Back to Journals » Journal of Pain Research » Volume 18
Restorative Neurostimulation for Patients with Mechanical Chronic Low Back Pain and Impaired Neuromuscular Control of the Lumbar Spine | A New Treatment Paradigm
Authors Gilligan CJ ![]() , Chavda AS, Ho JS
, Chavda AS, Ho JS ![]() , Lee DW, Langhorst M, Yih ET, Amann M
, Lee DW, Langhorst M, Yih ET, Amann M
Received 21 May 2025
Accepted for publication 11 September 2025
Published 4 November 2025 Volume 2025:18 Pages 5799—5813
DOI https://doi.org/10.2147/JPR.S525057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Dawood Sayed
Christopher J Gilligan,1 Avinash S Chavda,2 Johnson S Ho,3 David W Lee,4 Meredith Langhorst,5 Erika T Yih,6 Marco Amann7
1Office of the Chief Medical Officer, Robert Wood Johnson University Hospital, New Brunswick, NJ, USA; 2Department of Interventional Pain Management, Virtuoso Spine and Joint, Carrollton, TX, USA; 3Department of Interventional Pain Management, New Jersey Spine and Orthopedic, West Orange, NJ, USA; 4Department of Pain Management, Fullerton Orthopedic Surgery Medical Group, Fullerton, CA, USA; 5Department of Pain Management and Non-Operative Care, OrthoIndy, Indianapolis, IN, USA; 6Department of Physical Medicine and Rehabilitation, Harvard Medical School and Spaulding Rehabilitation Hospital, Boston, MA, USA; 7Department of Neurosurgery, Orthopädisches Krankenhaus Schloss Werneck, Werneck, Germany
Correspondence: Johnson S Ho, New Jersey Spine and Orthopedic, 375 Mount Pleasant Ave, Suite 205, West Orange, NJ, 07052, USA, Email [email protected]
Abstract: Chronic low back pain (CLBP) is a symptom of an underlying pathology. There are distinct phenotypes of CLBP, including neuropathic, nociplastic and nociceptive, or mechanical CLBP. We present a comprehensive clinical overview of restorative neurostimulation for refractory, disabling, mechanical CLBP. Impaired neuromuscular control and consequent degeneration of the multifidus muscles are implicated in the development and persistence of mechanical low back pain. Restorative neurostimulation targets these processes and aims to reverse these degenerative changes in the muscles and mechanoreceptor in the muscle spindles and, therefore, restore motor control of the multifidus muscles, playing an important role for functional stability of the lumbar spine. We detail the theory and rationale of the technology as well as appropriate patient identification and current trial evidence in this comprehensive overview of restorative neurostimulation.
Keywords: restorative neurostimulation, arthrogenic muscle inhibition, neurostimulation, chronic mechanical low back pain, multifidus muscle, neuromuscular control
Introduction
Low back pain (LBP) is a prevalent clinical complaint with staggering socioeconomic impact. LBP is the leading cause of years lived with disability worldwide, with the proportion of people disabled by LBP increased by over 50% between 1995 and 2015.1 Direct healthcare spending on LBP in the United States was estimated as high as $90.6 billion, with indirect costs including disability benefits and missed days from work as high as $535 billion.2 While most acute episodes resolve spontaneously, roughly 10% of patients progress on to develop CLBP.3 Therefore, developing treatments with effective long-term outcomes for low back pain cannot be overstated.
Chronic low back pain (CLBP) is always a symptom that stems from an underlying pathophysiology. Depending on origin of the noxious stimuli, CLBP may be typified as having three distinct phenotypes, neuropathic, nociplastic, nociceptive, or a combination of these.4 Neuropathic CLBP is caused by inflammation or injury to nerves, including neural compression, neoplasms, or Persistent Spinal Pain Syndrome Type 2, formerly referred to as failed back surgery syndrome. Nociceptive CLBP results from overload or damage to lumbar spine interverbal discs, vertebral body endplates, facet joints, and/or adjacent tissue,5 which may occur consequent to disruption of the lumbar spine’s stabilizing system.6–12 Nociplastic CLBP arises from altered processing and perception of pain in the central nervous system (CNS), often despite the absence of significant ongoing peripheral tissue damage.13,14 The predominant type of pain is an important factor in determining approach for management. Most patients with CLBP with no indication for spine surgery suffer from mechanical (musculoskeletal) pain that is predominantly nociceptive in nature.15–17 Although non-surgical treatment options including physical and chiropractic therapy, medications, injections, and medial branch or basivertebral nerve rhizotomy provide relief and functional improvement for some, they often provide only temporary relief or are ineffective for most of these patients.18–27 While spinal cord stimulation is an option for intractable neuropathic pain, it is not ideal for the treatment of predominantly nociceptive mechanical CLBP.28,29
Pathophysiology of Mechanical CLBP
Nociceptive or mechanical CLBP is often associated with degeneration and impaired motor control of multifidus (MF) muscles, a group of paraspinal back muscles with origin from transverse processes to insertion along spinous processes of vertebrae, that traverse the lumbosacral junction and contribute to significantly functional stability of the lumbar spine.12,30–32 They comprise deep, intermediate, and superficial fascicles, each with unique anatomical architecture and function. The multifidus muscle has unique architecture compared with other voluntary contractile muscles of the spine. There is a higher concentration of spindles, an anatomical structure within the muscle more closely associated with a proprioceptive function providing the predominant segmental and overall lumbar stability. Deep MF fascicles have the lowest volume and shortest muscle fibers, connecting between adjacent vertebrae to facilitate proprioceptive feedback and intersegmental stability. Intermediate MF fascicles, with broad attachments spanning more vertebral levels play a role in intersegmental movement. Finally, superficial MF fascicles have the largest volume and longest muscle fibers, providing optimal posterior spinal extension and rotation. Additionally, key anatomical considerations exist as each MF fascicle layer is not always present at all spinal levels, leading to important physiological consequences. For instance, the intermediate MF fascicle is often absent at L5, corresponding to an increased incidence of disc prolapse at that level.33
Arthrogenic Muscle Inhibition
Arthrogenic muscle inhibition (AMI) refers to a protective neurological response to joint injury which leads to altered afferent signaling, reflexive muscle inhibition, reduced somatic sensation, neuroplastic compensations in higher brain centers, and decreased motor output to the musculature surrounding a joint.34 In acute LBP due to a disc-related, sprain or strain injury, AMI of the deep MF fascicles leads to an immediate loss of functional stability around the painful segment. Indeed, in a porcine model, experimentally induced disc injury causes inhibition of MF activity.35 Failure for MF activity to spontaneously resume can lead to a self-sustaining cycle of persistent motor control impairment and chronification of nociceptive, mechanical CLBP.11,36 Altered timing of deep MF fascicle recruitment and abnormal activation of MF have been demonstrated in electromyography (EMG) studies of patients with CLBP.37–40 This etiology is distinctly different from back pain with radicular symptoms, which suggests a neuropathic or neuro-compressive source.
Multifidus Motor Control Impairment
Motor control of the MF muscles involves somatosensory afferent fibers of the peripheral nervous system, as well as the sensory and motor cortex of the CNS. The proprioceptive feedback from the multifidus muscle spindle is altered due to collagen deposition within this structure. Neuroplastic alterations in higher brain centers that occur with AMI likely play a role in perpetuating impairments in motor control.9 In patients with CLBP, transcranial magnetic stimulation studies have shown alterations in patterns of facilitation and inhibition of the M1 motor cortex region that controls the MF.41 Furthermore, organization of primary motor cortex differs between individuals with and without CLBP.42 Those with CLBP demonstrate reduced discrete cortical organization of inputs to back muscles, resulting in increased overlap in representation of motor cortical areas to deep MF and longissimus erector spinae muscles, and loss of ability for differential firing of these two muscles (ie, co-contraction).43 In the primary motor cortex, central processing changes occurring in the context of ongoing AMI, with altered proprioception, reactive disuse, and consequent degeneration of the muscle may contribute to impaired control and functional stability of the lumbar spine that is sustained in patients with CLBP.9 Additionally, pain may prevent patients from maintaining normal levels of activity and conditioning, leading to further disuse atrophy of the MF muscles and other core stabilizers causing a vicious cycle of decreased neural drive and impaired functional stability of the lumbar spine.
