables were age (continuous) and gender (1=boy, 0=girl).
Individual-domain variables: Cognitive difficulties used items from the UNICEF Child Functioning Module, yielding a total score ranging from 0 to 18 (Cronbach’s α = 0.813), with higher scores indicating greater cognitive difficulties.61 EIU was measured with a five-item Likert scale assessing salience, withdrawal, tolerance, relapse, and conflict, with responses from 1 (never) to 4 (very often). The index was computed as the mean score (Cronbach’s α = 0.831) and has demonstrated good reliability and cross-national validity.62,63
Family-domain variables: Parent-child relationship was measured with a single item (“Can you talk about things that concern you with your parents?”), rated on a four-point Likert scale (hardly ever, occasionally, fairly often, often).64–66 Family financial situation was assessed with a single item rating their family’s economic circumstances on a 5-point scale (1 = very poor, 5 = very good), with higher scores indicating better financial situation. Both items function as brief surveillance indicators widely used in HBSC and related large-scale adolescent health surveys.17,64,67
School and peer-domain variables: School belonging was measured with two items assessing the sense of being an important member of the classroom and school community, rated on a five-point scale (0 = fully disagree to 4 = fully agree) with higher scores indicating stronger belonging.68 Recess experiences were assessed with three items rated on a five-point scale (fully agree to fully disagree): “I am frightened of recesses or of going to recess”, “I feel lonely at recesses”, and “I would like to have more organized program at recesses”. Items were reverse-scored and summed to a total score ranging from 0 to 12, with higher values indicating more positive recess experiences. Research has linked negative affect during recess to social exclusion and peer victimization,38 suggesting these items capture theoretically relevant aspects of the informal peer environment. Number of close friends was assessed by asking whether students have a close friend they can talk to confidentially, with responses ranging from no close friends (0) to several close friends (3).
Perceived community inclusion: Social inclusion was measured using the ten-item Experiences of Social Inclusion Scale (ESIS), assessing subjective experiences of social connectedness, belonging, and agency.40 Items were rated on a 5-point scale and linearly transformed to range from 0 to 100 following THL recommendation,40 with higher scores indicating greater perceived social inclusion (Cronbach’s α = 0.955). As noted above, ESIS scores reflect individual perceptions of community inclusion rather than objective neighborhood or structural characteristics.
Analytic Strategy
The complete-case analytic sample (N =69,800) represented 80.1% of the initial SHPS cohort (N = 87,215). Little’s MCAR test indicated that data were not missing completely at random, χ2(4421) = 9995.99, p < 0.001. To evaluate the practical consequences of listwise deletion, we compared participants with complete data against those excluded due to missing data across all study variables (Supplementary Tables 1–3). All standardized mean differences for continuous variables were below 0.10, indicating trivial magnitude. However, boys were overrepresented in the incomplete group (60.5% vs. 39.5%; φ = 0.11, p < 0.001). Gender was included as a covariate in all models, which helps account for this imbalance, although residual bias from differential missingness cannot be excluded. Alternative approaches such as multiple imputation or FIML may better accommodate non-MCAR conditions; however, given the trivial observed differences and the need for a consistent sample across models, complete-case analysis was retained.
We estimated blockwise Ordinary Least Squares (OLS) regression models for each outcome with five sequential analytic domains: demographic background, individual, family, school and peer, and perceived community inclusion. Variables within each domain were entered simultaneously using forced entry. This sequential entry strategy was designed to estimate the incremental explanatory contribution of each domain after accounting for prior domains. The ordering of domains reflects analytic convention informed by theoretical proximity to the individual rather than a claim about causal or developmental sequence.
We report R2, adjusted R2, domain-level ΔR2 and standardized coefficients (β) with 95% confidence intervals. Variance inflation factors indicated acceptable multicollinearity (all VIF<2.0). Residual plots, Q-Q plots, and Cook’s distance values (all < 1) were examined and confirmed no substantial violations of regression assumptions. Given the exceptionally large sample size, statistical significance alone is an insufficient criterion for substantive interpretation. We therefore prioritize the magnitude of standardized coefficients and incremental R2 values over p-values in interpreting findings.
To examine cross-level buffering, exploratory moderation analyses tested three theory-driven interactions: ESIS × cognitive difficulties, school belonging × cognitive difficulties, and Parent-child relationship × cognitive difficulties. These interactions were selected on theoretical grounds, with cognitive difficulties treated as the focal individual vulnerability and community inclusion, school belonging, and parent-child relationship representing protective factors from distinct analytic domains. Interactions involving EIU were not tested because the theoretical basis for EIU-specific buffering effects is less developed, and expanding the interaction set without clear rationale would increase Type I error risk. Each interaction term was added separately as a sixth step to the full model after grand-mean centering. False discovery rate (FDR) correction (Benjamini-Hochberg, q = 0.05) was applied across all tests (3 interactions × 4 outcomes = 12 tests). We interpreted interaction effects using both FDR-corrected significance and effect magnitude, with ΔR2 ≥ 0.010 adopted as the conservative threshold for substantive interpretation. This threshold was informed by evidence that interaction effects in behavioral research are typically small and often account for about 1% of incremental variance.69 Only interactions meeting both criteria are discussed in the main text; significant interactions below this threshold are reported in Supplementary Table 4.
Results
Sample Characteristics
The final analytic sample comprised 69,800 Finnish adolescents (47.0% boys) aged 13–19 years (M=15.54, SD=0.58). Table 1 presents descriptive statistics for all study variables. Mean scores indicated relatively low levels of depressive symptoms, anxiety, and loneliness, and relatively high life satisfaction in this community sample.
