")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Respiratory Symptoms, Disease Burden, and Quality of Life in Australian Adults According to GOLD Spirometry Grades: Data from the BOLD Australia Study
Authors Zhou Y , Ampon MR, Abramson MJ , James AL, Maguire GP, Wood-Baker R, Johns DP, Marks GB , Reddel HK , Toelle BG
Received 13 July 2023
Accepted for publication 30 October 2023
Published 30 November 2023 Volume 2023:18 Pages 2839—2847
DOI https://doi.org/10.2147/COPD.S425202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Yijun Zhou,1 Maria R Ampon,2 Michael J Abramson,3 Alan L James,4 Graeme P Maguire,5 Richard Wood-Baker,6 David P Johns,6 Guy B Marks,1,7 Helen K Reddel,2,8,9 Brett G Toelle1,8,9
1The Woolcock Institute of Medical Research, The University of Sydney, Sydney, NSW, Australia; 2Australian Centre for Airways Disease Monitoring, The Woolcock Institute of Medical Research, The University of Sydney, Sydney, NSW, Australia; 3School of Public Health & Preventive Medicine, Monash University, Melbourne, VIC, Australia; 4Sir Charles Gairdner Hospital, Perth, WA, Australia; 5Curtin Medical School, Curtin University, Perth, WA, Australia; 6Melbourne School of Population and Global Health, University of Melbourne, Melbourne, VIC, Australia; 7South Western Sydney Clinical School, University of New South Wales, Sydney, NSW, Australia; 8Faculty of Medicine, Health and Human Science, Macquarie University, Sydney, NSW, Australia; 9Sydney Local Health District, Sydney, NSW, Australia
Correspondence: Brett G Toelle, Woolcock Institute of Medical Research, 431 Glebe Point Road, Glebe, NSW, 2037, Australia, Email [email protected]
Purpose: Population data on the burden of chronic obstructive pulmonary disease (COPD) are often based on patient-reported diagnoses of COPD, emphysema or chronic bronchitis, without spirometry. We aimed to investigate the relationship between health burden, quality of life and severity of airway obstruction in Australian adults aged ≥ 40 years.
Methods: We used data from the BOLD Australia study, which included randomly selected adults aged ≥ 40 years from six study sites to reflect the sociodemographic and geographic diversity of the Australian population (n = 3522). Participants with post-bronchodilator airflow limitation (ratio of forced expiratory volume in 1 second FEV1 to forced vital capacity < 0.7) were grouped by GOLD spirometry grades 1– 4. Quality of life was assessed with Short Form 12 (SF-12) Health Survey Questionnaire. Health burden was assessed as lost time off work or social activities, and healthcare utilization.
Results: Of the study sample, 2969 participants did not have airflow limitation, 294 (8.4%) were classified as GOLD Grade 1, 212 (6.0%) as GOLD 2 and 43 (1.2%) as GOLD 3– 4. Participants with higher GOLD grades had more respiratory symptoms, more comorbidities and greater burden than those with lower GOLD grades. The scores of mental and physical subscales of SF-12 were lower, indicating worse quality of life, from the no airflow limitation group to the GOLD 3– 4 group (P = 0.03 and P < 0.001, respectively).
Conclusion: Greater airflow limitation is associated with greater burden and poor quality of life. Interventions to prevent, or reduce the level of, airflow limitation will reduce the symptom burden and improve quality of life for patients.
Keywords: chronic obstructive pulmonary disease, airflow limitation, comorbidities, The Burden of Obstructive Lung Disease, quality of life
Introduction
Chronic obstructive pulmonary disease (COPD) is the most prevalent chronic respiratory disease that leads to a significant burden on health.1 In 2017, COPD was the seventh leading cause of global disability.2 In 2019, COPD caused 3.23 million deaths globally, making it the third leading cause of death.3 In Australia, COPD was one of the top 5 leading causes of death; there were 7113 deaths due to COPD in 2018, and COPD was the third leading cause of overall disease burden in Australia in 2015.4,5 Moreover, COPD is associated with multimorbidity including osteoporosis, diabetes, hypertension, cardiovascular disease, depression, and lung cancer.1,6–8
Because of the significant worldwide burden of COPD, the Global initiative for chronic Obstructive Lung Disease (GOLD) has created evidence-based guidelines that are updated annually.1 According to the self-reported data from the 2017–18 Australian Bureau of Statistics (ABS) National Health Survey (NHS), approximately 4.8% of Australians aged 45 years and over have COPD.9 The weighted prevalence of COPD in Australians, based on the ratio of post-bronchodilator forced expiratory volume in 1 second to forced vital capacity (FEV1/FVC) <0.7, was estimated to be 8.3% in adults aged 40+ years, and 19.8% in adults aged 75+ years.10 Although COPD is relevant in Australia and associated with a significant health burden, previous Australian studies have not reported indirect burdens such as lost time off work or social activities and healthcare utilization in community-living patients with a diagnosis of COPD based on GOLD spirometric criteria. Indeed, core Australian data on COPD from the Australian Institute of Health and Welfare (AIHW) come from surveys in which people with COPD are identified only by self-reporting a diagnosis of COPD, emphysema or chronic bronchitis, without lung function testing.4
COPD is a highly symptomatic disease that requires symptom-based treatments.1 The physical and emotional symptoms of COPD are known to have a negative impact on the quality of life in patients.11 Because COPD is irreversible and progressive, quality of life is a useful tool for assessing COPD severity and treatment outcomes.