Restorative Treatment Paradigm
In order to prevent progression and recurrence of mechanical CLBP accompanied by multifidus dysfunction, the priority of management should be functional restoration rather than symptomatic or palliative treatment.11 Therefore, management may include physical therapy, which can help patients unlearn maladaptive behaviors and movement patterns developed as a result of pain avoidance and fear. Physical therapy exercises targeted at isolated activation of the deep MF muscles are associated with more successful outcomes compared to exercises that stabilize the core back muscles more generally.6 In some cases, biofeedback with ultrasound guidance can help patients achieve voluntary isolated MF contractions, but this approach has not proven feasible in routine clinical practice. When successful, targeted exercises to elicit isolated deep MF contractions may restore neural activation and reduce back pain severity and recurrence rates.6,44 Improved functional stability is believed to be a primary consequence of motor control restoration rather than reversal of the degenerative pathological processes, including muscle fibrosis and fatty infiltration.11 Unfortunately, due to pain, ongoing AMI, and co-contraction with other core muscles, attempts at isolated activation of deep MF muscles with physical therapy and exercise alone has not proven feasible for many patients.45
In other conditions such as knee osteoarthritis with resultant AMI of the quadriceps, transcutaneous neuromuscular electrical stimulation of the motor point has been successfully used to initiate contraction of inhibited quadriceps muscles.46–51 Transcutaneous electrical stimulation, however, is not precise enough to stimulate the medial branches of the dorsal ramus and does not penetrate to sufficiently induce deep MF fascicles contraction. Direct stimulation of the muscle mass requires substantially more energy to elicit a physiologic contraction than stimulating the nerve that innervates the muscle and can be painful for patients.52 Direct electrical stimulation of the motor component of the L2 dorsal ramus medial branch nerve has been shown to effectively elicit strong isolated MF contractions, overriding underlying AMI.53 This observation has led to the development of restorative neurostimulation for refractory mechanical CLBP.
Restorative Neurostimulation
Dorsal ramus medial branch nerves innervate MF muscles. The dorsal ramus nerve contains mixed sensory and motor fibers and gives rise to the lateral and the medial branches on the superior border of the transverse process. The medial branch runs along the junction between the transverse process and the superior articular process, and then descends caudally and posteriorly, accompanying vessels that arise from the lumbar artery and vein. The medial branch nerve also innervates the capsules of the facet joints, skin, and ligaments medial to the facet joint line.
The ReActiv8 (Mainstay Medical; Dublin Ireland) implantable ‘restorative’ neurostimulation system was approved by the FDA in June 2020 to treat refractory musculoskeletal CLBP associated with MF dysfunction. It delivers electrical stimulation to bilateral L2 dorsal ramus medial branch nerves to elicit smooth, well-tolerated isolated contractions of lumbar MF muscles and thus override the underlying AMI.54 While in a prone or lateral decubitus position, patients self-administer up to two 30-minute sessions per day during which the system elicits two 10-second multifidus contractions per minute. The reactivation of the muscle with consequent afferent proprioceptive signaling facilitates restoration of MF motor control and functional stability to the lumbar spine. Several clinical trials have shown that this therapy leads to improvements in pain, disability, and quality of life that ar substantial and long-lasting.6,54–56 Alternative peripheral nerve stimulator systems do exist that target nerves to multifidus muscles; however, they function primarily via a mechanism of modulating pain signals, compared to Reactiv8’s system with mechanism to restore multifidus muscle function.
Indications and Patient Selection
The ReActiv8 neurostimulation system is indicated for management of intractable chronic low back pain associated with multifidus muscle dysfunction, as evidenced by imaging or physiological testing in adults who have failed therapy including pain medications and physical therapy and are not candidates for spine surgery.57
The clinical trials that generated the published clinical evidence included patients with a diagnosis of chronic, disabling mechanical LBP with a pain intensity of ≥6.0 on a 10-cm visual analog scale (VAS); Oswestry disability index (ODI) of ≥21 on a scale from 0 to 100, no significant radicular symptoms, LBP on at least half of the days from the previous year, refractory to ≥90 days of conservative medical management including physical therapy and medications, and a positive prone instability test that is consistent with impaired MF neuromuscular control and consequent lumbar segmental instability.53,54 See Figure 1 for an evidence-based patient indication flow chart for selection of patients with CLBP for restorative neurostimulation.
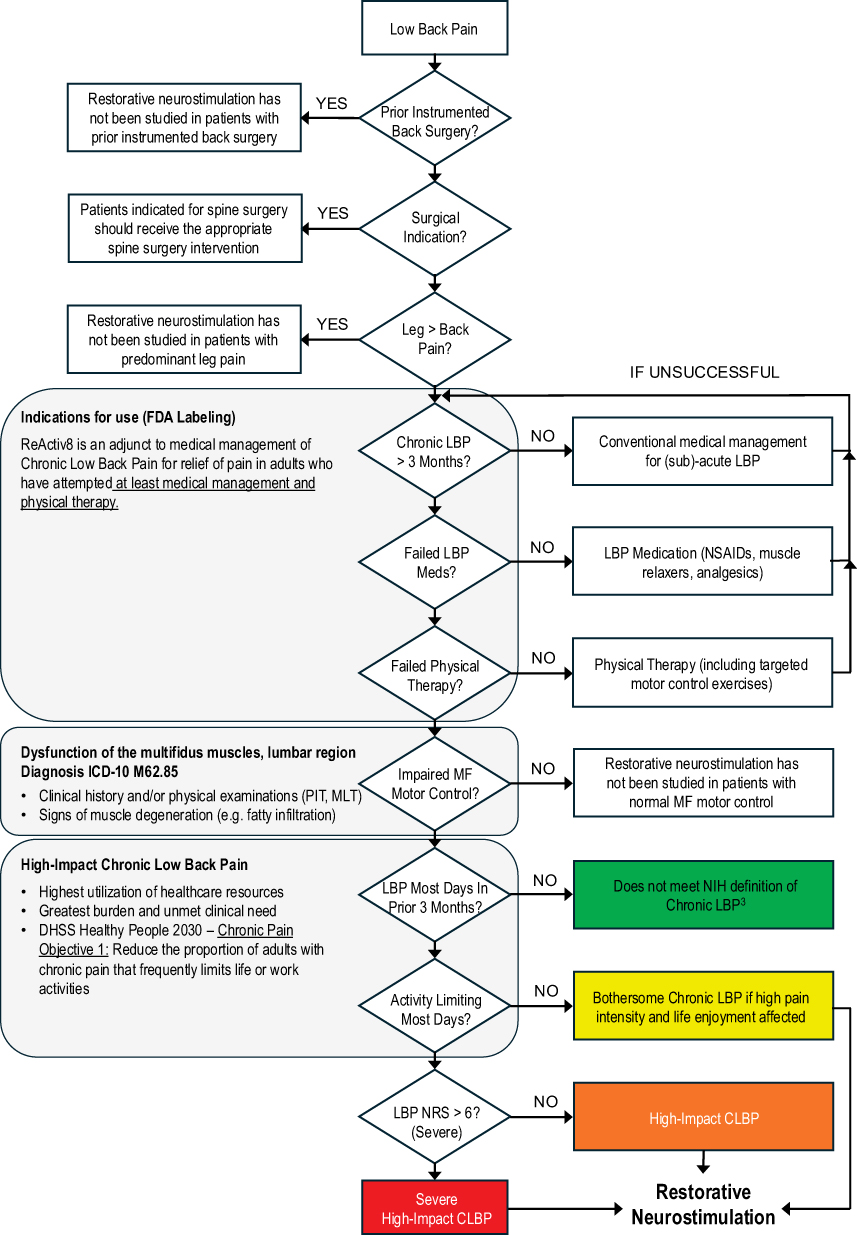 |
Figure 1 Evidence-based patient indication flow chart. |
Patient Identification
Identification of patients with MF dysfunction is based on medical history, and physical examination findings including the prone instability test (PIT), multifidus lift test (MLT), or the aberrant movements test. Diagnostic imaging demonstrates atrophy, fibrosis, and fatty infiltration of MF muscles as a secondary sign of degenerative loss of neuromuscular control and is used to exclude surgical indications such as nerve compression, fracture, or tumor. Before being considered for Restorative Neurostimulation, patients should have completed a structured program of physical therapy including guidance and education on home exercises that address engagement of the MF muscle into movement patterns and motion control.
