Back to Journals » Psychology Research and Behavior Management » Volume 18
Resilience Factors and Their Association with Anxiety and Depressive Symptoms: An Intergenerational Perspective
Authors Drapisz A, Walfisch R, Shilton T, Hertz-Palmor N ![]() , Dekel I, Mosheva M, Gothelf D, Barzilay R
, Dekel I, Mosheva M, Gothelf D, Barzilay R
Received 1 May 2025
Accepted for publication 1 December 2025
Published 12 December 2025 Volume 2025:18 Pages 2379—2386
DOI https://doi.org/10.2147/PRBM.S530960
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Adi Drapisz,1 Ron Walfisch,1 Tal Shilton,1 Nimrod Hertz-Palmor,2 Idit Dekel,1 Mariela Mosheva,1 Doron Gothelf,1 Ran Barzilay3– 5
1The Division of Child & Adolescent Psychiatry, the Edmond and Lily Safra Children’s Hospital, Sheba, Ramat Gan, Israel; 2MRC Cognition and Brain Sciences Unit, University of Cambridge, Cambridge, UK; 3Department of Psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 4Lifespan Brain Institute of Children’s Hospital of Philadelphia and Penn Medicine, Philadelphia, PA, USA; 5Department of Child and Adolescent Psychiatry and Behavioral Science, Children’s Hospital of Philadelphia, Philadelphia, PA, USA
Correspondence: Ran Barzilay, Department of Psychiatry, Perelman School of Medicine, University of Pennsylvania, Hospital of the University of Pennsylvania, 34th and Spruce Street, Philadelphia, PA, 19104, USA, Tel +1(484)6957937, Email [email protected]
Background: Characterizing variability in youth mental health trajectories from risk to resilience is crucial for elucidating the heterogeneity present within clinical populations. Limited knowledge exists regarding the intergenerational associations of resilience factors. The present study aimed to examine the associations between resilience factors and psychopathology in youth referred for outpatient psychiatric evaluation and their parents.
Methods: Dyads of children and their parents (N=99; 99 children and 99 parents) treated in a child and adolescent psychiatry outpatient clinic completed assessments for resilience factors and internalizing psychopathology. Internalizing symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9) and the Generalized Anxiety Disorder 7-item scale (GAD-7); resilience factors were measured using the Risk and Resilience (R&R) battery, focusing on self-reliance and emotion regulation.
Results: Youth’s emotion regulation and self-reliance demonstrated inverse associations with their anxiety and depressive composite score, derived by averaging standardized PHQ-9 and GAD-7 scores to represent internalizing symptoms (β=− 0.5, p < 0.0001; β=− 0.27, p = 0.001 respectively). Parental emotion regulation was inversely associated with parental anxiety and depressive symptoms (β=− 0.70, p < 0.0001), but parental self-reliance was not (β=0.04, p=0.67). No intergenerational correlation was identified between parent-child anxiety and depressive symptoms (P-values> 0.38) nor between resilience factors (P-values> 0.47). Lastly, multivariate analyses revealed no association for parental anxiety and depressive symptoms or resilience factors with child symptoms.
Conclusion: These findings contribute to the growing body of evidence on the relationship between the resilience factors of emotional regulation and self-reliance and anxiety-depression symptoms in youth. However, no intergenerational associations were observed between of resilience factors and internalizing psychopathology in both parents and youth.
