Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Retrospective Study of Real-World Treatment Patterns of Subcutaneous Semaglutide Use Among Patients with Metabolic Dysfunction-Associated Steatohepatitis in the United States
Authors Kim Y, Zeng N, Winer-Jones JP ![]() , Bonafede M, Lobo F, O'Donnell J, Ryan T
, Bonafede M, Lobo F, O'Donnell J, Ryan T
Received 19 August 2025
Accepted for publication 7 October 2025
Published 22 October 2025 Volume 2025:17 Pages 743—754
DOI https://doi.org/10.2147/CEOR.S546841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Yestle Kim,1 Ni Zeng,2 Jessamine P Winer-Jones,2 Machaon Bonafede,2 Francis Lobo,1 John O’Donnell,1 Taylor Ryan2
1Health Economics and Outcomes Research Madrigal Pharmaceuticals, Inc, West Conshohocken, PA, USA; 2Real World Evidence, Veradigm, Chicago, IL, USA
Correspondence: Yestle Kim, Health Economics and Outcomes Research, Madrigal Pharmaceuticals, West Conshohocken, PA, USA, Email [email protected]
Background: Interim results from the ESSENCE clinical trials indicate that 72-week treatment with high-dose subcutaneous (SC) semaglutide may result in metabolic dysfunction-associated steatohepatitis (MASH) resolution and improvements in fibrosis. As some patients with MASH have been prescribed SC semaglutide for the treatment of comorbid type 2 diabetes and/or obesity, this study assessed real-world 72-week treatment patterns among patients with MASH.
Methods: In a linked electronic health records (Veradigm Network EHR) and claims (Komodo Health) dataset, adults (≥ 18 years old) with a MASH diagnosis, who initiated treatment with SC semaglutide between 7/1/2018 and 6/30/2023, were identified. Other causes of liver disease (eg, viral hepatitis) or severe complications (eg, cirrhosis) were excluded. The study period included ≥ 52 weeks before and ≥ 72 weeks after the first SC semaglutide claim. A subgroup analysis was conducted among those who received the brand approved for 2.4 mg/week dosage (SC semaglutide 2.4) and among people at risk for MASH. Patient characteristics and treatment patterns are reported.
Results: This study identified 6,537 patients with MASH, who initiated treatment with SC semaglutide, 358 of whom received only the brand approved for 2.4 mg/week dosage. Patients were ~50 years old, and a majority were female. Non-persistence occurred in 68.4% of the overall SC semaglutide cohort and 78.5% of the SC semaglutide 2.4 subgroup. The mean time to non-persistence was 24.8 (19.3) and 20.1 (16.9) weeks in the SC semaglutide and SC semaglutide 2.4 groups, respectively. In the SC semaglutide 2.4 subgroup, 182 patients (50.8%) reached the recommended dosage of 2.4 mg/week, and 28 (7.8%) reached the recommended dosage within the first 16 weeks and sustained that dosage for ≥ 56 weeks. Trends were similar among patients at risk for MASH.
Conclusion: In a real-world setting, very few patients achieved the treatment regimen associated with MASH resolution and improvements in fibrosis.
Keywords: metabolic dysfunction-associated steatohepatitis, non-alcoholic steatohepatitis, metabolic dysfunction–associated fatty liver disease, semaglutide, GLP-1 receptor agonist
Introduction
Metabolic dysfunction-associated steatohepatitis (MASH) is the progressive, fibrotic, inflammatory subtype of metabolic dysfunction-associated steatotic liver disease, associated with severe complications, including cirrhosis, hepatocellular cancer, end-stage liver disease, and liver transplantation.1,2 Potentially arising from underlying insulin resistance,3,4 MASH is commonly comorbid with other metabolic conditions, such as obesity and type 2 diabetes.5,6 In one recent study, 54% of patients with MASH had a comorbid diagnosis of type 2 diabetes, and 77% had a comorbid diagnosis of obesity.7 As prior studies have shown that a reduction in body mass is associated with MASH resolution and a regression of fibrosis,8,9 current guidelines recommend weight loss as a first-line therapy for MASLD and the metabolic comorbidities associated with MASH.10–12
Subcutaneous (SC) semaglutide is a glucagon-like peptide-1 receptor agonist (GLP-1 RA) approved in the US for the treatment of type 2 diabetes, obesity, and, most recently, MASH.13,14 Among patients with diabetes and/or obesity, SC semaglutide has been associated with decreases in body weight, changes in body composition, and improvements in quality of life.15 Interim 72-week data from the ongoing Phase 3 ESSENCE clinical trial indicated that sustained treatment of SC semaglutide at a dosage of 2.4 mg/week can result in MASH resolution and fibrosis improvement among patients with MASH.16 In that trial, patients were directed to reach a recommended dosage of 2.4 mg/week after the first 16 weeks and maintain that dosage for another 56 weeks for a total of 72 weeks of continuous treatment; however, existing real-world research has shown high rates of discontinuation among individuals taking SC semaglutide or other GLP-1 RAs, particularly among those diagnosed with obesity without type 2 diabetes.17–20
While SC semaglutide was only recently approved for the treatment of MASH, some patients with MASH have been prescribed SC semaglutide for the treatment of comorbid obesity and/or type 2 diabetes.11,12 As a result, it is possible to assess the real-world utilization of SC semaglutide among patients with MASH. The primary aim of this retrospective study was to assess real-world 72-week treatment patterns of SC semaglutide among patients with MASH with a focus on those who reached a dosage of 2.4 mg/week. The secondary aim was to explore SC semaglutide treatment patterns among a cohort of patients who are at-risk for MASH.
Methods
Data Sources and Ethical Compliance
This retrospective, observational cohort study used electronic health records (EHR) from the Veradigm Network EHR Database linked with insurance claims data from the Komodo Health Healthcare Map. The EHR dataset consists of de-identified patient records sourced from ambulatory/outpatient primary care and specialty settings. The insurance claims data contains de-identified inpatient, outpatient, and pharmacy claims; only closed claims were used for this study. Because the linked dataset is certified as statistically de-identified under the HIPAA Privacy Rule, the use of the data did not constitute research with human subjects. Therefore, this study did not require institutional review board approval.
This study was conducted in compliance with the Declaration of Helsinki and is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.21
Study Cohort
Patients with ≥1 pharmacy claim for SC semaglutide between July 1, 2018, and June 30, 2023, were identified, and their index date was the date of their earliest prescription for SC semaglutide during that period. Patients were required to be ≥18 years old on the index date and have a diagnosis of MASH (International Classification of Diseases, 10th Edition, Clinical Modification: K75.81) any time before the index date, on the index date, or up to 1 year after the index date. Patients were excluded if they 1) had a prescription for SC semaglutide before their index date, 2) had a diagnosis of viral hepatitis, alcoholism or alcoholic liver disease, opioid disorders, type 1 diabetes, gestational diabetes, or bariatric surgery at any time in their medical record, or 3) had a diagnosis of cirrhosis, decompensated cirrhosis, ascites, encephalopathy, varices, liver transplant, or hepatic cell carcinoma any time before their index date. Patients were required to have ≥52 weeks of continuous enrollment in claims data before their index date and ≥72 weeks of continuous enrollment after their index date. A subgroup of patients who only received the brand of SC semaglutide approved for 2.4 mg dosing (Wegovy) was also identified and labeled the SC Semaglutide 2.4 mg subgroup. This subgroup was identified because the recommended dosing schedule for this brand of SC semaglutide matches the schedule used in the ESSENCE clinical trial for patients with MASH.16
Time Periods
The baseline period was the 52 weeks preceding the index date. The follow-up period was the 72-week time period following and inclusive of the index date. This follow-up period was chosen to replicate the 72-week time period used in the interim analysis of the ESSENCE clinical trial for SC semaglutide.16
Patient Characteristics
Patient demographics, including age, sex, race, region, and year of index, were captured on the index date. Prior diagnoses of type 2 diabetes, obesity (diagnosis or BMI ≥30), and hyperlipidemia were captured in the baseline period from claims data. Body mass index (BMI) was captured for the subset of patients with a BMI measurement in the EHR in both the baseline and follow-up periods. If multiple BMI values were captured during the baseline period, the value captured closest to the index date was used. If multiple BMI values were captured during the follow-up period, the value captured closest to the end of follow-up was used.
