Back to Journals » International Journal of General Medicine » Volume 19
Restaging pN Classification in Early Gastric Cancer with Inadequate Lymph Node Retrieval: Multi-Institutional Development and Prognostic Validation of a Revised Staging System
Authors Nie X ![]() , Li G, Liu Z, Ke B, Yang Z, Ye Z, Zhang T, Wang X, Yang K
, Li G, Liu Z, Ke B, Yang Z, Ye Z, Zhang T, Wang X, Yang K ![]() , You Q, Zhou T, Li Y, Zhang R, Ren P, Wang W, Tian Y, Zhang K, Deng J
, You Q, Zhou T, Li Y, Zhang R, Ren P, Wang W, Tian Y, Zhang K, Deng J
Received 12 January 2026
Accepted for publication 8 May 2026
Published 13 May 2026 Volume 2026:19 595436
DOI https://doi.org/10.2147/IJGM.S595436
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ching-Hsien Chen
Xinyang Nie,1 Gang Li,2 Zhiqiang Liu,3 Bin Ke,1 Zuli Yang,4 Zaisheng Ye,5 Tao Zhang,6 Xiangyu Wang,7 Kun Yang,8 Qi You,9 Tong Zhou,10 Yong Li,11 Rupeng Zhang,1 Peng Ren,12 Wei Wang,13 Yantao Tian,14 Kecheng Zhang,15 Jingyu Deng1
1Department of Gastric Surgery, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin Key Laboratory of Digestive Cancer, Tianjin’s Clinical Research Center for Cancer, Tianjin, 300060, People’s Republic of China; 2Department of General Surgery, The Affiliated Cancer Hospital of Nanjing Medical University & Jiangsu Cancer Hospital & Jiangsu Institute of Cancer Research, Nanjing, Jiangsu, 210009, People’s Republic of China; 3Department of Gastric Surgery, Anyang Tumor Hospital, Anyang, Henan, 455000, People’s Republic of China; 4Department of Gastrointestinal Surgery, Department of General Surgery, The Sixth Affiliated Hospital, Sun Yat-Sen University, Guangzhou, Guangdong, 510655, People’s Republic of China; 5Department of Gastric Surgical Oncology, Clinical Oncology School of Fujian Medical University, Fujian Cancer Hospital (Fujian Branch of Fudan University Shanghai Cancer Center), Fuzhou, Fujian, 350000, People’s Republic of China; 6Department of Gastric Cancer, Cancer Hospital of Dalian University of Technology (Liaoning Cancer Hospital & Institute), Shenyang, Liaoning, 110801, People’s Republic of China; 7Department of Gastrointestinal Surgery, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou, Fujian, 350015, People’s Republic of China; 8Department of General Surgery & Laboratory of Gastric Cancer, State Key Laboratory of Biotherapy/ Collaborative Innovation Center of Biotherapy and Cancer Center, West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, People’s Republic of China; 9Department of Gastroenterological Surgery, Harbin Medical University Cancer Hospital, Harbin Medical University, Harbin, Heilongjiang, 150081, People’s Republic of China; 10The Second Department of Gastrointestinal Surgery, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, 637000, People’s Republic of China; 11Department of Gastrointestinal Surgery, Department of General Surgery, Guangdong Provincial People’s Hospital, Southern Medical University, Guangzhou, Guangdong, 510080, People’s Republic of China; 12Department of Esophageal Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Tianjin’s Clinical Research Center for Cancer, Tianjin, Tianjin, 300060, People’s Republic of China; 13Department of Gastric Surgery, Sun Yat-Sen University Cancer Center, Guangzhou, 510060, People’s Republic of China; 14Department of Pancreatic and Gastric Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, People’s Republic of China; 15Department of General Surgery, the First Medical Center, Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China
Correspondence: Jingyu Deng, Department of Gastric Surgery, Tianjin Medical University Cancer Institute & Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin, Tianjin Key Laboratory of Digestive Cancer, Tianjin’s Clinical Research Center for Cancer, Tianjin, 300060, People’s Republic of China, Email [email protected] Kecheng Zhang, Department of General Surgery, the First Medical Center, Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China, Email [email protected]
Objective: This study aimed to propose and validate a new and practical lymph node (LN) staging strategy to mitigate staging migration due to examined LN (ELN) retrieval and improve the accuracy of prognostic evaluation for early gastric cancer (EGC) patients.
Background: EGC patients often face staging inaccuracies due to inadequate ELNs, as there is no clear standard for ELN retrieval requirements.
Methods: From an initial cohort of 7001 EGC patients across fifteen large institutions in China, 6566 eligible patients were included as the training and validation cohort after applying predefined exclusion criteria. We analyzed these data to determine the optimal cutoff value for the number of ELNs, construct a prediction model, and propose a new LN staging method distinct from that of the latest AJCC guidelines. Subsequently, 2094 patients (from 2326 with survival data available in the multicenter dataset) and 1944 patients (from 5262 initially retrieved from the SEER database after exclusions) were included as independent test cohorts to evaluate model performance, including the correlation between ELNs and metastatic LNs (MLNs) and survival differences.
Results: This study found that ≤ 20 ELNs were inadequate for accurate LN evaluation in EGC patients. In the test cohort, MLNs was positively associated with ELNs. A model was constructed, and accurate MLNs could be displayed after correction for patients with inadequate ELNs. Survival analysis revealed significant differences between patients with different pNM (pN modified) stages in both the multicenter test cohort and the SEER test cohort.
Conclusion: Model-corrected pNM staging may improve staging migration and survival prediction than the AJCC staging, showing great clinical applicability for EGC patients with ELN ≤ 20. A flowchart outlines a study on early gastric cancer patients, examining lymph nodes and metastasis risks.A study of 6566 early gastric cancer (EGC) patients across 15 Chinese centers determined the optimal examined lymph node (ELN) cutoff for lymph node metastasis (LNM) risk. Data was split into training and validation cohorts. A logistic regression model predicted LNM, correcting for insufficient ELNs and predicting metastatic lymph nodes (MLNs). 2094 multicenter and 1944 SEER EGC patients with survival data were tested. AJCC staging was redefined based on corrected ELNs/MLNs, grouped into PN stages and survival analysis was performed comparing pre- and post-correction differences.