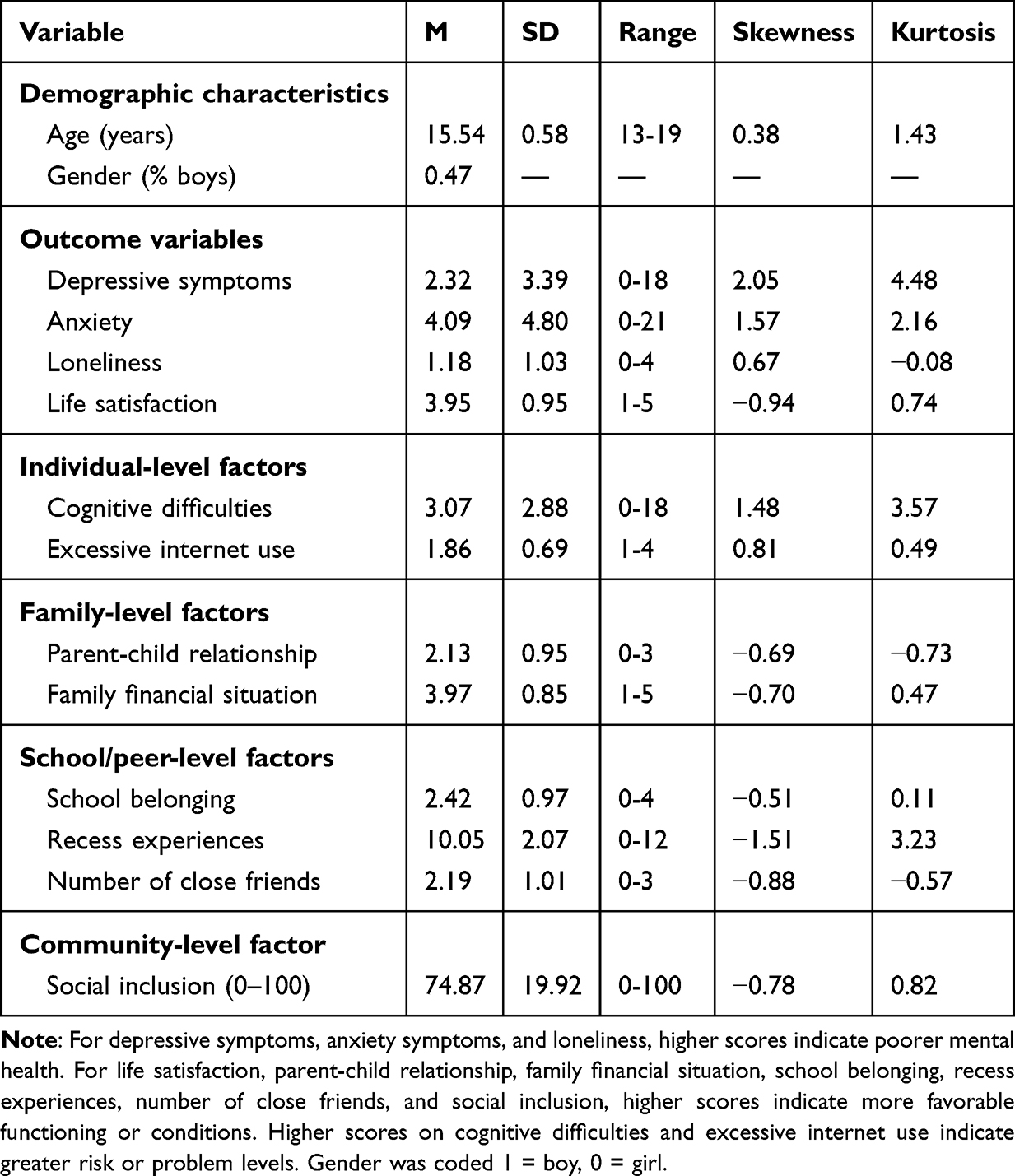 |
Table 1 Descriptive Statistics and Distributions of Study Variables |
Zero-order correlations (Supplementary Table 5) showed substantial intercorrelations among outcomes. Depression and anxiety demonstrated the strongest association (r = 0.72, p < 0.001). At the individual domain, cognitive difficulties showed the strongest correlations with all outcomes (r = 0.43 to 0.58). Perceived community social inclusion showed robust correlations with all four outcomes, with the strongest associations observed for life satisfaction (r = 0.67, p < 0.001) and depression (r = −0.61, p < 0.001).
Blockwise Regression Models
Blockwise regression results (Table 2) showed final models explained 41.3–51.9% of outcome variance across the four outcomes. Figure 1 shows the incremental variance (ΔR2) contributed by each analytic domain across outcomes.
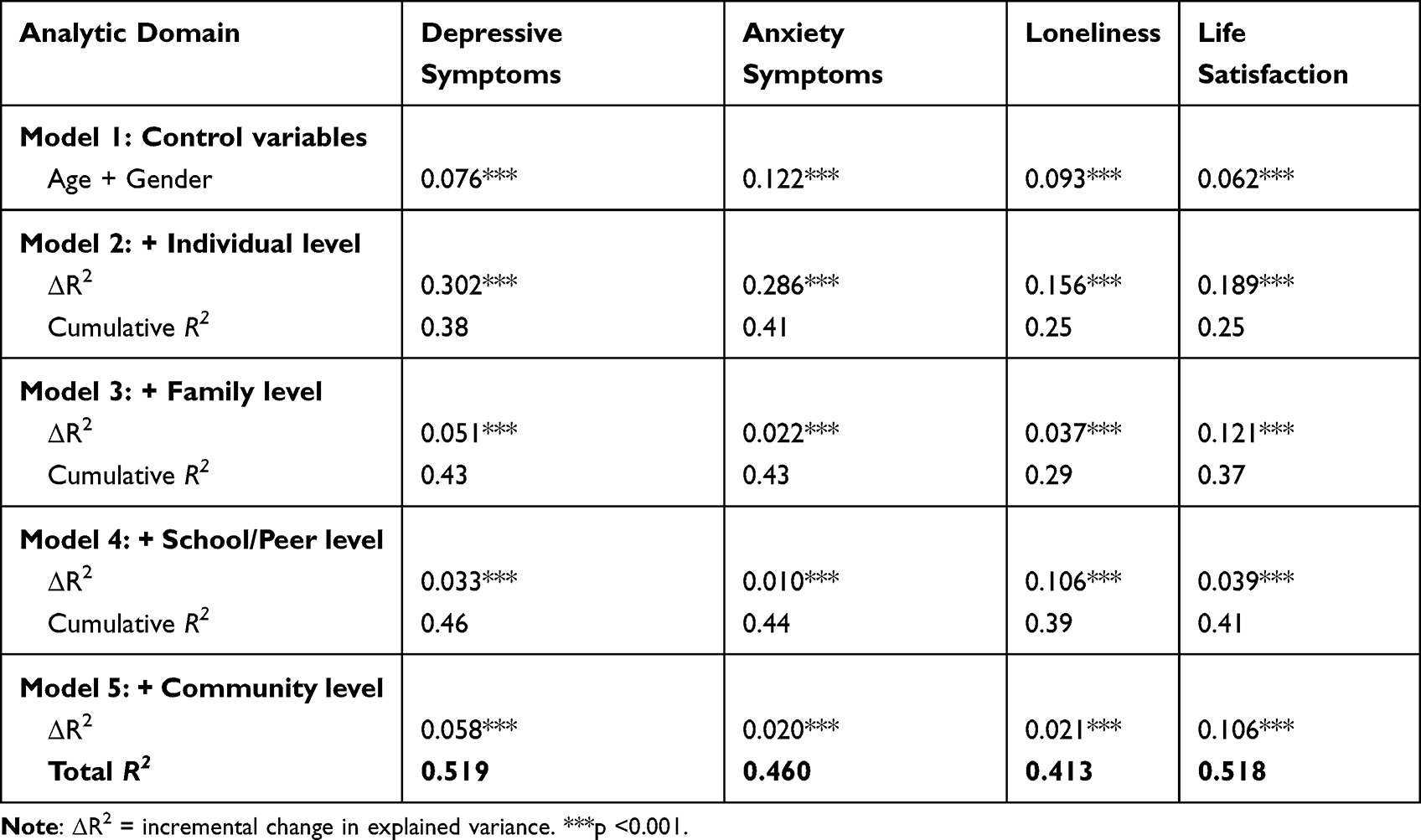 |
Table 2 Incremental Variance Explained by Analytic Domains in Blockwise OLS Regression Models |
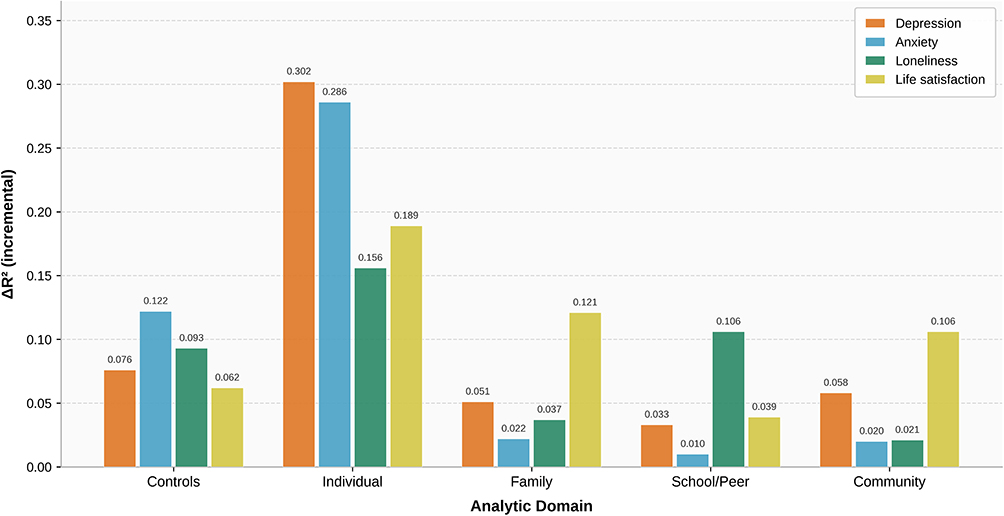 |
Figure 1 Incremental Variance Explained by Analytic Domains Across Four Mental Health Outcomes. Note: Bars represent domain-level change in explained variance (ΔR2) at each step of the blockwise OLS regression models. ΔR2 indicates the incremental variance explained by each domain after all previously entered