Back to Journals » Journal of Pain Research » Volume 15
Restorative Neurostimulation: A Clinical Guide for Therapy Adoption
Authors Chakravarthy K, Lee D, Tram J, Sheth S, Heros R ![]() , Manion S, Patel V
, Manion S, Patel V ![]() , Kiesel K, Ghandour Y
, Kiesel K, Ghandour Y ![]() , Gilligan C
, Gilligan C ![]()
Received 10 March 2022
Accepted for publication 26 May 2022
Published 20 June 2022 Volume 2022:15 Pages 1759—1774
DOI https://doi.org/10.2147/JPR.S364081
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Krishnan Chakravarthy,1,2 David Lee,3 Jennifer Tram,1 Samir Sheth,4 Robert Heros,5 Smith Manion,6 Vikas Patel,7 Kyle Kiesel,8 Yousef Ghandour,9 Christopher Gilligan10
1Department of Anesthesiology and Pain Medicine, University of California San Diego Health Sciences, San Diego, CA, USA; 2VA San Diego Healthcare System, San Diego, CA, USA; 3Fullerton Orthopedic Surgery Medical Group, Fullerton, CA, USA; 4Sutter Health System, Roseville, CA, USA; 5Spinal Diagnostics PC, Tualatin, OR, USA; 6Advent Health Pain Specialists, Merriam, KS, USA; 7Department of Orthopedic Surgery, University of Colorado, Denver, CO, USA; 8Department of Physical Therapy, University of Evansville, Evansville, IN, USA; 9Physical Rehabilitation Network (PRN), University of St. Augustine, San Diego, CA, USA; 10Division of Pain Medicine, Brigham & Women’s Hospital/Harvard Medical School, Boston, MA, USA
Correspondence: Krishnan Chakravarthy, Department of Anesthesiology and Pain Medicine, University of California San Diego Health Sciences, San Diego, CA, USA, Email [email protected]
Abstract: In this review, we present a comprehensive clinical approach to restorative neurostimulation, a novel form of stimulation for refractory chronic mechanical low back pain, targeting impaired neuromuscular control and degeneration of the multifidus muscle. We focus on patient identification, technique guidance, and review of the scientific background and clinical evidence. As our understanding of back pain grows, there is clear evidence that impaired neuromuscular control and consequent degeneration of the multifidus muscle contribute to mechanical low back pain development and maintenance. We provide clinical guidance regarding an implantable restorative neurostimulation system that targets impaired neuromuscular control. Supported by results from a randomized, active-sham-controlled clinical trial with long-term follow-up, we provide clinicians with a comprehensive overview and practical clinical guidance for the adoption of this therapy modality.
Keywords: restorative neurostimulation, multifidus, arthrogenic inhibition, neuromodulation, chronic mechanical low back pain, neuromuscular control
Introduction
Low back pain has an enormous impact on our society. Globally it is the leading cause of years lived with disability,1 and in the US, it has an estimated annual cost of $200 billion dollars.2 Eighty percent of adults will have low back pain at some point in their lives,2 and there is a 7.3% global point prevalence for activity limiting low back pain.3 While most episodes of acute low back pain episodes resolve, approximately 10% of patients develop chronic low back pain.4 The percentage of the population with years of healthy life lost due to disability (YLD) due to low back pain has increased by >50% from 1995 to 2015.1 The importance of treating lower back pain effectively, therefore, cannot be understated.
Chronic low back pain (CLBP) can include components of (1) neuropathic pain, (2) nociceptive pain, (3) nociplastic pain or some combination of these three.5 Management of CLBP requires individualized therapies based on the predominant type of pain. Neuropathic CLBP arises from inflammation or injury to nerves.6,7 Nociplastic CLBP is mediated by altered perception and processing of pain in the central nervous system, usually in the absence or after resolution of any significant peripheral tissue damage.8,9 Neuropathic and nociplastic CLBP can be challenging to manage with treatments including pharmacological treatment, epidural injections, spinal cord stimulation – all of which provide palliative and temporary analgesia. Nociceptive CLBP is caused by stimulation of nociceptors in the lumbar spine or adjacent spinal muscles or tissue.6 Nociceptive pain may arise from disruption of the stabilizing system of the lumbar spine comprising the passive structures of the spinal column, the spinal muscles or the neural system controlling these muscles.10–16 In regards to spinal musculature, the lumbar multifidus (MF) is the largest of the back muscles to transverse the lumbosacral junction and plays an important role in stabilizing and supporting the lumbar spine.
The lumbar MF is comprised of deep, intermediate, and superficial fascicles, which have different anatomical architectures and functions. The deep MF fascicles have the smallest fiber bundle length and lowest muscle volume and are thought to provide intersegmental stability17 and proprioceptive feedback from the lumbar spine; therefore, injury to the deep MF fascicle will disrupt function at this level.16 The intermediate MF fascicles have broad attachments to the lateral spinous processes and help facilitate intersegmental movement.17 The superficial MF fascicles have the largest muscle volume and longest fibers, which provide rotation and spinal extension.17 Notably, not every MF layer is always present at the level of each spinous process; for example, the intermediate MF is commonly absent at L5 with important physiologic consequences including increased incidence of L5 prolapse.17
The central nervous system, specifically the motor cortex, also facilitates dynamic stability of the MF and lumbar spine. There is evidence for impaired corticomotor control of the MF in patients with CLBP. The paradigms of double-pulse transcranial magnetic stimulation (TMS) (a combination of conditioning and test TMS pulses) are useful in motor control studies to probe the excitability of M1 circuits surrounding the corticospinal cells and regulating their excitability.18 The short-interval intracortical inhibition (SICI) paradigm probes the excitability of GABAA circuits, and the short-interval intracortical facilitation (SICF) probes glutamatergic circuits.19 TMS has demonstrated alterations in short-interval intracortical inhibition and facilitation of the M1 motor cortex region controlling the MF in patients with CLBP.20 Central processing changes in the primary motor cortex may contribute to sustained impaired control and functional stability of the lumbar spine in patients with CLBP.13
Arthrogenic inhibition of the MF muscle is theorized to lead to impaired motor control, particularly of the deep fascicles that provide functional segmental stability. Electromyographic (EMG) studies have demonstrated altered timing of deep fascicle MF recruitment in patients with CLBP.10 Furthermore, CLBP may result in patient behavioral modifications that lead to further disuse, degeneration, and atrophy of the MF. A cycle of reduced neural drive and decreased lumbar spine stability results (Figure 1).