Laboratory Test
Alanine aminotransferase (ALT), aspartate aminotransferase (AST), platelet, albumin, and hemoglobin A1C (HbA1c) lab results were captured in the baseline and follow-up periods from the EHR. Where sufficient lab results were available, the aspartate transaminase-to-platelet ratio index (APRI), fibrosis-4 (FIB-4) score, and NAFLD fibrosis score (NFS) were calculated for the baseline and follow-up periods.
Persistence and Dosing Patterns
SC semaglutide persistence and dosing patterns were measured in the 72-week follow-up period using claims data. For both the full cohort and the 2.4 mg subgroup, treatment patterns were measured among all patients. For the SC semaglutide 2.4 mg subgroup, treatment patterns and dosing patterns were also measured among patients who received ≥1 dose of 2.4 mg SC semaglutide at any time during follow-up and patients who received ≥1 dose of 2.4 mg SC semaglutide within 16 weeks of their index date.
Non-persistence was defined as having a gap in SC semaglutide treatment of ≥45 days. For the SC semaglutide 2.4 mg subgroup analysis, non-persistence on the 2.4 dosage was also examined. Restarting was defined as a new prescription for the treatment of interest (any dose or the 2.4 mg dose, depending on the analysis) after a period of non-persistence. For the subgroup analyses, dosage reductions from 2.4 mg/week were also captured. Where appropriate, this study captured the time to reach a dosage of 2.4 mg/week, the time on a dosage of 2.4 mg/week, the time to non-persistence, the time to restart, and the time on reduced dosage.
Sensitivity and Exploratory Analyses
As a sensitivity analysis, non-persistence and restarts were reassessed using a 60-day gap definition and a 90-day gap definition. As an exploratory analysis, the analysis was repeated among a separate cohort of individuals at risk for MASH who received only the brand of SC semaglutide approved for 2.4 mg dosing. Patients were considered at risk for MASH if they had a diagnosis of obesity and a diagnosis of ≥1 other metabolic risk factor (type 2 diabetes, hypertension, hyperlipidemia, or metabolic syndrome). Individuals at risk for MASH had to meet all other study criteria and could not have a diagnosis of MASH at any time in their available data.