Keywords: stomach, neoplasm, lymph node, metastasis, prognosis
Introduction
Gastric cancer (GC) is a prevalent malignant tumor worldwide. According to the latest global reports, there are nearly one million new cases of GC, making it the fifth most common cancer worldwide. Tragically, approximately 650,000 individuals succumb to GC, ranking it as the fifth leading cause of cancer-related deaths, following lung cancer, colorectal cancer, liver cancer and breast cancer.1 Compared with those in Western countries, the number of GC cases and deaths in China remains high, accounting for approximately half of the number of GC cases and deaths in the world.2 Due to the use of relatively rigorous screening programs, the proportion of patients identified as having early gastric cancer (EGC) is increasing among patients with GC. According to the definition provided by the Japanese Society of Gastrointestinal Endoscopy in 1962, EGC is a lesion confined to the mucosa and submucosa regardless of the status of lymph node metastasis (LNM).3 Some patients with EGC can be treated via endoscopic resection. The current clear criterion for endoscopic resection is a differentiated mucosal tumor less than 2 cm in diameter without ulceration. However, in most cases, surgical treatment is still necessary and will bring the best prognosis to EGC patients.4
Research findings on the survival outcomes of EGC patients have not yielded consistent results. Most Eastern studies have reported that the 5-year overall survival (OS) rate of EGC patients is more than 90%. In contrast, Western studies have shown a broader range of 5-year OS rates, varying from 68% to 92%.5,6 The prognosis of EGC patients is influenced by two major factors: LNM and depth of wall invasion. However, only LNM has been demonstrated to be an independent prognostic factor.7 Previous statistical analyses have indicated an LNM rate of approximately 20% among EGC patients, highlighting the importance of adequate examination of examined lymph nodes (ELNs) to thoroughly assess metastatic lymph nodes (MLNs).8–10 While ELNs count positively correlates with MLNs detection, quantitative ELN thresholds remain controversial.11,12 The American Joint Committee on Cancer (AJCC)13 and the Chinese Society of Clinical Oncology (CSCO)14 recommend >16 ELNs for accurate pN staging, while recent large-scale studies have suggested that >30 is optimal in GC.15 We previously demonstrated that <16 ELNs caused pN underestimation and significantly reduced overall survival.16 Similarly, <10-15 ELNs increased.17 However, these thresholds are mainly derived from advanced GC. In EGC, the prevalence of LNM is lower and the number of MLNs is fewer, which paradoxically necessitates a higher number of ELNs to reliably detect all metastatic nodes. Currently, no clear ELNs requirement exists specifically for EGC. Given the critical role of accurate LNM evaluation in determining postoperative pTNM staging per AJCC guidelines and its strong prognostic implications, inadequate ELNs retrieval may lead to pN misclassification and subsequent bias in survival assessment, ie., stage migration. Therefore, we aim to define the optimal ELNs cutoff value for EGC, construct and validate an accurate prediction model for MLNs, and more importantly, apply this model to mathematically correct the pN category in patients with inadequate ELNs retrieval, achieving a more precise assessment of patient prognosis.
Materials and Methods
Patients and Eligibility Criteria
This research is a multicenter retrospective study. The clinicopathological data of 7001 patients of EGC from fifteen large medical centers of China included Tianjin Medical University Cancer Institute and Hospital, The General Hospital of the People’s Liberation Army, Xijing Hospital of Air Force Medical University, Sun Yat-sen University Cancer Hospital, Jiangsu Cancer Hospital, Anyang Cancer Hospital of Henan Province, Sixth Affiliated Hospital of Sun Yat-sen University, Fujian Cancer Hospital, The Cancer Institute and Hospital of Chinese Academy of Medical Sciences, Liaoning Cancer Hospital, Fujian Provincial Hospital, Affiliated Hospital of North Sichuan Medical College, Affiliated Cancer Hospital of Harbin Medical University, West China Hospital of Sichuan University, and Guangdong Provincial People’s Hospital were collected between 2005 to 2015.
Patients satisfying the following criteria were included: underwent radical gastrectomy for GC, pathologically confirmed EGC adenocarcinoma, and none accepted neoadjuvant therapy. The patients would be excluded if the following conditions occurred: accompanied by relevant missing data, accompanied by other synchronous malignancy, presence of residual GC, and no performing endoscopic submucosal dissection or resection biopsy. Missing data for key variables were below 5%, and complete case analysis was applied. Ultimately, a total of 6566 patients for data analysis was included, and they were divided into training and validation cohorts according to a certain proportion. Additionally, a total of 2326 patients with survival data from Tianjin Medical University Cancer Institute and Hospital, Sun Yat-sen University Cancer Hospital, Sixth Affiliated Hospital of Sun Yat-sen University, Fujian Cancer Hospital, and Anyang Cancer Hospital of Henan Province were collected. After screening and excluding missing data and lost follow-up data, a total of 2094 EGC patients from multicenter with complete data were used to survival analysis as the internal test cohort. The flow diagram of the selection process was presented in Additional file 1: Figure S1A–B. All patients provided informed consent for the use of their data for scientific purposes prior to surgery. The study protocol adhered to the regulations of the Declaration of Helsinki (as revised in Edinburgh 2000) and ethical approval was obtained from the Tianjin Medical University cancer institute and hospital institutional review board (bc2022220).
Retrieval of Patients from the SEER Database
We conducted an analysis of the SEER database to identify GC cases that met similar inclusion criteria to those mentioned above, spanning from January 2000 to December 2019. Initially, 5262 cases of EGC were retrieved. Cases with incomplete information regarding age, tumor location, tumor size, differentiation type, depth of tumor invasion, MLNs, ELNs were excluded. This refined dataset, eventually comprising 1944 cases, was designated as the SEER test cohort. The flow diagram of the selection process was presented in Additional file 1: Figure S1C.