The Burden of Obstructive Lung Disease (BOLD) Australia study collected measures of lung function by spirometry and self-reported outcomes by questionnaires including indirect burdens (defined as lost time off work or social activities and healthcare utilization), respiratory symptoms, comorbidities, and quality of life.12 Although the GOLD 2023 report1 has proposed an assessment tool based on symptoms and exacerbation history, the BOLD Australia database did not have complete information on the ABE assessment tool, especially the exacerbation history and the Australian and New Zealand guidelines for the management of COPD (COPD-X)13 has not yet adopted the ABE classification. BOLD Australia could still provide an opportunity to more thoroughly understand the impacts of different GOLD grades of airflow limitation in Australians aged ≥40 years.
Our study aimed to investigate the relationship between health burden and different GOLD grades of severity of airflow limitation in Australian adults aged ≥40 years.
Methods
Sample
We used data from the BOLD Australia study, which is the largest geographically diverse population-based study of spirometrically confirmed COPD in Australia. It was a cross-sectional study conducted between 2006 and 2012 of individuals aged ≥40 years from six study sites across Australia, including Sydney, rural New South Wales, Melbourne, Tasmania (Hobart and Launceston) and Busselton and Broome in Western Australia.12 In Western Australia, participants were recruited from a household census data in Broome and local aboriginal communities within the Kimberley region or were randomly recruited from the Busselton Health Study. The study design and detailed information for the sample selection were published previously.12,14 Participants who were not contactable, institutionalized, or aged younger than 40 years were excluded. Participants in the BOLD Australia study who were missing spirometry test results were excluded from these analyses. Data for all six Australian sites are included in this analysis; some results from the Sydney site have been published previously in an analysis of data from 17 BOLD countries.15
Description of Variables
All participants completed the BOLD core questionnaire that included details of demographics, smoking status, occupational exposures, respiratory medication use, and respiratory symptoms (Supplementary Information S1).12,16 Socioeconomic status was reported by using quintiles of Socio-Economic Indexes for Areas (SEIFA), with SEIFA 1 being the “most disadvantaged” and SEIFA 5 being the “least disadvantaged” area.17 Occupational exposures were reported as having worked in a dusty job for at least 1 year.
Respiratory symptoms included cough, phlegm, wheeze, and breathlessness. Activity limitation due to breathlessness was measured by the modified Medical Research Council (mMRC) dyspnoea scale.18 We defined “linically important breathlessness” as mMRC dyspnoea grade ≥2. Specific comorbidities reported were asthma, heart disease, hypertension, diabetes, lung cancer, and stroke. The disease-related indirect burdens reported were lost time off work or social activities, and healthcare utilization. Healthcare utilization included visits to a general practitioner (GP) and hospitalizations in the last 12 months, due to breathing problems.
Quality of life was reported as domain scores of the Short-Form (SF)-12 questionnaire.19 The BOLD Australia survey did not collect the answer to all SF-12 questions for Indigenous participants, those participants only answered the first question in the SF-12 questionnaire (“In general, would you say your health is ….”). Thus, we use the result of the first question (SF-1) in the SF-12 to define self-reported general health status. We defined participants who reported excellent, very good, and good as good or above general health. Since there were no Australian norms available, the physical and mental component summary scores (PCS, MCS) of SF-12 were computed using US norms.19
Spirometry was measured according to the American Thoracic Society/European Respiratory Society standards, using the EasyOne spirometer (ndd Medizintechnik, Zürich, Switzerland).12,16 All spirograms were reviewed and quality graded by a senior respiratory scientist.12 The highest recorded post-bronchodilator forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) from acceptable trials20 were collected. Spirometry predicted values were calculated using the Global Lung Function Initiative (GLI) reference equations.21 Caucasian predicted values were used. The severity of airflow limitation was graded using the GOLD criterion for COPD (post-bronchodilator FEV1/FVC ratio <0.70): mild, GOLD 1, FEV1 ≥ 80% predicted; moderate, GOLD 2, 50% ≤ FEV1 < 80% predicted; severe or very severe, GOLD 3 or 4, FEV1 < 50% predicted.1
Statistical Analysis
All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC). The study population was grouped according to GOLD spirometry grades (No airflow limitation, GOLD 1, GOLD 2, and GOLD 3–4). Data are presented as numbers with proportions for categorical variables and means ± standard deviations (SD) or median with interquartile range [IQR] for continuous variables. The differences between groups were assessed using χ2 tests for categorical variables, analysis of variance for continuous variables that followed normal distributions, and Wilcoxon rank-sum tests for continuous variables that did not follow normal distributions. A p-value <0.05 was considered statistically significant.