Medical History
Key questions to obtain on history when identifying patients with MF dysfunction include how and when the pain started, range of activities or postures that typically provoke the pain, treatments already tried and whether they provide relief, if the pain is getting worse over time, if the pain is constant or waxing and waning, and how the pain affects patient’s daily life and function. Efforts with manual therapy, pain medications, and injections or ablation procedures typically only gives temporary pain relief, as these primarily “palliative” approaches do not address the underlying pathophysiology of MF dysfunction and will often only temporarily mask the pain without achieving durable, sustained relief.
Patients typically report load-dependent LBP features associated with changing postures, standing up from a seated position, or performing tasks from a lumbar flexed position. Small movements with repeated changes of the center of gravity cause pain, as well as lifting of heavy items. These symptoms indicate lack of neuromuscular control of MF muscles to stabilize the lumbar spine and prevent unshielded movement of lumbar spinal segments, resulting in tissue overload and nociceptive pain. Increased pain is often seen and reported with weightlifting in a gym setting as such forms of training typically addresses predominantly larger muscle groups, contributing to even more tissue overload and pain particularly when without adequate neuromuscular control dynamically stabilizing these movement segments. LBP becomes chronic when disability persists greater than 3 months. Patients with mechanical CLBP associated with MF dysfunction are often burdened with this condition for years as demonstrated in the multiple studies associated with Restorative Neurostimulation.
Physical Observations and Examinations
Patients with mechanical CLBP will often exhibit physical finding observations including aberrant movement patterns, sagittal imbalance postures, and guarding mechanisms to movement while also showing signs of stiffness. Small-load movements precipitate back pain and are evident from medical history. Over time, these patients tend to have more challenges with maintaining an upright posture and start to walk with forward-flexed posture creating sagittal imbalance and further precipitating LBP.
The aberrant movement patterns will be initially noticed with return to upright standing from a fully lumbar flexed position. Normally, hip extensors initiate pelvis posterior rotation prior to concentric contraction of the spinal extensors. Lumbopelvic rhythm describes the kinematic relationship between the lumbar spine and hip joints during movement in the sagittal plane. In cases of MF dysfunction, the order may be reversed. In some cases, patients may exhibit an instability catch, where they cannot smoothly fully flex, then extend their lumbar spine back to neutral, and instead have a “catch” in their motion. Additionally, they may even demonstrate positive Gower’s sign, using their hands to walk up their legs with trying to return to an erect posture. The patients start to limit their movements in hopes of preventing further episodes of their “back going out”. They develop alternative movement and muscle recruitment patterns leading to spine stiffness and compression areas that generates more load onto spinal segments. This deleterious cycle continues, and the patient’s daily life becomes increasing limited by the mechanical CLBP.
A standard musculoskeletal physical exam includes gait analysis. A forward-flexed posture while walking, although may indicate an underlying neuropathic origin of pain, can also be a sign of lumbar MF dysfunction. For this reason, in-depth medical history is paramount to make the distinction. Range-of-motion testing is also important for thorough evaluation. Straight leg and neuromotor testing are performed to rule out neuropathic origins of pain. PIT allows for assessment of pain from lumbar segmental instability arising from MF dysfunction. MLT allows for gentle palpation of the paraspinal tissue while assessing for MF balance and function.
Prone Instability Test
The PIT is used to identify CLBP caused by lumbar segmental instability related to MF dysfunction. It has high inter-rater reliability (K=0.87) and face validity,58 with two studies showing a correlation between positive PIT and lumbar MF dysfunction as measured by EMG and ultrasound.59–61 To perform PIT, patient is placed in prone position with their anterior superior iliac spine overlying the edge of the examination table, with a relaxed and neutral spine and hips flexed at approximately 45 degrees. With the patient in this position, a posterior-to-anterior (PA) pressure is applied to each individual lumbar vertebral segment and patient reports if the PA movement reproduces their index pain.
To do this, the examiner first identifies the L1 spinous process landmark by locating the 12th rib and palpating one level below. The examiner then places their wrist base (pisiform bone) over the respective spinous process and shifts slightly laterally until their hypothenar eminence is directly over the patient’s spinous process, thus creating a contact point that allows for generation of PA glide pressure without superficial bony pain. Locking the elbow, the examiner then applies a rhythmic PA force downward, creating shear force at the respective level, that is thus repeated at each vertebral level working caudally from L1 to L5.
If pain is reproduced at a segment from the PA glide pressure, the examiner’s testing hand is maintained in contact at the painful level, with patient instructed to lift their feet 5 cm off the floor to voluntarily activate their entire posterior back muscles. The examiner then repeats the PA pressure maneuver at the same level. A positive (abnormal) PIT is identified if the pain is eliminated or significantly reduced with patient engaging their entire posterior back musculature, suggesting a segmental stabilization (motor control) deficit at that vertebral level. The PIT is considered negative (normal) if no pain is reproduced with the PA glide at any level, or if the pain does not abate with the PA glide pressure even in the activated stabilizing muscles condition. In the latter cases, when all maneuvers are painful regardless of whether stabilizing musculature is activated, lack of pain reduction is not an exclusion criterion, but may suggest an additional hyper-inflammatory state caused by abnormalities of neuromuscular control.
Multifidus Lift Test
The MLT identifies MF dysfunction via noting of MF thickness change with manual palpation. The lumbar MF muscles can be palpated just lateral to the spinous process in a slight gutter between the spinous process and longissimus muscle. When the patient begins to lift one upper extremity, automatic involuntary activation of contralateral MF muscle normally occurs, with associated thickness change that can be appreciated by simple palpation. This test has also been validated using dynamic ultrasound imaging measuring MF thickness change.61 Reduced or absent thickness change at a palpated side during lifting of contralateral upper extremity reflects MF dysfunction. Like the PIT, the MLT has high interrater reliability (K=0.75 to.81).62 However, unlike the PIT, the MLT recruits all the MF fascicles at a specific level instead of specifically recruiting the deep fascicles, so MLT is less specific for functional instability. In fact, given that the deep fascicles of the MF have the lowest volume, they are likely only a small contributor to the palpated muscle thickness change.
To perform the MLT, patient is positioned in a prone position on the examination table with a pillow under their pelvis to reduce lumbar lordosis, and upper extremities resting at about 120 degrees shoulder abduction and 90 degrees elbow flexion. The MF muscle in the gutter just lateral to the L4 and L5 spinous processes is then lightly palpated with fingertips, and patient is instructed to lift one arm 5 cm off the table while the examiner assess for onset timing and volume quantity of MF muscle thickness change that should accompany this movement. The MLT is negative (normal) if the examiner appreciates a brisk MF muscle contraction directly underneath their fingertips, representing MF muscle activation that typically occurs immediately prior to physical visualization of contralateral upper extremity motion. The MLT is positive (abnormal) if reduced or no MF contraction is appreciated, or excessive contraction of the adjacent longissimus muscle occurs and consequently pushes fingertips medially toward the spinous process.
Diagnostic Imaging
The MF may be evaluated using diagnostic imaging options including magnetic resonance imaging (MRI) and ultrasound.63 If AMI of the MF is left untreated, ongoing disuse can rapidly lead to MF atrophy, fibrosis, and fatty infiltration. MF atrophy can be evaluated using ultrasound and MRI modalities to measure MF cross-sectional area.64,65 Additionally, MRI can evaluate degree of fatty infiltration,65 which is graded on a scale with Grade 0 being normal muscle with up to 10% fatty infiltration of the MF cross-sectional area, Grade 1 with 10–50% fatty infiltration (mild-moderate MF atrophy), and Grade 2 with >50% fatty infiltration (moderate-severe MF atrophy).60 Although impaired MF motor control and abnormalities on diagnostic imaging are typically correlated, causality is unclear, as abnormal imaging findings often exist independently of pain and motor dysfunction,64,66–70 and may be reversed in some cases with appropriate rehabilitation.71 Nonetheless, in the presence of CLBP, a combined approach with careful history and physical exam along with use of ultrasound and/or MRI may inform procedural interventions directed at MF dysfunction.72
MRI can precisely show multi-segmental degenerative findings such as facet joint degeneration, impaired joint faces with mild effusions and signs of arthrosis, degenerative disc spaces, or osteochondrosis. Mild signs of misalignment such as antero- or retrolisthesis in supine MRI compared to alignment in standing x-ray films demonstrate micro-movements due to inhibited neuromuscular control of the MF. X-ray and MRI are primarily used to exclude surgical indications but also to verify and prove multi-segmental degenerative findings predicted from patient history and physical exam.