Construction and Verification of the Prediction Model
A total of 6566 patients were randomly divided into training cohort (70%) and validation cohort (30%). The random split was performed using SPSS with a fixed random seed and stratification by center. According to the results of postoperative pathological examination, EGC patients in different groups were divided into positive lymph node metastasis (PLNM) group and negative lymph node metastasis (NLNM) group. In this study, the optimal cut-off value (corresponding to the maximum value of the Yoden’s index) of ELN corresponding to the prediction of LNM in this data is used to define whether the ELN count is sufficient. The number of adequate ELNs defined and selected in this study was 20, and the results of the Yoden’s index for different ELN counts are presented in Table S1.
The independent risk factors of LNM were determined by multivariate analysis. Variables with P<0.05 in univariate analysis were entered into multivariate binary logistic regression using forward stepwise selection. Based on the β coefficient of independent risk variables, a logistic prediction model was established to predict the probability of LNM. The performance of the model was verified by drawing nomogram, ROC and calibration graphs. In addition, the artificial neural network (ANN) model was used to include logistics variables for verification. Internal validation was performed using the held-out validation cohort (30% of data), and no cross-validation was applied. The ANN architecture consisted of an input layer with 10 predictors, two hidden layers (5 nodes each), and an output layer with 2 nodes (PLNM and NLNM). The softmax transfer function and scaled conjugate gradient training algorithm were applied. The training group was used to train the neural network, while the verification group was used to evaluate the final neural network, and to construct the topological hierarchical structure of the neural network model. The final neural network fitting results were represented using the normalized importance percentage graph and a bar diagram was drawn. Finally, the area under the operating characteristic curve (AUC) of the recipients of the model was calculated to compare and evaluate diagnostic accuracy using the chi-square test. The superiority of the fitting prediction model was evaluated by plotting the calibration curve, and the net benefit rate was evaluated by the DCA curve.
Construction of Modified pN Stage and Survival Analysis
The multicenter test cohort and the SEER test cohort were included, and the patients with survival data were substituted into the model for survival test. Among them, OS was the study endpoint which defined as the time interval from the date of surgery to the last date of follow-up or death. The correction procedure was performed as follows: (a) Obtain the predicted probability of LNM (P) from the logistic model; (b) For patients with ELNs ≤20, calculate the expected number of MLNs in unexamined lymph nodes: (20 – actuals ELN) × P; (c) Calculate predicted total MLNs = actual MLNs + (20 – actual ELN) × P; (d) Assign pNM stage according to AJCC 8th edition pN categories (N0: 0, N1: 1‑2, N2: 3‑6, N3a: 7‑15, N3b: ≥16) based on corrected MLNs. (Figure S2A) It should be noted that the corrected MLN count and pNM stage are model-derived estimates rather than directly observed pathological data. The correlation between ELNs and MLNs and the difference in survival will be further analyzed before and after correction.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics (version 26.0; IBM Corp, New York, NY). χ2 test or Fisher exact test was used for univariate analysis to evaluate the correlation between clinicopathological characteristics and LN involvement of patients with EGC. The factors with 2-tailed P < 0.05 were included in the multivariate analysis. Multivariate binary logistic regression analysis was used to further screen independent risk factors for LNM in patients with EGC. R statistical software (version 4.3.1, the R Foundation for Statistical Computing) was used to draw nomogram, ROC, and calibration graphs. Comparisons of the predictive value of each model were performed using the likelihood-ratio test, Akaike Information Criterion, and Bayesian Information Criterion by R statistical software. A model with low AIC, low BIC, and high likelihood-ratio score had a better predictive value. The accepted level of significance was P less than 0.05. The correlation between ELNs and MLNs was calculated by fitting linear model using Origin 2024 (Origin, Northampton, MA, USA). The Kaplan–Meier method was used for graphical representation of the OS curves and the Log rank test was used to assess the differences between the survival curves, and the relative graphs were generated using GraphPad Prism 9 (GraphPad, San Diego, CA). For all Cox regression models, the proportional hazards assumption was tested using Schoenfeld residuals (all P>0.05). The ANN model and further statistical analyses were performed using IBM SPSS Statistics software.
Results
Clinical and Pathological Characteristics in the Multicenter Dataset
The following is a summary of the clinicopathological characteristics of the 6566 EGC patients included in this study. Overall, 70.61% of the patients were male, while 29.39% were female. Patients were separated into groups of individuals who were less than 65 years old (71.29%) and those who were more than 65 years old (28.71%) based on their ages at the time of operation. The tumors were mainly located in the lower 1/3 (56.88%), followed by the upper 1/3 (21.06%), middle 1/3 (15.93%), and more than 1/3 of the stomach (6.12%). Tumors with a maximum diameter less than 2 cm accounted for 55.92%, and those with a maximum diameter greater than 2 cm accounted for 44.08%. According to the degree of differentiation, the tumors were divided into moderate or good type (39.95%) and undifferentiated or poor type (60.05%). According to the Lauren classification, the patients were divided into intestinal type (44.36%), diffuse type (31.69%) and mixed type (23.94%). There were 2846 patients with pT1a stage EGC (43.34%) and 3720 patients with pT1b stage EGC (56.66%). According to the pN stage, the patients were divided into 5 groups that were consistent with the TNM stage: pN0 (84.01%), pN1 (9.05%), pN2 (4.84%), pN3a (1.71%) and pN3b (0.40%). There were 367 patients with perineural invasion (5.59%) and 612 patients with lymphovascular invasion (9.32%). After grouping by the number of ELNs, 3743 patients had > 20 ELNs, accounting for 57.01% of the total (Table S2). The data were randomly divided into a training cohort (4597) and a validation cohort (1969) at a ratio of approximately 7:3, and a comparison of clinicopathological factors between the cohorts is shown in Table S3. The results showed that there were no statistically significant differences in the variables between the two cohorts.