domains were taken into account. Total explained variance for the final models is reported in Table 2. The sequential entry order reflects analytic convention and does not imply causal or developmental ordering. |
Three key patterns emerged from the blockwise analyses (See Figure 2 for standardized coefficients and Table 3 for full model details).
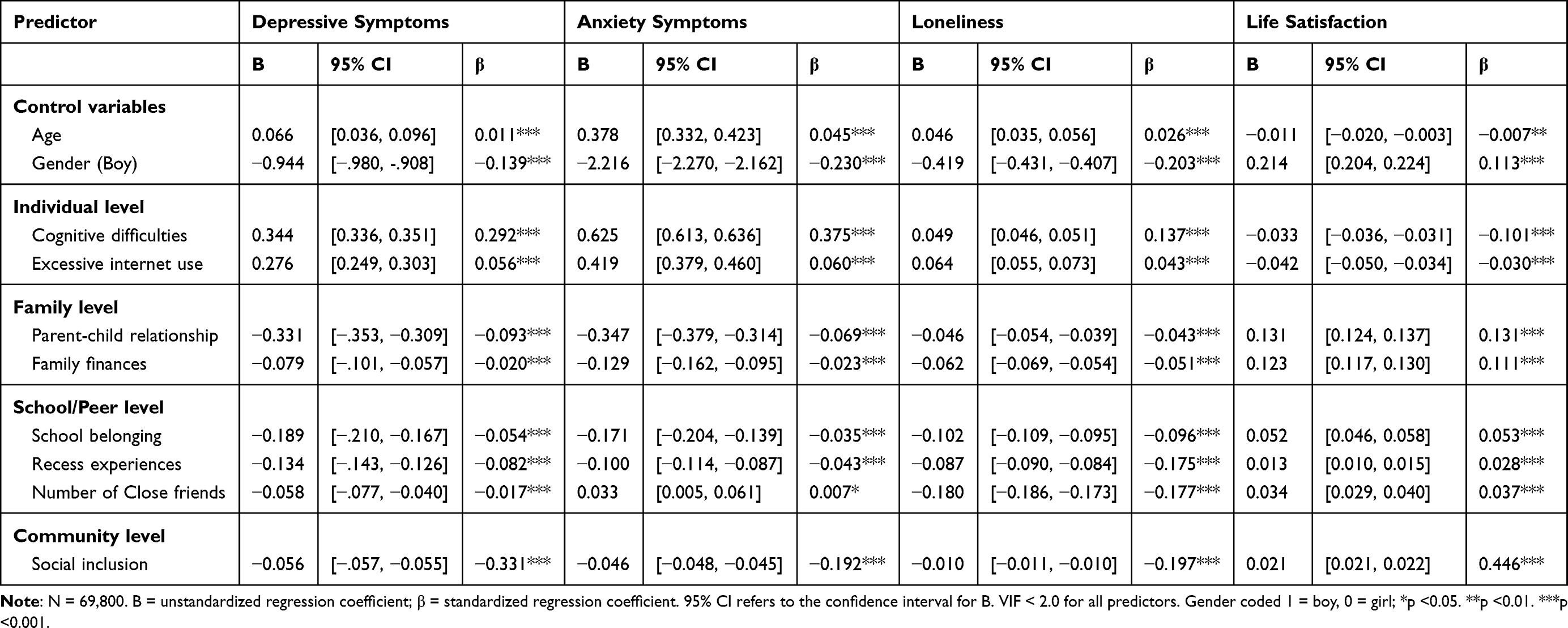 |
Table 3 Standardized Coefficients in Final Model 5 of Blockwise OLS Regression Predicting Adolescent Mental Health |
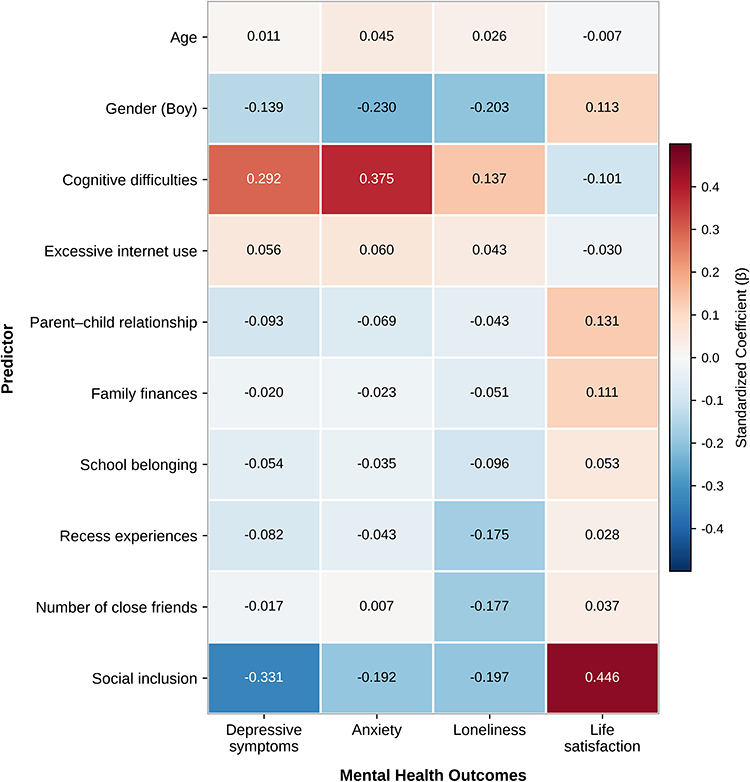 |
Figure 2 Standardized Coefficients (β) of Key Predictors Across Mental Health Outcomes. Note: Color intensity indicates effect strength; negative values (blue) indicate protective associations for depression, anxiety, and loneliness; positive values (red) indicate favorable associations for life satisfaction. All coefficients from full Model 5 (Table 3). |
First, individual domain contributed the largest incremental variance across all outcomes (ΔR2 = 0.156–0.302), though with marked variation. Cognitive difficulties demonstrated the strongest associations with anxiety (β = 0.375) and depression (β = 0.292), but substantially weaker relationships with loneliness (β = 0.137) and life satisfaction (β = −0.101). This fourfold difference in effect sizes indicates marked outcome-specific variation in cognitive associations.