A multivariate logistic regression model was used to analyze general health by the severity of airflow limitation, and multiple linear regression was used in the multiple variable analyses with PCS and MCS. In this analysis, the selection of potential confounders for adjustment was based on a causal inference approach, using Directed Acyclic Graphs (DAGs). As shown in Figures S1–S3, these identified age, sex, body mass index (BMI) status, smoking status, socioeconomic status, heart disease, hypertension, and diabetes as potential confounders, because they may open a back-door pathway association between exposure and outcome, therefore, should be adjusted for in the analyses.22
Results
From among 10760 eligible participants in the BOLD Australia study,12 3518 (32.7%) participants with acceptable pre- and post-bronchodilator spirometry results were included in the present analysis. Using minimal information data collected from those who chose not to participate, we found that the sample included in this analysis was younger and more likely to have self-reported diagnosed respiratory disease. Among all participants, 2969 (84.4%) did not have airflow limitation, 294 (8.4%) were classified as GOLD stage 1, 212 (6.0%) GOLD 2 and 43 (1.2%) GOLD 3 or 4.
Table 1 describes the demographic characteristics of all participants. The characteristics of age, gender, ethnicity, smoking status, BMI status, highest education, and experience of working in a dusty job were significantly different among the four groups. However, there were no significant differences in socioeconomic status among the four groups.
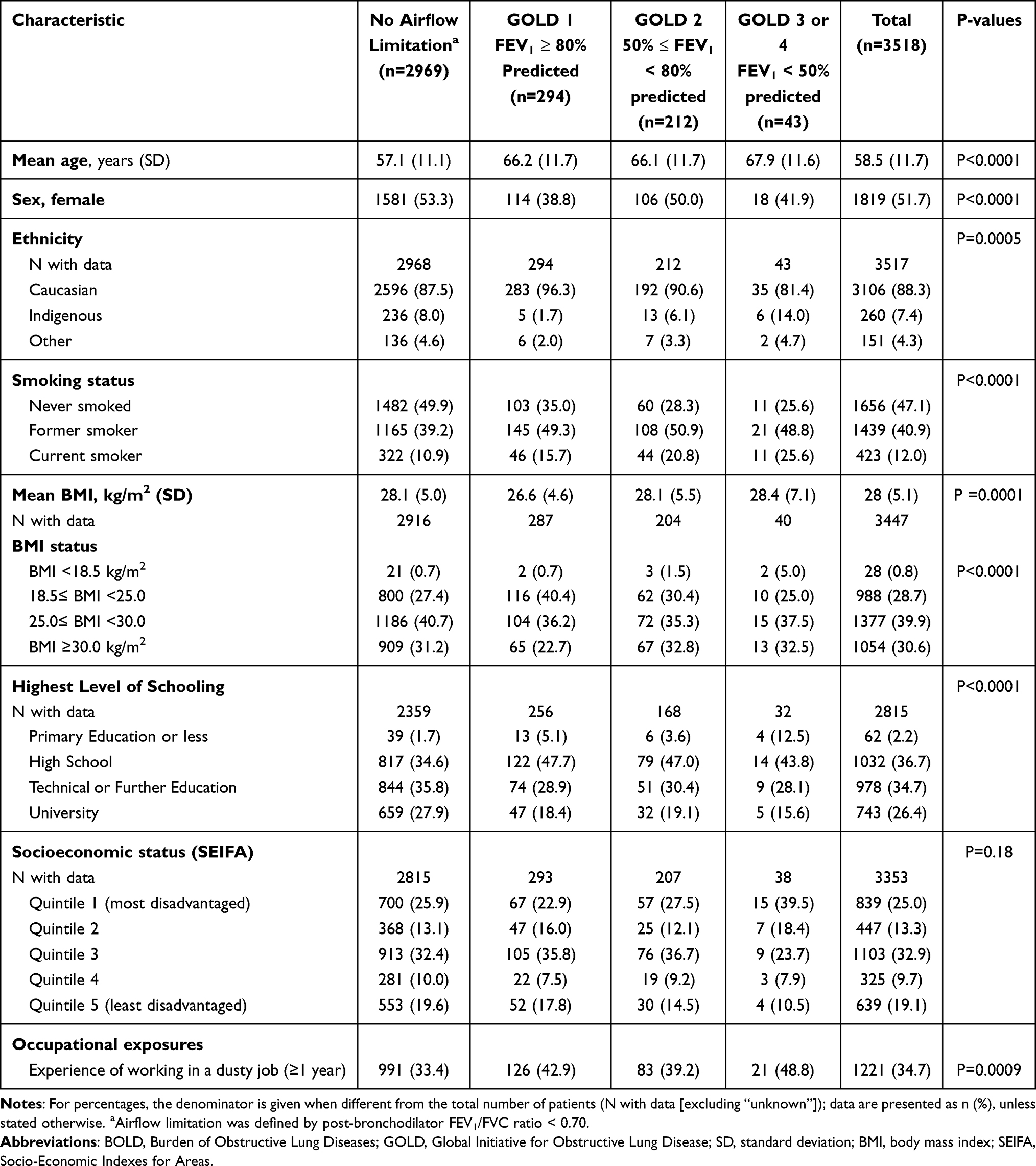 |
Table 1 Demographic Characteristics of the BOLD Australia Sample, by GOLD Spirometric Grades |
From the no airflow limitation group to the GOLD 3 or 4 group, the proportions having any of the self-reported respiratory symptoms were increased, and there were significant differences across the four groups (Table 2). Almost three quarters (72.1%) of the GOLD 3 or 4 group reported using respiratory medications, compared with 41.5% of those with GOLD 2 and 20.4% of GOLD 1. The proportions of having current asthma, hypertension, diabetes, lung cancer, stroke, and having 2 or more comorbidities were reported most frequently in the GOLD 3 or 4 group, followed by GOLD 2, GOLD 1, and no airflow limitation groups (Table 2). Only the GOLD 2 group reported a higher proportion of having heart disease compared to the GOLD 3 or 4 group.