Data Analysis
This analysis was descriptive in nature. Continuous variables are reported as mean and standard deviation (SD), while categorical variables are reported as number (n) and percent. Laboratory results are reported as median and interquartile range (IQR). Missing data, such as lab tests with claims but no EHR record, were not imputed. Descriptive statistics were generated using SAS V9.4 (SAS Institute, Cary, NC).
Results
The main analysis included 6,537 individuals with MASH who had ≥1 prescription for SC semaglutide, 358 of whom were included in the SC semaglutide 2.4 mg subgroup (Figure 1). In the overall SC semaglutide cohort, the mean (SD) age was 53.0 (10.8) years, and 65.3% were female (Table 1). Among the patients in the SC semaglutide 2.4 mg subgroup, the mean (SD) age was 48.9 (10.1) years, and 71.5% were female. Type 2 diabetes and obesity, respectively, were documented in the baseline period among 77.8% and 75.4% of the overall SC semaglutide cohort and among 16.5% and 90.8% of the SC semaglutide 2.4 mg subgroup.
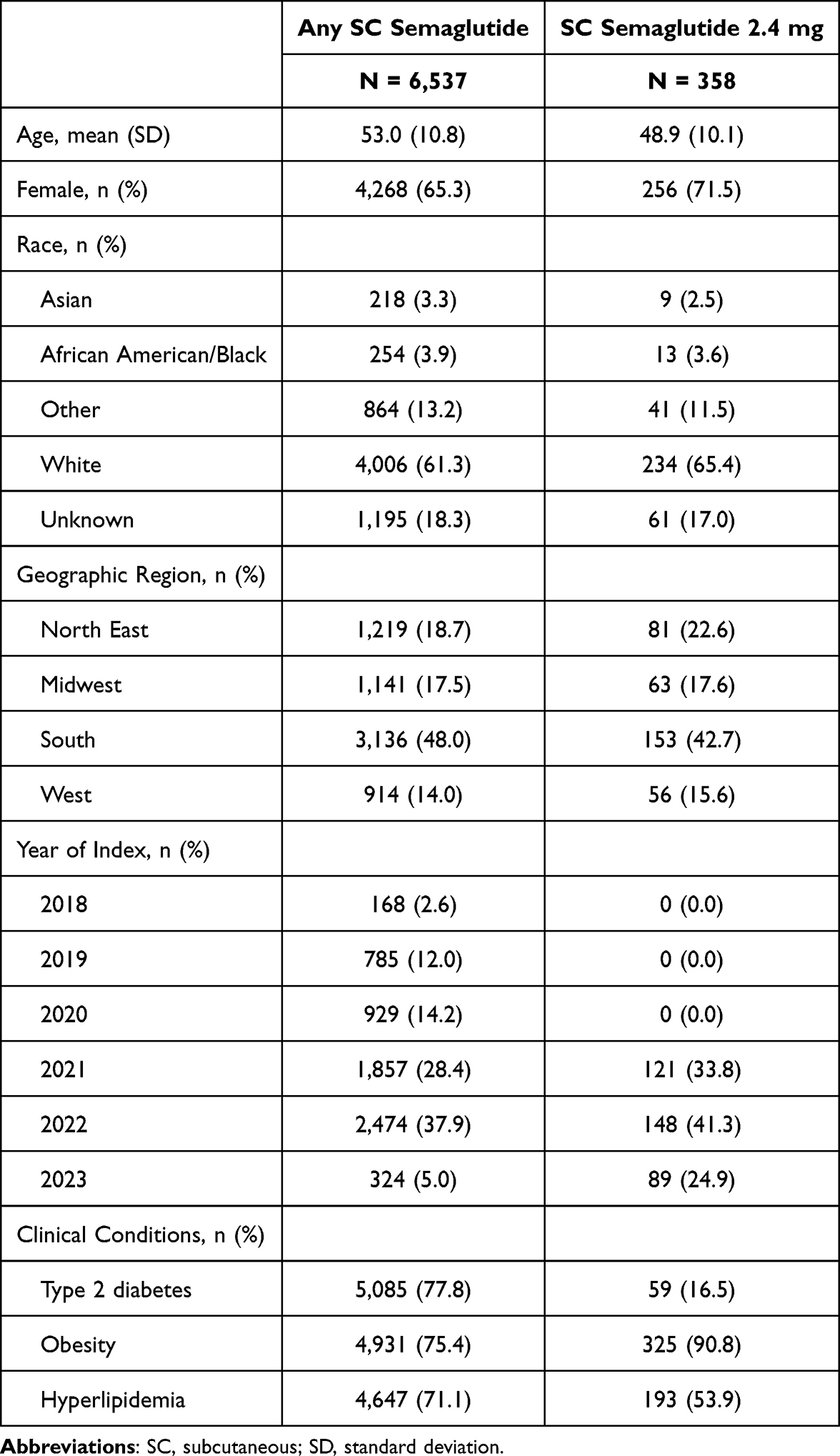 |
Table 1 Patient Characteristics |
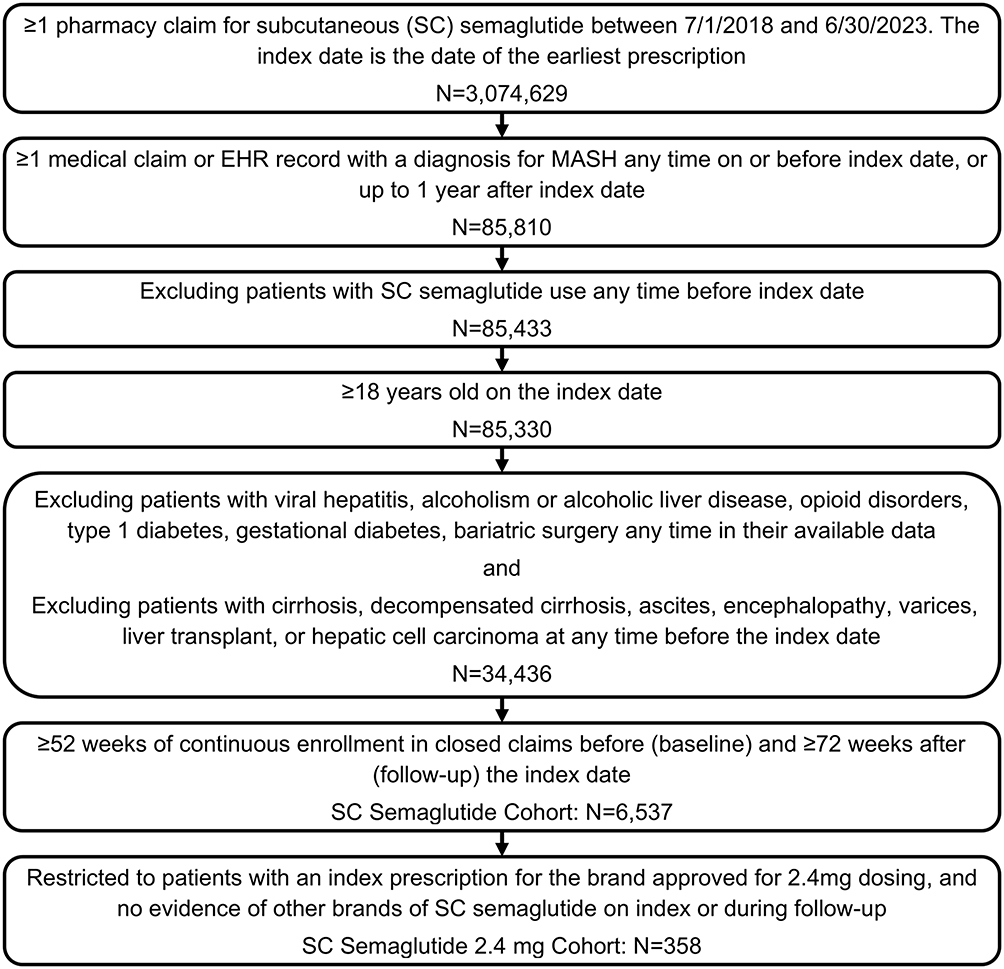 |
Figure 1 MASH Cohort Patient Selection. |
Baseline and follow-up BMI values were available for 24.2% of the overall SC semaglutide cohort and 22.1% of the SC semaglutide 2.4 mg subgroup (Table 2). On average, baseline BMI values were captured 3 months before index, and follow-up values were captured 1 year after index. Mean and median BMI values, among all patients with sufficient BMI data regardless of treatment persistence, decreased by 1–2 points between baseline and follow-up.
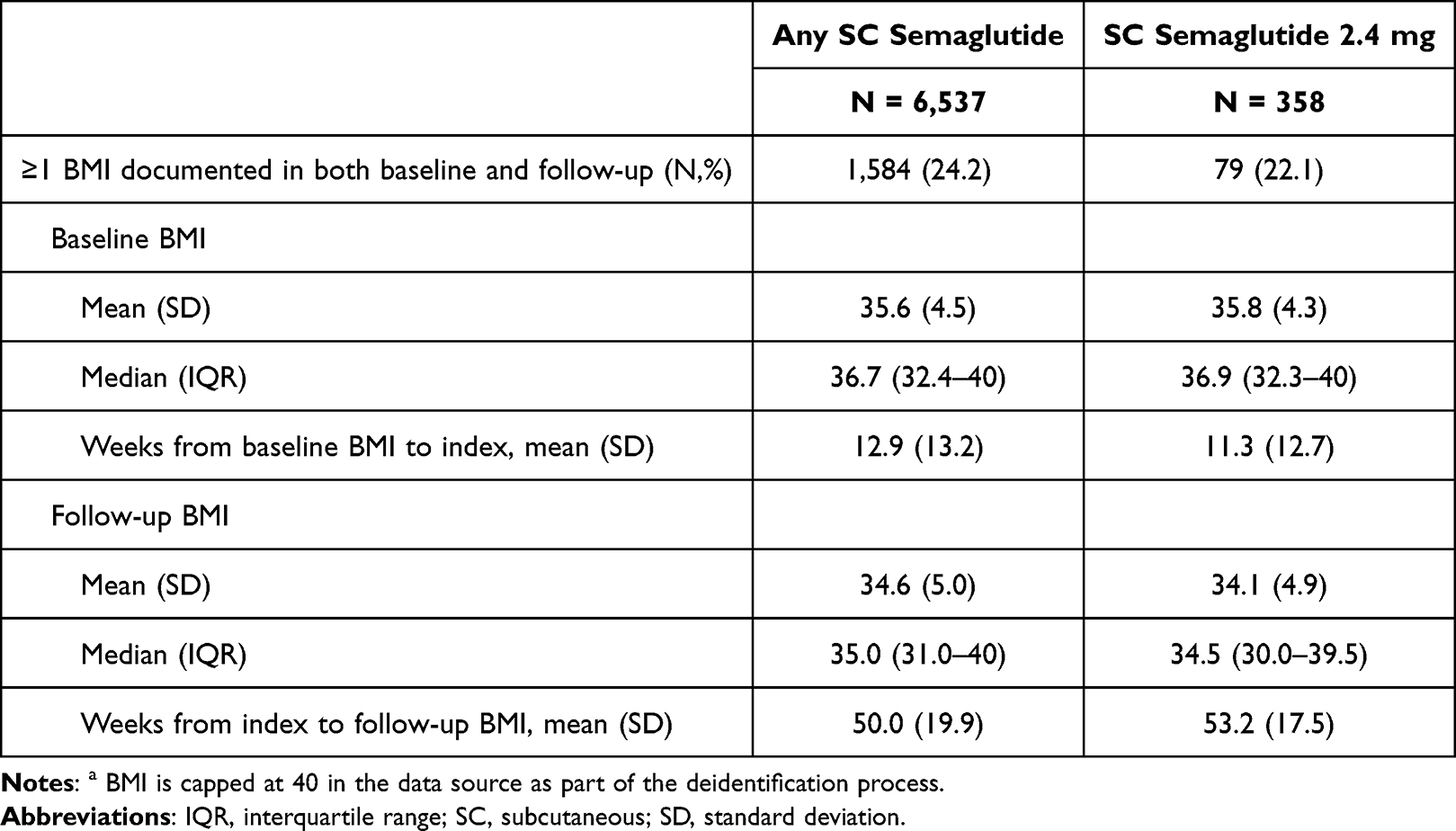 |
Table 2 Body Mass Index (BMI) in Baseline and Follow-Upa |
Liver and diabetes-related test results among those with a test result in the baseline period are reported in Supplementary Table 1. Median FIB-4, APRI, and NFS test results were similar between baseline and follow-up; however, they were only available among <10% of patients. Consistent with the expected treatment indication, median (IQR) HbA1c values were 7.3 (6.2–8.6) for the 11.6% of the overall SC semaglutide cohort with a baseline value and 5.6 (5.0–5.8) for the 7.3% of the SC semaglutide 2.4 mg subgroup with a baseline value.
