Back to Journals » Infection and Drug Resistance » Volume 16
Retrospective Analysis of Sensitivity Characteristics of Enterobacteriaceae: A Study Based on Specimen Types, Sex, and Age Bracket of Patients
Authors Wen H, Xie S, Liu Y, Liang Y, Zhang P, Wang X, Li J ![]()
Received 13 December 2022
Accepted for publication 16 March 2023
Published 27 March 2023 Volume 2023:16 Pages 1753—1765
DOI https://doi.org/10.2147/IDR.S401341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Hainan Wen,1 Shoujun Xie,1 Yanchao Liu,1 Yueyi Liang,1 Pan Zhang,1 Xiaohui Wang,1 Jianhui Li2
1Department of Clinical Laboratory, Affiliated Hospital of Chengde Medical University, Chengde, Hebei, People’s Republic of China; 2Department of Preventive Medicine, Chengde Medical University, Chengde, Hebei, People’s Republic of China
Correspondence: Jianhui Li, Email [email protected]
Objective: Enterobacteriaceae have displayed widespread trends of antimicrobial resistance in recent years. Therefore, we aimed to analyse the antimicrobial susceptibility of common bacteria and explore the significance in treatment and research of infections induced by Enterobacteriaceae.
Methods: We retrospectively analysed 10,775 antimicrobial susceptibility test results acquired over a 6-year period in the affiliated hospital of Chengde Medical University. We divided the data based on specimen type (blood, sputum, pus, or urine), and population characteristics (age bracket and sex) for analysis. We mainly analysed the antimicrobial susceptibility of Escherichia coli (Eco), Klebsiella pneumoniae (Kpn), and Enterobacter cloacae (Ecl).
Results: In our study, it was found that the resistance rates of Eco, Kpn, and Ecl to most antimicrobial agents were significantly different (P < 0.05) on specimen type and age bracket. The Eco from sputum had the highest resistance rates except ciprofloxacin (CIP), levofloxacin (LVX), and gentamicin (GEN); the Kpn from urine had the highest resistance rates to all antimicrobial agents; the Ecl from urine had the highest resistance rates to most antimicrobial agents. The Eco from geriatric patients had the highest resistance rates except GEN and SXT; the Kpn from adult patients had the lowest resistance rates to most antimicrobial agents except LVX. The Eco isolated from males had higher resistance rates to most antimicrobial agents except CIP, LVX, and NIT than those isolated from females; the Kpn showed significant differences in antimicrobial susceptibility to only 5 out of 22 antimicrobial agents (P < 0.05); the Ecl showed significant differences in susceptibility only to two antimicrobial agents, LVX and TOB (P < 0.01).
Conclusion: The antimicrobial susceptibility of Enterobacteriaceae was significantly different among specimen type, age bracket and sex of patients, which is of great significance for the treatment and research of infection.
Keywords: Enterobacteriaceae, antimicrobial sensitivity, drug resistance, specimen type, infection
Introduction
Enterobacteriaceae consists of a large group of Gram-negative bacilli with similar morphology and biological characteristics, which widely exist in the environment. They are also part of the normal intestinal flora of humans and animals. Enterobacteriaceae are common bacteria that cause community and healthcare-related infections and are particularly important in the context of antimicrobial resistance.1 With time and the widespread use of antimicrobial, Enterobacteriaceae have evolved to develop resistance to antimicrobial.2 According to the Center for Disease Control’s (CDC) description of the antimicrobial-resistant pathogens, Klebsiella species, E. coli, and Enterobacter species are the most crucial emerging resistance threats worldwide, especially their carbapenem-resistant strains.3
Carbapenem-resistant strains were initially reported in the 1980s and rapidly spread worldwide.4 According to epidemiological data, different carbapenemase-producing Enterobacteriaceae are becoming more prevalent in different parts of the world. Bacterial infections caused by carbapenem-resistant Enterobacteriaceae (CRE), which are resistant to all classes of current antimicrobial agents, have become a serious challenge in the fight against bacterial infections in public health.5–7 In the past 20 years, CRE has spread rapidly worldwide, leading to the rise of antimicrobial resistance. It is not clear whether the CRE was primitive or evolved to be resistant against antimicrobial. Based on the theory of biological evolution, the application of antimicrobial is an important factor in the formation of CRE. As a result, infections caused by CRE would spread, hospital admissions would become longer, thereby increasing economic and social expenses, and mortality would rise.8 A study in the United States (US) from 2011 to 2014 found that 10% of Klebsiella pneumoniae are resistant to carbapenems, and 16–36% of E. coli are resistant to third-generation cephalosporins.9 A European study found that, in clinical cases, the percentage of K. pneumoniae resistant to third-generation cephalosporins was 31%, and that of E. coli resistant to carbapenems and third-generation cephalosporins was 8% and 12%, respectively.10 The Greek System for Antibiotic Resistant Research showed that the carbapenem resistance rate was 1% in 2001; however, by 2008 this rate increased to 30% in hospital wards and 60% in intensive care units.11 According to the China Bacterial antimicrobial resistance Monitoring Network (CHINET), in 2005 the isolation rate of CRE was only 2.1%; however, it increased to 11.4% in 2019. The resistance rates of K. pneumoniae to imipenem (IPM) and meropenem (MEM) increased from 3.0% and 2.9% in 2005 to 25.3% and 26.8% in 2019, respectively.12 This indicated that the antimicrobial resistance rate of K. pneumoniae increased with the increase in number of isolated antimicrobial-resistant strains.