 |
Table 2 Respiratory Symptoms Respiratory Medication Use and Comorbidities of the BOLD Australia Sample, by GOLD Spirometric Grades |
Participants with GOLD 3 or 4 reported the highest proportions of lost time off work or lost time for social activities (25.6%), and healthcare utilization (25.8% for GP visits and 5.9% for hospitalizations), followed by GOLD 2, GOLD 1, and no airflow limitation groups (Table 3). However, although the proportion of healthcare utilization varied across groups, among those who had reported any healthcare utilization, there were no significant differences in the median number of GP visits or median number of hospitalizations across the four groups.
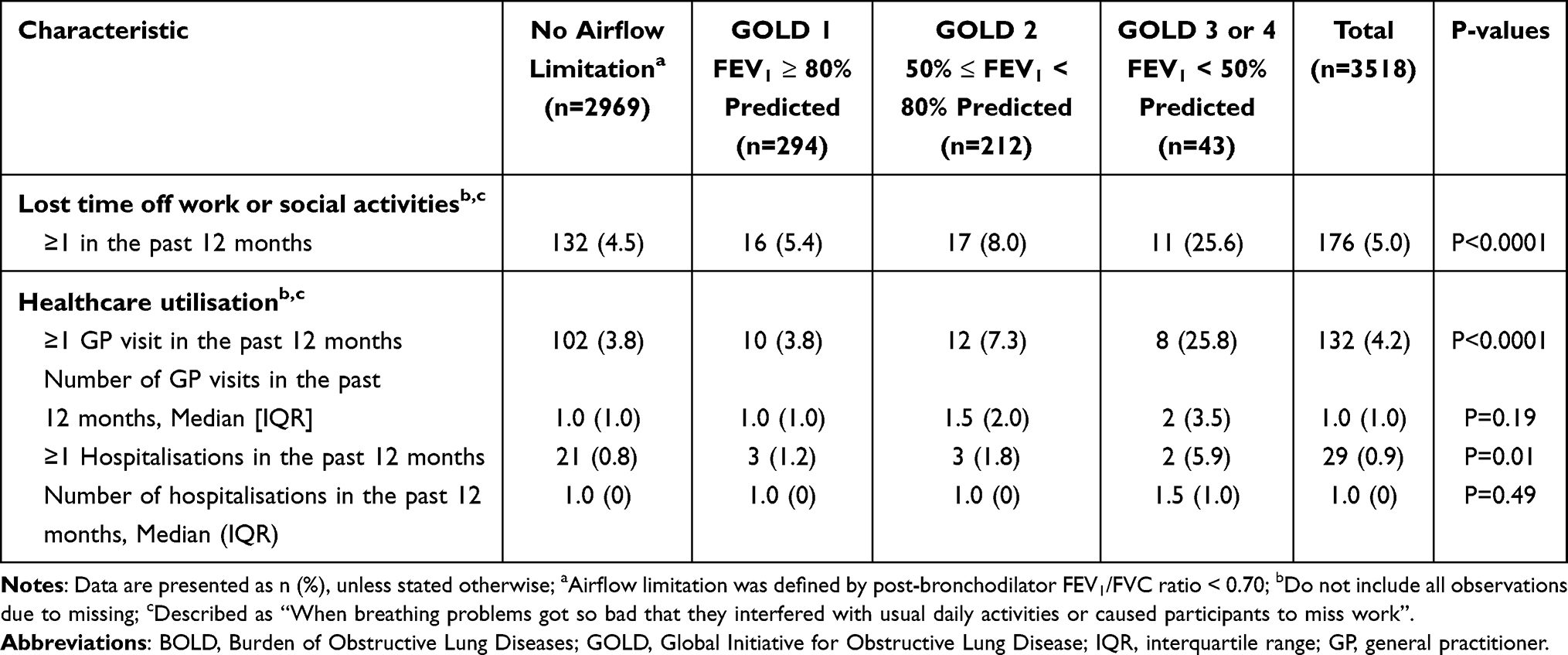 |
Table 3 Lost Time from Work/Social Activities and Hospital/GP Visits of the BOLD Australia Sample, by GOLD Spirometric Grades |
Quality of life among the four groups is compared in Table 4. Regarding general health, the no airflow limitation group reported the highest proportion of excellent general health and the lowest proportion of poor general health, while the GOLD 3 or 4 group reported the lowest proportion of excellent and highest proportion of poor health. The proportion of self-reported good or above general health decreased as airflow limitation became worse across the groups. The PCS and MCS also decreased from the no airflow limitation group to the GOLD 3 or 4 group.