Persistence and Dosing Patterns
During the 72-week follow-up period, 68.4% of the overall SC semaglutide cohort and 78.5% of the SC semaglutide 2.4 mg subgroup were non-persistent on treatment using a 45-day gap definition, with the mean times to non-persistence being 24.8 (19.3) and 20.1 (16.9) weeks, respectively (Figure 2). Restarts occurred among 52.2% of those who stopped any SC semaglutide and 33.8% of those in the SC semaglutide 2.4 mg subgroup. The time to restart was 14.8 (11.8) weeks for the overall SC semaglutide cohort and 19.1 (15.9) weeks for the SC semaglutide 2.4 mg subgroup. Among the 77 patients in the SC semaglutide 2.4 mg subgroup who were persistent on therapy, 66 (85.7%) reached a dosage of 2.4 mg/week at some point during the 72-week follow-up with the mean (SD) time to reach a dosage of 2.4 mg/week of 18.8 (13.6) weeks; while only 28 (36.4%) reached a dosage of 2.4 mg/week within the first 16 weeks after index.
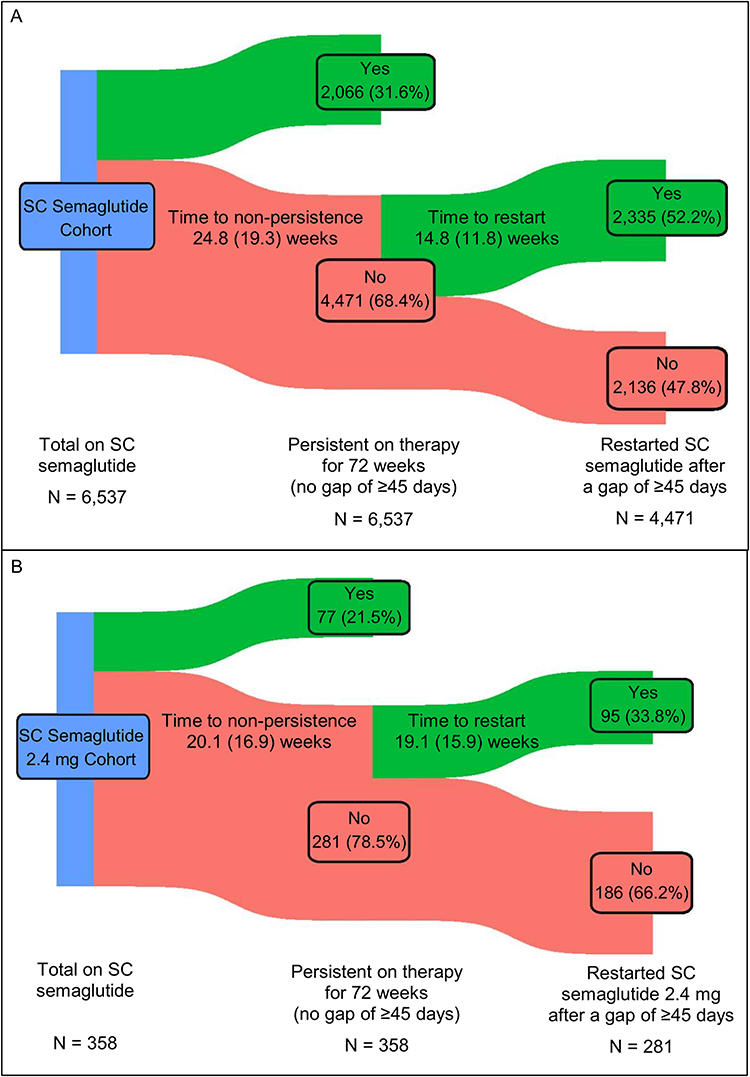 |
Figure 2 Subcutaneous (SC) Semaglutide Treatment Patterns for the (A) overall SC Semaglutide Cohort and for the (B) SC Semaglutide 2.4 mg Cohort. |
Among all patients in the SC semaglutide 2.4 mg subgroup, regardless of persistence on therapy, 182 (50.8%) patients reached a dosage of 2.4 mg/week at some point during the 72-week follow-up, and 94 (26.3%) did so within the first 16 weeks. Of those who reached a dosage of 2.4 mg/week within 16 weeks, 28 (29.8%) sustained on a dosage of 2.4 mg/week for ≥56 weeks, accounting for 7.8% of all patients in the SC semaglutide 2.4 mg subgroup (Table 3). Among the 69 (73.4%) patients who reached a dosage of 2.4 mg/week within 16 weeks and were nonpersistent, the mean (SD) duration of 2.4 mg/week therapy was 21.3 (16.9) weeks, and 29.0% of those who stopped restarted the 2.4 mg/week dosage after an average break of 13.1 (7.3) weeks.