To survive the action of antimicrobial, bacteria constantly search for new strategies, called “resistance mechanisms”. Bacteria evolve to produce specific proteins that determine their resistance mechanisms. Over time, bacterial resistance mechanisms may change, leading to more resistant infections, and antibiotic-resistant bacteria can share their resistance genes with other bacteria that have not been exposed to antimicrobial. Enterobacteriaceae can often develop one or more resistance genes against effective antimicrobial. The main mechanisms of antimicrobial resistance in Enterobacteriaceae include the synthesis of carbapenemase enzymes, extended-spectrum beta-lactamases (ESBLs), AmpC enzymes, and porin loss, which reduces drug permeability.13 Common enzymes in resistant strains are K. pneumoniae carbapenemase, imipenem’s metallo-beta-lactamase, New Delhi metallo-beta-lactamase (NDM), Verona integron-encoded metallo-beta-lactamase, which are among the most important acquired resistances.14 This means that once bacteria carry multiple resistance genes, treating infections and developing antimicrobial are a huge challenge.
With the increased detection rate of CRE, carbapenem antimicrobial are not the most effective barrier to infection. Therefore, in addition to developing novel antimicrobial agents, healthcare workers should strengthen their awareness of monitoring and analysing bacterial resistance, use infection control and antimicrobial management strategies, and stop chains of transmission. This should be part of a proactive approach to tackling antimicrobial resistance at the regional, national, and international levels.15
Methods
Test Methods and Data Collection
A retrospective analysis was performed between July 2016 and December 2021 on clinical specimens from patients treated at the Affiliated Hospital of Chengde Medical University, a 2500-bed tertiary-care hospital in China. We collected patients’ clinical data using the hospital’s laboratory information system. Specimens from patients suspected of having an infection were collected in accordance with the hospital’s specimen collection manual. Positive blood cultures and other samples were plated on blood agar, eosin methylene blue, and chocolate agar (Biokont, Wenzhou, China), and incubated at 35°C with 5% CO2 for 18–24 h. Pure colonies on solid media were identified using matrix-assisted laser desorption/ionisation time of flight mass spectrometry (bioMérieux, Paris, France) according to the manufacturer’s instructions. During the study period, antimicrobial susceptibility testing was performed for all isolates from each specimen using VITEK 2 automated systems (bioMérieux, Paris, France) AST-GN09 cards and E-test strips according to the Clinical and Laboratory Standards Institute guideline breakpoints.16 The types of antimicrobial agents include ampicillin, piperacillin, amoxicillin-clavulanic acid, ampicillin-sulbactam, piperacillin-tazobactam, aztreonam, imipenem, meropenem, ciprofloxacin, levofloxacin, gentamicin, tobramycin, cefazolin, cefuroxime, ceftazidime, ceftriaxone, cefotaxime, cefepime, cefoxitin, nitrofurantoin, sulfamethoxazole-trimethoprim. E. coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853, and K. pneumoniae ATCC BAA-1705 (American Type Culture Collection) were used as the quality control strains to ensure the quality of the procedure.
Statistical Analysis
The trend tests were performed by linear-by-linear combinations using SPSS (version 19.0). Trend bar charts were made using Origin (version 8.5). The differences in specimen type, and age bracket and sex of patients among Enterobacteriaceae, including E. coli, K. pneumoniae, and E. cloacae, were analysed using R × C chi-square test.
Results
A total of 10,755 strains of clinical Enterobacteriaceae were isolated, including E. coli (5,08 strains, 50.28%), K. pneumoniae (3034 strains, 28.21%), E. cloacae (711 strains, 6.61%), Proteus mirabilis (483 strains, 4.49%), Klebsiella oxytoca (312 strains, 2.9%), Serratia marcescens (205 strains, 1.91%), and others (602 strains, 5.6%).
In our study, we analysed data on susceptibility of Enterobacteriaceae to common antimicrobial agents from 2016 to 2021. We found that the antimicrobial agents against which Enterobacteriaceae demonstrated decreased resistance rates included ampicillin (AMP: 88.73%~82.21%), amoxicillin-clavulanic acid (AMC: 31.21%~13.62%), cefazolin (CZO:64.19%~53.62%), cefuroxime (CXM: 55.93%~50.55%), and ceftriaxone (CRO: 50.19%~45.66%), and those against which an increased antimicrobial resistance rate was observed included imipenem (IPM:2.41%~6.07%), meropenem (MEM: 2.22%~5.75%) (Figure 1). Furthermore, we analysed the trend of antimicrobial resistance rate from 2016 to 2021 and found that although the antimicrobial resistance rate of some antimicrobial increased or decreased, only the trend change of IPM and MEM showed a significant difference (Table 1).