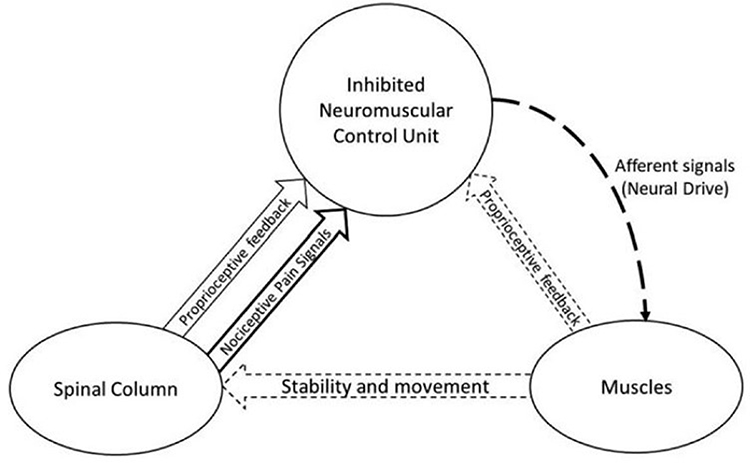 |
Figure 1 Illustration showing the three subsystems. Nociceptive pain signals leads decreased neural drive from the neuromuscular control unit. This lends to decrease in feedback and stability/movement of the multifidi. Note: Reproduced from this article which was published in Neuromodulation, 12, Marc Russo, Kristiaan Deckers, Sam Eldabe, Kyle Kiesel, Chris Gilligan, John Vieceli, Peter Crosby, Muscle Control and Non-specific Chronic Low Back Pain, 1-9, Copyright Elsevier 2019.10 |
Diagnostic tests and studies to evaluate the MF include MRI or ultrasound imaging, EMG studies and physical exam maneuvers, such as the prone instability test (PIT) and the multifidus lift test (MLT). Although EMG may be used to evaluate MF recruitment in patients with CLBP, the use of EMG for the evaluation of MF dysfunction has several limitations. Surface EMG is not sufficient to record activity from the deeper MF layers, thus necessitating the use of deep needle electrodes or fine wires.10 Even with the use of more invasive EMG approaches, it is difficult to definitively isolate deep fascicle MF activity from that of the surrounding deep lumbar back muscles. MRI and ultrasound imaging can provide further anatomic information, particularly to the size and make-up of the MF, but ultimately has little clinical utility in proving motor control dysfunction. Ultrasound imaging may demonstrate decreased changes in MF thickness after muscle activation in patients with low back pain, but it is unclear if these imaging results can be reliably used to predict treatment outcomes.10 Additionally, any pathological findings in imaging studies may have been pre-existing and not pain-related. Therefore, a neuromuscular physical examination is essential to diagnosing MF dysfunction as the etiology of CLBP.
Once MF dysfunction has been appropriately diagnosed, interventions aimed at activating and restoring functionality to the MF muscle should be considered. Restoration of function rather than symptomatic treatment should be the priority to prevent recurrence and progression of CLBP.15 Therapeutic interventions include targeted physical therapy exercises to activate the deep MF muscles, but isolated activation of the deep MF muscle is often difficult due to non-volitional control of the muscle as well as ongoing neural inhibition. For example, while the MF may play a role in facilitating spinal extension, it is certainly not the only muscle involved in this action, therefore basic spinal extension exercises may not necessarily improve deep MF motor control.15 Despite these difficulties in their execution, exercises that specifically activate the deep MF are associated with more successful treatment outcomes than exercises that generally stabilize the core back muscles as a whole, including the MF, erector spinae and transverse abdominis muscles.10 Ultrasound guided biofeedback exercises can help patients practice voluntary contraction of the MF. When successful, targeted MF exercises may restore neural activation, reduce the severity of back pain, and decrease the frequency of recurrence.10
Re-establishing voluntary control of the MF muscle may not be feasible for every patient with physical therapy and exercise alone. In these instances, direct electrical stimulation of the MF may be a suitable alternative. Transcutaneous neuromuscular electrical stimulation (NMES) has already been used successfully to initiate contraction of the quadriceps muscles in patients with knee osteoarthritis and subsequent arthrogenic inhibition of the quadriceps.21–26 However, transcutaneous electrical stimulation does not allow for targeted MF contraction, nor does it penetrate deeply enough to cause contraction of the deep MF fascicles. Therefore, direct electrical stimulation of the lumbar medial branches may be used to override arthrogenic inhibition of the MF muscle and elicit isolated contractions of all the MF fascicles innervated by this medial branch. Typically, this intervention targets the L2 medial branch at the L3 transverse process because the muscle fascicles that the L2 medial branch innervates cover adjacent levels extending to the caudal spine.27 Successful restoration of motor control and functional stability of the lumbar spine may then allow for lifestyle changes and increased participation in treatments including physiotherapy and exercises to prevent relapse or recurrence.
Diagnostic Criteria and Patient Identification
Sources of CLBP comprise of discs, joints, fascia, muscles, ligaments, the vertebral endplate or a combination of these. These are pain sources and not etiologies. Each of these sources may have pain as a result of impaired neuromuscular control. This is separate from pain symptoms in the extremities, which suggests a neuropathic source of pain (ie, lumbosacral radiculopathy, plexopathy). The patient history and physical examination may assist with diagnosing the source of low back pain, however no conclusive pathognomonic signs presently exist. Similarly, radiographic or advanced imaging is not necessarily diagnostic – with radiographic findings possibly being incidental in nature.28 Imaging may assist in ruling out certain causes of back pain, such as traumatic causes or tumors. The combination of history and multiple provocative maneuvers has allowed for increased accuracy in diagnosis (ie, sacroiliac joint dysfunction).
MF dysfunction is a likely mechanism underlying development and/or maintenance of pain, at least initially as a result of suboptimal tissue loading.29 Diagnosing of MF dysfunction is mainly based on physical examination, which includes two well-reported provocative maneuvers: the prone instability test (PIT) and the multifidus lift test (MLT).
The Prone Instability Test (PIT)
The prone instability test (PIT) is intended to identify when a patient has CLBP because of a lumbar segmental instability related to MF muscle dysfunction. The PIT test was used in the original selection criteria in the Reactiv8-A and Reactiv8-B studies and may be looked upon as the preferred test when evaluating the role of MF. Additionally, the pain/no pain feedback provided with the PIT demonstrates the impact of functional stabilization of the MF – for both the patient and physician.
The PIT is performed with the patient prone in a relaxed and neutral spine posture with their anterior superior iliac spine (ASIS) on the edge of the exam table and hips flexed to approximately 45 degrees (Figure 2). The first step is to perform a posterior to anterior pressure (PA) on each of the lumbar segments. To perform the glide, the examiner first finds the L1 spinous process, placing the base of their wrist (pisiform bone) over the spinous process, and then moves slightly lateral so the hypothenar eminence is directly over the spinous process. This contact point is important to allow for the examiner to create the PA glide pressure without superficial bony pain.
 |
Figure 2 Demonstration of the multifidus lift test (MLT). |
The examiner locks in their elbow and produces a rhythmic PA vertical force, creating movement at the desired level (Figure 2). The patient is to report if the PA shear movement creates pain. The PA pressure is repeated at each lumbar level working caudally from L1 to L5. To find the landmark of the L1 spinous process, we locate the 12th rib and palpate one level down.