Construction and Validation of a Predictive Model for LNM
Univariate analysis was performed on the risk of LNM in the training cohort of EGC patients. Sex, tumor location, tumor size, differentiation type, Lauren type, pT stage, ELN count (bounded by 20), perineural invasion and lymphovascular invasion were significantly associated with LN involvement in patients with EGC and were thus included in multivariate analysis. Multivariate analysis using a multiple logistic regression model confirmed that sex (P=0.003), tumor location (P=0.001), tumor size (P<0.001), differentiation type (P<0.001), pT stage (P<0.001), ELN count (bounded by 20, P<0.001), and lymphovascular invasion (P<0.001) were found to be independent predictors of LNM (Table 1 and Figure 1A).
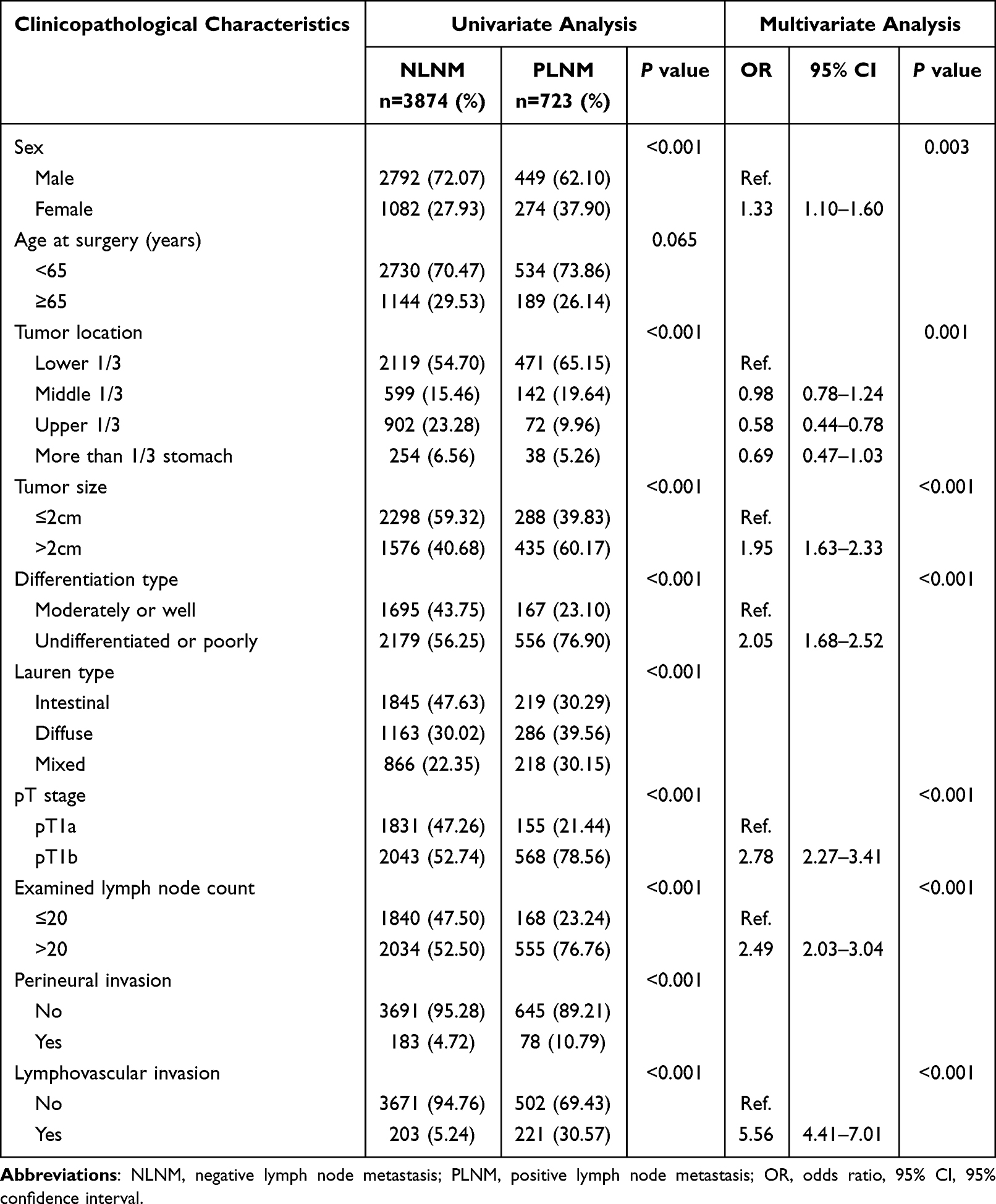 |
Table 1 Univariate and Multivariate Analysis of LNM Risk in Training Cohort |
 |
Figure 1 Construction and verification of LNM prediction model: (A) Nomogram graph of risk factors for LNM from multivariate logistic regression analysis in training cohort; (B) Receiver operating characteristic curve of prediction model for LNM of training cohort; (C) Receiver operating characteristic curve of prediction model for LNM of validation cohort; (D) The calibration curve of LNM prediction model in the training cohort; (E) The calibration curve of LNM prediction model in the validation cohort; (F) Receiver operating characteristic curve based on artificial neural network (ANN) model; (G) ANN model for predicting LNM in EGC. |
A logistic prediction model was established to predict the probability of LNM based on the β coefficients of the aforementioned seven independent risk variables that were identified via multivariate analysis. The ROC curve was plotted using the training cohort, and the AUC, which was 0.789 (95% CI, 0.771–0.807), was used to evaluate the discriminant ability of the model. The accuracy of the prediction model was confirmed using the validation cohort, and the AUC was 0.775 (95% CI, 0.748–0.802). The calibration curve and DCA curve were generated at the same time, confirming the model’s superiority (Figure 1B–E). We also established an ANN model and assessed its ability to predict LNM in EGC patients. The structure of the established ANN model was presented and affected by nine important predictors, of which the number of ELNs (bound by 20) was a relatively high factor. The predictive model demonstrated the AUC was 0.781 (95% CI, 0.767–0.797) (Figure 1F and G).