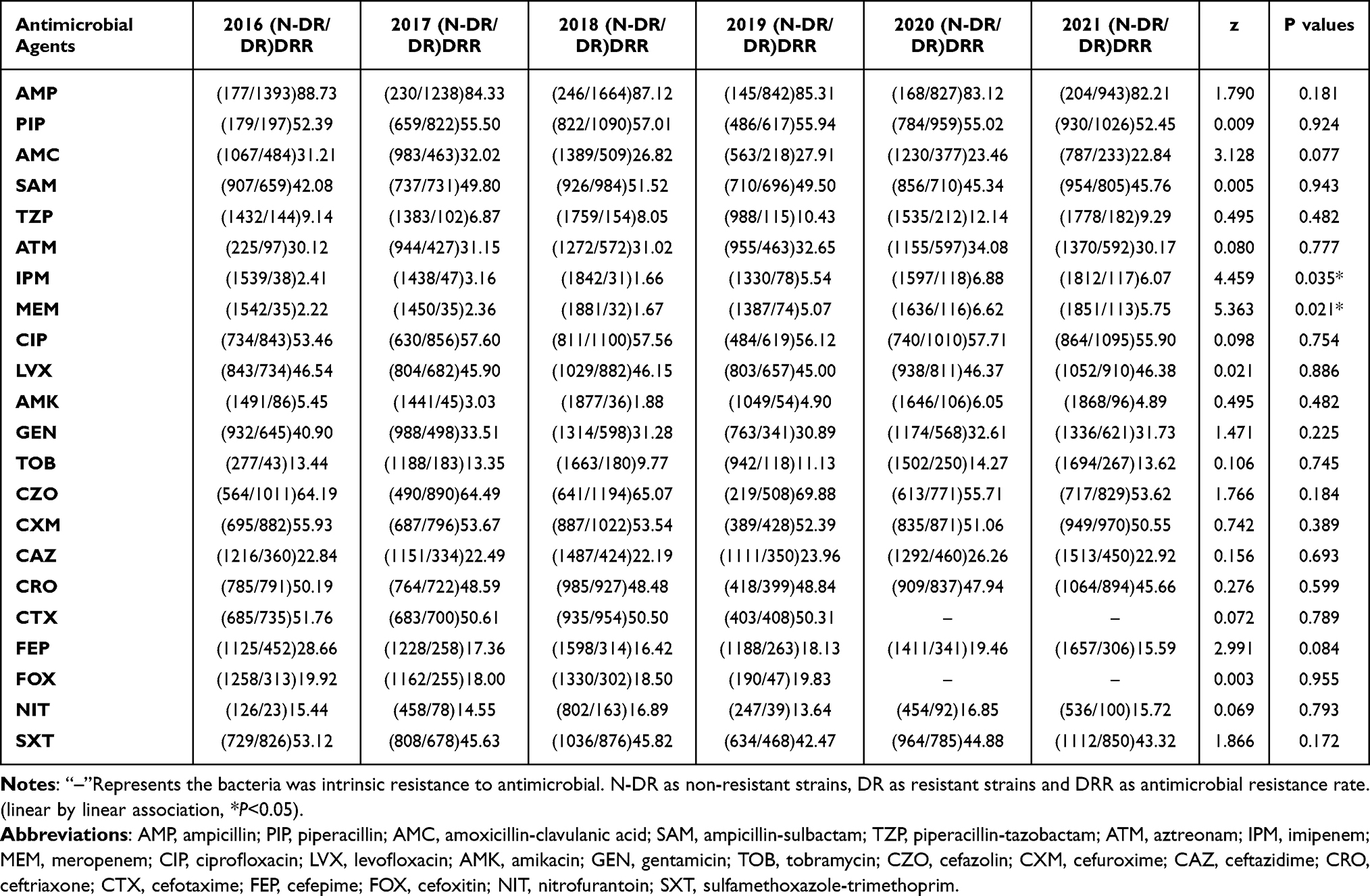 |
Table 1 Trends in Antimicrobial Resistance Rates of Enterobacteriaceae from 2016 to 2021 |
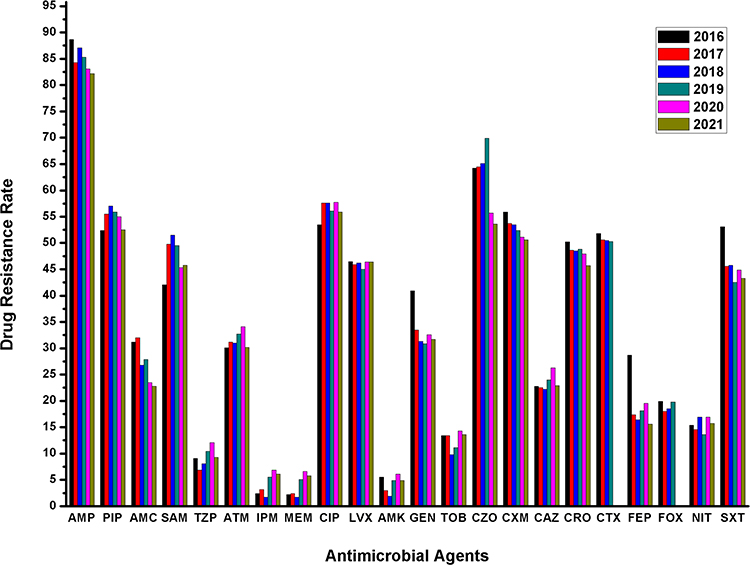 |
Figure 1 Changes in resistance rates of Enterobacteriaceae to common antimicrobial agents from 2016 to 2021. Abbreviations: AMP, ampicillin; PIP, piperacillin; AMC, amoxicillin-clavulanic acid; SAM, ampicillin-sulbactam; TZP, piperacillin-tazobactam; ATM, aztreonam; IPM, imipenem; MEM, meropenem; CIP, ciprofloxacin; LVX, levofloxacin; AMK, amikacin; GEN, gentamicin; TOB, tobramycin; CZO, cefazolin; CXM, cefuroxime; CAZ, ceftazidime; CRO, ceftriaxone; CTX, cefotaxime; FEP, cefepime; FOX, cefoxitin; NIT, nitrofurantoin; SXT, sulfamethoxazole-trimethoprim. |
We compared our antimicrobial resistance data of the top three bacteria among Enterobacteriaceae with that from the CHINET. The antimicrobial resistance rates was different from those reported by CHINET (2016–2020); However, the trend of antimicrobial resistance were similar. We emphatically analysed the antimicrobial resistance trends of top three bacteria, which had obvious differences in antimicrobial agent sensitivity. However, the trend of resistance against cefepime (FEP), a fourth-generation cephalosporin, was significantly different and the antimicrobial resistance rate decreased every year. These findings indicated that carbapenem-resistant E. coli was not prevalent in China or in a hospital. For K. pneumoniae, we found that the resistance to IPM and MEM increased significantly, which has the same trend as in the national antimicrobial resistance data. These findings indicated that carbapenem-resistant K. pneumoniae has increased in recent years, and aminoglycoside-resistant strains have also increased. We found that the sensitivity of E. cloacae to IPM and MEM also increased significantly, which has the same trend as in the national antimicrobial resistance data. Therefore, through the analysis of antimicrobial resistance of the above three kinds of bacteria and comparison with the national antimicrobial resistance data, we found that the detection rate of CRE is increasing every year; however, there are great differences between different bacterial species.(Figure 2, data are shown in Supplementary Table).