Second, perceived community social inclusion showed substantial independent associations with several outcomes. Despite being entered last in the sequential domain structure, social inclusion showed the largest standardized association in the life satisfaction model (β = 0.446) and the largest standardized negative association among contextual predictors in the depression model (β = −0.331). The incremental variance explained by the community domain (ΔR2 = 0.020–0.106) was substantial for life satisfaction and depression, and was comparable to or larger than that of some earlier-entered domains. Third, loneliness displayed a unique pattern dominated by school and peer domain factors. School and peer variables contributed ΔR2 = 0.106 for loneliness, compared with ten times their contribution to anxiety (ΔR2 = 0.010). This specificity was particularly evident in the differential associations of close friendships (β = −0.177 for loneliness vs. β = −0.017 for depression) and recess experiences (β = −0.175 for loneliness vs. β = −0.043 for anxiety).
Gender showed consistent associations across outcomes, with boys reporting lower internalizing symptoms and loneliness but higher life satisfaction (all p < 0.001). Age associations were minimal. Family financial situation showed significant but modest associations with all outcomes.
Exploratory Cross-Level Moderation
Buffering effects were minimal across most tested interactions (Supplementary Table 4). No interactions met the conservative threshold for substantive interpretation (ΔR2 ≥ 0.010) except for depression. For this outcome, three interactions exceeded the threshold: ESIS × cognitive difficulties (ΔR2 =0.019), school belonging × cognitive difficulties (ΔR2 =0.014), and parent-child relationship × cognitive difficulties (ΔR2 =0.011). Even these effects were modest in magnitude. Overall, these findings provide limited evidence for cross-level buffering and are more consistent with additive main effects than with strong interaction effects.
Discussion
This large-scale study of Finnish adolescents examined associations between factors across five analytic domains and four mental health outcomes, providing a systematic empirical examination relevant to the proximal dominance assumption in ecological research. Three patterns warrant discussion: the substantial associations of perceived community social inclusion with key outcomes after adjustment for other analytic domains, the outcome-specific nature of ecological associations, and the limited evidence for cross-level buffering effects. Because the study is cross-sectional, all interpretations below should be read as describing patterns of association rather than established causal relationships.
Perceived Community Social Inclusion and Proximal Dominance Assumption
The findings align with a challenge to the proximal dominance assumption. Perceived community social inclusion showed the largest standardized association with life satisfaction and the largest standardized negative association among contextual predictors with depression, after controlling for individual, family, and school domain factors. These associations suggest that broader social environments, as experienced and perceived by adolescents, may carry substantial psychological significance above and beyond more proximal domains as measured in the present study.
This pattern aligns with recent Finnish evidence which identified perceived social inclusion as a significant predictor of Finnish adolescent wellbeing, though that study did not control for the comprehensive range of domains examined here.70 The larger associations observed in the present study relative to Oh and Thomas,47 who reported moderate neighborhood social cohesion effects on adolescent depression, may reflect differences in measurement scope. The ESIS captures not only social cohesion but also perceived agency and belonging across multiple community contexts, and may therefore index a broader dimension of community experience.40 It should be noted, however, that ESIS and several outcome measures share a self-report basis and conceptually adjacent content. The high zero-order correlations between ESIS and life satisfaction (r = 0.67) and depression (r = −0.61) raise the possibility that shared method variance contributes to the observed associations.
The differential pattern of associations across outcomes provides some basis for theoretical interpretation, while acknowledging that the cross-sectional design precludes causal inference. For depressive symptoms, the association between perceived community social inclusion and depression is consistent with the role of broader social validation in the context of cognitive models of depression71 and neurobiological evidence on adolescent social reward sensitivity.72 For anxiety, the comparatively weaker association with perceived community social inclusion corresponds with contemporary models distinguishing depression’s social-evaluative focus from anxiety’s threat-detection orientation.73 This distinction has potential implications for intervention design, though intervention inferences require longitudinal confirmation.
Cognitive Vulnerabilities: Outcome-Specific Variation
The marked variation in associations between cognitive difficulties and different outcomes parallels what we term a “cognitive penetrance gradient”.74 This pattern suggests that mental health outcomes differ in their dependence on cognitive functioning relative to social and environmental factors, though the underlying mechanisms remain to be established.
Our findings partially support and extend Beck’s cognitive specificity hypothesis.71,73 While previous research distinguished cognitive patterns between depression and anxiety,21,22 the present study suggests a broader spectrum of cognitive involvement across four distinct outcomes. Anxiety showed the strongest cognitive association, consistent with models emphasizing attention biases and executive dysfunction.75 However, the weak association with loneliness is in line with the interpretation that adolescent loneliness may more directly reflect actual social isolation rather than cognitive distortion, though alternative explanations cannot be excluded.76 A recent meta-analysis similarly suggests that social skill training and peer contact opportunities may be more effective than purely cognitive interventions for reducing adolescent loneliness.77
For life satisfaction, the minimal association with cognitive difficulties aligns with previous international evidence and suggests that life satisfaction may involve integration across multiple domains.78 Compensatory factors, particularly perceived community social inclusion, may help maintain wellbeing despite cognitive challenges.