If the PA pressure produces pain in a segment, the tester maintains their testing hand in contact with the painful level and asks the patient to lift their feet (5 cm lift) off the floor (Figure 2). Once the feet are lifted, the entire posterior back musculature is activated, and the examiner repeats the PA pressure. If the pain is abolished or substantially reduced, the PIT test is considered positive (abnormal) and suggests a segmental stabilization deficit at that level.30 It is best to test each level and document the findings for each level. If the PA glide does not produce pain at any level, or the pain does not abate when the PA glide is performed during the muscle activation condition, the PIT is considered negative (normal).
The PIT has a high interrater reliability (K = 0.87) and a face validity.30 Two studies have demonstrated the relationship between lumbar MF dysfunction and the PIT test as measured by ultrasound and EMG.31,32
Multifidus Lift Test (MLT)
The multifidus lift test (MLT) is intended to identify MF muscle dysfunction via a palpation technique. At the lower levels of the lumbar spine, the MF muscle can be palpated, just lateral to the spinous process in a slight depression between the spinous process and the longissimus muscle (Figure 3). Research has demonstrated that the MF muscle is activated automatically when the patient lifts their upper extremity and that the EMG activity in the muscle during the extremity lift is related to thickness change in the muscle as measured by ultrasound imaging. The thickness change in the muscle can also be detected by a simple palpation technique that was validated in a research study. Reduced or absent thickness change during the extremity lifting procedure is thought to reflect MF muscle dysfunction in patients with CLBP.
 |
Figure 3 Demonstration of the prone instability test (PIT). |
In comparison with the PIT, the MLT is not specific to recruitment of the deep multifidus fascicles and therefore is less specific to the detection of functional instability. The contraction which is felt is a summation of the contractions of all MF fascicles at that level. The contribution of the deep MF is expected to be the smallest contributor. The intermedia and superficial muscles associated with voluntary motions may still recruit, even if the deep fascicles are completely inhibited.33
To perform the MLT, the patient is positioned on the plinth in a prone position with a pillow under their pelvis to reduce lumbar lordosis. The patient’s upper extremities are placed at approximately 120 degrees of shoulder abduction with the elbows flexed to approximately 90 degrees (Figure 3). Next, the examiner palpates over the MF muscle just adjunct to the L4 and L5 spinous process. Once the palpation point has been determined, the examiner asks the patient to lift their contralateral arm off the table (5 cm lift) and palpates for the MF muscle thickness change. A normal response (negative test) is a brisk MF contraction coming directly up under the tester’s fingertips. Often, the tester will appreciate the MF muscle activation prior to observing extremity movement. An abnormal response (positive test) is either a reduced or absent contraction, or an excessive contraction of adjacent longissimus muscle (tester will feel the longissimus muscle pushing their finger medially toward the spinous process and will not appreciate the thickness change of MF muscle directly under their fingertips).
Hebert et al reported the reliability (K = 0.75 to 0.81) of the multifidus lift test (MLT), a palpation technique designed to test for MF function.34 The test has additionally been validated using ultrasound imaging measure of thickness change of the MF.35
Diagnostic Imaging Criteria
Multifidus muscle atrophy often develops if inhibition goes untreated. Both ultrasound and MRI may be used to assess MF atrophy. Ultrasound may be used to measure the cross-sectional area of the muscle,36 while MRI allows for the measurement of the cross-sectional area, as well as the grade of fatty infiltration, of the multifidus muscle (Figure 4). 37 Specifically, Grade 0 is a normal muscle with up to 10% of the cross-sectional area of the MF, Grade 1 is 10–50% and is considered a mild-to-moderate MF atrophy, Grade 2 is >50% is considered moderate-severe MF atrophy.37 There is some dispute as to whether MF atrophy can be correlated with disability and function,36,38–41 There is, however, value when imaging is available to visualize the MF directly. MF atrophy itself should never be relied upon as a criterion for motor dysfunction. Rather, it is a direct indication of the level of degeneration present, which when correlated with history and physical examination, may prompt further evaluation of the MF.42
 |
Figure 4 Grade scoring of multifidi atrophy. Reproduced from Kjaer et al, 2007.42 |
Summary of Scientific Background
Core stabilization exercises have historically been prescribed for the treatment of generalized low back pain symptoms, independent of etiology. Physiologically, the use of core stabilization exercises is appropriate for patients with spinal instability due to muscle weakness or imbalance.
There are several published studies on the efficacy of therapeutic exercises specifically targeting the MF muscles. Those studies that have focused on the MF have shown positive outcomes.43 In practice, many patients find it difficult to perform targeted MF exercises due to pain. Additionally, there may be an element of arthrogenic muscle inhibition – particularly in advanced disease states of chronic low back pain – which further prohibit contractions.44 Researchers have utilized transcutaneous stimulation of the lumbar paraspinal muscles, which was reported to be tolerated reasonably well in older adults with CLBP,45 however, selective transcutaneous stimulation of the MF muscle is not possible.
Stimulating the muscle mass directly requires substantially more energy than stimulating the motor nerve innervating the muscle, and the energy required to activate the deeper MF fascicles is considered painful by many participants.46 Electrical stimulation of the medial branches elicits smooth MF contractions. It is repetitive isolated activation of the MF that over time improves muscle activation, may allow for reversal of MF atrophy and facilitate restoration of motor control to the MF (when used alongside an exercise program), thereby increasing spinal stability.
Summary of Clinical Data
The simulation of the medial branch of the lumbar dorsal ramus was first described by Deckers et al.47 The procedure was originally performed utilizing a two-incision technique in which standard SCS leads were placed bilaterally at the junction of the transverse process and superior articular process of L3 with the lead body parallel to the spinal column.48 This feasibility study informed the development of a dedicated restorative neurostimulation system that included a proprietary four-electrode lead with distal passive fixation tines to mitigate the risk of lead migration and the design of the prospective multicenter clinical trial (ReActiv8-A). The trial included 53 subjects, and at one year, 57% of had ≥2-point reduction in the single-day pain numeric rating scale (NRS), 60% had ≥10-point functional improvement in the Oswestry Disability Index (ODI), and 81% had ≥0.03-point health-related quality of life improvement in EQ-5D index compared to baseline values. The implant technique was amended after an investigation determined that the lateral approach subjected the lead to repetitive shearing forces generated by two layers of fascia moving in opposing directions.49
In the modified implant approach, both leads are inserted at the L4 midline where the layers of fascia fuse together. This approach has since been utilized in the most recent prospective, multicenter, randomized, active sham-controlled ReActiv8-B trial.50 To be eligible for participation in the ReActiv8-B trial,46 a positive prone instability test was required, demonstrating multifidus motor control impairment in addition to pain intensity (VAS ≥7), disability (ODI ≥21), and other criteria.