Keywords: transgenerational resilience, self-reliance, emotion-regulation, depression, anxiety
Introduction
Clinicians and clinical researchers often focus on risk factors to understand developmental psychopathology. This focus, however, does not fully explain individual variation in mental health in the face of adversity.1 Resilience factors can provide further explanation of this variability.1,2 Resilience factors are constructs that contribute to resilience outcomes and act as protective factors against the development of mental health disorders.3 Better understanding of the factors that lead to resilience outcomes can be critical for prevention and early treatment of mental health conditions.1
Internalizing disorders such as anxiety and depression are among the most prevalent psychiatric conditions in children and adolescents, with lifetime prevalence estimates ranging from 10% to 20%.3,4 These disorders are associated with significant emotional distress, impaired functioning, academic difficulties, and increased risk for suicidality. While there is ample data on childhood anxiety and depression risk factors, less is known about their resilience factors.4
The existing data points to a few resilience factors in childhood, among them were relationships and caregiving, emotion regulation skills, self awareness and self reliance.1,4–6 Among youth hospitalized in psychiatric clinics, emotional resilience factors such as emotion regulation and self-reliance have been shown to play a key role in reducing distress and supporting recovery.7,8 The close environment can also harbor resilience factors, with parental factors highly contributing to risk or resilience trajectories in the child.7 Parental support has been shown to enhance emotional resilience in children through mechanisms such as consistent caregiving, emotional validation, and modeling of adaptive coping strategies.9 While resilience has been extensively studied within individuals, less is known about its potential intergenerational aspects, specifically, whether resilience-related characteristics in parents, such as emotion regulation and self-reliance, are associated with these factors and internalizing symptoms in their children.
Conversely, parental psychopathology or lack of emotional availability may undermine resilience and increase vulnerability to internalizing symptoms. Building on this, there is growing recognition of the intergenerational transmission of resilience, the ways in which adaptive traits and coping capacities may be conveyed from parents to their children through genetic, environmental, and relational mechanisms. In recent years, there’s a growing interest in intergenerational resilience, with much of the literature focused on Holocaust survivors and their families. Although historically specific, these studies provide valuable insight into intergenerational mechanisms of adaptation and coping relevant to broader population.8 Data shows that parental and offspring resilience, as an outcome, is positively related.9 There is little data regarding parent-child resilience factors’ correlation and their predictive value on child psychopathology.1 While prior studies have demonstrated associations between resilience factors and internalizing psychopathology, these relationships have rarely been examined in clinical outpatient populations or within an intergenerational framework. The current study therefore extends existing knowledge by investigating these associations among youth referred for psychiatric evaluation and their parents.8 To our knowledge, no prior studies have examined intergenerational correlations of resilience factors (self-reliance and emotion regulation) and their associations with psychopathology in a clinical outpatient youth population. This study proposed three specific hypotheses: (1) Higher levels of emotional regulation and self-reliance in both youth and parents would be associated with lower levels of anxiety and depressive symptoms; (2) emotion regulation and self-reliance would be positively correlated between parents and their children; and (3) Parental resilience factors and internalizing symptoms would be associated with those of their children.
Methods
Study Design and Sample
A cross-sectional study was conducted among youth and their parents attending the Child and Adolescent Psychiatry Outpatient Clinic at Sheba Medical Center, a tertiary care hospital in central Israel. Between June 11 and December 7, 2020, a total of 127 youth-parent dyads were approached prior to their first appointment at the clinic. Patients and parents completed the study’s assessments upon admission to the clinic. Exclusion criteria were intellectual disability (n=2), autism spectrum disorder (n=1), and psychotic spectrum disorders (n=1), patients chose not to participate in the study, 14 had incomplete data due to partial response of the questionnaires, thus were not included in the analysis. The final sample comprised 99 patients (aged 10–18 years) and their 99 parents.
Procedure
Patients and parents completed the study assessments at intake, prior to their first clinical appointment. After providing informed consent (and assent for youth), participants completed self-administered online questionnaires via a secure digital platform (Qualtrics). Parents also provided sociodemographic information. Both parents and youth completed the clinical questionnaires described in the Measurements section.
Ethics
All youth participants provided assent, informed consent was obtained from their parents. The study was approved by the Sheba Medical Center Institutional Review Board (SMC-7212-20).
Measurement and Procedures
Patients and parents completed self-administered online questionnaires online through a secured digital platform (Qualtrics). Parents provided sociodemographic information, including age, sex, educational attainment, household income, and recent employment change related to the COVID-19 pandemic.