 |
Figure 2 Changes in resistance rates of E.coli, K. pneumoniae and E.cloacae to common antimicrobial agents from 2016 to 2021. (A and B) Resistance rates of E.coli, (C and D) Resistance rates of K.pneumoniae, (E and F) Resistance rates of E.cloacae. (A, C and E) Resistance rates from CHINET, (B, D and F) Resistance rates from Affiliated Hospital of Chengde Medical University. Abbreviations: AMP, ampicillin; PIP, piperacillin; AMC, amoxicillin-clavulanic acid; SAM, ampicillin-sulbactam; TZP, piperacillin-tazobactam; ATM, aztreonam; IPM, imipenem; MEM, meropenem; CIP, ciprofloxacin; LVX, levofloxacin; AMK, amikacin; GEN, gentamicin; TOB, tobramycin; CZO, cefazolin; CXM, cefuroxime; CAZ, ceftazidime; CRO, ceftriaxone; CTX, cefotaxime; FEP, cefepime; FOX, cefoxitin; NIT, nitrofurantoin; SXT, sulfamethoxazole-trimethoprim. |
To further explore the factors influencing Enterobacteriaceae susceptibility to antimicrobial agents, we analysed the susceptibility of all Enterobacteriaceae to antimicrobial agents from 2016 to 2021, based on various dimensions, such as specimen type, and age bracket and sex of the patients.
For the specimen type, we found that Enterobacteriaceae isolated from blood, sputum, pus, and urine showed significant differences in response to all antimicrobial agents (Table 2). We retrospectively analysed the differences in antimicrobial susceptibility of E. coli, K. pneumoniae, and E. cloacae from different specimen types. E. coli showed significant differences in susceptibility to all antimicrobial agents (P < 0.01) except gentamicin (GEN). E. coli from sputum had the highest resistance rates to most antimicrobial agents except ciprofloxacin (CIP), levofloxacin (LVX), and GEN, whereas those from pus had the lowest resistance rates to most antimicrobial agents except CIP, LVX, and GEN. K. pneumoniae showed significant differences in the susceptibility to all antimicrobial agents (P < 0.01). After comparing the antimicrobial resistance rates of K. pneumoniae isolated from different specimens, we found K. pneumoniae from urine had the highest resistance rates to all antimicrobial agents, whereas those from pus had the lowest resistance rates. Enterobacter cloacae showed significant differences in the susceptibility to most antimicrobial agents (P < 0.01) except AMK and NIT. We found that the E. cloacae from urine had the highest resistance rates to most antimicrobial agents, except AMK, GEN, TOB, and NIT, whereas the E. cloacae from pus had the lowest resistance rates to most antimicrobial agents, except NIT and sulfamethoxazole-trimethoprim (SXT).
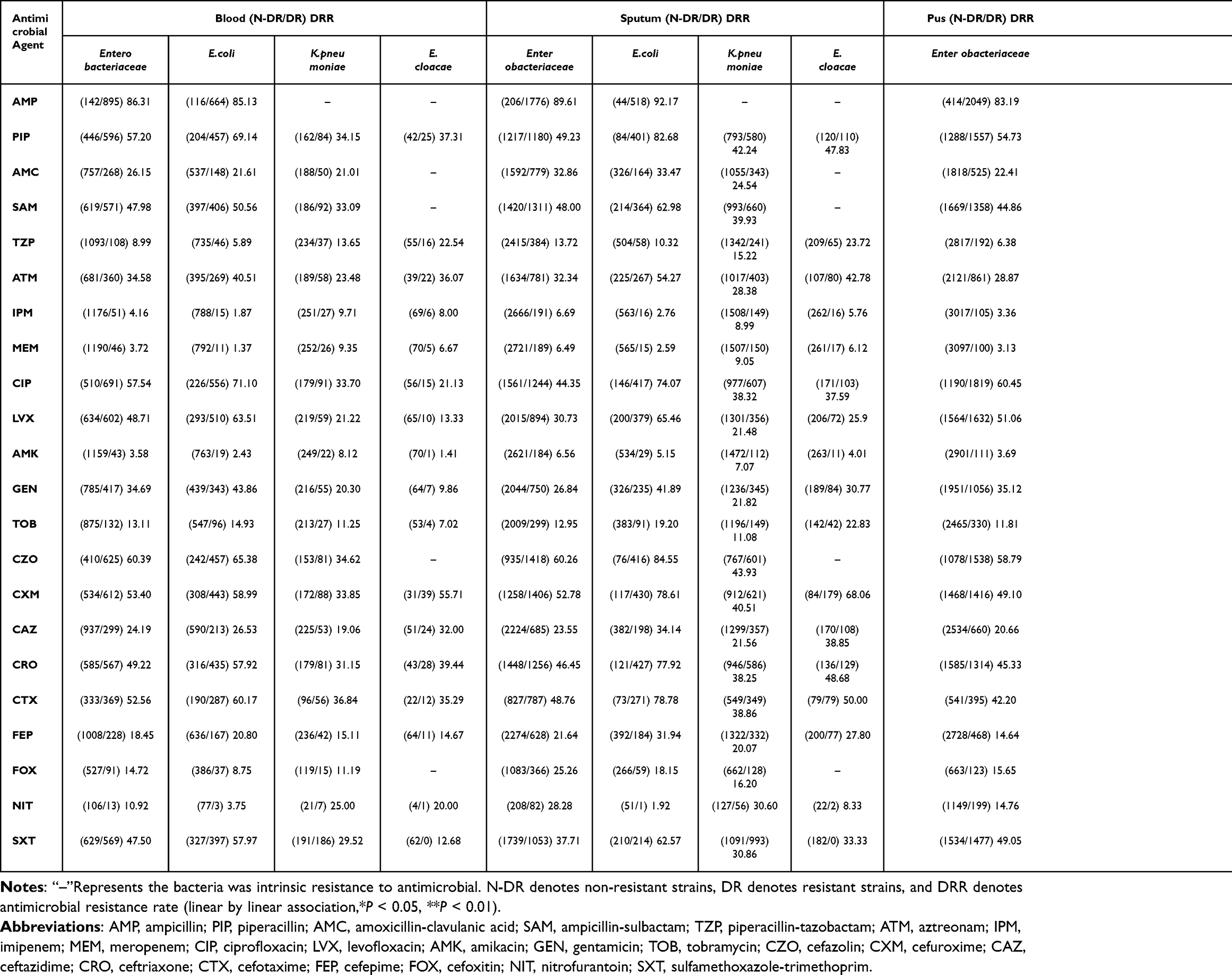 |
Table 2 Differences in Antimicrobial Susceptibility of Enterobacteriaceae, E.coli, K.pneumoniae and E.cloacae Isolated from Different Specimens |