In this trial, 204 patients were implanted with a permanent lumbar medial branch nerve stimulator and randomized 1:1 to therapeutic- or low-level sham stimulation 14 days after implant. The composite primary endpoint was the difference in proportions of responders in the treatment and the sham-control groups at 120 days post-randomization. A responder was defined as a participant who responded with ≥30% reduction from baseline in 7-day recall of average CLBP visual analog scale (VAS) pain ratings without an increase in baseline pain medications. Following assessment of the primary endpoint at 120 days, patients in the control group crossed over to receive levels of electrical stimulation as in the treatment group. In the treatment group, the responder rate at 120 days was 57.1%, compared to 46.6% percent in the control group, a trend that did not reach statistical significance. Despite this, the mean group difference in VAS improvement (−3.3 cm vs −2.4 cm, difference of −0.9 cm; 95% CI −1.6 to −0.1 cm; p = 0.032) was significant in favor of the treatment, as was the prespecified intention-to-treat (ITT) cumulative proportion of the responder analysis of the primary outcome data. Although the primary endpoint was inconclusive, overall data from the blinded phase of this trial are consistent with a clinically meaningful benefit at 120 days. After unblinding and the switch from sham to therapeutic stimulation in the sham-control group, improvements increased over time out to 1 year in the combined cohort.
Secondary efficacy outcome measures included ODI, EQ-5D-5L index, percentage-pain-relief (PPR), subject global impression of change (SGIC) and proportion of subjects with LBP resolution (defined as a VAS of ≤2.5 cm at follow-up). Four out of the five secondary endpoints were statistically significant in favor of treatment. Only the difference in proportion of subjects with LBP resolution was not significant (34% vs 27.7%; difference of 6.3%; 95% CI −6.5 to 19.0%; P = 0.335). At 1 year, 64% of patients reported an improvement in VAS of ≥50%, 52% of patients reported low back pain resolution, and 69% reported an improvement of ≥15 points in ODI.50 The incidence of serious procedure- or device-related adverse events and overall safety profile compared favorably with rates published for other implantable neurostimulator therapies for chronic pain and no lead migrations were reported.50
A longitudinal follow-up of 156 patients from the ReActiv8-B trial for whom complete 2-year data were available showed that the proportion of participants with ≥50% CLBP relief was 71%, and 65% reported CLBP resolution (VAS ≤ 2.5 cm); 61% had a reduction in ODI of ≥20 points, 76% had improvements of ≥50% in VAS and/or ≥20 points in ODI, and 56% had these substantial improvements in both VAS and ODI.51 Mean EQ-5D had improved from 0.585 to 0.798, which approached the US population norm. A total of 87% of participants had continued device use during the second year for a median of 43% of the maximum duration, and 60% (34 of 57) had voluntarily discontinued (39%) or reduced (21%) opioid intake.
The overall incidence of related serious adverse events (SAEs) from the Reactiv8-B trial was 8 of 204 (3.9%). There were six cases of surgical infection, one case of intraoperative airway obstruction, and one case of non-radicular patch numbness of the thigh. After the six-month follow-up, there were no further SAEs reported. Importantly, there were no incidences of lead migration, which typically plague neuromodulation systems.
A recent publication by Mitchell et al reported on four-year data for subjects from the original Reactiv8-A study. Of the original 53 patients enrolled, 34 patients were followed-up. The four-year results showed continued reduction in NRS, ODI, and EQ-5D scores.52
Initial evidence has shown restorative neurostimulation of the L2 medial branches to be a viable option for the treatment of nociceptive low back pain. The studies show that therapeutic benefits accrue with time, consistent with the restorative mechanism of action. The two-year data from the ReActiv8-B trial and the four-year data from the ReActiv8-A study show that the therapeutic benefit is substantial and durable.
Restorative Neurostimulation Trialing
The relevance of temporary screening trials for neuromodulation devices depends on the trial’s ability to: 1) replicate the mechanism of action (MOA), 2) establish an effective programming solution, 3) elicit a clinically meaningful treatment effect within the trial period and 4) predict future responders (or non-responders).
Above all, the ability of the trial to reproduce the therapeutic mechanism and treatment effect of the permanent device is essential to enriching the population with likely responders.
Unlike SCS and other analgesic approaches, the clinical benefits of restorative neurostimulation accrue gradually over time with patient individual trajectories, which makes it impossible to reach a meaningful treatment effect within the typical screening trial period. Therefore, patient selection relies on the clinical diagnosis of functional instability secondary to multifidus neuromuscular dysfunction. An earlier section in this paper provided details on physical assessments and radiological measures that guide appropriate patient selection.
Because isolated multifidus contractions are fundamental to the mechanism of action, trial stimulation is performed intra-operatively after lead placement with the patient under sedation or general anesthesia to verify that stimulation elicits smooth multifidus contractions. The simulated pulse amplitude is titrated to a level that elicits isolated, smooth, and well-tolerated multifidus contractions during programming visits. There were no reports of patients in whom such an appropriate contraction pattern could not be achieved. This means that a pre-implantation trial to assess the adequacy of programming solutions is also unnecessary.
In summary, careful multidisciplinary patient selection, a restorative rather than palliative mechanism of action and demonstrated durability of clinically meaningful improvements in over two thirds of patients eliminate the need for trials for restorative neurostimulation.
Implantation Technique and Clinical Stimulation Parameters
Preoperative and Patient Positioning
While in preoperative holding, the authors confirm and mark the desired location for the internal pulse generator (IPG) pocket. The authors find it helpful for patients to wear an IPG template for a period of time prior to surgery to establish the ideal location for the IPG site. In the operating room, the patient is placed on the fluoroscopy table in the prone position, with pillows or other bolsters placed underneath the abdomen to minimize lumbar lordosis. Preparing the skin and draping the surgical field is done in a typical sterile fashion.
Imaging and Guide Needles
The L3 vertebral body is identified under fluoroscopy, and a true anterior-posterior (AP) view is obtained. The C-arm should be tilted in a cranio-caudal fashion such that the superior endplate of L3 is flattened to the furthest extent possible. The endplate should be flat when viewed in both the AP and lateral views.