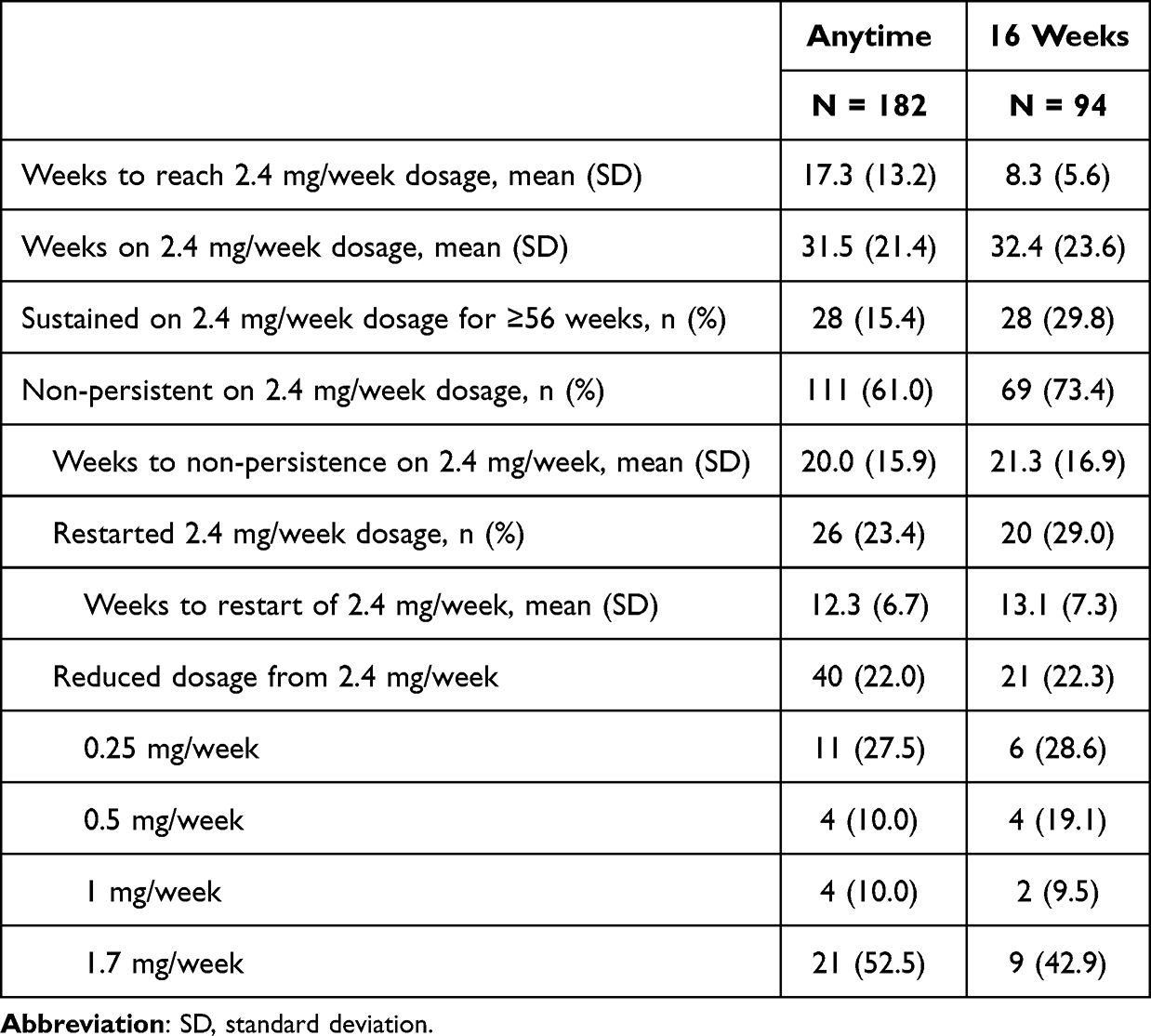 |
Table 3 Treatment Patterns Among the Patients in the SC Semaglutide 2.4 mg Cohort (N = 358) Who Reached a Dosage of 2.4 mg/week |
Sensitivity Analysis
To account for challenges in obtaining refills, the treatment patterns analysis was repeated using 60-day and 90-day gap definitions for non-persistence. The percentage of the overall SC semaglutide cohort and the SC semaglutide 2.4 mg subgroup who were non-persistent decreased to 62.0% and 76.0%, respectively, when a 60-day gap definition was applied and to 52.2% and 71.8%, respectively, when a 90-day gap definition was applied (Table 4). For those in the SC semaglutide 2.4 mg subgroup who reached a dosage of 2.4 mg/week within 16 weeks, the mean duration on a dosage of 2.4 mg increased to 34.5 (23.6) weeks and 37.3 (23.9) weeks, while the percentage of patients who sustained on the dosage of 2.4 mg/week for ≥56 weeks increased to 33.0% and 37.2%, respectively, when a 60-day or 90-day gap definition was applied (Table 5).
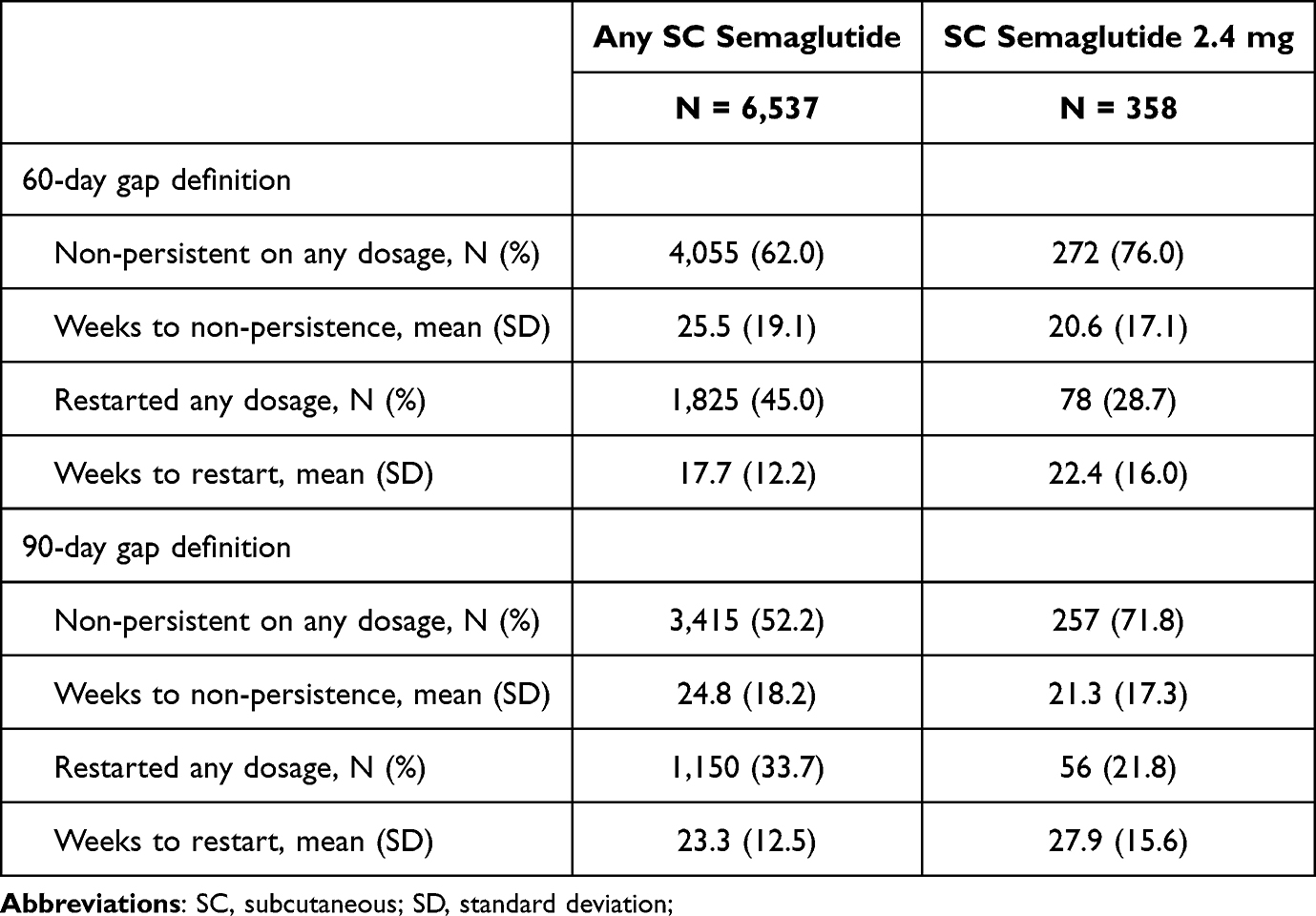 |
Table 4 Sensitivity Analysis of SC Semaglutide Treatment Patterns Using a 60-Day or 90-Day Gap Definition |
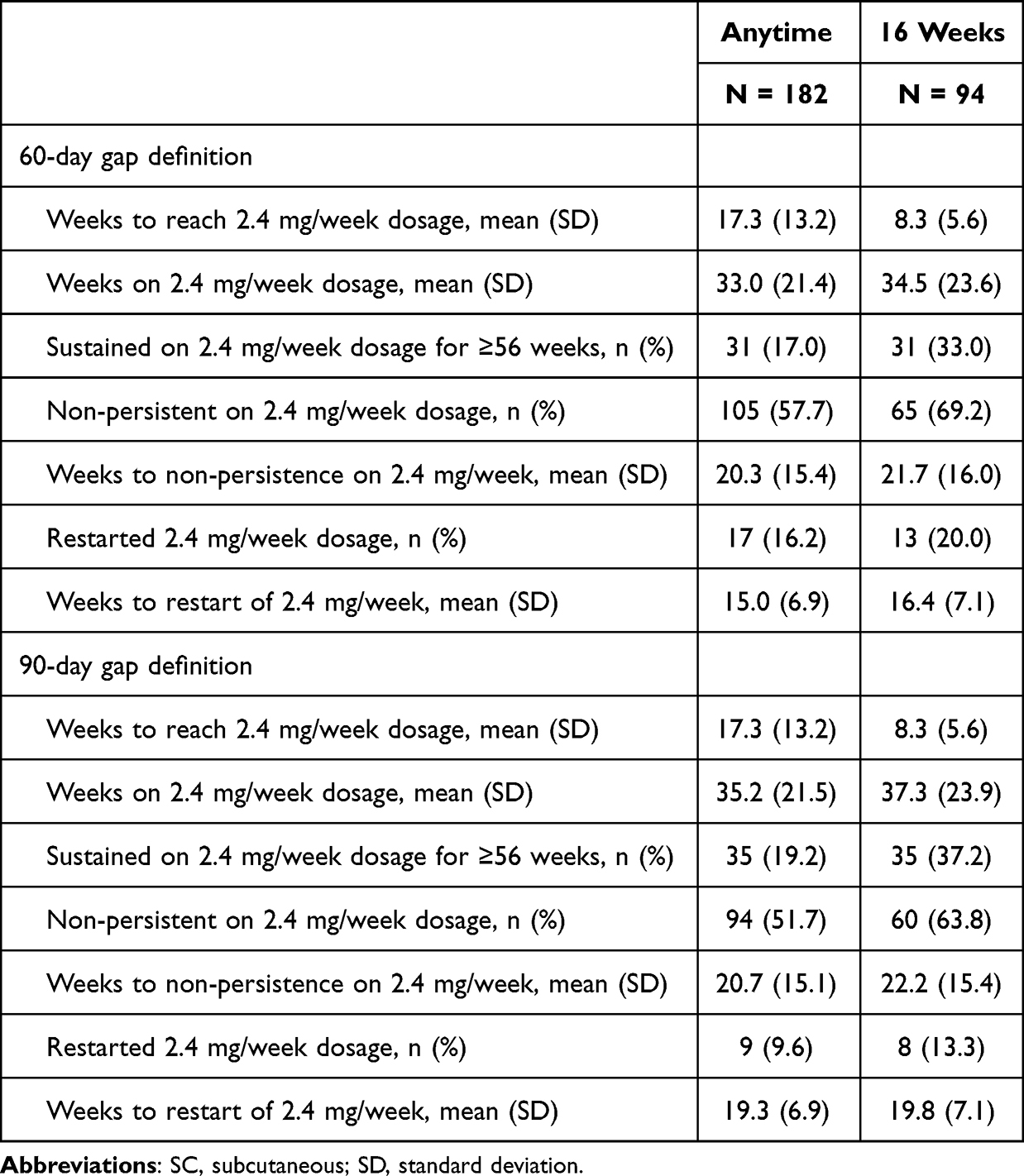 |
Table 5 Sensitivity Analysis of Treatment Patterns Among Patients in the SC Semaglutide 2.4 mg Cohort (N = 358) Who Reached a Dose of 2.4 mg Using a 60-Day or 90-Day Gap Definition |
Exploratory Analysis: At Risk for MASH Cohort
To further examine the robustness of the study findings, the subgroup analysis was repeated among a cohort of patients at risk for MASH. Individuals were defined as at-risk for MASH if they had evidence of obesity and ≥1 other metabolic risk factor any time before and up to 1 year after their first claim for SC semaglutide and no diagnosis for MASH at any time in their available record. A total of 20,454 individuals at risk for MASH who met all other criteria for the 2.4 mg subgroup analysis were identified and included in the exploratory analysis (Supplementary Figure 1).