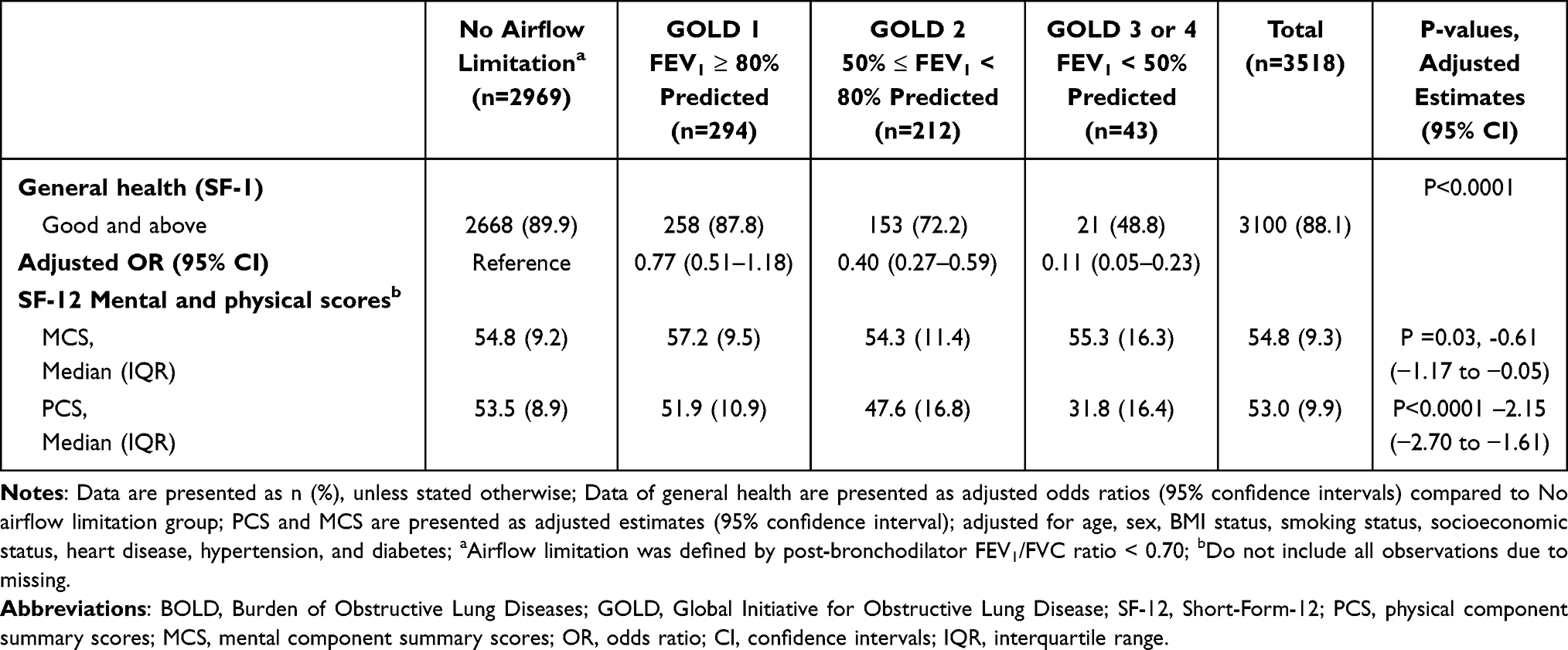 |
Table 4 Quality of Life (SF-12) of the BOLD Australia Sample, by GOLD Spirometric Grades |
Discussion
To our knowledge, this is the first Australian study to evaluate the relationship between respiratory symptoms, comorbidities, indirect health burdens, quality of life, and GOLD spirometry grades in a general population sample including healthy subjects and subjects with COPD. We found, in adults aged ≥40 years, that presence of respiratory symptoms and respiratory medication use was associated with worse airflow limitation. The likelihood of multimorbidity and disease-related indirect burden (lost time off work or social activities and healthcare utilization) also increased with worsening/increasing airflow limitation. Additionally, the quality of life evaluated by SF-12, including general health SF-1, MCS, and PCS, deteriorated as the GOLD spirometry grade severity worsened. However, the mental component scale (MCS) did not deteriorate as much as the GOLD spirometry grade severity worsened.