From the AP position, a spinal needle is advanced to contact the junction between the base of the L3 superior articular process and the transverse process. The ideal location is at the superior edge of the transverse process, just lateral to the pedicle and facet joint. The needle should be placed perpendicular to the plane of the intertransversarii muscle. A second guide needle is then placed on the contralateral side in an identical fashion (Figure 5). The placement of the spinal needles is intended to help guide the trajectory of the introducer needle when utilized (step 4).
 |
Figure 5 Fluoroscopic anterior-posterior view showing initial placement of guide needles. |
Surgical Access and Fascial Entry
Remaining in the AP position, the L4 spinous process is identified fluoroscopically. The midpoint between the inferior edge of the L3 spinous process and the superior edge of the L4 spinous process is marked. An incision line from this point, extending caudally about 1-1/2” is marked (Figure 6) An incision is made along this line, and the subcutaneous tissues are dissected until the supraspinous ligament is identified.
 |
Figure 6 Fluoroscopic anterior-posterior view showing skin incision/entry site. |
A needle entry point is determined so that the angle of approach towards the guide needle target will be approximately 45 degrees. A small stab incision is made through the supraspinous ligament, as close to the midline as possible. It is important to avoid being too lateral from midline with the approach to mitigate shear forces on the lead once placed.
A small strain-relief pocket 1–2 inches in diameter is made in the subcutaneous tissue at the inferior aspect of the incision, ipsilateral to the IPG.
Delivery Needle and Guidewire Placement
In AP view, the delivery needle is passed through the stab incision, angling laterally and anteriorly towards the guide needle. The ideal trajectory of the delivery needle will appear to traverse the inferolateral one-third of the pedicle in AP view. Once the tip of the delivery needle has touched the transverse process or is overlying it, the c-arm should be rotated to provide a true lateral view.
From the lateral view, the trajectory of the delivery needle towards the guide needle should approximate a 45-degree angle. The tip of the needle should be advanced slowly and cautiously through the plane of the intertransversarius muscle. In fluoroscopy, the needle will appear to be directed towards the posterior-inferior aspect of the L2-3 neural foramen. In this view, the tip of the delivery needle is ideally hugging the transverse process and is pointed at the posterior-inferior corner of the L2 vertebra (Figure 7).
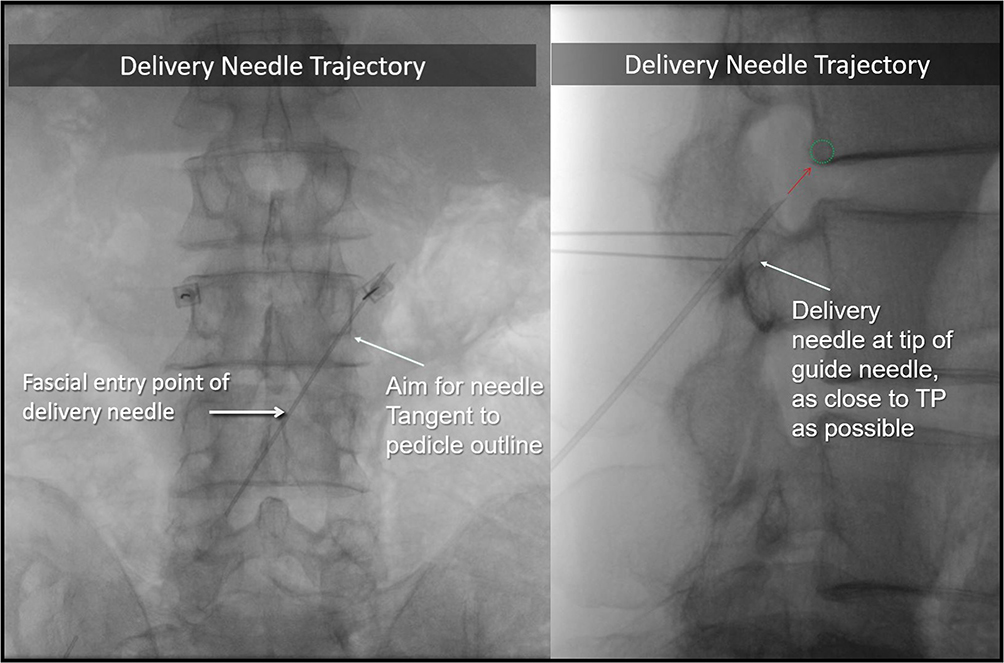 |
Figure 7 Fluoroscopic anterior-posterior view (left) and lateral view (right) with delivery needle placement. |
Proper needle position should then be confirmed from the AP view. The needle should be angled laterally and as close as possible to the pedicle.
A guidewire is then passed through the delivery needle so that the tip of the guidewire extends out of and distal to the delivery needle. If the guidewire is noted to immediately and sharply angle upwards (in a cranial direction), then the tip of the delivery needle is still posterior to the intertransversarius. In this case, the guidewire is brought into the delivery needle, which is then advanced slightly.
When the guidewire passes through the delivery needle and is pointed at the posterior-inferior corner of the L2 vertebra, the delivery needle can be withdrawn over the guidewire. The guidewire should remain in its original position. This is then performed on the contralateral side until both guidewires are satisfactorily positioned.
Introducer Sheath and Lead Placement
The introducer sheath (with dilator inside) is then passed over the guidewire. Resistance may be encountered initially if the stab incision through the supraspinous ligament (step 3) was not sufficient to allow passage of the sheath. Advancing the sheath with a gentle spiraling or twisting motion may be of benefit.
Once through this plane, attention is turned to the lateral view and the sheath slowly advances towards the plane of the intertransversarius. Resistance may again be encountered at this location. The introducer sheath is advanced until the dilator tip appears at the midpoint of the neural foramen. The tip of the introducer sheath must pass through the intertransversarius to facilitate appropriate placement of the tines of the lead. The orange hub of the introducer system is rotated counterclockwise and gently removed while holding the sheath in place.
The ReActiv8 lead is then carefully passed through the delivery sheath so that the distal-most electrode is aligned with the plane of the intertransversarius (Figure 8). Lead position should be confirmed from the AP view as well, with the lead hugging the lateral aspect of the pedicle (Figure 9).
 |
Figure 8 Fluoroscopic anterior-posterior view (left) and lateral view (right) with leads appropriately positioned for medial branch nerve stimulation. Noticed the AP view showing the strain relief loop. |
 |
Figure 9 Fluoroscopic anterior-posterior view with implantation of leads and implantable pulse generator (IPG). |
The sheath is gently and slowly retracted over the lead so that the distal tip of the sheath is just proximal to the most distal electrode, thus deploying the most distal tine anterior to the intertransversarius muscle. The lead is then gently pulled posteriorly (“tug test”) to ensure the proximal tine has been deployed across the posterior aspect of the intertransversarius. When the lead is pulled posteriorly and pushed anteriorly, one should sense slight resistance in both directions and will appreciate a few millimeters of AP movement of the lead when performed under live fluoroscopy. The contralateral lead is then placed in a similar fashion.