Overall, patient characteristics and treatment patterns among individuals at risk for MASH were similar to those among patients with MASH. Specifically, the mean (SD) age was 48.3 (10.1) years, 78.5% of the participants were female, and 85.0% had a baseline diagnosis or a BMI indicating obesity (Supplementary Table 2). For the 21.8% with a BMI in baseline and follow-up, mean and median BMI values, among all patients regardless of treatment persistence, decreased by roughly 2 percentage points over follow-up. With the exception of ALT values, liver and diabetes-related labs were similar to those among patients with MASH in the SC semaglutide 2.4 mg subgroup (Supplementary Table 1). Median (IQR) ALT values were 19 points lower for at-risk patients (21 [15–30]) compared to patients with MASH (40 [23–66]) at baseline and 7 points lower at follow-up (at risk: 19 [14–28]; MASH: 26 [18–48]).
During the 72-week follow-up period, 16,081 (78.6%) individuals at risk for MASH were non-persistent; the mean time to non-persistence was 19.7 (16.9) weeks, and 35.8% of those who stopped treatment restarted before the end of follow-up (Supplementary Table 2). Among those at risk for MASH, 10,519 (51.4%) reached a dosage of 2.4 mg/week at some point during the 72-week follow-up, and 5,140 (25.1%) did so within the first 16 weeks. Of those who reached a dosage of 2.4 mg/week within 16 weeks, 1,731 (33.7%) continued on a dosage of 2.4 mg/week for ≥56 weeks, accounting for 8.5% of the at-risk for MASH cohort. Among the 3,499 (68.1%) who reached a dosage of 2.4 mg/week within 16 weeks and were non-persistent, the mean (SD) duration of therapy was 19.9 (15.9) weeks, and 1,230 (35.2%) of those who stopped restarted the 2.4 mg/week dosage after an average break of 14.1 (10.7) weeks.