Both parents and youth completed the following measures: (1) Depression screening was conducted using the Patient Health Questionnaire-9 (PHQ-9).10 The PHQ-9 consists of 9 items, each rated on a 4-point Likert scale from 0 (“not at all”) to 3 (“nearly every day”), yielding a total score ranging from 0–27. Scores between 5–9 indicate mild depression, 10–14 moderate, 15–19 moderately severe, and ≥20 severe depression. Internal consistency in the study sample was high, with Cronbach’s α values of 0.88 for youth and 0.87 for parents. (2) Anxiety screening using the Generalized Anxiety Disorder 7 questionnaire (GAD-7).11 The GAD-7 is a self-report measure that quantifies the frequency of seven anxiety symptoms over the past 2 weeks. Items are scored on a 4-point scale (0 = “not at all” to 3 = “nearly every day”), with total scores ranging from 0–21. Cut points of 5, 10, and 15, are interpreted as mild, moderate, and severe anxiety, respectively. (3) Resilience factors were evaluated using the Risk and Resilience (R&R) battery,12 which assesses seven domains: self-reliance, peer victimization, emotion regulation, positive and negative aspects in close relationships, neighborhood safety/cohesiveness and stressful life events. This tool has demonstrated acceptable internal consistency and construct validity in both youth and adult populations.12,13 In the study sample, the self-reliance and emotion regulation subscales also demonstrated acceptable internal consistency (Cronbach’s α values > 0.75 in both parents and youth). This study focused on the intrapersonal factors of self-reliance and emotion regulation, as these have shown strong associations with internalizing symptoms in prior research.1,14 Importantly, all instruments used in this study (PHQ-9, GAD-7, and the Risk and Resilience [R&R] battery) have been validated in adolescent and adult populations, including clinical samples, supporting their appropriateness for the present study population.10–13