Testing and Tunneling
The proximal end of each lead is connected to a portable generator to verify normal impedance readings. Each electrode of each lead is sequentially activated on each side, and ipsilateral MF contraction should be confirmed either visually, by palpation, or both. The leads are then disconnected.
Attention is then turned to the previously identified and marked site for the IPG. The pocket is made utilizing standard surgical technique, and then a tunneling tool is used to connect the pocket and the midline incision (it is recommended that the introducer sheaths be left in place until tunneling has been completed for protective purposes.)
Only once step 6 is complete can the introducer sheaths be safely withdrawn, taking care to ensure that the lead remains intact.
Strain-Relief Loops and Final Steps
The leads are then tunneled from the midline incision to the pocket, leaving adequate lead at the incision site to allow for strain relief formation. The leads are coiled into the strain relief pocket in such a way that they enter the superior aspect of the pocket, coil in a single loop, and then exit the caudal aspect of the pocket towards the IPG. Note: For a right-sided IPG location, the loop will run in a counterclockwise direction, and for a left-sided IPG they will run clockwise.
Both electrodes should then be cleaned and dried and then plugged into the ReActiv8 implantable pulse generator. This in turn is placed carefully into the pocket while assuring that any residual lead is anterior to the IPG. Final muscle twitch testing is performed, and the correct system placement is verified and documented with AP and lateral images. Both incisions are then closed in a typical fashion.
Future Landscape and Indication Expansion
Presently, there are limited therapeutic options to address this specific etiology of lower back pain. Therapeutic options for low back pain involve corticosteroid injections or ablation of nerves, which transmit nociceptive pain signals. These traditionally involve repeated procedures with temporary and palliative pain relief. Furthermore, the use of palliative treatments may often lead to further weakening of the multifidi muscles resulting in motor dysfunction and sagittal imbalance, and as a result, worsened functional instability. This not only worsens the debility of the patient but also strains the medical system. Multifidi stimulation dramatically changes the treatment paradigm, focusing on restoration of function and potentially ending the need for ongoing procedures.
With evidence supporting the use of restorative neurostimulation in the lumbosacral spine, application to address various other chronic pain etiologies is a natural evolution. For example, future studies in axial neck and thoracic spine pain may also demonstrate meaningful treatment effects.
In the original Reactiv8-A and B studies, patients with prior history of spine surgeries were excluded. The purpose of those original studies was to study the effectiveness of restorative therapy for low back pain without the addition of confounding variables. Post-laminectomy syndrome (also called failed back surgery syndrome, FBSS), used to describe patients that present with persistent or recurring low back pain, with or without referred pain to the lower extremities, is quite common. The incidence of FBSS, depending on the type of surgery performed, is estimated to be between 10% and 40%.53 The pathogenesis of FBSS is primarily structural. Myofascial pain can also be a pain generator, secondary to intraoperative insult to the muscles, and compounded by postural changes in the postoperative period.54 Clinically, multifidus atrophy as a result of underlying inhibition and functional instability may be observed in these patients at the unfused segmental levels. In patients where the innervation and musculature near the painful level remain intact, restorative neurostimulation may potentially provide clinical benefits. This may be another subject of a future clinical trial.
A common sequela of fusion is adjacent segment disease.55 This occurs secondary to the displacement of physiologic stresses placed above and below previously fused levels. The use of neurostimulation to improve functional stability may potentially deter or postpone the onset of this issue.
Restorative neurostimulation may be applied to non-spinal anatomical targets where there are radiographic or clinical findings of muscle atrophy and/or functional instability. Examples of targets include peripheral joints – where both radiofrequency ablation and peripheral nerve stimulation have been used with increased frequency.56
Abbreviations
CLBP, chronic low back pain; NSAIDs, non-steroidal anti-inflammatory drugs; MF, multifidus muscle; TMS, transcranial magnetic stimulation; EMG, electromyographic; MRI, magnetic resonance imaging; PIT, prone instability test; MLT, multifidus lift test; RCT, randomized controlled trial; YLD, years lived with disability; NRS, numeric rating scale; ODI, Oswestry Disability Index; EQ-5D, EuroQOL health-related quality of life measure; VAS, visual analog-scale pain ratings; PPR, percentage of pain relief; SGIC, subject global impression of change; IPG, implantable pulse generator; AP, anterior-posterior; PA, posterior to anterior; ASIS, anterior superior iliac spine.
Acknowledgments
Third-party editing assistance was provided by Allison Foster, PhD, of Foster Medical Communications. Research funding provided by Mainstay Medical LLC.
Disclosure
Dr Krishnan Chakravarthy has stock options and is a consultant to Mainstay Medical, outside the submitted work; Dr David Lee reports Speakers Bureau from Mainstay Medical, outside the submitted work; Dr Samir Sheth reports personal fees from Boston Scientific, personal fees from SPR, personal fees from Medtronic, personal fees from Nevro, outside the submitted work; Dr Robert Heros reports grants, personal fees from Abbott, personal fees from Biotronik, personal fees from Boston Scientific, grants from Ethos Laboratories, grants, personal fees from Mainstay Medical, grants from Nevro, grants from Saluda, outside the submitted work; Dr Smith Manion reports personal fees from Mainstay Medical, outside the submitted work; Dr Vikas Patel reports personal fees from Mainstay Medical, during the conduct of the study; Dr Kyle Kiesel reports personal fees from Mainstay Medical, during the conduct of the study; Dr Christopher Gilligan reports personal fees from Mainstay Medical, during the conduct of the study; personal fees from Medtronic, personal fees from Abbott, personal fees from Saluda, personal fees from Persica, personal fees from Iliad Lifesciences, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. James S, Theadom A, Ellenbogen RG, Bannick MS, Montjoy-Venning W, Lucchesi LR. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(1):56–87. doi:10.1016/S1474-4422(18)30415-0