Regarding the age bracket, we found that Enterobacteriaceae isolated from paediatric, adult, and geriatric patients showed significant differences in response to most antimicrobial agents except NIT and SXT. Simultaneously, we retrospectively analysed the differences in antimicrobial susceptibility of E. coli, K. pneumoniae, and E. cloacae. E. coli showed significant differences in the susceptibility to the following antimicrobial agents (P < 0.05): AMC, SAM, piperacillin-tazobactam (TZP), ATM, CIP, LVX, AMK, CXM, ceftazidime (CAZ), CRO, CTX, FEP, cefoxitin (FOX), and SXT. E. coli from geriatric patients had the highest resistance rates to most antimicrobial agents except GEN and SXT, whereas those from paediatric patients had the lowest resistance rates to most antimicrobial agents except PIP, AMC, GEN, CZO, and SXT. K. pneumoniae showed significant differences in the susceptibility to all antimicrobial agents (P < 0.01). K. pneumoniae from adult patients had the lowest resistance rates to most antimicrobial agents except LVX, whereas those from paediatric and geriatric patients almost had the highest resistance rates to all antimicrobial agents. E. cloacae showed significant differences in the susceptibility to most antimicrobial agents (P < 0.05) except IPM, AMK, and CXM. In contrast to the antimicrobial resistance rates of E. cloacae, those of E. coli and K. pneumoniae were not visibly related to the age bracket of the patients (Table 3).
 |
Table 3 Differences in Antimicrobial Susceptibility of Enterobacteriaceae, E.coli, K.pneumoniae and E.cloacae Isolated from Patients of Different Age Brackets |
Regarding the sex, we found significant differences between Enterobacteriaceae isolated from males and females in response to almost antimicrobial agents except CRO (P < 0.05). We retrospectively analysed the differences in antimicrobial susceptibility of E. coli, K. pneumoniae, and E. cloacae. E. coli showed significant differences in susceptibility to most antimicrobial agents (P < 0.01). In the comparison of the antimicrobial resistance rates of E. coli isolated from males and females, the E. coli isolated from males had higher resistance rates to most antimicrobial agents except CIP, LVX, and NIT than those isolated from females. K. pneumoniae showed significant differences in antimicrobial susceptibility to only 5 out of 22 antimicrobial agents (P < 0.05). Although there were no significant differences in susceptibility to most antimicrobial based on the sex of the patients, the resistance rates to all antimicrobial were slightly higher in strains isolated from males than in those from females. E. cloacae showed significant differences in susceptibility only to two antimicrobial agents, LVX and TOB (P < 0.01). In the comparison with the antimicrobial resistance rates of E. cloacae, we did not find differences in antimicrobial resistance rates (Table 4).