The Peer Specificity of Loneliness
Loneliness showed exceptional sensitivity to school and peer domain factors, with this domain contributing approximately ten times more incremental variance than for anxiety. The specificity is particularly evident in friendship effects. Number of close friends showed a strong negative association with loneliness but negligible associations with depression or anxiety.
These findings both support and refine the evolutionary theory of loneliness,79 which conceptualizes loneliness as a signal for social disconnection. A recent Norwegian study found that difficulty communicating with peers was more strongly associated with loneliness than difficulty communicating with parents.31 This parallel supports the present finding that peer domain factors showed stronger associations with loneliness than family domain factors.
Similarly, the association between recess experiences and loneliness extends recent work38,39 and highlights the potential importance of informal peer interaction. This finding has particular relevance in the Finnish context, where schools maintain regular breaks providing multiple opportunities for unstructured peer interaction.
Theoretical and Practical Implications
We propose an Asymmetric Ecological Model that highlights three patterns. First, level asymmetry: in mid-adolescence, perceived community social inclusion showed associations with life satisfaction and depression comparable to or exceeding certain proximal domain factors, but not others. Second, outcome asymmetry: mental health indicators exhibit distinct ecological signatures. Individual vulnerability associations were strongest for internalizing symptoms, peer-centric associations were strongest for loneliness, and multi-domain associations were most evident for life satisfaction. Third, a main-effect-dominant architecture: risk and protective factors predominantly contributed additively, with only modest, outcome-specific interactions detected for depression. This pattern aligns with evidence that environmental protective factors typically operate through promotive rather than buffering pathways.80,81
These findings have potential implications for public health approaches to adolescent mental health. If longitudinal or experimental evidence were to confirm the present associations, community strategies that strengthen participation, belonging, and inclusion in everyday youth environments may complement individual and family approaches. The finding that family financial situation retained modest but significant associations with all outcomes parallels prior Nordic research documenting residual socioeconomic gradients in adolescent wellbeing even within comprehensive welfare systems. Schools should continue investing in belonging and peer engagement programs, with particular attention to students with few close friends. The finding that protective factors predominantly showed additive rather than buffering associations, if replicated longitudinally, would suggest that population-level environmental approaches may benefit all adolescents rather than only those with identified vulnerabilities.
The present findings do not support a simple rebalancing of investment from individual therapy toward community-level prevention. Rather, they are consistent with a layered approach in which community and individual interventions are considered complementary rather than competing priorities.
Strengths and Limitations
This study’s primary strength is its large sample size, providing statistical power to detect small effects and test interactions precisely. Comprehensive assessment across five analytic domains and four mental health outcomes enables systematic comparison rarely possible in smaller studies. The use of validated ESIS scale also strengthened measurement of the perceived community social inclusion construct.
Several limitations require explicit acknowledgment. First and most importantly, the cross-sectional design precludes causal inference. The observed associations are consistent with the interpretation that perceived community social inclusion is associated with better mental health, but they are equally consistent with the reverse: adolescents with better mental health may be more likely to perceive themselves as socially included. The discussion of possible mechanisms should be read as theoretically motivated interpretation rather than causal explanation. Longitudinal or experimental designs are needed to address the direction of these associations.
Second, all key variables were assessed through adolescent self-report, introducing the possibility of shared method variance. The high zero-order correlations between ESIS and life satisfaction and between ESIS and depression are particularly notable in this regard. Perceived social inclusion and life satisfaction both involve broad subjective evaluations of one’s social world, so part of their strong association may reflect shared evaluative tone rather than a genuinely distinct ecological effect. Additionally, one recess experience item (“I feel lonely at recesses”) overlaps conceptually with the general loneliness outcome, which may partly contribute to the strength of that association, although the two constructs differ in scope (situational vs. general). Future research using multi-method or informant-report designs would help disentangle these possibilities.
Third, single-item measures for loneliness, life satisfaction, parent-child relationship, and family financial situation provide more limited construct coverage than multi-item instruments and may attenuate the detection of smaller but meaningful associations. These measures may have attenuated some associations, but the direction and extent of any resulting bias cannot be determined in the present study.
Fourth, the analytic strategy used blockwise OLS regression, which treats all variables at a single level of analysis. The SHPS data do not contain school- or community-level cluster identifiers, which precluded a multilevel modelling approach. As a result, what we term “community-domain” associations reflect individual-level perceptions of community social inclusion rather than aggregated structural characteristics of communities. The ecological claim embedded in these findings is therefore limited to the individual perceptual level. Future research using multilevel designs with structural community measures would provide a stronger test of ecological theory.
Fifth, missing data were not missing completely at random, and boys were overrepresented in the excluded group. Although effect sizes for outcome variables were trivial across complete and incomplete cases, and gender was included as a covariate, residual bias from differential missingness cannot be excluded.
Sixth, the study was conducted in Finland, a high-welfare Nordic society with relatively low income inequality and universal school-based services. The ecological associations observed here may not generalize directly to societies with higher material inequality or less comprehensive youth welfare infrastructure.
Conclusion
This study examined associations between factors across five analytic domains and four mental health outcomes in a large, broadly representative national school-based sample of Finnish adolescents. The findings are consistent with a challenge to the proximal dominance assumption: perceived community social inclusion showed the largest standardized association with life satisfaction and the largest standardized negative association among contextual predictors with depression, after adjustment for individual, family, and school domain factors. Different mental health outcomes showed distinct ecological signatures, with cognitive difficulties strongest for internalizing symptoms, school and peer factors strongest for loneliness, and perceived community social inclusion showing the broadest relevance across outcomes.
Protective factors were observed predominantly in additive rather than interactive patterns, providing limited support for cross-level buffering. Together, these patterns are consistent with the proposed Asymmetric Ecological Model, in which the relative salience of ecological domains differs across outcomes rather than following a uniform proximity hierarchy.
These findings highlight the potential importance of perceived community social inclusion alongside more proximal ecological factors in understanding adolescent mental health. Approaches that strengthen social inclusion in everyday youth environments may complement individual and family interventions in adolescent mental health promotion, though these implications should be interpreted in light of the cross-sectional design and the self-reported nature of the key measures.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work the authors used ChatGPT 5.1 in order to improve the readability and language of the manuscript. After using this tool, the authors reviewed and edited the content as needed and took full responsibility for the content of the publication.
Data Sharing Statement
The data used in this study are available from Finnish Social Science Data Archive, http://services.fsd.tuni.fi/catalogue/FSD3551. The dataset is available by permission from the data depositor.