Discussion
In this real-world study of SC semaglutide use by patients with MASH, half of the patients reached a dosage of 2.4 mg/week, and less than a third of patients remained persistent on therapy for 72 weeks regardless of SC semaglutide dosage. Persistence was poorer, and restarts were less common among patients prescribed only the brand approved for 2.4 mg/week dosing. Only 7.8% of patients prescribed the brand approved for 2.4 mg/week dosing reached a dosage of 2.4 mg/week within the first 16 weeks and sustained on that dosage for an additional 56 weeks. Non-persistence was slightly lower when 60-day and 90-day gap definitions were applied, but the overall trends were consistent. Treatment patterns among patients at risk for MASH were very similar to those among patients with MASH. This suggests that, in the real-world setting, patients may struggle to adhere to and maintain the dosing regimen that was associated with liver-related benefits in the ESSENCE trial, in which 83.5% of patients were able to maintain a dosage of 2.4 mg/week for the 72-week duration of the study.16
While this study was particularly interested in persistence on higher dosages of SC semaglutide, the findings are consistent with prior studies of GLP-1 RAs. Among US patients with type 2 diabetes, estimates of 12-month non-persistence ranged from 36% (135-day gap) to 52% (60-day gap), while estimates of 12-month non-persistence among patients with obesity and no type 2 diabetes ranged from 50% (135-day gap) to 68% (60-day gap).17–20 Notably, non-persistence was higher among patients with obesity compared to type 2 diabetes and among patients who initiated on the brand approved for 2.4 mg/week dosing compared to the brand approved for lower dosing.17,20 While these estimates of non-persistence are lower than those observed in this study, they also were measured over a shorter time period (52 weeks vs 72 weeks).
Notably, the real-world persistence observed in this study is substantially lower than the persistence observed in the clinical trial setting. In the interim analysis of the ESSENCE clinical trial, 88% of the 534 patients assigned to receive once-weekly subcutaneous semaglutide were on treatment at the end of the 72-week follow-up period.16 However, it has previously been shown that medication persistence is commonly lower in real-world practice compared to the clinical trial setting due to a variety of factors, including financial barriers, patient characteristics, and physician motivations.22
Limitations
One challenge with this analysis was that the pharmacy claims used to identify that a prescription was filled do not capture the treatment indication for which the medication is being prescribed, and the dosing recommendations for SC semaglutide vary by treatment indication. When the treatment indication is type 2 diabetes, the dosing schedule for SC semaglutide stops at the lowest dosage (0.5 mg/week to 2 mg/week) that achieves blood glucose control.14 In contrast, when the treatment indication is weight loss, the dosing schedule for SC semaglutide matches the schedule used in the ESSENCE clinical trial of SC semaglutide for the treatment of MASH.13 As the majority of patients in the SC Semaglutide cohort were prescribed the brand indicated for type 2 diabetes, the clinical intention was not to reach a dosage of 2.4 mg/week. While receipt of only the brand approved for 2.4 mg/week dosing was used as a proxy for determining the intended dosing schedule, real-world target dosages and titrations likely varied based on individual patient and prescriber decision-making. In addition, the sample size of patients with MASH taking only the brand approved for 2.4 mg dosing was relatively small, which makes the results subject to outliers; however, treatment patterns were similar among patients in the much larger cohort of patients at risk for MASH.
Other limitations of this study include those common to all studies that use routinely collected claims and EHR data that were not gathered for specific research purposes. These include data entry errors, missing data, and coding specificity limitations. This study included only patients with 124 weeks of continuous health insurance coverage, and the results may not be generalizable to patients with less stable insurance, without insurance, or with insurance types not included in the dataset, such as health coverage for military veterans. In addition, this analysis could not capture medication received from a compounding pharmacy, as these drugs are not assigned National Drug Codes, or medications that were paid for out-of-pocket. This may result in an overestimation of non-persistence. In addition, this study cannot confirm if the medications were used as prescribed, as patients may have dose reduced at home, which could result in both an overestimation of overall non-persistence and an underestimation of 2.4 mg/week dosage non-persistence. Treatment adherence has also been shown to vary by indication, as prior studies have shown that beliefs about necessity, which may differ by indication, influence treatment adherence.23–25 As the patients with MASH in this real-world study were receiving SC semaglutide treatment for the treatment of type 2 diabetes or obesity, these results may not be generalizable to patients who are prescribed SC semaglutide for the treatment of MASH rather than the treatment of its related comorbidities.
Furthermore, this analysis did not capture the reasons for stopping treatment, which could include side effects, lack of benefit, patient preference, changes to insurance benefits, physician advice, disruptions in supply, or other reasons. In addition, as this analysis was focused on SC semaglutide, switching to a different GLP-1 RA was defined as a discontinuation event. Lastly, BMI was measured among a mix of persistent and non-persistent patients, which may underestimate the efficacy of the therapy.
Conclusions
Long-term, real-world persistence on SC semaglutide was low among patients with MASH, particularly among those taking the highest dosage of SC semaglutide (2.4 mg/week). This suggests patients in a real-world setting may struggle to achieve and maintain the treatment regimen that was associated with the resolution of steatohepatitis and reduction in liver fibrosis in the interim results of the ESSENCE clinical trial.
Abbreviations
ALT, alanine aminotransferase; APRI, aspartate transaminase-to-platelet ratio index; AST, aspartate aminotransferase; BMI, body mass index; EHR, electronic health records; FIB-4, fibrosis-4; GLP-1 RA, glucagon-like peptide-1 receptor against; HbA1c, hemaglobin A1C; IQR, interquartile range; MASH, metabolic dysfunction-associated steatohepatitis; NFS, nonalcoholic fatty liver disease fibrosis score; SC, subcutaneous; SD, standard deviation.
Data Sharing Statement
The data that support the findings of this study were used under license from Veradigm and Komodo Health. Due to data use agreements and its proprietary nature, restrictions apply regarding the availability of the data. Further information is available from the corresponding author.
Ethics Approval and Informed Consent
The linked dataset only contains de-identified data as per the de-identification standard defined in Section §164.514(a) of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy Rule. The process by which the data is de-identified is attested to through a formal determination by a qualified expert as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule. Because this study used only de-identified patient records, it is therefore no longer subject to the HIPAA Privacy Rule and is therefore exempt from Institutional Review Board approval and for obtaining informed consent according to US law. This study was conducted in compliance with the Declaration of Helsinki and used only de-identified data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Madrigal Pharmaceuticals.
Disclosure
T Ryan, N Zeng, JP Winer-Jones, and M Bonafede are employees of Veradigm, which received fees from Madrigal Pharmaceuticals related to this work. Y Kim, F Lobo, and J O’Donnell are employees of Madrigal Pharmaceuticals. The authors report no other conflicts of interest in this work.
References
1. Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023;78(6):1966. doi:10.1097/HEP.0000000000000520
2. Sheka AC, Adeyi O, Thompson J, Hameed B, Crawford PA, Ikramuddin S. Nonalcoholic steatohepatitis: a review. JAMA. 2020;323(12):1175–1183.