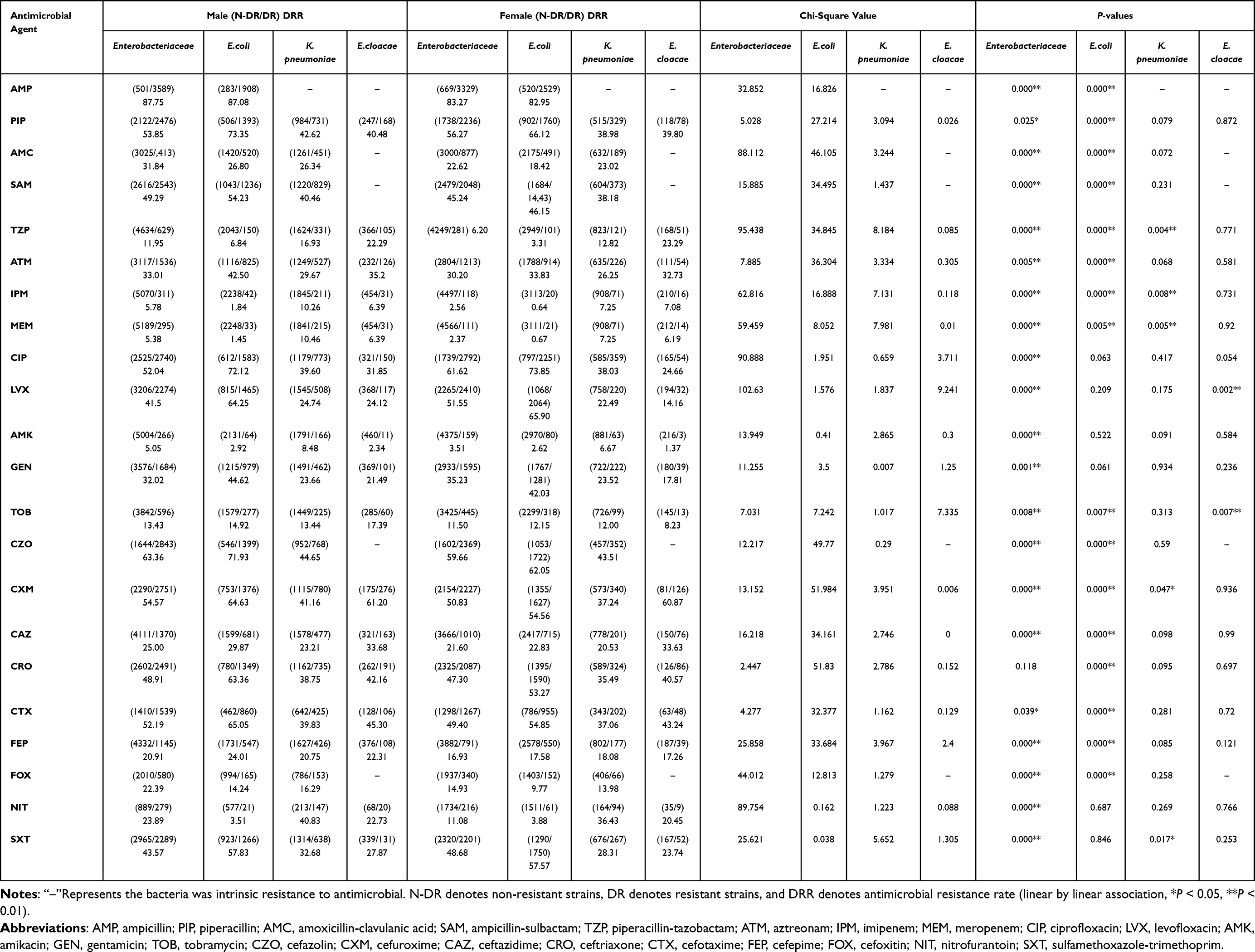 |
Table 4 Differences in Antimicrobial Susceptibility of Enterobacteriaceae, E.coli, K.pneumoniae and E.cloacae Isolated from Patients of Different Sex |
Discussion
In this study, we analysed the antimicrobial susceptibility data of Enterobacteriaceae-related infections from 2016 to 2021 that expounded its antimicrobial susceptibility trends in recent years in Affiliated Hospital of Chengde Medical University, which were different from those reported in national data.12,17–20 The antimicrobial susceptibility trends of Enterobacteriaceae observed in our study is generally consistent with those in China, which indicates that the results truly reflect the epidemic status of Enterobacteriaceae in recent years. However, the results indicate a challenge for medical workers working on infection-related issues. According to the US CDC report on antibiotic resistance, 131,900 cases infected by ESBL-producing Enterobacteriaceae were estimated in 2013, whereas 197,400 cases were estimated in 2019. In 2013, 118,00 cases infected by CRE were estimated, whereas 13,100 cases were estimated in 2019.3 K. pneumoniae and E. cloacae showed increasing resistance to carbapenems and β-lactam antimicrobial such as IPM, MEM, SAM, TZP, and ATM every year. This indicates that the carbapenem-resistant strains have caused an increase in infections in recent years, which is a major challenge to fight. One relatively good news is that the susceptibility of E. coli to most antimicrobial agents has remained stable in recent years.
In the retrospective study, although the trend of antimicrobial resistance was similar in different regions of China, the resistance rate of bacteria belonging to the same genus varied greatly between different hospitals and regions. We speculate that the difference in bacterial resistance rate between hospitals may be related to differences in the administration of antimicrobial and endemic strains in the area. Nevertheless, there is no denying that the increase in infections caused by resistant strains is a serious issue.
In our further analysis, we found an interesting phenomenon of obvious differences in the susceptibility of bacteria to antimicrobial agents depending on specimen type, and age bracket and sex of the patients, which has rarely been reported in literature.
Further analysis found that Enterobacteriaceae showed significant differences in antimicrobial resistance based on specimen type. In general, the spectrum of bacterial infections in one hospital or region should be similar; however, the antimicrobial susceptibility of bacteria causing infections in different sites vary greatly. A study in Taiwan21 found that the rates of isolated ESBL-producing E. coli and K. pneumoniae from sputum and urine were higher than those from blood. This indicates that Enterobacteriaceae isolated from urine and sputum specimens have higher antimicrobial resistance. This is consistent with a part of our findings, because only K. pneumoniae isolated from urine specimens had a high antimicrobial resistance rate in our study. However, the antimicrobial resistance rate of E. coli isolated from sputum was higher than that of the above research. We did not analyse the resistance genes of antimicrobial-resistant strains, and ESBL is only a part of the resistance mechanism. However, we hypothesised that this might be related to the infection of specific sites caused by bacteria with certain antimicrobial-resistance genes and the distribution and accumulation concentration of antimicrobial agents in the body.