Ethical Approval
The Finnish School Health Promotion Study (SHPS) is an anonymous and voluntary classroom survey conducted by the Finnish Institute for Health and Welfare (THL). The SHPS research plan was evaluated within THL’s institutional ethical review procedures prior to data collection. The present study was a secondary analysis of de-identified survey data and involved no intervention with human participants. In Finland, ethical review in the human sciences is guided by the Finnish National Board on Research Integrity (TENK) guidelines, Ethical principles of research with human participants and ethical review in the human sciences in Finland (2019). The Finnish Medical Research Act (488/1999) applies to medical research involving intervention in the integrity of a person and therefore did not apply to the present secondary analysis of anonymized survey data. Accordingly, no new ethical approval was required under Finnish ethical guidance for this study. For the China-based authors, the study also met the exemption conditions under Article 32 of the 2023 Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects of the People’s Republic of China, which allows exemption for research using legally obtained anonymized or publicly available data that does not harm individuals’ rights and interests or involve sensitive personal information. All procedures were conducted in accordance with the Declaration of Helsinki.
Funding
This study was funded by the European Union [grant number 101081327]. Views and opinions expressed are however those of the author(s) only and do not necessarily reflect those of the European Union or the REA (European Research Executive Agency). Neither the European Union nor the granting authority can be held responsible for them.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cao H, Wu Y, Yin H, Sun Y, Yuan H, Tao M. Global trends in the incidence of anxiety disorders from 1990 to 2019: joinpoint and age-period-cohort analysis study. JMIR Public Health Surveillance. 2024;10(1):e49609. doi:10.2196/49609
2. Lu B, Lin L, Su X. Global burden of depression or depressive symptoms in children and adolescents: a systematic review and meta-analysis. J Affect Disord. 2024;354:553–16. doi:10.1016/j.jad.2024.03.074
3. Twenge JM, Haidt J, Blake AB, McAllister C, Lemon H, Le Roy A. Worldwide increases in adolescent loneliness. J Adolescence. 2021;93(1):257–269. doi:10.1016/j.adolescence.2021.06.006
4. Wang Z, Dou Y, Yang X, et al. Global, regional, and national burden of mental disorders among adolescents and young adults, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Transl Psychiatry. 2025;15(1):397. doi:10.1038/s41398-025-03623-w
5. Sacco R, Camilleri N, Eberhardt J, Umla-Runge K, Newbury-Birch D. A systematic review and meta-analysis on the prevalence of mental disorders among children and adolescents in Europe. Eur Child Adolesc Psychiatry. 2024;33(9):2877–2894. doi:10.1007/s00787-022-02131-2
6. Cosma A, Shynar A, Taut D, Schrijvers K, Catunda C, Schnohr C. A focus on adolescent mental health and well-being in Europe, Central Asia and Canada. Vol 1. WHO Regional Office for Europe; 2023. Available from: http://hdl.handle.net/1854/LU-01HWD5VWWVV069GA4B225Y4RCE.
7. WHO. World Mental Health Report: Transforming Mental Health for All.
8. Kauhanen L, Wan Mohd Yunus WMA, Lempinen L, et al. A systematic review of the mental health changes of children and young people before and during the COVID-19 pandemic. Eur Child Adolesc Psychiatry. 2023;32(6):995–1013. doi:10.1007/s00787-022-02060-0
9. Madigan S, Racine N, Vaillancourt T, et al. Changes in depression and anxiety among children and adolescents from before to during the COVID-19 pandemic: a systematic review and meta-analysis. JAMA Pediatr. 2023;177(6):567–581. doi:10.1001/jamapediatrics.2023.0846
10. Racine N, McArthur BA, Cooke JE, Eirich R, Zhu J, Madigan S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: a meta-analysis. JAMA Pediatr. 2021;175(11):1142–1150. doi:10.1001/jamapediatrics.2021.2482
11. Clayborne ZM, Varin M, Colman I. Systematic review and meta-analysis: adolescent depression and long-term psychosocial outcomes. J Am Acad Child Adolesc Psychiatry. 2019;58(1):72–79. doi:10.1016/j.jaac.2018.07.896
12. Viner RM, Ozer EM, Denny S, et al. Adolescence and the social determinants of health. Lancet. 2012;379(9826):1641–1652. doi:10.1016/S0140-6736(12)60149-4
13. Bronfenbrenner U, Morris PA. The bioecological model of human development. In: Handbook of Child Psychology. John Wiley & Sons, Ltd; 2007. doi:10.1002/9780470147658.chpsy0114
14. Slimmen S, Timmermans O, Lechner L, Oenema A. A socio-ecological approach of evidence on associations between social environmental factors and mental health outcomes of young adults: a systematic review. Soci Sci Humanities Open. 2024;10:101068. doi:10.1016/j.ssaho.2024.101068
15. Branje S, de Moor EL, Spitzer J, Becht AI. Dynamics of identity development in adolescence: a decade in review. J Res Adolescence. 2021;31(4):908–927. doi:10.1111/jora.12678
16. Dahl RE, Allen NB, Wilbrecht L, Suleiman AB. Importance of investing in adolescence from a developmental science perspective. Nature. 2018;554(7693):441–450. doi:10.1038/nature25770
17. Currie C, Zanotti C, Morgan A, et al. Social Determinants of Health and Well-Being among Young People: Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey. WHO Regional Office for Europe; 2012. Available from: https://www.who.int/europe/publications/i/item/9789289014236.