Relevant ICD-10 Diagnosis Codes
Currently, the most appropriate ICD-10-CM diagnosis code that indicate medical necessity with reporting multifidus dysfunction is M62.85: “for the diagnosis of dysfunction of the multifidus muscles in the lumbar region” bringing the highest level of diagnostic specificity for providers to diagnose this condition. A secondary diagnosis code for reporting symptomatology is M54.59: “for other low back pain” is also appropriate. These codes were updated in the October 2024 ICD-10-CM code update to add a higher level of specificity to the medical condition of the patient, particularly those that are candidates for restorative neurostimulation. The relevant procedure codes for restorative neurostimulation implantation are CPT1 Code 64590: “Insertion or replacement of peripheral or gastric neurostimulator pulse generator or receiver, direct or inductive coupling” and CPT1 Code 64555: “Percutaneous implantation of neurostimulator electrode array, peripheral nerve (excludes sacral nerve)”.
Clinical Trial Evidence
Deckers et al first described lumbar medial branch stimulation in 2013;73 a multicenter feasibility study successfully repurposed SCS leads, which when placed bilaterally at the superior articular process and transverse process of the L3 junction led to at least a 50% pain relief for half of subjects after 5 months.53 This feasibility study suggested the need for dedicated electrodes for medial branch stimulation and led to the creation of a restorative neurostimulation system including four-electrode leads with passive fixation tines to minimize risk of lead migration.
The subsequent prospective international, multi-center (ReActiv8-A) trial evaluated this proprietary system in 53 subjects with on average 14 years of severe, disabling CLBP.6 After one year, compared to baseline, 57% of subjects had ≥2 point pain reduction on the numeric rating scale (NRS), 60% had ≥10 point functional improvement on the ODI, and 81% had ≥0.03-point health-related quality of life improvement on the EQ-5D (EuroQOL health-related quality of life measure) index. Mid-study, the surgical implantation technique was modified from two lateral incisions at the L3 level, to one single midline incision at the L4 level from which both leads are inserted towards the L2 medial branches as they cross the L3 transverse process. This new technique mitigated the high incidence of lead fractures from fascial shearing forces observed during the study and remained the approach of choice throughout the most recent prospective, multi-center, randomized, active sham-controlled ReActiv8-B trial.54
The ReActiv8-B (https://clinicaltrials.gov/study/NCT02577354) was a pivotal, sham-controlled Randomized Control Trial (RCT) IDE study with the US FDA. This trial included 204 patients with CLBP (VAS ≥6 cm; ODI ≥21 points), despite conservative medical management consisting of medications and physical therapy, with evidence of MF neuromuscular impairment demonstrated by positive PIT, and no indications for spine surgery. Patients were evenly randomized to sham stimulation vs therapeutic stimulation and those undergoing sham stimulation crossed over to therapeutic levels after 120 days. Responders were defined as those with at least 30% VAS pain rating recall without changes in medication prescribed and taken for back pain. At 120 days, difference among responder proportions was inconclusive; however, pre-specified cumulative proportion of responder analysis of the primary outcome data and mean group difference in VAS improvement were significant in favor of treatment. Moreover, the mean group differences in the secondary outcome measures were also statistically significant and clinically meaningful.
Following crossover, improvements across all outcome measures increased through 1 year, with efficacy outcomes consistently showing significant (P<0.0001) and clinically meaningful improvements compared to baseline, and 64% of participants having experienced 50% or greater improvement. 52% reported resolution of CLBP (LBP-VAS <2.5 cm) and 69% of subjects reported at least a 15-point improvement in ODI.54 There were no lead migrations noted from the study. The serious adverse event incidence was 8/204 (3.9%) and all occurred prior to the 120-day follow-up period. Six pocket-related infections resolved following device removal and antibiotics, one intraoperative upper airway obstruction occurred and was resolved, and one participant developed an ongoing non-radicular patch of numbness on the surface of his thigh. Notably, no lead migrations were observed. The overall safety profile compared favorably with that of other implantable neurostimulator therapies for chronic pain.
The published data through 3-years demonstrated that 77% of subjects had ≥50% CLBP relief, 63% had at least a 20-point reduction in ODI, 56% had both, 83% had at least one of the two, and 67% had resolution of CLBP (VAS ≤2.5 cm).55,56 Mean EQ-5D improved from 0.585 to 0.805, approaching the US population norm. A total of 71% had voluntarily discontinued (49%) or reduced (22%) opioid intake. The side-by-side comparison of completed-cases analysis (N=133) and imputed intention-to-treat analysis (N=204) showed a relatively small difference, which did not impact the statistical significance or clinical relevance of the results.
In 2021, Mitchell et al published four-year completers-analysis for 34 of the 53 patients from the Reactiv8-A study, demonstrating durable improvements in NRS, ODI, and EQ-5D scores and persistent treatment satisfaction.74 At four years, 73% of patients experienced clinically meaningful improvement with ≥2 points on NRS, 76% with ≥10 points on ODI, and 62% of patients reported clinically important improvement in both NRS and ODI. A notable 97% of patients reported that they were “Very Satisfied” with the treatment.
Also in 2021, Thomson et al reported the two-year completers-analysis of a prospective post-market (https://clinicaltrials.gov/study/NCT01985230) follow-up of 42 patients treated for longstanding (13.7±10.2 years) mechanical CLBP.75 Of the 37 patients completing 2-year follow-up, 57% experienced a greater than 50% improvement in pain; 65% were reporting mild to negligible pain (NRS≤3), and 51% had an improvement by 15-points or more in ODI with 43% having a 20-point or greater improvement.
The most recent article concerning the ReActiv8-B pivotal RCT published by Gilligan et al56 in 2024 reported the prospective five-year longitudinal study follow-up comparing outcomes of patients with CLBP from the pivotal study who were implanted with the ReActiv8 system. This report demonstrated the continued durability of effectiveness in patients with refractory CLBP associated with MF dysfunction treated with restorative neurostimulation. At five years (N=126 completers), CLBP VAS had improved from 7.3 to 2.4 cm (−4.9; 95% CI: −5.3 to −4.5 cm; P<0.0001), and 71.8% of participants had a reduction by at least 50%. The ODI improved from 39.1 to 16.5 (−22.7; 95% CI: −25.4 to −20.8; P<0.0001), and 61.1% of participants had reduction by at least 20-points. The EQ-5D-5L index improved from 0.585 to 0.807 (0.231; 95% CI: 0.195 to 0.267; P<0.0001) again approaching population normals without LBP. Although completed-case results were attenuated by the mixed-effects model, conclusions and statistical significance were maintained. Of 52 subjects who were on opioids at baseline and attended a fifth-year visit, 46% completely discontinued and 23% decreased opioid intake. No lead migrations were observed. The authors concluded that over a five-year period, restorative neurostimulation provided clinically substantial and durable benefits with a favorable safety profile in patients with refractory CLBP associated with MF muscle dysfunction.
Numerous systematic reviews have examined the effectiveness of various therapies for CLBP, but none have specifically focused on MF stimulation, whether delivered percutaneously or via an implanted device. Recently, Copley et al49 conducted a comprehensive systematic review and meta-analysis to assess whether electrical stimulation of the MF muscle can override pain-related inhibition and improve function and stability in CLBP patients. Their analysis included six studies, 5 of 6 were restorative neurostimulation, and the total number of 419 participants. The follow-up periods ranged from 1.5 to 48 months. The results showed a weighted pooled mean pain reduction by 2.9 units, with a 95% confidence interval of 0.6 to 5.2 units. Additionally, the probability of achieving a pain reduction by more than 2 units was 0.84 (ranging from 0.68 to 0.98). The reported weighted pooled mean effect for ODI was an improvement of 14.7 units (95% CI: 11.1–18.3) with an estimated probability of an improved ODI score (>10 points) was 0.88 (0.71–0.99). Notably, the meta-analysis indicated that greater pain reduction over time was associated with longer follow-up periods.