Statistical Analysis
Sample characteristics were described using means and standard deviations for continuous variables, and percentages for categorical variables. Given the substantial comorbidity and shared underlying liability between depression and anxiety,15,16 standardized PHQ-9 and GAD-7 scores were averaged to create a composite “anxiety-depression” scale representing internalizing symptoms. This transdiagnostic composite is supported by prior work demonstrating overlapping genetic, clinical, and dimensional features of anxiety and depression and was used to enhance statistical power and minimize type I error.
Linear regression models were constructed to examine associations between resilience factors (self-reliance and emotion regulation) and internalizing symptoms in youth and parents. All models included age, sex, and parental socioeconomic status as covariates. Intergenerational associations were assessed using Pearson correlation coefficients and multiple regression analyses. Although hierarchical or multilevel modelling would better capture intergenerational data structures, the current exploratory study’s sample size limited this approach; therefore, standard linear regression models were used to examine within- and between-generation associations. Effect sizes with 95% confidence intervals were reported to aid interpretation and are presented in Tables 1–3. Statistical significance was set at α < 0.05. Analyses were conducted using IBM SPSS statistics version 25.0.
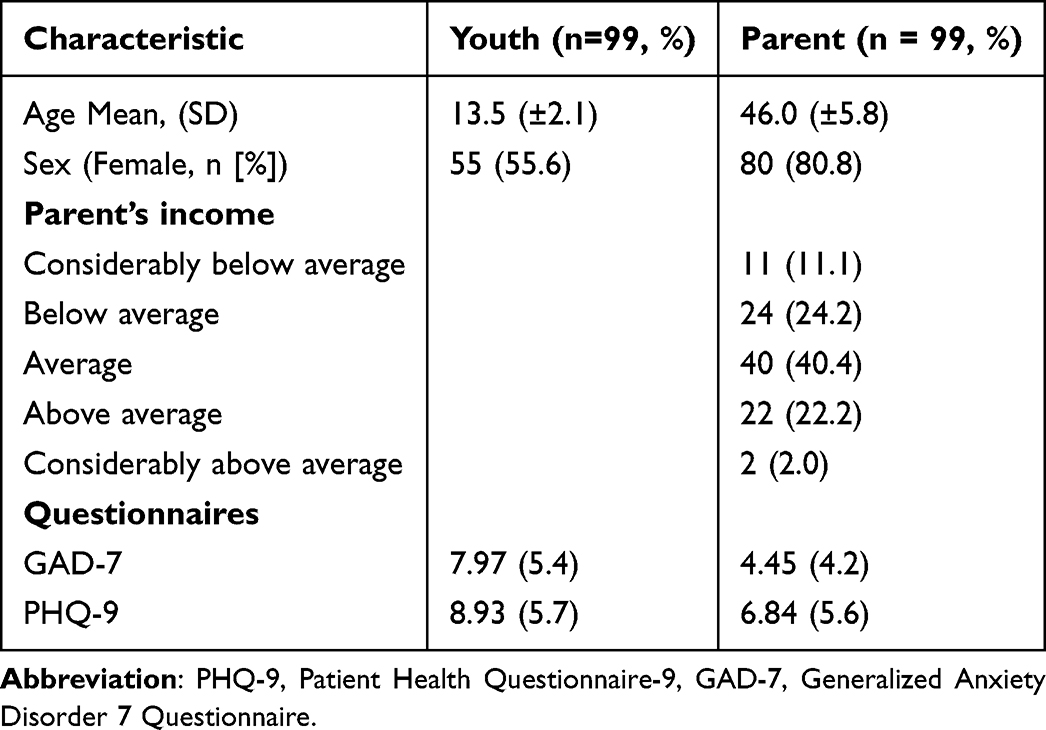 |
Table 1 Sociodemographic and Clinical Characteristics of the Study Sample (n = 99) |
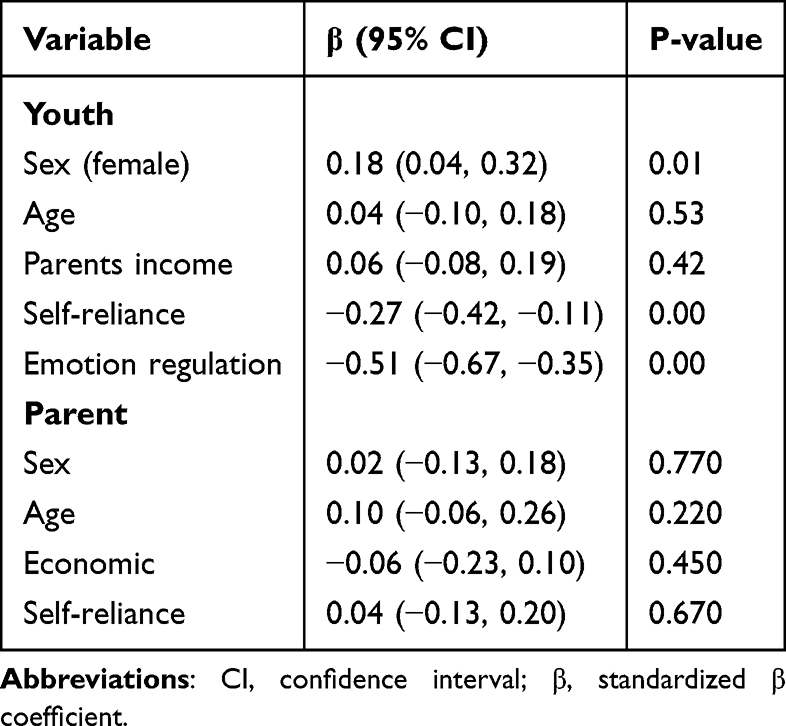 |
Table 2 Association of Sociodemographic Characteristics, Self-Reliance, and Emotion Regulation with Depression-Anxiety Scores: Results from Multiple Linear Regression Analysis |
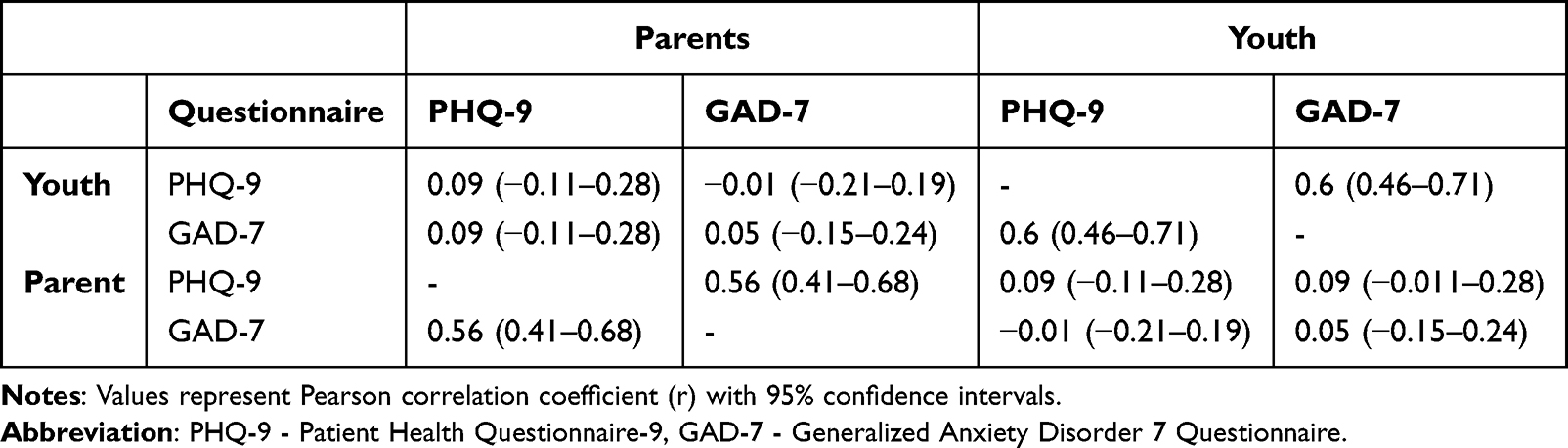 |