3. Bril F, Sanyal A, Cusi K. Metabolic syndrome and its association with nonalcoholic steatohepatitis. Clin Liver Dis. 2023;27(2):187–210. doi:10.1016/j.cld.2023.01.002
4. Godoy-Matos AF, Silva Júnior WS, Valerio CM. NAFLD as a continuum: from obesity to metabolic syndrome and diabetes. Diabetol Metab Syndr. 2020;12(1):60. doi:10.1186/s13098-020-00570-y
5. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi:10.1016/j.jhep.2019.06.021
6. Quek J, Chan KE, Wong ZY, et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2023;8(1):20–30. doi:10.1016/S2468-1253(22)00317-X
7. Tapper EB, Bonafede M, Fishman J, et al. Healthcare resource utilization and costs of care in the United States for patients with non-alcoholic steatohepatitis. J Med Econ. 2023;2023:1–14. doi:10.1080/13696998.2023.2184967
8. Koutoukidis DA, Koshiaris C, Henry JA, et al. The effect of the magnitude of weight loss on non-alcoholic fatty liver disease: a systematic review and meta-analysis. Metabolism. 2021;115:154455. doi:10.1016/j.metabol.2020.154455
9. Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, et al. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology. 2015;149(2):367–378.e5. doi:10.1053/j.gastro.2015.04.005
10. European Association for the Study of the Liver (EASL). European Association for the Study of Diabetes (EASD), European Association for the Study of Obesity (EASO). EASL-EASD-EASO clinical practice guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). Obesity Facts. 2024;17(4):374–443. doi:10.1159/000539371.
11. Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. AASLD practice guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023;77(5):1797–1835. doi:10.1097/HEP.0000000000000323
12. Cusi K, Isaacs S, Barb D, et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the diagnosis and management of nonalcoholic fatty liver disease in primary care and endocrinology clinical settings: co-sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr Pract. 2022;28(5):528–562. doi:10.1016/j.eprac.2022.03.010
13. Novo Nordisk Inc. WEGOVY (Semaglutide) Injection, for Subcutaneous Use. U.S. Food and Drug Administration Website. Available from: https://www.Accessdata.Fda.Gov/Drugsatfda_docs/Label/2025/215256s024lbl.Pdf.
14. Novo Nordisk Inc. OZEMPIC (Semaglutide) Injection, for Subcutaneous Use. U.S. Food and Drug Administration Website. Available from: https://Www.Accessdata.Fda.Gov/Drugsatfda_docs/Label/2017/209637lbl.Pdf.
15. Pantanetti P, Cangelosi G, Alberti S, et al. Changes in body weight and composition, metabolic parameters, and quality of life in patients with type 2 diabetes treated with subcutaneous semaglutide in real-world clinical practice. Front Endocrinol. 2024:15. doi:10.3389/fendo.2024.1394506.
16. Sanyal AJ, Newsome PN, Kliers I, et al. Phase 3 trial of semaglutide in metabolic dysfunction–associated steatohepatitis. N Engl J Med. 2025;2025:1. doi:10.1056/NEJMoa2413258
17. Do D, Lee T, Peasah SK, Good CB, Inneh A, Patel U. GLP-1 receptor agonist discontinuation among patients with obesity and/or type 2 diabetes. JAMA Netw Open. 2024;7(5):e2413172. doi:10.1001/jamanetworkopen.2024.13172
18. Weiss T, Carr RD, Pal S, et al. Real-world adherence and discontinuation of glucagon-like peptide-1 receptor agonists therapy in type 2 diabetes mellitus patients in the United States. Patient Prefer Adherence. 2020;14:2337–2345. doi:10.2147/PPA.S277676
19. Polonsky WH, Arora R, Faurby M, Fernandes J, Liebl A. Higher rates of persistence and adherence in patients with type 2 diabetes initiating once-weekly vs daily injectable glucagon-like peptide-1 receptor agonists in US clinical practice (STAY study). Diabetes Ther. 2022;13(1):175–187. doi:10.1007/s13300-021-01189-6
20. Gleason PP, Urick BY, Marshall LZ, Friedlander N, Qiu Y, Leslie RS. Real-world persistence and adherence to glucagon-like peptide-1 receptor agonists among obese commercially insured adults without diabetes. J Manag Care Spec Pharm. 2024;30(8):860–867. doi:10.18553/jmcp.2024.23332
21. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for Reporting Observational Studies. PLoS Med. 2007;4(10):e296. doi:10.1371/journal.pmed.0040296
22. Andrade SE, Walker AM, Gottlieb LK, et al. Discontinuation of antihyperlipidemic drugs--do rates reported in clinical trials reflect rates in primary care settings? N Engl J Med. 1995;332(17):1125–1131. doi:10.1056/NEJM199504273321703
23. Schüz B, Marx C, Wurm S, et al. Medication beliefs predict medication adherence in older adults with multiple illnesses. J Psychosom Res. 2011;70(2):179–187. doi:10.1016/j.jpsychores.2010.07.014
24. Foot H, La Caze A, Gujral G, Cottrell N. The necessity–concerns framework predicts adherence to medication in multiple illness conditions: a meta-analysis. Patient Educ Couns. 2016;99(5):706–717. doi:10.1016/j.pec.2015.11.004
25. DiMatteo MR, Haskard KB, Williams SL. Health beliefs, disease severity, and patient adherence: a meta-analysis. Med Care. 2007;45(6):521–528. doi:10.1097/MLR.0b013e318032937e
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pro-Neurotensin as a Potential Novel Diagnostic Biomarker for Detection of Nonalcoholic Fatty Liver Disease
Mohamed AA, Abo-Elmatty DM, Ezzat O, Mesbah NM, Ali NS, Abd El Fatah AS, Alsayed E, Hamada M, Hassnine AA, Abd-Elsalam S, Abdelghani A, Hassan MB, Fattah SA
Diabetes, Metabolic Syndrome and Obesity 2022, 15:1935-1943
Published Date: 22 June 2022
Statin Monotherapy Not Inferior to Aspirin or Combined Aspirin and Statins Reducing the Incidences of Cirrhosis, HCC, and Mortality in MAFLD/MASH Patients: A Population Cohort Study
Lee CH, Huang YH, Hsu TJ, Yen TH, Hsieh SY
International Journal of General Medicine 2024, 17:6495-6511
Published Date: 27 December 2024
A Review of the Therapeutic Potential of Ginseng and Its Bioactive Components in Nonalcoholic Fatty Liver Disease
Hao L, Li S, Li C, Zhang Z, Hu X, Yan H
Drug Design, Development and Therapy 2025, 19:83-96
Published Date: 8 January 2025
Exploring Mechanisms of Lang Qing Ata in Non-Alcoholic Steatohepatitis Based on Metabolomics, Network Pharmacological Analysis, and Experimental Validation

Li S, Zhu H, Zhai Q, Hou Y, Yang Y, Lan H, Jiang M, Xuan J
Drug Design, Development and Therapy 2025, 19:1681-1701
Published Date: 11 March 2025
Serum LEAP2 Levels Across the Spectrum of Metabolic Dysfunction-Associated Fatty Liver Disease: A Potential Noninvasive Biomarker for Severity Stratification
Huang X, Deng Z, Li X, Yan S, Zhong K, Yuan F, Liu L, Deng C, Liu T, Zhao R, Buhe A, Li T, Zhao H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2439-2450
Published Date: 22 July 2025