Survival Analysis and LN Correlation of EGC Patients After Model Correction
The multicenter dataset with survival data and the SEER validation dataset were used as the test cohorts to test the predictive efficacy of the model, and the specific clinicopathological characteristics are shown in Tables S4–S5. First, we found that patients with > 20 ELNs had better survival in the survival analysis of the two datasets (all P<0.0001). Moreover, according to the β coefficient of the independent variables of the logistic regression model, the probability of LNM (P) was calculated (Figure S2B). After further correction for EGC patients with insufficient ELNs, the predicted MLN number and pNM stage were obtained by using the formula. In the multicenter test cohort, survival analysis of patients with different stages showed that the 5-year OS rates of patients with pN0, pN1, and pN2 + pN3 disease were 97.96%, 96.26%, and 89.84%, respectively. However, the difference between the independent stages was not statistically significant. The corrected 5-year OS rates of pN0M, pN1M and pN2M + pN3M patients were 98.22%, 97.12% and 89.78%, respectively, and there were significant differences between different stages (pN0M vs. pN1M, P=0.0012; pN0M vs. pN2M + pN3M, P=0.0044; pN1M vs. pN2M + pN3M, P<0.0001). This trend was also consistent in the SEER test cohort, and the difference between different pNM intervals after correction was highly significant (all P<0.0001) (Figure 2).
 |
Figure 2 The survival analysis in multicenter test cohort and SEER test cohort: (A) Kaplan-Meier curves of EGC patients with ELN ≤ 20 and ELN > 20 in multicenter test cohort; (B) Kaplan-Meier curves of EGC patients with different pN stages in multicenter test cohort; (C) Kaplan-Meier curves of EGC patients with different pNM stages after correction in multicenter test cohort; (D) Kaplan-Meier curves of EGC patients with ELN ≤ 20 and ELN > 20 in SEER test cohort; (E) Kaplan-Meier curves of EGC patients with different pN stages in SEER test cohort; (F) Kaplan-Meier curves of EGC patients with different pNM stages after correction in SEER test cohort. |
In this study, the number of ELNs and the number of MLNs in EGC patients were linearly fitted, and the correlation trend between the two was judged by the coefficient (Y=aX+b) of the linear equation. The number of ELNs was positively associated with the number of MLNs in EGC patients in both the multicenter test cohort (a=0.020) and the SEER test cohort (a=0.044). After model correction, the number of MLNs was nearly unrelated to the number of ELNs in the two datasets (multicenter cohort: a=−0.003, SEER cohort: a=−0.004). When the condition was limited to patients with insufficient ELNs, the number of MLNs approached a fixed value after correction (multicenter cohort: b=1.588, SEER cohort: b=1.695), and the linear slope of the correlation analysis was lower than that before (multicenter cohort: a=−0.005 vs. a=0.038, SEER cohort: a=−0.015 vs. a=0.036). Finally, in LNM patients with ≤ 20 ELNs, the above trend was more significant after model correction (multicenter cohort: a=0.057, b=3.495 vs. a=0.149, b=0.839; SEER cohort: a=−0.005, b=3.567 vs. a=0.077, b=1.312) (Figure 3).
 |
Figure 3 The correlation between the counts of ELNs and MLNs of EGC patients: (A) shows total EGC patients in multicenter test cohort; (B) shows EGC patients with LNM in multicenter test cohort; (C) shows EGC patients with LNM and ELN ≤20 in multicenter test cohort; (D) shows total EGC patients in SEER test cohort; (E) shows EGC patients with LNM in SEER test cohort; (F) shows EGC patients with LNM and ELN ≤20 in SEER test cohort. |
Evaluation and Validation of the Model
Based on the different pN stages, we calculated the TNM and modified TNM stages of the patients, and the survival curves are shown in Figure 4A–D. There were some differences in the number of patients with different TNM stages before and after correction in the multicenter dataset (IA vs. IAM: 1655 vs. 1172, IB vs. IBM: 249 vs. 700, IIA vs. IIAM: 141 vs. 164, IIB vs. IIBM: 40 vs. 48, IIIB vs. IIIBM: 9 vs. 10) of the SEER dataset (IA vs. IAM: 1592 vs. 462, IB vs. IBM: 222 vs. 1244, IIA vs. IIAM: 98 vs. 197, IIB vs. IIBM: 26 vs. 35, IIIB vs. IIIBM: 6 vs. 6). Moreover, the survival rates of patients with different TNM stages also exhibited different degrees of change before and after correction. In the multicenter test cohort, the 5-year OS rates of patients with stage IA, IB, IIA, IIB and IIIB disease were 97.96%, 96.26%, 92.71%, 83.17%, and 74.07%, respectively. After correction, the 5-year OS rates of patients with IAM, IBM, IIAM, IIBM and IIIBM were 98.22%, 97.12%, 93.64%, 78.04% and 74.07%, respectively. In the SEER test cohort, the 5-year OS rates of patients with stage IA, IB, IIA, IIB and IIIB disease were 73.62%, 61.90%, 50.33%, 60.00%, and 16.67%, respectively, and those of patients with stage IAM, IBM, IIAM, IIBM and IIIBM disease were 79.38%, 70.79%, 55.57%, 49.67% and 16.67%, respectively (Figure 4E and F). The results showed varying increases in the 5-year OS rates for patients with stage IA, IB, and IIA after model adjustment, whereas stages IIB and IIIB show varying decreases in 5-year OS.