We found that the proportions of people having any respiratory symptoms and using respiratory medications were progressively higher from the no airflow limitation group to the GOLD 3 or 4 group. However, we found that large proportions of participants in the GOLD 2 and GOLD 3 or 4 group (post-bronchodilator FEV1 < 80% predicted) did not receive any respiratory medication treatment in the past 12 months. The reason for these COPD patients not receiving respiratory medication may be misdiagnosis or underdiagnosis, as reported in the BOLD Australia study,23 and as also observed internationally.24,25 These findings help confirm the importance of spirometry in the diagnosis of COPD in real-life clinical practice, especially in primary care.
A previous global BOLD paper reported that participants with airflow limitation (GOLD 1 to 4) were more likely to suffer from heart disease, hypertension, and stroke than those without COPD, and only having diabetes had a weak association between participants with and without COPD, consistent with our findings.15 Previous studies found that patients with both asthma and COPD had worse lung function,26 we also found that the proportion having current asthma was increased from participants without airflow limitation to GOLD 3 or 4.
Previous studies found that adults with COPD had more work absences than the general population.27 We also showed a trend toward increased time lost from work or daily activities with higher GOLD spirometry grades. We observed that the proportion of healthcare utilization increased across grades of airflow limitation, as observed previously.28 However, for participants who visited GPs or hospitalizations in 12 months, the number of GP visits and hospitalizations was not significantly different across the four groups. These results may be attributed to the small number of participants in the GOLD 2 and GOLD 3 or 4 group.
We found that general health was independently associated with the severity of GOLD spirometry grades. The proportion of participants reporting good or above general health status significantly decreased from participants without airflow limitation to participants with GOLD 3 or 4. Previous studies also reported that COPD is related to poorer health status.15 We also observed that the negative impact on quality of life increased with increasing severity of GOLD spirometry grades, which has also been reported previously.15,28 The impact of COPD was greater on the physical than the mental aspects of quality of life, which was similar to previous studies.15,29
The main strengths of this study included the data from a large nationwide population sample, the use of standardized methods of data collection, together with a high level of quality control, increasing the internal validity of the analyses.12,16 The study protocol and core questionnaire were harmonized with the BOLD international protocol, allowing for comparisons between countries.30
However, our study also had several limitations. The cross-sectional design did not allow for the assessment of causality or long-term outcomes. The low overall response rate may introduce the possibility of selection bias, with participants included in this analysis being slightly younger and more likely to self-report a diagnosis of respiratory disease compared with those who provided only minimal data.12 The GOLD 2023 report introduced an ABE assessment tool to assess the severity of COPD, but the BOLD Australia dataset did not include complete information about exacerbations required by the GOLD ABE assessment tool. Thus, we used the GOLD spirometry grades to assess the severity of COPD in our analysis. BOLD Australia also did not collect data on depression, which has been confirmed to be associated with worse health status in patients with COPD.31
Another limitation was that the information on comorbidities in BOLD Australia was collected from the self-reported questionnaire, which could introduce recall bias. The BOLD Australia data did not include the answer to all SF-12 questions for Indigenous participants, so we could not calculate the MCS and PCS of those participants. Participants were not a completely random sample of the Australian population as the six study sites themselves were not randomly selected. Another limitation is that the BOLD Australia study was conducted between 2006 and 2012, the study data is old and could not provide recent information. However, post-hoc weights were used in previous work to adjust prevalence estimates to reflect the Australian population better; in this analysis sample prevalence estimates were used.12 Finally, the single spirometry measurement was also a limitation as spirometry results can vary between days, resulting in differences in diagnostic criteria.32
Nonetheless, our findings have significant implications for the development of COPD management strategies. These findings confirm the value of the GOLD grades of airflow limitation for providing insight into the impact and burden of COPD. Therefore, the GOLD grades of airflow limitation remain important to health professionals in clinical practice. Further research should include information on the exacerbation history, which may provide a more comprehensive indication of the impact of different severities of COPD. Further research is also needed to improve prevention and treatment strategies for airflow limitation, which may help to reduce future long-term risks. Patients with COPD may benefit from improved interventions in the future.
Conclusion
This study comprehensively characterized respiratory symptoms, disease-related indirect burdens, and quality of life in Australian adults aged 40 years and over, according to GOLD spirometry grade. Adults with greater severity of airflow limitation, as indicated by higher GOLD grades, had more frequent respiratory symptoms and comorbidities compared with those with lower grades or without airflow limitation. The severity of airflow limitation was also associated with indirect burdens in terms of lost time off work or social activities, and healthcare utilization. Additionally, higher severity of airflow limitation was related to a lower quality of life. The effects of different airflow limitation grades on the physical aspects of quality of life were stronger than on the mental aspects. These findings confirm the utility of the GOLD spirometry grades for providing insight into the impact and burden of COPD. Most importantly, there was significant variation across the GOLD grades, especially with regard to the use of respiratory medicines.