It is well known that the human body has differences in immunity at different age brackets, and it can rely on its own immune system to resist bacterial infections. Antimicrobial are external interventions provided to fight infections when the immune capacity of the body is insufficient. We found that Enterobacteriaceae showed great differences in antimicrobial susceptibility based on the age bracket of the patients from whom they are isolated. However, a similar significant difference in resistance rates was not observed for E. cloacae. In a previous study,22 older women (aged > 65 years) were reported to have E. coli with higher resistance rates to AMP, CIP, and co-trimoxazole. The increasing resistance of Enterobacteriaceae is often associated with the higher use of antimicrobial.23,24 Although we did not analyse medication management of infections caused by Enterobacteriaceae, our results show that paediatric patients have strains with the highest rates of resistance to certain antimicrobial agents, suggesting that antimicrobial resistance is not only related to the amount of drug used. In our findings, E. coli and K. pneumoniae isolated from adults had the lowest antimicrobial resistance to most antimicrobial agents. Another study showed that adding pentoxifylline to antimicrobial in murine neonatal sepsis promoted an anti-inflammatory milieu through the inhibition of plasma tumour necrosis factor and the enhancement of interleukin 10 production in the plasma and organs without increasing bacterial growth.25 This is more likely to be related to the immune system.
We initially predicted that there might be differences in antimicrobial susceptibility based on the dimension of sex of the patients, which was confirmed by our results. However, the differences in antimicrobial susceptibility based on sex of the patients is more obvious in E. coli; the antimicrobial resistance rates of strains isolated from males was significantly higher than those of strains isolated from females. A study of antimicrobial susceptibility based on sex of the patients from whom the specimen was isolated showed that the susceptibility to most antimicrobial agents of strains isolated from males was significantly higher than those of strains isolated from females. Further, E. coli showed sensitivity differences to most antimicrobial agents based on sex of the patients.26 Another study showed that E. coli strains isolated from male patients were more resistant to antimicrobial agents.27 Currently, there is no study regarding the mechanism of this aspect; however, we speculate that there must be internal and external factors influencing this difference. On the one hand, the difference in hormones between males and females leads to differences in their antimicrobial environment; on the other hand, it may be related to the individual differences in the use of antimicrobial agents.
In conclusion, the antimicrobial susceptibility of Enterobacteriaceae was significantly different among specimen type, age bracket and sex of patients. The antimicrobial susceptibility observed in our study is in line with the current infection situation. However, the antimicrobial resistance rate of one hospital or region should be the guidance for the rational use of drugs. Furthermore, the difference in bacterial susceptibility to antimicrobial means that it provides data basis for clinical rational drug use and further research on bacterial drug resistance.
Data Sharing Statement
All relevant data are within the manuscript. The data underlying the findings of this study, except the data on China’s bacterial antimicrobial resistance, are retained at the Affiliated Hospital of Chengde Medical University and will not be made openly accessible because of ethical and privacy concerns.
Ethical Approval Statement
Ethical approval from the Institutional Review Board of the Affiliated Hospital of Chengde Medical University. All the clinical samples were part of the routine hospital laboratory procedure and there was no additional burden on patients. We declare that our study complies with the Declaration of Helsinki.
Acknowledgments
This study was supported by the Natural Science Foundation of Chengde Medical University (grant nos. 201627).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no competing interests in this work.
References
1. van Duin D, Paterson DL. Multidrug-resistant bacteria in the community: trends and lessons learned. Infect Dis Clin North Am. 2016;30(2):377–390. doi:10.1016/j.idc.2016.02.004
2. o’malley PA. A most dangerous outbreak: New Delhi metallo-β-lactamase-1 carbapenemase-producing Enterobacteriaceae. Clin Nurse Spec. 2020;34(1):13–16. doi:10.1097/NUR.0000000000000497
3. Centres for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2019. US Department of Health and Human Services, Centres for Disease Control and Prevention; 2019.
4. vink JP, Otter JA, Edgeworth JD. Carbapenemase-producing Enterobacteriaceae - once positive always positive? Curr Opin Gastroenterol. 2020;36(1):9–16. doi:10.1097/MOG.0000000000000596
5. Magiorakos AP, Srinivasan A, Carey R, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
6. Goic-Barisic I, Seruga Music M, Kovacic A, Tonkic M, Hrenovic J. Pan drug-resistant environmental isolate of Acinetobacter baumannii from Croatia. Microb Drug Resist. 2017;23(4):494–496. doi:10.1089/mdr.2016.0229
7. li L, Yu T, Ma Y, et al. The genetic structures of an Extensively Drug Resistant (XDR) Klebsiella pneumoniae and its plasmids. Front Cell Infect Microbiol. 2019;8:446. doi:10.3389/fcimb.2018.00446
8. Lee C-M, Lai -C-C, Chiang H-T, et al. Presence of multidrug-resistant organisms in the residents and environments of long-term care facilities in Taiwan. J Microbiol Immunol Infect. 2017;50(2):133–144. doi:10.1016/j.jmii.2016.12.001
9. weiner L, Webb A, Limbago B, et al. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the national healthcare safety network at the centers for disease control and prevention, 2011–2014. Infect Control Hosp Epidemiol. 2016;37(11):1288–1301. doi:10.1017/ice.2016.174
10. Weist K, Högberg LD. ECDC publishes 2015 surveillance data on antimicrobial resistance and antimicrobial consumption in Europe. Eurosurveillance. 2016;21(46):30401. doi:10.2807/1560-7917.ES.2016.21.46.30399
11. Souli M, Galani I, Antoniadou A, et al. An outbreak of infection due to β-lactamaseࢭ Klebsiella pneumoniae carbapenemase 2–producing K. pneumoniae in a Greek university hospital: molecular characterization, epidemiology, and outcomes. Clin Infect Dis. 2010;50(3):364–373. doi:10.1086/649865
12. Hu F, Guo Y, Zhu D, et al. Anonymous. Monitoring of bacterial drug resistance in CHINET tertiary hospital in 2019. Chin J Infect Chemother. 2020;20(3):11.