18. Masten AS. Global perspectives on resilience in children and youth. Child Development. 2014;85(1):6–20. doi:10.1111/cdev.12205
19. Currie C, Morgan A. A bio-ecological framing of evidence on the determinants of adolescent mental health - A scoping review of the international Health Behaviour in School-Aged Children (HBSC) study 1983–2020. SSM Popul Health. 2020;12:100697. doi:10.1016/j.ssmph.2020.100697
20. Marquez J, Humphrey N, Black L, Wozmirska S. This is the place: a multi-level analysis of neighbourhood correlates of adolescent wellbeing. Soc Psychiatry Psychiatr Epidemiol. 2024;59(6):929–946. doi:10.1007/s00127-023-02531-y
21. Rabner JC, Ney JS, Kendall PC. Cognitive functioning in youth with anxiety disorders: a systematic review. Clin Child Fam Psychol Rev. 2024;27(2):357–380. doi:10.1007/s10567-024-00480-9
22. Schumacher A, Campisi SC, Khalfan AF, Merriman K, Williams TS, Korczak DJ. Cognitive functioning in children and adolescents with depression: a systematic review and meta-analysis. Eur Neuropsychopharmacol. 2024;79:49–58. doi:10.1016/j.euroneuro.2023.11.005
23. Shannon H, Bush K, Villeneuve PJ, Hellemans KG, Guimond S. Problematic social media use in adolescents and young adults: systematic review and meta-analysis. JMIR Mental Health. 2022;9(4):e33450. doi:10.2196/33450
24. Jensen M, George MJ, Russell MR, Odgers CL. Young adolescents’ digital technology use and mental health symptoms: little evidence of longitudinal or daily linkages. Clin Psychol Sci. 2019;7(6):1416–1433. doi:10.1177/2167702619859336
25. Odgers CL, Jensen M. Annual research review: adolescent mental health in the digital age: facts, fears, and future directions. J Child Psychol Psychiatr. 2020;61(3):336–348. doi:10.1111/jcpp.13190
26. Jespersen A, Madden RA, Whalley HC, et al. Socioeconomic status and depression—a systematic review. Epidemiol Rev. 2025;47(1):mxaf011. doi:10.1093/epirev/mxaf011
27. Ridley M, Rao G, Schilbach F, Patel V. Poverty, depression, and anxiety: causal evidence and mechanisms. Science. 2020;370(6522):eaay0214. doi:10.1126/science.aay0214
28. Elgar FJ. 81. Trends and socioeconomic inequalities in youth mental health, 2019 to 2022: evidence from the gallup world poll. J Adolesc Health. 2024;74(3):S43–S44. doi:10.1016/j.jadohealth.2023.11.279
29. Corell M, Friberg P, Petzold M, Löfstedt P. Socioeconomic inequalities in adolescent mental health in the Nordic countries in the 2000s - A study using cross-sectional data from the health behaviour in school-aged children study. Arch Public Health. 2024;82(1):20. doi:10.1186/s13690-024-01240-5
30. Zapf H, Boettcher J, Haukeland Y, Orm S, Coslar S, Fjermestad K. A systematic review of the association between parent-child communication and adolescent mental health. JCPP Advances. 2024;4(2):e12205. doi:10.1002/jcv2.12205
31. Madsen KR, Damsgaard MT, Petersen K, Qualter P, Holstein BE. Loneliness and ease of communication with parents and friends: cross-sectional study of adolescents in Denmark. BMC Public Health. 2025;25(1). doi:10.1186/s12889-025-22947-2
32. Arnarsson ÁM, Potrebny T, Torsheim T, Eriksson C. Time-trends in Nordic adolescents’ communication with their parents. Nordisk välfärdsforskning. 2019;4(2):88–100. doi:10.18261/issn.2464-4161-2019-02-06
33. Raniti M, Rakesh D, Patton GC, Sawyer SM. The role of school connectedness in the prevention of youth depression and anxiety: a systematic review with youth consultation. BMC Public Health. 2022;22(1):2152. doi:10.1186/s12889-022-14364-6
34. Allen K-A, Greenwood CJ, Berger E, et al. Adolescent school belonging and mental health outcomes in young adulthood: findings from a multi-wave prospective cohort study. School Mental Health. 2024;16(1):149–160. doi:10.1007/s12310-023-09626-6
35. Birrell L, Werner-Seidler A, Davidson L, Andrews JL, Slade T. Social connection as a key target for youth mental health. Mental Health Prev. 2025;37:200395. doi:10.1016/j.mhp.2025.200395
36. Alsarrani A, Hunter RF, Dunne L, Garcia L. Association between friendship quality and subjective wellbeing among adolescents: a systematic review. BMC Public Health. 2022;22(1):2420. doi:10.1186/s12889-022-14776-4
37. Ye Z, Wu D, He X, et al. Meta-analysis of the relationship between bullying and depressive symptoms in children and adolescents. BMC Psychiatry. 2023;23(1):215. doi:10.1186/s12888-023-04681-4
38. Lodewyk KR, McNamara L. Children’s recess affect, enjoyment, physical activity, and opportunities by victimization, developmental level, school region, and recess location. Physical Educator. 2025;82(4):456–480. doi:10.18666/TPE-2025-V82-I4-12394
39. McNamara L, Lodewyk K, Franklin N. Recess: a study of belongingness, affect, and victimization on the playground. Child Sch. 2018;40(2):114–121. doi:10.1093/cs/cdy006
40. Leemann L, Martelin T, Koskinen S, Härkänen T, Isola A-M. Development and psychometric evaluation of the experiences of social inclusion scale. J Human Develop Capabilities. 2022;23(3):400–424. doi:10.1080/19452829.2021.1985440
41. Oxoby R. Understanding social inclusion, social cohesion, and social capital. Int J Social Econ. 2009;36(12):1133–1152. doi:10.1108/03068290910996963
42. Davisson EK, Andrade FC, Godwin J, Hoyle R, Rosenbaum JE. Adolescent reports of subjective socioeconomic status: an adequate alternative to parent-reported objective and subjective socioeconomic status? PLoS One. 2025;20(1):e0317777. doi:10.1371/journal.pone.0317777
43. Lange MK, Just-Nørregaard V, Winding TN, Lin C-Y. How does subjective social status at school at the age of 15 affect the risk of depressive symptoms at the ages of 18, 21, and 28? A longitudinal study. PLoS One. 2023;18(12):e0296349. doi:10.1371/journal.pone.0296349
44. Altinay L, Alrawadieh Z, Hudec O, Urbančíková N, Evrim Arici H. Modelling social inclusion, self-esteem, loneliness, psychological distress, and psychological resilience of refugees: does hospitableness matter? J Business Res. 2023;162:113901. doi:10.1016/j.jbusres.2023.113901
45. Breedvelt JJF, Tiemeier H, Sharples E, et al. The effects of neighbourhood social cohesion on preventing depression and anxiety among adolescents and young adults: rapid review. BJPsych Open. 2022;8(4):e97. doi:10.1192/bjo.2022.57
46. Zhou J, Zhu N, Suwada K, Toikko T. The protective role of social inclusion: loneliness as a mediator between excessive internet use and depressive symptoms in adolescents. Psychol Res Behav Manag. 2025;18:1701–1715. doi:10.2147/PRBM.S532794
47. Oh J, Thomas MMC. The mediating role of neighborhood social cohesion and trust in the relationship between childhood material hardship and adolescent depression. Health Place. 2024;85:103162. doi:10.1016/j.healthplace.2023.103162
48. Shareck M, Sersli S, Aubé E, et al. Neighborhood physical and social environments and social inequalities in health in older adolescents and young adults: a scoping review. Int J Environ Res Public Health. 2023;20(8):5474. doi:10.3390/ijerph20085474
49. Crone EA, van Drunen L. Development of self-concept in childhood and adolescence: how neuroscience can inform theory and vice versa. Human Development. 2024;68(5–6):255–271. doi:10.1159/000539844
50. OECD. Social spending. 2024. Available from: https://www.oecd.org/en/topics/social-spending.html.
51. THL. School Health Promotion Study: Eight- and Ninth-Graders in Basic Education and First- and Second-Year Students in Upper Secondary Education; 2019. doi:10.60686/t-fsd3551
52. THL. School health promotion study - THL. Finnish Institute for Health and Welfare (THL), Finland. 2024. Available from: https://thl.fi/en/research-and-development/research-and-projects/school-health-promotion-study.