Data Sharing Statement
The data that support the findings of this study are available at reasonable request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Human/Animal Ethics Approval Declaration
The BOLD Australia Study was approved by the Human Research Ethics Committee of the University of Sydney (ref. no. 12-2006/9724) and complies with the Declaration of Helsinki. Each study site also obtained local HREC approval, including approval from the Western Australian Aboriginal Health Information and Ethics Committee. Informed participant consent was obtained as per site-specific ethics approvals.
Acknowledgments
The BOLD study in Australia was funded by the National Health & Medical Research Council, Project Grant 457385. The BOLD study in Sydney was funded by grants from Air Liquide P/L, AstraZeneca P/L, Boehringer Ingelheim P/L, GlaxoSmithKline Australia P/L and Pfizer Australia P/L.
Operations Centre: Mrs Tessa E. Bird and Dr Wei Xuan (Woolcock Institute of Medical Research). Sydney: Professor Christine R. Jenkins, Mrs Tessa E. Bird, Dr Kate Hardaker and Dr Paola Espinel (Woolcock Institute of Medical Research).
Busselton: the late Professor A. W. (Bill) Musk, Dr Michael L. Hunter, Ms Elspeth Inglis and Ms Peta Grayson (University of Western Australia). Kimberley: Professor David N. Atkinson, Mr Dave Reeve, Dr Nathania Cooksley, Dr Matthew Yap, Ms Mary Lane, Dr Wendy Cavilla and Ms Sally Young (University of Western Australia). Melbourne: Ms Angela Lewis, Ms Joan Raven, Ms Joan Green and Ms Marsha Ivey (Monash University). Tasmania: Professor E. Haydn Walters, Mrs Carol Phillips and Ms Loren Taylor (University of Tasmania). NSW Rural: Dr Phillipa J. Southwell, Dr Bruce J. Graham, Dr Brian Spurrell, Mrs Robyn Paton, Ms Melanie Heine, Ms Cassandra Eccleston and Dr Julie Cooke (Charles Sturt University).
Disclosure
MJA holds investigator initiated grants from Pfizer, Boehringer-Ingelheim, Sanofi and GSK. He has conducted an unrelated consultancy for Sanofi. He has also received a speaker’s fee from GSK. MJA and RWB report cohort grants from the National Health & Medical Research Council. GBM has received funding for advisory boards with AstraZeneca. HKR holds investigator initiated grants from AstraZeneca, GlaxoSmithKline, Novartis, Perpetual Philanthropy. She has received consulting fees from AstraZeneca and GlaxoSmithKline and honoraria from AstraZeneca, GlaxoSmithKline, TEVA, Boehringer-Ingelheim, Sanofi, Getz, Chiesi and Alkem. HKR holds leadership roles in the Global Initiative for Asthma (GINA) and National Asthma Council (NAC). All other authors declare no competing interests in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for prevention, diagnosis and management of COPD: 2023 report. global initiative for chronic obstructive lung disease; [updated December 05, 2022]. Available from: https://goldcopd.org/2023-gold-report-2/.
2. Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1736–1788.
3. World Health Organization (WHO). Chronic obstructive pulmonary disease (COPD). WHO; 2023 [updated March 16 2023]. Available form: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
4. Australian Institute of Health Welfare. Chronic obstructive pulmonary disease (COPD), associated comorbidities and risk factors. AIHW. Available form: https://www.aihw.gov.au/reports/chronic-respiratory-conditions/copd-associated-comorbidities-risk-factors.
5. Australian Institute of Health Welfare. Australian burden of disease study 2015: interactive data on disease burden. AIHW. [updated 2020]. Available from: https://www.aihw.gov.au/reports/burden-of-disease/abds-2015-interactive-data-disease-burden.
6. Sarkar M, Bhardwaj R, Madabhavi I, Khatana J. Osteoporosis in chronic obstructive pulmonary disease. Clin Med Insights Circ Respir Pulm Med. 2015;9:S22803.
7. Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32(4):962–969. doi:10.1183/09031936.00012408
8. Yohannes AM, Alexopoulos GS. Depression and anxiety in patients with COPD. Eur Respir Review. 2014;23(133):345–349. doi:10.1183/09059180.00007813
9. Australian Bureau of Statistics (ABS). National health survey: first results. ABS. [Updated 2017-2018]. Available from: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/national-health-survey-first-results/latest-release.