Table 3 Pearson Correlations Between Youth and Parent Anxiety and Depression Symptoms (n = 99) |
Results
Clinical and sociodemographic data including age, sex and parents’ income of the adolescent outpatients (n=99) and their parents (n=99) are shown in Table 4. On average, adolescents reported mild levels of anxiety and depression, while parents reported lower symptom levels. Although mean symptom scores reflected mild severity, all participants were referred to tertiary psychiatric care for specialized evaluation due to functional impairment, comorbid presentations, or persistent emotional and behavioral difficulties reported by caregivers or educational staff. Anxiety and depression scores were correlated in youth (r=0.6, p<0.01) and in parents (r=0.56, p<0.01). Two statistical models were constructed to assess the associations between resilience factors and symptoms of anxiety and depression in both youth and their parents. The first model demonstrated that resilience factors in youth were significantly inversely associated with anxiety and depressive symptomatology (emotion regulation, β=−0.51, 95% CI = −0.67, −0.35, p <0.0001; self-reliance,β=−0.27, 95% CI = −0.42, −0.11, p = 0.001) (Table 2). The second model indicated that, among parents, emotion regulation was significantly inversely associated with anxiety and depressive symptoms (β=−0.70, 95% CI=−0.85, −0.54, p <0.0001), whereas self-reliance was not (β=0.04, 95% CI = −0.13, 0.20, p=0.67) (Table 2).
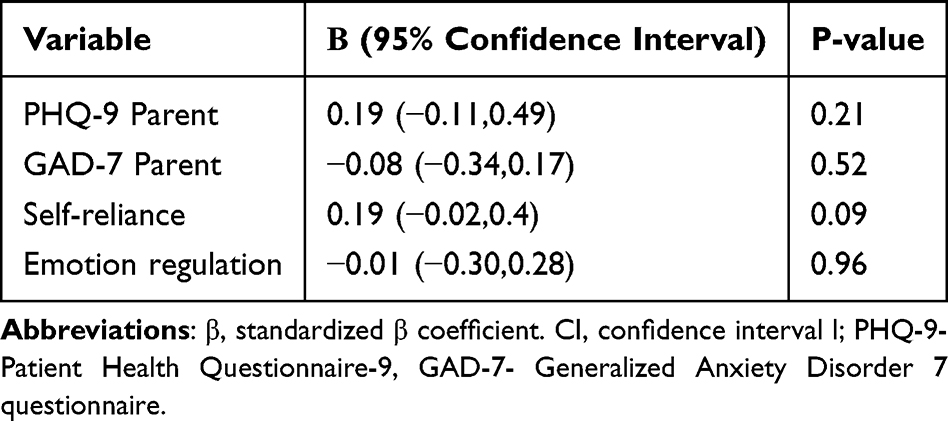 |
Table 4 Association Between Parent’s Psychopathology, Self-Reliance, Emotion Regulation in a Linear Regression Analysis with Youth’s Depression-Anxiety Scale as Dependent Variable |
Next, the study investigated intergenerational associations of anxiety-depression and resilience factors. There was no statistically significant correlation between youth anxiety or depression with the parents’ anxiety or depression (all p-values > 0.38) (Table 3).