2. Rubin DI. Epidemiology and risk factors for spine pain. Neurol Clin. 2007;25(2):353–371. doi:10.1016/j.ncl.2007.01.004
3. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–2367. doi:10.1016/S0140-6736(18)30480-X
4. Meucci RD, Fassa AG, Faria NMX. Prevalence of chronic low back pain: systematic review. Rev Saude Publica. 2015;49:73. doi:10.1590/S0034-8910.2015049005874
5. Nijs J, Apeldoorn A, Hallegraeff H, et al. Low back pain: guidelines for the clinical classification of predominant neuropathic, nociceptive, or central sensitization pain. Pain Physician. 2015;18(3):E333–E346. PMID: 26000680. doi:10.36076/ppj.2015/18/E333
6. Baron R, Binder A, Attal N, Casale R, Dickenson AH, Treede RD. Neuropathic low back pain in clinical practice. Eur J Pain. 2016;20(6):861–873. doi:10.1002/ejp.838
7. Thomson S, Huygen F, Prangnell S, et al. Appropriate referral and selection of patients with chronic pain for spinal cord stimulation: European consensus recommendations and e-health tool. Eur J Pain. 2020;24(6):1169–1181. doi:10.1002/ejp.1562
8. Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W. Nociplastic pain: towards an understanding of prevalent pain conditions. Lancet. 2021;397(10289):2098–2110. doi:10.1016/S0140-6736(21)00392-5
9. Chimenti RL, Frey-Law LA, Sluka KA. A mechanism-based approach to physical therapist management of pain. Phys Ther. 2018;98(5):302–314. doi:10.1093/ptj/pzy030
10. Russo M, Deckers K, Eldabe S, et al. Muscle control and non-specific chronic low back pain. Neuromodulation. 2018;21(1):1–9. doi:10.1111/ner.12738
11. Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):
12. Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J Spinal Disord. 1992;5(4):
13. Ebenbichler GR, Oddsson LI, Kollmitzer J, Erim Z. Sensory-motor control of the lower back: implications for rehabilitation. Med Sci Sports Exerc. 2001;33(11):1889–1898. doi:10.1097/00005768-200111000-00014
14. Hodges PW, Bailey JF, Fortin M, Battié MC. Paraspinal muscle imaging measurements for common spinal disorders: review and consensus-based recommendations from the ISSLS degenerative spinal phenotypes group. Eur Spine J. 2021;30(12):3428–3441. doi:10.1007/s00586-021-06990-2
15. Hodges PW, Danneels L. Changes in structure and function of the back muscles in low back pain: different time points, observations, and mechanisms. J Orthop Sports Phys Ther. 2019;49(6):464–476. doi:10.2519/jospt.2019.8827
16. Freeman MD, Woodham MA, Woodham AW. The role of the lumbar multifidus in chronic low back pain: a review. PM R. 2010;2(2):142–146. doi:10.1016/j.pmrj.2009.11.006
17. Rosatelli AL, Ravichandiran K, Agur AM. Three-dimensional study of the musculotendinous architecture of lumbar multifidus and its functional implications. Clin Anat. 2008;21(6):539–546. doi:10.1002/ca.20659
18. Kujirai T, Caramia MD, Rothwell JC, et al. Corticocortical inhibition in human motor cortex. J Physiol. 1993;471(1):501–519. doi:10.1113/jphysiol.1993.sp019912
19. Ziemann U, Reis J, Schwenkreis P, et al. TMS and drugs revisited 2014. Clin Neurophysiol. 2014;125:S15. doi:10.1016/S1388-2457(14)50065-X
20. Massé-Alarie H, Beaulieu LD, Preuss R, Schneider C. Corticomotor control of lumbar multifidus muscles is impaired in chronic low back pain: concurrent evidence from ultrasound imaging and double-pulse transcranial magnetic stimulation. Exp Brain Res. 2016;234(4):1033–1045. doi:10.1007/s00221-015-4528-x
21. Imoto AM, Peccin S, Almeida GJM, Saconato H, Atallah ÁN. Effectiveness of electrical stimulation on rehabilitation after ligament and meniscal injuries: a systematic review. Sao Paulo Med J. 2011;129(6):414–423. doi:10.1590/s1516-31802011000600008
22. Stevens JE, Mizner RL, Snyder-Mackler L. Quadriceps strength and volitional activation before and after total knee arthroplasty for osteoarthritis. J Orthop Res. 2003;21(5):775–779. doi:10.1016/S0736-0266(03)00052-4
23. Stevens-Lapsley JE, Balter JE, Wolfe P, Eckhoff DG, Kohrt WM. Early neuromuscular electrical stimulation to improve quadriceps muscle strength after total knee arthroplasty: a randomized controlled trial. Phys Ther. 2012;92(2):210–226. doi:10.2522/ptj.20110124
24. Avramidis K, Strike PW, Taylor PN, Swain ID. Effectiveness of electric stimulation of the vastus medialis muscle in the rehabilitation of patients after total knee arthroplasty. Arch Phys Med Rehabil. 2003;84(12):1850–1853. doi:10.1016/S0003-9993(03)00429-5
25. Stevens JE, Mizner RL, Snyder-Mackler L. Neuromuscular electrical stimulation for quadriceps muscle strengthening after bilateral total knee arthroplasty: a case series. J Orthop Sports Phys Ther. 2004;34(1):21–29. doi:10.2519/jospt.2004.34.1.21
26. Kim KM, Croy T, Hertel J, Saliba S. Effects of neuromuscular electrical stimulation after anterior cruciate ligament reconstruction on quadriceps strength, function, and patient-oriented outcomes: a systematic review. J Orthop Sports Phys Ther. 2010;40(7):383–391. doi:10.2519/jospt.2010.3184
27. Lonnemann ME, Paris SV, Gorniak GC. A morphological comparison of the human lumbar multifidus by chemical dissection. J Man Manip Ther. 2008;16(4):E84–E92. doi:10.1179/jmt.2008.16.4.84E
28. Babińska A, Wawrzynek W, Czech E, Skupiński J, Szczygieł J, Łabuz-Roszak B. No association between MRI changes in the lumbar spine and intensity of pain, quality of life, depressive and anxiety symptoms in patients with low back pain. Neurol Neurochir Pol. 2019;53(1):74–82. doi:10.5603/PJNNS.a2018.0006
29. Brumagne S, Diers M, Danneels L, Moseley GL, Hodges PW. Neuroplasticity of sensorimotor control in low back pain. J Orthop Sports Phys Ther. 2019;49(6):402–414. doi:10.2519/jospt.2019.8489
30. Denteneer L, Stassijns G, De Hertogh W, Truijen S, Van Daele U. Inter- and intrarater reliability of clinical tests associated with functional lumbar segmental instability and motor control impairment in patients with low back pain: a systematic review. Arch Phys Med Rehabil. 2017;98(1):151–164.e6. doi:10.1016/j.apmr.2016.07.020