Most recently, in 2025, another randomized controlled trial, Restorative Neurostimulation Therapy Compared to Optimal Medical Management: A Randomized Evaluation (RESTORE) for the Treatment of Chronic Mechanical Low Back Pain due to Multifidus,50 provided compelling Level I evidence as a superior treatment for CLBP due to multifidus dysfunction (https://clinicaltrials.gov/study/NCT04803214). The objective in the RESTORE trial was, at one year, to evaluate change in ODI and other patient-reported outcomes between a randomized group who received optimal medical management (OMM) and a randomized group who received ReActiv8. At the one-year follow-up, the ReActiv8 group (n=94 completers) reported significant functional improvements (ie, lower ODI scores) than those in the OMM group (n=94 completers) (ODI: −20.0±1.8 vs −3.0 ± 1.3, p<0.001). Furthermore, the pain ratings from the ReActiv8 group reduced significantly where the OMM group remained largely unchanged (NRS: −3.6±0.3 vs −0.6±0.2, p<0.001).
Practical Implications
Utilizing restorative neurostimulation targeting the MF to treat CLBP requires close coordination between various clinical and administrative team members to accurately identify appropriate patients and obtain insurance approval. Additionally, clear and consistent messaging from all clinicians can help set patient expectations with regards to the time frame for symptom improvement, spectrum of possible recovery trajectories, and importance of patient compliance with ongoing physical therapy.
Where Does Restorative Neurostimulation Fit?
Restorative neurostimulation can be helpful in the management of patients with CLBP in multiple settings. Physicians practicing in interventional pain clinics as well as physical medicine and rehabilitation clinics, where many patients with CLBP seek care, may consider discussing restorative neurostimulation as a therapeutic option if symptoms persist despite conservative care and physical examination testing confirms MF dysfunction. Spine surgeons may also consider it an additional tool in the management of patients with CLBP who are not candidates for spinal fusion surgery. Implantation of the neurostimulator may be performed at an ambulatory surgical center or a hospital operating room setting.
Multidisciplinary Approach
A multidisciplinary approach combining input from pain management physicians, physical therapists, spine surgeons, and pain psychologists is useful for identifying optimal candidates for neuromodulation, including restorative neurostimulation. Ideally, these teams can coordinate closely on patients. For example, a pain management physician who sees a patient with CLBP and suspects MF dysfunction based on physical exam and/or imaging studies may subsequently send the patient to physical therapy to work on motor control retraining.76 Depending on imaging findings, they may also choose to send the patient for consultation with a spine surgery team to evaluate their candidacy for surgical options. If the pain persists despite physical therapy, then the pain management physician and spine surgery team may make a joint decision weighing the patient’s likelihood of long-term benefit with traditional surgical options against the option of neurostimulation. A pain psychologist can also be helpful in confirming the patient’s candidacy for an implanted device. With a multidisciplinary approach, careful patient selection can improve overall outcomes.
Documentation
Although among payors there is no consensus on documentation requirements for prior approval, at a minimum it needs to support alignment of medical history and diagnosis with the indication for restorative neurostimulation in the presence of MF dysfunction. Best documentation practices include a complete medical history including other treatments that have been tried and failed, documentation of physical therapy sessions and compliance with those sessions, physical examination and aberrant movement patterns observed, results of the PIT and MLT, imaging demonstrating MF atrophy and fatty infiltration and/or a surgical consultation that rules out a surgical indication. Although little data exists to support its implementation, psychological evaluation may be considered to confirm implantation readiness.
No Trial Stimulation
Due to the rehabilitative mechanism of action of restorative neurostimulation, clinical benefits accrue gradually over many months albeit at various timing from early to later response rates. Therefore, a trial period intended to enrich patient selection and predict future responders is futile within what is considered an acceptable trial duration. Furthermore, patients subject to invasive treatments for chronic pain are known to experience a considerable placebo response that may last for several months. The overall high rate of responders with the patient selection criteria discussed herein diminishes any cost/effectiveness potential from doing a trial, even if an effective one were feasible. At the time of surgical implantation of the device, the implanter does confirm that stimulation causes contraction of the MF muscles prior to implanting the pulse generator, and this confirmation step constitutes a physiologic trial of the device’s ability to trigger MF contractions.77
Individual Recovery Trajectories
Many putative degenerative mechanisms are involved in the development of CLBP each with its own time course.11 The underlying pathophysiologic processes of MF dysfunction and related functional segmental instability is best characterized through medical history and physical exam. Disease pathways and expressions of each of these mechanisms differ among patients and consequently, no two recovery trajectories are alike. For this reason, patients respond to restorative neurostimulation in different manners. There are fast responders, slow responders, and everything in between. Although the responsiveness does not appear to be related to multifidus volume or to the extent of the pathology seen on imaging, the exact mechanism as to why the patients are responding in different manners is a subject of ongoing evaluation. While individual recovery trajectories vary, the typical result with restoration of neuromuscular control and return of functional segmental stability is universal and has been demonstrated in multiple RCT and real-world evidence studies.
Patient Expectations and Compliance
Due to the variable pace of recovery, managing patient expectations is an important component to success of restorative neurostimulation. Since in most cases the condition has developed over many years, it cannot be expected that the underlying pathology should normalize within a few days or weeks. Therefore, patients should be prepared to be compliant and to expect noticeable improvement typically at 6–8 weeks after activation with ongoing improvement that may continue over the course of the first 6–12 or even 18 months of therapy. Even the initial reactivation of the deep muscle fibers does not result in immediate return to normal movement patterns. With robust return of proprioception and engagement over time, functional improvements are seen first, followed by improvement in pain. Patients who are counseled on AMI will have a greater understanding of the restorative mechanism of the therapy, and therefore their recovery timeline. Studies of the therapy to date have not shown any signs of tolerance or habituation to the therapy through up to five-years of follow-up.
Resolution of Pain
Over half of patients report resolution of pain 1 year into therapy, and several who attained pain resolution that persisted even after a stimulation holiday without relapse have requested device removal. Before honoring such requests for removal, it is important that patients be fully informed about the implications and potential outcomes. LBP relapse after prior episode resolution is common, and if the device does not cause patient discomfort, explantation should not be recommended. Some experienced implanting physicians have asked their patients to turn off the stimulation for a period of 1–6 months and re-evaluate their functional spine stability before explanting for reason of successful pain resolution.
Other Practical Considerations and Implications
Activation and programming of the system to start the therapy occurs approximately 2 weeks after the implant procedure. The first result patients typically experience is increased lumbar stability resulting in increased activity levels or functional improvement rather than immediate pain relief. Even after 6 weeks of increased stability and improved function, patients may not yet report relevant pain relief. After 3 months, most patients report initial pain reduction, although the individual onset is subject to variation as described above with early or late responders.
In addition to starting the stimulation, it is recommended that guided physical therapy and home exercises learned from the conservative treatment period be performed. Once familiar with the therapy regimen, a well-prepared patient can start motor control training at a low intensity with the goal of reintegrating the MF – now accessible through neurostimulation – into daily motion.
Discussion
As the evidence base supporting lumbosacral spine restorative neurostimulation has grown, interest has also grown in applying restorative neurostimulation to various other chronic pain conditions. Future studies could examine whether axial neck and thoracic spine pain indications may also derive meaningful treatment outcomes, as cervical and thoracic spine anatomy exhibit similarities to that of the lumbar spine. However, we should not let these potentially new indications draw our focus away from the bird in hand. Restorative neurostimulation therapy was developed and studied specifically for patients suffering from severe, disabling, refractory, nonsurgical mechanical CLBP due to MF dysfunction without effective, durable treatment options and we must primarily continue to focus on improving selection and treatment effectiveness for this specific patient population and important unmet clinical need.
Although pain medicine physicians may try various diagnostic procedures such as focused epidural injections or facet injections to help identify the pain source, most patients with back pain often have multiple pain generators. There exists a large population of patients who are not candidates for spine surgery, but who continue to experience refractory symptoms despite repeated injections, therapy, and pharmacological management. In this gray zone lies tremendous opportunity for treatment of patients who have been diagnosed with MF dysfunction, lumbar region where no viable option existed previously. For carefully selected patients in this population, restorative neurostimulation has been demonstrated to be an appropriate treatment option based on the totality of evidence using this treatment therapy for treating this specific patient population.