 |
Figure 4 Survival analysis in test cohorts: (A) Kaplan-Meier curves of EGC patients with different 8th AJCC staging groups in multicenter test cohort; (B) Kaplan-Meier curves of EGC patients with different modified staging groups in multicenter test cohort; (C) Bar chart of the number of EGC patients in different stages before and after correction in multicenter test cohort; (D) The bar chart of 5-year survival rate of EGC patients with different stages before and after correction in multicenter test cohort; (E) Kaplan-Meier curves of EGC patients with different 8th AJCC staging groups in SEER test cohort; (F) Kaplan-Meier curves of EGC patients with different modified staging groups in SEER test cohort; (G) Bar chart of the number of EGC patients in different stages before and after correction in SEER test cohort; (H) The bar chart of 5-year survival rate of EGC patients with different stages before and after correction in SEER test cohort. |
Finally, we performed Cox regression analysis of the different grouping methods, including grouping by pN stage according to the AJCC guidelines and pNM stage, to identify the best grouping method for predicting survival efficacy. Cox regression analysis of the AIC, BIC, and −2log-likelihood values revealed that the pNM stage had lower AIC, BIC, and −2log-likelihood values than did the pN stage in both the multicenter cohort (AIC, pN stage vs. pNM stage = 486.13 vs. 484.04; BIC, pN stage vs. pNM stage = 487.93 vs. 485.84; −2log-likelihood value, pN stage vs. pNM stage = 484.12 vs. 482.04; all P<0.0001) and the SEER cohort (AIC, pN stage vs. pNM stage = 10,257.93 vs. 10229.10; BIC, pN stage vs. pNM stage = 10,262.50 vs. 10233.67; −2log-likelihood value, pN stage vs. pNM stage = 10,255.93 vs. 10227.10; all P<0.0001) (Table 2). Therefore, we considered that the pNM stage had better discrimination ability than the pN stage given the evident improvement in the accuracy of the prognostic prediction of patients with EGC.
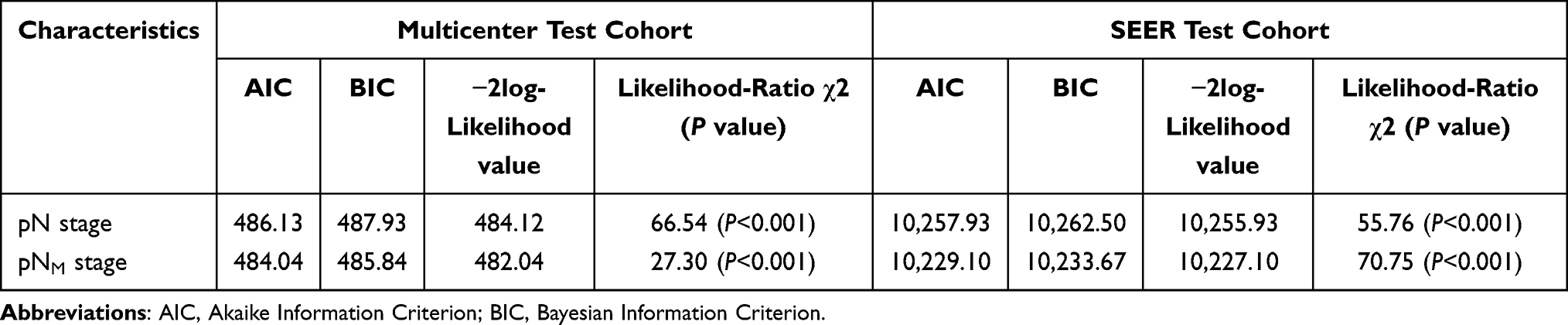 |
Table 2 Prognostic Performance of Different LN Staging System in Test Cohorts |
Discussion
LNM can strongly affect the prognosis of patients with GC. Currently, this has become an important topic in the field of GC that cannot be ignored, especially when EGC is considered by most people to be a curable malignant disease.18,19 Studies have shown that in patients with EGC, the 5-year and 10-year survival rates of patients who undergo gastrectomy and extended (D2) LN dissection are 2–3% greater than those of patients who undergo localized (D1) LN dissection.20 Hence, ensuring an adequate number of ELNs in EGC patients, determining the presence of LNM, and accurately assessing the number of MLNs are crucial for evaluating postoperative pTNM stage and prognosis. Based on the analysis of a large-scale multicenter cohort of EGC patients in China, we developed a LNM prediction model and validated it across Eastern and Western populations, showing its potential cross-ethnic applicability. We further propose a novel LN staging system based on the 8th edition AJCC guidelines, which may offer improved staging accuracy and prognostic stratification capacity compared with the current AJCC pN system, thereby potentially enhancing precision management for EGC.
Previous studies have shown that insufficient ELNs may lead to evaluation bias in pN staging,15,16 but there is no standard definition of sufficient ELNs in EGC. Based on large-scale data analysis, this study determined that 20 ELNs serves as the optimal cut-off value for assessing LNM risk in EGC which was greater than the 16 in patients with GC.16 Considering that patients with EGC had fewer MLNs than did those with GC, more ELNs were needed to ensure the detection of MLNs, which was also in line with this trend. Then, we analyzed the clinicopathological data of 6566 EGC patients from fifteen medical centers in South and North China, which represented the basic disease information and general therapeutic level of EGC in China. We found that sex, tumor location, tumor size, differentiation type, pT stage, and lymphovascular invasion were important risk factors for LNM in patients with EGC. These results were also consistent with those of other small-scale studies.21–23 Additionally, this study suggests for the first time that insufficient ELNs represent a critical independent risk factor for LNM. This result has also been confirmed in ANN analysis. Given the better performance of the logistic algorithm in our comparative assessment, we finally chose to build the prediction model using logistic regression.