31. Hebert JJ, Koppenhaver SL, Magel JS, Fritz JM. The relationship of transversus abdominis and lumbar multifidus activation and prognostic factors for clinical success with a stabilization exercise program: a cross-sectional study. Arch Phys Med Rehabil. 2010;91(1):78–85. doi:10.1016/j.apmr.2009.08.146
32. Sung W, Hicks GE, Ebaugh D, et al. Individuals with and without low back pain use different motor control strategies to achieve spinal stiffness during the prone instability test. J Orthop Sports Phys Ther. 2019;49(12):899–907. doi:10.2519/jospt.2019.8577
33. Wakeling JM, Uehli K, Rozitis AI. Muscle fibre recruitment can respond to the mechanics of the muscle contraction. J R Soc Interface. 2006;3(9):533–544. doi:10.1098/rsif.2006.0113
34. Hebert JJ, Koppenhaver SL, Teyhen DS, Walker BF, Fritz JM. The evaluation of lumbar multifidus muscle function via palpation: reliability and validity of a new clinical test. Spine J. 2015;15(6):1196–1202. doi:10.1016/j.spinee.2013.08.056
35. Kiesel KB, Uhl TL, Underwood FB, Rodd DW, Nitz AJ. Measurement of lumbar multifidus muscle contraction with rehabilitative ultrasound imaging. Man Ther. 2007;12(2):161–166. doi:10.1016/j.math.2006.06.011
36. Rahmani N, Kiani A, Mohseni-Bandpei MA, Abdollahi I. Multifidus muscle size in adolescents with and without back pain using ultrasonography. J Bodyw Mov Ther. 2018;22(1):147–151. doi:10.1016/j.jbmt.2017.05.016
37. Faur C, Patrascu JM, Haragus H, Anglitoiu B. Correlation between multifidus fatty atrophy and lumbar disc degeneration in low back pain. BMC Musculoskelet Disord. 2019;20(1):414. doi:10.1186/s12891-019-2786-7
38. Le Cara EC, Marcus RL, Dempsey AR, Hoffman MD, Hebert JJ. Morphology versus function: the relationship between lumbar multifidus intramuscular adipose tissue and muscle function among patients with low back pain. Arch Phys Med Rehabil. 2014;95(10):1846–1852. doi:10.1016/j.apmr.2014.04.019
39. Rezazadeh F, Taheri N, Okhravi SM, Hosseini SM. The relationship between cross-sectional area of multifidus muscle and disability index in patients with chronic non-specific low back pain. Musculoskelet Sci Pract. 2019;42:1–5. doi:10.1016/j.msksp.2019.03.005
40. Goubert D, De Pauw R, Meeus M, et al. Lumbar muscle structure and function in chronic versus recurrent low back pain: a cross-sectional study. Spine J. 2017;17(9):1285–1296. doi:10.1016/j.spinee.2017.04.025
41. Sions JM, Elliott JM, Pohlig RT, Hicks GE. Trunk muscle characteristics of the multifidi, erector spinae, psoas, and quadratus lumborum in older adults with and without chronic low back pain. J Orthop Sports Phys Ther. 2017;47(3):173–179. doi:10.2519/jospt.2017.7002
42. Kjaer P, Bendix T, Sorensen JS, Korsholm L, Leboeuf-Yde C. Are MRI-defined fat infiltrations in the multifidus muscles associated with low back pain? BMC Med. 2007;5(1):2. doi:10.1186/1741-7015-5-2
43. Willemink MJ, van Es HW, Helmhout PH, Diederik AL, Kelder JC, van Heesewijk JPM. The effects of dynamic isolated lumbar extensor training on lumbar multifidus functional cross-sectional area and functional status of patients with chronic nonspecific low back pain. Spine. 2012;37(26):E1651–1658. doi:10.1097/BRS.0b013e318274fb2f
44. Rice DA, McNair PJ. Quadriceps arthrogenic muscle inhibition: neural mechanisms and treatment perspectives. Semin Arthritis Rheum. 2010;40(3):250–266. doi:10.1016/j.semarthrit.2009.10.001
45. Hicks GE, Sions JM, Velasco TO, Manal TJ. Trunk muscle training augmented with neuromuscular electrical stimulation appears to improve function in older adults with chronic low back pain: a randomized preliminary trial. Clin J Pain. 2016;32(10):898–906. doi:10.1097/AJP.0000000000000348
46. Sions JM, Crippen DC, Hicks GE, Alroumi AM, Manal TJ, Pohlig RT. Exploring neuromuscular electrical stimulation intensity effects on multifidus muscle activity in adults with chronic low back pain: an ultrasound imaging-informed investigation. Clin Med Insights Arthritis Musculoskelet Disord. 2019;12:1179544119849570. doi:10.1177/1179544119849570
47. Deckers K, De Smedt K, Van Buyten JP, et al. A new therapy for patients with Chronic Low Back Pain (CLBP): results of a European multicenter feasibility study. In:
48. Deckers K, De Smedt K, van Buyten JP, et al. Chronic low back pain: restoration of dynamic stability. Neuromodulation. 2015;18(6):
49. Deckers K, De Smedt K, Mitchell B, et al. New therapy for refractory chronic mechanical low back pain—restorative neurostimulation to activate the lumbar multifidus: one year results of a prospective multicenter clinical trial. Neuromodulation. 2018;21(1):48–55. doi:10.1111/ner.12741
50. Gilligan C, Volschenk W, Russo M, et al. An implantable restorative-neurostimulator for refractory mechanical chronic low back pain: a randomized sham-controlled clinical trial. Pain. 2021;162(10):2486–2498. doi:10.1097/j.pain.0000000000002258
51. Gilligan C, Volschenk W, Russo M, et al. Long-term outcomes of restorative neurostimulation in patients with refractory chronic low back pain secondary to multifidus dysfunction: two-year results of the ReActiv8-B pivotal trial. Neuromodulation. 2021. doi:10.1016/j.neurom.2021.10.011
52. Mitchell B, Deckers K, De Smedt K, et al. Durability of the therapeutic effect of restorative neurostimulation for refractory chronic low back pain. Neuromodulation. 2021;24(6):1024–1032. doi:10.1111/ner.13477
53. Chan C, Peng P. Failed back surgery syndrome. Pain Med. 2011;12(4):577–606. doi:10.1111/j.1526-4637.2011.01089.x
54. Waguespack A, Schofferman J, Slosar P, Reynolds J. Etiology of long-term failures of lumbar spine surgery. Pain Med. 2002;3(1):18–22. doi:10.1046/j.1526-4637.2002.02007.x
55. Wang T, Ding W. Risk factors for adjacent segment degeneration after posterior lumbar fusion surgery in treatment for degenerative lumbar disorders: a meta-analysis. J Orthop Surg Res. 2020;15(1):582. doi:10.1186/s13018-020-02032-7
56. Shorter E, Sannicandro AJ, Poulet B, Goljanek-Whysall K. Skeletal muscle wasting and its relationship with osteoarthritis: a mini-review of mechanisms and current interventions. Curr Rheumatol Rep. 2019;21(8):40. doi:10.1007/s11926-019-0839-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Restorative Neurostimulation for Patients with Mechanical Chronic Low Back Pain and Impaired Neuromuscular Control of the Lumbar Spine | A New Treatment Paradigm
Gilligan CJ, Chavda AS, Ho JS, Lee DW, Langhorst M, Yih ET, Amann M
Journal of Pain Research 2025, 18:5799-5813
Published Date: 4 November 2025