Similarly, examination of resilience factors also showed no correlation between youth and parent self-reliance or emotion regulation (all p-values>0.47). Linear regression showed that neither parent anxiety or depression nor parents’ resilience factors were associated with youth anxiety and depressive symptoms (all p-values>0.09) (Table 4).
Discussion
This study describes the association of two resilience factors, emotion regulation and self-reliance, with anxiety and depressive symptoms in youth psychiatric outpatients and their parents. In line with this study hypothesis, youth emotion regulation and self-reliance exhibited inverse associations with anxiety and depressive symptoms. In parents, only emotion regulation was inversely associated with anxiety and depression, whereas self-reliance was not. Although resilience and emotion regulation are conceptually related, the R&R battery defines emotion regulation as one of several distinct resilience-related domains. Accordingly, while some conceptual overlap is expected, the observed associations likely reflect both shared and unique contributions to adaptive functioning. Emotion regulation and self-reliance are theoretically related constructs that both contribute to adaptive coping and resilience. Although some conceptual overlap may exist, the R&R battery operationalizes these as distinct subdomains with separate item structures and internal consistency. The present findings therefore suggest that both factors, while related, independently contribute to lower anxiety-depression symptoms rather than reflecting circularity. Contrary to the study hypothesis, no intergenerational associations of anxiety-depression and resilience factors was found. As this was a cross-sectional study, the analyses address intergenerational associations rather than transmission. Accordingly, causal inferences regarding the directionality or mechanisms of resilience across generations cannot be made. The findings regarding association between emotion regulation and anxiety-depression in both youth and parents strengthens and supports earlier works. Regarding self-reliance, results in youth are aligned with previous works in youth.17 These results extend prior work on resilience by moving beyond community and trauma-exposed populations to focus on youth referred for outpatient psychiatric evaluation, thereby providing unique evidence from a clinical sample. Resilience is influenced from both genetic and close environment.1,7 These interpretations should be viewed as plausible, hypothesis-generating perspectives rather than conclusive evidence, given the limitations of the study design. Therefore, one would expect parents’ and youth resilience factors to correlate. The lack of association between parent-child resilience factors and anxiety-depression may therefore be counterintuitive. There are several plausible explanations for this finding. As a multidimensional construct, resilience is composed of different variables, some stable over time and others may shift and be influenced by life circumstances and events.1,18 Given this notion, different resilience factors as shifting “states”, influenced by current circumstances, or as stable “traits”. The state/trait distinction may enable us to suggest alternative interpretations for the absence of intergenerational correlation observed. If resilience factors are conceptualized as “states”, it is possible that parents bringing their mental-health-help-seeking youth to receive treatment are under the influence of their current proactiveness that may strengthen their sense of self-reliance. If resilience factors as “traits”, it is reasonable to assume that youth characteristics are influenced by both parents. At the time of clinic intake, only the parent who accompanied the patient completed the questionnaires. It is plausible that this parent was the more resilient of the two. Another plausible interpretation of the intergenerational results may be related to the period the data was obtained. During the COVID-19 pandemic, the referrals were made by the parents, and not by educational staff, as in pre-pandemic era.19 This may mean that this study was biased to include “resilient parents”, who were able to use their resources and reach out to the psychiatric outpatient clinic to seek help for their children. Lastly, the dyads of parent-youth completing the questionnaires were