Based on the independent risk factors included in the above analysis, we recognized that patients with an adequate number of ELNs were more likely to develop LNM, which also meant that patients with insufficient ELNs had more undetected potential MLNs. An incorrect metastatic LN count will lead to pN and even pTNM stage migration directly, ultimately leading to incorrect survival expectations.16,24,25 This view has been proposed as early as in previous studies, but there is no complete data to support this phenomenon in patients with EGC. Therefore, we constructed an LNM prediction model and observed its good predictive performance through a highly representative high-capacity data cohort. Based on the logistic regression model, we calculated the expected LNM probability, identified the MLNs in the potential unexamined LNs, and finally obtained the pNM staging. To test the performance of the model and pNM staging, we fitted a multicenter validation database with survival data from China and the SEER database, which cover the EGC patients in Eastern and Western countries to a great extent, respectively. In different validation cohorts, it was shown that EGC patients with < 20 ELNs had worse survival, which also showed that insufficient ELNs could be used as an important prognostic factor. Comparatively, the corrected pNM classification proposed in this study had considerable resemblance to the pN classification proposed by the 8th edition of the AJCC guidelines, with the exception that patients with <20 ELNs were promoted to one higher nodal class. In fact, this change had a great impact on the evaluation of the patients’ prognosis. The use of pNM staging method appeared to better reflect the survival differences of patients with different stages than pN classification, which was reflected in both the multicenter test cohort and the SEER test cohort. This suggests that even if there are differences in patient characteristics and survival outcomes between the Chinese and SEER datasets, the proposed classification method may be applicable to EGC patients in different populations, although further validation is needed.
Moreover, we found that the number of MLNs in patients with EGC was positively associated with the number of ELNs, and this trend was not obvious after model correction. This difference was more significant in the subgroup. When the condition was limited to patients with insufficient ELNs and those with PLNM, the number of MLNs increased after model correction than before and does not change significantly or even tends to be stable with the change of ELN. This suggests that the calibration model might help identify more MLNs and obtain more accurate pNM staging. Compared with that of patients in the normal pN category, the OS distribution of EGC patients in each subgroup (N0M, N1M, and N2M+N3M) in the pNM category was more distinct, and the overall number of MLNs was more stable, which indicated that the pNM category had improved discrimination and homogeneity in this dataset. Finally, we used multiple indices, including the likelihood ratio test, AIC, and BIC, to evaluate and compare the prognostic value of different LN staging systems. After comparison, this staging method showed better model fit than the 8th edition of AJCC classification guidelines in both populations, suggesting potential clinical utility. Therefore, this model could be more effective and widely used in the clinic, such as in areas where high-quality gastrectomy cannot be effectively performed (ELNs≤20) or where resources are limited, as it may provide more accurate individualized staging and OS prediction. However, given its model-derived nature, prospective validation in independent cohorts is required before routine clinical adoption.
Although this study has potential clinical value, several limitations should be acknowledged. First, the prediction model was developed based on a Chinese multicenter dataset, which may have resulted in incomplete inclusion of relevant variables. Second, given the relatively small number of EGC patients and the long study period required to accrue sufficient cases, temporal heterogeneity in surgical techniques and perioperative management may have influenced the results. Third, it is difficult to achieve full consistency between the variables in the multicenter validation cohort and those in the SEER database. Although the trends of the results are similar, independent external validation is still necessary. Next, we plan to collaborate with more medical centers worldwide to further refine the model and confirm the robustness of our findings using large, diverse populations with adequate variable information. The ultimate goal is to provide additional reference for future updates of the AJCC staging guidelines and potentially inform amendments to the pN staging criteria.
Conclusion
In conclusion, this study suggests that insufficient ELNs are an important contributor to LNM in patients with EGC. Through the development of a prediction model and reclassification of EGC patients with fewer than 20 ELNs, a new pNM category is proposed as a model‑derived correction, which may reduce staging migration and could improve survival outcome accuracy. Our findings were generally validated in large datasets from both Eastern and Western populations, but given the estimated nature of the correction, further external validation is needed before confirming broad clinical applicability.
Data Sharing Statement
Due to ethical restrictions, the raw data cannot be made publicly available. However, de-identified data may be obtained from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The experiments related to human specimens were performed according to the Institutional Research Ethics Committee of Tianjin Medical University Cancer Institute and Hospital (Tianjin, China) (Ethics Approval License: bc2022220).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Scientific and technological innovation 2030 ‘Research on precise diagnosis and treatment strategy of gastric cancer based on new molecular typing system,’ a major project in ‘Research on prevention and treatment of cancer, cardiovascular, cerebrovascular, respiratory and metabolic diseases’ (2023ZD0501500).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024. doi:10.3322/caac.21834
2. Nie Y, Wu K, Yu J, et al. A global burden of gastric cancer: the major impact of China. Expert Rev Gastroenterol Hepatol. 2017;11(7):651–13. doi:10.1080/17474124.2017.1312342
3. S H, F J, Rl S, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2021;71(3). doi:10.3322/caac.21660
4. Kakeji Y, Ishikawa T, Suzuki S, et al. A retrospective 5-year survival analysis of surgically resected gastric cancer cases from the Japanese Gastric Cancer Association nationwide registry (2001–2013). Gastric Cancer. 2022;25(6):1082–1093. doi:10.1007/s10120-022-01317-6
5. Espinel J. Treatment modalities for early gastric cancer. WJGE. 2015;7(12):1062. doi:10.4253/wjge.v7.i12.1062
6. Bollschweiler E. Treatment of early gastric cancer in the Western World. WJG. 2014;20(19):5672. doi:10.3748/wjg.v20.i19.5672
7. Okajima K. Prognostic factors of gastric cancer patients. a study by univariate and multivariate analysis. Jpn J Gastroenterol Surg, Nihon Shokaki Geka Gakkai zasshi. 1997;30(3):700–711. doi:10.5833/jjgs.30.700
8. Asakawa Y, Ohtaka M, Maekawa S, et al. Stratifying the risk of lymph node metastasis in undifferentiated-type early gastric cancer. World J Gastroenterol. 2015;21(9):2683–2692. doi:10.3748/wjg.v21.i9.2683
9. Roviello F, Rossi S, Marrelli D, et al. Number of lymph node metastases and its prognostic significance in early gastric cancer: a multicenter Italian study. J Surg Oncol. 2006;94(4):275–280. doi:10.1002/jso.20566
10. Zhao X, Cai A, Xi H, et al. Predictive factors for lymph node metastasis in undifferentiated early gastric cancer: a systematic review and meta-analysis. J Gastrointest Surg. 2017;21(4):700–711. doi:10.1007/s11605-017-3364-7
11. de Manzoni G, Verlato G, Roviello F, et al. The new TNM classification of lymph node metastasis minimises stage migration problems in gastric cancer patients. Brit J Cancer. 2002;87(2):171–174.