53. Aalto A-M, Elovainio M, Kivimäki M, Uutela A, Pirkola S. The beck depression inventory and general health questionnaire as measures of depression in the general population: a validation study using the composite international diagnostic interview as the gold standard. Psychiatry Res. 2012;197(1–2):163–171. doi:10.1016/j.psychres.2011.09.008
54. Blom EH, Bech P, Högberg G, Larsson JO, Serlachius E. Screening for depressed mood in an adolescent psychiatric context by brief self-assessment scales – testing psychometric validity of WHO-5 and BDI-6 indices by latent trait analyses. Health Qual Life Outcomes. 2012;10(1):149. doi:10.1186/1477-7525-10-149
55. Löwe B, Decker O, Müller S, et al. Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med Care. 2008;46(3):266–274. doi:10.1097/MLR.0b013e318160d093
56. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Internal Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
57. Burns-Cusato M, Cusato B. Where in the world is this research taking us? Collaborating on publishable research with undergraduates abroad. Front Psychol. 2019;10:10. doi:10.3389/fpsyg.2019.00010
58. Mossman SA, Luft MJ, Schroeder HK, et al. The generalized anxiety disorder 7-item scale in adolescents with generalized anxiety disorder: signal detection and validation. Ann Clin Psychiatry. 2017;29(4):227–234A.
59. Raudenská P. Single-item measures of happiness and life satisfaction: the issue of cross-country invariance of popular general well-being measures. Humanit Soc Sci Commun. 2023;10(1):861. doi:10.1057/s41599-023-02299-1
60. Mund M, Freuding M, Möbius K, Horn N, Neyer F. The stability and change of loneliness across the life span: a meta-analysis of longitudinal studies. Personality Social Psychol Rev. 2020;24(1):24–52. doi:10.1177/1088868319850738
61. Arora A. Measuring child functioning: the UNICEF/Washington group module. Unicef Data. 2017. Available from: https://data.unicef.org/resources/measuring-child-functioning-unicefwashington-group-model/.
62. Griffiths M. A ‘components’ model of addiction within a biopsychosocial framework. J Subst Use. 2005;10(4):191–197. doi:10.1080/14659890500114359
63. Škařupová K, Ólafsson K, Blinka L. Excessive Internet Use and its association with negative experiences: quasi-validation of a short scale in 25 European countries. Computers Human Behav. 2015;53:118–123. doi:10.1016/j.chb.2015.06.047
64. Abdulhamed R, Lonka K, Hietajärvi L, Ikonen R, Klemetti R. Anxiety and depression symptoms and their association with discrimination and a lack of social support among first- and second-generation immigrant adolescents. Int J Intercultural Relations. 2022;87:193–205. doi:10.1016/j.ijintrel.2022.03.001
65. Meisner MW, Lenzenweger MF, Storebø OJ, Petersen LS, Bach B, Simonsen E. Co-occurrence of borderline and schizotypal personality disorders: a scoping review. Nordic J Psychiatry. 2024;78(1):1–9. doi:10.1080/08039488.2023.2254299
66. Karjalainen V, Rantanen A, Matikka A, Koivisto AM, Joronen K. Perhetekijöiden ja sosioekonomisten tekijöiden yhteys ammattiin opiskelevien nuorten itsearvioituun ahdistuneisuuteen. Hoitotiede. 2017;29(2):113–124.
67. Currie C, Nic Gabhainn S, Godeau E, et al. Inequalities in young people’s health | HBSC study. WHO Regional Office for Europe; 2008. https://www.hbsc.org/publications/reports/inequalities-in-young-peoples-health/.
68. Finell E, Tolvanen A, Claeson A-S, Helenius J. How student perceptions of stuffy air and unpleasant odour are associated with students’ well-being: cross-level interaction effects of school climate. J Environ Psychol. 2024;93:102211. doi:10.1016/j.jenvp.2023.102211
69. Aguinis H, Beaty JC, Boik RJ, Pierce CA. Effect size and power in assessing moderating effects of categorical variables using multiple regression: a 30-year review. J Appl Psychol. 2005;90(1):94–107. doi:10.1037/0021-9010.90.1.94
70. Ahrnberg H, Appelqvist-Schmidlechner K, Mustonen P, Fröjd S, Aktan-Collan K. Determinants of positive mental health in adolescents–a cross-sectional study on relationships between positive mental health, self-esteem, character strengths and social inclusion. Int J Mental Health Promotion. 2021;23(3):361–374. doi:10.32604/IJMHP.2021.016408
71. Beck AT, Bredemeier K. A unified model of depression: integrating clinical, cognitive, biological, and evolutionary perspectives. Clin Psychol Sci. 2016;4(4):596–619. doi:10.1177/2167702616628523
72. Schriber RA, Guyer AE. Adolescent neurobiological susceptibility to social context. Develop Cognitive Neurosci. 2016;19:1–18. doi:10.1016/j.dcn.2015.12.009
73. Clark DA, Beck AT. Cognitive Therapy of Anxiety Disorders: Science and Practice. Guilford Press; 2011.
74. Schweizer S, Parker J, Leung JT, Griffin C, Blakemore S-J. Age-related differences in affective control and its association with mental health difficulties. Develop Psychopathol. 2020;32(1):329–341. doi:10.1017/S0954579419000099
75. Mogg K, Bradley BP. Anxiety and threat-related attention: cognitive-motivational framework and treatment. Trends Cognitive Sci. 2018;22(3):225–240. doi:10.1016/j.tics.2018.01.001
76. Spithoven AWM, Bijttebier P, Goossens L. It is all in their mind: a review on information processing bias in lonely individuals. Clinic Psychol Rev. 2017;58:97–114. doi:10.1016/j.cpr.2017.10.003
77. Eccles AM, Qualter P. Review: alleviating loneliness in young people – a meta-analysis of interventions. Child Adolescent Mental Health. 2021;26(1):17–33. doi:10.1111/camh.12389
78. OECD. PISA 2015 Results (Volume III): Students’ Well-Being. OECD; 2017.
79. Cacioppo JT, Cacioppo S. The growing problem of loneliness. Lancet. 2018;391(10119):426. doi:10.1016/S0140-6736(18)30142-9
80. Fergus S, Zimmerman MA. Adolescent resilience: a framework for understanding healthy development in the face of risk. Annu Rev Public Health. 2005;26(1):399–419. doi:10.1146/annurev.publhealth.26.021304.144357
81. Rueger SY, Malecki CK, Pyun Y, Aycock C, Coyle S. A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychol Bull. 2016;142(10):1017–1067. doi:10.1037/bul0000058
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Totally All Alone with My Thoughts: Development, Psychometric Properties and Correlates of the Loneliness Automatic Thoughts Questionnaire
Rose AL, Goldberg JO, Flett GL, Nepon T, Besser A
Psychology Research and Behavior Management 2024, 17:1073-1085
Published Date: 12 March 2024
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025