13. Codjoe FS, Donkor ES. Carbapenem resistance: a review. Med Sci. 2018;6(1):1. doi:10.3390/medsci6010001
14. Nordmann P, Poirel L. The difficult-to-control spread of carbapenemase producers among Enterobacteriaceae worldwide. Clin Microbiol Infect. 2014;20(9):821–830. doi:10.1111/1469-0691.12719
15. Huttner A, Harbarth S, Carlet J, et al. Antimicrobial resistance: a global view from the 2013 world healthcare-associated infections forum. Antimicrob Resist Infect Control. 2013;2(1):1–13. doi:10.1186/2047-2994-2-31
16. Clinical and Laboratory Standards Institute. M100 Performance Standards for Antimicrobial Susceptibility Testing.
17. Hu F, Guo Y, Zhu D, et al. Anonymous. Monitoring of bacterial drug resistance in CHINET tertiary hospital in 2016. Chin J Infect Chemother. 2017;17(5):11. doi:10.16718/j.1009-7708.2017.05.001
18. Hu F, Guo Y, Zhu D, et al. Anonymous. Monitoring of bacterial drug resistance in CHINET tertiary hospital in 2017. Chin J Infect Chemother. 2018;18(3):11. doi:10.16718/j.1009-7708.2018.03.001
19. Hu F, Guo Y, Zhu D, et al. Anonymous. Monitoring of bacterial drug resistance in CHINET tertiary hospital in 2018. Chin J Infect Chemother. 2019;20(1):11. doi:10.16718/j.1009-7708.2020.01.001
20. Hu F, Guo Y, Zhu D, et al. Anonymous. Monitoring of bacterial drug resistance in CHINET tertiary hospital in 2020. Chin J Infect Chemother. 2021;21(4):11. doi:10.16718/j.1009-7708.2021.04.001
21. Liu HC, Hung YP, Lin HJ, et al. Antimicrobial susceptibility of clinical Enterobacteriaceae isolates at the emergency department in a regional hospital: a threat of extended spectrum beta-lactamase-producers among nursing home residents. J Microbiol Immunol Infect. 2016;49(4):584–590. doi:10.1016/j.jmii.2015.10.001
22. Gobernado M, Valdés L, Alós JI, et al. Spanish surveillance group for urinary pathogens. Antimicrobial susceptibility of clinical Escherichia coli isolates from uncomplicated cystitis in women over a 1-year period in Spain. Rev Esp Quimioter. 2007;20(1):68–76.
23. Sedláková MH, Urbánek K, Vojtová V, et al. Antibiotic consumption and its influence on the resistance in Enterobacteriaceae. BMC Res Notes. 2014;7:454. doi:10.1186/1756-0500-7-454
24. Joseph NM, Bhanupriya B, Shewade DG, et al. Relationship between antimicrobial consumption and the incidence of antimicrobial resistance in Escherichia coli and Klebsiella pneumoniae isolates. J Clin Diagn Res. 2015;9(2):DC08–DC12. doi:10.7860/JCDR/2015/11029.5537
25. Speer EM, Diago-Navarro E, Ozog LS, et al. A neonatal murine Escherichia coli sepsis model demonstrates that adjunctive pentoxifylline enhances the ratio of anti- vs. pro-inflammatory cytokines in blood and organ tissues. Front Immunol. 2020;11:577878. doi:10.3389/fimmu.2020.577878
26. Linhares I, Raposo T, Rodrigues A, et al. Frequency and antimicrobial resistance patterns of bacteria implicated in community urinary tract infections: a ten-year surveillance study (2000–2009). BMC Infect Dis. 2013;13(1):2000–2009. doi:10.1186/1471-2334-13-19
27. Chatterjee N, Ghosh RR, Chatterjee M, et al. Correlation of demographic profile and antibiotic resistance in patients with urinary tract infection attending a teaching hospital in Kolkata. J Med Sci Clin Res. 2014;2(11):2806–2816.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Differentiation Between Acinetobacter Baumannii Colonization and Infection and the Clinical Outcome Prediction by Infection in Lower Respiratory Tract
Feng DY, Zhou JX, Li X, Wu WB, Zhou YQ, Zhang TT
Infection and Drug Resistance 2022, 15:5401-5409
Published Date: 12 September 2022
Analysis of Characteristics, Pathogens and Drug Resistance of Urinary Tract Infection Associated with Long-Term Indwelling Double-J Stent
Li Y, Jiang L, Luo S, Hu D, Zhao X, Zhao G, Tang W, Guo Y
Infection and Drug Resistance 2023, 16:2089-2096
Published Date: 8 April 2023