12. Bouvier AM, Haas O, Piard F, Roignot P, Bonithon-Kopp C, Faivre J. How many nodes must be examined to accurately stage gastric carcinomas? Results from a population based study. Cancer. 2002;94(11):2862–2866. doi:10.1002/cncr.10550
13. H SI, Palis B, Langdon-Embry M, Ajani J, Sano T. Validation of the 8th Edition of the AJCC TNM staging system for gastric cancer using the national cancer database. Ann Surg Oncol. 2017;24(12):3683–3691. doi:10.1245/s10434-017-6078-x
14. Wang FH, Zhang XT, Li YF, et al. The Chinese Society of Clinical Oncology (CSCO): clinical guidelines for the diagnosis and treatment of gastric cancer, 2021. Cancer Commun. 2021;41(8):747–795. doi:10.1002/cac2.12193
15. Sano T, Coit DG, Kim HH, et al. Proposal of a new stage grouping of gastric cancer for TNM classification: international Gastric Cancer Association staging project. Gastric Cancer. 2017;20(2):217–225. doi:10.1007/s10120-016-0601-9
16. Deng J, Zhang R, Pan Y, et al. Comparison of the staging of regional lymph nodes using the sixth and seventh editions of the tumor-node-metastasis (TNM) classification system for the evaluation of overall survival in gastric cancer patients: findings of a case-control analysis involving a single institution in China. Surgery. 2014;156(1):64–74. doi:10.1016/j.surg.2014.03.020
17. Schwarz RE, Smith DD. Clinical impact of lymphadenectomy extent in resectable gastric cancer of advanced stage. Ann Surg Oncol. 2007;14(2):317–328. doi:10.1245/s10434-006-9218-2
18. Brisinda G, Crocco A, Tomaiuolo P, Santullo F, Mazzari A, Vanella S. Extended or limited lymph node dissection? A gastric cancer surgical dilemma. Ann Surg. 2012;256(6):e30–31. doi:10.1097/SLA.0b013e31827693c3
19. Brisinda G, Chiarello MM, Crocco A, Adams NJ, Fransvea P, Vanella S. Postoperative mortality and morbidity after D2 lymphadenectomy for gastric cancer: a retrospective cohort study. World J Gastroenterol. 2022;28(3):381–398. doi:10.3748/wjg.v28.i3.381
20. An L, Gaowa S, Cheng H, Hou M. Long-term outcomes comparison of endoscopic resection with gastrectomy for treatment of early gastric cancer: a systematic review and meta-analysis. Front Oncol. 2019;9:725. doi:10.3389/fonc.2019.00725
21. Liu C, Zhang R, Lu Y, et al. Prognostic role of lymphatic vessel invasion in early gastric cancer: a retrospective study of 188 cases. Surg Oncol. 2010;19(1):4–10. doi:10.1016/j.suronc.2008.10.003
22. Folli S, Morgagni P, Roviello F, et al. Risk factors for lymph node metastases and their prognostic significance in early gastric cancer (EGC) for the Italian Research Group for Gastric Cancer (IRGGC). Jpn J Clin Oncol. 2001;31(10):495–499. doi:10.1093/jjco/hye107
23. Asakawa Y. Stratifying the risk of lymph node metastasis in undifferentiated-type early gastric cancer. WJG. 2015;21(9):2683. doi:10.3748/wjg.v21.i9.2683
24. Deng J, Liu J, Wang W, et al. Validation of clinical significance of examined lymph node count for accurate prognostic evaluation of gastric cancer for the eighth edition of the American Joint Committee on Cancer (AJCC) TNM staging system. Chin J Cancer Res. 2018;30(5):477–491. doi:10.21147/j.issn.1000-9604.2018.05.01
25. Deng J, Liang H, Sun D, Zhang R, Zhan H, Wang X. Prognosis of gastric cancer patients with node-negative metastasis following curative resection: outcomes of the survival and recurrence. Can J Gastroenterol. 2008;22(10):835–839. doi:10.1155/2008/761821
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of the Clinical Efficacy of Intensity-Modulated Radiotherapy Combined with Transcatheter Arterial Chemoembolization for Hepatocellular Carcinoma with Extrahepatic Oligometastasis and Prognostic Factors for Patient Survival
Luo Y, Huang X, Chen J, Zhang S
International Journal of General Medicine 2023, 16:1271-1278
Published Date: 12 April 2023
Survival in Thyroid Cancer in Sweden From 1999 To 2018
Zitricky F, Koskinen A, Sundquist K, Sundquist J, Liska V, Försti A, Hemminki A, Hemminki K
Clinical Epidemiology 2024, 16:659-671
Published Date: 2 October 2024
Magnetic Resonance Imaging Radiomics-Based Model for Prediction of Lymph Node Metastasis in Cervical Cancer
Shi Z, Lu L
International Journal of General Medicine 2025, 18:1371-1381
Published Date: 7 March 2025
Effectiveness of Palliative Chemotherapy and Associated Prognostic Factors in Advanced Small Bowel Adenocarcinoma: A Propensity Score-Matched Analysis
Wonglhow J, Dechaphunkul A, Sathitruangsak C, Sunpaweravong P, Wetwittayakhlang P
Cancer Management and Research 2025, 17:2893-2903
Published Date: 25 November 2025