There may be some utility for restorative neurostimulation both pre-operatively and post-operatively in patients undergoing lumbar spinal fusion surgery. Pre-operatively, neurostimulation could potentially be used in an attempt to restore motor control and strengthen to the remaining muscle, or potentially reverse degenerative changes in an effort to postpone or avoid surgery.12 Post-operatively, adjacent segment disease is a common sequela of spinal fusion surgery, in which physiologic stresses which pre-operatively were distributed across the fused levels are primarily displaced post-operatively to the levels directly above and below the fusion, ultimately causing degeneration of these levels.78 Future studies may evaluate the benefits of using neurostimulation to improve functional stability either to treat adjacent segment disease or even pre-emptively to potentially deter or postpone the onset of adjacent segment disease.
What Further Research is Required?
In addition to exploring the advantages of restorative neurostimulation for new indications, future research should primarily aim to better characterize different phenotypes of CLBP and clarify how these different groups respond to restorative neurostimulation. Some patients become pain-free once motor control to the deep MF is restored and continue to do well even if the stimulator is no longer used. After a prolonged period without regression, a subset of this group may eventually request device removal. A small group requires continuous stimulation and regress if neurostimulation is ceased, likely because their restorative processes are not (yet) able to overcome the existing maladaptive changes that have occurred.
Some work has already attempted to classify different groups within those who suffer from CLBP. High-impact chronic pain (HICP) describes a subset of patients with CLBP associated with substantial restriction in work, social, and self-care activities participation for 6 or more months.79,80 Several algorithms based on patient responses to various validated tools have been proposed to identify these patients.80,81 Compared to those with low-impact chronic pain, patients with HICP have over double the annual overall and spine-related per person healthcare costs, use opioid medications at a rate almost 4 times as high, and on average use over 5 times the morphine equivalent daily dose.80 Overall, they comprise about 40% of patients with chronic spinal pain,80 representing >10 million American adults.82 Previous work has identified four long-term course trajectories of LBP – “no or occasional mild”, “persistent mild”, “persistent severe”, and “fluctuating between mild and severe pain” – with findings showing that trajectory membership and respective presence of LBP remain relatively fixed over time.83,84 Therefore, those with HICP are likely to continue to have significant restrictions in their quality of life, higher healthcare costs, and higher opioid use – making them a high-yield population to study from both a healthcare and economic standpoint. Considering the heterogeneity of health- and quality-of-life-related outcome measures within the chronic pain population, correctly identifying and targeting the HICP population in clinical research and practice can lead to an improved understanding of chronic pain risk factors, causes, and consequences, and allow for the development and advancement of tailored pain interventions. Restorative neurostimulation’s ability to help shift patients from more severe to less severe trajectories positions this technology well to provide better and etiology-specific therapies for patients with CLBP.
Disclosure
CJG provides consulting for Iliad Lifesciences, Saluda, Persica, Presidio, and Biotronik. He serves on the Board of Directors of the International Neuromodulation Society and serves as Editor-in-Chief of Pain Practice. He also reports stock from Mainstay Medical. DWL reports consultation for Boston Scientific, Abbott, Mainstay Medical, Johnson & Johnson, Vertos Medical, Biotronik. ML reports personal fees from Mainstay Medical, outside the submitted work. MA reports personal fees for travel, presentation, and consulting from Mainstay Medical. The authors report no other conflicts of interest in this work.
References
1. James SL, Theadom A, Ellenbogen RG, et al. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019;18(1):56–87. doi:10.1016/S1474-4422(18)30415-0
2. Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008;8(1):8–20. doi:10.1016/j.spinee.2007.10.005
3. Meucci RD, Fassa AG, Faria NMX. Prevalence of chronic low back pain: systematic review. Rev Saude Publica. 2015; 49:S0034–89102015000100420. doi:10.1590/S0034-8910.2015049005874
4. Shala R. Chronic nociplastic and neuropathic pain: how do they differentiate? Pain. 2022;163(6):e786–e786. doi:10.1097/j.pain.0000000000002576
5. Baron R, Binder A, Attal N, Casale R, Dickenson AH, Treede RD. Neuropathic low back pain in clinical practice. Eur J Pain. 2016;20(6):861–873. doi:10.1002/ejp.838
6. Russo M, Deckers K, Eldabe S, et al. Muscle control and non-specific chronic low back pain. Neuromodulation. 2018;21(1):1–9. doi:10.1111/ner.12738
7. Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383–389. doi:10.1097/00002517-199212000-00001
8. Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J Spinal Disord. 1992;5(4):390–397. doi:10.1097/00002517-199212000-00002
9. Ebenbichler GR, Oddsson LI E, Kollmitzer J, Erim Z. Sensory-motor control of the lower back: implications for rehabilitation. Med Sci Sports Exercise. 2001;33(11):1889–1898. doi:10.1097/00005768-200111000-00014
10. Hodges PW, Bailey JF, Fortin M, Battié MC. Paraspinal muscle imaging measurements for common spinal disorders: review and consensus-based recommendations from the ISSLS degenerative spinal phenotypes group. Eur Spine J. 2021;30(12):3428–3441. doi:10.1007/s00586-021-06990-2
11. Hodges PW, Danneels L. Changes in structure and function of the back muscles in low back pain: different time points, observations, and mechanisms. J Orthop Sports Phys Ther. 2019;49(6):464–476. doi:10.2519/jospt.2019.8827
12. Freeman MD, Woodham MA, Woodham AW. The role of the lumbar multifidus in chronic low back pain: a review. Pm&r. 2010;2(2):142–146. doi:10.1016/j.pmrj.2009.11.006
13. Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W. Nociplastic pain: towards an understanding of prevalent pain conditions. Lancet. 2021;397(10289):2098–2110. doi:10.1016/S0140-6736(21)00392-5
14. Chimenti RL, Frey-Law LA, Sluka KA. A mechanism-based approach to physical therapist management of pain. Phys Ther. 2018;98(5):302–314. doi:10.1093/ptj/pzy030
15. Bogduk N. On the definitions and physiology of back pain, referred pain, and radicular pain. Pain. 2009;147(1):17–19. doi:10.1016/j.pain.2009.08.020
16. Deyo RA, Weinstein JN. Low back pain. N Engl J Med. 2001;344(5):363–370. doi:10.1056/NEJM200102013440508
17. Förster M, Mahn F, Gockel U, et al. Axial low back pain: one painful area – many perceptions and mechanisms. PLoS One. 2013;8(7):e68273. doi:10.1371/journal.pone.0068273
18. Abdel Shaheed C, Maher CG, Williams KA, McLachlan AJ. Efficacy and tolerability of muscle relaxants for low back pain: systematic review and meta-analysis. Eur J Pain. 2017;21(2):228–237. doi:10.1002/ejp.907
19. Boff TA, Pasinato F, Ben ÂJ, Bosmans JE, van Tulder M, Carregaro RL. Effectiveness of spinal manipulation and myofascial release compared with spinal manipulation alone on health-related outcomes in individuals with non-specific low back pain: randomized controlled trial. Physiotherapy. 2020;107:71–80. doi:10.1016/j.physio.2019.11.002
20. Saragiotto BT, de Almeida MO, Yamato TP, Maher CG. Multidisciplinary biopsychosocial rehabilitation for nonspecific chronic low back pain. Phys Ther. 2016;96(6):759–763. doi:10.2522/ptj.20150359
21. Chou R, Deyo R, Friedly J, et al. Nonpharmacologic therapies for low back pain: a systematic review for an American College of Physicians clinical practice guideline. Ann Intern Med. 2017;166(7):493. doi:10.7326/M16-2459