outpatients, not the more acute patients from closed wards. It is possible that outpatients, who experience less severe psychopathology compared to inpatients, are children of more resilient parents with the ability to support and provide treatment preventing a deterioration in their youth ‘s condition. More research is needed on intergenerational effects in more severe clinical populations. Contrary to this study hypothesis and earlier studies, anxiety and depression were not intergenerationally associated in this study sample. It is widely accepted that genetic determinants of internalizing disorders are highly correlated.16,20 Studies show a strong association between parental depression and child anxiety and depression.21 If, as suggested above, there is a “resilient parent” bias, it may have influenced the present findings. Proactive parents who bring their youth referred for outpatient psychiatric evaluation to the clinic may have stronger sense of self-reliance, which has been associated with reduced risk for anxiety and depression.22
The results of this study should be considered within the context of several limitations. First, the sample size was limited and may have been underpowered to detect intergenerational effects. While post hoc power analysis confirmed sufficient power to detect medium effects, smaller intergenerational associations may have gone undetected, and the findings should be interpreted with caution given the cross-sectional nature of the design and limited sample size. In particular, the cross-sectional design does not allow conclusions about temporal or causal relationships and therefore cannot meaningfully distinguish between state and trait aspects of resilience. In addition, no control groups of either healthy controls or more severe inpatients, limiting generalizability of the study findings. Additionally, parent assessments were obtained from only one caregiver, which may have omitted important perspectives from the other parent and introduced bias, limiting the representativeness of family-wide dynamics. This study assessment focused on only two resilience factors, which may not capture the full complexity of the resilience construct. Moreover, reliance on self-report measures may introduce reporting bias; however, the instruments used are well-validated and widely applied in both clinical and research contexts. Formal psychodiagnostic interviews were not conducted, which may limit diagnostic precision, though the study focused on dimensional symptom measures and resilience factors across diagnostic categories. Finally, this was a cross-sectional study without longitudinal follow-up during or after treatment, which could have established and strengthen the relationship and directionality between parental and youth ‘s resilience and psychopathology. Taken together, these limitations constrain the generalizability of this study findings, which should be considered exploratory and require replication in larger, longitudinal, and more diverse samples.
In conclusion, this study strengthens the evidence suggesting emotion regulation and self-reliance as resilience factors for anxiety and depression in youth. Parental psychopathology and resilience factors were not associated with the youth’s psychopathology and resilience factors. Further research is warranted to elucidate the intergenerational dimensions of resilience and their underlying mechanisms.
Data Sharing Statement
Data available upon request.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board at Sheba Medical Center (7212-20-SMC). Informed assent/consent was obtained from the patients and their parents.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Dr. Barzilay is supported by the National Institute of Mental Health, grant numberK23MH120437. Nimrod Hertz-Palmor is supported by the Gates Cambridge Trust.
Disclosure
Dr Barzilay serves on the scientific boards and holds equity in “Taliaz Health”, outside of the submitted work. The authors report no other conflicts of interest in this work.
References
1. Southwick SM, Bonanno GA, Masten AS, Panter-Brick C, Yehuda R. Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur J Psychotraumatol. 2014;5(1). doi:10.3402/ejpt.v5.25338
2. Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. 2000;71(3):543–562. doi:10.1111/1467-8624.00164