10. Toelle BG, Ampon RD, Abramson MJ, et al. Prevalence of chronic obstructive pulmonary disease with breathlessness in Australia: weighted using the 2016 Australian census. Intern Med J. 2021;51(5):784–787. doi:10.1111/imj.15325
11. Viegi G, Pistelli F, Sherrill D, Maio S, Baldacci S, Carrozzi L. Definition, epidemiology and natural history of COPD. Eur Respir J. 2007;30(5):993–1013. doi:10.1183/09031936.00082507
12. Toelle BG, Xuan W, Bird TE, et al. Respiratory symptoms and illness in older Australians: the Burden of Obstructive Lung Disease (BOLD) study. Med J AU. 2013;198(3):144–148. doi:10.5694/mja11.11640
13. Dabscheck E, George J, Hermann K, et al. COPD‐X Australian guidelines for the diagnosis and management of chronic obstructive pulmonary disease: 2022 update. Med J AU. 2022;217(8):415–423. doi:10.5694/mja2.51708
14. Cooksley NA, Atkinson D, Marks GB, et al. Prevalence of airflow obstruction and reduced forced vital capacity in an Aboriginal Australian population: the cross‐sectional BOLD study. Respirology. 2015;20(5):766–774. doi:10.1111/resp.12482
15. Janson C, Marks G, Buist S, et al. The impact of COPD on health status: findings from the BOLD study. Eur Respir J. 2013;42(6):1472–1483. doi:10.1183/09031936.00153712
16. Buist AS, Vollmer WM, Sullivan SD, et al. The Burden of Obstructive Lung Disease initiative (BOLD): rationale and design. J Chronic Obstr Pulm Dis. 2005;2(2):277–283. doi:10.1081/COPD-57610
17. Australian Bureau Of Statistics. Socio-economic indexes for areas (SEIFA). Australian Bureau of Statistics; 2011.
18. Bestall J, Paul E, Garrod R, Garnham R, Jones P, Wedzicha J. Usefulness of the medical research council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
19. Kosinski M, Ware JE, Turner-Bowker DM, Gandek B. User’s Manual for the SF-12v2 Health Survey: With a Supplement Documenting the SF-12® Health Survey. QualityMetric Incorporated; 2007.
20. Miller M. ATS/ERS task force: standardisation of spirometry. Eur Respir J. 2005;26:319–338. doi:10.1183/09031936.05.00034805
21. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur Respiratory Soc. 2012;40:1324–1343.
22. Lederer DJ, Bell SC, Branson RD, et al. Control of confounding and reporting of results in causal inference studies. Guidance for authors from editors of respiratory, sleep, and critical care journals. Ann Am Thorac Soc. 2019;16(1):22–28. doi:10.1513/AnnalsATS.201808-564PS
23. Petrie K, Toelle BG, Wood-Baker R, et al. Undiagnosed and misdiagnosed chronic obstructive pulmonary disease: data from the BOLD Australia Study. Int J Chron Obstruct Pulmon Dis. 2021;16:467. doi:10.2147/COPD.S287172
24. Diab N, Gershon AS, Sin DD, et al. Underdiagnosis and overdiagnosis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(9):1130–1139. doi:10.1164/rccm.201804-0621CI
25. Reddel HK, Vestbo J, Agustí A, et al. Heterogeneity within and between physician-diagnosed asthma and/or COPD: NOVELTY cohort. Eur Respir J. 2021;58(3):2003927. doi:10.1183/13993003.03927-2020
26. Menezes AMB, de Oca MM, Pérez-Padilla R, et al. Increased risk of exacerbation and hospitalization in subjects with an overlap phenotype: COPD-asthma. Chest. 2014;145(2):297–304. doi:10.1378/chest.13-0622
27. Dierick BJ, Flokstra-de Blok BM, van der Molen T, et al. Work absence in patients with asthma and/or COPD: a population-based study. NPJ Prim Care Respir Med. 2021;31(1):9. doi:10.1038/s41533-021-00217-z
28. Choi HS, Yang D-W, Rhee CK, et al. The health-related quality-of-life of chronic obstructive pulmonary disease patients and disease-related indirect burdens. Korean J Intern Med. 2020;35(5):1136. doi:10.3904/kjim.2018.398
29. Varela ML, De Oca MM, Halbert R, et al. Sex-related differences in COPD in five Latin American cities: the PLATINO study. Eur Respir J. 2010;36(5):1034–1041. doi:10.1183/09031936.00165409
30. Buist AS, McBurnie MA, Vollmer WM, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370(9589):741–750. doi:10.1016/S0140-6736(07)61377-4
31. Gudmundsson G, Gislason T, Lindberg E, et al. Mortality in COPD patients discharged from hospital: the role of treatment and co-morbidity. Respir Res. 2006;7(1):1–8. doi:10.1186/1465-9921-7-109
32. Schermer TR, Robberts B, Crockett AJ, et al. Should the diagnosis of COPD be based on a single spirometry test? NPJ Prim Care Respir Med. 2016;26(1):1–8. doi:10.1038/npjpcrm.2016.59
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.