22. Enke O, New HA, New CH, et al. Anticonvulsants in the treatment of low back pain and lumbar radicular pain: a systematic review and meta-analysis. CMAJ. 2018;190(26):E786–E793. doi:10.1503/cmaj.171333
23. Rathmell JP. A 50-year-old man with chronic low back pain. JAMA. 2008;299(17):2066. doi:10.1001/jama.299.13.jrr80002
24. Rubinstein SM, de Zoete A, van Middelkoop M, Assendelft WJJ, de Boer MR, van Tulder MW. Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain: systematic review and meta-analysis of randomised controlled trials. BMJ. 2019;l689. doi:10.1136/bmj.l689
25. Saragiotto BT, Machado GC, Ferreira ML, Pinheiro MB, Abdel Shaheed C, Maher CG. Paracetamol for low back pain. In:Cochrane Database of Systematic Reviews. Vol. 2019. Cochrane Back and Neck Group; 2016. doi:10.1002/14651858.CD012230
26. Abdel Shaheed C, Maher CG, Williams KA, Day R, McLachlan AJ. Efficacy, tolerability, and dose-dependent effects of opioid analgesics for low back pain: a systematic review and meta-analysis. JAMA Intern Med. 2016;176(7):958. doi:10.1001/jamainternmed.2016.1251
27. Urquhart DM, Wluka AE, van Tulder M, et al. Efficacy of low-dose amitriptyline for chronic low back pain: a randomized clinical trial. JAMA Intern Med. 2018;178(11):1474. doi:10.1001/jamainternmed.2018.4222
28. Deer TR, Mekhail N, Provenzano D, et al. The appropriate use of neurostimulation of the spinal cord and peripheral nervous system for the treatment of chronic pain and ischemic diseases: the neuromodulation appropriateness consensus committee. Neuromodulation. 2014;17(6):515–550. doi:10.1111/ner.12208
29. Thomson S, Huygen F, Prangnell S, et al. Appropriate referral and selection of patients with chronic pain for spinal cord stimulation: european consensus recommendations and e‐health tool. Eur J Pain. 2020;24(6):1169–1181. doi:10.1002/ejp.1562
30. Kim C, Gottschalk L, Eng C, Ward S, Lieber R. 160. The multifidus muscle is the strongest stabilizer of the lumbar spine. Spine J. 2007;7(5):76S. doi:10.1016/j.spinee.2007.07.188
31. Shahidi B, Hubbard JC, Gibbons MC, et al. Lumbar multifidus muscle degenerates in individuals with chronic degenerative lumbar spine pathology: Multifidus degeneration in low back pain. J Orthop Res. 2017;35(12):2700–2706. doi:10.1002/jor.23597
32. Teichtahl AJ, Urquhart DM, Wang Y, et al. Fat infiltration of paraspinal muscles is associated with low back pain, disability, and structural abnormalities in community-based adults. Spine J. 2015;15(7):1593–1601. doi:10.1016/j.spinee.2015.03.039
33. Rosatelli AL, Ravichandiran K, Agur AM. Three-dimensional study of the musculotendinous architecture of lumbar multifidus and its functional implications. Clin Anat. 2008;21(6):539–546. doi:10.1002/ca.20659
34. Lepley AS, Lepley LK. Mechanisms of arthrogenic muscle inhibition. J Sport Rehab. 2022;31(6):707–716. doi:10.1123/jsr.2020-0479
35. Hodges PW, Galea MP, Holm S, Holm AK. Corticomotor excitability of back muscles is affected by intervertebral disc lesion in pigs. Eur J Neurosci. 2009;29(7):1490–1500. doi:10.1111/j.1460-9568.2009.06670.x
36. Brumagne S, Diers M, Danneels L, Moseley GL, Hodges PW. Neuroplasticity of sensorimotor control in low back pain. J Orthop Sports Phys Ther. 2019;49(6):402–414. doi:10.2519/jospt.2019.8489
37. Kiesel KB, Butler RJ, Duckworth A, et al. Experimentally induced pain alters the EMG activity of the lumbar multifidus in asymptomatic subjects. Man Ther. 2012;17(3):236–240. doi:10.1016/j.math.2012.01.008
38. Hodges PW, Moseley GL, Gabrielsson A, Gandevia SC. Experimental muscle pain changes feedforward postural responses of the trunk muscles. Exp Brain Res. 2003;151(2):262–271. doi:10.1007/s00221-003-1457-x
39. Moseley GL, Nicholas MK, Hodges PW. Does anticipation of back pain predispose to back trouble? Brain. 2004;127(10):2339–2347. doi:10.1093/brain/awh248
40. Moseley GL, Nicholas MK, Hodges PW. Pain differs from non-painful attention-demanding or stressful tasks in its effect on postural control patterns of trunk muscles. Exp Brain Res. 2004;156(1):64–71. doi:10.1007/s00221-003-1766-0
41. Massé-Alarie H, Beaulieu LD, Preuss R, Schneider C. Corticomotor control of lumbar multifidus muscles is impaired in chronic low back pain: concurrent evidence from ultrasound imaging and double-pulse transcranial magnetic stimulation. Exp Brain Res. 2016;234(4):1033–1045. doi:10.1007/s00221-015-4528-x
42. Elgueta-Cancino E, Schabrun S, Hodges P. Is the organization of the primary motor cortex in low back pain related to pain, movement, and/or sensation? Clin J Pain. 2018;34(3):207–216. doi:10.1097/AJP.0000000000000535
43. Tsao H, Danneels LA, Hodges PW. ISSLS prize winner: smudging the motor brain in young adults with recurrent low back pain. Spine. 2011;36(21):1721–1727. doi:10.1097/BRS.0b013e31821c4267
44. Willemink MJ, van Es HW, Helmhout PH, Diederik AL, Kelder JC, van Heesewijk JPM. The effects of dynamic isolated lumbar extensor training on lumbar multifidus functional cross-sectional area and functional status of patients with chronic nonspecific low back pain. Spine. 2012;37(26):E1651–E1658. doi:10.1097/BRS.0b013e318274fb2f
45. Rice DA, McNair PJ. Quadriceps arthrogenic muscle inhibition: neural mechanisms and treatment perspectives. Semin Arthritis Rheumatism. 2010;40(3):250–266. doi:10.1016/j.semarthrit.2009.10.001
46. Imoto AM, Peccin S, Almeida GJM, Saconato H, Án A. Effectiveness of electrical stimulation on rehabilitation after ligament and meniscal injuries: a systematic review. Sao Paulo Med J. 2011;129(6):414–423. doi:10.1590/S1516-31802011000600008
47. Stevens JE, Mizner RL, Snyder-Mackler L. Quadriceps strength and volitional activation before and after total knee arthroplasty for osteoarthritis. J Orthop Res. 2003;21(5):775–779. doi:10.1016/S0736-0266(03)00052-4
48. Stevens-Lapsley JE, Balter JE, Wolfe P, Eckhoff DG, Kohrt WM. Early neuromuscular electrical stimulation to improve quadriceps muscle strength after total knee arthroplasty: a randomized controlled trial. Phys Ther. 2012;92(2):210–226. doi:10.2522/ptj.20110124
49. Copley S, Batterham A, Shah A, et al. Systematic review and meta-analysis of stimulation of the medial branch of the lumbar dorsal rami for the treatment of chronic low back pain. Neuromodulation. 2024;27(8):1285–1293. doi:10.1016/j.neurom.2024.08.002
50. Schwab F, Mekhail N, Patel KV, et al. Restorative neurostimulation therapy compared to optimal medical management: a randomized evaluation (RESTORE) for the treatment of chronic mechanical low back pain due to multifidus dysfunction. Pain Ther. 2025;14(1):401–423. doi:10.1007/s40122-024-00689-0
51. Kim KM, Croy T, Hertel J, Saliba S. Effects of neuromuscular electrical stimulation after anterior cruciate ligament reconstruction on quadriceps strength, function, and patient-oriented outcomes: a systematic review. J Orthop Sports Phys Ther. 2010;40(7):383–391. doi:10.2519/jospt.2010.3184
52. Sions JM, Crippen DC, Hicks GE, Alroumi AM, Manal TJ, Pohlig RT. Exploring neuromuscular electrical stimulation intensity effects on multifidus muscle activity in adults with chronic low back pain: an ultrasound imaging–informed investigation. Clin Med Insights Arthritis Musculoskelet Disord. 2019;12:117954411984957. doi:10.1177/1179544119849570
53. Deckers K, De Smedt K, van Buyten JP, et al. Chronic low back pain: restoration of dynamic stability. Neuromodulation. 2015;18(6):478–486. doi:10.1111/ner.12275
54. Gilligan C, Volschenk W, Russo M, et al. An implantable restorative-neurostimulator for refractory mechanical chronic low back pain: a randomized sham-controlled clinical trial. Pain. 2021;162(10):2486–2498. doi:10.1097/j.pain.0000000000002258
55. Gilligan C, Volschenk W, Russo M, et al. Three-year durability of restorative neurostimulation effectiveness in patients with chronic low back pain and multifidus muscle dysfunction. Neuromodulation. 2022:S1094715922012545. doi:10.1016/j.neurom.2022.08.457.