3. Nauta MH, Festen H, Reichart CG, et al. Preventing mood and anxiety disorders in youth: a multi-centre RCT in the high risk offspring of depressed and anxious patients. BMC Psychiatry. 2012;12(1):31. doi:10.1186/1471-244X-12-31
4. Fritz J, de Graaff AM, Caisley H, van Harmelen AL, Wilkinson PO. A systematic review of amenable resilience factors that moderate and/or mediate the relationship between childhood adversity and mental health in young people. Front Psychiatry. 2018;9:9. doi:10.3389/fpsyt.2018.00230
5. Legault L, Anawati M, Flynn R. Factors favoring psychological resilience among fostered young people. Child Youth Serv Rev. 2006;28(9):1024–1038. doi:10.1016/j.childyouth.2005.10.006
6. Mestre JM, Núñez-Lozano JM, Gómez-Molinero R, Zayas A, Guil R. Emotion regulation ability and resilience in a sample of adolescents from a suburban area. Front Psychol. 2017;8:8. doi:10.3389/fpsyg.2017.01980
7. Osório C, Probert T, Jones E, Young AH, Robbins I. Adapting to stress: understanding the neurobiology of resilience. Behav Med. 2017;43(4):307–322. doi:10.1080/08964289.2016.1170661
8. Denov M, Fennig M, Rabiau MA, Shevell MC. Intergenerational resilience in families affected by war, displacement, and migration: “It runs in the family. J Fam Soc Work. 2019;22(1):17–45. doi:10.1080/10522158.2019.1546810
9. Shrira A, Mollov B, Mudahogora C. Complex PTSD and intergenerational transmission of distress and resilience among Tutsi genocide survivors and their offspring: a preliminary report. Psychiatry Res. 2019;271:121–123. doi:10.1016/j.psychres.2018.11.040
10. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
11. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder. Arch Intern Med. 2006;166(10):1092. doi:10.1001/archinte.166.10.1092
12. Moore TM, White LK, Barzilay R, et al. Development of a scale battery for rapid assessment of risk and resilience. Psychiatry Res. 2020;288:112996. doi:10.1016/j.psychres.2020.112996
13. White LK, Barzilay R, Moore TM, et al. Risk and resilience measures related to psychopathology in youth. Child Psychiatry Hum Dev. 2023;54(4):961–972. doi:10.1007/s10578-021-01296-2
14. Adrian M, Jenness JL, Kuehn KS, Smith MR, McLaughlin KA. Emotion regulation processes linking peer victimization to anxiety and depression symptoms in adolescence. Dev Psychopathol. 2019;31(3):999–1009. doi:10.1017/S0954579419000543
15. Barzilay R, White LK, Moore TM, et al. Association of anxiety phenotypes with risk of depression and suicidal ideation in community youth. Depress Anxiety. 2020;37(9):851–861. doi:10.1002/da.23060
16. Kendler KS, Gardner CO, Gatz M, Pedersen NL. The sources of co-morbidity between major depression and generalized anxiety disorder in a Swedish national twin sample. Psychol Med. 2007;37(3):453–462. doi:10.1017/S0033291706009135
17. Hussong AM, Midgette AJ, Thomas TE, Coffman JL, Cho S. Coping and mental health in early adolescence during COVID-19. Res Child Adolesc Psychopathol. 2021;49(9):1113–1123. doi:10.1007/s10802-021-00821-0
18. Ungar M, Theron L. Resilience and mental health: how multisystemic processes contribute to positive outcomes. Lancet Psychiatry. 2020;7(5):441–448. doi:10.1016/S2215-0366(19)30434-1
19. McNicholas F, Kelleher I, Hedderman E, et al. Referral patterns for specialist child and adolescent mental health services in the Republic of Ireland during the COVID-19 pandemic compared with 2019 and 2018. BJPsych Open. 2021;7(3):e91. doi:10.1192/bjo.2021.48
20. Shore L, Toumbourou JW, Lewis AJ, Kremer P. Review: longitudinal trajectories of child and adolescent depressive symptoms and their predictors – a systematic review and meta‐analysis. Child Adolesc Ment Health. 2018;23(2):107–120. doi:10.1111/camh.12220
21. Wickersham A, Leightley D, Archer M, Fear NT. The association between paternal psychopathology and adolescent depression and anxiety: a systematic review. J Adolesc. 2020;79(1):232–246. doi:10.1016/j.adolescence.2020.01.007
22. Karademas EC. Self-efficacy, social support and well-being. Pers Individ Dif. 2006;40(6):1281–1290. doi:10.1016/j.paid.2005.10.019
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Vitamin B12, Folate, Homocysteine, Inflammatory Mediators (Interleukin-6, Tumor Necrosis Factor-α and C-Reactive Protein) Levels in Adolescents with Anxiety or Depressive Symptoms
Tan Y, Zhou L, Huang J, Chen X, Wu Y, Song X, Wang J, Hu H, Yang Q
Neuropsychiatric Disease and Treatment 2023, 19:785-800
Published Date: 7 April 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025