56. Gilligan C, Volschenk W, Russo M, et al. Five-year longitudinal follow-up of restorative neurostimulation shows durability of effectiveness in patients with refractory chronic low back pain associated with multifidus muscle dysfunction. Neuromodulation. 2024;27(5):930–943. doi:10.1016/j.neurom.2024.01.006
57. FDA. ReActiv8 - PMA Approval. 2020. Available from: https://fda.report/PMA/P190021.
58. Denteneer L, Stassijns G, De Hertogh W, Truijen S, Van Daele U. Inter- and intrarater reliability of clinical tests associated with functional lumbar segmental instability and motor control impairment in patients with low back pain: a systematic review. Arch Phys Med Rehabil. 2017;98(1):151–164.e6. doi:10.1016/j.apmr.2016.07.020
59. Hebert JJ, Koppenhaver SL, Magel JS, Fritz JM. The relationship of transversus abdominis and lumbar multifidus activation and prognostic factors for clinical success with a stabilization exercise program: a cross-sectional study. Arch Phys Med Rehabil. 2010;91(1):78–85. doi:10.1016/j.apmr.2009.08.146
60. Sung W, Hicks GE, Ebaugh D, et al. Individuals with and without low back pain use different motor control strategies to achieve spinal stiffness during the prone instability test. J Orthop Sports Phys Ther. 2019;49(12):899–907. doi:10.2519/jospt.2019.8577
61. Kiesel KB, Uhl TL, Underwood FB, Rodd DW, Nitz AJ. Measurement of lumbar multifidus muscle contraction with rehabilitative ultrasound imaging. Manual Ther. 2007;12(2):161–166. doi:10.1016/j.math.2006.06.011
62. Hebert JJ, Koppenhaver SL, Teyhen DS, Walker BF, Fritz JM. The evaluation of lumbar multifidus muscle function via palpation: reliability and validity of a new clinical test. Spine J. 2015;15(6):1196–1202. doi:10.1016/j.spinee.2013.08.056
63. Larivière C, Gagnon DH, Preuss R. Structural remodeling of the lumbar multifidus, thoracolumbar fascia and lateral abdominal wall perimuscular connective tissues: medium-term test-retest reliability of ultrasound measures. J Bodywork Movement Ther. 2021;27:265–273. doi:10.1016/j.jbmt.2021.03.017
64. Rahmani N, Kiani A, Mohseni-Bandpei MA, Abdollahi I. Multifidus muscle size in adolescents with and without back pain using ultrasonography. J Bodyw Mov Ther. 2018;22(1):147–151. doi:10.1016/j.jbmt.2017.05.016
65. Faur C, Patrascu JM, Haragus H, Anglitoiu B. Correlation between multifidus fatty atrophy and lumbar disc degeneration in low back pain. BMC Musculoskelet Disord. 2019;20(1):414. doi:10.1186/s12891-019-2786-7
66. Hides JA, Belavý DL, Stanton W, et al. Magnetic resonance imaging assessment of trunk muscles during prolonged bed rest. Spine. 2007;32(15):1687–1692. doi:10.1097/BRS.0b013e318074c386
67. Le Cara EC, Marcus RL, Dempsey AR, Hoffman MD, Hebert JJ. Morphology versus function: the relationship between lumbar multifidus intramuscular adipose tissue and muscle function among patients with low back pain. Arch Phys Med Rehabil. 2014;95(10):1846–1852. doi:10.1016/j.apmr.2014.04.019
68. Rezazadeh F, Taheri N, Okhravi SM, Hosseini SM. The relationship between cross-sectional area of multifidus muscle and disability index in patients with chronic non-specific low back pain. Musculoskeletal Sci Pract. 2019;42:1–5. doi:10.1016/j.msksp.2019.03.005
69. Goubert D, De Pauw R, Meeus M, et al. Lumbar muscle structure and function in chronic versus recurrent low back pain: a cross-sectional study. Spine J. 2017;17(9):1285–1296. doi:10.1016/j.spinee.2017.04.025
70. Sions JM, Elliott JM, Pohlig RT, Hicks GE. Trunk muscle characteristics of the multifidi, erector spinae, psoas, and quadratus lumborum in older adults with and without chronic low back pain. J Orthop Sports Phys Ther. 2017;47(3):173–179. doi:10.2519/jospt.2017.7002
71. Hides JA, Lambrecht G, Richardson CA, et al. The effects of rehabilitation on the muscles of the trunk following prolonged bed rest. Eur Spine J. 2011;20(5):808–818. doi:10.1007/s00586-010-1491-x
72. Kjaer P, Bendix T, Sorensen JS, Korsholm L, Leboeuf-Yde C. Are MRI-defined fat infiltrations in the multifidus muscles associated with low back pain? BMC Med. 2007;5(1):2. doi:10.1186/1741-7015-5-2
73. Deckers K, Adam AA, Adam N, Rens A, Adam N. Resolving chronic non-specific low back pain requires a new approach. Neromodulation. 2013;16:e176.
74. Mitchell B, Deckers K, De Smedt K, et al. Durability of the therapeutic effect of restorative neurostimulation for refractory chronic low back pain. Neuromodulation. 2021;24(6):1024–1032. doi:10.1111/ner.13477
75. Thomson S, Chawla R, Love-Jones S, et al. Restorative Neurostimulation For Chronic Mechanical Low Back Pain: Results From A Prospective Multi-Centre Longitudinal Cohort. Pain Ther. 2021;10(2):1451–1465. doi:10.1007/s40122-021-00307-3
76. Tsao H, Druitt TR, Schollum TM, Hodges PW. Motor training of the lumbar paraspinal muscles induces immediate changes in motor coordination in patients with recurrent low back pain. J Pain. 2010;11(11):1120–1128. doi:10.1016/j.jpain.2010.02.004
77. Eldabe S, Duarte RV, Gulve A, et al. Does a screening trial for spinal cord stimulation in patients with chronic pain of neuropathic origin have clinical utility and cost-effectiveness (TRIAL-STIM)? A randomised controlled trial. Pain. 2020;161(12):2820–2829. doi:10.1097/j.pain.0000000000001977
78. Wang T, Ding W. Risk factors for adjacent segment degeneration after posterior lumbar fusion surgery in treatment for degenerative lumbar disorders: a meta-analysis. J Orthop Surg Res. 2020;15(1):582. doi:10.1186/s13018-020-02032-7
79. Interagency Pain Research Coordinating Committee. National Pain Strategy. Office of the Assistant Secretary for Health, US Department of Health and Human Services. Available from: https://www.iprcc.nih.gov/node/5/national-pain-strategy-report.
80. Herman PM, Broten N, Lavelle TA, Sorbero ME, Coulter ID. Health care costs and opioid use associated with high-impact chronic spinal pain in the United States. Spine. 2019;44(16):1154–1161. doi:10.1097/BRS.0000000000003033
81. Von Korff M, DeBar LL, Krebs EE, Kerns RD, Deyo RA, Keefe FJ. Graded chronic pain scale revised: mild, bothersome, and high-impact chronic pain. Pain. 2020;161(3):651–661. doi:10.1097/j.pain.0000000000001758
82. Pitcher MH, Von Korff M, Bushnell MC, Porter L. Prevalence and Profile of High-Impact Chronic Pain in the United States. J Pain. 2019;20(2):146–160. doi:10.1016/j.jpain.2018.07.006
83. Chen Y, Campbell P, Strauss VY, Foster NE, Jordan KP, Dunn KM. Trajectories and predictors of the long-term course of low back pain: cohort study with 5-year follow-up. Pain. 2018;159(2):252–260. doi:10.1097/j.pain.0000000000001097
84. Dunn KM, Campbell P, Jordan KP. Long-term trajectories of back pain: cohort study with 7-year follow-up. BMJ Open. 2013;3(12):e003838. doi:10.1136/bmjopen-2013-003838
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Restorative Neurostimulation: A Clinical Guide for Therapy Adoption
Chakravarthy K, Lee D, Tram J, Sheth S, Heros R, Manion S, Patel V, Kiesel K, Ghandour Y, Gilligan C
Journal of Pain Research 2022, 15:1759-1774
Published Date: 20 June 2022